Back to Journals » International Journal of General Medicine » Volume 15
Knowledge, Attitude, and Practice of Bee Venom Acupuncture Therapy on Rheumatoid Arthritis Among Patients in Saudi Arabia
Authors Sharaf SE, Alsanosi S ![]() , Alzahrani AR, Al-Ghamdi SS, Sharaf SE
, Alzahrani AR, Al-Ghamdi SS, Sharaf SE ![]() , Ayoub N
, Ayoub N
Received 26 November 2021
Accepted for publication 20 January 2022
Published 5 February 2022 Volume 2022:15 Pages 1171—1183
DOI https://doi.org/10.2147/IJGM.S351315
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Shahd E Sharaf,1,2 Safaa Alsanosi,1 Abdullah R Alzahrani,1,2 Saeed S Al-Ghamdi,1,2 Sharaf E Sharaf,2– 4 Nahla Ayoub1,2
1Department of Pharmacology and Toxicology, Faculty of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia; 2Saudi Toxicology Society, Umm Al-Qura University, Makkah, Saudi Arabia; 3Pharmaceutical Chemistry Department, College of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia; 4Clinical Research Administration, Executive Administration of Research and Innovation, King Abdullah Medical City in the Holy Capital, Makkah, Saudi Arabia
Correspondence: Sharaf E Sharaf
Pharmaceutical Chemistry Department, College of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia
, Tel +966532660411
Email [email protected]
Introduction: Bee venom acupuncture therapy (BVT) is an alternative therapy used worldwide by patients with different chronic diseases due to its therapeutic effects on conditions such as rheumatoid arthritis (RA). Previous studies have illustrated the clinical effects of BVT on RA, but such a study has yet to be performed in Saudi Arabia (SA). It is important to evaluate BVT awareness among citizens of SA to measure the feasibility of conducting clinical trials of BVT in patients with RA in SA. This study aims to measure the knowledge, attitude, and practice (KAP) of BVT on RA and other chronic diseases in SA. This will help determine whether patients with RA have sufficient knowledge to be enrolled in clinical trials.
Patients and Methods: A cross-sectional study of 180 patients with RA in SA was conducted using a KAP questionnaire on BVT. Individuals completed an online questionnaire using the Survey Monkey website. Data were obtained by self-completion of the online KAP questionnaire regarding BVT.
Results: A total of 180 patients with RA and other chronic diseases, with a mean age of 45 years (18– 70 years), participated in the study. The results of the questionnaire showed that 55% of the participants demonstrated a good knowledge of BVT treatment; however, they also reported a poor attitude (55%) and practice (55%). Participants with RA demonstrated higher severity of disease (80%) than those with other chronic diseases. Participants with RA showed better KAP responses towards BVT than those with other chronic diseases. Participants with school education only and those who were beekeepers demonstrated significantly better KAP responses (P < 0.05) compared to participants who had received university education and those who were not beekeepers, respectively.
Conclusion: Participants with strong RA knowledge may prove that patients from SA can be enrolled in BVT clinical trials. The participants’ poor attitudes and practices may be due to BVT being expensive and unavailable in many cities in SA.
Keywords: bee venom acupuncture therapy, rheumatoid arthritis, knowledge, attitude, practice, Saudi Arabia
Introduction
Bee venom acupuncture therapy (BVT) is an alternative medicine that has been increasingly used in the treatment of chronic diseases, such as rheumatoid arthritis (RA). Recent studies have indicated that the active compound in bee venom, melittin, may be useful as a therapeutic treatment for chronic diseases. However, it remains unclear how knowledgeable patients are about BVT, as well as their understanding of how it is being used. One way to obtain this data is through the knowledge, attitude, and practice (KAP) tool. KAP is a powerful research tool, used in both quantitative and qualitative research, in which participants are given a questionnaire to determine their knowledge of, and attitudes toward, a given medical intervention.1–4 The data collected are statistically analyzed, allowing researchers to identify potential misunderstandings, develop future research, and guide the population towards optimal health outcomes. In addition, KAP studies can be used to determine the specific points of strength and weaknesses which can be used to structure or update educational programs to improve the overall KAP level and increase the general awareness among a specific group.
