Back to Journals » Infection and Drug Resistance » Volume 14
Knowledge and Awareness of Physicians About Rational Antibiotic Use and Antimicrobial Resistance Before and After Graduation: A Cross-Sectional Study Conducted in Malatya Province in Turkey
Received 4 May 2021
Accepted for publication 22 June 2021
Published 5 July 2021 Volume 2021:14 Pages 2557—2568
DOI https://doi.org/10.2147/IDR.S317665
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Adem Kose,1 Cemil Colak2
1Department of Infectious Diseases and Clinical Microbiology, Faculty of Medicine, Inonu University, Malatya, Turkey; 2Department of Biostatistics, and Medical Informatics, Faculty of Medicine, Inonu University, Malatya, Turkey
Correspondence: Adem Kose
Department of Infectious Disease and Clinical Microbiology, Faculty of Medicine, Inonu University, Elazig Yolu 10. Km, Battalgazi, Malatya, 44280, Turkey
Tel +90 4223410660/ 4405
Fax +90 4223411220
Email [email protected]
Background: We aimed to evaluate the level of theoretical knowledge of rational antibiotic use and awareness about emergence of multidrug resistance (MDR) among the senior students at a medical school and the actively-working family physicians.
Methods: This cross-sectional research was carried out between 1 February and 30 April 2019 in Malatya province. Two-hundred twenty-five senior students in the Inonu University Medical School (Group 1) and 230 actively-working family physicians in Malatya primary health care services who were found to be eligible (Group 2) were included in this study. Power analysiscalculated the minimum of 240 participants with a proportion difference of 0.18 between the groups, a type I error of 0.05 and a type II error of 0.20. A questionnaire including seven sections and 28 questions was applied to the participants.
Results: Doctors were more hesitant in pre-graduation and more self-confident in the post-graduation period for the decision to start antibiotic treatment. In addition, doctors forget their theoretical knowledge of antibiotics over time and are unable to follow current developments after graduation. The most important concern in the pre-graduation period was the choice of antibiotics from the wrong group, while in the post-graduation period it is the fear of the presence of unproven infection.
Conclusion: Physicians’ antibiotic prescribing habits, attitudes and behaviors vary before and after graduation. Sustainable education for antibiotic use for physicians after graduation can contribute positively to reduce of antimicrobial resistance rates and to increase awareness about the use of rational antibiotics.
Keywords: antimicrobial resistance, multidrug resistance, knowledge, awareness, rational antibiotic use, MDR
Introduction
Globally, antibiotics are among the most prescribed drugs. A study from the UK showed that 30% of the patients who visit primary care physicians are prescribed some form of antibiotic.1 Modern medicine is intricately linked to the rational use of antimicrobials to treat infections, but the emergence of multidrug resistant (MDR) microorganisms threatens future generations.2 Irrational antibiotic use is a serious problem throughout the world. The use of unnecessary antibiotics causes a heavy burden on the economy of developing countries, such as Turkey.3
As a result of excessive and irrational antibiotic use, MDR microorganisms are increasing all over the world, which has resulted in an increase in the cost of treatment and has become a universal public health problem, leading to high morbidity and mortality rates.4–6 The World Health Organization (WHO) reported that more than 25,000 people die each year because of infections that arise from resistant bacteria in Western countries; and the cost of approximately 1.5 billion euros.7 Compared with Systemic Antimicrobial Consumption of European Countries (ESAC-Net), Turkey had the highest antibiotic use in Europe. Thus, the Turkish government already published a Rational Drug Use National Action Plan 2013–2017, with quantitative targets to reduce the use of antibiotics.8 The rate of irrational use of antibiotics is high among patients who attend primary health care facilities in Turkey.9 The use of antimicrobial drugs is closely related to the knowledge and attitudes of the physicians, as well as the antibiotic prescription behavior of the health care professionals. All these factors contribute to the increase of MDR.10 The rapid increase in population, low socioeconomic status, and the differences in the theoretical knowledge of the physicians who prescribe the antibiotics, are some of the factors that may cause the rate of increase.11,12 The most important factor in starting antibiotic treatment for a patient is the presence of active infection and the evidence of its positive culture result. On the other hand, during empirical antibiotic treatment for a potential infection requires predicting the most probable factors that may cause infection.13 There are few studies on the attitudes of physicians towards antibiotic treatment in Turkey; and the studies regarding the subject are not enough. Therefore, this study was conducted to understand the problems and to offer solutions to provide more rational antibiotic use in Turkey.
In this study, we aimed to investigate rational antibiotic use through the evaluation of antimicrobial prescription habits, the level of theoretical knowledge of rational antibiotic use and awareness about antimicrobial resistance among senior medical students in comparison to family physicians in the Malatya province in Turkey.
