Back to Journals » Clinical Optometry » Volume 13
Knowledge and Attitude of Refractive Error Among Public High School Students in Gondar City
Authors Assef NL ![]() , Tegegn MT
, Tegegn MT ![]() , Wolde SY
, Wolde SY
Received 29 May 2021
Accepted for publication 9 July 2021
Published 20 July 2021 Volume 2021:13 Pages 201—208
DOI https://doi.org/10.2147/OPTO.S322438
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Natnael Lakachew Assefa, Melkamu Temeselew Tegegn, Sara Yirgalem Wolde
Department of Optometry, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Melkamu Temeselew Tegegn
Department of Optometry, College of Medicine and Health Sciences, University of Gondar, PO Box: 196, Gondar, Ethiopia
Tel +251-9-47-30-41-25
Email [email protected]
Introduction: Refractive error (RE) is the main cause of visual impairment and blindness in the world. Lack of knowledge and unfavorable attitude of refractive error can have long-term consequences and dramatic effects in children and adults, such as loss of educational and employment opportunities, loss of economic gain for individuals, families, and societies, and impaired quality of life.
Aim: The aim of this study was to assess the level of knowledge and attitude of refractive error among public high school students in Gondar city, Northwest Ethiopia.
Methods: A school-based cross-sectional study was conducted on 390 public high school students. Those participants were selected by applying a systematic random sampling technique with an interval of 4. Data were collected using a pre-tested structured questionnaire through face-to-face interviews. The collected data were entered into Epi Info version 7.0 and exported into SPSS version 20 for analysis. Results were described using tables and text.
Results: A total of 390 study participants were included in this study with a 92.4% response rate. The overall proportion of good knowledge and a favorable attitude towards a refractive error were 53.8% and 52.1%, respectively. From the study participants, 38.7%, 41.7%, and 64.1% did not know the definition, the risk factors, and the symptoms of refractive error, respectively. Moreover, about 31.3% of the participants believed that wearing spectacle could damage their eyes, whereas 44.1% of the participants agreed with the need for spectacle correction for young people with RE.
Conclusion: The proportion of good knowledge and a favorable attitude towards refractive error among public high school students were fair. We recommended that eye care practitioners be committed to increasing the knowledge and attitude of students towards refractive error through eye health education to reduce visual impairment due to refractive error.
Keywords: refractive error, knowledge, attitude, public high school, Gondar
Introduction
Refractive error (RE) is a defect in the eye, in which refracted rays do not converge on the retina, which is classified as myopia, hyperopia, and astigmatism.1 Uncorrected RE is a major cause of visual impairment and blindness, globally. The World Health Organization has made RE correction a priority in the global initiative to eliminate avoidable blindness: Vision 2020 - the Right to Sight.2
RE affect a large proportion of the population worldwide irrespective of age, sex, and ethnic group. It is estimated that 1.4 million children are blind worldwide out of the 45 million people, such refractive errors can be easily diagnosed, measured, and corrected with spectacles and other methods to attain the normal vision.3,4 The prevalence of RE among high school students varies depending on the region, race, and ethnicity ranging from 9.6% in South Africa5 to 73.9% in Singapore.6 Furthermore, the national survey of blindness and low vision in 2005/6 showed that refractive error was the second cause of low vision in Ethiopia, which accounts for 33.4% of the total burdens of low vision.7 Uncorrected RE has the huge potential of hindering school performance which may subsequently impact on the psychological and socioeconomic activities in later life.4,8–11
Various factors are believed to be responsible for refractive errors remaining uncorrected in developing countries and it is mainly related to lack of awareness and recognition of the problem at a personal, family, community, and public health level.9 Due to impaired vision, people may not be able to complete their education, find it difficult to obtain employment, and may not be able to live a full life. However, this can easily be corrected by wearing glasses.12
Besides, in developing countries, routine eye screening and examinations are uncommon because of a lack of knowledge and limited resources. Thus, refractive errors are believed to be diagnosed late when patients are already impaired or blind.13,14 Lack of knowledge of visual impairment from refractive errors can have long-term consequences and dramatic effects in children and adults, such as a loss of educational and employment opportunities, loss of economic gain for individuals, families, and societies, and affect the quality of life.13
Lack of knowledge, stigma, and erroneous beliefs towards refractive errors has been shown to play a major role in the uptake of refractive services in different continents.15
Early detection and management of the refractive error are very much important to prevent visual impairment, blindness, and its sequela. To tackle the problem, good level of knowledge and a favorable attitude towards refractive error among students play a significant role to detect any manifestations of refractive error.16 Unfortunately in the study area, there was no school visual screening opportunity for early detection and limited access to eye care services to enhance knowledge. Moreover, there is no evidence to show the level of knowledge and attitude of refractive error in Ethiopia as well as the study area among public high school students. Therefore, this study aimed to determine the level of knowledge and attitude towards refractive error among public high school students, Gondar city, Northwest Ethiopia. Besides, this study will provide evidence that helps to design strategies to counteract the effect of refractive error in public high school students. Finally, this study will also serve as baseline information for those who want to study further for developing school-based programs and awareness enhancement towards refractive error in the future.