The Korean Movement Disorders Society conducted a KAP survey in 2014 to determine patients’ knowledge on the use of BVT and stem cell therapy to treat Parkinson’s disease. The results showed that half of the patients with Parkinson’s disease in the study expressed their interest in trying this treatment. However, patients reported that they were hesitant due to a lack of evidence on the safety and efficacy of this treatment.5 Meanwhile, a small part of this population reported that using BVT and stem cells to treat Parkinson’s disease is a remarkable idea that requires no evidence to prove it. The researchers concluded that the treatment depends on how knowledgeable the patients were regarding BVT. The patients’ attitudes towards using BVT to treat their disease, regardless of whether they believed in the evidence, was the basis for the researcher recommending further research into the use of BVT for different diseases.5 The present study uses a similar questionnaire, with slight modifications, addressed to patients with RA. The present study focuses on the use of BVT for treating different diseases in patients from Saudi Arabia (SA), measuring their KAP towards such treatment. The goal of the current study was to determine the health outcomes of patients using BVT to treat their disease, and whether the patients understood the concepts behind BVT, or use it regardless of their KAP. This is relevant in SA due to the significance of the bee in the Holy Qur’an. Due to the large Muslim population in SA, there is an abundance of mobile bee sting centers that apply a rudimentary form of this treatment, though rarely in a manner consistent with medical research. By discussing patients’ awareness of BVT and their reasons for using it, we hope to obtain a better understanding of the KAP regarding this novel treatment, thereby obtaining results similar to those of a Korean study.5 Furthermore, the results of this study along with other related studies can be essential for clinical pharmacists, toxicologists and physicians in the future to structure or update BVT clinical practice recommendations6 and medical education programs7 of using BVT as a natural replacement or supporting treatment therapy for patients with RA and other clinical conditions to enhance the patient’s awareness levels and improve their practice,8,9 disease management,10 and quality of life.11
Materials and Methods
Ethical Approval
The questionnaire proposal was submitted to the Faculty of Medicine’s Biomedical Ethics Committee at Umm AL-Qura University (UQU) in Makkah, Saudi Arabia. The committee gave this study questionnaire unconditional approval, granted the use of verbal consent, and gave this study an approval number: HAPO-02-K-012-2020-11-490 which complies with the Declaration of Helsinki.
Sample Size
The sample size was calculated using Slovin’s formula, with a population size of 433 patients with RA in SA from a recently published study by Almoallim et al, 2020, with a confidence interval (CI) of 0.90, and margin of error of 5%.12
The number of participants in the present study was 180 as 168 participants were required to achieve the CI, leaving room for participant dropout.
Study Design
The questionnaire used in this study was cross-sectional, and participants were randomly approached by sending the electronic questionnaire throughout SA over a period of three months to reach the highest number of patients using BVT. The study aims and objectives were described to the participants using a brochure (in English and Arabic languages), which explained the basis of the study, allowing participants to understand the questions being asked so that they could provide informed consent and complete their responses. The questionnaire was based on one used in a previous study.5 Approval was received for using the KAP BVT questionnaires from the previous study to edit, translate, and validate them to match our inclusion and exclusion criteria and research scope. The questionnaire was designed in English and translated into Arabic, the local spoken language, by proficient speakers of both languages, and revised to suit the general population. Every KAP question in each section was marked as one point, and a total score of over 50% of the participants’ (n = 180) responses indicated a good mark, while total responses lower than 50% were considered poor. This method was obtained from previously published studies.2–4
Questionnaire
The questionnaire was used to assess participants’ KAP regarding BVT. The questionnaire contained 42 questions in five parts: sociodemographic, clinical diagnosis, knowledge, attitude, and practice, using an online cloud-based questionnaire development software (Survey Monkey). The questionnaire was presented online to patients using BVT treatment, via a Survey Monkey website link. The questionnaire was divided into five main sections: the first part included sociodemographic information, including gender, age, education level, and current employment, with special attention paid to beekeepers. The second part concerned the patients’ clinical history: RA, osteoarthritis (OA), migraine, delayed pregnancy (DP), cancer, epilepsy or seizures, thyroid diseases, administration of prescribed medication, and disease improvement. The third to fifth parts discussed BVT and KAP.5 The knowledge section asked participants about their beliefs towards BVT, whether they believed that it was effective and safe, whether they had heard about it, and from where they obtained such information. The attitude section reflected participants’ viewpoints towards BVT, regarding how much they knew about it and their feelings towards its usage. The practice section asked the participants how they were receiving BVT: how long they had been using it, how many stings they received at once, place of stinging, administration of complementary bee products such as honey, pollen, and royal jelly, with the administration period of three parts in compression with sociodemographic and clinical diagnosis parts of the questionnaire. Data were collected from patients located all around SA, and validation of this questionnaire was performed through a pilot sample conducted using 20 randomly selected patients who were undergoing BVT. The participants were informed of the aims of the study and consented to participate. The questionnaire was edited and the final version was used in the current study (Appendix).
Study Populations (Inclusion/Exclusion Criteria)
The selection criteria included male and female Saudi national patients aged ≥18 years who were using BVT. The exclusion criteria included non-Saudi patients, patients who had never used BVT, those with the inability to consent, and participants with medical backgrounds (all health professionals).
Data Storage
All responses to the questionnaire were downloaded from the Survey Monkey website and held on a secure server.
Statistical Analysis
We received a complete case analysis of the answers provided by respondents who completed all 42 questions from the five-part survey. Participants who provided incomplete responses to the questionnaire were excluded. The data were collected from the spreadsheets provided by Survey Monkey, transferred to Microsoft Excel for coding, and transferred to GraphPad Prism version 8.4.3 for statistical analysis. Descriptive statistics were used for the description of demographic KAP variables. A chi-square test was used to detect whether there was a significant difference between KAP and the variables. Statistical significance was determined at a P-value <0.05.
