Back to Journals » Infection and Drug Resistance » Volume 15
Knowledge, Attitude and Practice (KAP) Assessment on LifeStyle, Public Health Measures Practiced by Society and Their Impact to Contain COVID-19 Transmission Among Afar Community in Selected Parts of Afar Region, Ethiopia
Authors Adugna B ![]() , Merera O, Negash W
, Merera O, Negash W ![]() , Abdulkadir O
, Abdulkadir O ![]() , Mohammed Y
, Mohammed Y ![]()
Received 22 November 2021
Accepted for publication 19 March 2022
Published 25 March 2022 Volume 2022:15 Pages 1277—1287
DOI https://doi.org/10.2147/IDR.S349019
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Biyansa Adugna, Olana Merera, Wossen Negash, Oumer Abdulkadir, Yasin Mohammed
Department of Veterinary Medicine, College of Veterinary Medicine, Samara University, Samara, Afar, Ethiopia
Correspondence: Biyansa Adugna, Email [email protected]
Introduction: Coronavirus disease (COVID-19) is an infectious disease caused by the SARS-CoV-2 virus, RNA family. It has continued to spread across the world after its first outbreak in China in 2019. On 11 March 2020 the WHO declared COVID-19 a pandemic given its global public health and economic impacts.
Objective: To assess knowledge, attitude and practice (KAP) on lifestyle, public health measures practiced by society and their impact to contain COVID-19 transmission in the Afar community, Afar Region, Ethiopia.
Methods: Community-based cross-sectional study design was conducted from May to July, 2020, on purposively selected districts and the Peasant Association (PA). Simple random sampling was applied to select households and study participants. Structured and semi-structured questionnaire was used to collect information from study participants. The collected data were entered into Microsoft Excel and transferred to SPSS version 20 for analysis. Both descriptive and analytical analysis was provided and a p-value of less than 0.05 was considered as statistically significant.
Results: Of the total (266) study participants, most of them had no formal education (61.7%) and were aged from 35– 40 (34.2%). More than half, 67.7% and 56.8%, of participants did not know chewing chat and smoking cigarettes as a risk factor for COVID-19, respectively. Almost half, 49.6%, of participants live in a house which is non-partitioned and without ventilation. The participants were took part in public gatherings such as funerals (27.1%), weddings (13.9%), meetings (13.5%) and went to a market (9%) during the pandemic. Nearly half (47.7%) of the study participants did not wear facemasks. Of the total, 27.4% and 71.4% participants lost their daily income more than and less than half, respectively.
Conclusion: This study revealed knowledge, attitude and practice of the community in the area to contain COVID-19 spread were minimal. Therefore, more improvement of public health measures will be required.
Keywords: Afar community, COVID-19 impact, public health measures
Introduction
Coronavirus disease (COVID-19) is an infectious disease caused by the SARS-CoV-2 virus, RNA family. Some strains of CoV are zoonotic, meaning they can be transmitted between animals and humans, but many strains are not zoonotic.1 The most likely ecological reservoirs for SARS-CoV-2 are bats, but it is believed that the virus jumped to humans from another intermediate animal host (either domestic or wild species, but not yet identified). After the first infections in China at the end of 2019, COVID-19 has continued to spread across the world.2
The World Health Organization (WHO) declared COVID-19 a pandemic on 11 March 2020 given its impact on the entire world population and the economy. It is important to remember that COVID-19 does not differentiate between borders, ethnicities, disability status, age or gender. The COVID-19 pandemic is exacting a huge toll on individuals, families, communities and societies across the world. While a lot is still unknown about the virus that causes COVID-19, it is transmitted through direct contact with respiratory droplets of an infected person, touching surfaces contaminated with the virus and touching their face (e.g., eyes, nose, mouth).2 There are also higher concentrations of airborne virus transmission in indoor community environments compared with outdoors, especially in small and poorly ventilated environments.3
Many countries are following the advice from the WHO regarding ways to reduce disease transmission, from isolation of infected individuals to implementation of nationwide lockdown. The planning and adjustment of public health measures at national and international levels are of utmost importance to ultimately reach and maintain a state of low level or no transmission of COVIDI-19 with coordinated and multidisciplinary responses.4,5 The COVID-19 pandemic has had an impact at global and national levels in all elements of food systems from primary supply to intermediate and final demand.6,7 The health systems of countries in Africa are weaker than those elsewhere in the world, with fewer health-care service infrastructures, ICUs, health-care professionals for its population and critically dependent on imported medicinal and pharmaceutical products.8,9 Public health measures to contain the spread of COVID-19 include testing and/or quarantine requirements, strong restrictions of non-essential travel, being fully vaccinated with WHO-approved vaccines and to have been tested negative with WHO-approved rRT-PCR tests.10 These measures are particularly difficult for the rural, poorest and most vulnerable communities.11
Developed nations who are traditionally known to assist the poorer ones during such tough times are now badly beaten and on stiff resistance in the battle against the virus themselves and are doing less to assist the developing nations. In developing country like Ethiopia, staying home during lockdown is too difficult because of poor living conditions, lack of basic infrastructure, lack of information due to lack of accessibility to official web platforms, lack of sufficient health service and lifestyle of the community as they depend on daily work income to sustain their basic needs. Therefore, this study aimed to investigate knowledge, attitude and practice on lifestyle, public health measures practiced by society and their impact to contain COVID-19 transmission in the Afar community in selected districts of Afar Regional State, Ethiopia.