Methods and Materials
Study Design, Setting, and Sampling
A school-based cross-sectional study was conducted in Gondar city, Northwest Ethiopia. Gondar city is located 738 km away from Northwest of Addis Ababa, the capital city of Ethiopia, and 173 km from the capital city of Amhara regional state, Bahir Dar city.
The University of Gondar tertiary eye care and training center is the only tertiary eye care center in the city that provides comprehensive eye care service for eight zones and serves as a major referral center for 14 million people living in the Amhara region, Northwest Ethiopia. According to Gondar city educational office unpublished data in 2020, there are 11 public high schools with a total number of 10,919 students.
All public high school students (grade nine and ten) in the selected school who were available during the study period were eligible to be included in the study. However, those students who had a hearing impairment and speech problem were excluded from the study.
Sample size was determined by using a single population proportion formula with the following assumptions: (n = Sample size, Z = The Value of z statistic at 95% confidence level = 1.96, P= Proportion 50% =0.5, d– Maximum tolerable error (marginal error) 5%= 0.05). By adding a 10% non-response rate, the final estimated sample size was 422. A systematic random sampling technique was employed. To assure representativeness, 30% of schools (4 high schools with a total of 1640 students) were selected by lottery method out of the total 11 high schools. The calculated sample size was proportional allocated to the selected school and then the study participants were selected by using a systematic random sampling technique with a sampling fraction of 4 [K=1640/422=4].
(n = Sample size, Z = The Value of z statistic at 95% confidence level = 1.96, P= Proportion 50% =0.5, d– Maximum tolerable error (marginal error) 5%= 0.05). By adding a 10% non-response rate, the final estimated sample size was 422. A systematic random sampling technique was employed. To assure representativeness, 30% of schools (4 high schools with a total of 1640 students) were selected by lottery method out of the total 11 high schools. The calculated sample size was proportional allocated to the selected school and then the study participants were selected by using a systematic random sampling technique with a sampling fraction of 4 [K=1640/422=4].
Operational Definitions
Knowledge
Knowledge was assessed by asked 10 multiple-choice questions about the definition, cause, symptoms, and treatment of refractive error which carried a total of 17 points. The participant who answered correctly was scored 1 and those who answered incorrectly were scored 0. The sum score ranges from 0 to 17 points. The overall knowledge of refractive error was categorized as good or poor using the median score value as a cut point. A participant who answered the median score, and above of the knowledge-related questions had good knowledge, while those participants who answered less than or equal to the median score had poor knowledge.
Attitude
Attitude was assessed based on the three-point Likert scale using 8 questions, and the score points range from 8 to 24. A participant who answered the median score, and above of the attitude-related questions had a favorable attitude, whereas those participants who answered less than or equal to the median score had an unfavorable attitude.
Data Collection Procedures and Quality Control
Data were collected using a pre-tested, and structured questionnaire through face-to-face interviews, which contained socio-demographic data and knowledge and attitude-related questions. The questionnaire was initially prepared in English, translated into Amharic (local language) by language expertise for data collection, and re-translated to English to check the consistency in the meaning of words and concepts. Four BSc Optometrists have participated in the data collection. The questionnaire validity was checked by doing pre-tested on 5% of the total sample size before the actual data collection period and the content of the questionnaire was modified accordingly.
Data completeness and accuracy were checked by the study supervisor at the end of the collection. The reliability of data was checked by a reliability test and has a Cronbach's alpha value of 0.77.