Results
Demographic Characteristics of the Participants
A total of 190 questionnaires were collected, of which 10 were excluded because of incomplete responses, giving a response rate of 94.7%. Thus, 180 questionnaires were included in this study. The participants’ demographic characteristics are shown in Table 1. There were 90 men (50%) and 90 women (50%) with chronic diseases. Most of the participants were aged between 18–40 years (60%), and the remaining were aged between 41–70 years (40%). Most participants (71.6%) received university education, 23.3% completed high school education, and 5% had middle educational qualifications. One hundred twenty (66%) of the participants were employed, of which 28.3% were beekeepers, with the majority (71.7%) not keeping bees, and 33.3% were unemployed.
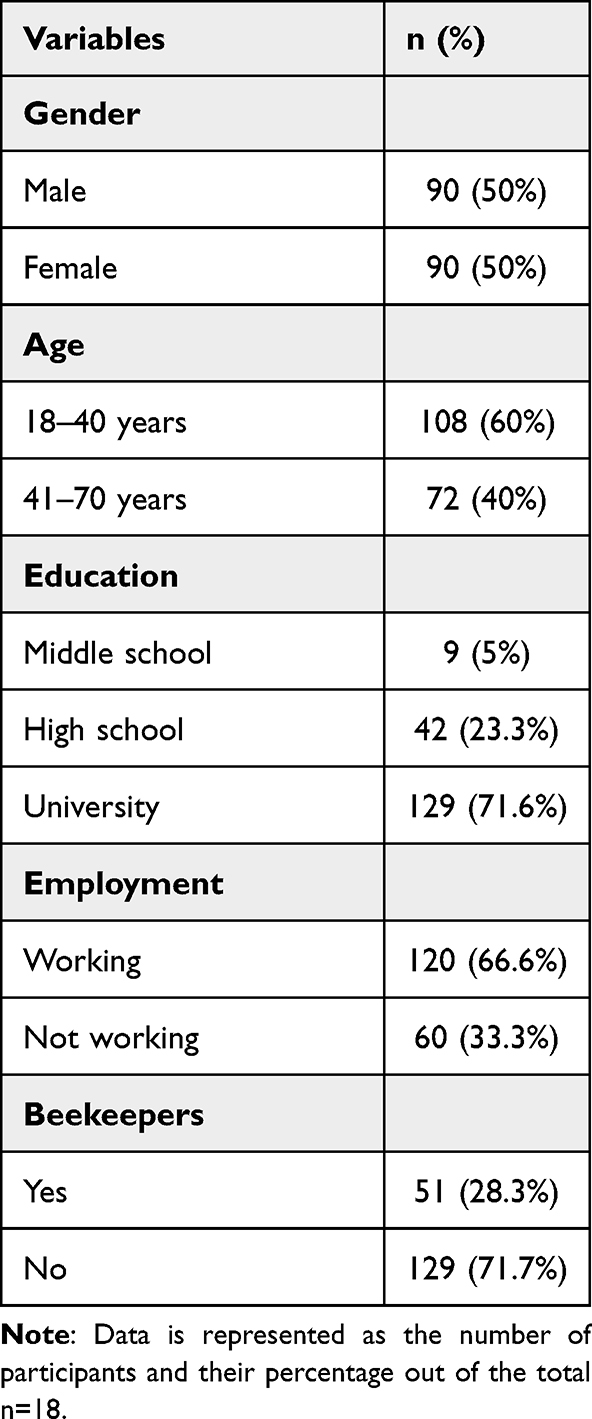 |
Table 1 Demographic Characteristics of the Participants |
Chronic Diseases of the Participants
The participants’ clinical chronic diseases are shown in Table 2. A total of 144 patients had RA (80%), 14 had OA (7.8%), 4 had migraine (2.2%), 5 had DP (2.8%), 4 had cancer (2.2%), 5 had epilepsy or seizures (2.8%), and 4 had thyroid diseases (2.2%). Most of the participants were in the group administered the prescribed medication (96.7%), and the remaining did not receive the prescribed medication (3.3%). Most participants’ diseases improved using prescribed medication (72.3%), while the remaining did not show improvement (27.7%).
