Back to Journals » Infection and Drug Resistance » Volume 14
Knowledge, Attitude and Practice on Hospital-Acquired Infection Prevention and Associated Factors Among Healthcare Workers at University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia
Authors Bayleyegn B ![]() , Mehari A, Damtie D
, Mehari A, Damtie D ![]() , Negash M
, Negash M ![]()
Received 7 November 2020
Accepted for publication 11 January 2021
Published 27 January 2021 Volume 2021:14 Pages 259—266
DOI https://doi.org/10.2147/IDR.S290992
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Biruk Bayleyegn,1 Addisu Mehari,2 Debasu Damtie,3 Markos Negash3
1Department of Clinical Hematology and Immunohematology, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Department of Medical Laboratory Sciences, Debre-Markos University, Debre Markos, Ethiopia; 3Department of Immunology and Molecular Biology, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Biruk Bayleyegn
Department of Clinical Hematology and Immunohematology, College of Medicine and Health Sciences, University of Gondar, P.O. Box 196, Gondar, Ethiopia
Tel +251927607039
Email [email protected]
Background: Hospital-acquired infections can be acquired by a patient or develop among hospital staff, as a more serious problem in low- and middle-income hospital settings. Assessing the level of knowledge, attitude and practice towards hospital-acquired infection prevention among healthcare workers and identifying the associated factors has an unquestionable importance of handling and management of these infections. Thus, in this study, we evaluated the knowledge, attitude and practice towards HAIs prevention and associated factors in healthcare workers at the University of Gondar Comprehensive Specialized Hospital, North West Ethiopia.
Methods: Hospital-based cross-sectional study was conducted among healthcare workers towards HAIs prevention from January to June 2019. Each study participant was selected by simple random sampling. Data were collected using structured self-administered questionnaires. Descriptive analysis was used to present frequency and percentage of the main findings. The association between independent variables and KAP scores on HAI prevention was calculated using Pearson’s Chi square and p-values less than 0.05 were considered as statistically significant.
Results: A total of 236 participants were included in this study with a 100% response rate; 90% and 57.2% of the participants had good knowledge and positive attitude towards HAI prevention, respectively. Meanwhile, only 36% of the study participants had good practice towards HAI prevention, suggesting less than satisfactory scores in this study. Level of education and work experience were significantly associated with safe-infection prevention attitude and practice (P value < 0.005).
Conclusion: Even though the respondents have good knowledge with a sympathetic attitude about HAI preventions, good knowledge did not translate into prudent practices. Level of education and work experience were the independent risk factors towards HAI prevention of attitude and practice. Provision of continual on-job and off-job trainings together with strict implementation of updated standard operational procedures (SOP) may reduce the identified gap.
Keywords: hospital-acquired infection, knowledge, attitude and practice, healthcare workers
Background
Hospital-acquired infections (HAIs) are sometimes termed as nosocomial infections (NIs), which the patient acquires during his stay or healthcare workers (HCWs) get during their day-to-day hospital activities.1,2 Infections are considered nosocomial if they appear 48 to 72 hours after hospital admission or within 10 days after discharge.3
Healthcare workers acquire these infections during specimen collection, processing and discarding, handling and discarding of medical equipment as well as during patient to HCWs direct interaction at the time of examination.4–6 Nosocomial infection commonly results in urinary tract infection (UTI), surgical site infection, lower respiratory tract infections, bloodstream infection and other non-bacterial infections.7 However, in low- and-middle-income countries the most common healthcare associated infection was surgical site infection.8,9 Moreover, NI is a major public health concern and leads to prolonged hospital stay, long-term disability and even deaths.10
Hospital-acquired infection preventions are a guideline containing a multitude of protocols needed to be implemented by HCWs, thus greatly reducing the magnitude of HAIs. Several factors such as poor awareness among HCWs and compliance associated with personal, logistical and organizational barriers exert their own effect on proper application of these protocols.11,12 However, based on available evidence in Ethiopia, HCWs’ adherence towards infection prevention protocol is still very low.13,14
Healthcare associated HAI occurs worldwide and mainly affects low- and middle-income countries, which believed to be 5.7–19.1 times greater than that of developed world.15 The overall estimate indicated that more than 2.5 million cases of HAI occur each year in the developing and developed world,16 about 90% of the infections were occurring in a resource limited setting.13,17 Thus, the incidence of HAIs has increased elsewhere in the world, in high-income countries 5–15% of hospitalized patients acquire HCAIs which can affect from 9% to 37% of those admitted to intensive care units.18 Even though the problems associated HAIs are often hampered by inadequate data, the high burden of HAI in resource constrained countries like Asia, Latin America and sub-Saharan Africa has been reported to be more than 40%.19 According to several studies in Ethiopia, HAIs increased by more than two fold from 5.7% in 2009 to 19.41% in 2018 among patients20–22 and may lead to increased occupational risk among HCWs. The study also revealed that there was a high prevalence of both lifetime (28.8%) and one-year (20.2%) HAI exposure among HCWs23 which indicated serious concern for both patients and healthcare providers.