Materials and Methods
Study Area
The study was carried out in selected parts of Afar Regional State, northeastern part of Ethiopia. Afar Regional State is located in the Great Rift Valley, comprising rangeland in Northeast Ethiopia with an estimated area of 95,958 km2. The region shares common international boundaries with the state of Eritrea in the north-east and Djibouti in the east. The Regional State has five administrative zones, which are further subdivided into 32 districts. Pastoralism and agro- pastoralism are the two major livelihood ways practiced in the region. The population of the region is estimated to be about 1.4 million of which 90% are pastoralists and 10% agro-pastoralists.12
Study Design and Period
A community-based cross-sectional study design was carried out from May to July, 2020.
Source Population
The source populations are all Afar community found in the Regional State.
Study Population
The study populations are all populations in the study area during the study period.
Sample Size Determination
A single population proportion formula (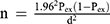 ) was used to calculate the sample size. Therefore, an expected prevalence rate of 50% (no previous study report) and absolute desired precision of 5% at confidence level of 95% was used.12 Accordingly, the sample size became 384. However, due to logistics and constraints faced during the study period a sample size of only 266 was conducted.
) was used to calculate the sample size. Therefore, an expected prevalence rate of 50% (no previous study report) and absolute desired precision of 5% at confidence level of 95% was used.12 Accordingly, the sample size became 384. However, due to logistics and constraints faced during the study period a sample size of only 266 was conducted.
Sampling Methods
Initially, Zone one among zones and Samara-Logia, Dubti and Asayta districts among zone one district and towns were purposively selected for the study due to their frontline location on the main road of Ethio-Djibouti, high population density/dynamics and their mobility to cities for markets. Kebeles and households were selected by simple random sampling. In rural communities peasant association (PA) and households from PA were selected purposively based on proximity to the main road, town and their mobility to town for markets. From the households either the husband or wife was selected as study participant.
Questionnaire Survey
The determinant factors most probably associated with COVID-19 were obtained from different literatures and physical observation of the experts’ experience to be included in questionnaire survey. A pre-tested question was conducted before the actual data were collected for validation of the questionnaire. In depth interviews using a structured and semi-structured questionnaire were conducted with the study participants to collect valuable information about the participants’ lifestyles, public health measures and their impact to contain pandemic COVID-19 spread. The questionnaire covers all socio-demographic information of the participants, their lifestyles and the daily activities that were a risk factor for transmission and spread of COVID-19 within the community and the public health measurements practiced to contain COVID-19 spread. Finally, they were asked the impact of COVID-19 on their lives. To maintain consistency of questionnaire and data, the English version questionnaire was translated to Afari language (local language) and Amharic language (when needed) then translated back to English by an English language expert.
Data Management and Analysis
To assure quality, data collectors were trained prior to data collection regarding technique, ethics of data collection and data collection process, by the principal investigator. A 5% pretest was conducted in a similar setting before the actual data collection. Frequent and timely supervision of data collectors was undertaken by principal investigators. The data were thoroughly cleaned just before coding and carefully entered into Microsoft Excel and exported to SPSS (version 20) statistical package software for analysis. Descriptive statistics were conducted to present data using tables and frequencies and proportions were used to summarize variables. The statistical tests were conducted and significance was considered at a p-value < 0.05.
Ethical Consideration
Before the study was conducted, an ethical clearance letter was obtained from Ethical Review Board of Samara University. Informed written consent was obtained from all study participants prior to enrollment in the study. For participants who were unable to write, a right thumbprint was taken as a signature. Participation in the study was voluntary and participants were informed of the right to refuse to take part in the study if not interested. Confidentiality of the participants’ information was ensured throughout the study. All the procedures involved in the study was accomplished according to the Declaration of Helsinki ethical standards and Ethical review committee of Samara University.
Results
Socio-Demographic Characteristics of Study Participants
Primarily, the goal of this paper is to present an overview of the first results of the KAP assessment on lifestyle, public health measures practiced by society and their impact to contain COVID-19 transmission in the Afar community in selected districts of Afar Region, Ethiopia.
From the total 266 participants, 39.5%, 37.6% and 22.9% of the respondents were from Dubti district, Asayita district and Samara-Logiya town, respectively. Regarding kebeles, the highest numbers of respondents were from Debel and Gebelayto with same respondents (35; 13.2%) and the lowest number of respondents was from Hinale (14; 5.3%). Among the total respondents, 34.2% of the respondents were aged between 35–40 years followed by 27.8% above 44 years, 25.2% were aged between 25–34 years and 12.8% of the respondents were aged between 15–24 years. The majority (174; 65.4%), of the respondents were male. Regarding educational status, most (61.7%) of the respondents had no formal education. According to residence of respondents, equal numbers (50%) of the study participants were involved in this study from rural and urban areas (Table 1).