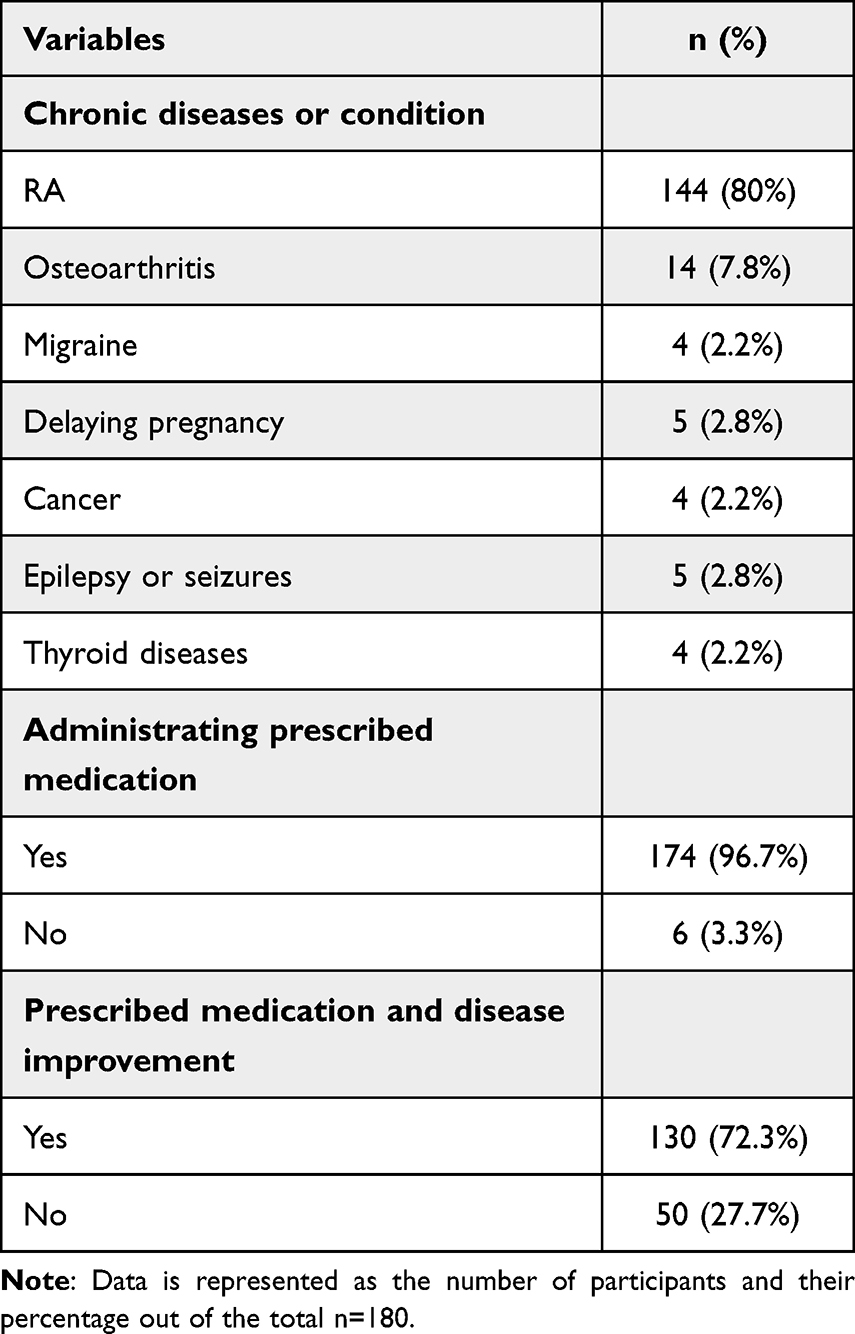 |
Table 2 Clinical Data and History of the Participants |
Knowledge Assessment
The overall percentage of knowledge of BVT was good among the participants, with a total of 55% (Figure 1). Figure 2 shows the total percentage distribution of knowledge among the participants. Approximately 55% (n = 99) had previously heard of BVT; however, only 45% had tried BVT for their diseases. We found that 55% of the participants (n = 99) believed that BVT was generally effective, and 55% reported that they believed BVT was more effective than bee honey (BH). There was a significant difference between participants aged between 18–40 years and older participants regarding their beliefs on whether BVT was more effective than BH. Interestingly, participants who had received only high school level education scored significantly higher (P <0.05) than participants with university education on whether they regarded BVT as being safe to use for the treatment of several diseases. Furthermore, participants who were not working scored significantly higher (P <0.05) than those who were working, regarding whether they believed BVT to be effective for many diseases, and whether they had tried BVT. Moreover, there was a significant difference (P <0.05) between participants who were beekeepers and those who were not beekeepers, in terms of whether they knew family and friends who had either tried BVT, believed that BVT was an effective therapy for treating many diseases, or had tried BVT themselves (Table 3).
 |
Table 3 The Participant’s Knowledge About BVT Association with the Participant’s Characteristics and Educational Background. N=180 |
 |
Figure 1 The total percentages of participant’s knowledge, attitude and practice about BVT. |
 |
Figure 2 The total distribution percentage of BVT knowledge among the participants. |
Participants with RA (n = 144) scored significantly higher (P <0.05) in all the knowledge questions compared with participants with other chronic diseases: 99% of participants with RA had heard about BVT, 92.4% knew friends and family who had tried BVT, 95.2% believed that BVT was effective in treating RA, 96% had tried BVT therapy, and 85.7% believed it was safe for the treatment of many diseases (Table 4).