Statistical Analysis
All the collected data were entered, coded, and cleaned to Epi Info version 7 and then exported into SPSS (Statistical Package for Social Science) version 20 for analysis. Frequency distribution and central tendency measures (mean, median) were used to summarize the descriptive part of the study. Pearson chi-squared test was conducted to determine factors associated with knowledge and attitude of refractive error. A variable with a p-value of less than 0.05 was considered statistically significant. Results were presented using tables and text as necessary.
Ethical Consideration
This study was conducted with the principle of the Declaration of Helsinki. Ethical approval was obtained from the Institutional Review Board (IRB) of the University of Gondar, College of Medicine and Health Sciences. Furthermore, a written letter of permission was obtained from the Gondar city education Office and schools’ director. Because the data were collected only by using the interviewer administered questionnaire, verbal informed consent was obtained from each of the study participants. For participants of age below 18 years, oral informed consent was taken from their parents or legal guardians and assent from themselves. The assent and verbal informed consent were approved by the University of Gondar Institutional Review board. All the study participants were informed about the purpose of the study, their right to refuse and withdraw from the study at any time. Confidentiality was also maintained through an anonymous questionnaire by excluding identifiers and using codes. Moreover, personal data was secured by storing data in a password-protected computer not used by others and the questionnaires were put in a locked cabinet.
Results
Socio-Demographic Characteristics of the Study Participants
