Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Knowledge Atlas of Insular Epilepsy: A Bibliometric Analysis
Authors Li M, Ma X, Mai C, Fan Z, Wang Y, Ren Y ![]()
Received 11 October 2022
Accepted for publication 6 December 2022
Published 14 December 2022 Volume 2022:18 Pages 2891—2903
DOI https://doi.org/10.2147/NDT.S392953
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Yu-Ping Ning
Manli Li,1 Xiaoli Ma,1 Chendi Mai,1 Zhiru Fan,1 Yangyang Wang,2 Yankai Ren1
1Department of Physiology, Sanquan College of Xinxiang Medical University, Xinxiang, People’s Republic of China; 2Ningxia Key Laboratory of Cerebrocranial Disease, Ningxia Medical University, Yinchuan, People’s Republic of China
Correspondence: Yankai Ren, Department of Physiology, Sanquan College of Xinxiang Medical University, Xinxiang, People’s Republic of China, Email [email protected] Yangyang Wang, Ningxia Key Laboratory of Cerebrocranial Disease, Ningxia Medical University, Yinchuan, People’s Republic of China, Email [email protected]
Objective: In order to determine research hotspots and prospective directions, this work used VOSviewer and CiteSpace to assess the current state of insular epilepsy research.
Methods: We looked for pertinent research about insular epilepsy published between the first of January 2000 and the thirtieth of April 2022 in the Web of Science Core Collection (WoSCC) database. CiteSpace and VOSviewer were used to build a knowledge atlas by analyzing authors, institutions, countries, keywords with citation bursts, keyword clustering, keyword co-occurrence, publishing journals, reference co-citation patterns, and other factors.
Results: A total of 305 publications on insular epilepsy were found. Nguyen DK had the most articles published (37), whereas Mauguière F and Isnard J had the highest average number of citations/publications (39.37 and 38.09, respectively). The leading countries and institutions in this field were the United States (82 papers) and Université de Montréal (40 papers). Authors, countries, and institutions appear to be actively collaborating. Hot topics and research frontiers included surgical treatment, functional network connectivity, and the application of neuroimaging methods to study insular epilepsy.
Conclusion: In summary, the most influential articles, authors, journals, organizations, and countries on the subject of insular epilepsy were determined by this analysis. This study investigated the area of insular epilepsy research and forecasted upcoming trends using co-occurrence and evolution methods.
Keywords: visualization analysis, insular epilepsy, CiteSpace, VOSviewer, bibliometrics
Introduction
Penfield reported the first case of epilepsy treated by insular surgery in 1947,1 and researchers subsequently became aware of the relationship between the insula and epilepsy. Until the 1950s, Guillaume and Mazars first proposed the concept of insular epilepsy.2 Subsequently, more researchers devoted themselves to the research field of insular epilepsy. For instance, Blum et al discovered in 1961 that insular and circum-insular lesions might cause cats to have autonomic-psychic experimental epilepsy.3 Due to the complex and atypical symptoms of insular epilepsy, such that it can mimic temporal, frontal, or parietal lobe onset seizures, making its differential diagnosis very difficult.4,5 Given the anatomical position of the insula, it is difficult for ordinary scalp electroencephalography (EEG) to record insular discharge.
Furthermore, surgery for insular epilepsy is extremely difficult, making research on insular epilepsy difficult. In 1964, Silfvenius et al6 reported the presence of epileptogenic foci in the insula in patients undergoing temporal lobectomy. However, as the group with added insula resection failed to improve the incidence of postoperative epilepsy and showed an increased incidence of hemiplegia, research in insular epilepsy encountered a bottleneck. When Isnard et al first identified intracranial insular seizures in 2 cases with atypical temporal lobe epilepsy in 2000, there was some progress.7 Next, in 2004, Isnard et al8 used stereotaxic electroencephalography (SEEG) to record insular discharge with simultaneous electrical cortical stimulation and systematically summarized the symptoms of insular seizures. In recent years, with an increased understanding of the insular epilepsy network and the development of imaging technology, micro neurosurgery, and SEEG, research in insular epilepsy has progressed. As a result, it is vital to summarize and organize the research on insular epilepsy conducted over the last 20 years.
Using software for correlation analysis, bibliometrics is a quantitative approach for describing and analyzing the dynamics and development of a discipline or study area.9,10 To conduct bibliometric and visual analyses for this work, we employed the bibliometrics-related software programs CiteSpace and VOSviewer.11,12 Recent systematic and narrative reviews on insular epilepsy highlight the diagnostic methods and surgical treatments of insular epilepsy.4,5 Bibliometrics differs from traditional narrative reviews providing readers with the current status and trends of global research in a certain research field, such as research themes and research cooperation. As far as we are aware, there has been no bibliometric study of research on insular epilepsy reported until now. We performed a quantitative study and visualization of cooperative networks (authors, institutions, and countries), co-citation references, published journals, keyword citation bursts, keyword clustering, and keyword co-occurrence in insular epilepsy over the previous two decades. As a result, the current study examines the fundamental, frontier, and hot themes in insular epilepsy research systematically and unbiasedly.
Methods
Sources of Data and Searching Strategy
Data were obtained using powerful search techniques of the Web of Science Core Collection (WoSCC), an expanded version of the Science Citation Index, as illustrated in Figure 1. In the topic field, the following search keywords were entered: “insula epilepsy” OR “insular epilepsy” OR “insula seizures” OR “insular seizures” OR “insula seizure” OR “insular seizure”. The period covered was from the January 1,2000 to April 30, 2022; the only language allowed was English, and the only types of papers acceptable were reviews and original research articles. Following the lead of earlier studies,9 two independent researchers examined the abstracts and titles and the criteria for inclusion were any publications relevant to insular epilepsy. Finally, 305 papers were considered for the subsequent study.
 |
Figure 1 Depicts a flow diagram of the literature’s initial screening procedures. |
Data Analysis and Visualization
The bibliometric analysis and data visualization were carried out using VOSviewer 1.6.18 and CiteSpace 6.1.R2. First, we constructed a text file called download XXX.txt that contained all of the records we had obtained from WoSCC in plain text. After that, these data were uploaded into CiteSpace and VOSviewer software for bibliometric and visual analysis. Drawing visual maps from the analysis of countries, journals, co-authors, co-citation references, co-occurring keywords, and their clusters. CiteSpace tracks keywords with significant historical citation bursts and examine annual publication counts and growth trends to identify research fronts and upcoming trends.
Results
Bibliometric Analysis of Publication Years
Figure 2 displays 305 articles on insular epilepsy publication dates between January 2000 and April 2022. With minor oscillations, the proportion of publications on insular epilepsy has typically increased over time. Before 2008, less than 10 articles were published each year. Since 2009, the number of published papers has risen to more than 10 per year. Each year from 2017 through 2021, more than 20 papers were published. In 2019, 33 articles were published, making it the year with the most articles. Only 6 articles had been published that year as of April 30th, 2022.