Hospital-acquired infection preventions are a process of placing a barrier between susceptible host and the microorganism which are an essential component of delivering safe and high-quality service at the facility level. Hence, HAI associated morbidity and mortality are preventable through infection prevention strategy like established representative infection control committee, good practice and safe procedure in proper waste handling, good sanitation, safety radiation and occupational protection.24–26
However, HAI prevention does not get enough attention in third world countries, including Ethiopia, particularly in the study area where the burden of infectious diseases is high. Therefore, this study was conducted to assess knowledge, attitude, practices and associated factors towards HAI prevention among HCWs at University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia. Information from this study will be submitted to the responsible body which will potentially assist in filling the gap towards HAI prevention application and indicate the measures to be taken to address the problem among HCWs HAI prevention.
Materials and Methods
Study Design, Period and Setting
Hospital based cross-sectional study was conducted among healthcare workers at the University of Gondar Comprehensive Specialized Hospital (UoGCSH) from January to June 2019. The hospital is found in Gondar town, Amhara region, 748 km from Addis Ababa, the capital of Ethiopia. Despite health service in Ethiopia is provided by governmental and nongovernmental (private) health institutions, the UoGCSH is a governmental teaching hospital, which provides teaching activities to medical and health science students and one of the oldest academic institutions in Ethiopia. It provides medical, surgical, psychiatric, and many other services to more than 5 million people of the Gondar province and the neighboring regions. The hospital has both inpatient, with more than 512 beds, and outpatient services.17 It also provides HIV/AIDS intervention activities in its ART clinic. The human resource report showed that UoGCSH has about 1200 workers and of these 613 were health related professionals during the study period.
Study Populations and Eligibility Criteria
All HCWs working at UoGCSH and who were potentially at high-risk – including doctors, nurses, health officers, anesthetics, physiotherapists, radiographers, pharmacists, laboratory scientists, midwives, optometrists and psychiatry – were considered as the source population. From all, HCWs who were full time employees of the hospital and had spent at least one year on the job were recruited in this study. Meanwhile, HCWs who were on annual, maternity and educational leave and those who were seriously ill and working at the administrative office during data collection period were excluded from the study.
Sampling Technique and Sample Size Determination
For this study the required number of study participants was calculated by using single population proportion and the final sample size was estimated to be 236 HCWs. Stratified sampling technique was applied to select the study unit proportionally and study participants were selected from each study unit by using simple random sampling procedure.
Data Collection Procedure and Quality Assurance
Data were collected using structured self-administered questionnaires that had been pre-tested on two health institutions. The questionnaire comprises of four sections that focus on socio demographic characteristics of study participants, seeking to ascertain the level of knowledge, attitude and practice towards HAI preventions. The data collection tool was first prepared in English, translated to Amharic (the local language) and then retranslated into English to check for consistency. Each possible answer was non-overlapping and necessary information was given to participants at the time of data collection. Before actual data collection, data collectors and supervisors were trained as well as supervisors and principal investigators strictly following the data collection process and giving feedback during the data collection period.
Operational Definition
Good knowledge: health workers who answered 70% of knowledge questions correctly. Poor knowledge: health workers who have answered less than 70% of questions concerning knowledge correctly. Favorable attitude: health workers have answered more than 70% of questions concerning the attitude favorably. Unfavorable attitude: health workers who have answered less than 70% of questions concerning the attitude favorably. Good practice: health workers who properly practiced 70% of practice questions. Poor practice: health workers who have practiced less than 70% of practice questions.27 Based on this cutoff value, a scoring system was used, 1 point was awarded for each correct response to good knowledge, favorable attitudes and good practices. Meanwhile, incorrect knowledge, negative attitudes and poor practices were given 0 points.
Statistical Analysis
The collected data were entered and cleaned using EPI Info 7.2.1 and analyzed by SPSS statistical software version 20. For the purposes of analysis, the outcome variables originally consisting of multiple categories were reduced to two levels. Univariant descriptive analysis was conducted by calculating frequency and percentage of the main findings. The association between independent variables and KAP scores on HAI prevention was calculated using Pearson’s Chi square. For all statistical tests, the decision was significant if the p-value is <0.05.
Result
Socio Demographic Characteristics
A total of 236 healthcare workers were participating in the study with a 100% response rate. Most respondents 143 (60.6%) were males and 102 (43.2%) were in the age range 26–30. Nurses, 148 (62.7%), were the most abundant participants based on their respective discipline and 131 (95.5%) of the HCWs have first Degree. Moreover, from the total 236 HCWs, majority of them (69.5%) have ≤ 5 years of work experience at UOGCSH (Table 1).