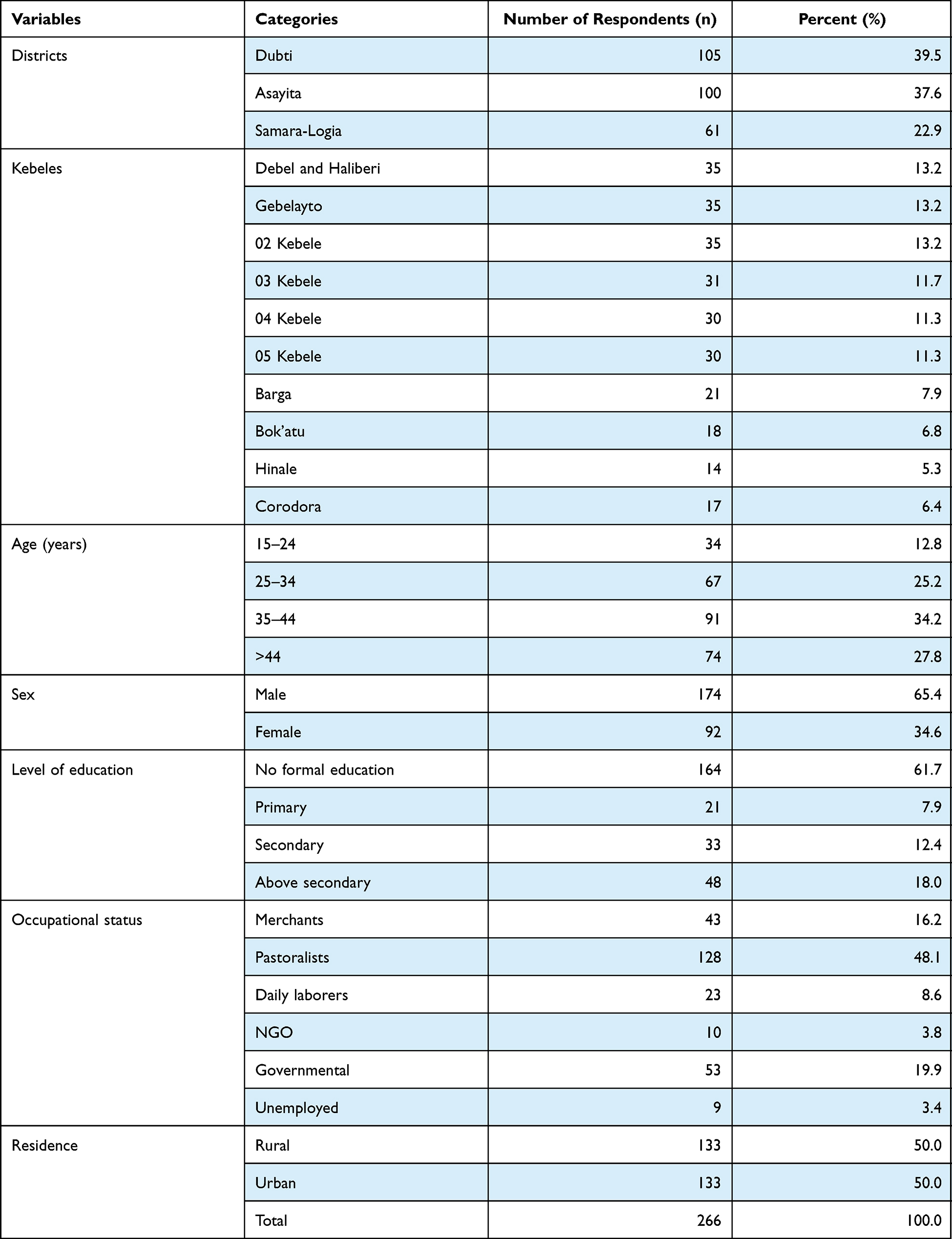 |
Table 1 Socio-Demographic Characteristics of the Participants (n = 266) |
Assessment of the Lifestyle of the Study Participants
With regard to housing style of the study participants, almost half (49.6%) of the respondents lived in a non-partitioned house without ventilation and 129 (48.5%) of the respondents had a partitioned house with ventilation. Of the total participants, 77 (28.9%) of the respondents were smokers of cigarettes and the majority (56.8%) of the respondents did not know smoking cigarettes was a risk factor for COVID-19 infection. With regard to chat/khat chewing habit, half (50%) of the study participants had a habit of chewing chat/khat. The majority (67.7%) of the respondents did not know chewing chat/khat was a predisposing factor for COVID-19 infection. With regard to the transportation history, almost (51.1%) of the respondents had history of transportation outside their district (Table 2).