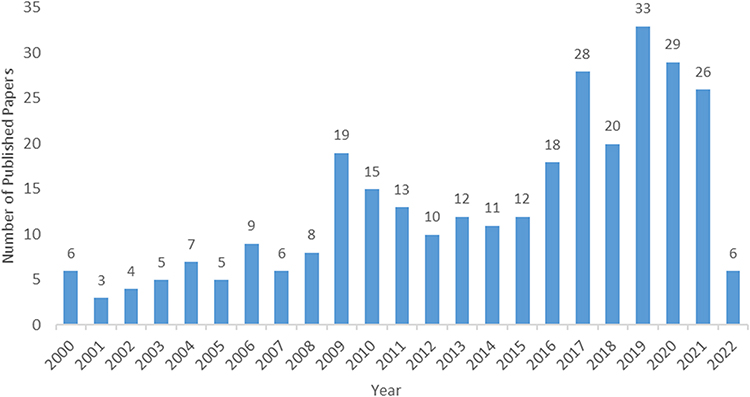 |
Figure 2 Shows the number of yearly publications changes from the first of January 2000 to the 30th of April 2022. |
Bibliometric Analysis of Journals
In this study, the publication volume of 81 journals was analyzed. First, journals with five or more publications in insular epilepsy research were visualized using VOSviewer (Figure 3). The journals with the most publications were then evaluated. Seven journals produced more than 10 publications annually, totalling 136 papers (44.6%). Journal of Neurosurgery (19, 6.2%), Epilepsy & Behavior (30, 9.8%), and Epilepsia (33, 10.8%) were the top three journals (Table 1).
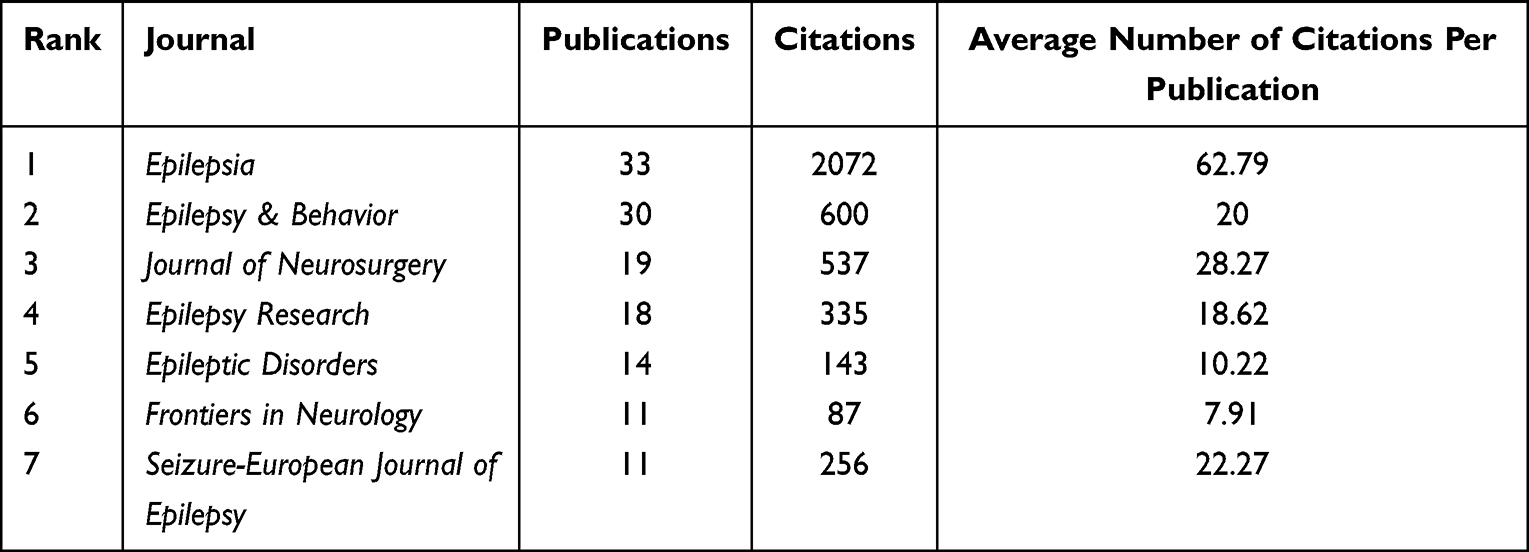 |
Table 1 List of the Journals Having More Than 10 Articles in the Field of Research on Insular Epilepsy |
 |
Figure 3 Visualization of the network for the published journals. The number of published papers increases with node size. The node connection lines show the strength of the connections between journals. The node’s colour shows how the number of articles published has changed over time. |
Countries and Institution Bibliometric Assessment
From the first of January 2000 to the thirtieth of April 2022, only 44 countries participated in insular epilepsy research. First, using VOSviewer, countries with three or more papers were shown (Figure 4). Table 2 provides the top five countries producing insular epilepsy research to further assess high-productivity countries. The USA, France, Canada, China, and Italy were the top 5 nations with articles published. 257 papers from these countries were published in total, making up 84.3% of all publications, the United States having the most (82, 26.9%) published articles. A total of 484 institutions were associated with the authors of the 305 papers. As shown in Table 2, the top five institutions with the most publications were Université de Montréal, Université Lyon 1, Hospital Civils Lyon, Capital Medical University, and Aix-Marseille University. These five institutions published 91 papers, accounting for 29.8% of all articles.The institution with the most publications was the Université de Montréal (40, 13.1%).