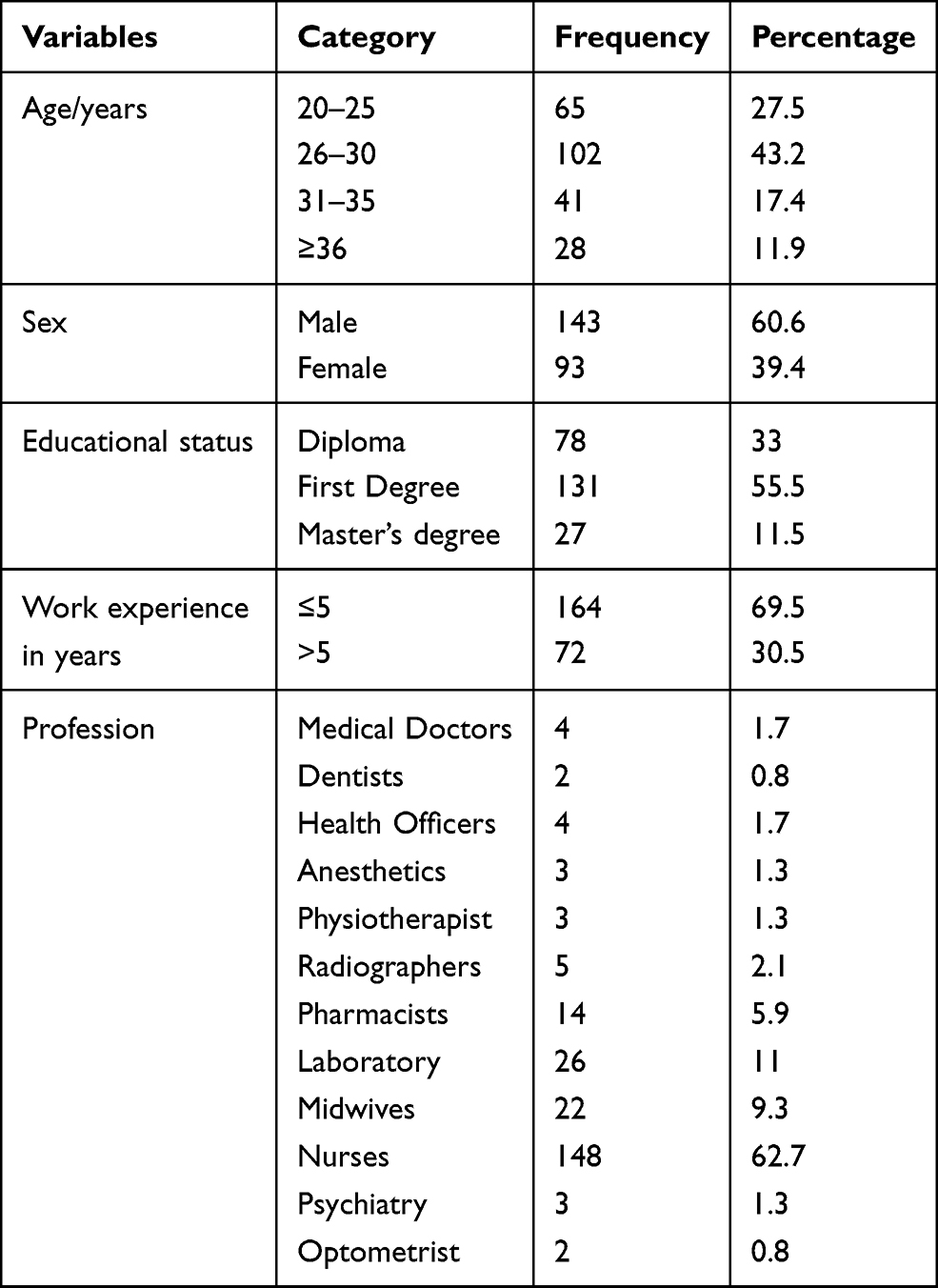 |
Table 1 Socio-Demographic Characteristics of Healthcare Workers at UoGCSH, Northwest Ethiopia, 2019 |
Knowledge of Healthcare Workers About HAI Prevention
In this study, the majority of respondents (90.2%) were found to be knowledgeable about HAI preventions. Among the study participants, the majority (96.6%) has better knowledge about the need for implementation of SOP in reduction of HAIs. Similarly, (95.3%) of the respondents know how NIs development is favored. Furthermore, more than 92% of study participants answered that hand washing before and after patient care and wearing personal protective equipment (PPE) were vital to prevent HAI (Table 2).
