Back to Journals » Advances in Medical Education and Practice » Volume 13
Knowledge and Competence Towards Critical Care Concepts Among Final Year Medical Students and Interns: A Cross-Sectional Study
Authors Dairi MS ![]() , Aljabri MK
, Aljabri MK ![]() , Bahakim AK
, Bahakim AK ![]() , Aljabri AA
, Aljabri AA ![]() , Alharbi TA, Alsehli AH
, Alharbi TA, Alsehli AH ![]() , Alotaibi AT
, Alotaibi AT ![]() , Alsufyani AA
, Alsufyani AA ![]() , Alsairafi RA
, Alsairafi RA ![]()
Received 24 April 2022
Accepted for publication 9 September 2022
Published 19 September 2022 Volume 2022:13 Pages 1091—1101
DOI https://doi.org/10.2147/AMEP.S372119
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Mohammad S Dairi,1 Moayad K Aljabri,2 Abdullah K Bahakim,2 Abdulkarim A Aljabri,2 Tayil A Alharbi,2 Anas H Alsehli,2 Alwaleed T Alotaibi,2 Abdulelah A Alsufyani,2 Rani A Alsairafi3
1Department of Internal Medicine, College of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia; 2Department of Medicine and Surgery, Umm Al-Qura University, Makkah, Saudi Arabia; 3Department of Surgery, Umm Al-Qura University, Makkah, Saudi Arabia
Correspondence: Mohammad S Dairi, Assistant Professor of Internal Medicine, Department of Internal Medicine, College of Medicine, Umm Al-Qura University, Makkah, Saudi Arabia, Tel +966555501560, Email [email protected]
Purpose: Critical care knowledge constitutes an essential component in medicine. Unfortunately, ICU knowledge acquisition is limited in many medical schools. This study is intended to measure the knowledge background, gaps, and the confidence toward critical care concepts among final year medical students and interns at Umm Al-Qura University, Saudi Arabia.
Methods: This was a cross-sectional study using a self-administered online questionnaire completed by final-year medical students and interns during January and February 2022. We collected data on demographics, academic year, critical care knowledge, competency, and satisfaction.
Results: Two-hundred-twenty-one (221) responses were analyzed. The male gender was 54.3%. A small proportion (15.8%) identified the lowest acceptable oxygen saturation in a normal person. Around three-quarters of the participants did not feel competent about nasal airway suctioning and endotracheal tube suctioning (65.6% and 75.6%, respectively). Only 7.2% of the responder correctly identified the three most useful physiological observations pertinent to quick SOFA criteria. Regarding the training adequacy for identifying critically ill patients, 59.3% answered that they are inadequately trained. Regarding the satisfaction level of exposure to critical care, 54% of the sample responded that they need further improvement.
Conclusion: Undergraduate students and interns have limited knowledge and confidence in critical care medicine. Thus, we highly recommend an early institution of a dedicated critical care training module in the medical school curriculum.
Keywords: intensive care unit, critically ill patient, curriculum, undergraduate medical students
Introduction
Critical care includes the knowledge, skills, attitudes, and problem-solving abilities needed for the perception and early management of patients with life-threatening conditions.1 Deficiencies in acute and emergency care knowledge are common, especially among junior doctors transitioning from undergraduate to postgraduate training.2,3 A significant percentage of hospital adverse events have been associated with less experienced physicians.4
Lack of adequate exposure to critically ill patients in undergraduate clinical rotations may lead to failure to recognize serious signs and symptoms and subsequent adverse patient-related outcomes.2
Early introduction to critical care teaching can improve undergraduate students’ knowledge base, confidence, and capability in their postgraduate training.2,5–9 Graduates should be well-prepared to understand the fundamental knowledge and concepts needed to manage critical conditions.10,11
Nevertheless, there is no universal curriculum for undergraduate critical care medicine.12 Several studies have been conducted worldwide among undergraduate medical students and junior physicians to assess their knowledge and confidence in critical illnesses in the past few years. A recent study conducted in Saudi Arabia, designed to estimate the perception of final year medical students in essential critical care concepts, demonstrated that 13% of students were confident in their ability to handle hypovolemic shock, and only 15% recognized the signs of a threatened airway.13
Similar results were found in a survey carried out in six different United Kingdom hospitals among trainee doctors, which demonstrated 31% of trainees revealed the lower end of the normal range for pulse oximetry (SpO2) was below 95%, whereas 5% thought it was below 90%.2 Another study designed to evaluate final year medical students’ perceptions of their knowledge and competence in life-threatening illnesses found that an overall high proportion of students lacked confidence in their ability to manage acute emergencies.14
A similar survey carried out in 2010 to determine the knowledge gap between medical students and newly qualified doctors in intensive care medicine found that only 12.5% of medical students were aware of the Surviving Sepsis Campaign compared to 62% of foundation year 1 junior doctors.15
In 2016, Umm Al-Qura University (UQU) updated its medical school curriculum in association with University College London, which is home to one of the best medical schools in the United Kingdom. The structure of this curriculum consists of 3 stages; The first stage attempts to improve the student’s linguistic ability and provide them with more basic science knowledge; The second stage begins in the second year, it enables students to achieve their scientific competencies in accordance with the SaudiMED Framework, which is affiliated with the National Commission for Academic Accreditation and Assessment. Finally, the third stage starts in the seventh year and it is a compulsory internship year.