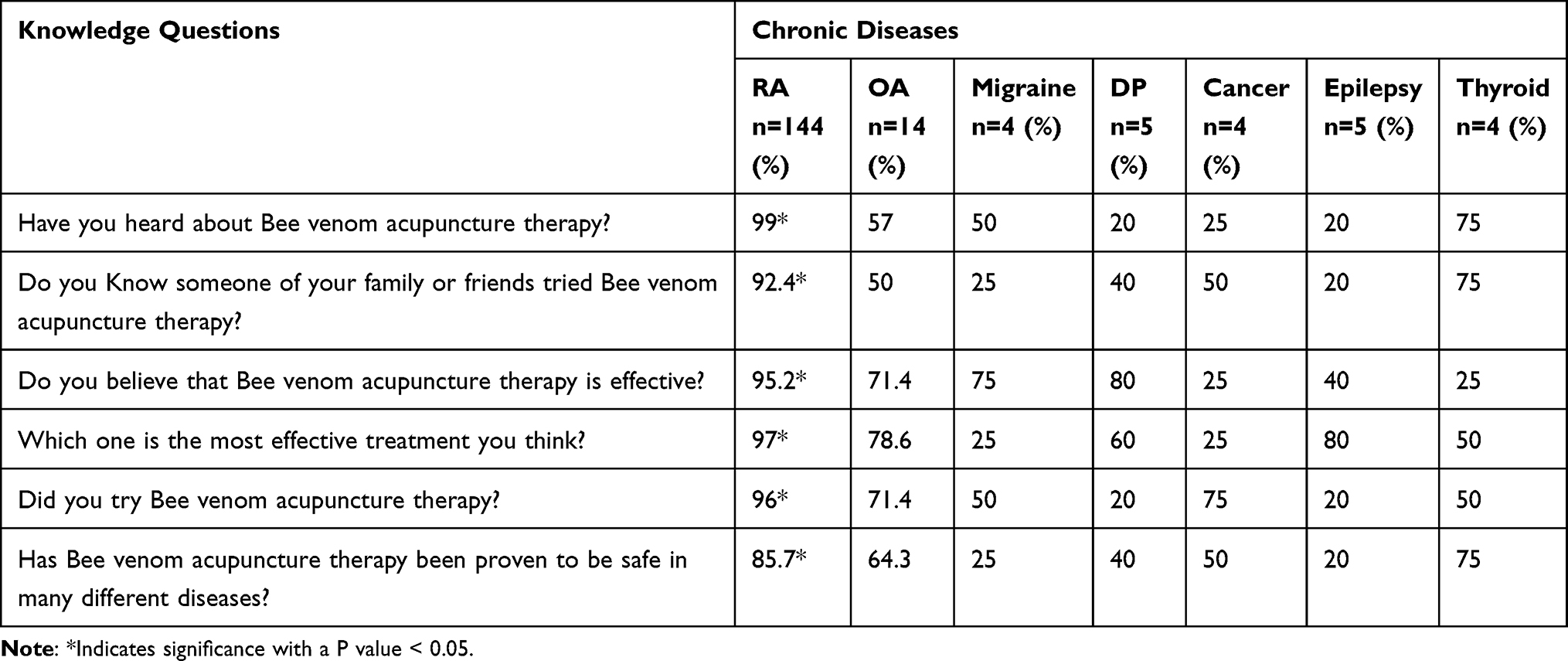 |
Table 4 The Participant’s Knowledge About BVT Association with the Participant’s Chronic Diseases. N=180 |
Attitude Assessment
The overall percentage of attitudes toward BVT was low among the participants, with a total percentage of 55.6% (Figure 1). Figure 3 shows the total percentage distribution of attitudes among participants. Approximately 40% of the participants (n = 72) believed that BVT was an effective medication for the treatment of SA, and 35% believed that it was expensive to use. In addition, 45% of the participants (n = 81) believed that BVT was the same as Chinese acupuncture therapy. We found that 50% of the participants (n = 90) believed that BVT was an effective treatment for their diseases, and 45% (n= 81) believed that BVT was promising for the treatment of chronic diseases. Participants who were working regarded BVT as being more effective in treating their diseases, compared with those who were not working (P <0.05). Interestingly, there was a significant difference between participants who had received only high school education and those who had received further education in terms of whether they considered BVT to be an effective treatment in SA. Participants who had received only high school education considered BVT to be a better treatment option for their diseases, albeit an expensive treatment, compared to those who had received university education (Table 5).
 |
Table 5 The Participant/s Attitude About BVT Association with the Participant’s Characteristics and Educational Background. N=180 |
 |
Figure 3 The total distribution percentage of BVT attitude among the participants. |
Interestingly, participants with RA (n = 144) scored significantly higher (P <0.05) in all the attitude questions compared with participants with other chronic diseases: 85% of participants with RA believe that BVT was an effective treatment in SA, 95% of them believe that BVT was a good treatment option for their diseases, and 89% had tried BVT therapy for their diseases (Table 6).
