Back to Journals » Advances in Medical Education and Practice » Volume 11
Knowledge, Attitude and Practice of Physicians Regarding Screening of Colorectal Cancer in Qatar: A Cross-Sectional Survey
Authors Mahmoud M, Parambil J ![]() , Danjuma M
, Danjuma M ![]() , Abubeker I, Najim M
, Abubeker I, Najim M ![]() , Ghazouani H, Al-Mohanadi D, Al-Mohammed A
, Ghazouani H, Al-Mohanadi D, Al-Mohammed A ![]() , Kartha A, Yassin MA
, Kartha A, Yassin MA ![]()
Received 30 June 2020
Accepted for publication 29 September 2020
Published 6 November 2020 Volume 2020:11 Pages 843—850
DOI https://doi.org/10.2147/AMEP.S268315
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Mohamed Mahmoud, 1 Jessiya Parambil, 1 Mohammed Danjuma, 1 Ibrahim Abubeker, 2 Mostafa Najim, 1 Hafedh Ghazouani, 1 Dabia Al-Mohanadi, 1 Ahmed Al-Mohammed, 1 Anand Kartha, 1 Mohamed A Yassin 3
1Department of Internal Medicine, Hamad Medical Corporation, Doha, Qatar; 2Internal medicine, Rochester Regional Health Unit, USA; 3Department of Medical Oncology, National Centre for Cancer Care and Research, Hamad Medical Corporation, Doha, Qatar
Correspondence: Jessiya Parambil
General Internal Medicine, Hamad General Hospital, Al-Rayyan Road, P O Box 3050, Doha, Qatar
Tel +974 30007415
Email [email protected]
Purpose: The aim of this study was to evaluate the rate of internal medicine residents’ and faculties’ (specialists and consultants) compliance to colorectal cancer screening in Hamad Medical Corporation (Doha, Qatar) and to identify barriers as well as facilitators that will assist in drawing up changes that would enhance physician-related cancer screening.
Methods: A cross-sectional web-based survey was distributed among internal medicine physicians at three component hospitals of Hamad Medical Corporation (HMC); focusing on knowledge and practice of colorectal cancer screening, its barriers and facilitators. Chi-square and t-test statistics were used to draw conclusions where appropriate.
Results: The response rate for the survey was 91% and over 75% of the survey respondents were post-graduate trainees. The majority (90.6%) of the physicians (n=144) mentioned that they would recommend colorectal cancer screening for their asymptomatic patients, though trainees tend to choose the correct modality of screening compared to the consultants, 86.21% vs 40.74%. Only 43.4% of the survey participants always to usually recommend screening to their patients in their clinics while only 29.4% do so for their inpatients. Even though there was no statistically significant difference among the frequency of outpatient colorectal cancer screening among trainees, specialists or consultants (p=0.628), there was a clear increase in the reported referrals as the training years or the years of experience increases (p=0.049 for trainees and p=0.009 for faculty). Unclear pathway was reported as the main obstacle to outpatient cancer screening by 30.2% (n= 48) and 54% (n=87) pointed out that an easy and clear pathway for cancer screening would facilitate the same.
Conclusion: While the attitude towards colorectal cancer screening is positive, the actual practice of recommendation is sub-optimal. Further initiatives are required to facilitate awareness and compliance to colorectal cancer screening.
Keywords: bowel cancer, screening, doctors, residents, Middle East
A Letter to the Editor has been published for this article.
A Response to Letter has been published for this article.
Introduction
Colorectal cancer is ranked as the third most commonly diagnosed cancer among both sexes combined, and the second most common cause of cancer-related death.1 Even though there is a relatively lower incidence among the Arab population,1,2 colorectal cancer is still the second most common cancer among Gulf Corporation Council (GCC) states.2 This mirrors the annual incidence of about 11.3% seen in the state of Qatar in 2018.3 Despite its adverse outcome, the natural history of the disease lends itself to interventions that could potentially alter some of its adverse outcomes. Colon cancer needs several years to progress from adenoma to carcinoma.4 Also, if the disease is localized, the survival rate reaches up to 90% compared to 10% if metastasis has already occurred.5,6 This affords clinicians and epidemiologist the requisite opportunity to commission and implement strategies targeting early detection and intervention (especially through universally accepted screening program).