A total of 390 study subjects were included in the study with a 92.4% response rate. Of the total study subjects, 226 (57.9%) were females. The mean age of study participants was 16 with a standard deviation of 2.0. Twenty-one (5.4%) of the respondents had a history of spectacle wear and 322 (82.6%) of study participants had no previous history of wearing spectacle in the family (see Table 1).
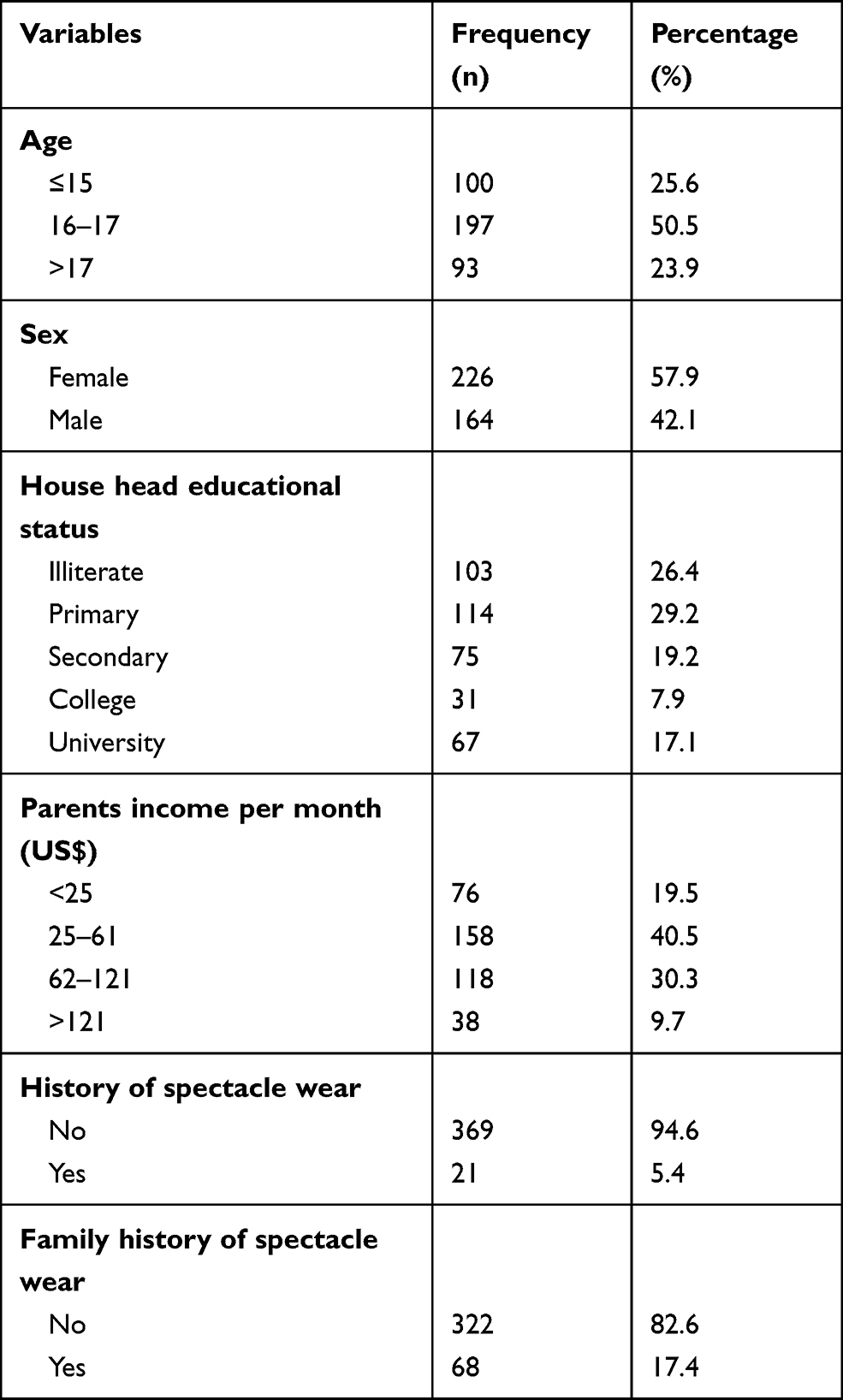 |
Table 1 Socio-Demographic Characteristics of the Study Participants in Gondar City, Northwest Ethiopia, 2020 (n=390, n= Sample Size) |
Knowledge Towards Refractive Error Among Public High School Students
Out of 390 study participants, 53.8% (95% CI: 49.2–59.0) had good knowledge of refractive error. Regarding detailed knowledge of refractive error, among the total study participants, 151 (38.7%), 250 (64.1%), and 163 (41.7%) did not know the definition, the symptoms, and the risk factors of refractive error, respectively. About 40% of the study participants believed that uncorrected RE reduces academic performance. Moreover, one hundred sixty-eight (43.1%) of participants responded that spectacle was used for the treatment of refractive error (Table 2).
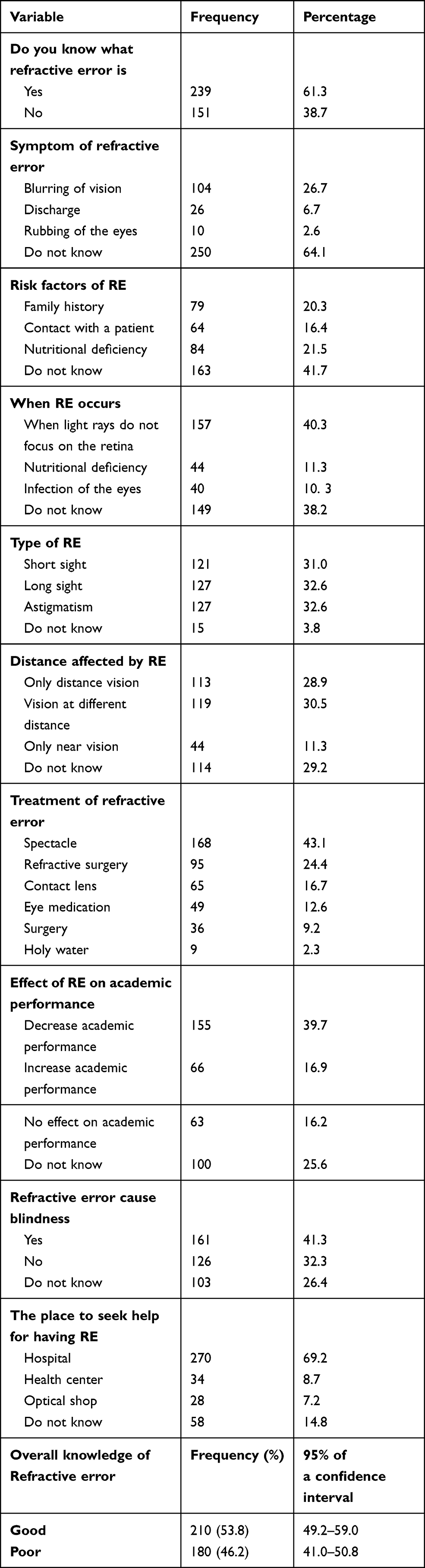 |
Table 2 Knowledge Towards Refractive Error Among Public High School Students in Gondar City, Northwest Ethiopia, 2020 (n=390, n= Sample Size) |
The Attitude of Public High School Students Towards Refractive Error
Among 390 study participants, 52.1% (95% CI: 47.4–56.9) had a favorable attitude towards refractive error. Regarding attitude towards refractive error, 157 (40.3%) participants agreed that refractive error can lead to blindness and 159 (40.8%) had a belief that wearing spectacles lead to dependency. One hundred forty two (36.4%) of the study participants agreed to the statement which states that young people who had refractive error do not need spectacle correction (Table 3).