Materials and Methods
Study Design
This study was carried out between 1 February and 30 April 2019 in Malatya, which has a population of approximately 750 thousand people. This survey study was designed in line with the information obtained from various published research articles,14,15 and a questionnaire form that we have prepared, including seven sections and twenty-eight questions. Section 1 consisted of demographic data such as age, gender, and professional experience of the individual. Section 2 consisted of four questions regarding data on personal antibiotic use. Section 3 consisted of three questions regarding the decision to start antibiotic treatment. Section 4 consisted of nine questions assessing the knowledge about rational antibiotic use. Section 5 consisted of four questions regarding antimicrobial resistance. Section 6 consisted of three questions assessing training on rational antibiotic use before graduation from medical school. Section 7 consisted of five questions in the form of “blanks-filling” regarding theoretical knowledge on antibiotic use. The principles and purpose of this survey study were explained to all participants. The verbal approval of all participants was obtained and a consent form was signed by each participant. The informed consent form was obtained from all participants included in the present study. Data were collected using face-to-face interviews. All the answers were recorded to by researchers. The names of the participants were kept confidential and this was stated to the patients in the beginning of the questionnaire. The collected data were compared among the groups.
Power Analysis
Power analysis suggested a minimum of 120 senior students and 120 family physicians (totaling 240 people) when considering a proportion difference of 0.18 between the groups, a type I error of 0.05 and a type II error of 0.20.
Inclusion and Exclusion Criteria
In this study, 225 senior students (group 1: the SS group) from Inonu University Medical School and 230 actively working family physicians in Malatya province (group 2: the FP group) were included. Non-medical professionals, physicians who do not work in primary care services, specialists from other branches, and physicians who were not actively working, even if they had experience to work as a family physician, were excluded from the study.
Ethical Approval and Consent to Participate
This study was approved by the Non-Interventional Ethics Committee at Inonu University (Approval no: 2019/01-8). Another necessary permission for e-prescription information system data was obtained from the Public Health Unit of Malatya Provincial Health Care Directorate (2019–1208). The informed consent form was obtained from all participants in this study.
Data Analysis
The quantitative data were given as mean±standard deviation, and qualitative data were summarized as numbers with percentages. Normal distribution was checked using the Kolmogorov–Smirnov test. Qualitative (nominal) data were analyzed by the Pearson Chi-Square test as appropriate. Comparison of proportions was made using the Bonferroni-adjusted Pearson Chi-Square test. A p<0.05 value was considered to be statistically significant. The IBM SPSS Statistics 25.0 software for Windows was used for analyses.
Results
General Demographic Characteristics of the Study Population
There were 455 participants in this study: Group 1 had 225 (49.5%), and Group 2 had 230 (50.5%) participants. In Group 1, there were 92 males (40.9%), 133 females (59.1%) between 21 and 28 years of age; the mean age was 24±1 year. In Group 2, there were 153 males (66.5%), 77 females (33.5%) between 25 and 66 years of age, and the mean age was 41±9 years. The professional experience of group 2 was; 32 individual (13.9%) having 1–5 years, 45 individuals (19.6%) having 6–10 years, and 153 individuals (66.5%) having 11 years of experience or more.
Analysis of the Results of the Responses to the Questionnaire
For the decision to start antibiotic treatment, it was observed that Group 1 was more hesitant, and Group 2 was more self-confident, but forgot their theoretical antibiotic knowledge over time, and they could not follow the current information because of the intensity of their work. While Group 1 thinks that antibiotic treatment is required mostly in the presence of sore throat, Group 2 believes that antibiotic treatment is required in the presence of prolonged cough and sputum. They stated that the biggest concern was the selection of antibiotics from the wrong group in Group 1, and performing unnecessary antibiotic treatment to patients in Group 2. While Group 1 starts antibiotic treatment with insufficient knowledge of antibiotics, Group 2 starts antibiotic treatment in cases with unproven infection. Group 1 decides to start antibiotic therapy in the presence of fever, and Group 2 decides to start antibiotic therapy in the presence of leukocytosis. As shown in Table 1, while Q2-3-5-6-7 were significantly different between groups (p<0.001), the other questions were not statistically significant (p>0.05).
