Back to Journals » Risk Management and Healthcare Policy » Volume 14
Knowledge, Attitude, and Perceived Risks Towards COVID-19 Pandemic and the Impact of Risk Communication Messages on Healthcare Workers in Saudi Arabia
Authors Mushi A, Yassin Y ![]() , Khan A
, Khan A ![]() , Yezli S, Almuzaini Y
, Yezli S, Almuzaini Y ![]()
Received 12 February 2021
Accepted for publication 2 June 2021
Published 5 July 2021 Volume 2021:14 Pages 2811—2824
DOI https://doi.org/10.2147/RMHP.S306402
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Marco Carotenuto
Abdulaziz Mushi,1 Yara Yassin,1 Anas Khan,1,2 Saber Yezli,1 Yasir Almuzaini1
1The Global Centre for Mass Gatherings Medicine, Ministry of Health, Riyadh, Saudi Arabia; 2Department of Emergency Medicine, College of Medicine, King Saud University, Riyadh, Saudi Arabia
Correspondence: Abdulaziz Mushi
Public Health Directorate, Global Centre for Mass Gatherings Medicine, Ministry of Health, Riyadh, Saudi Arabia
Tel +966506830492
Email [email protected]
Purpose: To investigate knowledge, attitude, and perceived risks towards COVID-19 pandemic among healthcare workers (HCWs) in Saudi Arabia. Besides, the impact of risk communication strategy on the attitude and practice of HCWs was investigated.
Patients and Methods: We conducted a cross-sectional study that targeted HCWs from various Saudi health facilities. We utilized a self-administrated, online-based questionnaire designed to assess basic knowledge of COVID-19, attitude and disease perception, and the impact of risk communication messages among HCWs.
Results: A total of 1691 responses were received in the study. The HCWs exhibited good levels of knowledge (total maximum score is 1) of COVID-19 concerning the modes of transportation of COVID-19 (0.82± 0.16), sample collection method for COVID-19 diagnosis (0.98± 0.08), transmission of infection from asymptomatic individuals (0.99± 0.11), and that antibiotics are not effective against the new COVID-19 (0.83± 0.38). Nearly one-third of the participants considered a high/very high possibility of acquiring COVID-19 infection. HCWs had good attitude scores concerning their willingness to deal with new COVID-19 patients (0.87± 0.33) and their beliefs in being educated on COVID-19 (0.99± 0.11). Almost all participants strongly agree/agree that it is important to take action to prevent the spread of COVID-19 within healthcare facilities and received health information messages. Notably, 93.4% of the participants stated that the received messages changed their attitude towards COVID-19 and its preventive measures. Good knowledge scores were significantly associated with age > 49 years old, higher educational level, and physician occupation. Similarly, good attitude scores were higher among males, HCWs aged 40– 49 years old, non-Saudi nationals, and physician and nurse occupations.
Conclusion: HCWs have fair knowledge and attitude towards the COVID-19 pandemic. The risk communication is an effective strategy to improve the attitude and practice of HCWs towards COVID-19 in Saudi Arabia.
Keywords: COVID-19 pandemic, knowledge, attitude, risk communication, perceived benefits, Saudi Arabia
Introduction
The novel coronavirus disease 2019 (Covid-19) has spread rapidly in different countries till becoming a global pandemic as declared by the World Health Organization (WHO) on March 11, 2020,1 causing a massive impact on healthcare services and economics.2 Given that no effective treatment is currently available, preventive measures represent the cornerstone in managing the pandemic, including quarantine and lockdown measures, facial masks, hand hygiene,3–5 and self-isolation in suspected cases.6 Nonetheless, community compliance is crucial for the successful implementation of these measures; the public’s perception about the risk of the disease and their knowledge about proper preventive strategies play a critical role in limiting pandemic spread.7 Recently, a growing body of evidence has tried to identify the level of knowledge and attitude towards the COVID-19 pandemic across different populations. However, these studies showed variable results as the population awareness and attitude regarding the COVID-19 can differ significantly by geographical distribution, age, gender, education level, and occupation.8,9
Healthcare workers (HCWs) represent the cornerstone in the fight against the COVID-19 pandemic. Previous reports showed that HCWs are at high risk of acquiring the infection and psychological distress during pandemics;10 besides, they play a crucial role in disseminating proper knowledge during an emergency.11 Therefore, it is imperative that HCWs have knowledge and attitude towards the COVID-19 pandemic to ensure their strict compliance to control measures and effectively disseminate accurate information about the pandemic.12 Nonetheless, the current body of published literature shows conflicting results regarding the level of HCWs’ knowledge and attitudes regarding COVID-19.12–14 Likewise, studies from the Middle East showed variable levels of HCWs’ knowledge and attitudes regarding COVID-19.15–17 Thus, big data and real-life evidence are needed to orient the already challenged healthcare systems during the pandemic and reflect the single community dynamics.18–20
As stated by WHO, risk communication is “the exchange of real-time information, advice, and opinions between experts and people facing threats to their health, economic or social well-being”.21 It is widely acknowledged that effective risk communication during a pandemic, which encompasses risk perception and measures to minimize it, can improve public perception of the benefits of preventive measures, compliance. Besides, it can mitigate exaggerated displays of panic in the form of uncontrolled buying of medications, goods, and personal protective equipment (PPE).11,22 Thus, a successful risk communication strategy should positively impact HCWs’ perceived risk of infection, knowledge, and attitude towards the COVID-19 pandemic.
Saudi Arabia is the largest county in the Arabian Peninsula. It has a well-established healthcare system that is offered for free to all residents. The health system in Saudi Arabia consists mainly of MOH-affiliated public hospitals, other governmental institutions, and the private sector.23 The healthcare system is equipped with 494 hospitals and 22.5 beds per 10,000 inhabitants.24 In 2019, there were a total of 113,000 physicians in Saudi Arabia.25 In Saudi Arabia, the authority has taken several risk communication measures to minimize the risk of COVID-19 transmission.26,27 These measures include a daily press conference by the Ministry of Health (MoH),28,29 public Health Hotline Center to provide reliable information and mitigate public concerns, professional media materials, using media platforms and social media to deliver scientific information in a public language,24 and mobile applications to provide educational information.30,31
Although recent reports have tried to evaluate public knowledge and attitude towards the COVID-19 pandemic in Saudi Arabia,32,33 little information is available concerning the impact of risk communication on HCWs’ knowledge and attitudes during this pandemic. This cross-sectional, survey-based study aimed to investigate knowledge, attitude, and perceived risks towards the COVID-19 pandemic among HCWs in Saudi Arabia. Besides, we assessed the impact of risk communication strategy on the attitude and practice of HCWs towards the COVID-19 pandemic. We hypothesized that the risk communications strategies provided by Saudi authorities led to good levels of HCWs’ knowledge and attitude towards the COVID-19 pandemic.