Amongst a range of problems associated, sub-optimal cancer-control includes the relatively low rate of adherence to screening protocols.7–9 About 30% of eligible adults in the United States of America, for example, are not getting screened as planned.10 These numbers were comparatively higher from several systematic studies in the Arab world.11 Studies have shown that a low rate of physician recommendations12–14 or patient’s unawareness of the disease burden12 often accounts for a low compliance rate as the main reasons for the increased incidence. Furthermore, at the medical residents’ level, studies have shown that the compliance to colorectal cancer screening is even poorer.15,16
In this study, we aim to comprehensively evaluate the rate of internal medicine residents’ and faculty compliance with colorectal cancer screening in Hamad medical corporation (Doha, Qatar), as well as identify barriers and facilitators that could potentially augment changes that could enhance physician-related cancer screening.
Study Methodology
This is a cross-sectional study that aimed to evaluate the practice of physicians regarding screening of colorectal cancer over four months (December 2018 to March 2019) at a tertiary healthcare organization (Hamad Medical Corporation [HMC]) in the state of Qatar. HMC constitutes of nine specialized and three community hospitals as well as specialized healthcare centers. The study sample included a wide spectrum of Internal Medicine Residency Program [IMRP] physicians ranging from trainees in different post-graduate year levels to faculty members (specialists and consultants). The sample size required to reach a confidence level of 95% with a margin of error of 5 was 165. A web-based standardized questionnaire [Table 1] was delivered via the corporation e-mail to the targeted population with an invitation to participate in a preventive health study. It included 14 questions that are designed to follow the Walsh and McPhee Systems Model of Clinical Preventive Care.17 The structure of the questionnaire was based on the study “Barriers to and Facilitators to Physician Recommendation of Colorectal Cancer Screening” by Guerra et al18 with adjustment in the questions to fit our system in HMC. A pre-specified respondent target of at least 60% was set to ensure reliable inferences that can be made at later stages. The responses were recorded in a Microsoft Excel database and analyzed.
 |
Table 1 Colorectal Cancer Screening Survey Questionnaire |
Statistical Analyses
For categorical variables, frequencies were reported and the Chi-square test or Fisher’s exact test was used where appropriate (n<5 or n=0) and using Yates Correction for the fact that both Pearson’s chi-square test and McNemar’s chi-square test are biased upward for a 2 x 2 contingency table. All analyses were carried out using IBM® SPSS® Statistics V26.
Results
We analyzed questionnaires correctly filled by 171 physicians with a response rate of 61%. The respondents were mainly from 3 constituent hospitals of Hamad Medical Corporation. The majority of the physicians were post-graduate trainees (n = 129, 75.44%, p = <0.001) [See Table 2].