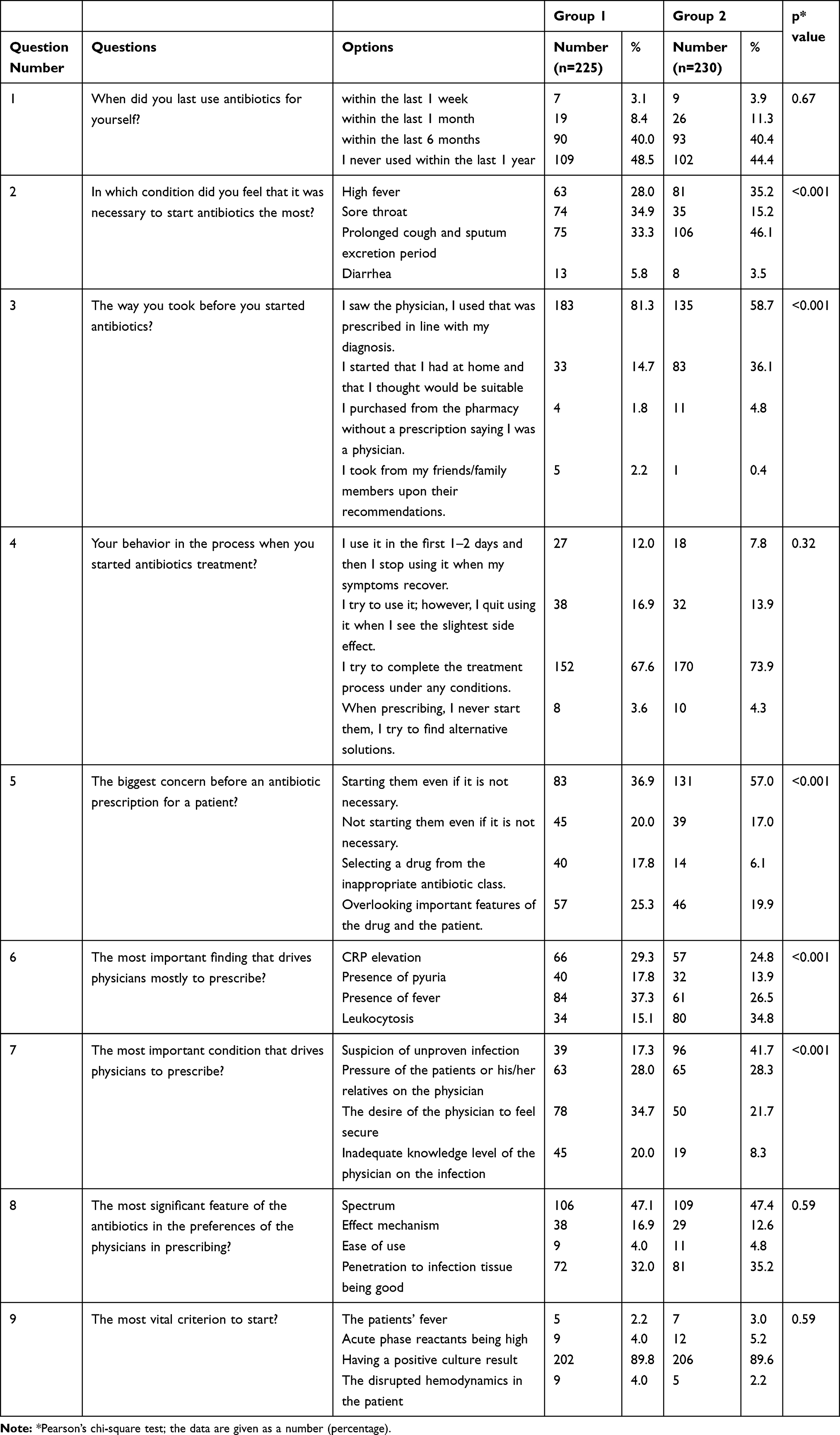 |
Table 1 The Behavior of the Groups About Personal Antibiotic Use and the Doctors’ Decisions in Starting the Antibiotics Treatment for Patients |
Both groups stated that the most important principle for rational use of antibiotics is the presence of infection and that the most unnecessary use of antibiotics is the treatment of the common cold. It was observed that Group 1 had better theoretical knowledge about combined antibiotic use, surgical prophylaxis and chemoprophylaxis purposes than Group 2. As presented in Table 2, although the differences between the groups were significant regarding Q10-11-14-15 (p<0.05), the differences between the groups were non-significant regarding other questions (p>0.05).
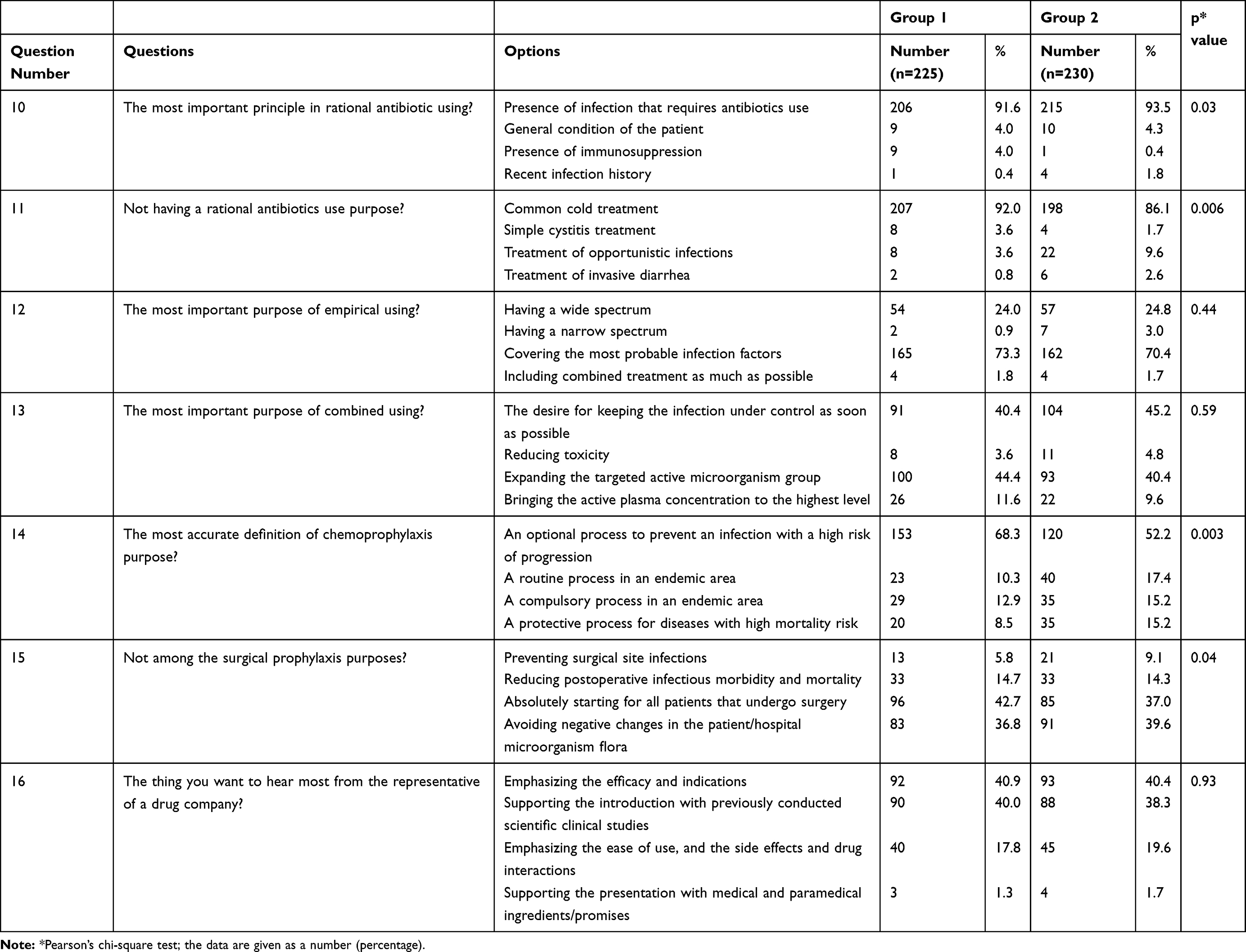 |
Table 2 The Distribution of the Questions and Answers Related to the Rational Use of Antibiotics |