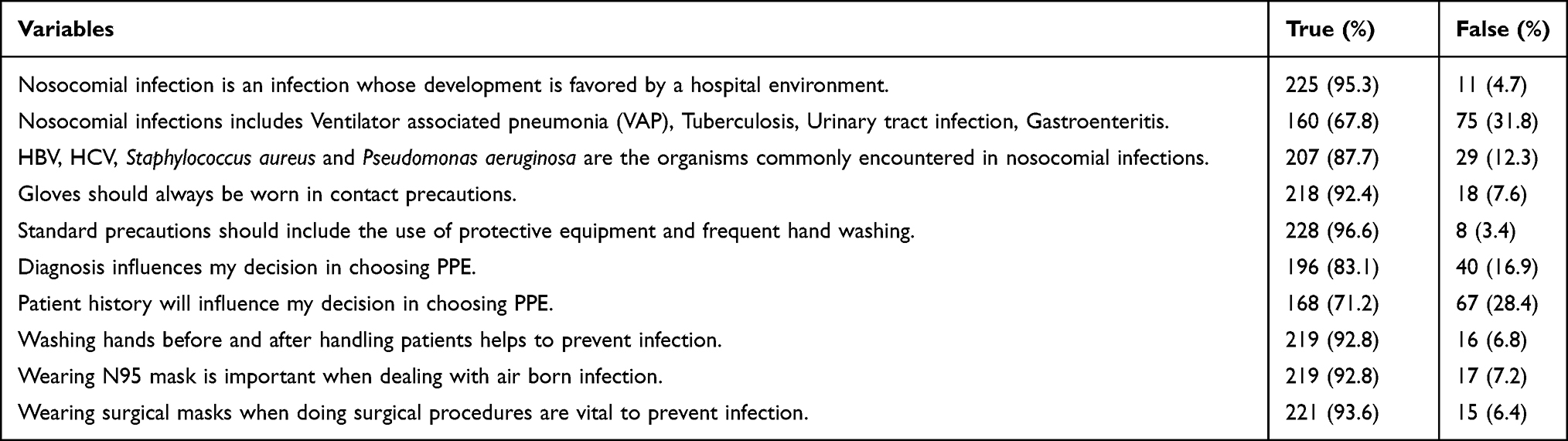 |
Table 2 Knowledge of Healthcare Workers About HAI Prevention at UoGCSH, 2019 |
Attitude of Healthcare Workers About HAI Prevention
More than half of the respondents, 135 (57.2%), had a favorable attitude towards HAI prevention. Two hundred seven (91.1%) study participants strongly agreed that use of antiseptic is necessary to prevent HAIs. A significant number of the respondents did not agree on the importance of changing mask as a measure of HAIs control (disagree plus not sure=46.2%) (Table 3).
 |
Table 3 Attitude of Healthcare Workers About HAI Prevention at UoGCSH, 2019 |
Practice of Healthcare Workers About HAI Prevention
Regarding infection prevention practice, the majority of the respondents have poor practice, 151 (64%), towards HAI prevention. Half of HCWs (50.4%) always change gloves before handling new patient, whereas 39.4% of respondents never use safety cabinets in the laboratory (Table 4).
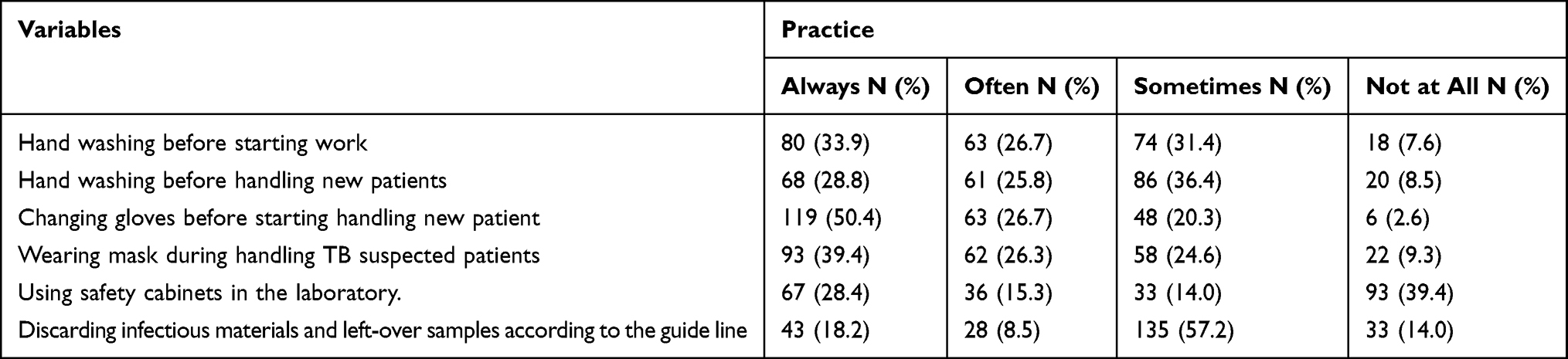 |
Table 4 Healthcare Workers Practice Towards HAI Prevention at UoGCSH, 2019 |
Factors Associated with Attitude and Practice of HCWs Towards HAI Prevention
Pearson’s Chi square was done to determine the association between independent variables with practice and attitude states of HCWs on HAI prevention. In this study, working experience and educational level of HCWs (P value 0.021 and 0.037 respectively) was a statistically significant association with attitude towards HAI prevention. Similarly, there was a significant association between practices towards HAI preventions versus educational status and level of experience of HCWs (P value=0.027 and 0.044, respectively). The finding also showed that the trend of good infection prevention practice was getting better and better as educational level increases from diploma through master’s levels (Table 5). In this study, did not find any associated factors which were significantly associated with knowledge about infection prevention.