These stages include horizontal and vertical modules; the horizontal module is the annual plan that containing integrated fundamentals of clinical science for the first three years and pure clinical science for the next three years. The vertical module consists of seven modules that start in the second year and finish in the final year. It includes family health, anatomy and imaging, pathologic science, use of pharmacology, research and evidence, clinical skills, Hajj and Umrah, and professional development.
Moreover, the learning content, teaching style, and assessment methods were all updated with an attempts to achieve early and adequate clinical exposure. In 2022 the interns and final year students are the first two batches that completed most of their curriculum in the new update and prepared for graduation. Therefore, this research aimed to assess the strength of the curriculum, knowledge, and competence in intensive care medicine and caring for critically ill patients among final year medical students and interns at UQU.
Materials and Methods
Study Design and Study Population
An online cross-sectional study was conducted between January and February 2022 at the college of medicine, UQU, Saudi Arabia, to explore the strength of the curriculum, knowledge, and competence in intensive care medicine among undergraduate medical students.
The average number of interns and final year medical students of UQU during the academic year 2022 is 480. With a confidence level of 95%, a margin of error of 5%, and a response distribution of 50%, the minimum recommended sample size for this study is 214, according to the software Sample Size Calculator (Raosoft, Inc., Seattle, WA, USA). However, 221 participants responded to the questionnaire and were included in the study; 101 were Interns and 120 final year medical students.