Both groups stated that the most negative result of irrational use of antibiotics was the development of antimicrobial resistance and could lead to treatment failure. For increasing awareness of antimicrobial resistance, Group 1 thought that written and visual media could be more effective, while Group 2 stated that strict antibiotic use policies and penal sanctions might be more effective. Both groups stated that post-graduation trainings could be used effectively for reducing antimicrobial resistance. To raise awareness of antimicrobial resistance, the slogan of both groups has been “Either awareness or resistance develops for antibiotics.” Both groups noted that antibiotic training at the Medical School was partially adequate, noting that good prescribing skills can be gained by evaluating patients in clinics, actively. In Table 3, Q19-20-21-23 were significantly different between the groups (p<0.05); the remaining questions were not significantly different (p>0.05).
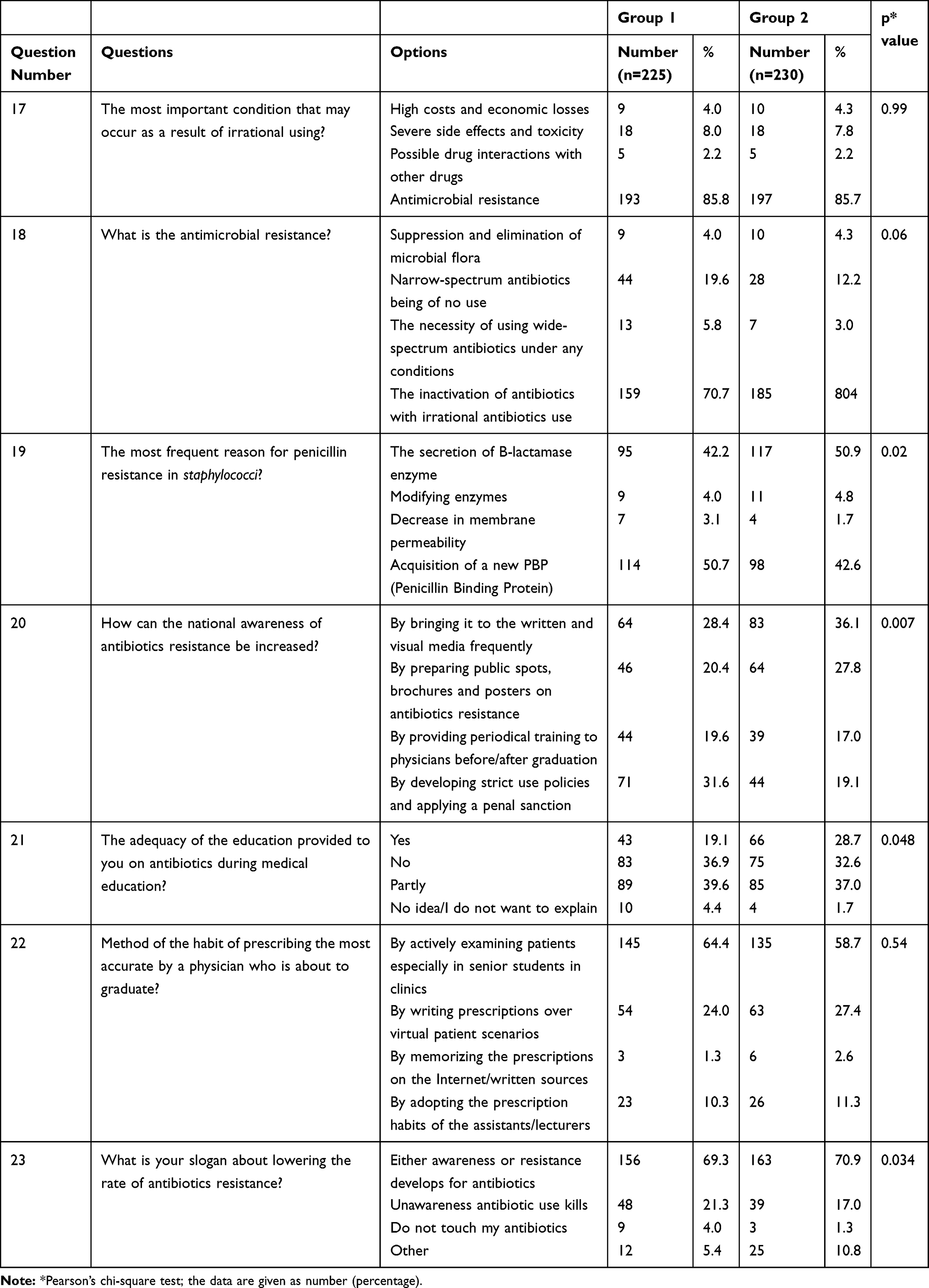 |
Table 3 The Distribution of the Antimicrobial Resistance and Awareness, Developing Recommendations and Slogans for Decreasing Antibiotic Resistance and Increasing Awareness |
Analysis of the Responses to Open Ended Questions
As shown in Table 4, Group 1 answered the gap-filling questions that required theoretical knowledge more correctly than Group 2.
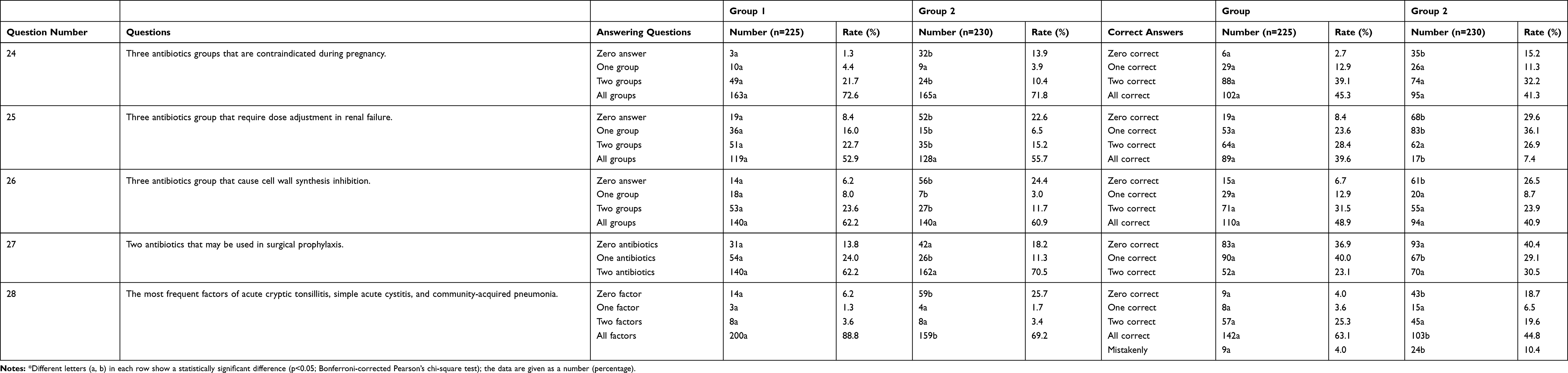 |
Table 4 Data of the Groups on Answering the Questions on Antibiotic Information (Fill in the Blanks)* |
According to the data from the e-prescription information system of Malatya Public Health Directorate, the rate of antibiotic prescription decreased in years when patients are admitting for primary health care services in Malatya. In the last three years, the rates of unnecessary prescriptions for antibiotics have decreased with postgraduate training courses on antibiotic use (Table 5).