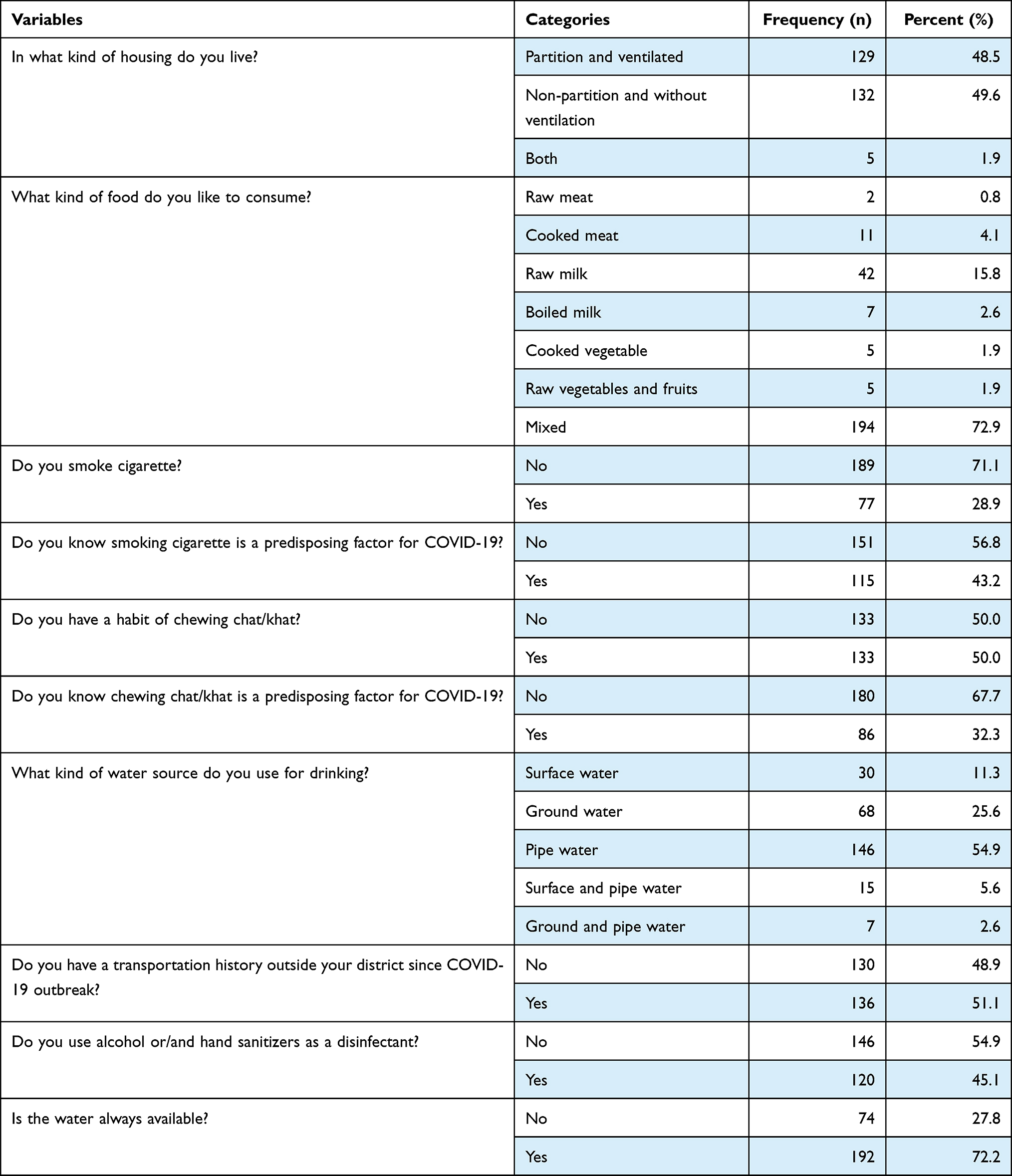 |
Table 2 Assessment of the Life Style of Participants |
Assessment of Public Health Measures Practiced by Society to Contain COVID-19 Transmission
In terms of COVID-19 preventive measures during transportation, the highest number (42.5%) of the participants wore a facemask and the lowest number (3.8%) used hand gloves and sanitizer or/and alcohol while 25.9% of the respondents did not use any preventive measures during transportation. Regarding zoonotic importance, the majority (64.3%) of the study participants stated that COVID-19 was not a zoonotic disease. In terms of sources of information about Covid-19, TV or/and radio (72.6%) was the most frequently used and other social media platforms (3.8%) were the least source of information by the respondents. Based on accessibility of health facilities for COVID-19, half (50.4%) of the respondents knew of a health-care facility for COVID-19 in their surrounding area. The majority (68%) of the study participants had visited health-care facility when they felt discomfort while a minority (32%) of the respondents had not visited a health-care facility when they felt discomfort since the outbreak of COVID-19. Based on symptoms and signs of COVID-19, the respondents stated as mixed type (78.9%), coughing (5.6%), fever (5.6%), difficulty in breathing (4.1%) and headache (1.5%) as symptoms of COVID-19 while (3.4%) of the respondents did not mention any symptoms or/and signs of COVID-19 (Table 3).