Methodology
Study Design and Population
We conducted a survey-based, cross-sectional study that targeted HCWs in Saudi Arabia aged over 18 years; HCWs from various health facilities were recruited regardless of their history of contact with suspected/confirmed COVID-19 cases. The participants were recruited through the period from May 20 to June 4, 2020, at the various healthcare institutions. All HCWs on duties were invited via online-based surveys; a healthcare worker who does not deliver services was excluded. All procedures were done after ethical approval from participating centers and the MOH in Saudi Arabia (IRB log. No.: 20–76M). The cover page of the online survey stated the main objectives of the study and informed the participants that their answers to the survey’s questions will be used to assess the study’s objectives. Thus, participants, who filled the survey, implied their consent to participate in the study. All personal data of the participants were anonymized or maintained with confidentiality. The was conducted in accordance with the Declaration of Helsinki.
Data Collection and Questionnaire Validation
We utilized a self-administrated, online-based questionnaire designed to assess the impact of risk communication among HCWs during the new COVID-19 pandemic in Saudi Arabia and collect information concerning HCWs’ knowledge and attitude towards the disease. The questionnaire was distributed online to eligible participants using a standardized platform. This platform was customized to permit only one response from every participant. Each participant received an email that enclosed the study’s objectives and the questionnaire link. The questionnaire was developed in English and Arabic by reviewing available surveys in the literature and WHO recommendations.8,13,34,35 Two public health experts then reviewed the questionnaire content.
The questionnaire consisted of four parts. The first part collected the demographics and professional characteristics of the included HCWs. The second part consists of seven questions that collect some basic information about the participant’s knowledge of COVID-19. The third part collected data regarding the attitude towards COVID-19, including HCWs’ willingness to deal with COVID-19 cases, COVID-19 education, level of knowledge in dealing with COVID-19, and level of adherence towards the standard precautionary measures stated by the MOH. The last part of the questionnaire consisted of eight items concerned with HCWs’ perception of risk communication principles. Besides, HCWs were asked about their level of trust towards the most commonly utilized sources of information about the COVID-19 pandemic. A scoring system was developed to score the knowledge and attitude of study participants, as described previously.36,37 Briefly, incorrect/inappropriate were given a 0 score, while one point was given for choosing the correct/appropriate answer; a correct/appropriate response was based on current literature and the good attitude. For multiple-choice questions with more than one correct answer, one score was given for the correct/appropriate response and for not choosing the incorrect/inappropriate responses. The question’s score was then divided by the total number of multiple-choices in the question to standardize the scores to be between 0 and 1. Additionally, overall mean scores, ranging from 0 to 1, were calculated for each section of the questionnaire (knowledge and attitude). They were then further divided into four categories to reflect the level of knowledge and attitude among HCWs: poor (score <0.25), below average (0.25 ≤ score < 0.50), above average (0.5 ≤ score < 0.75), and good (score ≥0.75).
Sample Size Calculation and Statistical Analysis
We used the Raosoft ® sample size calculator to calculate the appropriate sample size for this survey using the following parameters: a 95% confidence interval, a response distribution of 50%, and a 3% margin of error. The targeted sample size was calculated to be 1067 participants. After adjusting for a projected 10% attrition, the target sample size for the study was 1200 participants. By the end of the study, we enrolled a larger sample size of 1746 HCWs after excluding participants who did not provide direct healthcare services.
Frequencies and percentages were used for categorical variables. Continuous variables were represented as means ±standard deviations (SD), minimum, and maximum. The association between categorical variables was evaluated by the Chi-square test or Fisher’s exact test, as appropriate. Continuous variables were assessed using the Independent t-test or One-way ANOVA. Bivariate and multivariate logistic regression models were also conducted between the variables and good knowledge/ attitude scores, respectively. All significance tests were two-sided, and a p-value of <0.05 was considered statistically significant. All analyses were performed using IBM SPSS Statistics version 25.0 (IBM Corp., Armonk, NY, USA).
Results
Study Population and Demographics
A total of 1691 responses were received in the study, with a mean age of 36.94 ±9.21 years and female predominance (53.6%). Nearly 55.4% of the HCWs worked within the MOH-affiliated sector. The majority of the sample were physicians (35%) and nurses (26.4%). Nearly half of the HCWs sample had already dealt with one or more suspected/confirmed COVID-19 cases (Table 1).
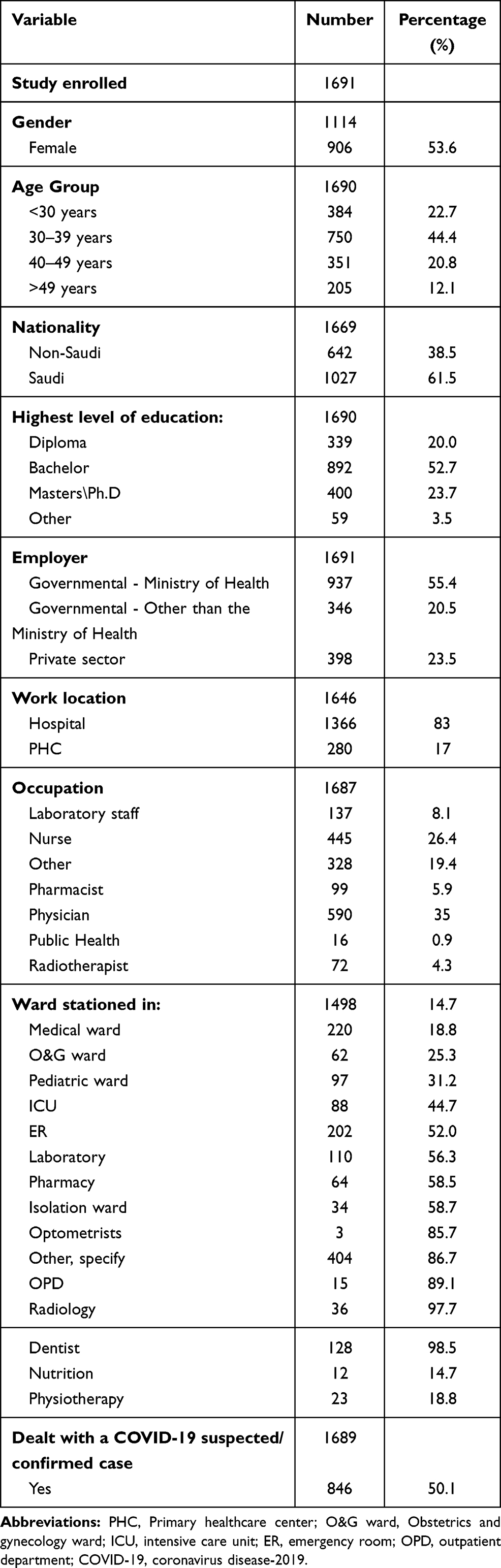 |
Table 1 Demographic and Professional Characteristics of the Study Population |
Knowledge and Attitude Towards COVID-19
Table 2 presented the knowledge and attitude scores of HCWs regarding COVID-19.