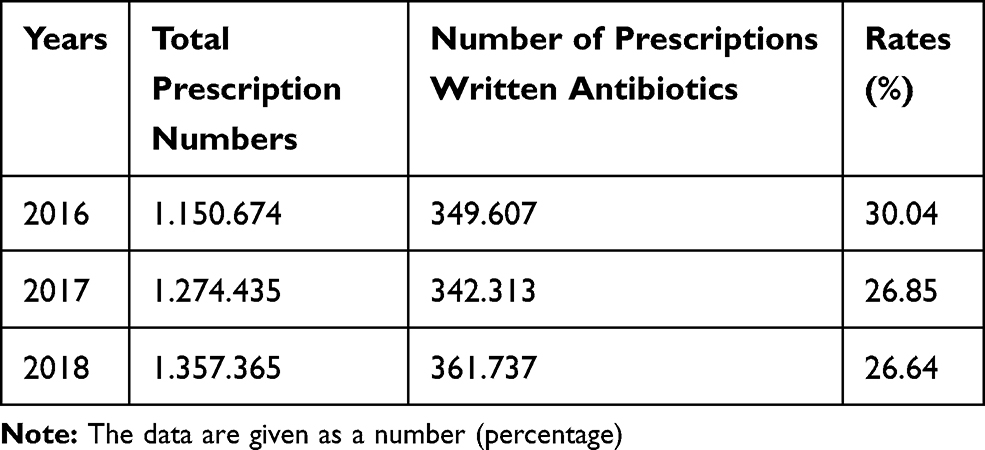 |
Table 5 Three-Year Antibiotic Consumption Rates by Years in Primary Health Care Services in Malatya Province in Turkey |
Discussion
In the present study, the survey was performed to medical school senior students and actively-working family physicians to determine antimicrobial prescription habits and to evaluate the level of theoretical knowledge of rational antibiotic use. Also, awareness about antimicrobial resistance were also evaluated in different levels of the profession. It was observed that doctors were more hesitant in pre-graduation period and more self-confident in post-graduation period in terms of decision to start antibiotic treatment. These different approaches might be associated with the lack of self-confidence in the professional experience of the physicians or may be due to lack of adequate time. The differences in knowledge, attitudes, and behaviors of physicians who prescribe antibiotics in primary health care facilities on decision to start treatment and the necessity of treatment may also cause the rates of increased antibiotic prescription.16 In addition, doctors forget their theoretical knowledge regarding rational antibiotic use and are unable to follow current developments due to the intensity of the work. Therefore, they are more likely to make mistakes. This situation has once again revealed the importance of postgraduate education programs. Training after graduation may be crucial in reducing the excessive rates of antibiotic usage. The most important concern in the pre-graduation period is the choice of antibiotics from the wrong group. In the post-graduation period, it is the fear of the presence of unproven infection.
Unnecessary antibiotic use and MDR are still significant problems in low socioeconomic countries.17,18 In our country, the efforts have been made to reduce unnecessary antibiotic use and to promote awareness for antimicrobial resistance levels of physicians with training before and after graduation. In addition, this issue is promoted in written and visual media to increase the public awareness. Furthermore, since 2014, measures have been taken to prevent over the counter sales of antibiotics in pharmacies. A study by Mahmood et al19 showed that the irrational antimicrobial use resulted in reduced quality of care, increased morbidity and mortality, and increased cases of adverse drug reactions and medication errors. Andrajati et al20 conducted a study through analyzing 788 oral prescriptions, which were prescribed by 28 doctors for acute pharyngitis and nonspecific respiratory infections at primary health care services, and 392 of them were evaluated for rationality according to local guidelines issued by Indonesian Ministry of Health. They found that 220 prescriptions did not meet the criteria for rational antibiotic prescription. In addition, they concluded that training for rational antibiotic use and physician experience were the factors associated with the rationality of antibiotic prescriptions. Since viral agents play roles in the etiology of the common cold, antibiotics have no use in its treatment.21 We found that both groups had a sufficient level of awareness of this subject.
The quality of a physician candidate’s pre-graduation education, the ability to apply their knowledge and skills can significantly affect attitudes and behaviors when starting antibiotic therapy. Many factors may influence doctors’ decisions, leading them to breach the principles of good clinical practice.22 Among these problems are the fear of possible future complications in their patients or a desire to fulfill patients’ expectations. Many physicians fear that they may miss out on the infection in the presence of leukocytosis, and often prefer to prescribe antibiotics to feel safe.23 The physicians who had less experience believed that the presence of fever was more important, and the suspicion of infection but nor proven by laboratory tests was the most important factor causing primary health care physicians to write antibiotics.24 Unfortunately, currently doctors can spare less time to patients for diagnosis because of overcrowded hospitals and primary care services. There is often pressure to prescribe antibiotics by patients and/or their relatives.25 One of the reasons of irrational antibiotic use is the expectation or demand of the patient regarding prescription of an antibiotic. Especially in our country “being a good doctor” is equivalent to writing an antibiotic prescription, insufficient examination facilities, and the need for the physician for feel safe by prescribing antibiotics by fearing that they might overlook an infection.26 The expectation of a patient to prescribe an antibiotic from the physician, keeping the equivalent of writing good medicine prescriptions, insufficient examination facilities, and the need for the physician to feel safe by prescribing antibiotics with the fear of missing a possible infection are among the most common causes of irrational antibiotic use.27
Antimicrobial resistance or MDR can be defined as the inefficiency of antibiotics in time due to the irrational/excessive use of antibiotics.28 The correct definition is made by Group 1 at higher rates which may be explained by that their theoretical knowledge. The most common reason for penicillin resistance in Staphylococci is the synthesis of a new PBP (Penicillin-Binding Protein).29 Although nearly half of Group 1 was thought in this way, more than half of Group 2 believed that beta-lactamase was secreted, which was wrong. This finding may suggest that both groups are inadequate or not up-to-date their knowledge of antimicrobial resistance mechanisms. The presence of comorbid conditions and diseases must be considered in a patient to who antibiotics are prescribed. If an antibiotic drug that is initiated for the treatment of an infection is administered without considering comorbid diseases, it will inevitably lead to undesirable outcomes.30 The ability to answer the questions on comorbid conditions and diseases (e.g., pregnancy and renal failure) and the percentages of accurate answers were higher at in Group 1. This suggests that Group 2 had forgotten the theoretical knowledge in time and they are more likely to make mistakes. This shows the importance of emphasizing the antibiotic awareness in the basic pharmacology courses.31 A new strategy to promote the use of narrow spectrum antibiotics as the first line treatment should be the goal o the current International Guidelines.32 The suggestions of the participants for promotion of the awareness of antimicrobial resistance were also of interest when planning the questionnaire. Among the suggestions that were included in our questionnaire, Group 1 defended the idea that periodic training before and after graduation; and the Group 2 defended that the issue should be brought to the agenda of written and visual media more frequently which would be more effective. We believe education of the physicians and the patients have paramount importance because behavior of the patients and their relatives are a major problem in our country. Physicians mainly prescribe the requested drugs in order to avoid verbal and physical assault in primary and secondary health care institutions. Furthermore, the education of physicians from different medical schools from different region of Turkey may be heterogenous. This may also be the reason of different responses of the subjects included in the present study.33
Limitations
Group 1 participants generally answered the questions together, they might be influenced by each other while answering and they might not have answered the questions objectively. Most of the participants in Group 2 wanted to change the answers to the questions requiring theoretical knowledge several times until the end of the questionnaire. However, the responses for both groups were recorded as accurate and objective as possible.