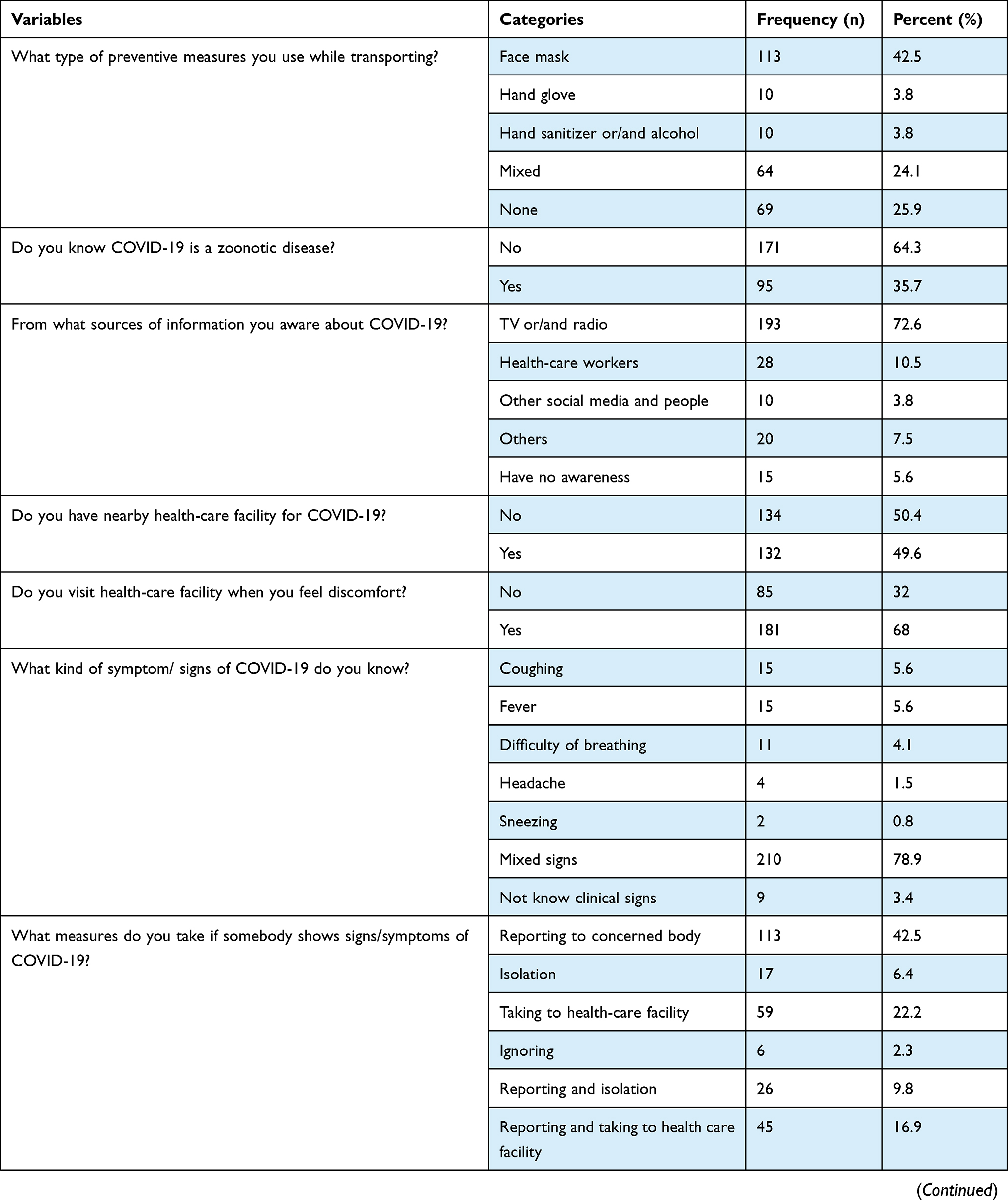 | 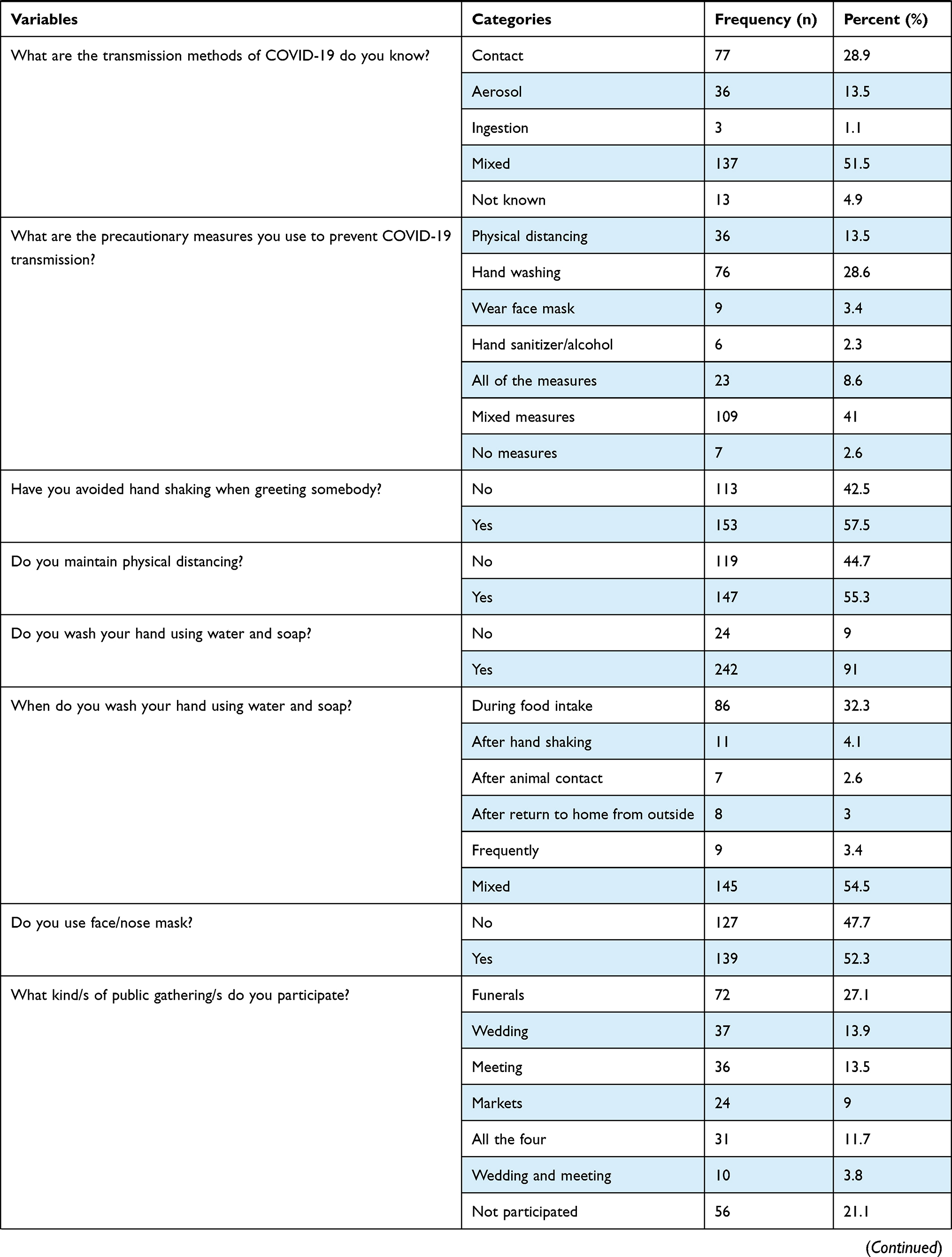 | 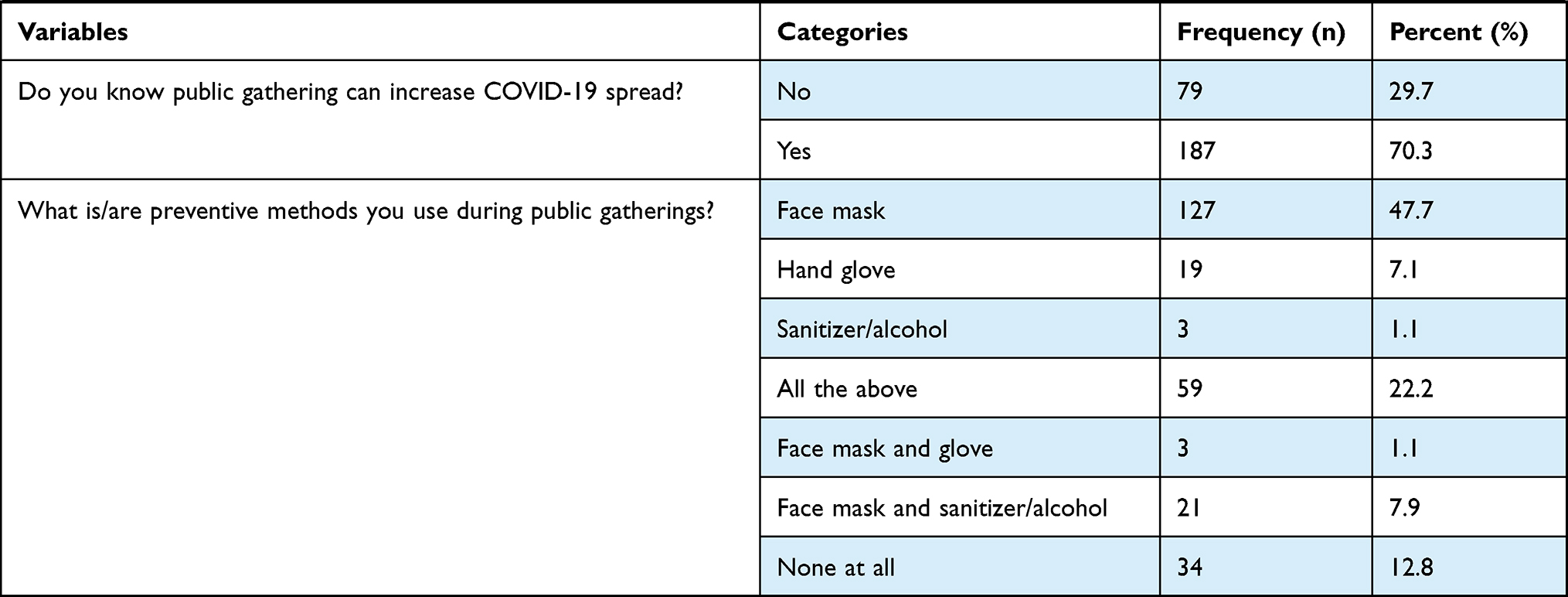 |
Table 3 Assessment of Public Health Measures Practiced by Society to Contain COVID-19 Transmission |
Regarding preventive measures to be taken by the participants if they or anyone have or feel COVID-19 symptoms/signs, 42.5% of the respondents stated that they report to the concerned body, 22.2% of the respondents stated that they went to a health-care facility, 16.9% of the respondents stated that they reported and went to a health-care facility, 9.8% of the respondents stated they reported and isolated while 2.3% of the respondents stated they were ignored by the community. Based on transmission methods of COVID-19, almost all (94.1%) of the respondents stated that COVID-19 was transmitted through mixed type (contact, aerosol and ingestion) while 4.9% of the respondents stated that they did not know any transmission methods of COVID-19 as a whole (Table 3).
In terms of precautionary measures for prevention of COVID-19 transmission, the majority of the participants used hand washing (28.6%) followed by physical distancing (13.5%) and wearing a facemask (3.4%). Of the total participants, more than half (57.5%) of the study participants were avoiding hand shaking when greeting somebody as a preventive measure of COVID-19 transmission. Regarding public gatherings during the COVID-19 pandemic, 27.1% of the respondents had participated in a funeral; 13.9% of the respondents had participated in a wedding; 13.5% of the respondents had participated in a meeting and 9% of the respondents had participated in a market. Of the total participants, the majority (70.3%) stated public gatherings as a risk factor for the spread of COVID-19 infection (Table 3).
Economic and Zoonotic Impact Assessment of COVID-19
With regard to impact assessment, nearly all (95.1%) of the study participants stated COVID-19 had an impact on economy/business. Majority (71.4%) of the respondents stated that they had lost nearly half of their daily income during the COVID-19 pandemic. The study participants reported that they lost their daily income due to loss of market (44%), loss of employment (9.8%) and lack of transportation (18.8%) during lockdown. With regard to zoonotic importance of COVID-19, 71.1% of the study participants had different species of domestic animals in their home. Of the total study participants, the majority (64.3%) of the respondents stated that there was no COVID-19 transmission from livestock to humans and only 35.7% of the respondents stated the possibility of COVID-19 transmission from livestock to humans (Table 4).
