Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 14
Knowledge and Attitude Among the Saudi Dentists Towards Coronectomy of Impacted Mandibular Third Molars
Authors Raqe Alqhtani N, Mohammed AlThobaiti S, Khalid AlOwais H, Abdulrhman Alabdulkarim M, Abdullah Aldossary R, Tabassum N ![]() , AlOtaibi M, Almeslet A
, AlOtaibi M, Almeslet A
Received 1 January 2022
Accepted for publication 23 April 2022
Published 12 May 2022 Volume 2022:14 Pages 113—121
DOI https://doi.org/10.2147/CCIDE.S356754
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Nasser Raqe Alqhtani,1 Sarah Mohammed AlThobaiti,2 Hayat Khalid AlOwais,2 Muneera Abdulrhman Alabdulkarim,2 Reef Abdullah Aldossary,2 Nafeesa Tabassum,3 Mohammed AlOtaibi,4 Asma Almeslet5
1Department of Oral and Maxillofacial Surgery and Diagnostic Science, College of Dentistry, Prince Sattam Bin Abdulaziz University, Al-Kharj, Saudi Arabia; 2College of Dentistry, Riyadh Elm University, Riyadh, Saudi Arabia; 3Department of Diagnostic Sciences, College of Dentistry, Dar Al Uloom University, Riyadh, Saudi Arabia; 4Department of Oral and Maxillofacial Surgery, Prince Sultan Military Medical City, Riyadh, Saudi Arabia; 5Department of Oral Maxillofacial Surgery and Diagnostic Sciences, Riyadh Elm University, Riyadh, Saudi Arabia
Correspondence: Nasser Raqe Alqhtani, Department of Oral and Maxillofacial Surgery and Diagnostic Science, College of Dentistry, Prince Sattam Bin Abdulaziz University, Al-Kharj, Saudi Arabia, Email [email protected] Nafeesa Tabassum, Department of Diagnostic Sciences, College of Dentistry, Dar Al Uloom University, Riyadh, Saudi Arabia, Tel +966577462974, Email [email protected]
Purpose: Compared to the complete extraction of impacted third molars that are in close proximity to the mandibular canal, the coronectomy procedure is used as an alternative, owing to its minimal risk of damaging the Inferior alveolar nerve. Despite clear coronectomy concepts mentioned in the literature, the procedure is debatable. This study aimed to assess the knowledge and attitude towards the coronectomy procedure among dentists in Saudi Arabia.
Patients and Methods: The 16 close-ended questionnaire was distributed electronically to 377 dentists over the country. It included the demographic data and the options given to their patients with complicated impacted third molars, and the number of coronectomy they have performed. The retrieved data were exported and transferred to the SPSS software program for analysis. The Chi-squared and Fisher’s exact tests were used as appropriate for comparisons. A P-value < 0.05 was considered significant.
Results: Only 54 (15%) participants performed coronectomy procedure, and only 28.3% of the participants advised their patients to do coronectomy. Nearly two-thirds of the participants (71.9%) were aware of coronectomy procedures, with no significant differences (P> 0.05) between the groups. About 68.9% of the participants agreed that coronectomy aims to protect inferior alveolar nerve damage. More than 60% of participants believed that coronectomy is a reliable technique, while 40.6% of participants claimed that they were capable of deciding whether to do coronectomy or extraction. No significant differences were found between the groups concerning most of the study variables (P> 0.05).
Conclusion: Knowledge of Saudi dentists towards coronectomy is good, while their attitude is still low. More learning strategies about coronectomy should be implemented.