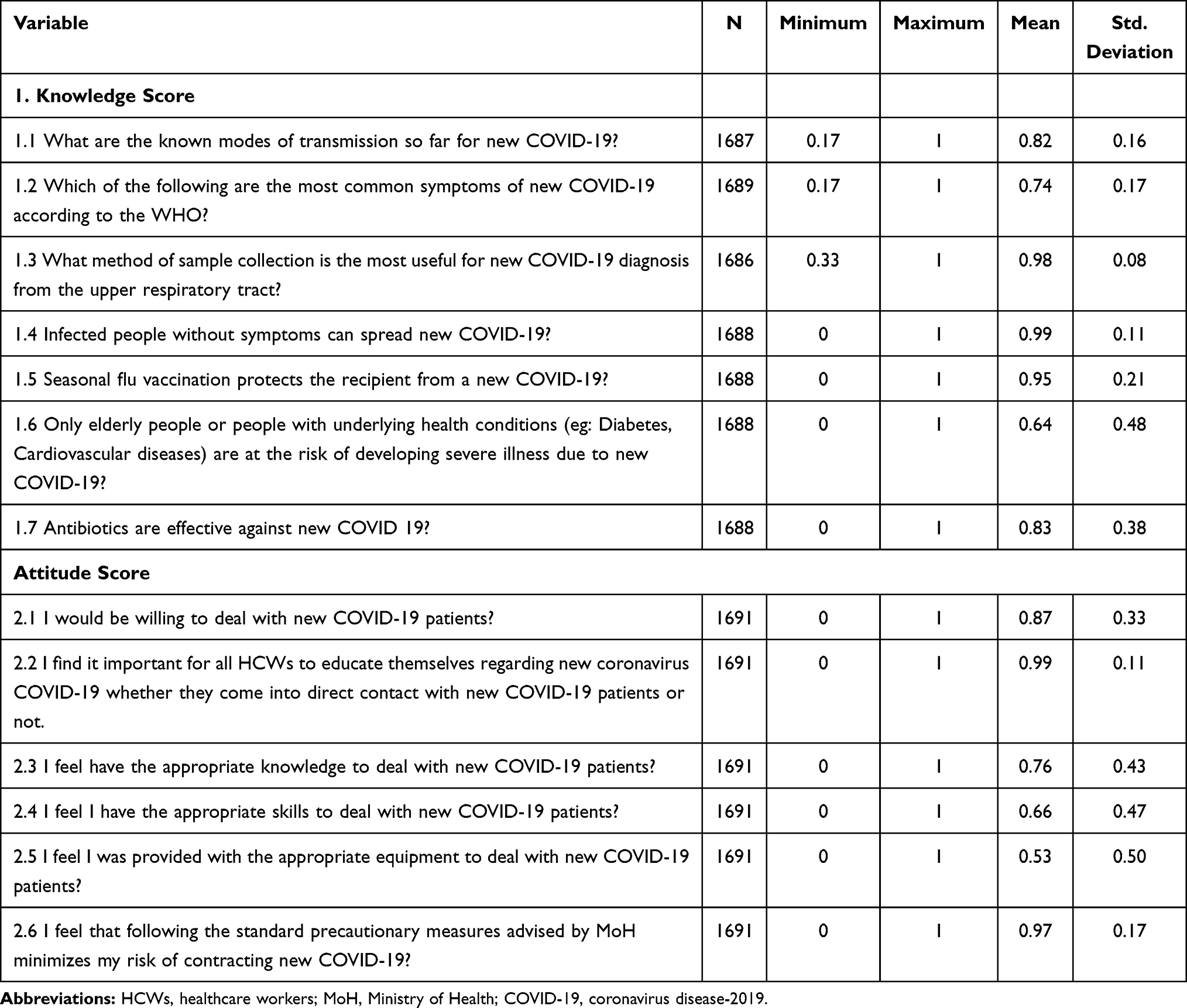 |
Table 2 The Knowledge and Attitude Scores of HCWs Regarding COVID-19 |
The HCWs exhibited good levels of knowledge of COVID-19 concerning the modes of transportation of COVID-19 (0.8±0.2), which sample collection method is the most useful for the diagnosis of COVID-19 (0.9±0.1), the knowledge of asymptomatic individuals infecting other healthy individuals (0.9±0.1), the knowledge that the seasonal flu vaccine does not protect recipients from the new COVID-19 (0.9±0.2), and antibiotics are not effective against the new COVID-19 (0.8±0.4). The level of the remaining two items was above average. The overall mean knowledge score was 0.9 ±0.1; 1343 participants (84.8%) had good level of knowledge (score >0.75) regarding COVID-19 pandemic (Figure 1).
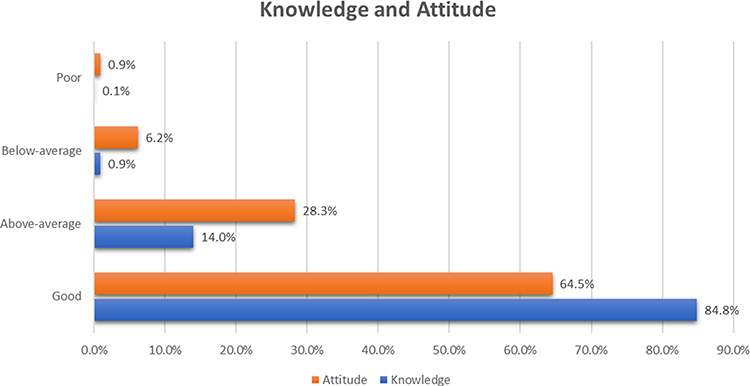 |
Figure 1 Level of knowledge and attitude towards COVID-19 pandemic among HCWs in Saudi Arabia. |
On the other hand, HCWs had good attitude scores concerning their willingness to deal with new COVID-19 patients (0.9±0.3), their beliefs in being educated on COVID-19 (0.9±0.1), their feeling of having the appropriate knowledge when dealing with new COVID-19 patients (0.8±0.4), and their feeling that following the standard precautionary measures advised by MOH would minimize HCWs risk of contracting new COVID-19 (0.9±0.2). The remaining two items were scored above average. The overall mean knowledge score was 0.8 ±0.2; 1091 participants (64.5%) had good level of attitude (score >0.75) regarding COVID-19 pandemic (Figure 1).