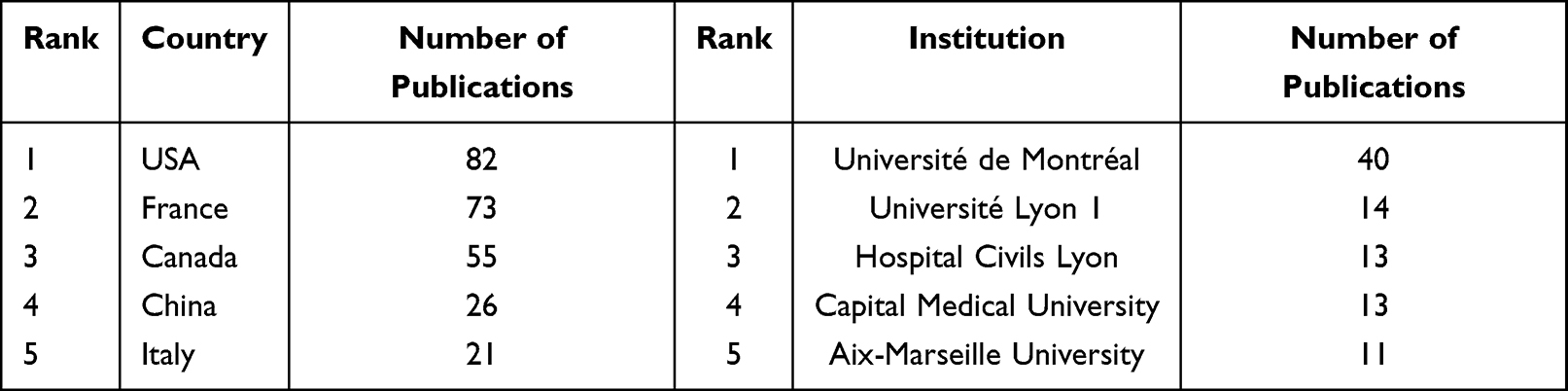 |
Table 2 Lists the Top 5 countries and Organizations Publishing Research on Insular Epilepsy |
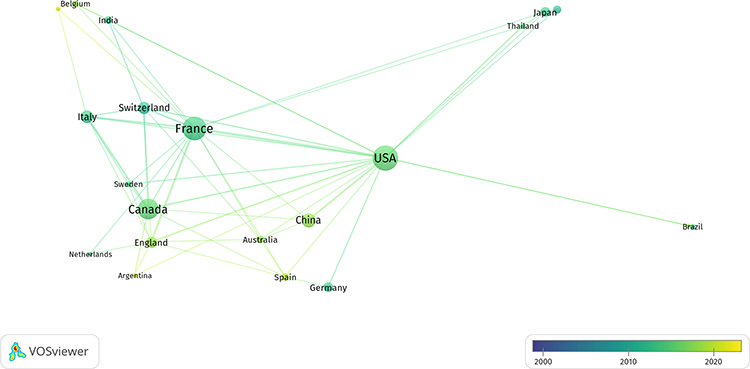 |
Figure 4 Network visualization of countries. The number of published studies increases with node size. The strength of the connections between nodes represents the relationships between countries. The node’s colour displays how the quantity of articles published over time has changed. |
Co-Authors’ Citations Analyses
We used VOSviewer to represent the authors with 5 or >5 publications. Figure 5 incorporates a time factor via overlay representation, with the colour gradient naturally expressing the active status of many researchers in recent times. The connecting lines indicate collaborations, the node colour denotes the time distribution (yearly average of published articles), and the node size shows the number of published papers. We compiled the researchers with more than 10 articles to learn which authors have significantly advanced the understanding of insular epilepsy research. Nguyen DK (37, 12.1%), Bouthillier A (30, 9.8%) and Boucher O (15, 4.9%) were the top 3 leading contributors by the number of publications (Table 3). From 2000 to 2022, the author with the most publications was Nguyen DK, with 37 publications. Bouthillier did not, however, have the highest average publication/citations. The top five researchers with the greatest average number of publications/citations were F. Mauguière, J. Isnard, L. Minotti, P. Kahane, and A. Bouthillier, indicating that these authors have a substantial academic impact in the field of research on insular epilepsy.
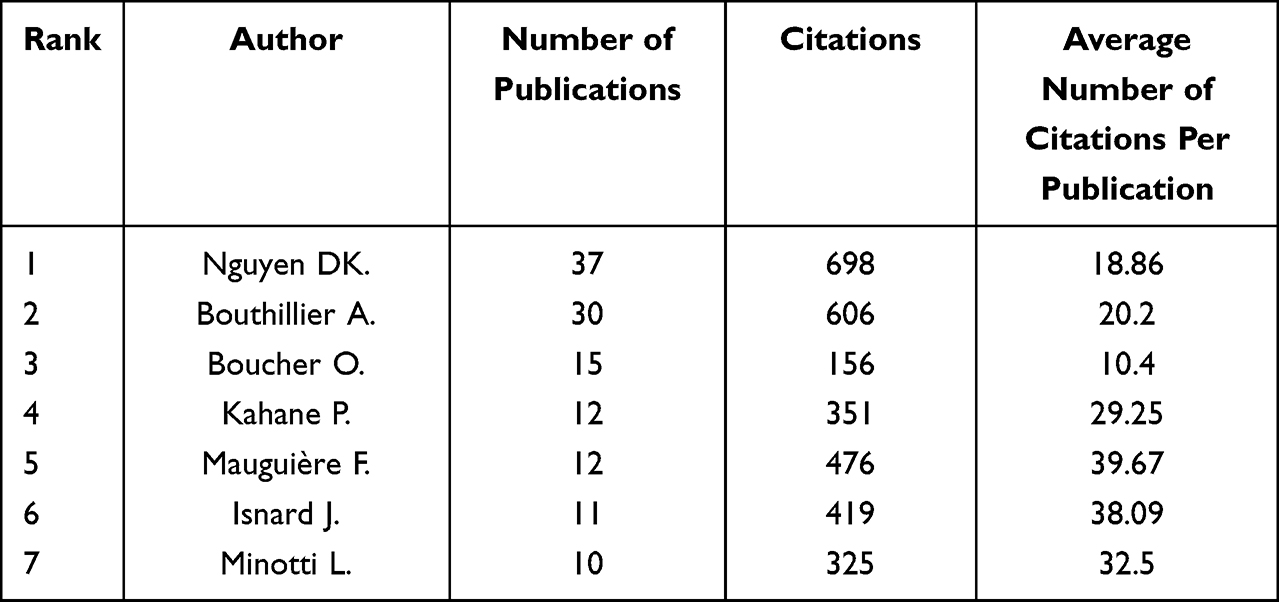 |
Table 3 The Most Influential Authors in the Field of Insular Epilepsy Research |
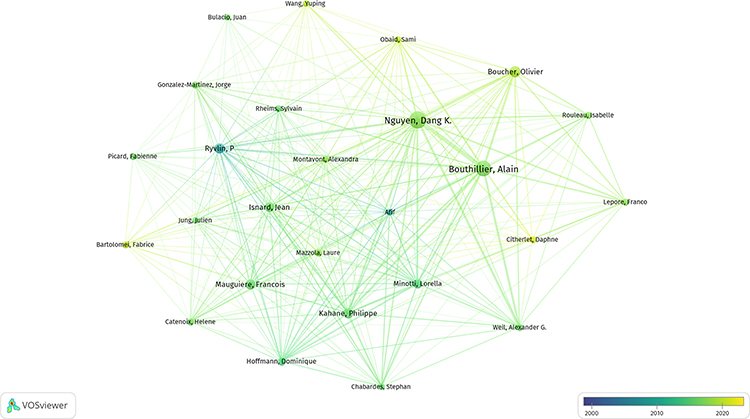 |
Figure 5 Network visualization of authors. The number of papers published increases with node size. The node connecting lines show the depth of the relationship between authors. The node’s colour shows how the number of articles published has changed over time. |
Co-Cited References Bibliometric Evaluation
To visualize the 7087 cited references, we used VOSviewer selecting the minimum number of citations to 15, a total of 68 references were used for the co-citation analysis of cited references (Figure 6). 1,5–8,13–39 The top 10 references are listed in Table 4.1,6–8,13–18 Isnard J. (2004; 127 times), Isnard J. (2000; 105 times), and Nguyen DK (2009; 81 times) were the top three co-cited references.
 |
Table 4 Shows the Top Ten Co-Cited References in the Field of Insular Epilepsy Research |
 |
Figure 6 Network visualization of co-cited references. The larger the node, the more citations. The node connecting lines show the association potency of various references referenced in the same article. The node colours represent different categories. |
Co-Occurring Keywords and Clusters Bibliometric Assessment
VOSviewer was used to draw a keyword co-occurrence network view of the 305 documents. For visualization, we chose 63 important keywords with a frequency of at least 10 (Figure 7). The top 10 co-cited keywords were insula (frequency: 128), epilepsy (frequency: 120), temporal lobe epilepsy (frequency: 83), cortex (frequency: 82), seizures (frequency: 76), surgery (frequency: 69), epilepsy surgery (frequency: 63), insular cortex (frequency: 34), surgical treatment (frequency: 31), and insular epilepsy (frequency: 30).