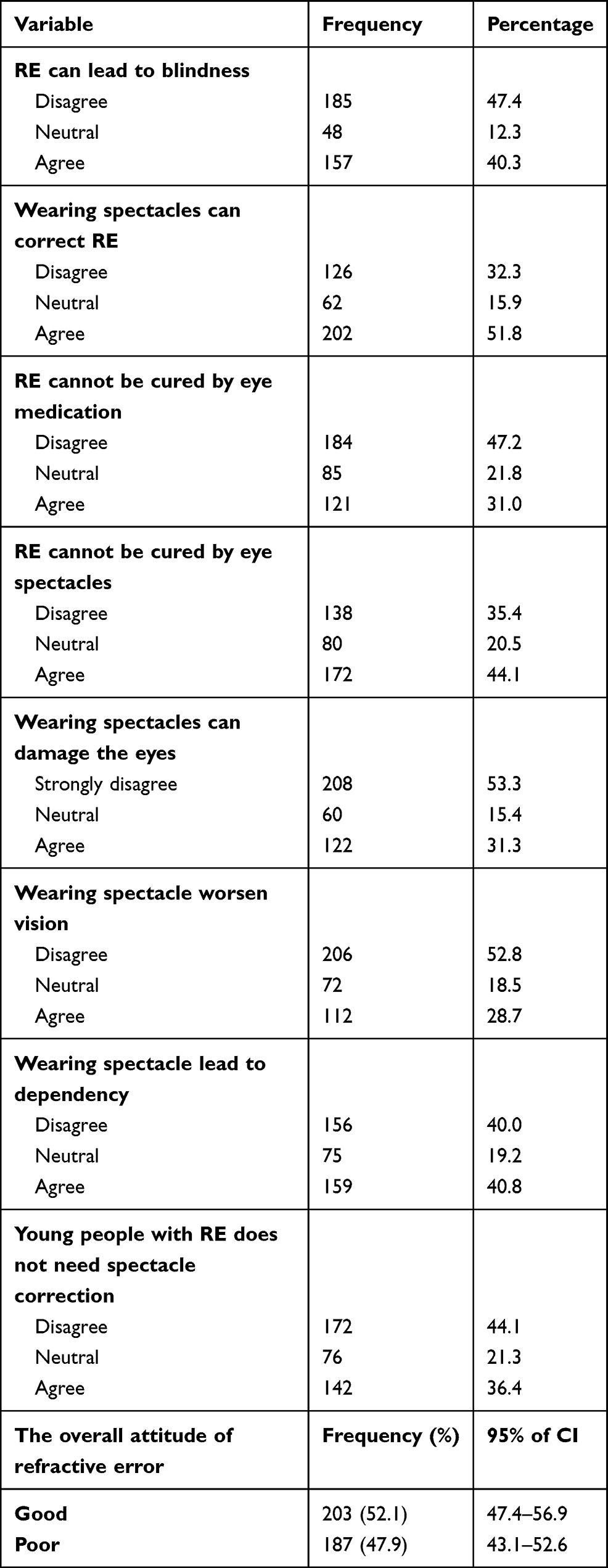 |
Table 3 Attitude Towards Refractive Error Among Public High School Students in Gondar City, Northwest Ethiopia, 2020 (n=390, n= Sample Size) |
Association of Knowledge and Attitude of Refractive Error with Socio-Demographic Characteristics of the Participants
By applying the chi-squared test, family history of spectacle wear was significantly associated with knowledge of refractive error (χ2=3.91, P-value=0.04), whereas age was significantly associated with the attitude of refractive error (χ2=8.28, P-value=0.02).On the contrary, sex, family educational status, having wearing spectacle, and parents’ monthly income were not significantly associated with knowledge and attitude of refractive error (P-value >0.05) (Table 4).