Risk Communication Practice
Nearly all participants (97.9%) received health information messages concerning COVID-19 and strongly agreed/agreed that it is important to take actions to prevent the spread of COVID-19 within healthcare facilities. Most (94.1%) HCWs felt a chance to develop COVID-19 while conducting their duties (Table 3).
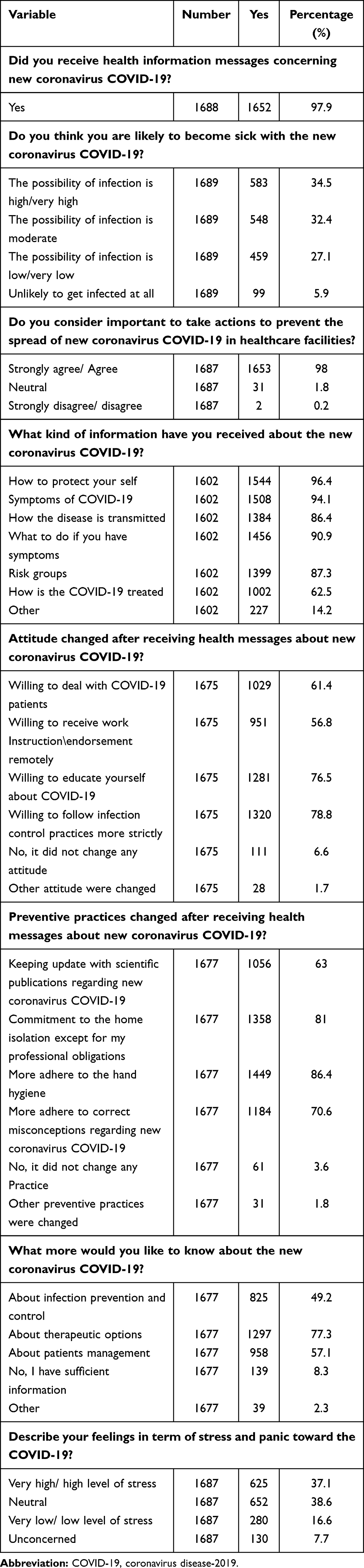 |
Table 3 Risk Communication Messages Practice |
Regarding the impact of the health messages on HCWs’ attitude, 93.4% of the participants stated that the received messages changed their attitude towards COVID-19, mainly in the form of applying stricter infection control practices (78.8%) and self-education about COVID-19 (76.5%). Besides, participants reported attitude changes regarding the willingness to deal with COVID-19 patients (61.4%) and receiving work instructions/endorsement remotely (56.8%). Preventive measures were also impacted after receiving health messages regarding COVID-19 (Table 3).
Finally, HCWs were asked about what type of information they would like to know more about regarding COVID 19; the majority reported that they would like to know more about therapeutic options (77.3%). Overall, the majority of the sample (89.4%) felt that there is a gap of information that they believe they need to have fulfilled (Table 3). The most trusted source regarding received information related to COVID 19, as reported by the HCWs, was the Saudi MOH (96.2%), followed by the WHO (56.4%).
Predictors of Good Knowledge and Attitude Levels
HCWs with higher education levels had higher knowledge mean scores (p <0.001). Besides, physicians and pharmacists had the highest knowledge mean scores than remaining occupations (p <0.001; Table 4). At the multivariate level, nurse occupation (OR 0.4, 95% CI 0.3–0.7, p =0.001), being a radiotherapist (OR 0.3, 95% CI 0.1–0.6, p =0.001), and public health occupation (OR 0.2, 95% 0.1–0.8, p =0.021) were independent negative predictors of good knowledge levels (Table 5).
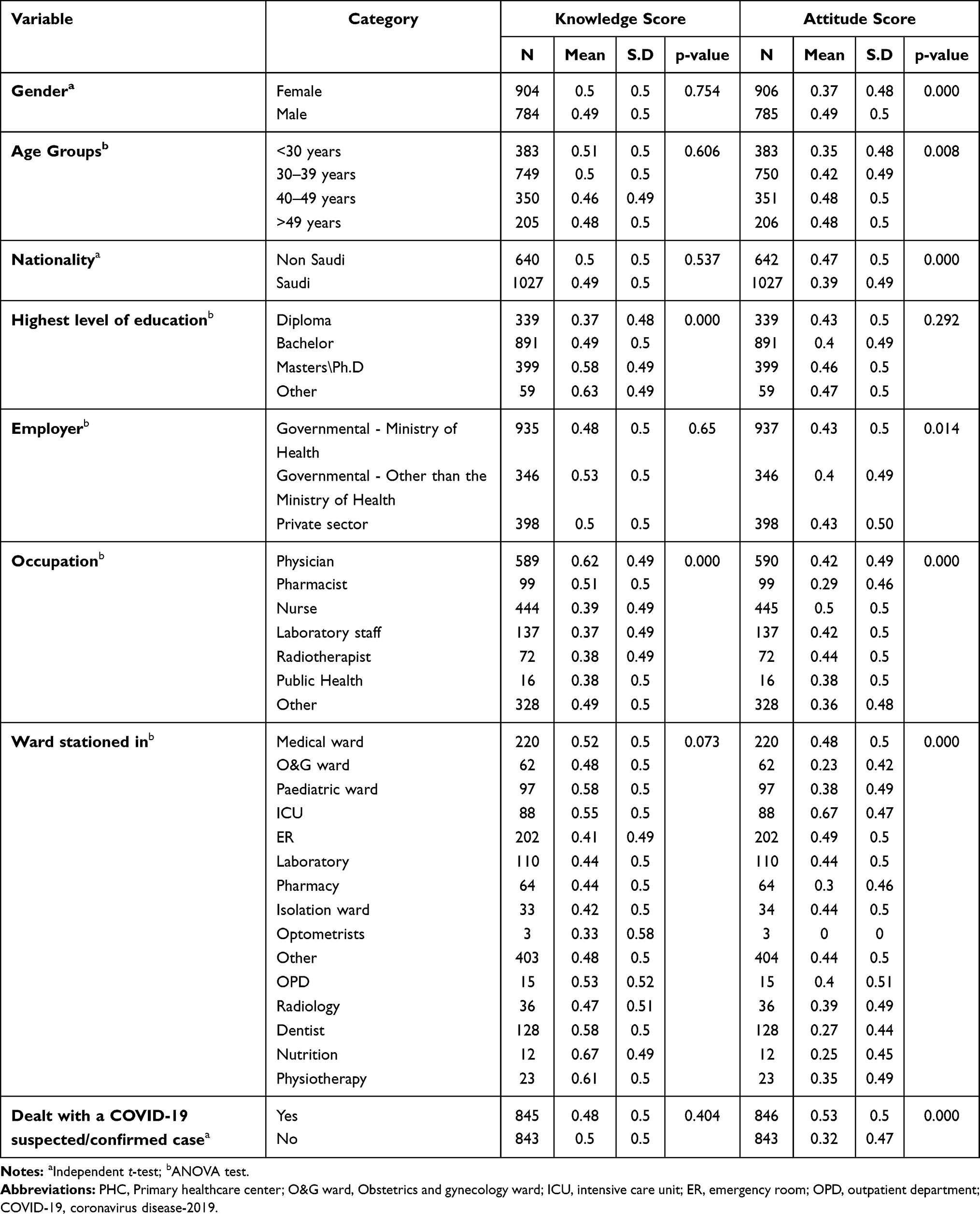 |
Table 4 The Association Between Knowledge/Attitude Scores and HCW’s Characteristics |
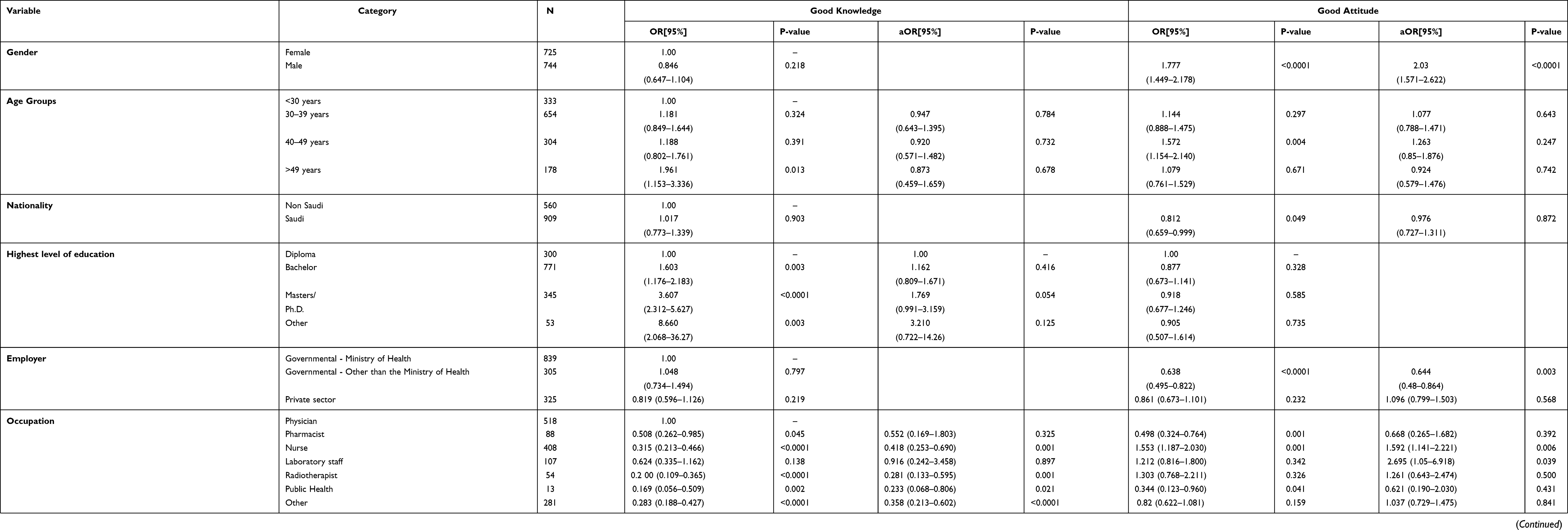 |
Table 5 The Univariate and Multivariate Regression Analysis for Predictors of Good Knowledge/Attitude Scores |