Sampling Strategy
A convenience sampling technique was applied to invite final year students and interns to this study. They were invited through social media applications such as WhatsApp and Twitter. The survey’s cover letter mentioned the study’s aim, objectives, and inclusion criteria.
Study Assessment Tools
A previously developed and validated self-administered online questionnaire was used for data collection.13,15 The questionnaire consisted of four sections. The first section covers participants’ demographic information and their academic year.
In the second section of the survey, participants are asked about their exposure to any special study modules focusing on intensive care and the extent of experience regarding critically ill patients. Participants are also asked if they think they have adequate training to identify critical patients in the ICU.
The third section measured their knowledge regarding basic concepts and management of life-threatening conditions in the critical care medicine field.
The fourth section of the questionnaire aimed to assess the competency with basic tools frequently used in daily intensive care units and caring for critically ill patients and if they were satisfied with critical care theoretical/clinical exposure.
Ethical Approval
This study was established after getting ethical approval from the ethical committee of the Faculty of Medicine, UQU, Saudi Arabia. (approval number: HAPO-02-K-012-2022-03-1034).
After the objectives and methodology of the study were explained, consent from the participants was obtained by answering the first question, “Do you agree to participate in this study?”.
The participants were told that their identifying information would not be collected, and all responses would be confidentially maintained.
Statistical Analysis
The datasheet was retracted as an Excel sheet, and statistical analysis was performed using Statistical Package for the Social Sciences (SPSS) software, version 26. Descriptive statistics were obtained to summarize data, synthesize, and report the variables. For categorical variables, percentages and frequencies were used.
Results
A total of 221 participated; 54.3% were males, 45.7% of the participants were interns, and 54.3% were in their final year. Just 13.1% of participants experienced theoretical teaching about ICU (Table 1).
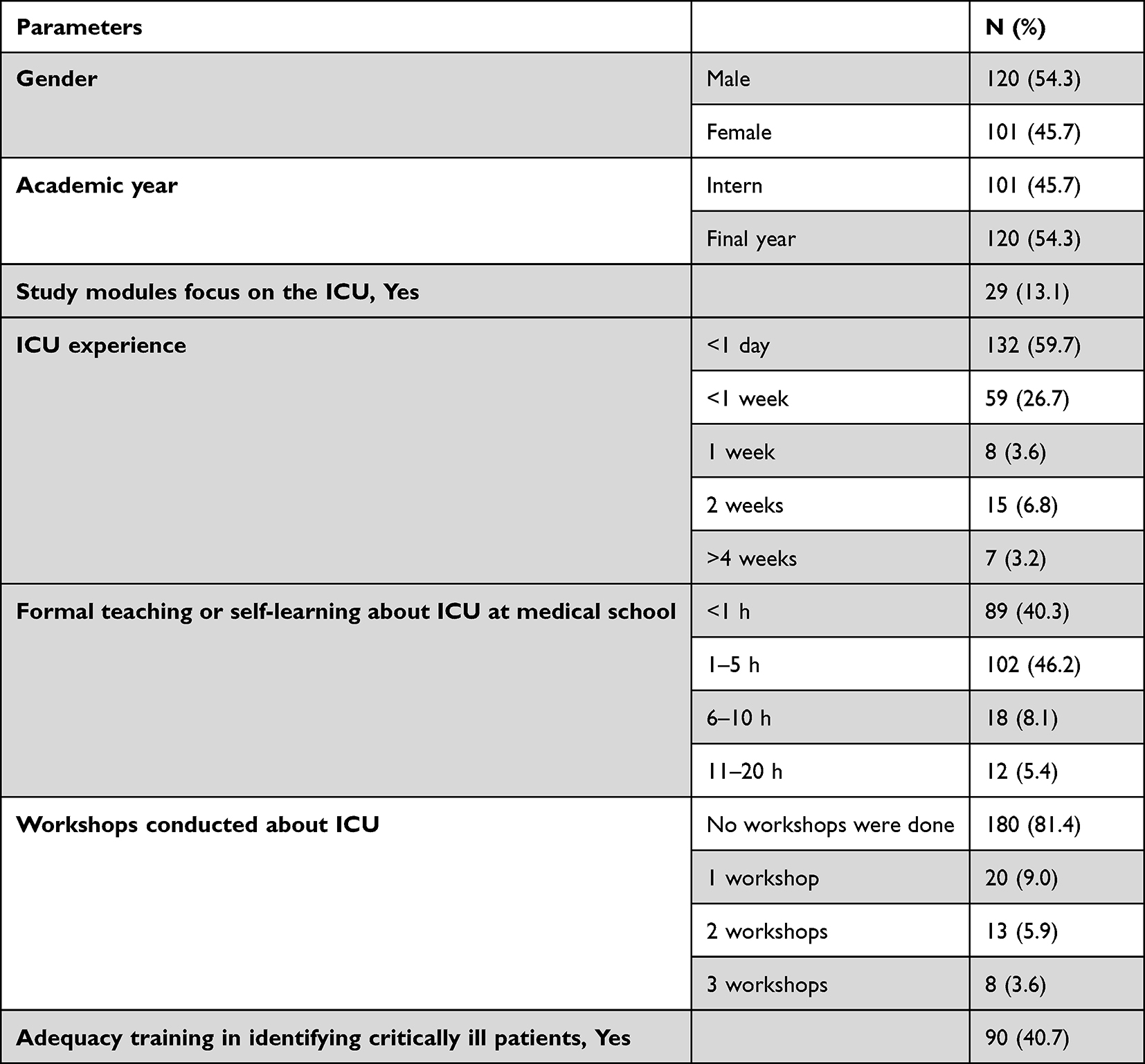 |
Table 1 Sociodemographic Characteristics of the Participants and Critical Care Education (N=221) |
Most of the participants (59.7%) had exposure to the ICU in less than a day, and 86.5% had formal teaching or self-learning about ICU in less than 5 h. Regarding ICU workshops, 81.4% did not attend any workshops, and 59.3% of the participants believed that they did not have adequate training for identifying critically ill patients (Table 1).
Responding to the average length of stay in adult ICU, 31.2% of the participants answered 5 days, and only 38.5% identified the usual nurse to patient ratio in the ICU. Regarding the frequency of physiological observations (RR, HR, BP, and O2 saturation) monitored for an ICU patient, the majority (34.8%) chose 30 min. More than two-thirds of the participants (68.8%) correctly identified the most alarming systolic blood pressure, while a small proportion (15.8%) recognized the lowest acceptable oxygen saturation in a normal individual. In terms of the earliest critical level of lactic acid, approximately 25% of the sample has identified it properly. Almost three-quarters (73.3%) of all the participants stated that the normal capillary refill time is about 1–2 s, and more than half of the participants (65.2%) recognized the correct targeted urine output in resuscitation (Table 2).
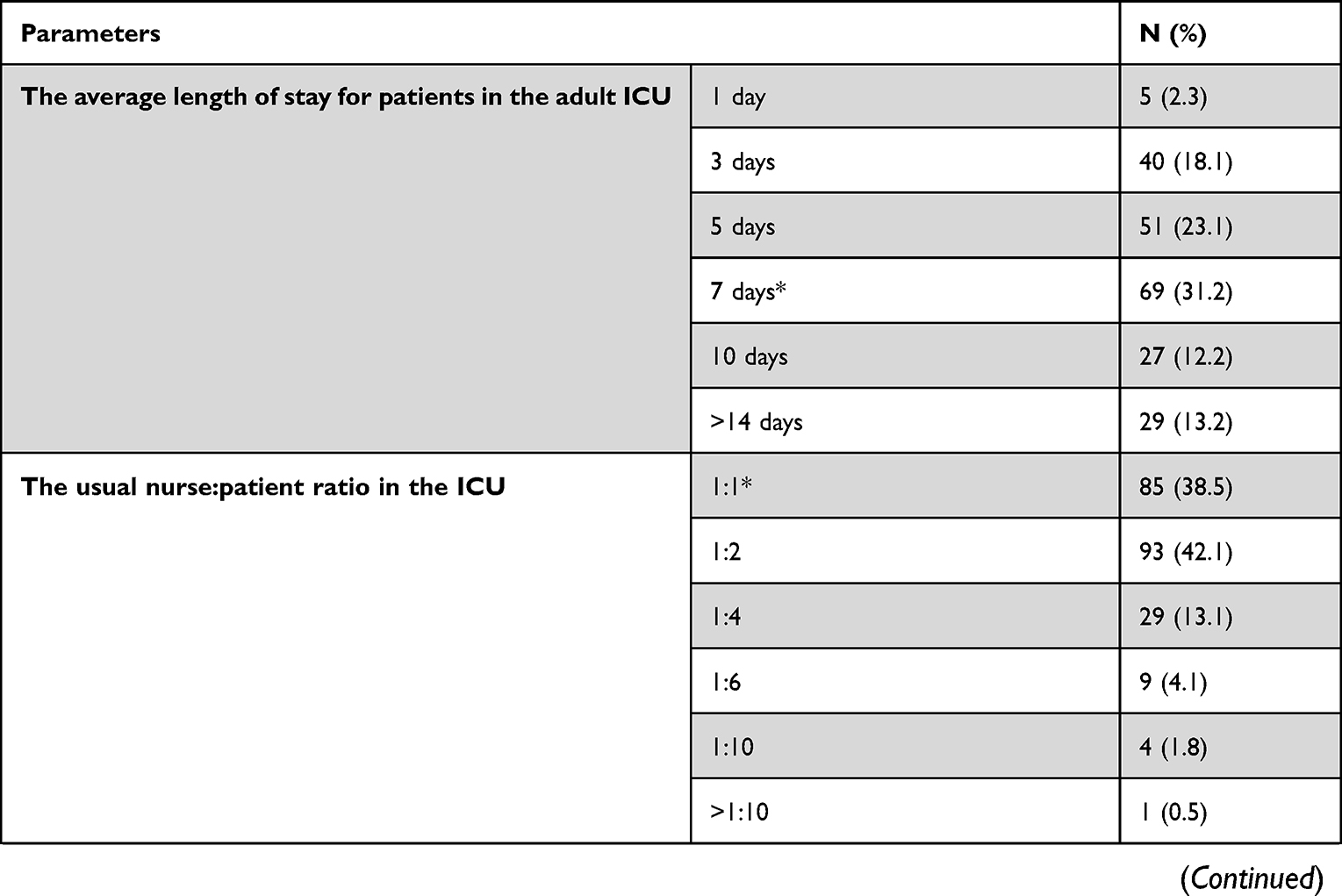 | 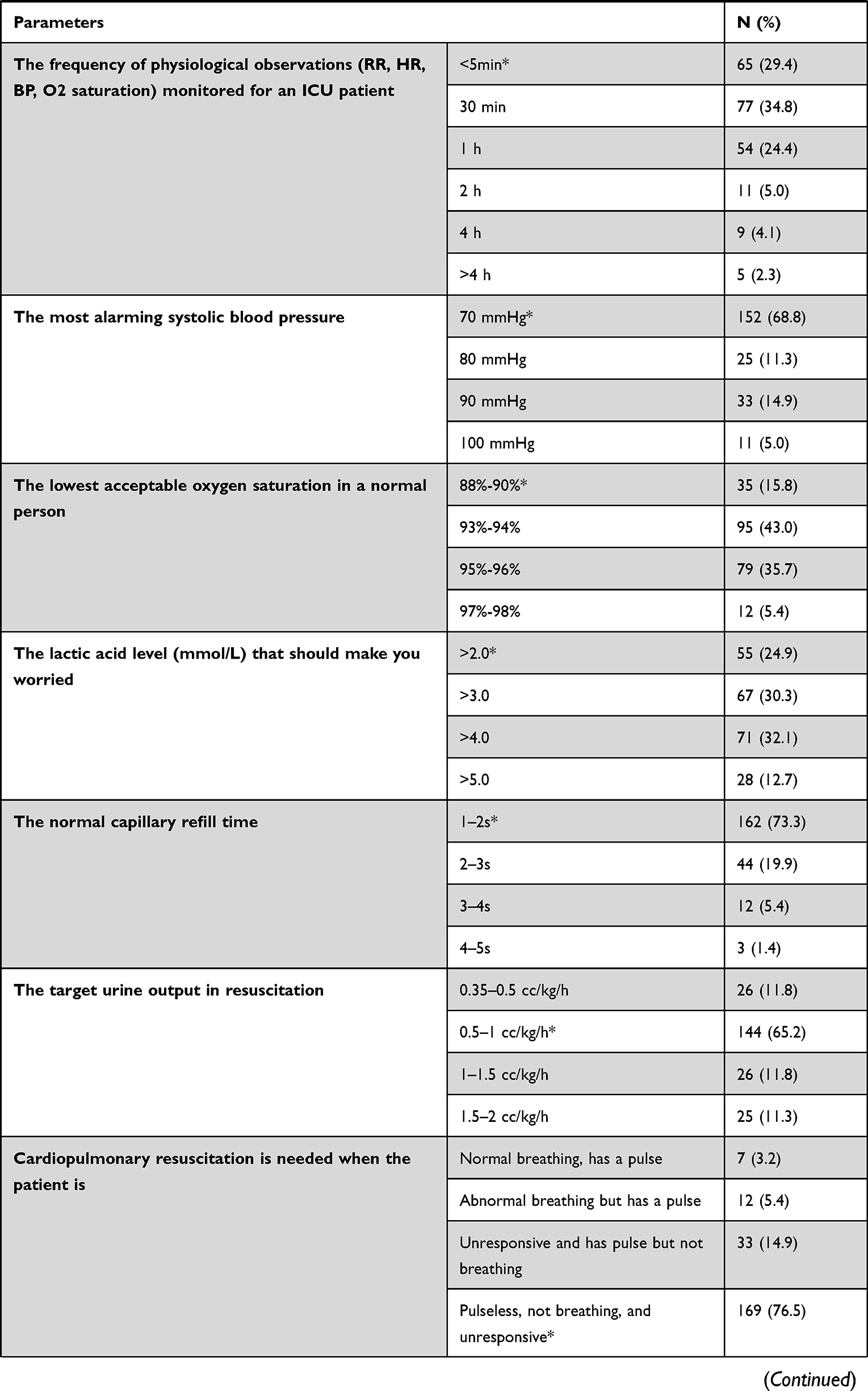 |  | 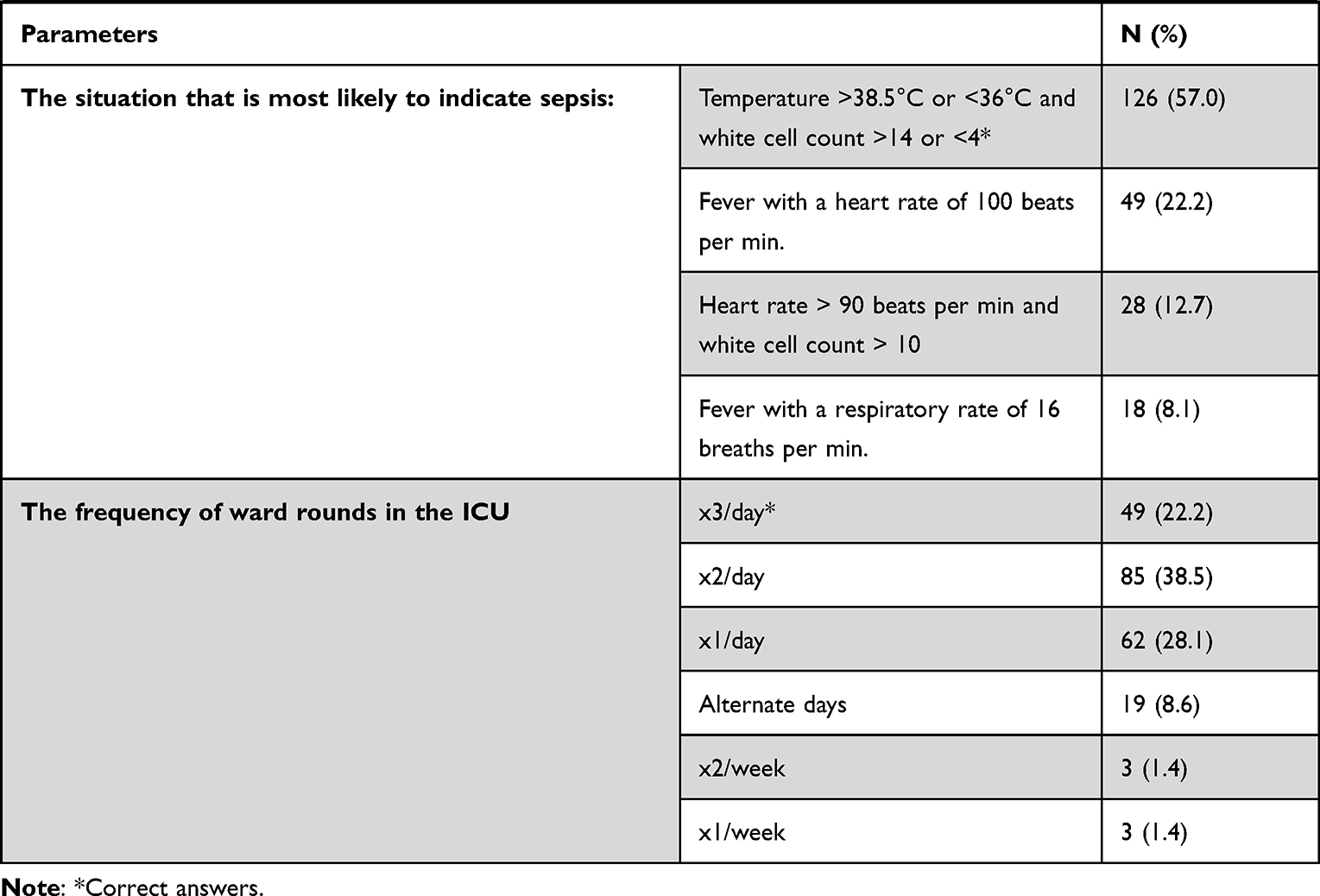 |
Table 2 Critical Care Knowledge of the Participants |
Concerning the competency regarding the basic tools frequently used in the intensive care unit for caring for critically ill patients, around two-thirds of the participants (65.6%) did not feel competent to do nasal airway/suction. Additionally, 75.6% were not comfortable with endotracheal tube suctioning. Regarding assessing patients with pulmonary edema, 45.2% of the participants lacked the competency to do so. A similar percentage of participants were found to lack competency in establishing an airway and mask ventilation techniques. Furthermore, 40.3% of the responders felt incompetent in using the O2 therapy devices (Table 3).
 |
Table 3 Competency with Basic Tools Frequently Used in Daily Intensive Care Unit and Caring for Critically Ill Patients |
When asked about the three physiological observations for identifying sick patients according to quick SOFA criteria, blood pressure was chosen the most (86%), level of consciousness (53.4%) and respiratory rate were chosen by 29.9% of the sample, whereas only 7.2% of the sample have correctly identified all three (Figure 1).