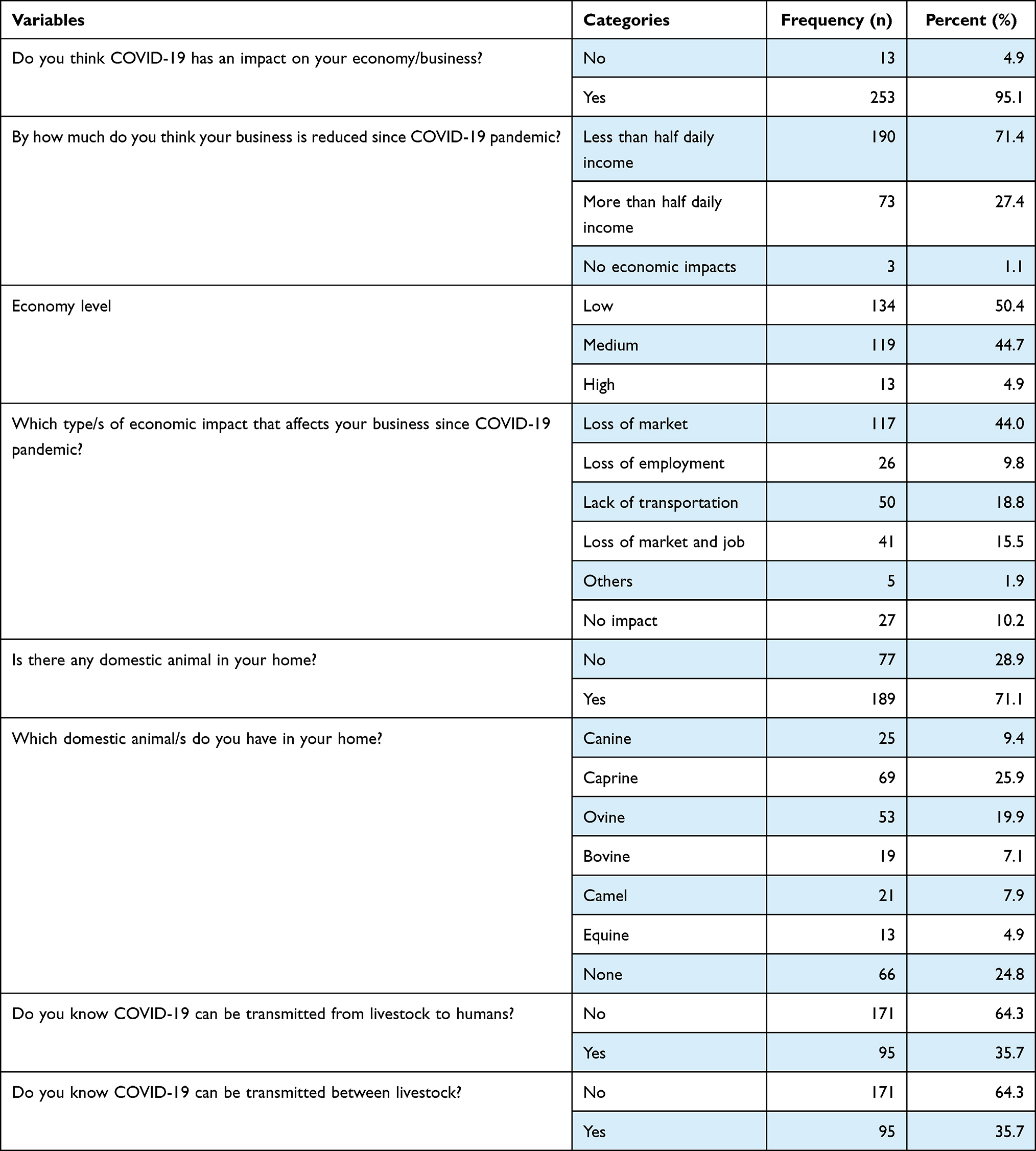 |
Table 4 Economic and Zoonotic Impact of COVID-19 |
Discussion
Since the outbreak in epicenter, Wuhan, in December 2019, COVID-19 has rapidly become a threat to public health and led to substantial socioeconomic damage worldwide. All over the world, flights have been canceled and transport systems have been closed. Millions of people have been put under lockdown in order to reduce the transmission of the virus.
With almost every country adopting aggressive non-therapeutic measures to control the spread of COVID-19, Ethiopia has followed the same trend; however, there is an ongoing debate as to whether measures have been adopted adequately and implemented efficiently since March 7, 2020 when the first COVID-19 case confirmed.
To our knowledge, this study is the first KAP assessment conducted related to COVID-19 in Afar Regional State, Ethiopia. Therefore, it provides valuable insights into public health to acquire appropriate knowledge, attitude and practice to prevent COVID-19 spread during the pandemic. In the present study more participants were male (65.4%) compared with female. This is similar to the results of study conducted in Bangladesh, male (57.1%)13 but it is inconsistent with a study reported in Iran14 with higher female (66.4%) participants. In our study, most of the participants had no formal education (61.7%) which is similar to another study conducted in Ethiopia.7
Our study also showed that almost all (94.4%) of the study participants were aware of COVID-19. The majority of participants had obtained information about COVID-19 from television (TV) and radio (72.6%). This finding is higher than the study conducted in other parts of Ethiopia Silte Zone, Southern Ethiopia15 and a study conducted in Cameroon with the information obtained from television (54.5%)16 but it is almost inline with a study conducted in Turkey.17 This indicates that television and radio are the main sources of information for the participants compared with other social media platforms. This discrepancy might be due to the different social media platforms used between the country and the study participants. In our study, the majority of the study participants answered that smoking cigarettes and chewing chat/khat were not a risk factor for COVID-19. In our result, the majority (51.1%) of the study participants had a transportation history out of their districts during the pandemic period. This indicates that there was a high probability of COVID-19 spread into the community in the study area and vice versa.