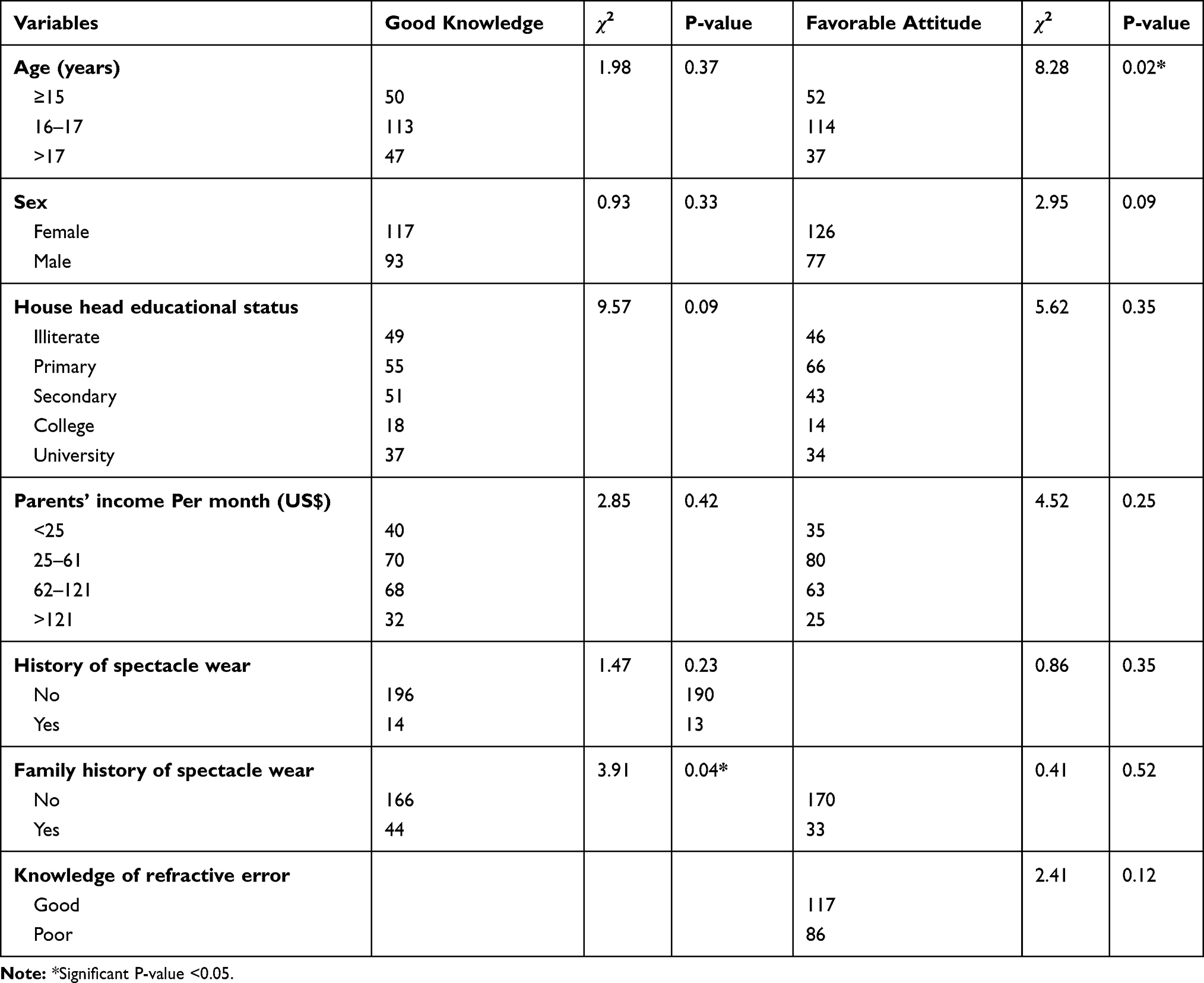 |
Table 4 Chi-Squared Test Showing the Association Between Knowledge and Attitude of Refractive Error and Socio-Demographic Characteristics Among Public High School Students, Gondar City, Northwest Ethiopia, 2020 (n=390, N=sample Size) |
Discussion
In the present study, 53.8% (95% CI: 49, 59) of participants had a good knowledge of refractive error, which is comparable with other studies done in India (56%)17 and Saudi Arabia (48.8%).18 However, the result of this study was higher than a study done in Tirupati (17%).19 This discrepancy might be due to variation in study population characteristics, sampling size, accessibility of eye care services, and utilization.