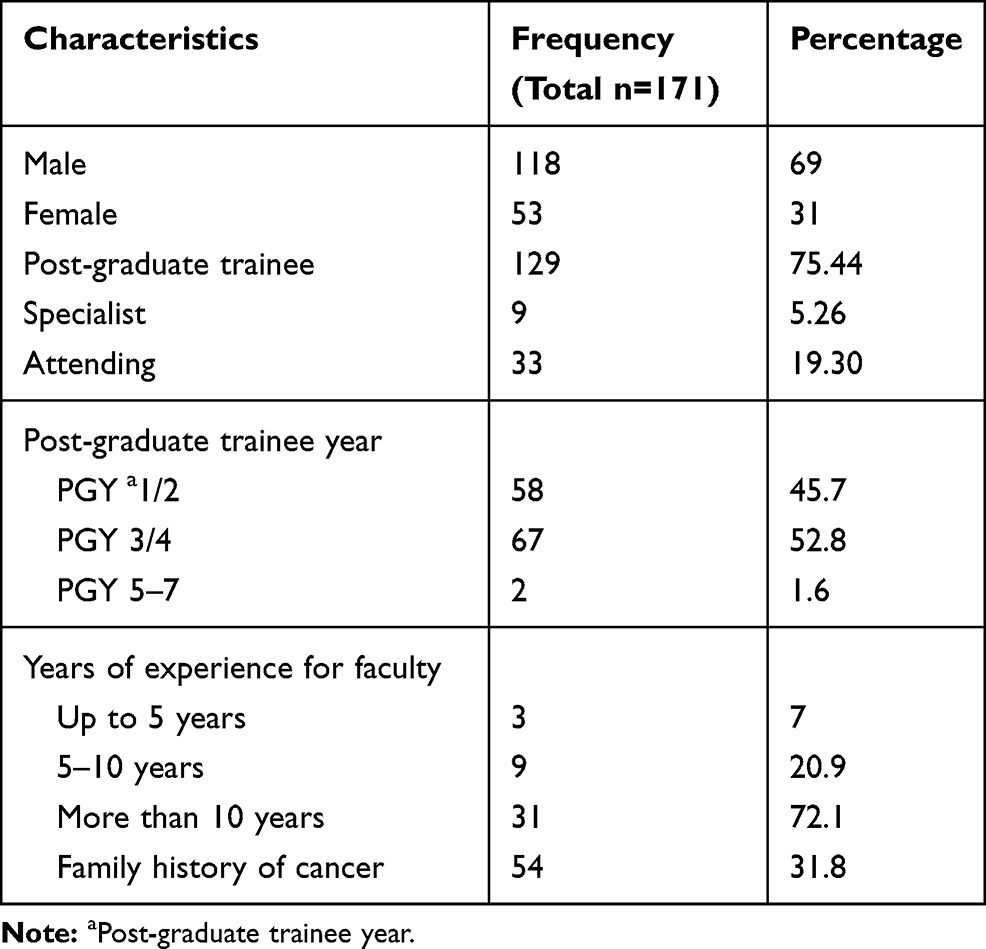 |
Table 2 Demographic Characteristics of Physicians Responded to the Survey |
Reported Practice of Cancer Screening
The majority of the physicians (90.6%, n=144) would recommend colorectal cancer screening for their asymptomatic patients [Table 3]. However, only half of them (54.9%, n = 90) were aware of the colorectal cancer screening pathway on Cerner (Electronic medical record platform currently used across HMC). Among post-graduate trainees, the senior residents tend to know the pathway better than the juniors (P 0.047). [Table 4]
 |
Table 3 Reported Practice of Cancer Screening |
 |
Table 4 Knowledge of Electronic Referral Pathway for Cancer Screening Stratified by Current Clinical Status, Trainee Year, Experience and Primary Site of Practice |
The majority of the physicians chose the correct modality for screening (68%, n=116) in the following descending order: colonoscopy every 10 years (49.4%), fecal immunochemical test (FIT) yearly (24.7%) and sigmoidoscopy every 5 years (1.3%) [Table 3]. Interestingly, post-graduate trainees tend to choose the correct modality of screening better when compared to consultants (86.21% vs 40.74%, p=0.0001). [Table 5]
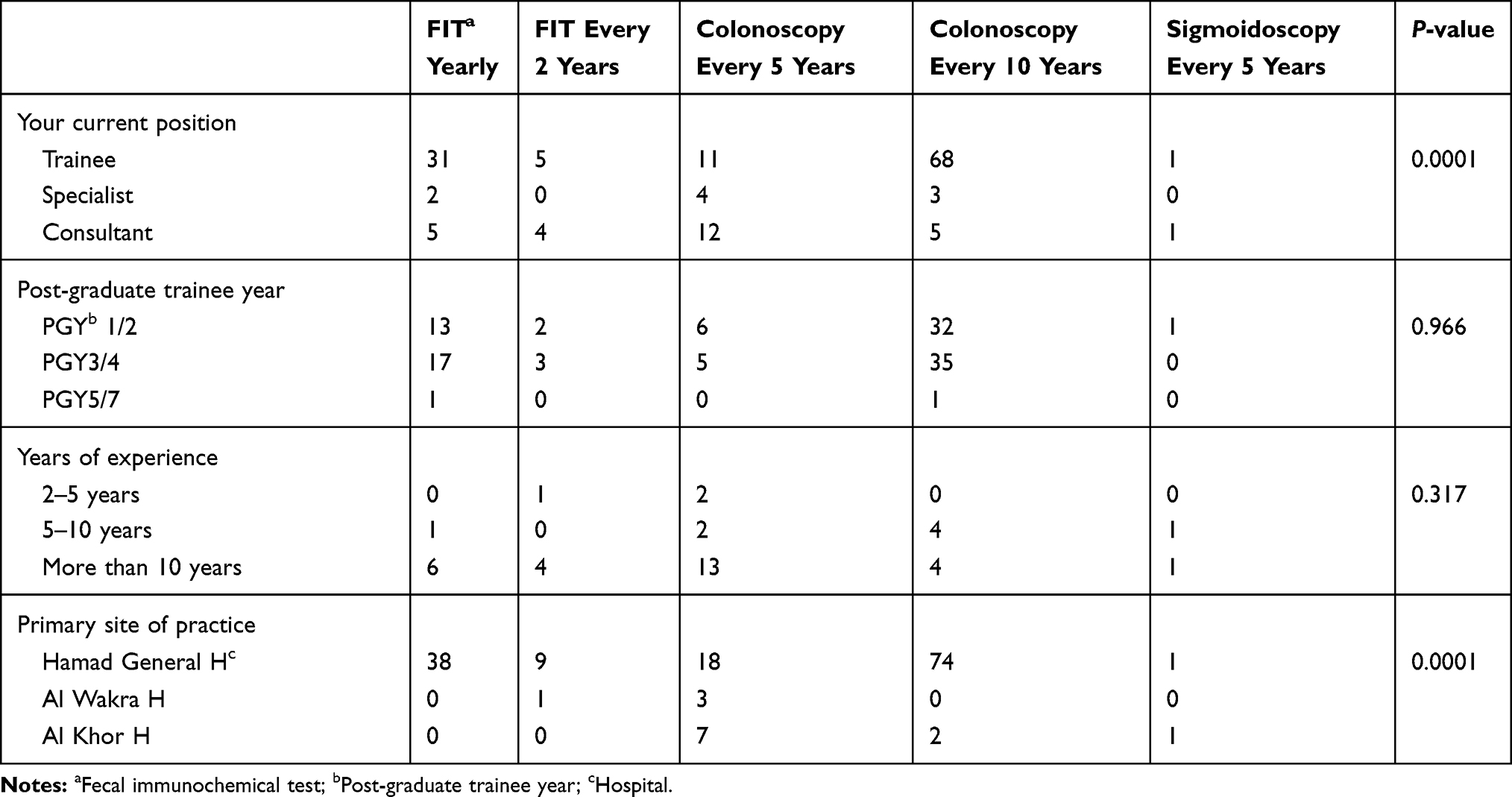 |
Table 5 Modality of Screening Stratified Across Position, Training Level, Experience and Place of Practice |
There was a tendency to recommend colorectal cancer screening more in the outpatient settings rather than in the inpatient settings (43.4% vs 29.4%) (Table 3). However, it should be considered that only 13.2% of the respondents were hospitalists