 |
Table 6 The Participant/s Attitude About BVT Association with the Participant’s Chronic Diseases. N=180 |
Practice Assessment
The overall percentage of practice towards BVT was poor, with a total percentage of 55.6% (Figure 1). Figure 4 shows the total percentage distribution of practice among the participants. Approximately 45% of the participants (n = 81) had at least one session of BVT per week, with 46% (n = 83) having at least two BVT stings per session. Moreover, 40% (n = 72) of patients underwent medical investigations before and after BVT treatment. In addition, 40% (n = 72) underwent BVT for at least one month. Participants who had received only high school education scored significantly higher (P <0.05) in the BVT practice questions than participants with university education. They received a minimum of two stings per session, with one session per week for a minimum of one month. The participants manifested signs of inflammation, including redness and swelling, after the stings, but felt better afterwards. Participants who were beekeepers scored significantly higher (P <0.05) in the questions relating to BVT practice than those who were not beekeepers. The participants underwent the same BVT procedure as discussed above and manifested the same signs but felt better after BVT (Table 7).
 |
Table 7 The Participant/s Practice About BVT Association with the Participant’s Chronic Diseases. N=180 |
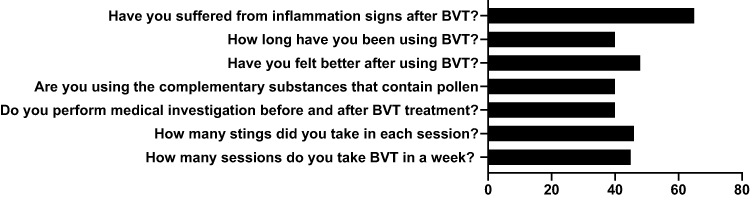 |
Figure 4 The total distribution percentage of BVT practice among the participants. |
Participants with RA (n = 144) scored significantly higher (P <0.05) in most of the practice questions compared with patients with other chronic diseases: 81% of participants with RA received a minimum of two stings per BVT session, 90.5% had one BVT session per week, 81% showed signs of inflammation (redness and swelling) after BVT, and 85.2% felt better after BVT (Table 8).
 |
Table 8 The Participant/s Practice About BVT Association with the Participant’s Characteristics and Educational Background. N=180 |
Discussion
To the best of our knowledge, this study was the first study to assess KAP of BVT among patients with RA and other clinical conditions in SA. Therefore, only limited comparisons of patient’s responses can be demonstrated with other similar studies in the field such as the study conducted by Korean Movement Disorders Society Red Tulip Survey et al, 2014.5 In this study, participants showed good knowledge of the worldwide effects of BVT on RA and other chronic diseases which was a higher percentage in comparisons with the results found in previous study.5 However, the participants showed a poor attitude towards its usage and only a few practiced BVT. This suggests that a good understanding of BVT does not necessarily lead to a positive attitude towards its use and increased practice. Even though the participants were aware of the benefits of BVT for RA, many participants did not comply with the treatment protocol, including the number of BVT sessions, stings, and the essential treatment period. However, this may have been due to several modifiable factors (self-efficacy, time management, and psychological factors such as motivation and depression) or non-modifiable factors (age, sex, and race) as shown in similar conducted studies.2–4 In addition, poor attitude and practice could be understood because BVT is expensive and causes irritative side effects such as redness, fever, and swelling compared to other prescribed medications, which provide relief without side effects.13–15 In addition, BVT may not be available in every city in the country and must be administered by a specialist under specific protocols, with a monitoring doctor to measure the efficacy and clinical outcomes of the treatment.
The results of this study indicate the effects of education on KAP assessments in participants. Interestingly, our results showed that the younger participants knew more about the use of BVT for the treatment of various chronic diseases compared to the older participants. Additionally, our results show that participants who received only school education showed better KAP responses than those with university education. Further, participants who were unemployed demonstrated a better response to the knowledge and attitude questions compared with the participants who were working. This can be explained by the development of medical research worldwide, and the development of new treatment and prevention plans to improve the clinical condition of the patients. Newly discovered therapeutic strategies are recognized by the younger generation, therefore younger people are often more informed than the older generation.
Additionally, the recent advancements in technology, allowing for communication and learning online, has helped increase access for younger participants to medical journals and public health-related information, which were not readily available 30 years ago. This has helped the younger generation to be more aware of available medical research, without needing a medical university degree.