In this study, 63.1% of participants knew the definition of refractive error which was higher than the study done in Nigeria (32%).8 The possible reason for this variation might be due to variation in utilization of eye care service of study participants. For instance, only 32% of study participants heard about the refractive error during an eye examination, while 69.4% of participants of the current study showed that eye care-seeking into hospital help for refractive error services which may increase the respondents’ information about the definition of refractive error.
Regarding the types of refractive error, 31% of the study participants heard about myopia, which was lower than a study done in Saudi Arabia (82%).20 This discrepancy might be due to the difference of study subjects who were 24% myopic in the previous study that might increase the information about myopia. Moreover, about 43.1% of participants of this believed that spectacle was used to treat refractive error which is consistent with other studies done in Nigeria (38%).8 Overall, this comparison implies that eye care practitioners devoted greater efforts to provide comprehensive information about refractive error through eye health education to reduce the burden of visual impairment due to refractive error.
In the current study, 52.1% (95% CI: 47.4–56.9) of participants had a favorable attitude of refractive error. This finding is in agreement with a previous study done in Ethiopia.16 On the other hand, about 31.3% of study participants believed that wearing spectacle could damage their eyes which is consistent with other studies done in Sudan (36.4%),21 and Saudi Arabia (33.6%).22 However, the result was lower than a study done in India (64%).23 This disparity might be due to variation in the study population; the previous study was done among rural dweller students while the current study was done in urban dweller students. This finding indicated that fear of spectacles damaging the eyes should be directly addressed and the concerns should be alleviated during consultations at eye care clinics.
In this study, 40.8% of participants agreed that wearing spectacle leads to dependency. Similarly, this was comparable with the study done in Saudi Arabia (42.2%).22
Out of the total study participants, 44.1% agreed that young people with refractive errors need spectacle for correction. This result was lower than the studies done in Ethiopia (87.7%),24 Sudan (63.3%),21 and Saudi Arabia (67.7%).22 This difference might be attributable due to the difference in the study population characteristics and study setting. All study participants in Saudi Arabia were females and 40.6% were already diagnosed with a refractive error which might increase the levels of knowledge and awareness about the refractive error.
This study showed that family history of spectacle wear was significantly associated with knowledge of refractive error (χ2=3.91, P-value=0.04). The possible reason for this association is that individuals having basic information about the problem and its management, those Individuals was served as the good messenger to transfer information to the family members.
In the present study, age was significantly associated with the attitude of refractive error (χ2=8.28, P-value=0.02). A possible explanation could be that increasing age creates increased awareness about the refractive error. Since the participants were students, as their level of education increased more likely to have a refractive error, which could bring an attitudinal shift to a favorable one.
The limitation of this study is that the study is more quantitative or limited information on the qualitative parts.
Conclusion
The proportion of good knowledge and a favorable attitude of refractive error among public high school students were fair. We recommended that eye care practitioners be committed to increasing the knowledge and attitude of students towards refractive error through eye health education to reduce visual impairment due to refractive error. Moreover, a large-scale both quantitative and qualitative study was recommended to known the actual knowledge and attitude of refractive error and its hidden factors.
Data Sharing Statement
All the necessary data are included in the manuscript, and if needed, the supporting data are available upon reasonable request to the corresponding author.
Acknowledgments
We are deeply indebted to acknowledge the University of Gondar, College of Medicine and health sciences for granted ethical approval to conduct the research. We would also like to acknowledge the study participants for their cooperation and willingness during data collection.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors report no conflicts of interest for this work and have no proprietary interest in any of the materials mentioned in this article.
References
1. Resnikoff S, Pascolini D, Mariotti SP, Pokharel GP. Global magnitude of visual impairment caused by uncorrected refractive errors in 2004. Bull World Health Organ. 2008;86(1):63–70. doi:10.2471/BLT.07.041210
2. WHO. Global initiative for the elimination of the 2006–2011 avoidable blindness action plan. Geneva: Organ Mund Health; 2007. GLOBAL INI.
3. Update V. Journal of community eye health review article. Community Eye Health. 2001;14(38):19–20.
4. Murthy GVS, Gupta SK, Ellwein LB, et al. Refractive error in children in an urban population in New Delhi. Investig Ophthalmol Vis Sci. 2002;43(3):623–631.