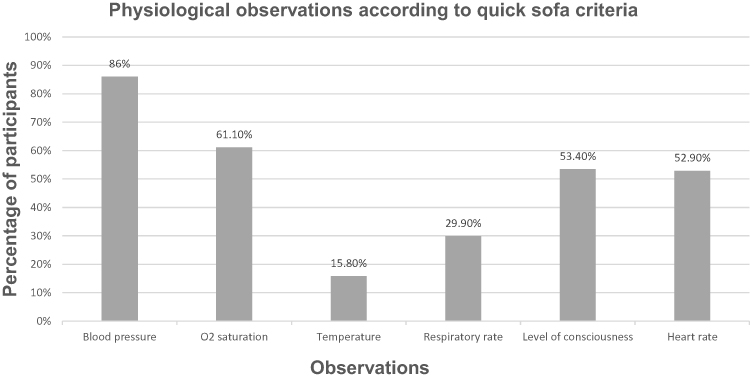 |
Figure 1 Three most useful physiological observations for identifying sick patients according to quick SOFA criteria. |
Upon answering the three tools used for the assessment of critically ill patients, the qSOFA score, SIRS criteria, and APACHE II score were selected (87.3%, 70.1% and 59.3%, respectively); however, exclusively, 30.3% of the participants have correctly chosen them all together (Figure 2).
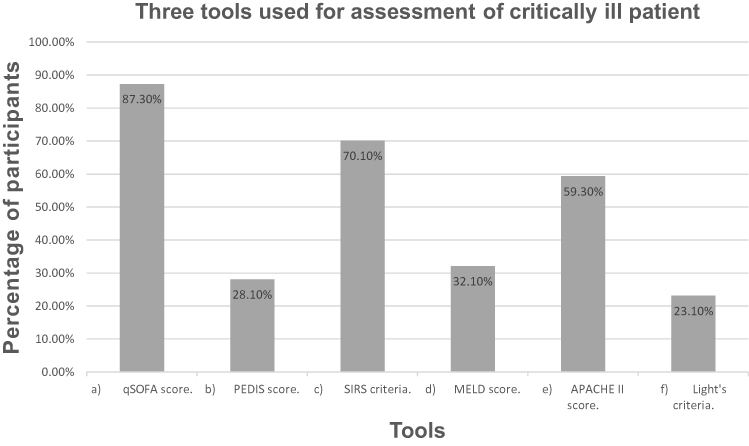 |
Figure 2 Three tools used for the assessment of critically ill patients. |
In evaluating the five most common clinical signs and assessments in investigating a critical illness, the participants emphasized GCS, airway patency, circulation adequacy, pulse rate, and pupils’ examination (Figure 3).
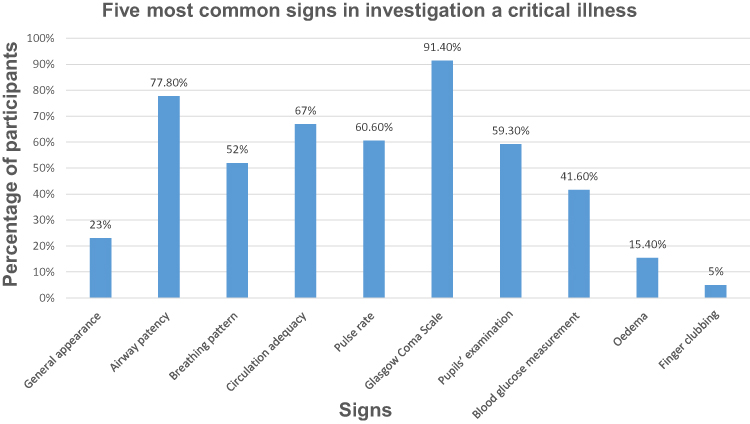 |
Figure 3 The five most common clinical signs and assessments in investigating a critical illness. |
Regarding the satisfaction level of exposure to critical care, more than half of the sample (54%) believed they needed improvement (Figure 4).
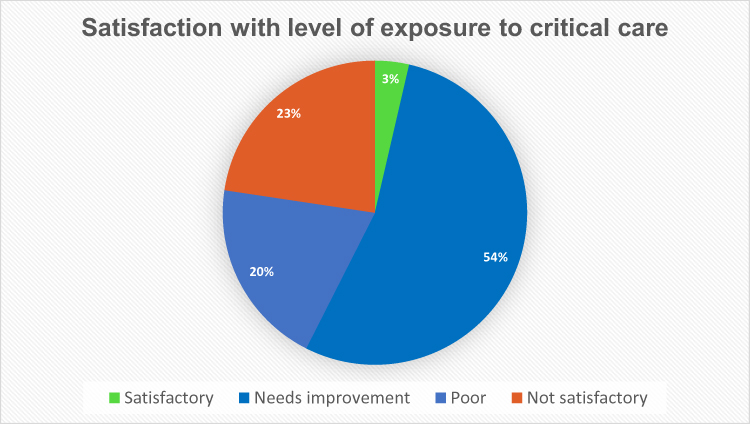 |
Figure 4 Satisfaction with the level of exposure to critical care. |
Discussion
A cross-sectional study was carried out between January and February 2022 and distributed via a social media platform. This study involved interns and final year medical students at the College of Medicine, Umm Al-Qura University. A high response rate was achieved, and a standardized, validated questionnaire was used to assess the level of knowledge and confidence toward the intensive care unit and care for critically ill patients.