In terms of awareness level of the respondents about COVID-19, all respondents were asked about symptoms/signs of COVID-19 infection and 78.9% stated as mixed type (coughing, fever, headache, sneezing and difficulty in breathing), followed by coughing (5.6%), fever (5.6%), difficulty in breathing (4.1%), headache (1.5%) and sneezing (0.8%). The participants were asked about the accessibility of public health services in their surroundings; 49.6%, less than half, of the respondents stated that they do not have facilities in their surroundings. The study participants were also asked about the preventive measures they took if they or anyone in their surroundings have or feel one of the COVID-19 symptoms, and 42.5% of the respondents stated that they report to the concerned body and 22.2% of the respondents stated that they went to the health facility. This study finding is more or less similar with a study conducted in Turkey.17
Furthermore, this study showed that lower knowledge (35.7%) was responded from the study participants regarding zoonotic transmission of COVID-19. In our study more than half of the study participants wore facemasks (53.4%) when they left their home, maintained physical distancing (53.3%), washed their hands using water and soap (91%) and avoided hand shaking (57.5%) when greeting somebody as preventive measures during the COVID-19 pandemic. This finding is higher than the findings of a study conducted in northern parts of Ethiopia7 and much lower than the finding of the study in China18 where nearly all of the participants (98.0%) wore facemasks when they left their home. This low practice of wearing facemasks in Ethiopia might be due to the inability to afford and the scarcity of facemasks in the country.
Conclusion and Recommendation
The study results revealed that many of the study participants had taken part in public gatherings such as funerals, weddings, meeting and markets without using public health measurement protocols. The knowledge, attitude and practice of the community in the area to contain COVID-19 spread are minimal. Therefore, more improved awareness of public health measures to contain COVID-19 spread in the community and epidemiological investigation of possible risk factors of COVID-19 will be required.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Shi J, Shi J, Wen Z, et al. Susceptibility of ferrets, cats, dogs, and other domesticated animals to SARS – coronavirus 2. Science. 2020;7015:1–10.
2. Woral Health Organization. Coronavirus disease 2019 (COVID-19) report; 2020.
3. Abarca RM. Measurements of Sars-Cov-2 RNA concentrations in indoor and outdoor air in Italy: implications for the role of airborne transmission. Nuevos Sist Comun e Inf. 2021;8:39.
4. Cascini F, Hoxhaj I, Zaçe D, et al. How health systems approached respiratory viral pandemics over time: a systematic review. BMJ Glob Heal. 2020;5(12):1–16.
5. Safety F, Businesses F. COVID-19 and food safety: guidance for food businesses; 2020: 1–6.
6. Schmidhuber J, Pound J, Qiao B. COVID-19: channels of transmission to food and agriculture. Covid. 2020;19(38):44.
7. Akalu Y, Ayelign B, Molla MD; Hospital AZ. Knowledge, attitude and practice towards COVID-19 among chronic disease patients at Addis Zemen hospital, Northwest Ethiopia. Infect Drug Resist. 2020;13:1949.
8. Iom un Migration. Iom Asia and the Pacific regional strategic preparedness and response plan COVID-19; 2020: 1–16.
9. ECA EC for. COVID-19 in Africa; 2020.
10. Cascini F, Causio FA, Failla G, et al. Emerging issues from a global overview of digital COVID-19 certificate initiatives. Front Public Heal. 2021;9:1–5.
11. Adhikari SP, Meng S, Wu Y, et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: a scoping review. Infect Dis Poverty. 2020;9:1–12.
12. Thrusfield M. Veterinary Epidemiology.
13. Banik R. Investigating knowledge, attitudes, and practices related to COVID-19 outbreak among Bangladeshi young adults: a web- based cross-sectional analysis; 2020: 1–13.
14. Erfani A, Shahriarirad R, Ranjbar K. Knowledge, attitude and practice toward the novel coronavirus (COVID-19) outbreak: a population-based survey in Iran; 2020.
15. Yesse M, Muze M, Kedir S, et al. Assessment of knowledge, attitude and practice toward COVID-19 and associated factors among health care workers in Silte zone, Southern Ethiopia. PLoS One. 2021;16:1–11. doi:10.1371/journal.pone.0257058
16. Ngwewondo A, Nkengazong L, Ambe LA, et al. Knowledge, attitudes, practices of/towards COVID 19 preventive measures and symptoms: a cross-sectional study during the exponential rise of the outbreak in Cameroon. PLoS Negl Trop Dis. 2020;14:1–15.
17. Knowledge Attitude and Practice (KAP). Endline report situation of Syrian refugees under COVID 19 pandemic; 2021.
18. Zhang M, Zhou M, Tang F, et al. Knowledge, attitude, and practice regarding COVID-19 among healthcare workers in Henan, China. J Hosp Infect. 2020;105(2):183–187. doi:10.1016/j.jhin.2020.04.012
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.