Keywords: coronectomy, impacted teeth, knowledge, attitude, inferior alveolar nerve damage, complicated exodontia, third molars
Introduction
Extraction of mandibular wisdom teeth is a common practice in dentistry.1–4 However, this procedure might be associated with multiple complications such as bleeding, dry socket, pain, and swelling.3,5,6 The most disturbing complication is temporary or permanent paresthesia and anesthesia of the inferior alveolar nerve (IAN).7–9 This complication is considered as an injury to the nerve, which might also accompany painful sensations related to the lower lips, including the skin covering the chin and gingiva10–12. The incidence of IAN injury when removing impacted third molars has been reported from 0.41% to 8.1% for the temporary lack of sensation and from 0.014% to 3.6% for prolonged signs and symptoms. However, with high-risk teeth, the incidence of IAN injury may raise up to 20%.13–15 To overcome the previously mentioned complications, a new surgical approach was developed decades ago known as coronectomy or partial odontectomy.16 Coronectomy is defined as the removal of the coronal part of the mandibular third molars leaving the roots untouched by positing the tooth 3 to 4 mm under the alveolar bone and always leaving the vitality of pulp tissue intact13,17–19. Panoramic and CBCT radiographs are used to evaluate the roots shape of the third molars indicated for coronectomy, their proximity to the inferior alveolar nerve, and the curvature or narrowing in the inferior mandibular canal.20,21
Although there are no signs of inferior alveolar nerve injury following coronectomy, some short-acting complications include pain, alveolitis, bleeding, swelling, and redness. However, the long-term complication mainly includes roots migration along the long axis of the tooth.16,19,22–24 Moreover, failure rates of coronectomy varied greatly in the literature, ranging from 2.3% to 38.4%.25 The direction of migration was found to be further away from the nerve towards the level of the bone, which appears to be the reason behind periodontium diseases and deep pockets. This, in turn, leads to a second surgical procedure to remove the roots, and it is considered the main disadvantage of the coronectomy19,26,27. Although coronectomy is still not evidence-based practice, it has recently gained popularity in dental practice and attracts many researchers.13,26,28–34 In a study by Crameri et al,29 conducted among maxillofacial surgeons in Switzerland to evaluate their attitudes toward this procedure, 51.6% considered coronectomy a non-reliable technique. However, 40.6% accept to propose this procedure in situations where a high risk of inferior alveolar nerve injury might happen.
Furthermore, several studies1,15,18,25–27,35–45 concluded that the complete removal of the mandibular wisdom molars has a greater risk of injuring the inferior alveolar nerve, and coronectomy procedure is considered a viable technique in managing such cases. To the best of our knowledge, no study has investigated the knowledge and attitude of Saudi dentists regarding coronectomy. This study aimed to assess the knowledge and attitudes toward the coronectomy procedure among a sample of dentists in Saudi Arabia.
Materials and Methods
This was a cross-sectional questionnaire-based study conducted among dentists in Saudi Arabia. The required sample size was calculated using an online Raosoft® sample size calculator, with a P-value of 0.05 (95% confidence interval), marginal error of 5%, and the target population was 19,622 dentists, based on the Ministry of Health statistical yearbook 2020. Thus, a total of 377 dentists were required for the study. The questionnaire was constructed based on the available literature on this topic.13,29,31 It was electronically prepared using Google forms and disseminated to the target dentists. The electronic survey consisted of 16 close-ended questions divided into three main sections. The first section was related to the demographic data, including age (≤ 30 years and > 30 years), gender (males and females), place of work (government and private), experience (< 5 years and ≥ 5 years), and specialty (general practitioner and specialist). In the second section, participants were asked about their awareness of coronectomy (coronectomy purpose, indications, surgical procedures, and complications). The third section included questions about their attitude (if the coronectomy is a reliable technique, their capability to decide to do coronectomy or extraction, their willingness to attend continuing education courses about coronectomy and using 3D imaging systems to diagnose third molar impaction). The participants were also asked if they have performed coronectomy, their satisfaction with the results, and the options given to patients with mandibular wisdom teeth in close positional relationship to the inferior alveolar nerve (IAN) and at risk of nerve damage (multiple-choice question). Data were collected in a master sheet (MS. Excel 2016), double-checked, and transferred to statistical software (SPSS v25, IBM Corp.) for further analysis. Descriptive data were tabulated and presented as frequencies and percentages. The differences between the groups were utilized using the Chi-squared test and Fisher’s exact test, as appropriate. The significance level was set at P-value < 0.05.
Results
A total of 360 responses were valid for analysis, with a response rate of 95.5%. Table 1 shows that most of the participants (88.1%) were under 30-year age group, had clinical experience of less than 5 years (87.2%), and were general practitioners (89.7%). More than half of the participants were males (51.7%), and 59.4% worked in the government sector.