without any outpatient services. Even though there was no statistically significant difference among the frequency of outpatient colorectal cancer screening among trainees, specialists or consultants (p=0.628), there was a clear increase in the reported referrals as the training years or the years of experience increases (p=0.049 for trainees and p=0.009 for faculty). [Table 6]. For inpatient settings, no such effect is noted.
 |
Table 6 Outpatient Bowel Cancer Screening by Physician Response Stratifies by Position, Trainee Level, Experience and Site of Practice |
Reported Impediments to Screening
The main two obstacles preventing the recommendation of colorectal cancer screening were unclear pathway (30.2%, n= 48) and scarcity of time whether in the clinic and during ward rounds (22.6%, n=36 and 29.6%, n=47), respectively [Table 7]. Of note, faculty members (specialists and consultants) were the highest group to report the unclear pathway of referral (P = <0.001) [Table 8].
 |
Table 7 Reported Impediments of Screening |
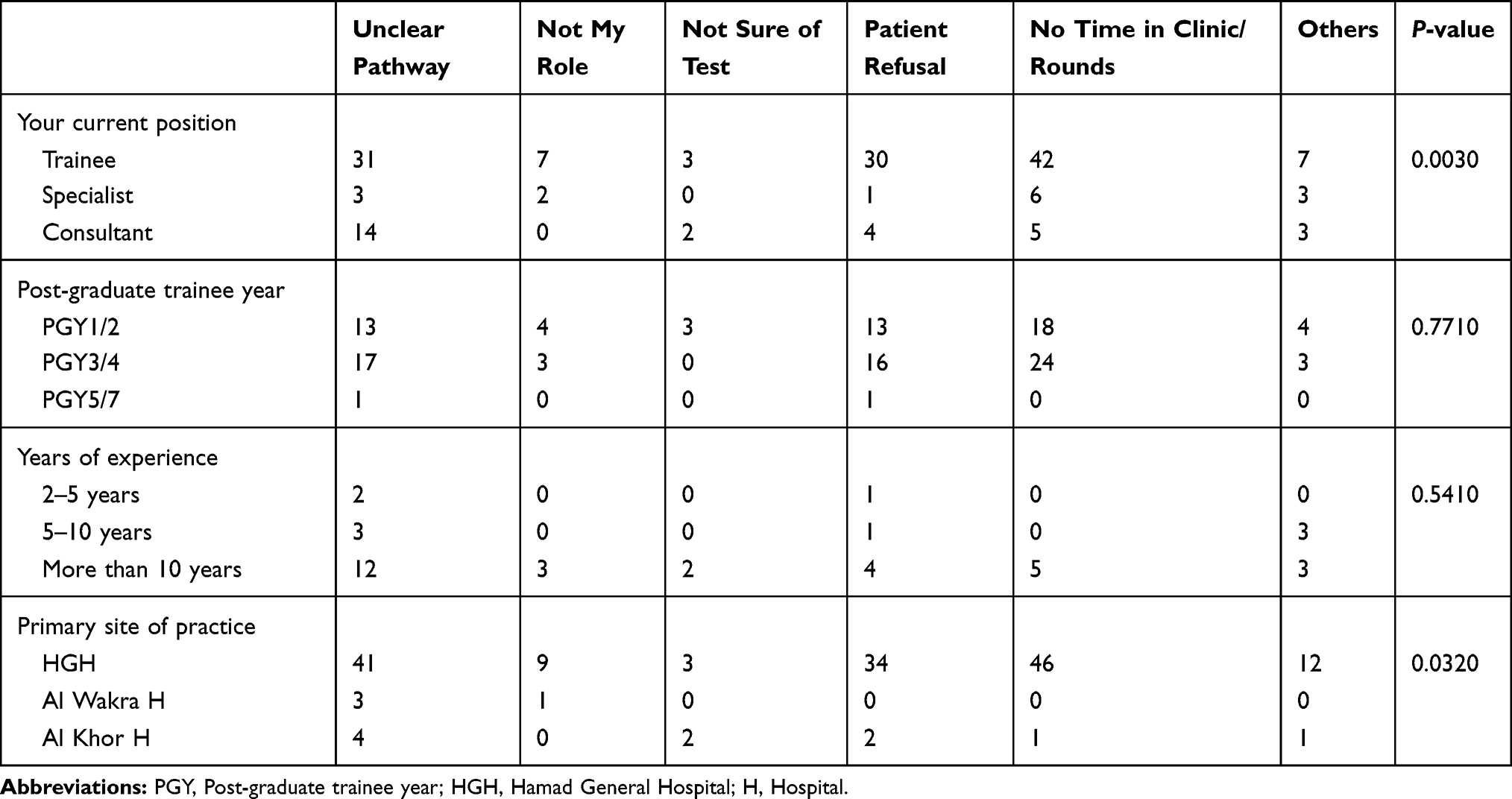 |
Table 8 Barriers to Recommending Bowel Cancer Screening Stratified by Position, Trainee Level, Experience and Place of Practice |
In an effort to explore suggested solutions, the majority of the survey respondents (54%, n=87) pointed out that an easy and clear pathway for cancer screening would help to improve compliance. Nonetheless, more than half of them (59.1%, n=94) still think that cancer screening referral should be done by a dedicated cancer screening program team rather than other physicians [Table 9].