Conclusion
Theoretical antibiotic knowledge is better in the pre-graduation period, but due to lack of experience, the decision to start treatment is a major problem in this group. In contrast, the self-confidence of doctors is higher in the post-graduation period, but the decision to start antibiotic treatment is easily made and awareness of MDR is lower due to various reasons such as decreased theoretical knowledge, pressure from the patients and their relatives. The presence of unproven infection seems to be the most important factor that encourages doctors to start antibiotics. Sustainable training for rational antibiotic use for physicians after graduation can contribute positively to reduce of antimicrobial resistance rates and to be more conscious about the use of rational antibiotics. Further studies should be conducted with more participants.
Acknowledgments
I would like to thank Professor Yasar Bayindir and Professor Yasemin Ersoy, who contributed their valuable ideas in the evaluation stage of this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bolin S, Moennig V, Kelso Gourley NE, Ridpath J. Monoclonal antibodies with neutralizing activity segregate isolates of bovine viral diarrhea virus into groups. Brief report. Arch Virol. 1988;99(1–2):117–123. doi:10.1007/BF01311029
2. Teixeira Rodrigues A, Roque F, Falcão A, Figueiras A, Herdeiro MT. Understanding physician antibiotic prescribing behaviour: a systematic review of qualitative studies. Int J Antimicrob Agents. 2013;41(3):203–212. doi:10.1016/j.ijantimicag.2012.09.003
3. Okyay RA, Erdogan A. Self-medication practices and rational drug use habits among university students: a cross-sectional study from Kahramanmaras, Turkey. PeerJ. 2017;5(1):e3990. doi:10.7717/peerj.3990
4. Bell BG, Schellevis F, Stobberingh E, Goossens H, Pringle M. A systematic review and meta-analysis of the effects of antibiotic consumption on antibiotic resistance. BMC Infect Dis. 2014;14(1):13. doi:10.1186/1471-2334-14-13
5. Gajdács M, Albericio F. Antibiotic resistance: from the bench to patients. Antibiotics (Basel). 2019;8(3):129. doi:10.3390/antibiotics8030129
6. Gajdács M. The concept of an ideal antibiotic: implications for drug design. Molecules. 2019;24(5):892. doi:10.3390/molecules24050892
7. Wozniak TM, Barnsbee L, Lee XJ, Pacella RE. Using the best available data to estimate the cost of antimicrobial resistance: a systematic review. Antimicrob Resist Infect Control. 2019;8(1):26. doi:10.1186/s13756-019-0472-z
8. Versporten A, Bolokhovets G, Ghazaryan L, et al.; WHO/Europe-ESAC Project Group. Antibiotic use in eastern Europe: a cross-national database study in coordination with the WHO Regional Office for Europe. Lancet Infect Dis. 2014;14(5):381–387. doi:10.1016/S1473-3099(14)70071-4
9. Sarklı FD, Artantas AB, Ugurlu M. Why do patients want antibiotics and why do phycsians prescribe antibiotics?: a cross-sectional Study in Primary Health Care. Ankara Med J. 2019;(1):133–142.