The results demonstrated that the attitude mean scores were significantly higher among males (p <0.001), older age groups (p =0.008), non-Saudis (p <0.001), HCWs work within a governmental sector other than the MOH (P=0.014), nurses (P<0.0001), HCWs stationed in ICU (P<0.0001), and HCWs with a history of dealing with COVID19 patient (P<0.0001; Table 4). At the multivariate level, male gender (OR 2, 95% CI 1.6–2.6; p <0.001), nurse occupation (OR, 1.6, 95% CI 1.1–2.2, p =0.006), being a laboratory staff (OR 2.7, 95% CI 1.1–6.9, p =0.039), being stationed in ICU (OR 2.9, 95% CI 1.5–5.8, p =0.001), being stationed in the ER (OR 1.8, 95% CI (1.1–2.9), p =0.017), and dealing with COVID-19 suspected/confirmed cases (OR 2.6, 95% CI 2–3.3, p <0.001) were independent positive predictors of good attitude score. On the other hand, working in governmental sectors other than the MOH (OR 0.6, 95% CI 0.5–0.9, p =0.003) was an independent negative predictor of good attitude score (Table 5).
There was a statistically significant positive correlation between knowledge and attitude (p < 0.0001).
Discussion
The landscape of the COVID-19 pandemic has changed dramatically in the EMR, including Saudi Arabia, with a sharp rise in the number of documented cases and related mortality.38 During this unprecedented time, community compliance with preventive measures and limited panic-related behaviors play a crucial role in the pandemic’s successful control.11 It is well-established that an improper risk management strategy can negatively impact public compliance to self-protective measures, especially when these measures interfere with normal activities or have socioeconomic impacts.39 Effective risk communication represents the cornerstone for a risk management strategy aiming to improve not only how people perceive health risks during the pandemic but also how they react to healthcare emergencies and adhere to self-protective measures.11,40–42 In the case of the COVID-19 pandemic, with its associated high transmission rates, morbidities, and mortality, lack of proper risk communication can exaggerate panic displays, increase public confusion, or lead to unfavorable perception towards the benefits of preventive measures.43 In this regard, HCWs are the frontline soldiers in the fight against COVID-19; previous reports demonstrated that HCWs account for up to 24% of the global number of documented COVID-19 cases.44 It is postulated that insufficient information about COVID-19 transmission, incubation period, and clinical symptoms are the main reasons for the high risk of infection among HCWs;45 thus, it is of paramount importance to ensure proper risk communication among this vulnerable group during the COVID-19 pandemic. Besides, HCWs are key players in the expert–public communication component of the risk communication strategy,46,47 and ensuring reliable risk perception in this group would potentially reflect on public perception and compliance during the pandemic.