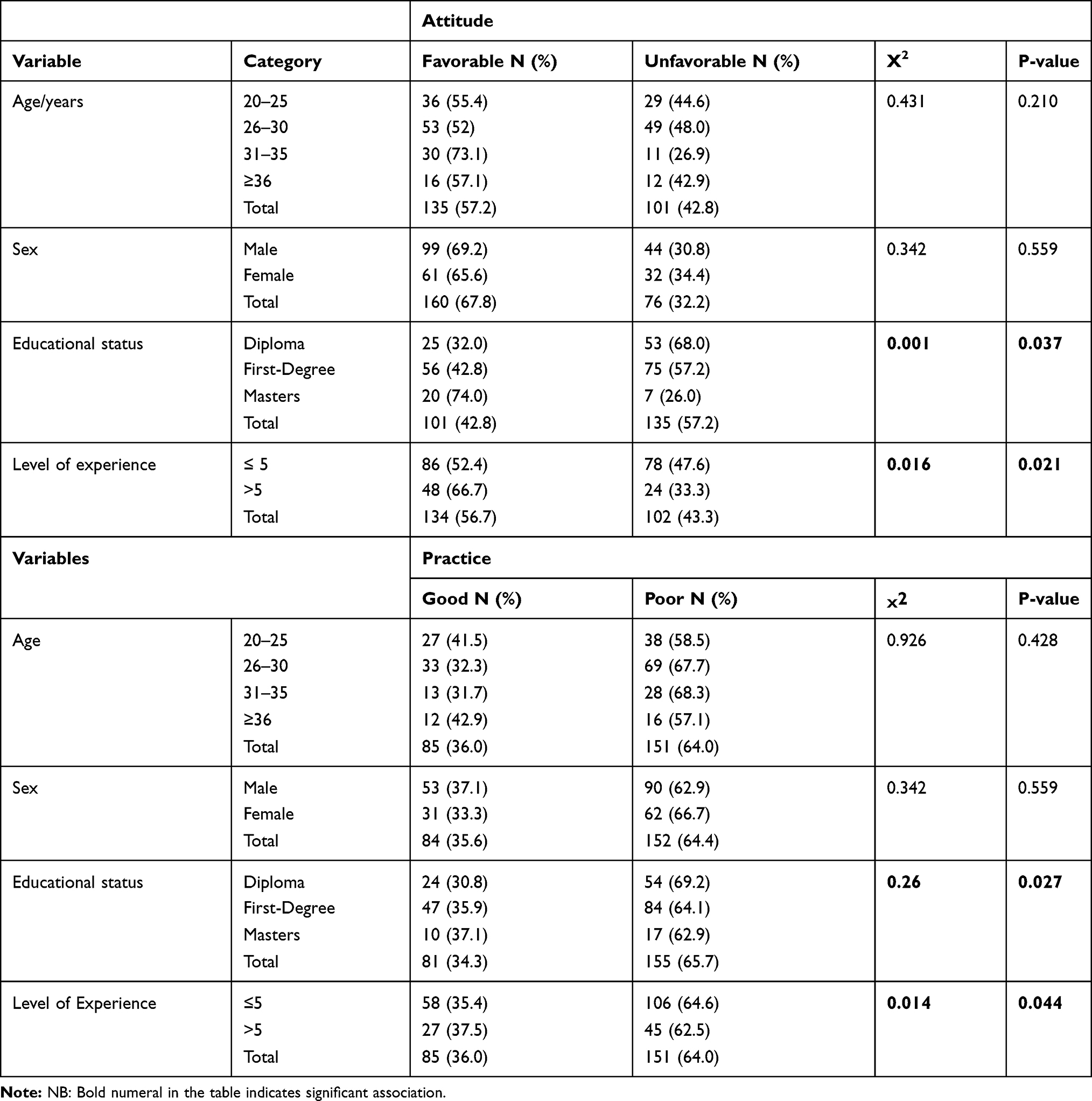 |
Table 5 Association of Socio-Demographic Variables with Attitude and Practice of Healthcare Workers Towards HAI Prevention at UoGCSH, 2019 |
Discussion
This study found that the majority of the HCWs (90.2%) had good knowledge regarding infection prevention, which is in line with the study conducted in Addis Ababa reported that 90% of healthcare workers had good knowledge.28 On the other hand, this finding was higher than the study conducted in Bahir Dar, Ethiopia and Gaza city, Palestine were 84.2% and 47.6% of respondents had good knowledge, respectively.27,29 This variation may be due to differences in the composition of respondents, instability of trained staffs in one hospital as well as the frequency of trainings given in infection prevention.