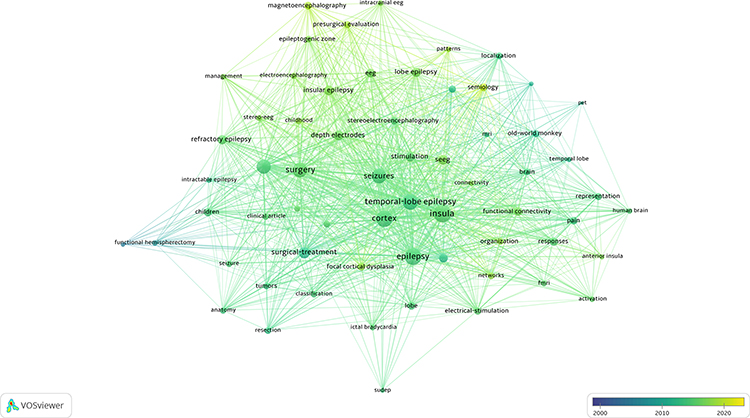 |
Figure 7 Network visualization of co-occurring keywords. The larger the circle node, the more frequent of an occurrence. The intensity of the association between the frequency of occurrence of several keywords in the same article is shown by the node connecting lines. The node’s colour displays how the frequency of occurrence has changed over time. |
We utilized CiteSpace to do cluster analysis of co-occurring keywords again to uncover topic groupings of co-occurring keywords. Nine clusters were discovered, with every cluster having an silhouette value of more than 0.7, indicating that the findings are consistent (Figure 8 and Table 5). We used CiteSpace to illustrate the co-clustering timeline view to better understand how these clusters evolved (Figure 9).
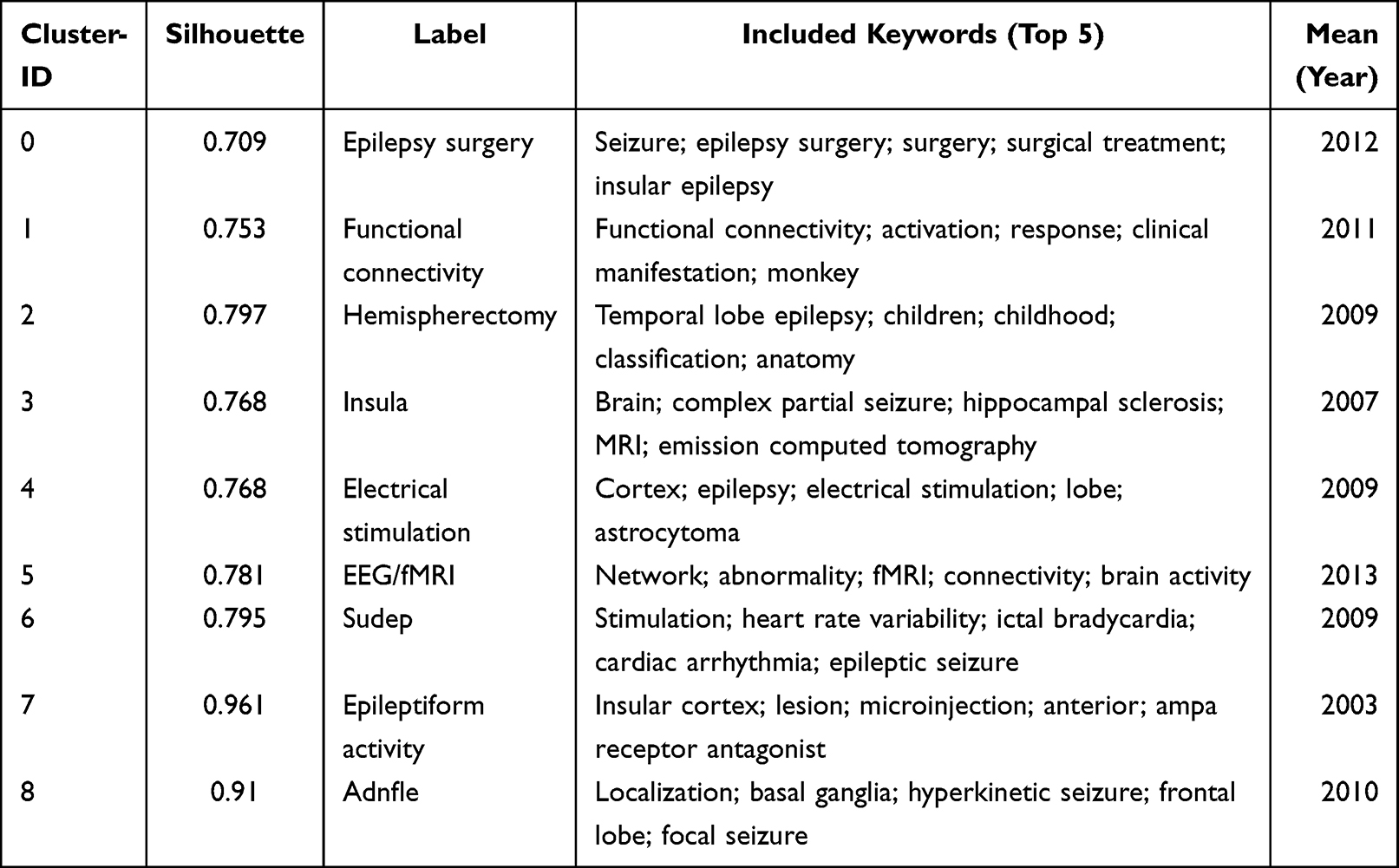 |
Table 5 Keyword Cluster Analysis in the Field of Insular Epilepsy Research |
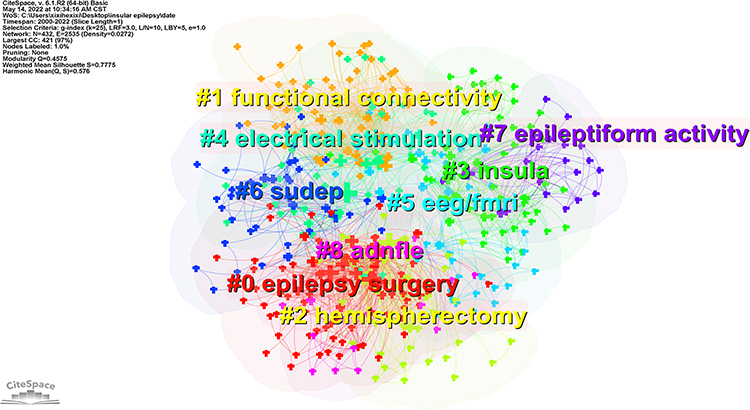 |
Figure 8 Visualization of the keywords cluster analysis. |
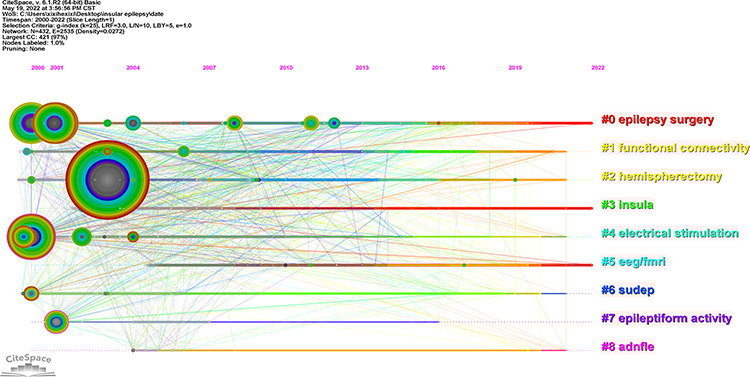 |
Figure 9 Shows a timeline picture of co-clustering from 2000 to 2022. The node’s size and colour represent the overall number of references and specific time slices. Two articles are co-cited in one article and are shown by different coloured lines. The clustering subjects for hot and non-hot topics over time. |
Keyword Bibliometric Analysis Using Citation Bursts
Then, we used CiteSpace to visualize the top 10 keywords with the most powerful citation bursts (Figure 10). The figure shows a blue line for the time interval and a red line for the time frame during which the keyword bursts were discovered. The four most recent citation burst keywords occurred in 2017 (insular epilepsy), 2018 (surgery), 2019 (organization, network), and 2020 (lobe epilepsy) and have all lasted until 2022.