10. Gualano MR, Gili R, Scaioli G, Bert F, Siliquini R. General population’s knowledge and attitudes about antibiotics: a systematic review and meta-analysis. Pharmacoepidemiol Drug Saf. 2015;24(1):2–10. doi:10.1002/pds.3716
11. Wright EP, Jain P. Survey of antibiotic knowledge amongst final year medical students. J Antimicrob Chemother. 2004;53(3):550–551. doi:10.1093/jac/dkh096
12. Aslam A, Gajdács M, Zin CS, et al. Evidence of the Practice of Self-Medication with Antibiotics among the Lay Public in Low- and Middle-Income Countries: a Scoping Review. Antibiotics (Basel). 2020;9(9):597. doi:10.3390/antibiotics9090597
13. Leekha S, Terrell CL, Edson RS. General principles of antimicrobial therapy. Mayo Clin Proc. 2011;86(2):156–167. doi:10.4065/mcp.2010.0639
14. Lukačišinová M, Fernando B, Bollenbach T. Highly parallel lab evolution reveals that epistasis can curb the evolution of antibiotic resistance. Nat Commun. 2020;11(1):1–14. doi:10.1038/s41467-020-16932-z
15. Porse A, Jahn LJ, Ellabaan MM, Sommer MO. Dominant resistance and negative epistasis can limit the co-selection of de novo resistance mutations and antibiotic resistance genes. Nat Commun. 2020;11(1):1–9. doi:10.1038/s41467-020-15080-8
16. Alothman A, Algwizani A, Alsulaiman M, Alalwan A, Binsalih S, Bosaeed M. Knowledge and attitude of physicians toward prescribing antibiotics and the risk of resistance in two reference hospitals. Infect Dis (Auckl). 2016;9:33–38. doi:10.4137/IDRT.S40047
17. Steffensen FH, Schønheyder HC, Sørensen HT. High prescribers of antibiotics among general practitioners--relation to prescribing habits of other drugs and use of microbiological diagnostics. Scand J Infect Dis. 1997;29(4):409–413. doi:10.3109/00365549709011839
18. Gajdács M, Urbán E, Stájer A, Baráth Z. Antimicrobial resistance in the context of the sustainable development goals: a brief Review. Eur J Invest Health Psychol Educ. 2021;11(1):71–82.
19. Mahmood A, Elnour AA, Ali AA, Hassan NA, Shebab A, Bhagavathula AS. Evaluation of rational use of medicines (RUM) in four government hospitals in UAE. Saudi Pharm J. 2016;24(2):189–196. doi:10.1016/j.jsps.2015.03.003
20. Andrajati R, Tilaqza A, Supardi S. Factors related to rational antibiotic prescriptions in community health centers in Depok City, Indonesia. J Infect and Public Health. 2017;10(1):41–48. doi:10.1016/j.jiph.2016.01.012
21. Troullos E, Baird L, Jayawardena S. Common cold symptoms in children: results of an Internet-based surveillance program. J Med Internet Res. 2014;16(6):e144. doi:10.2196/jmir.2868
22. Seid MA, Hussen MS. Knowledge and attitude towards antimicrobial resistance among final year undergraduate paramedical students at University of Gondar, Ethiopia. BMC Infect Dis. 2018;18(1):312. doi:10.1186/s12879-018-3199-1
23. Ayranci U, Akgun Y, Unluoglu I, Kiremitci A. Antibiotic prescribing patterns for sore throat infections in a university-based primarycare clinic. Ann Saudi Med. 2005;25(1):22–28. doi:10.5144/0256-4947.2005.22
24. Dallas A, van Driel M, Morgan S, et al. Antibiotic prescribing for sore throat: a cross-sectional analysis of the ReCEnT study exploring the habits of early-career doctors in family practice. Fam Pract. 2016;33(3):302–308. doi:10.1093/fampra/cmw014
25. O’Doherty J, Leader LFW, O’Regan A, Dunne C, Puthoopparambil SJ, O’Connor R. Over prescribing of antibiotics for acute respiratory tract infections; a qualitative study to explore Irish general practitioners’ perspectives. BMC Fam Pract. 2019;20(1):27. doi:10.1186/s12875-019-0917-8
26. Axente C, Licker M, Moldovan R, et al. Antimicrobial consumption, costs and resistance patterns: a two year prospective study in a Romanian intensive care unit. BMC Infect Dis. 2017;17(1):358. doi:10.1186/s12879-017-2440-7
27. Masoud A, Noori Hekmat S, Dehnavieh R, Haj-Akbari N, Poursheikhali A, Abdi Z. An investigation of prescription indicators and trends among general practitioners and specialists from 2005 to 2015 in Kerman, Iran. Int J Health Policy Manag. 2018;7(9):818–827. doi:10.15171/ijhpm.2018.28
28. Aslam B, Wang W, Arshad MI, et al. Antibiotic resistance: a rundown of a global crisis. Infect Drug Resist. 2018;11:1645–1658. doi:10.2147/IDR.S173867
29. Buroni S, Pollini S, Rossolini GM, Perrin E. Editorial: evolution of genetic mechanisms of antibiotic resistance. Front Genet. 2019;10:983. doi:10.3389/fgene.2019.00983
30. Llor C, Bjerrum L. Antimicrobial resistance: risk associated with antibiotic overuse and initiatives to reduce the problem. Ther Adv Drug Saf. 2014;5(6):229–241. doi:10.1177/2042098614554919
31. Pulcini C, Gyssens IC. How to educate prescribers in antimicrobial stewardship practices. Virulence. 2013;4(2):192–202. doi:10.4161/viru.23706
32. Huttner B, Saam M, Moja L, et al. How to improve antibiotic awareness campaigns: findings of a WHO global survey. BMJ Glob Health. 2019;4(3):e001239. doi:10.1136/bmjgh-2018-001239
33. Gajdács M, Szabó A. [Physicians’ opinions towards antibiotic use and resistance in the southeastern region of Hungary]. Orv Hetil. 2020;161(9):330–339. doi:10.1556/650.2019.31598
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.