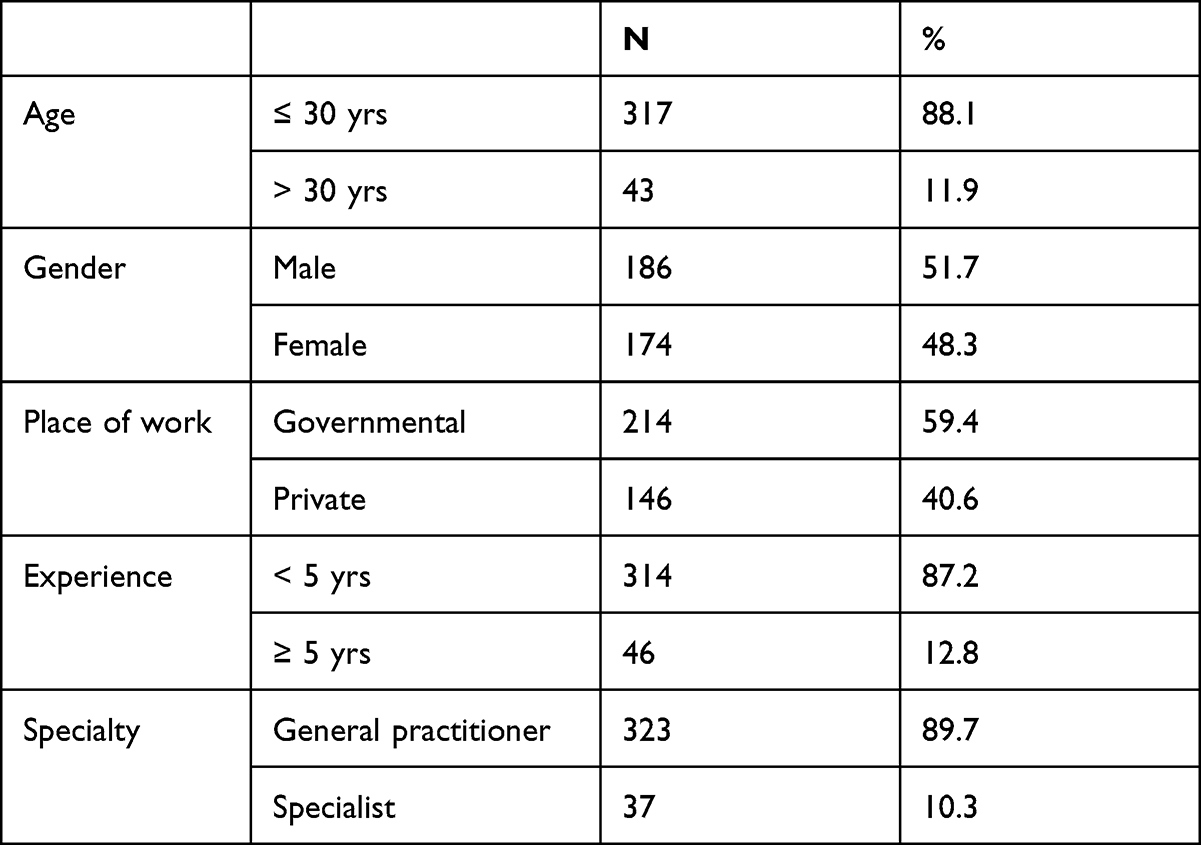 |
Table 1 Characteristics of the Study Sample |
As presented in Tables 2 and 3, nearly two-thirds of the participants (71.9%) were aware of coronectomy procedures, with no significant differences (P> 0.05) between the groups. 65.6% were aware of coronectomy indications, with no significant differences (P> 0.05) between the groups. However, less percentage (53.9%) were aware of coronectomy complications; also, with no significant differences (P> 0.05) between the groups. About two-thirds of the participants (68.9%) agreed that the purpose of coronectomy is to protect against IAN damage (Table 2) with no significant differences (P> 0.05) were found between the groups.