Thus, we aimed to understand the impact of risk communication on the perceived risk and attitude towards COVID-19 among HCWs in Saudi Arabia. Our results demonstrated that only one-third of the HCWs perceived themselves at a high possibility of acquiring COVID-19 infection. Nonetheless, HCWs within the Kingdom positively perceived the benefits of preventive measures and health messages; these messages positively changed HCW’s attitude and practice towards COVID-19-related preventive measures. Besides, the majority of the HCWs stated that there is a gap of information that needs to be fulfilled. To our knowledge, there no published reports about the impact of risk communication among HCWs in Saudi Arabia. In a recent report by Abolfotouh et al,48 HCWs from Saudi Arabia exhibited a high level of concerns about acquiring COVID-19 infection and a high level of support of actions taken by healthcare authorities to minimize infection risk. Besides, HCWs in this report stated an unmet gap regarding the information about COVID-19 in the media.48 In another report that covered ten countries from America, Europe, and Asia, the information received from government and healthcare professionals was a significant predictor of proper COVID-19 risk perception,49 highlighting the beneficial role of risk communication on the perceived risk and attitude towards COVID-19 pandemic. Thus, healthcare authorities in the Kingdom should implement continuous education programs and training that support HCWs with updated information and protocols on minimizing the risk of COVID-19 infection in the hospital setting. Besides, clear and pertinent guidance about applying preventive measures during COVID-19 should be developed to aid HCWs in minimizing the risk of infection. Future research should also focus on the impact of different risk communication strategies on the HCWs’ knowledge and attitude.
Proper knowledge is a major determinant of any successful control strategy during health emergencies. Previous reports highlighted that the high level of knowledge was a driven factor for proper implementation of preventive measures and authority’s directives during previous outbreaks such as severe acute respiratory syndrome (SARS) and H1N1 influenza.50,51 Particularly, the importance of proper knowledge among HCWs cannot be overstated, owing to their high risk of infection and the public view of HCWs as a trusted source of information during a health crisis. This survey found that HCWs from Saudi Arabia had good knowledge about basic COVID-19 information such as mode of transmission, clinical presentation, and standard of care. Such good knowledge can be viewed in the context of effective risk communication, as stated earlier. Such findings are in line with reports from China,12 Egypt,15 and Pakistan.13 On the contrary, a recent report from the United Arab Emirates demonstrated a poor level of knowledge among HCWs.16 Notably, our findings demonstrated that good knowledge was significantly associated with older age, and the educational level above diploma degree and physician occupation. We postulated that these findings stem from the fact that the elderly are more vulnerable to severe presentations of COVID-19 and, hence, they are more eager for self-education about basic information of the COVID-19 pandemic. Likely, physicians are more likely to get in direct contact with COVID-19 cases than other specialties –such as pharmacists and laboratory staffs-. Our findings come in agreement with Abdel Wahed et al,15 in which physicians and HCWs with an educational level above diploma had significantly higher knowledge scores. Previous studies further support the impact of age and education on the knowledge level during previous outbreaks.52 Therefore, it is essential to launch targeted educational campaigns covering HCWs with low educational level, non-physician occupations, and non-MOH workers.
Behavioral changes are critical for the successful implementation of any precautionary measures and risk communication strategy. Previous reports demonstrated that attitude and perception are major driving factors for behavioral changes during outbreaks.53 In this regard, HCWs are at increased risk of psychological stress, burnout, and occupational stigma, especially during the time of pandemic.15,48 Such factors may be associated with negative personal feelings towards the work environment during the pandemic, dealing with new cases, and the response of the government to the epidemic management.54,55 In return, the unfavorable attitude by HCWs can lead to improper self-protection practice and delayed diagnosis.15 In this report, we found that HCWs from Saudi Arabia had good attitude levels towards dealing with COVID-19, governmental actions to minimize the risk of infection, and their level of knowledge and preparation to face the pandemic. Such findings are in line with reports from China,12 Egypt,15 and Pakistan.13 HCWs from these countries exhibited fair levels of attitude towards the COVID-19 pandemic in dealing with confirmed cases and measures to minimize the spread of infection. Concerning the predictors of good attitude levels, we found that the male gender was an independent positive predictor of good attitude score. Such findings may be attributed to the higher level of education among males in Saudi Arabia, gender difference in employment status, higher exposure to pandemic-related information among males, and the fact that males are more likely to suffer from more severe forms of COVID-19 than females.56 Besides, the results showed that nurse occupation, being stationed in ICU or ER, and dealing with COVID-19 suspected/confirmed cases were independent positive predictors of good attitude score. Such findings are expected since these occupations deal closely with hospitalized COVID-19 cases and accumulate more experience, knowledge, and favorable attitude.57
Study Limitations
While the present study has the strength of a large sample size and comprehensive coverage of HCWs from different institutions and levels of care, we acknowledge the existence of some limitations in this survey. Our survey was based on a self-reported, online-based survey that might suffer from selective participation, difficulties in measuring attrition rates, and liability to participants’ feelings during survey filling. Besides, the questionnaire was not validated quantitatively, which might have affected the precision of our conclusion.
Conclusion
Our results demonstrated that HCWs felt a notable change in their attitude after receiving proper information about COVID-19 from health authorities. Thus, healthcare authorities in the Kingdom should implement continuous education programs and training that support HCWs with updated information and protocols on minimizing the risk of COVID-19 infection in the hospital setting. Besides, clear and pertinent guidance about applying preventive measures during COVID-19 should be developed to aid HCWs in minimizing the risk of infection. On the other hand, HCWs from Saudi Arabia exhibited fair levels of knowledge and attitude towards COVID-19; however, the knowledge of HCWs towards the impact of old age on the outcomes of COVID-19 and the presentation of the disease was unsatisfactory. Higher levels of knowledge and attitude were significantly associated with higher educational levels, physician occupation, and working in MOH affiliated hospitals. Therefore, it is essential to launch targeted educational campaigns covering HCWs with low educational level, non-physician occupations, and non-MOH workers.
Disclosure
The authors report no conflicts of interest in this work.
References
1. (WHO) WHO. Rolling updates on coronavirus disease (COVID-19).