In the study, almost all study subjects, 225 (95.3%), were aware that HAIs are contracted in hospital environment. This finding is higher than a similar study conducted in Nigeria, which was reported as 80.3%.30 We also found that HCWs at the UOG Hospital have good knowledge on the use of protective equipment and hand washing (96.6%). This finding is similar to that reported among healthcare staff in India (90%),31 but higher than figures reported Cairo in Elgalea Government Hospital (73.1%) and Cleopatra Private Hospital (72.7%).32 It is also much better than the findings at the University of Port Harcourt Teaching Hospital, Nigeria (UPTH) in which more than half of the HCWs (55.4%) lack good knowledge of hand washing.33 This satisfactory level of knowledge by the respondents may be due to the frequent provision of trainings and refreshment seminars regarding infection prevention as well as HCWs know the basics of infection prevention and control measures as it is the foremost portion of their profession.
The need of positive attitudes about infection prevention is unquestionable to prevent HAIs. More than half of the respondents (57.2%) had a favorable attitude about infection prevention. In spite of this fact, a significant number (42.8%) of HCWs in this study had unfavorable attitude to infection prevention. The attitude level of participants in our study is found to be similar to that conducted in Bahir Dar city of Ethiopia (55.6%).27 On the other hand, this finding was far lower than the study finding in Dessie referral hospital, Ethiopia in which the reported level of favorable attitude was 76.4%.9 This difference might be attributed by the variation in academic background of the study respondents, sample size variation as well as implementation and availability of HAIs prevention protocols. As well in many settings, hand washing may be seen as a trivial issue that is not routinely taken seriously, especially in non-surgical and non-invasive procedures. Our study also revealed that statistically significant association between attitude towards HAIs prevention and working experience as well as the educational level of HCWs (P value 0.016 and 0.037, respectively), thus good level of knowledge is not accompanied with a positive attitude.
In spite of good knowledge, safe infection prevention practice was low (36%). Educational level and work experience of HCWs are significantly associated with the practice (0.027 and 0.044 respectively) towards HAI prevention. This finding was much lower than similar studies conducted in Bahir Dar, Ethiopia (54.2%) and Mekele (42.9%).27,34 This lower result might be due to differences in availability of sanitary facilities and logistics required for HAI prevention activities at the study sites. The other possible explanation might be experienced HCWs transferred to other hospitals in order to take an advantage of living in the capital city of the country.
Our study showed that half of respondents always change gloves before handling new patients. This result was smaller than the study conducted in Naples, Italy in which only 57.3% always change gloves.35 The possible reason for this might be due to the poor availability of materials (gloves) which enforces the HCWs to use the already available material for multiple patients.
Similarly, 28.8% of the study subjects wash their hands before handling new patients, which are lower than the study conducted in Addis Ababa, Ethiopia.28 The likely reason might be the differences in logistics and facilities. Other parameters attributed to good practice were also not implemented positively by HCWs which indicates that facilities and materials are poorly accessible. Day to day practice of safe infection prevention is mandatory for both the patients and HCWs consequently reduces HAIs but in our study, we found the level of good practice is unsatisfactory.
Limitation of the Study
The main limitation of this study was single site which is unable to generalize about the other nongovernmental healthcare workers.
Conclusion and Recommendation
Healthcare workers in this study had sufficient knowledge towards infection prevention, but their attitude and implementation of safe practices were substandard. The healthcare workers’ practice was unsatisfactory for the basic elements of the components like hand washing, wearing PPE, discarding infectious materials and leftover samples, which will at some point increases the chance of HAIs. Moreover, risk factors like educational level and work experience of HCWs are significantly associated with practice and attitude towards HAI prevention. Therefore, provision of continual on-job and off-job trainings together with strict implementation of updated SOP in clinical specimen handling and disposal are recommended. Additionally, hospitals should provide infection prevention facilities and supplies, continuous water supply, hand washing sinks and all necessary PPE to improve infection prevention practices of healthcare workers.