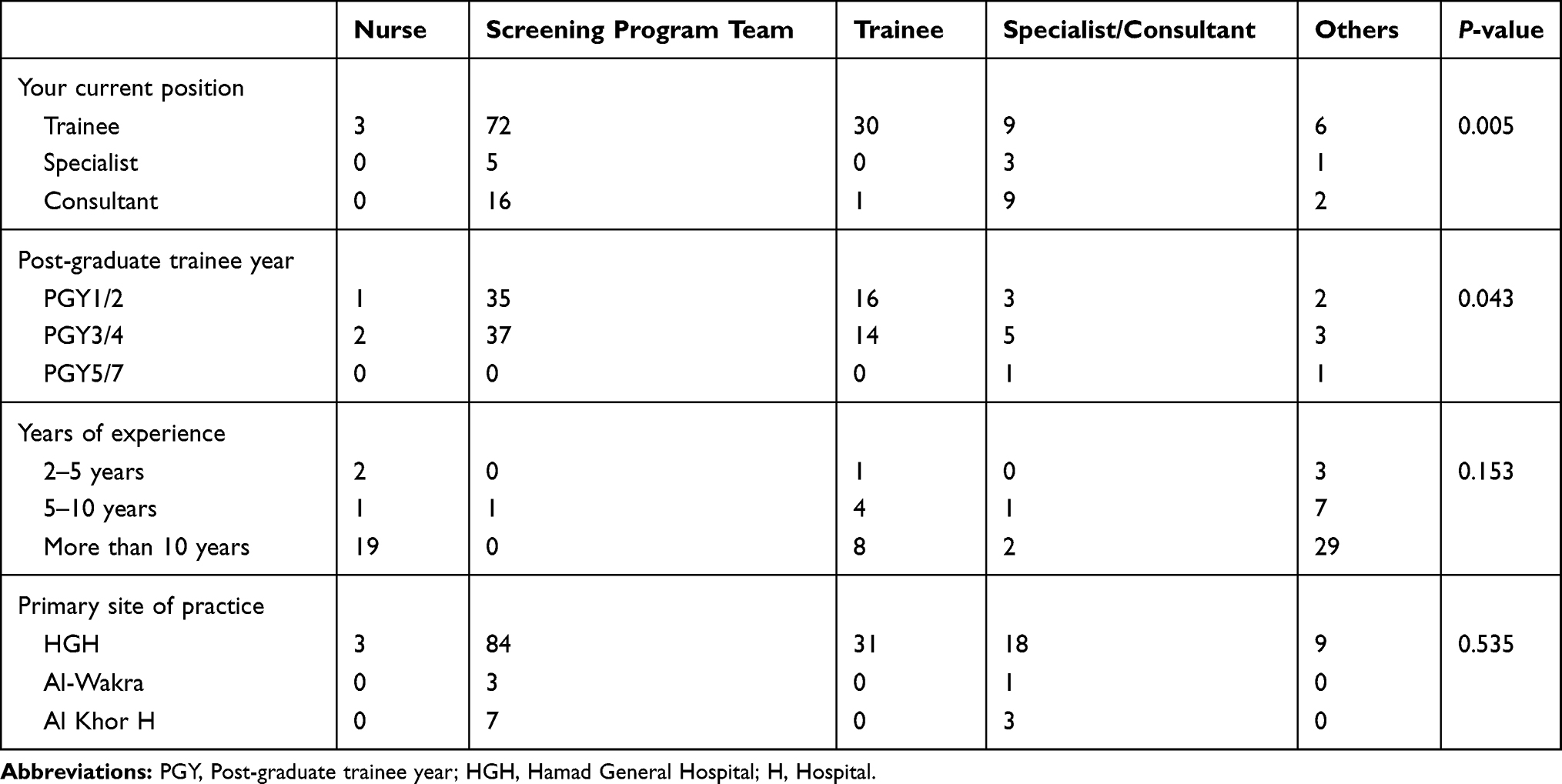 |
Table 9 Output of Whom Should Screen Asymptomatic Patients for Bowel Cancer Response Stratified by Position, Trainee Year, Experience |
Discussion
Cancer is still one of the major causes of mortality and morbidity.1 With the expected population growth and the rate of aging societies, the number of cases is bound to increase exponentially. It has been well established that early detection of colorectal cancer by screening asymptomatic average-risk individuals increases the rate of successful treatment as well as the chance of survival. The USPSTF (United States Preventive Services Task Force) recommendation for colorectal cancer screening spans the age group 50–75 years using either fecal occult blood testing annually, sigmoidoscopy every 5 years, or colonoscopy every 10 years.19
Cancer has been a healthcare priority for Qatar for more than 20 years. The National Cancer Program (NCP) within the Ministry of Public Health was formed to oversee implementation of the National Cancer Strategy, which was launched in 2011.20 The cancer screening registry was established in 2015 and the first national colorectal cancer screening program started in 2016.
In the state of Qatar, the latest national screening program launched in 2015 recommend screening all asymptomatic adults, men and women, age 50–74 annually follows Fecal Immunochemical Test (FIT) annually for screening with a referral for colonoscopy within 30 days if the FIT is positive.21 The General Medicine department at Hamad Medical Corporation holds a unique place in Qatar healthcare in terms of the vast service area it covers and its academic contribution in teaching one of the largest residency programs (IMRP).