2. World Health Organization. Weekly Operational Update on COVID-19 October 23, 2020. 2020.
3. Alzyood M, Jackson D, Aveyard H, Brooke J. COVID-19 reinforces the importance of handwashing. J Clin Nurs. 2020;29(15–16):2760–2761. doi:10.1111/jocn.15313
4. Głabska D, Skolmowska D, Guzek D. Population-based study of the influence of the COVID-19 pandemic on hand hygiene behaviors-polish adolescents’ COVID-19 experience (place-19) study. Sustain. 2020;12(12):4930. doi:10.3390/SU12124930
5. Beiu C, Mihai M, Popa L, Cima L, Popescu MN. Frequent hand washing for COVID-19 prevention can cause hand dermatitis: management tips. Cureus. 2020;12(4). doi:10.7759/cureus.7506
6. Güner R, Hasanoğlu İ, Aktaş F. Covid-19: prevention and control measures in community. Turkish J Med Sci. 2020;50(SI–1):571–577. doi:10.3906/sag-2004-146
7. Lau JTF, Griffiths S, Choi KC, Tsui HY. Widespread public misconception in the early phase of the H1N1 influenza epidemic. J Infect. 2009;59(2):122–127. doi:10.1016/j.jinf.2009.06.004
8. Zhong B-L, Luo W, Li H-M, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745–1752. doi:10.7150/ijbs.45221
9. Abdelhafiz AS, Mohammed Z, Ibrahim ME, et al. Knowledge, Perceptions, and Attitude of Egyptians Towards the Novel Coronavirus Disease (COVID-19). J Community Health. 2020;45(5):881–890. doi:10.1007/s10900-020-00827-7
10. Selvaraj SA, Lee KE, Harrell M, Ivanov I, Allegranzi B. Infection Rates and Risk Factors for Infection among Health Workers during Ebola and Marburg Virus Outbreaks: a Systematic Review. J Infect Dis. 2018;218(suppl_5):S679–S689. doi:10.1093/infdis/jiy435
11. Abrams EM, Greenhawt M. Risk Communication During COVID-19. J Allergy Clin Immunol Pract. 2020;8(6):1791–1794. doi:10.1016/j.jaip.2020.04.012
12. Zhang M, Zhou M, Tang F, et al. Knowledge, attitude, and practice regarding COVID-19 among healthcare workers in Henan, China. J Hosp Infect. 2020;105(2):183–187. doi:10.1016/j.jhin.2020.04.012
13. Saqlain M, Munir MM, Rehman SU, et al. Knowledge, attitude, practice and perceived barriers among healthcare workers regarding COVID-19: a cross-sectional survey from Pakistan. J Hosp Infect. 2020;105(3):419–423. doi:10.1016/j.jhin.2020.05.007
14. Kassie BA, Adane A, Tilahun YT, Kassahun EA, Ayele AS, Belew AK. Knowledge and attitude towards COVID-19 and associated factors among health care providers in Northwest Ethiopia. PLoS One. 2020;15(8 august):e0238415. doi:10.1371/journal.pone.0238415
15. Abdel Wahed WY, Hefzy EM, Ahmed MI, Hamed NS. Assessment of knowledge, attitudes, and perception of health care workers regarding COVID-19, a cross-sectional study from Egypt. J Community Health. 2020;45(6):1. doi:10.1007/s10900-020-00882-0
16. Bhagavathula AS, Aldhaleei WA, Rahmani J, Mahabadi MA, Bandari DK. Knowledge and perceptions of COVID-19 among health care workers: cross-sectional study. JMIR Public Health Surveill. 2020;6(2):e19160. doi:10.2196/19160
17. El-Nassir A, Mohammed S. Knowledge, attitudes, and practices towards COVID-19 among health care workers in primary health care units Dar El Salam, Sohag, Egypt. Sohag Med J. 2021;25(1).
18. Bragazzi NL, Dai H, Damiani G, Behzadifar M, Martini M, Wu J. How big data and artificial intelligence can help better manage the covid-19 pandemic. Int J Environ Res Public Health. 2020;17(9):3176. doi:10.3390/ijerph17093176
19. Damiani G, Allocco F, Malagoli P. COVID-19 vaccination and patients with psoriasis under biologics: real-life evidence on safety and effectiveness from Italian vaccinated healthcare workers. Clin Exp Dermatol. 2021. doi:10.1111/ced.14631
20. Damiani G, Gironi LC, Grada A, et al. COVID-19 related masks increase severity of both acne (maskne) and rosacea (mask rosacea): multi-center, real-life, telemedical, and observational prospective study. Dermatol Ther. 2021;34(2):e14848. doi:10.1111/dth.14848
21. WHO. General information on risk communication.
22. Cope JR, Frost M, Richun L, Xie R. Assessing knowledge and application of emergency risk communication principles among public health workers in China. In: Disaster Medicine and Public Health Preparedness. Vol. 8. Cambridge University Press;2014:199–205. doi:10.1017/dmp.2014.29
23. Walston SL, Al-Harbi Y, Al-Omar B. The changing face of healthcare in Saudi Arabia. Ann Saudi Med. 2008;28(4):243–250. doi:10.5144/0256-4947.2008.243
24. Ministry of Health Saudi Arabia. Saudi Arabia’s Experience in Health Preparedness and Response to COVID-19 Pandemic.; 2020. Available from: https://www.moh.gov.sa/en/Ministry/MediaCenter/Publications/Documents/COVID-19-NATIONAL.pdf.
25. Saudi Arabia physicians total number 2010-2019 | statista. Available from: https://www.statista.com/statistics/608539/total-number-of-physicians-in-saudi-arabia/. Accessed March 1, 2021.
26. Yezli S, Khan A. COVID-19 social distancing in the Kingdom of Saudi Arabia: bold measures in the face of political, economic, social and religious challenges. Travel Med Infect Dis. 2020;37:101692. doi:10.1016/j.tmaid.2020.101692
27. Atique S, Itumalla R. Hajj in the Time of COVID-19. Infect Dis Health. 2020;25(3):219–221. doi:10.1016/j.idh.2020.04.001
28. Saudi Arabia Ministry of Health. Protect against COVID-19 [Internet]; 2020. Available from: https://covid19awareness.sa/en/home-page.
29. MOH News. Coronavirus Follow-up Committee Holds its 20th Meeting. Available from: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-03-10-008.aspx.
30. Saudi Arabia Ministry of Health. (Tetamman) App, E-Services [Internet]. 2020. Available from: https://www.moh.gov.sa/en/eServices/Pages/Rest-assured.aspx.
31. Saudi Arabia Ministry of Health. (Mawid) Service: e-Services [Internet]. Available from: https://www.moh.gov.sa/en/eServices/Pages/cassystem.aspx.