Abbreviations
HAIs, Hospital-acquired infections; HCWs, Healthcare Workers; KAP, Knowledge, Attitude and Practice; NIS, Nosocomial Infections; UoGCSH, University of Gondar Comprehensive specialized Hospital; SOP, Standard Operational Procedures; PPE, Personal Protective Equipment.
Data Sharing Statement
All data regarding the results of the study is included in the manuscript without restriction.
Ethics Approval and Consent to Participate
Ethical clearance was approved by the ethical and review committee (ERC) of the University of Gondar, College of Medicine and Health Sciences. The support letter was submitted to the University of Gondar comprehensive specialized hospital and then permission was obtained from the hospital director and department/section heads. In accordance with the declaration of Helsinki, written informed consent was obtained from each individual respondent after verbal explanation about the purpose and importance of the study before the data collection process. All information from participants was kept confidential by using code numbers and there was no personal identification which is left on the questionnaire.
Acknowledgments
We the authors express our gratitude to the University of Gondar Hospital management and the study participants.
Author Contributions
All authors made a significant contribution in the conception, study design, execution, acquisition of data, analysis and interpretation. Also, all authors took part in drafting, revising or critically reviewing a manuscript. Finally, all the authors have agreed on the journal to which the manuscript has been submitted and gave final approval of the version to be published as well as agreed to be accountable for all aspects of the work.
Funding
There is no governmental or non-governmental funding for this study.
Disclosure
The authors report no conflicts of interest regarding the present study.
References
1. Mayhall CG. Hospital Epidemiology and Infection Control.
2. Curtis DE, Hlady CS, Kanade G, Pemmaraju SV, Polgreen PM, Segre AM. Healthcare worker contact networks and the prevention of hospital-acquired infections. PLoS One. 2013;8(12):e79906. doi:10.1371/journal.pone.0079906
3. Meena P, Gaurav P. Assessment of Health care professionals knowledge, attitude and practice towards infection control in labour room. Int J Ayurveda Pharm Res. 2016;4(4).
4. Mortell M, Balkhy HH, Tannous EB, Jong MT. Physician ‘defiance’towards hand hygiene compliance: is there a theory–practice–ethics gap? J Saudi Heart Assoc. 2013;25(3):203–208. doi:10.1016/j.jsha.2013.04.003
5. Abdallah SA, Al-Shatti L, Al-Awadi B, Al-Hammad N. Disinfectants use awareness among college of nursing students and nurses in some healthcare settings, Kuwait. Middle East J Sci Res. 2012;12(7):964–969.
6. Mortell M. Hand hygiene compliance: is there a theory-practice-ethics gap? Br J Nurs. 2012;21(17):1011–1014. doi:10.12968/bjon.2012.21.17.1011
7. WHO. Report on the Burden of Endemic Health Care-Associated Infection Worldwide. A systematic review of the literature; 2011.
8. Allegranzi B, Bischoff P, de Jonge S, et al. New WHO recommendations on preoperative measures for surgical site infection prevention: an evidence-based global perspective. Lancet Infect Dis. 2016;16(12):e276–e287. doi:10.1016/S1473-3099(16)30398-X
9. Gezie H, Leta E, Admasu F, Gedamu S, Dires A, Goshiye D. Health care workers knowledge, attitude and practice towards hospital acquired infection prevention at Dessie referral hospital. Clin J Nurs Care Pract. 2019;3:059–063.
10. Uwaezuoke S, Obu H. Nosocomial infections in neonatal intensive care units: cost-effective control strategies in resource-limited countries. Niger J Paediatr. 2013;40(2):125–132.
11. Mehta Y, Gupta A, Todi S, et al. Guidelines for prevention of hospital acquired infections. Indian J Crit Care Med. 2014;18(3):149. doi:10.4103/0972-5229.128705
12. Suchitra J, Devi NL. Impact of education on knowledge, attitudes and practices among various categories of health care workers on nosocomial infections. Indian J Med Microbiol. 2007;25(3):181. doi:10.4103/0255-0857.34757
13. Desta M, Ayenew T, Sitotaw N, Tegegne N, Dires M, Getie M. Knowledge, practice and associated factors of infection prevention among healthcare workers in Debre Markos referral hospital, Northwest Ethiopia. BMC Health Serv Res. 2018;18(1):1–10. doi:10.1186/s12913-018-3277-5
14. Geberemariyam BS, Donka GM, Wordofa B. Assessment of knowledge and practices of healthcare workers towards infection prevention and associated factors in healthcare facilities of West Arsi District, Southeast Ethiopia: a facility-based cross-sectional study. Arc Public Health. 2018;76(1):69.