The results of our study confirm our hypothesis that suggested a low compliance rate with screening protocols. The percentage of medical residents, which constituted 70% of the doctors we surveyed, offering colorectal cancer screening in outpatient settings was 76%. These numbers correlate well with previous compliance rates in the published literature.8,15,22 However, the proportion of physicians consistently offering bowel cancer screening was as low as 10%. This disparity suggests that an intervention to encourage and remind the physicians to offer screening tests might be helpful to narrow the gap. This is supported by the fact that a significant proportion (91%) of physicians recommends and support bowel cancer screening. In an attempt to ascertain the exact reason accounting for the low compliance, we observed that having an unclear screening pathway was the main obstacle to outpatient bowel cancer screening (as reported by about 33.3% [n= 43]) of the respondents. The newly-implemented electronic medical record system could be one of the major factors contributing to this obstacle. One solution is by offering doctors practical sessions on how to place electronic screening orders, and group those screening tests in a single folder for easy access. Other suggested options will be to post-cancer screening flyers in the doctor’s clinic with a high throughput of eligible patient cohorts. Additionally, we found insufficient consultation time in the clinic as a consistent impediment to screening updates by eligible groups. This could be addressed by scheduling a prior discussion between the nurse and the patient to evaluate his or her eligibility for the screening tests. This will save time as well as allow the doctor to concentrate on explaining the importance of the screening tests to the patients.
The impact of reliable knowledge of screening programs cannot be overestimated. Indeed, the findings from our survey were consistent with that from published reports which showed that the higher the trainee level, the more likely they are to offer screening tests.13,23 Even though the majority of our survey respondents chose guideline-recommended age group for cancer screening, a significant proportion failed to identify the appropriate test. This could potentially be addressed by adding a screening didactic lecture series to the medical resident curriculum. This method has been shown to be effective in improving compliance rates by 30%.24 Furthermore, about 57% of the surveyed respondents suggested the establishment of a cancer screening program team to take care of implementing the screening programs to the eligible population.
The principal strength of our study lies in its novelty as it represents the first systematic attempts at identifying and proposing solutions to cancer screening deficits in this part of the world. Like most observational surveys our study was limited by having as much as 90% of the surveyed doctors from one hospital out of the HMC hospitals. But it could be also considered that the trainees are mainly based on this institution and that would explain the mismatch to some extent. Furthermore, the number of faculty was less compared to trainees, which could be increased to draw a robust solid conclusion. It should be also noted that 21.42% of the consultants were not involved in running any outpatient services which might have accounted for this observation.
This study provides an insight into a problem that further work can be done in the future to solidify our results and offer major solutions.
Conclusion
This study looked into the gap in the physicians’ knowledge, attitude and practice with regards to cancer screening. While the attitude towards colorectal cancer screening is positive, the actual practice of recommendation is scarce. The knowledge of guidelines’ appropriate colorectal cancer screening age and appropriate tests need further reinforcement. We also conclude that further steps like cancer screening specific education sessions for physicians as well as creating clear pathways in the electronic medical record system and collaborating with the national cancer screening team may provide an opportunity to make needed improvements in the compliance of colorectal cancer screening for age-appropriate asymptomatic individuals.
Statement of Ethics
This study was based on a voluntary anonymous survey to test the knowledge of the participating clinician. The survey was approved by the Internal Medicine education department. IRB approval was not required as it was done as part of the medical education survey.
Acknowledgments
Internal medicine residency program for scientific support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel R, Torre L, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424.
2. Ali Hussein Alhurry A, Rezaianzadeh A, Rahimikazerooni S, et al. A review of the incidence of colorectal cancer in the middle east. Ann Colorectal Res. 2017. doi:10.5812/acr.46292
3. Cancer today - population fact sheets [Internet]. Gco.iarc.fr; 2020 [cited September 3, 2020]. Available from: https://gco.iarc.fr/today/data/factsheets/populations/634-qatar-fact-sheets.pdf.
4. Winawer S, Fletcher R, Miller L, et al. Colorectal cancer screening: clinical guidelines and rationale. Gastroenterology. 1997;112(2):594–642. doi:10.1053/gast.1997.v112.agast970594
5. Dolan N, Ferreira M, Davis T, et al. Colorectal cancer screening knowledge, attitudes, and beliefs among veterans: does literacy make a difference? J Clin Oncol. 2004;22(13):2617–2622. doi:10.1200/JCO.2004.10.149
6. SEER cancer statistics review, 1973–1996 [Internet]. Seer.cancer.gov; 2020 [cited September 3, 2020]. Available from: https://seer.cancer.gov/archive/csr/1973_1996/overview.pdf.