32. Almofada SK, Alherbisch RJ, Almuhraj NA, et al. Knowledge, attitudes, and practices toward COVID-19 in a Saudi Arabian population: a cross-sectional study. Cureus. 2020;12(6). doi:10.7759/cureus.8905
33. Alhazmi A, Ali MHM, Mohieldin A, Aziz F, Osman OB, Ahmed WA. Knowledge, attitudes and practices among people in Saudi Arabia regarding COVID-19: a cross-sectional study. J Public Health Res. 2020;9(3):1867. doi:10.4081/jphr.2020.1867
34. Olum R, Chekwech G, Wekha G, Nassozi DR, Bongomin F. Coronavirus Disease-2019: knowledge, attitude, and practices of health care workers at Makerere University Teaching Hospitals, Uganda. Front Public Health. 2020;8. doi:10.3389/fpubh.2020.00181
35. WHO. Coronavirus disease (COVID-19) outbreak. Emergencies - Diseases.
36. Yezli S, Mushi A, Yassin Y, Maashi F, Khan A. Knowledge, attitude and practice of pilgrims regarding heat-related illnesses during the 2017 hajj mass gathering. Int J Environ Res Public Health. 2019;16(17):3215. doi:10.3390/ijerph16173215
37. Yezli S, Yassin Y, Mushi A, et al. Knowledge, attitude and practice (KAP) survey regarding antibiotic use among pilgrims attending the 2015 Hajj mass gathering. Travel Med Infect Dis. 2019;28:52–58. doi:10.1016/j.tmaid.2018.08.004
38. Dil S, Dil N, Maken ZH. COVID-19 trends and forecast in the eastern mediterranean region with a particular focus on Pakistan. Cureus. 2020. doi:10.7759/cureus.8582
39. Vaughan E, Tinker T. Effective health risk communication about pandemic influenza for vulnerable populations. Am J Public Health. 2009;99(SUPPL. 2):S324. doi:10.2105/AJPH.2009.162537
40. Damiani G, Gironi LC, Kridin K, et al. Mask-induced Koebner phenomenon and its clinical phenotypes: a multicenter, real-life study focusing on 873 dermatological consultations during COVID-19 pandemics. Dermatol Ther. 2021;34(2):e14823. doi:10.1111/dth.14823
41. Cristaudo A, Pigliacelli F, Pacifico A, Damiani G, Iacovelli P, Morrone A. Teledermatology and hygiene practices during the COVID-19 pandemic. Contact Dermatitis. 2020;83(6):536. doi:10.1111/cod.13683
42. Cinelli E, Fabbrocini G, Fattore D, Marasca C, Damiani G, Annunziata MC. Safe distance, safe patients! Therapeutic management of oncological patients affected by cutaneous and mucosal adverse events during the COVID-19 pandemic: an Italian experience. Support Care Cancer. 2020;28(9):3991–3993. doi:10.1007/s00520-020-05563-1
43. Sumo J, George G, Weah V, et al. Risk communication during disease outbreak response in post-Ebola Liberia: experiences in Sinoe and Grand Kru counties. Pan Afr Med J. 2019;33(Suppl 2):4. doi:10.11604/pamj.supp.2019.33.2.16877
44. Chen P, Lei J, Chen F, Zhou B. Experiences and perceptions risk of health-care workers from coronavirus: a protocol for systematic review. Medicine. 2020;99(20). doi:10.1097/MD.0000000000020308
45. Ali S, Noreen S, Farooq I, Bugshan A, Vohra F. Risk assessment of healthcare workers at the frontline against COVID-19. Pak J Med Sci. 2020;36(COVID19–S4):S99–S103. doi:10.12669/pjms.36.COVID19-S4.2790
46. Zhang L, Li H, Chen K. Effective risk communication for public health emergency: reflection on the COVID-19 (2019-nCoV) Outbreak in Wuhan, China. Healthc (Basel, Switzerland). 2020;8(1). doi:10.3390/healthcare8010064
47. Glik DC. Risk communication for public health emergencies. Annu Rev Public Health. 2007;28(1):33–54. doi:10.1146/annurev.publhealth.28.021406.144123
48. Abolfotouh MA, Almutairi AF, Banimustafa AA, Hussein MA. Perception and attitude of healthcare workers in Saudi Arabia with regard to Covid-19 pandemic and potential associated predictors. BMC Infect Dis. 2020;20(1):719. doi:10.1186/s12879-020-05443-3
49. Dryhurst S, Schneider CR, Kerr J, et al. Risk perceptions of COVID-19 around the world. J Risk Res. 2020:1–13. doi: 10.1080/13669877.2020.1758193
50. Lau JTF, Yang X, Tsui H, Kim JH. Monitoring community responses to the SARS epidemic in Hong Kong: from day 10 to day 62. J Epidemiol Community Health. 2003;57(11):864–870. doi:10.1136/jech.57.11.864
51. Lau JTF, Kim JH, Tsui H, Griffiths S. Anticipated and current preventive behaviors in response to an anticipated human-to-human H5N1 epidemic in the Hong Kong Chinese general population. BMC Infect Dis. 2007;7(1). doi:10.1186/1471-2334-7-18
52. Alhazmi AM, Alshammari SA, Alenazi HA, et al. Community’s compliance with measures for the prevention of respiratory infections in Riyadh, Saudi Arabia. J Fam Commun Med. 2019;26(3):173–180. doi:10.4103/jfcm.JFCM_4_19
53. Tang CSK, Wong CY. An outbreak of the severe acute respiratory syndrome: predictors of health behaviors and effect of community prevention measures in Hong Kong, China. Am J Public Health. 2003;93(11):1887–1889. doi:10.2105/ajph.93.11.1887
54. Teck YW, Koh GCH, Seng KC, et al. Concerns, perceived impact and preparedness in an avian influenza pandemic - a comparative study between healthcare workers in primary and tertiary care. Ann Acad Med Singapore. 2008.
55. Balkhy HH, Abolfotouh MA, Al-Hathlool RH, Al-Jumah MA. Awareness, attitudes, and practices related to the swine influenza pandemic among the Saudi public. BMC Infect Dis. 2010;10(1). doi:10.1186/1471-2334-10-42
56. Galasso V, Pons V, Profeta P, Becher M, Brouard S, Foucault M. Gender differences in COVID-19 attitudes and behavior: panel evidence from eight countries. Proc Natl Acad Sci U S A. 2020;117(44):27285–27291. doi:10.1073/pnas.2012520117
57. Liyew B, Dejen tilahun A, Kassew T. Knowledge, attitude, and associated factors towards physical assessment among nurses working in intensive care units: a multicenter cross-sectional study. Crit Care Res Pract. 2020;2020. doi:10.1155/2020/9145105
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.