15. Saleem Z, Godman B, Hassali MA, Hashmi FK, Azhar F, Rehman IU. Point prevalence surveys of health-care-associated infections: a systematic review. Pathog Glob Health. 2019;113(4):191–205. doi:10.1080/20477724.2019.1632070
16. Cassini A, Plachouras D, Eckmanns T, et al. Burden of six healthcare-associated infections on European population health: estimating incidence-based disability-adjusted life years through a population prevalence-based modelling study. PLoS Med. 2016;13(10):e1002150. doi:10.1371/journal.pmed.1002150
17. Yazie TD, Sharew GB, Abebe W. Knowledge, attitude, and practice of healthcare professionals regarding infection prevention at Gondar University referral hospital, northwest Ethiopia: a cross-sectional study. BMC Res Notes. 2019;12(1):563. doi:10.1186/s13104-019-4605-5
18. Haque M, Sartelli M, McKimm J, Bakar MA. Health care-associated infections–an overview. Infect Drug Resist. 2018;11:2321. doi:10.2147/IDR.S177247
19. Tietjen L, Bossemeyer D, McIntosh N. Infection Prevention: Guidelines for Healthcare Facilities with Limited Resources. Jhpiego Corporation; 2003.
20. Messele G, Woldemedhin Y, Demissie M, Mamo K, Geyid A. Common causes of nosocomial infections and their susceptibility patterns in two hospitals in Addis Ababa. Ethiop J Health Biomed Sci. 2009;2(1):3–8.
21. Yallew WW, Kumie A, Yehuala FM. Point prevalence of hospital-acquired infections in two teaching hospitals of Amhara region in Ethiopia. Drug Healthc Patient Saf. 2016;8:71. doi:10.2147/DHPS.S107344
22. Ali S, Birhane M, Bekele S, et al. Healthcare associated infection and its risk factors among patients admitted to a tertiary hospital in Ethiopia: longitudinal study. Antimicrob Resist Infect Control. 2018;7(1):2. doi:10.1186/s13756-017-0298-5
23. Reda AA, Fisseha S, Mengistie B, Vandeweerd J-M. Standard precautions: occupational exposure and behavior of health care workers in Ethiopia. PLoS One. 2010;5(12):e14420. doi:10.1371/journal.pone.0014420
24. Loftus MJ, Guitart C, Tartari E, et al. Hand hygiene in low-and middle-income countries. Int J Infect Dis. 2019;86:25–30. doi:10.1016/j.ijid.2019.06.002
25. Hussein S, Estifanos W, Melese E, Moga F. Knowledge, attitude and practice of infection prevention measures among health care workers in wolaitta sodo Otona teaching and referral hospital. J Nurs Care. 2017;6(416):2167–1168.1000416.
26. Let T Infection prevention guideline for health care facilities with limited resource. JHPHIEGO; 2011.
27. Gulilat K, Tiruneh G. Assessment of knowledge, attitude and practice of health care workers on infection prevention in health institution Bahir Dar city administration. Sci J Public Health. 2014;2(5):384–393. doi:10.11648/j.sjph.20140205.13
28. Tenna A, Stenehjem EA, Margoles L, Kacha E, Blumberg HM, Kempker RR. Infection control knowledge, attitudes, and practices among healthcare workers in Addis Ababa, Ethiopia. Infect Control Hosp Epidemiol. 2013;34(12):1289. doi:10.1086/673979
29. Eljedi A, Dalo S. Compliance with the national palestinian infection prevention and control protocol at governmental paediatric hospitals in gaza governorates. Sultan Qaboos Univ Med J. 2014;14(3):e375.
30. Iliyasu G, Dayyab FM, Habib ZG, et al. Knowledge and practices of infection control among healthcare workers in a Tertiary Referral Center in North-Western Nigeria. Ann Afr Med. 2016;15(1):34. doi:10.4103/1596-3519.161724
31. Sharma R, Sharma M, Koushal V. Hand washing compliance among healthcare staff in Intensive Care Unit (ICU) of a multispecialty hospital of North India. J Hosp Adm. 2012;1(2):27–33. doi:10.5430/jha.v1n2p27
32. Abd Elaziz K, Bakr I. Assessment of knowledge, attitude and practice of hand washing among health care workers in Ain Shams University hospitals in Cairo. J Prev Med Hyg. 2009;50(1):19–25.
33. Alex-Hart BA, Opara PI. Handwashing practices amongst health workers in a teaching hospital. Am J Infect Dis. 2011;7(1):8–15. doi:10.3844/ajidsp.2011.8.15
34. Gebresilassie A, Kumei A, Yemane D. Standard precautions practice among health care workers in public health facilities of Mekelle special zone, Northern Ethiopia. J Community Med Health Educ. 2014;4(3):286.
35. Parmeggiani C, Abbate R, Marinelli P, Angelillo IF. Healthcare workers and health care-associated infections: knowledge, attitudes, and behavior in emergency departments in Italy. BMC Infect Dis. 2010;10(1):35. doi:10.1186/1471-2334-10-35
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.