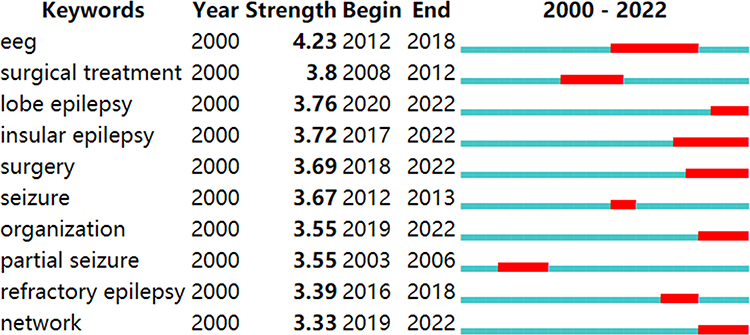 |
Figure 10 Shows the top ten terms (keywords) with the most citation bursts. Blue line for the time interval and red line for the time frame during which the keyword bursts were discovered. The bold text refers to the start and end time and intensity of the keywords burst. |
Discussion
General Information
This is the very first study to examine the topic of insular epilepsy research using CiteSpace and VOSviewer to identify research hotspots and breakthroughs. Although the concept of insular epilepsy has existed for nearly 70 years, breakthroughs were not achieved until Isnard et al7 first recorded insular seizures in 2000. Therefore, we searched WoSCC for articles published from January 2000 to the thirtieth of April 2022. Based on the inclusion criteria, a total of 305 articles were obtained. These 305 articles came from 1409 authors from 484 institutions in 44 countries, were published in 81 journals, and cited 7087 articles from 1172 journals. In general, but with significant oscillations, the number of publications in insular epilepsy studies has grown during the previous two decades. Since 2017, the number of published papers has exceeded 20 per year, which indicates that insular epilepsy is receiving more and more attention from scholars and becoming a new focus in epilepsy research.
Network
Journal Network
Even though an analysis of the published journals cannot describe the current status of insular epilepsy research nor anticipate future research trends, these journals play a crucial role in insular epilepsy research. Thus, these journals are appropriate for creating a theoretical basis and publishing high-quality articles. In our study, 305 articles were published in 81 journals. Further analysis and statistics of the journals revealed that most insular epilepsy research was published in journals belonging to the field of epilepsy and neurosurgery, followed by a small number of comprehensive journals. Most publications were published in Epilepsia Journal, with the highest average amount of citations per article. The analysis of papers recently published in this journal revealed topics related to diagnoses, such as the use of magnetoencephalography to assist diagnosis40 and treatment, including surgical treatment4,41 and stereotactic thermocoagulation.42
Country and Institution Network
This study examined publishing volumes from 44 different countries and 484 different institutions. In our study, the number of articles in the top five countries and institutions reached 84.3% and 29.8% respectively. These findings show that the top effect is highly significant, most articles are produced by academics from a small number of countries and institutions, and the distribution of countries and institutions producing papers on this subject is relatively uneven.
Author Network
The key research forces and representative academics in insular epilepsy research can be found through the author’s cooperation network analysis. Our results also show that the top five authors have a clear cooperative relationship with each other. The two authors with the highest average citations/publication, namely Mauguière F and Isnard J, published breakthrough articles in 2000 and 2004.7,8 Recent collaborative articles by these two authors mainly focus on electrical stimulation for insular epilepsy or refractory epilepsy43,44 and the analysis of clinical manifestations of insular epilepsy.45
Co-Cited References Network
Analysis of the cooperative network of co-cited references can reveal the basis of an existing research field. Isnard J. (2004; 127 times), Isnard J. (2000; 105 times), and Nguyen DK (2009; 81 times) were the top three co-cited references. As noted above, the two articles by Isnard J et al in 2000 and 2004 were breakthroughs. Nguyen DK’s 2009 article clarified the complexity and diversity of clinical manifestations of insular epilepsy.13
Research Frontiers and Hot Topics in Insular Epilepsy
Keywords reveal the essential nature of an article. In bibliometric analysis, terms with a high frequency are utilized to discover research hotspots and frontiers. Through keyword clustering analysis, keyword co-occurrence analysis, and a keyword clustering timeline map that illustrates changes in research hotspots and keywords with citation bursts, we investigated the hotspots and frontiers of insular epilepsy research in this article. Our findings suggest that clusters 0, “epilepsy surgery”, 1, “functional connectivity”, and 5, “EEG/fMRI”, maybe hot issues and possibilities in insular epilepsy research.