7. Costanza M, Stoddard A, Zapka J, Gaw V, Barth R. Physician compliance with mammography guidelines: barriers and enhancers. J Am Board Fam Pract. 1992;5(2):143–152.
8. Hudson S, Ferrante J, Ohman-Strickland P, et al. Physician recommendation and patient adherence for colorectal cancer screening. J Am Board Fam Med. 2012;25(6):782–791. doi:10.3122/jabfm.2012.06.110254
9. Nodora J, Martz W, Ashbeck E, Jacobs E, Thompson P, Martínez M. Primary care physician compliance with colorectal cancer screening guidelines. Cancer Causes Control. 2011;22(9):1277–1287. doi:10.1007/s10552-011-9801-0
10. Klabunde C, Joseph D, King J, White A, Plescia M Vital signs: colorectal cancer screening test use — United States, 2012 [Internet]. Cdc.gov; 2013 [cited September 3, 2020]. Available from: https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6244a4.htm.
11. Arafa M, Farhat K. Colorectal cancer in the arab world–screening practices and future prospects. Asian Pac J Cancer Prev. 2015;16(17):7425–7430. doi:10.7314/APJCP.2015.16.17.7425
12. Koo J, Leong R, Ching J, et al. Knowledge of, attitudes toward, and barriers to participation of colorectal cancer screening tests in the Asia-Pacific region: a multicenter study. Gastrointest Endosc. 2012;76(1):126–135. doi:10.1016/j.gie.2012.03.168
13. Akerman S, Aronson S, Cerulli M, Akerman M, Sultan K. Resident knowledge of colorectal cancer screening assessed by web-based survey. J Clin Med Res. 2014;6(2):120–126.
14. Sahin M, Aker S, Arslan H. Barriers to colorectal cancer screening in a primary care setting in Turkey. J Community Health. 2016;42(1):101–108. doi:10.1007/s10900-016-0235-1
15. Zack D, DiBaise J, Quigley E, Roy H. Colorectal cancer screening compliance by medicine residents: perceived and actual. Am J Gastroenterol. 2001;96(10):3004–3008. doi:10.1111/j.1572-0241.2001.04678.x
16. Struewing J, Pape D, Snow D. Improving colorectal cancer screening in a medical residents’ primary care clinic. Am J Prev Med. 1991;7(2):75–81. doi:10.1016/S0749-3797(18)30941-3
17. Walsh J, McPhee S, Systems A. Model of clinical preventive care: an analysis of factors influencing patient and physician. Health Educ Q. 1992;19(2):157–175. doi:10.1177/109019819201900202
18. Guerra C, Schwartz J, Armstrong K, Brown J, Halbert C, Shea J. Barriers of and facilitators to physician recommendation of colorectal cancer screening. J Gen Intern Med. 2007;22(12):1681–1688. doi:10.1007/s11606-007-0396-9
19. Screening for colorectal cancer: U.S. preventive services task force recommendation statement. Ann Intern Med. 2008;149(9):627. doi:10.7326/0003-4819-149-9-200811040-00243
20. Cancer screening [Internet]. Moph.gov.qa; 2020 [cited September 3, 2020]. Available from: https://www.moph.gov.qa/english/derpartments/undersecretaryoffice/spp/nationalcancerprogram/cancerscreening/Pages/default.aspx.
21. Guidelines for colorectal cancer screening in the state of Qatar [Internet]. Moph.gov.qa; 2015 [cited September 3, 2020]. Available from: https://www.moph.gov.qa/Admin/Lists/PublicationsAttachments/Attachments/20/Guidelines%20for%20Colorectal%20Cancer%20Screening%20V1.2015.pdf.
22. Malhotra A, Aziz K, Freston J Colorectal cancer screening: a retrospective study of compliance with guidelines in a university-based primary care practice [Internet]. Primarycare.imedpub.com; 2006 [cited September 3, 2020]. Available from: https://primarycare.imedpub.com/abstract/colorectal-cancer-screening-a-retrospective-study-of-compliance-with-guidelines-in-a-universitybased-primary-care-practice-1365.html.
23. Richards D, Leung K, Madan A. Baseline knowledge of colorectal cancer screening and surveillance guidelines in internal medicine residents. Am J Gastroenterol. 2008;103(p):S539. doi:10.14309/00000434-200809001-01375
24. Friedman M, Borum M. Colorectal cancer screening of African Americans by internal medicine resident physicians can be improved with focused educational efforts. J Natl Med Assoc. 2007;99(9):1010–1012.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.