Our results show that participants who were beekeepers demonstrated better responses regarding BVT knowledge and practice than non-beekeeper participants. This is also related to the fact that most beekeepers live in rural areas and tend to receive only school education, rather than a university education, to remain close to their farms to take care of their duties.15
Beekeepers demonstrated better responses towards BVT, which is likely because of their role in the process. Many participants who were beekeepers reported that they believed that BVT was a natural treatment with beneficial effects for chronic diseases, as they believed it to be a safe way to treat and manage chronic diseases such as RA.16
The most common chronic disease identified among the 180 participants was RA, with 80% (n = 144) of the participants having it. In addition, participants with RA gave better responses to BVT KAP questions than those with other chronic diseases. This can be explained by the fact that BVT has been clinically proven to be an effective treatment for RA. Participants with RA (80%) demonstrated that they believed BVT to be effective, safe, and capable of treating RA symptoms. It has been reported that BVT works to treat RA through TAK1\IRAK1\NF-kB signaling, which inhibits the transduction of TNF-α, IL-6, and IL-1, resulting in reduced joint pain and inflammation.17 In addition, BVT affects IL-1β, IL-6, TNF-α, TGF-β1, IFNγ, total oxidant status, total antioxidant status, DNA damage levels, and myeloperoxidase, all of which explain its immunomodulatory, antigenotoxic, antioxidant, and anti-inflammatory effects.18,19 Further, BVT can help patients with RA, even in the late stages of the disease, which has been shown in many previous studies.18,20–22
The results show that participants demonstrated good knowledge of BVT, but poor attitudes and low rates of practice. Participants with RA gave better responses about the KAP of BVT than participants with other chronic diseases, indicating potential clinical therapeutic effects of BVT on RA in SA. Treatment with BVT is expensive, not easily available, and accompanied by inflammation-irritating side effects, which may explain the poor attitude and practice scores. There are few pre-clinical and clinical studies of the direct effects of BVT on RA in SA, therefore this would be the next recommended step in the field. In addition, BVT involves many compounds, such as apamin, melittin, and mast cell-degranulating peptide, and it is essential to illustrate the most critical component of BVT with the most positive clinical outcome for RA.23 The results of this study along with other related studies5,13,15 can be used to develop medical education programs to improve BVT public awareness, structure clinical practice recommendations and improving RA management and patient’s quality of life which can be observed on other previous similar studies.6–10 Additionally, it is important to study the toxicity of melittin metabolites (toxicogenomic) and the in vivo LD50. Moreover, it is important to conduct clinical trials to compare the anti-inflammatory and anti-arthritic effects of BVT and/or melittin with the most current medications available for RA, such as methotrexate, to illustrate the potential use of BVT and/or melittin as replacement treatments for patients with RA in SA. This will facilitate the sequential steps towards official registration of BVT as a replacement therapy for RA after assuring it’s safety and efficacy among the patients.5
Conclusion
In conclusion, 180 participants with RA showed good knowledge of BVT but poor attitude and practice regarding its usage, which may be improved by many factors, such as lowering the cost of BVT, managing the side effects, and increasing the availability of BVT around SA. The present study recommends establishing medical education programs with the help of a team of clinicians (clinical pharmacists, physicians and toxicologists) to increase the awareness and clinical practice of BVT in patients with RA in SA, with the help of the health authorities and MOH. The good understanding of BVT among the citizens in SA with RA will facilitate clinical studies to be conducted, to allow researchers to establish clinical evidence for its use in treating RA. Thus, it is essential to validate and verify the anti-inflammatory effects of BVT by running clinical trials on patients with RA to register it as a replacement or supportive treatment therapy for RA in SA.
Acknowledgments
Special thanks to College of Medicine, Umm Al-Qura University for supporting this clinical study. We would like to thank Dr. Hend Ahmadoh, consultant obstetrician, infertility and IVF at the maternity hospital in Makkah Al-Mukarramah and a member of the International Complementary Medicine Organization contribution process of pilot recruiting before the main survey distribution from the mobile bee centers in Makkah region.
Disclosure
The authors declare there is no conflict of interest for this study.
References
1. Launiala A. How much can a KAP survey tell us about people’s knowledge, attitudes and practices? Some observations from medical anthropology research on malaria in pregnancy in Malawi. Anthropol Matters. 2009;11:1–13.