Epilepsy Surgery
Surgery for insular epilepsy is difficult because the insula is situated in the deep part of the Sylvian fissure and interacts with the surrounding brain regions, blood arteries, and other structures.46,47 As a result, surgical treatment of insular epilepsy has always been a hot topic and frontier in insular epilepsy research. When insular epilepsy was first proposed, insular cortectomy was applied. However, this surgical method did not improve outcomes and had high complications due to technical limitations, causing it to be gradually abandoned.2,6
The development of novel surgical techniques, electrophysiological monitoring, and navigation tools over recent decades has greatly improved the outcomes after insular corticectomy.18,48 It is believed that partial or complete resection of the insula can improve the prognosis of insular epilepsy.18,49 For patients with magnetic resonance imaging (MRI)-negative insular epilepsy, precise monitoring and implantation of invasive EEG — especially SEEG — are needed to explore the epilepsy-causing network so that the epilepsy area can be resected in a targeted manner.50–52
Alternative surgical modalities for insular resection include SEEG-guided radiofrequency thermocoagulation (RFT),42,53–55 MRI-guided laser ablation (laser interstitial thermal therapy (LITT)),56–58 gamma knife radiosurgery,54,59 and responsive neurostimulation.60 Interestingly, when we collated the data, we found that although scholars have continued to research traditional craniotomy insular cortextomy, such as bipolar electro-coagulation with cortextomy,61 more scholars are focusing on minimally invasive procedures, especially LITT.62–66
Functional Connectivity
It is well known that seizures can disturb brain networks and lead to connectivity disturbances.67 As the insula has various functions and forms extensive functional network connections with almost all other brain regions, the manifestations of insular epilepsy are complex and diverse and may even mimic other focal epilepsies. Some scholars have recently begun to study complex networks of functional connectivity in insular epilepsy, and this topic has gradually become a frontier of insular epilepsy research. By analyzing interictal high-frequency oscillations (HFOs) using magnetoencephalography (MEG), Yin et al68 found that patients with insular epilepsy showed alterations in the insula-based connectivity network. They also reported that alterations in this network might be responsible for interictal brain dysfunction in patients with insular epilepsy. Rachidi et al69 recently summarized the application of direct cortical stimulation (DCS) to the insula, mapping the functional network connections of the insula to help understand where insular seizures start and how they propagate. Zhao et al70 showed that insular epilepsy could broadly disrupt the brain metabolic network using fluorine-18-fluorodeoxyglucose positron emission tomography (18F-FDG-PET) imaging. Additional MatLab tools have been developed to study and analyze functional connectivity networks in insular epilepsy.71
EEG/fMRI
Given the anatomical position of the insula, general EEG and MRI cannot be used to effectively study insular epilepsy. In parallel with the development of EEG and MRI technology, especially SEEG and functional MRI (fMRI), research on insular epilepsy has made breakthroughs. Recently, Peltola et al52 used SEEG to analyze the different symptoms of anterior and posterior insular seizures, thereby helping determine the actual onset zone of insular seizures. Insular epilepsy can be further subdivided into insulo-opercular epilepsy, opercular epilepsy, and insular cortex epilepsy, as shown using SEEG combined with PET.51 As a non-invasive neuroimaging method, fMRI plays a crucial role in the study of insular epilepsy. Recently, some scholars have used fMRI to find structural connectivity changes in insular epilepsy.72 Due to the complexity of insular epilepsy, it is often necessary to combine EEG/SEEG, fMRI, MEG, etc., in practical applications.54,73 Given continuous development in auxiliary examination technology, EEG/fMRI has always been a hot topic and frontier in insular epilepsy research.
Limitations
There are several limitations to this study. First, data were gathered from a single database. Although WoS encompass various journals, it is impossible to include all journals containing insular epilepsy research. Thus, our analysis of data may not be comprehensive enough. Second, our search terms may not be perfect enough to retrieve all publications in the research field.And also only two article types and English language articles were included in our study, which, to some extent, makes the analysis incomplete. Finally, while bibliometric analysis employing professional software is objective, various authors’ perspectives and assessments of the same content may differ, possibly resulting in human errors.
Conclusion
The understanding of insular epilepsy is still lacking, and it is a very complex problem for clinical and basic study. Through bibliometric analysis, this study tracked the advancement of insular epilepsy research from 2000 to 2022. We selected significant publications, authors, journals, and nations using 305 papers we downloaded from WoS and further examined the research network. According to our findings, we selected minimally invasive surgery, functional connectivity, and MEG, SEEG, and fMRI applications as hot issues and prospects in insular epilepsy exploration.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Key specialized research and development breakthrough program in Henan province (202102310081).
Disclosure
The authors report no competing interests.
References
1. Penfield W. Some observations on the cerebral cortex of man. Proc R Soc Lond B Biol Sci. 1947;134(876):329–347. doi:10.1098/rspb.1947.0017
2. Guillaume J, Mazars G, Mazars Y. [Surgical indications in the so-called temporal epilepsy]. Bull Med. 1953;67(17):387–388. French
3. Blum B, Liban E. Autonomic-psychic experimental epilepsy in the cat due to insular and circum-insular lesions. Epilepsia. 1961;2:243–250. doi:10.1111/j.1528-1167.1961.tb06235.x
4. Laoprasert P, Ojemann JG, Handler MH. Insular epilepsy surgery. Epilepsia. 2017;58(Suppl 1):35–45. doi:10.1111/epi.13682
5. Obaid S, Zerouali Y, Nguyen DK. Insular epilepsy: semiology and noninvasive investigations. J Clin Neurophysiol. 2017;34(4):315–323. doi:10.1097/WNP.0000000000000396
6. Silfvenius H, Gloor P, Rasmussen T. Evaluation of insular ablation in surgical treatment of temporal lobe epilepsy. Epilepsia. 1964;5:307–320. doi:10.1111/j.1528-1157.1964.tb03338.x
7. Isnard J, Guenot M, Ostrowsky K, Sindou M, Mauguiere F. The role of the insular cortex in temporal lobe epilepsy. Ann Neurol. 2000;48(4):614–623. doi:10.1002/1531-8249(200010)48:4<614::AID-ANA8>3.0.CO;2-S