The current study found a deficiency in critical care exposure to the ICU. More than half the participants (59.7%) had an exposure of less than 1 day; in addition, 86.5% had formal teaching or self-learning about ICU in less than 5 h. Our results align with a previous study among medical students in Saudi Arabia.13 The time spent self-learning about ICU is less than 5 h for 82.1% of the subject. However, this is higher than a study performed in England, which reported a value of just 42.9%.15 This discrepancy could be attributed to the different study designs and sample sizes.
Our research demonstrated that half of the sample (54%) believed that they needed more exposure to critical care. This finding is consistent with other studies.15–18
We found that 65.6% of the sample did not feel competent with nasal airway/suctioning, and 75.6% were also incompetent with endotracheal tube suctioning; this agrees with a study conducted in Saudi Arabia.13
Many critical care associations and organizations have advocated for critical care education to be included as a dedicated block in medical school curricula.1,19–21 Critical care is exceptional in that it offers a wide range of clinical experiences and clear, measurable cognitive and procedural learning results. Critical care units are good places to develop communication skills, professionalism, and systems-based approaches like triage and bundling.22
Despite the clear benefits of focused education in this field, critical care is still inconsistently taught to undergraduate medical students worldwide.16,23 According to a survey of Irish medical schools, most critical care student placements were shorter than 5 days and included no procedural training.22 Furthermore, a study of intensive care education in English-speaking medical schools found that intensive care education was compulsory in just 31%. In contrast, a survey of Australian and New Zealand medical schools found that mandatory teaching of critical care was offered by 56% of medical schools. The duration of such teaching in most curricula was less than 1 week.16,23
Dispersed and non-core-focused teaching is the current undergraduate acute/critical care education.16,24 A structured curriculum model is required, with explicit learning objectives, a combination of bedside, classroom, and eLearning activities, procedural skills training, enriched evaluation of teaching and teaching techniques, and a formal student assessment process.22
According to the literature, undergraduate medical students have indicated an interest in critical care medicine and desire further exposure.18,25
Early exposure to critical care as a unique field, in the form of a well-structured curriculum, may inspire students to pursue critical care as a career path, increasing the existing low interest in this vital specialty.25,26 A recent study conducted in United States, assessed ICU curricular efficacy and impact with a pre and posttest and end of curriculum survey, an integrated ICU curriculum was implemented within the third-year internal medicine clerkship, demonstrated that 73% of students strongly agree that their overall clerkship experience improved as a result of their curriculum, with regard to attitudes, more than half of the sample reported increased comfort in their ability to participate in the management of critically ill patients. Students also reported an increased likelihood of applying for an ICU sub-internship during their fourth year of medical school.27 One key feature towards the importance of early training in critical care is that it is also assists students to be prepared for their clinical practice in the future. There is evidence that preparing students for this type of thing can assist them to become more confident in their transitions between year-levels in a medical program, but also in their transition to clinical practice.28
In the central area of Saudi Arabia in 2015, there were only 43 critical care consultants for 458 tertiary critical care beds, with a lower ratio in other locations.29
It is important to improve undergraduate knowledge and competencies to ensure patient safety. For maximum patient safety, obstacles such as a full curriculum, limited staff, and a lack of funding should be overcome.12
Limitations of the Study
The current study has some limitations. First, only one medical school was surveyed; therefore, this might affect the generalizability of the study. However, our sample size and high response rate support the validity of these research findings. Second, we did not include objective tools to assess the competency.
Conclusion and Recommendations
Undergraduate medical students have overall inadequate critical care exposure and competency, and they need further improvement aiming to prepare them with the desired skills and knowledge. Therefore, we recommend integrating critical care education in the forms of dedicated lectures, workshops, and hands-on clinical training in medical school’s curriculum. Future research is needed to assess the effect of such an early exposure and to find any obstacles in order to optimize the learning outcomes. Additionally, objective measurements of competency in critical care abilities should be included in future evaluations.
Data Sharing Statement
All the data related to this study is available upon request.
Acknowledgment
The authors would like to express their gratitude and appreciation to all participants in our study.
Disclosure
The authors report no conflicts in this work.
References
1. Fessler HE. Undergraduate medical education in critical care. Crit Care Med. 2012;40(11):3065–3069. doi:10.1097/CCM.0b013e31826ab360
2. Smith GB. Knowledge of aspects of acute care in trainee doctors. Postgrad Med J. 2002;78(920):335–338. doi:10.1136/pmj.78.920.335
3. Perkins GD, Barrett H, Bullock I, et al. The Acute Care Undergraduate TEaching (ACUTE) Initiative: consensus development of core competencies in acute care for undergraduates in the United Kingdom. Intensive Care Med. 2005;31(12):1627–1633. doi:10.1007/s00134-005-2837-4
4. Barber N. Reducing prescribing error: competence, control, and culture. Qual Saf Health Care. 2003;12(90001):29i–32. doi:10.1136/qhc.12.suppl_1.i29
5. Wilson RM, Runciman WB, Gibberd RW, Harrison BT, Newby L, Hamilton JD. The Quality in Australian Health Care Study. Med J Aust. 1995;163(9):458–471. doi:10.5694/j.1326-5377.1995.tb124691.x
6. Morris F, Tordoff SG, Wallis D, Skinner DV. Cardiopulmonary resuscitation skills of preregistration house officers: five years on. BMJ. 1991;302(6777):626–627. doi:10.1136/bmj.302.6777.626
7. Sanders AB, Criss E, Witzke D, Levitt MA. Survey of undergraduate emergency medical education in the United States. Ann Emerg Med. 1986;15(1):1–5. doi:10.1016/S0196-0644(86)80477-2
8. Wu AW, Folkman S, McPhee SJ, Lo B. Do house officers learn from their mis- takes? JAMA. 1991;265(16):2089–2094. doi:10.1001/jama.1991.03460160067031
9. Cooper N. Patient at risk! Clin Med. 2001;1(4):309–311. doi:10.7861/clinmedicine.1-4-309
10. General Medical Council: Tomorrow’s Doctors. 2009. Outcomes and Standards for Undergraduate Medical Education. ISBM 978-0- 901458-36-0.:108 General Medical Council: Tomorrow’s Doctors.