2. Sharaf S, Al-Shalabi B, Althani G, et al. Obesity self-management: knowledge, attitude, practice, and pharmaceutical use among healthy obese individuals in Saudi Arabia. Int J Fam Community Med. 2021;5(4):110–121. doi:10.15406/ijfcm.2021.05.00232
3. Sharaf S, Alharbi YS, Alsharif RS, et al. Hypertension self-management and antihypertensive prevalence amid patients in Saudi Arabia via knowledge, attitude, and practice assessment. Int J Fam Community Med. 2021;5(4):123–133. doi:10.15406/ijfcm.2021.05.00233
4. Sharaf S, Alsaedi M, Bannani A, et al. Knowledge, attitude, practice, and pharmaceutical outcomes of type 2 diabetes mellitus self-management among patients in Makkah Region, Saudi Arabia. Pharm Pharmacol Int J. 2021;9:8. doi:10.15406/ppij.2021.09.00333
5. Chung SJ, Koh SB, Ju YS, Kim JW; Korean Movement Disorders Society Red Tulip Survey P. Nationwide survey of patient knowledge and attitudes towards human experimentation using stem cells or bee venom acupuncture for Parkinson’s disease. J Mov Disord. 2014;7(2):84–91. doi:10.14802/jmd.14012
6. Chawla R, Madhu SV, Makkar BM, et al. RSSDI-ESI clinical practice recommendations for the management of type 2 diabetes mellitus 2020. Indian J Endocrinol Metab. 2020;24(1):1–122. doi:10.4103/ijem.IJEM_225_20
7. Shiferaw WS, Akalu TY, Desta M, Kassie AM, Petrucka PM, Aynalem YA. Effect of educational interventions on knowledge of the disease and glycaemic control in patients with type 2 diabetes mellitus: a systematic review and meta-analysis of randomised controlled trials. BMJ Open. 2021;11(12):e049806–e. doi:10.1136/bmjopen-2021-049806
8. Arikpo D, Edet ES, Chibuzor MT, Odey F, Caldwell DM. Educational interventions for improving primary caregiver complementary feeding practices for children aged 24 months and under. Cochrane Database Syst Rev. 2018;5(5):CD011768–CD. doi:10.1002/14651858.CD011768.pub2
9. Askland K, Wright L, Wozniak DR, Emmanuel T, Caston J, Smith I. Educational, supportive and behavioural interventions to improve usage of continuous positive airway pressure machines in adults with obstructive sleep apnoea. Cochrane Database Syst Rev. 2020;4(4):CD007736–CD. doi:10.1002/14651858.CD007736.pub3
10. Fairall LR, Folb N, Timmerman V, et al. Educational outreach with an integrated clinical tool for nurse-led non-communicable chronic disease management in primary care in South Africa: a pragmatic cluster randomised controlled trial. PLoS Med. 2016;13(11):e1002178–e. doi:10.1371/journal.pmed.1002178
11. 2030 SAV. Quality of life program 2021. Available from: https://www.vision2030.gov.sa/v2030/vrps/qol/.
12. Almoallim H, Hassan R, Cheikh M, et al. Rheumatoid Arthritis Saudi Database (RASD): disease characteristics and remission rates in a tertiary care center. Open Access Rheumatol. 2020;12:139–145. doi:10.2147/OARRR.S260426
13. Silva J, Monge-Fuentes V, Gomes F, et al. Pharmacological alternatives for the treatment of neurodegenerative disorders: wasp and bee venoms and their components as new neuroactive tools. Toxins. 2015;7(8):3179–3209. doi:10.3390/toxins7083179
14. Feás X. Human fatalities caused by hornet, wasp and bee stings in Spain: epidemiology at state and sub-state level from 1999 to 2018. Biology (Basel). 2021;10(2):73. doi:10.3390/biology10020073
15. Pucca MB, Cerni FA, Oliveira IS, et al. Bee updated: current knowledge on bee venom and bee envenoming therapy. Front Immunol. 2019;10:2090. doi:10.3389/fimmu.2019.02090
16. Cherniack EP, Govorushko S. To bee or not to bee: the potential efficacy and safety of bee venom acupuncture in humans. Toxicon. 2018;154:74–78. doi:10.1016/j.toxicon.2018.09.013
17. Im EJ, Kim SJ, Hong SB, Park JK, Rhee MH. Anti-inflammatory activity of bee venom in BV2 microglial cells: mediation of MyD88-dependent NF-kappaB signaling pathway. Evid Based Complement Alternat Med. 2016;2016:3704764. doi:10.1155/2016/3704764
18. Chen SY, Zhou P, Qin Y. [Treatment of rheumatoid arthritis by bee-venom acupuncture]. Zhen Ci Yan Jiu. 2018;43(4):251–254. Chinese. doi:10.13702/j.1000-0607.170506
19. Kocyigit A, Guler EM, Kaleli S. Anti-inflammatory and antioxidative properties of honey bee venom on Freund’s complete adjuvant-induced arthritis model in rats. Toxicon. 2019;161:4–11. doi:10.1016/j.toxicon.2019.02.016
20. Lee JA, Son MJ, Choi J, Jun JH, Kim J-I, Lee MS. Bee venom acupuncture for rheumatoid arthritis: a systematic review of randomised clinical trials. BMJ Open. 2014;4(11):e006140. doi:10.1136/bmjopen-2014-006140
21. Lee JA, Son MJ, Choi J, Yun KJ, Jun JH, Lee MS. Bee venom acupuncture for rheumatoid arthritis: a systematic review protocol. BMJ Open. 2014;4(4):e004602. doi:10.1136/bmjopen-2013-004602
22. Ghoreschi K, Fischer J, Biedermann T. Manifestation of rheumatoid arthritis during subcutaneous allergen-specific immunotherapy with bee venom. J Allergy Clin Immunol. 2012;130(6):
23. Müller UR. Hymenoptera venom proteins and peptides for diagnosis and treatment of venom allergic patients. Inflamm Allergy Drug Targets. 2011;10(5):420–428. doi:10.2174/187152811797200704
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.