8. Isnard J, Guenot M, Sindou M, Mauguiere F. Clinical manifestations of insular lobe seizures: a stereo-electroencephalographic study. Epilepsia. 2004;45(9):1079–1090. doi:10.1111/j.0013-9580.2004.68903.x
9. Guo Y, Xu ZY, Cai MT, Gong WX, Shen CH. Epilepsy with suicide: a bibliometrics study and visualization analysis via CiteSpace. Front Neurol. 2021;12:823474. doi:10.3389/fneur.2021.823474
10. Zhan J, Ma Y, Zhao D, et al. Knowledge atlas of post-traumatic epilepsy research: based on citespace visualization analysis. Epilepsy Res. 2021;178:106790. doi:10.1016/j.eplepsyres.2021.106790
11. van Eck NJ, Waltman L. Software survey: vOSviewer, a computer program for bibliometric mapping. Scientometrics. 2010;84(2):523–538. doi:10.1007/s11192-009-0146-3
12. Chen C. Searching for intellectual turning points: progressive knowledge domain visualization. Proc Natl Acad Sci U S A. 2004;101(Suppl 1):5303–5310. doi:10.1073/pnas.0307513100
13. Nguyen DK, Nguyen DB, Malak R, et al. Revisiting the role of the insula in refractory partial epilepsy. Epilepsia. 2009;50(3):510–520. doi:10.1111/j.1528-1167.2008.01758.x
14. Ryvlin P, Minotti L, Demarquay G, et al. Nocturnal hypermotor seizures, suggesting frontal lobe epilepsy, can originate in the insula. Epilepsia. 2006;47(4):755–765. doi:10.1111/j.1528-1167.2006.00510.x
15. Augustine JR. Circuitry and functional aspects of the insular lobe in primates including humans. Brain Res Brain Res Rev. 1996;22(3):229–244. doi:10.1016/s0165-0173(96)00011-2
16. Ostrowsky K, Isnard J, Ryvlin P, Guenot M, Fischer C, Mauguiere F. Functional mapping of the insular cortex: clinical implication in temporal lobe epilepsy. Epilepsia. 2000;41(6):681–686. doi:10.1111/j.1528-1157.2000.tb00228.x
17. von Lehe M, Wellmer J, Urbach H, Schramm J, Elger CE, Clusmann H. Insular lesionectomy for refractory epilepsy: management and outcome. Brain. 2009;132(Pt 4):1048–1056. doi:10.1093/brain/awp047
18. Malak R, Bouthillier A, Carmant L, et al. Microsurgery of epileptic foci in the insular region. J Neurosurg. 2009;110(6):1153–1163. doi:10.3171/2009.1.JNS08807
19. Gras-Combe G, Minotti L, Hoffmann D, Krainik A, Kahane P, Chabardes S. Surgery for nontumoral insular epilepsy explored by stereoelectroencephalography. Neurosurgery. 2016;79(4):578–588. doi:10.1227/NEU.0000000000001257
20. Weil AG, Le NM, Jayakar P, et al. Medically resistant pediatric insular-opercular/perisylvian epilepsy. Part 2: outcome following resective surgery. J Neurosurg Pediatr. 2016;18(5):523–535. doi:10.3171/2016.4.PEDS15618
21. Proserpio P, Cossu M, Francione S, et al. Insular-opercular seizures manifesting with sleep-related paroxysmal motor behaviors: a stereo-EEG study. Epilepsia. 2011;52(10):1781–1791. doi:10.1111/j.1528-1167.2011.03254.x
22. Pugnaghi M, Meletti S, Castana L, et al. Features of somatosensory manifestations induced by intracranial electrical stimulations of the human insula. Clin Neurophysiol. 2011;122(10):2049–2058. doi:10.1016/j.clinph.2011.03.013
23. Stephani C, Fernandez-Baca VG, Maciunas R, Koubeissi M, Luders HO. Functional neuroanatomy of the insular lobe. Brain Struct Funct. 2011;216(2):137–149. doi:10.1007/s00429-010-0296-3
24. Surbeck W, Bouthillier A, Weil AG, et al. The combination of subdural and depth electrodes for intracranial EEG investigation of suspected insular (perisylvian) epilepsy. Epilepsia. 2011;52(3):458–466. doi:10.1111/j.1528-1167.2010.02910.x
25. Afif A, Minotti L, Kahane P, Hoffmann D. Anatomofunctional organization of the insular cortex: a study using intracerebral electrical stimulation in epileptic patients. Epilepsia. 2010;51(11):2305–2315. doi:10.1111/j.1528-1167.2010.02755.x
26. Kurth F, Zilles K, Fox PT, Laird AR, Eickhoff SB. A link between the systems: functional differentiation and integration within the human insula revealed by meta-analysis. Brain Struct Funct. 2010;214(5–6):519–534. doi:10.1007/s00429-010-0255-z
27. Craig AD. How do you feel--now? The anterior insula and human awareness. Nat Rev Neurosci. 2009;10(1):59–70. doi:10.1038/nrn2555
28. Afif A, Chabardes S, Minotti L, Kahane P, Hoffmann D. Safety and usefulness of insular depth electrodes implanted via an oblique approach in patients with epilepsy. Neurosurgery. 2008;62(5Suppl 2):479–480. doi:10.1227/01.neu.0000326037.62337.80
29. Dobesberger J, Ortler M, Unterberger I, et al. Successful surgical treatment of insular epilepsy with nocturnal hypermotor seizures. Epilepsia. 2008;49(1):159–162. doi:10.1111/j.1528-1167.2007.01426.x
30. Kahane P, Landre E, Minotti L, Francione S, Ryvlin P. The Bancaud and Talairach view on the epileptogenic zone: a working hypothesis. Epileptic Disord. 2006;8(Suppl 2):S16–26.
31. Duffau H, Capelle L, Lopes M, Bitar A, Sichez JP, van Effenterre R. Medically intractable epilepsy from insular low-grade gliomas: improvement after an extended lesionectomy. Acta Neurochir. 2002;144(6):563–72;discussion 572–3. doi:10.1007/s00701-002-0941-6
32. Ostrowsky K, Magnin M, Ryvlin P, Isnard J, Guenot M, Mauguiere F. Representation of pain and somatic sensation in the human insula: a study of responses to direct electrical cortical stimulation. Cereb Cortex. 2002;12(4):376–385. doi:10.1093/cercor/12.4.376
33. Duffau H, Capelle L, Lopes M, Faillot T, Sichez JP, Fohanno D. The insular lobe: physiopathological and surgical considerations. Neurosurgery. 2000;47(4):801–10;discussion 810–1. doi:10.1097/00006123-200010000-00001
34. Cukiert A, Forster C, Andrioli MS, Frayman L. Insular epilepsy. Similarities to temporal lobe epilepsy. Case report. Arq Neuropsiquiatr. 1998;56(1):126–128. doi:10.1590/s0004-282x1998000100022
35. Roper SN, Levesque MF, Sutherling WW, Engel JJ. Surgical treatment of partial epilepsy arising from the insular cortex. Report of two cases. J Neurosurg. 1993;79(2):266–269. doi:10.3171/jns.1993.79.2.0266
36. Oppenheimer SM, Gelb A, Girvin JP, Hachinski VC. Cardiovascular effects of human insular cortex stimulation. Neurology. 1992;42(9):1727–1732. doi:10.1212/wnl.42.9.1727
37. Yasargil MG, von Ammon K, Cavazos E, Doczi T, Reeves JD, Roth P. Tumours of the limbic and paralimbic systems. Acta Neurochir. 1992;118(1–2):40–52. doi:10.1007/BF01400725
38. Hanbery J, Jasper H. The non-specific thalamocortical projection system. J Neurosurg. 1954;11(1):24–25. doi:10.3171/jns.1954.11.1.0024
39. Dylgjeri S, Taussig D, Chipaux M, et al. Insular and insulo-opercular epilepsy in childhood: an SEEG study. Seizure. 2014;23(4):300–308. doi:10.1016/j.seizure.2014.01.008
40. Mohamed IS, Gibbs SA, Robert M, Bouthillier A, Leroux JM, Khoa ND. The utility of magnetoencephalography in the presurgical evaluation of refractory insular epilepsy. Epilepsia. 2013;54(11):1950–1959. doi:10.1111/epi.12376