5. Naidoo KS, Raghunandan A, Mashige KP, et al. Refractive error and visual impairment in African Children in South Africa. Invest Ophthalmol Vis Sci. 2003;44(9):3764–3770. doi:10.1167/iovs.03-0283
6. Quek TPL, Chua CG, Chong CS, et al. Prevalence of refractive errors in teenage high school students in Singapore. Ophthalmic Physiol Opt. 2004;24(1):47–55. doi:10.1046/j.1475-1313.2003.00166.x
7. Berhane Y, Worku A, Bejiga A, et al. Prevalence and causes of blindness and low vision in Ethiopia. Ethiop J Health Dev. 2007;21(3):204–210.
8. Ebeigbe JA, Kio F, Okafor LI. Attitude and beliefs of Nigerian undergraduates to spectacle wear. Ghana Med J. 2013;47(2):70–73.
9. Ayanniyi AA, Adepoju FG, Ayanniyi RO, Morgan RE. Challenges, attitudes, and practices of the spectacle wearers in a resource-limited economy. Middle East Afr J Ophthalmol. 2010;17(1):83–87. doi:10.4103/0974-9233.61223
10. Smith TST, Frick KD, Holden BA, Fricke TR, Naidoo KS. Potential lost productivity resulting from the global burden of uncorrected refractive error. Bull World Health Organ. 2009;87(6):431–437. doi:10.2471/BLT.08.055673
11. Zhu M, Tong X, Zhao R, et al. Visual impairment and spectacle coverage rate in Baoshan district, China: population-based study. BMC Public Health. 2013;13(1). doi:10.1186/1471-2458-13-311
12. Fylan F, Grunfeld EA. Visual illusions? Beliefs and behaviors of presbyope clients in optometric practice. Patient Educ Couns. 2005;56(3):291–295. doi:10.1016/j.pec.2004.03.003
13. Malla OK. Vision 2020: the right to sight. Kathmandu Univ Med J. 2004;2(1):2.
14. Spoerer P. How to Make Spectacles at Low Cost. World Health Organization;1987:200.
15. Rosman M, Wong TY, Wong W, Wong ML, Saw SM. Knowledge and beliefs associated with refractive errors and under-correction: the Singapore Malay eye study. Br J Ophthalmol. 2009;93(1):4–10. doi:10.1136/bjo.2007.132506
16. Alemayehu AM, Belete GT, Adimassu NF. Knowledge, attitude, and associated factors among primary school teachers regarding a refractive error in school children in Gondar city, Northwest Ethiopia. PLoS One. 2018;13(2):31–40. doi:10.1371/journal.pone.0191199
17. Domi N, Manoj P, Peter P, et al. A study to assess the knowledge regarding refractive errors among high school students in selected high schools Mangaluru with a view to prepare information booklet. Indian J Public Health Res Dev. 2020;11(04):219–223.
18. Alruwaili WS, Alruwaili MS, Alkuwaykibi MK. Prevalence and awareness of refractive errors among Aljouf University medical students. Egypt J Hosp Med. 2018;70(1):29–32. doi:10.12816/0042958
19. Sreelatha M, Kalavakunta Leela M, Sudha RP. A study to assess the knowledge on refractive errors and related risk factors of school children in selected government schools, Tirupati. J Nurs Health Sci. 2019;8(5):66–74.
20. Chowdhury S. Chakraborty P pratim. Universal health coverage - there is more to it than meets the eye. J Fam Med Prim Care. 2017;6(2):169–170. doi:10.4103/jfmpc.jfmpc_13_17
21. Alrasheed SH, Naidoo KS, Clarke-Farr PC. Attitudes and perceptions of Sudanese high-school students and their parents towards spectacle wear. Afr Vis Eye Health. 2018;77(1):1–7.
22. Alswailmi F, Mohamed A, Gomma S, Khalafallah H, Mohamed H. Attitude of female undergraduates towards spectacle correction of refractive errors. COJ Nurs Healthcare. 2018;4:422–426.
23. Dhoble P, Agarwal R, Patel C, Anand G, Sharma J, Sabde Y. Study to assess the psychosocial aspects of refractive errors and effectiveness of health education in correcting stigmas related to spectacle use in high-school students of rural India. Int J Med Sci Public Health. 2013;2(3):716. doi:10.5455/ijmsph.2013.060520131
24. Desalegn A, Tsegaw A, Shiferaw D, Woretaw H. Knowledge, attitude, practice and associated factors towards spectacles use among adults in Gondar town, northwest Ethiopia. BMC Ophthalmol. 2016;16(1):1–11. doi:10.1186/s12886-016-0357-3
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.