11. Alansari MA. Quality of undergraduate critical care medical education in the Kingdom of Saudi Arabia. Where do we stand? Saudi Med J. 2014;35(1):95–96
12. Smith CM, Perkins GD, Bullock I, Bion JF. Undergraduate training in the care of the acutely ill patient: a literature review. Intensive Care Med. 2007;33(5):901–907. doi:10.1007/s00134-007-0564-8
13. Al Ansari M, Al Bshabshe A, Al Otair H, et al. Knowledge and Confidence of Final-Year Medical Students Regarding Critical Care Core-Concepts, a Comparison between Problem-Based Learning and a Traditional Curriculum. J Med Educ Curric Dev. 2021;8:238212052199966. doi:10.1177/2382120521999669
14. Harrison GA, Hillman KM, Fulde GWO, Jacques TC. The Need for Undergraduate Education in Critical Care (Results of a Questionnaire to Year 6 Medical Undergraduates, University of New South Wales and Recommendations on a Curriculum in Critical Care). Anaesth Intensive Care. 1999;27(1):53–58.
15. Kelly D. The Knowledge of Medical Students and Newly Qualified Doctors concerning the Specialty of Intensive Care Medicine. J Intensive Care Soc. 2011;12(2):98–106. doi:10.1177/175114371101200205
16. Shen J, Joynt GM, Critchley LAH, Tan IKS, Lee A. Survey of current status of intensive care teaching in English-speaking medical schools. Crit Care Med. 2003;31(1):293–298. doi:10.1097/00003246-200301000-00047
17. Almeida ADM, Albuquerque LC, Bitencourt AGV. Medicina intensiva na graduação médica: perspectiva do estudante. Rev Bras Ter Intensiva. 2007;19(4):456–462. doi:10.1590/S0103-507X2007000400009
18. Lyss-Lerman P, Teherani A, Aagaard E, Loeser H, Cooke M, Harper GM. What Training Is Needed in the Fourth Year of Medical School? Views of Residency Program Directors. Acad Med. 2009;84(7):823–829.
19. Frankel HL, Rogers PL, Gandhi RR, Freid EB, Kirton OC, Murray MJ. What is taught, what is tested: findings and competency-based recommendations of the Undergraduate Medical Education Committee of the Society of Critical Care Medicine. Crit Care Med. 2004;32(9):1949–1956. doi:10.1097/01.CCM.0000134403.44704.91
20. Carvalho P. Early introduction to critical care medicine: a student curriculum. Med Educ. 2007;41(5):513–514. doi:10.1111/j.1365-2929.2007.02739.x
21. Luks A, King M. Early introduction to critical care medicine: really good stuff. Med Educ. 2011;45(5):515. doi:10.1111/j.1365-2923.2011.03954.x
22. O’Connor E, Martin-Loeches I. A blueprint for improving undergraduate education in intensive care medicine. Crit Care. 2016;20(1):212. doi:10.1186/s13054-016-1383-5
23. Whereat SE, McLean AS. Survey of the current status of teaching intensive care medicine in Australia and New Zealand medical schools. Crit Care Med. 2012;40(2):430–434. doi:10.1097/CCM.0b013e31823295fe
24. Mila GB, Caturla J. Teaching critical care in Europe: analysis of a survey. Critical Care Med. 1996;24(4):696–704.
25. Lorin S, Heffner J, Carson S. Attitudes and perceptions of internal medicine residents regarding pulmonary and critical care subspecialty training. Chest. 2005;127(2):630–636. doi:10.1378/chest.127.2.630
26. Neves FBCS, Vieira PSPDG, Cravo EA. Motivos relacionados à escolha da medicina intensiva como especialidade por médicos residentes. Rev Bras Ter Intensiva. 2009;21(2):135–140. doi:10.1590/S0103-507X2009000200004
27. Gergen D, Raines J, Lublin B, Neumeier A, Quach B, King C. Integrated critical care curriculum for the third-year internal medicine clerkship. MedEdPORTAL. 2020;3:11032. doi:10.15766/mep_2374-8265.11032
28. Moro C, Spooner A, McLean M. How prepared are students for the various transitions in their medical studies? An Australian university pilot study. MedEdPublish. 2019;8(8):25. doi:10.15694/mep.2019.000025.1
29. Al-Omari A, Abdelwahed HS, Alansari MA. Critical care service in Saudi Arabia. Saudi Med J. 2015;36(6):759–761. doi:10.15537/smj.2015.6.11204
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.