41. Freri E, Matricardi S, Gozzo F, Cossu M, Granata T, Tassi L. Perisylvian, including insular, childhood epilepsy: presurgical workup and surgical outcome. Epilepsia. 2017;58(8):1360–1369. doi:10.1111/epi.13816
42. Mullatti N, Landre E, Mellerio C, et al. Stereotactic thermocoagulation for insular epilepsy: lessons from successes and failures. Epilepsia. 2019;60(8):1565–1579. doi:10.1111/epi.16092
43. Mazzola L, Mauguiere F, Isnard J. Functional mapping of the human insula: data from electrical stimulations. Rev Neurol (Paris). 2019;175(3):150–156. doi:10.1016/j.neurol.2018.12.003
44. Mazzola L, Royet JP, Catenoix H, Montavont A, Isnard J, Mauguiere F. Gustatory and olfactory responses to stimulation of the human insula. Ann Neurol. 2017;82(3):360–370. doi:10.1002/ana.25010
45. Hagiwara K, Jung J, Bouet R, et al. How can we explain the frontal presentation of insular lobe epilepsy? The impact of non-linear analysis of insular seizures. Clin Neurophysiol. 2017;128(5):780–791. doi:10.1016/j.clinph.2017.01.022
46. Nieuwenhuys R. The insular cortex: a review. Prog Brain Res. 2012;195:123–163. doi:10.1016/B978-0-444-53860-4.00007-6
47. Uddin LQ, Nomi JS, Hebert-Seropian B, Ghaziri J, Boucher O. Structure and function of the human insula. J Clin Neurophysiol. 2017;34(4):300–306. doi:10.1097/WNP.0000000000000377
48. von Lehe M, Parpaley Y. Insular cortex surgery for the treatment of refractory epilepsy. J Clin Neurophysiol. 2017;34(4):333–339. doi:10.1097/WNP.0000000000000393
49. Boucher O, Rouleau I, Escudier F, et al. Neuropsychological performance before and after partial or complete insulectomy in patients with epilepsy. Epilepsy Behav. 2015;43:53–60. doi:10.1016/j.yebeh.2014.11.016
50. Park YS, Lee YH, Shim KW, et al. Insular epilepsy surgery under neuronavigation guidance using depth electrode. Childs Nerv Syst. 2009;25(5):591–597. doi:10.1007/s00381-008-0764-8
51. Wang X, Hu W, Mcgonigal A, et al. Electroclinical features of insulo-opercular epilepsy: an SEEG and PET study. Ann Clin Transl Neurol. 2019;6(7):1165–1177. doi:10.1002/acn3.789
52. Peltola ME, Trébuchon A, Lagarde S, et al. Anatomoelectroclinical features of SEEG-confirmed pure insular-onset epilepsy. Epilepsy Behav. 2020;105:106964. doi:10.1016/j.yebeh.2020.106964
53. Ma K, Luan G, Wang X, et al. Magnetoencephalography STOUT method adapted to radiofrequency thermocoagulation for mr-negative insular epilepsy: a case report. Front Neurol. 2021;12:683299. doi:10.3389/fneur.2021.683299
54. Ryvlin P, Nguyen DK. Insular seizures and epilepsies: ictal semiology and minimal invasive surgery. Curr Opin Neurol. 2021;34(2):153–165. doi:10.1097/WCO.0000000000000907
55. Catenoix H, Isnard J, Guenot M, Petit J, Remy C, Mauguiere F. The role of the anterior insular cortex in ictal vomiting: a stereotactic electroencephalography study. Epilepsy Behav. 2008;13(3):560–563. doi:10.1016/j.yebeh.2008.06.019
56. Ryvlin P, Picard F. Invasive investigation of insular cortex epilepsy. J Clin Neurophysiol. 2017;34(4):328–332. doi:10.1097/WNP.0000000000000395
57. Alexander H, Cobourn K, Fayed I, Oluigbo CO. Magnetic resonance-guided laser interstitial thermal therapy for the treatment of nonlesional insular epilepsy in pediatric patients: technical considerations. Pediatr Neurosurg. 2020;55(3):155–162. doi:10.1159/000509006
58. Gireesh ED, Lee K, Skinner H, et al. Intracranial EEG and laser interstitial thermal therapy in MRI-negative insular and/or cingulate epilepsy: case series. J Neurosurg. 2020:1–9. doi:10.3171/2020.7.JNS201912
59. Irislimane M, Mathieu D, Bouthillier A, Deacon C, Nguyen DK. Gamma knife surgery for refractory insular cortex epilepsy. Stereotact Funct Neurosurg. 2013;91(3):170–176. doi:10.1159/000343205
60. Chen H, Dugan P, Chong DJ, Liu A, Doyle W, Friedman D. Application of RNS in refractory epilepsy: targeting insula. Epilepsia Open. 2017;2(3):345–349. doi:10.1002/epi4.12061
61. Ding H, Zhou J, Guan Y, et al. Bipolar electro-coagulation with cortextomy in the treatment of insular and insulo-opercular epilepsy explored by stereoelectro-encephalography. Epilepsy Res. 2018;145:18–26. doi:10.1016/j.eplepsyres.2018.05.007
62. Consales A, Cognolato E, Pacetti M, et al. Magnetic Resonance-Guided Laser Interstitial Thermal Therapy (MR-gLiTT) in Pediatric Epilepsy Surgery: state of the Art and Presentation of Giannina Gaslini Children’s Hospital (Genoa, Italy) Series. Front Neurol. 2021;12:739034. doi:10.3389/fneur.2021.739034
63. Alexander H, Cobourn K, Fayed I, et al. Magnetic resonance-guided laser interstitial thermal therapy for the treatment of non-lesional insular epilepsy in pediatric patients: thermal dynamic and volumetric factors influencing seizure outcomes. Childs Nerv Syst. 2019;35(3):453–461. doi:10.1007/s00381-019-04051-0
64. Hawasli AH, Bandt SK, Hogan RE, Werner N, Leuthardt EC. Laser ablation as treatment strategy for medically refractory dominant insular epilepsy: therapeutic and functional considerations. Stereotact Funct Neurosurg. 2014;92(6):397–404. doi:10.1159/000366001
65. Perry MS, Donahue DJ, Malik SI, et al. Magnetic resonance imaging-guided laser interstitial thermal therapy as treatment for intractable insular epilepsy in children. J Neurosurg Pediatr. 2017;20(6):575–582. doi:10.3171/2017.6.PEDS17158
66. Hale AT, Sen S, Haider AS, et al. Open resection versus laser interstitial thermal therapy for the treatment of pediatric insular epilepsy. Neurosurgery. 2019;85(4):E730–E736. doi:10.1093/neuros/nyz094
67. Englot DJ, D’Haese PF, Konrad PE, et al. Functional connectivity disturbances of the ascending reticular activating system in temporal lobe epilepsy. J Neurol Neurosurg Psychiatry. 2017;88(11):925–932. doi:10.1136/jnnp-2017-315732
68. Yin C, Zhang X, Xiang J, et al. Altered effective connectivity network in patients with insular epilepsy: a high-frequency oscillations magnetoencephalography study. Clin Neurophysiol. 2020;131(2):377–384. doi:10.1016/j.clinph.2019.11.021
69. Rachidi I, Minotti L, Martin G, et al. The insula: a stimulating Island of the brain. Brain Sci. 2021;11:11. doi:10.3390/brainsci11111533
70. Zhao B, Seguin C, Ai L, et al. Aberrant metabolic patterns networks in insular epilepsy. Front Neurol. 2020;11:605256. doi:10.3389/fneur.2020.605256
71. Sun K, Wang H, Bai Y, Zhou W, Wang L. MRIES: a matlab toolbox for mapping the responses to intracranial electrical stimulation. Front Neurosci. 2021;15:652841. doi:10.3389/fnins.2021.652841
72. Obaid S, Rheault F, Edde M, et al. Structural Connectivity Alterations in Operculo-Insular Epilepsy. Brain Sci. 2021;11:8. doi:10.3390/brainsci11081041
73. Chourasia N, Quach M, Gavvala J. Insular magnetoencephalography dipole clusters in patients with refractory focal epilepsy. J Clin Neurophysiol. 2021;38(6):542–546. doi:10.1097/WNP.0000000000000718
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.