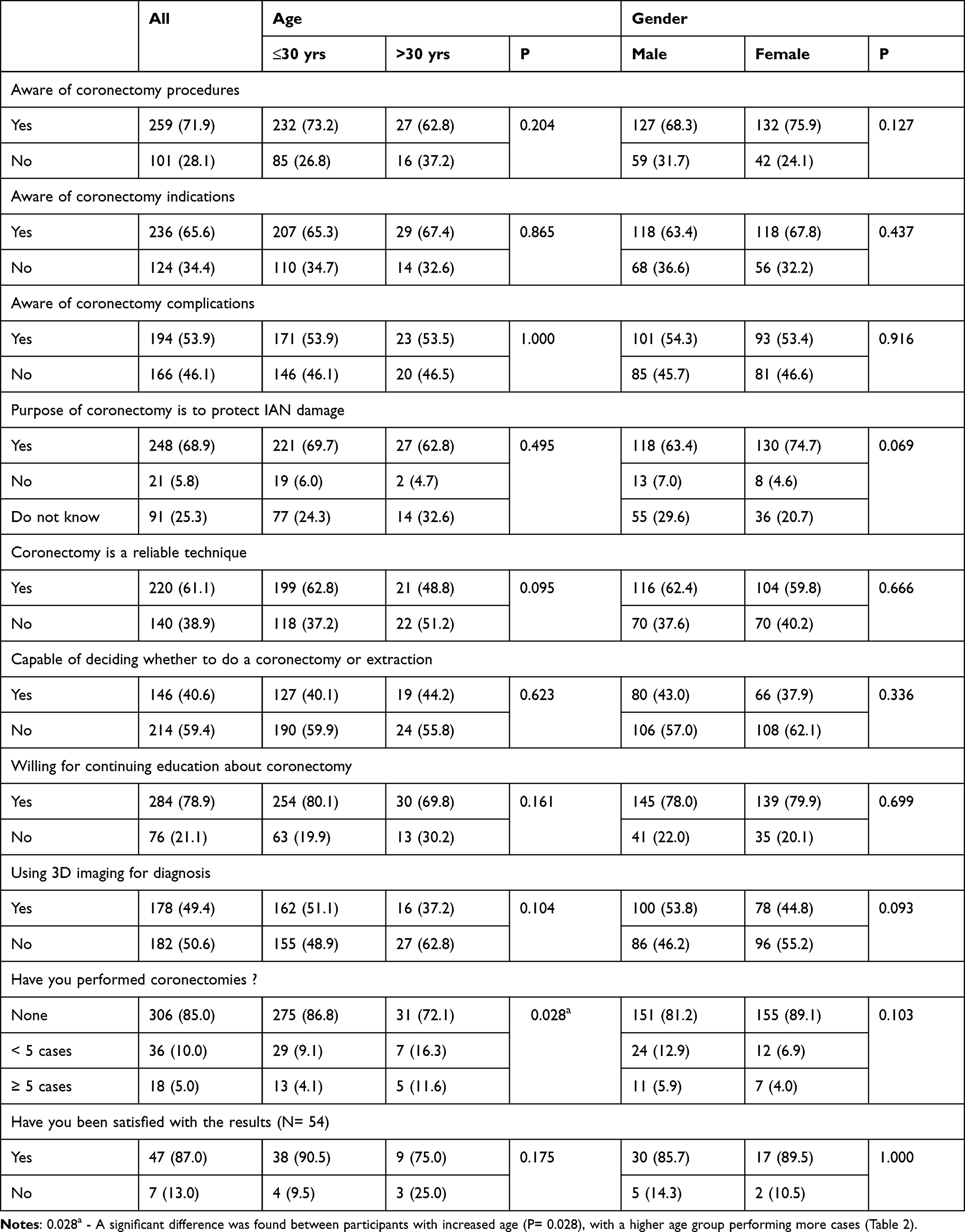 |
Table 2 Response to the Study Questions for All Participants According to the Age and Gender |
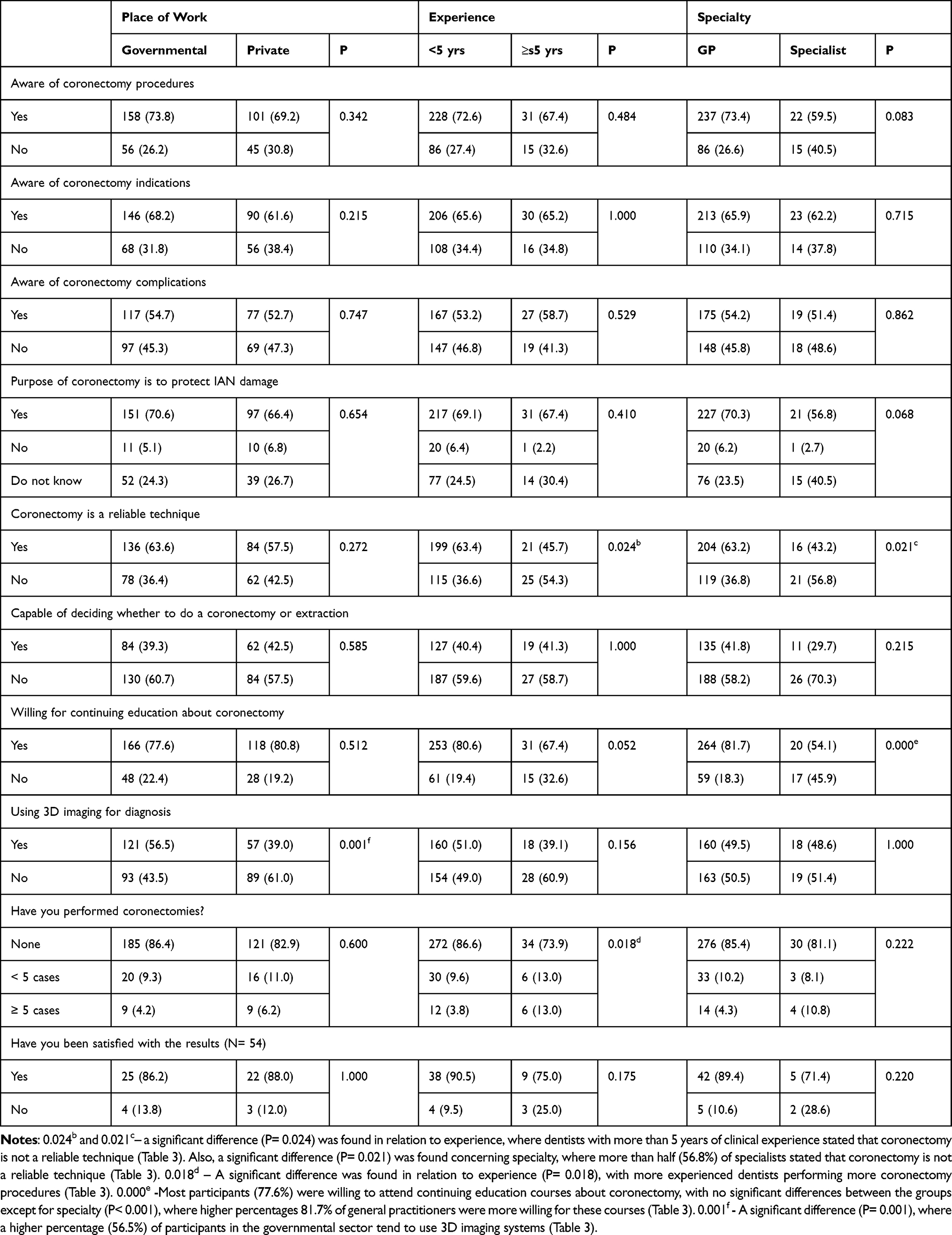 |
Table 3 Response to the Study Questions According to Place of Work, Experience, and Specialty |
More than 60% of participants believed that coronectomy is a reliable technique. No significant differences (P> 0.05) were found between the participants concerning age groups, gender, and place of work. However, a significant difference (P= 0.024) was found in relation to experience, where dentists with more than 5 years of clinical experience stated that coronectomy is not a reliable technique (Table 3). Also, a significant difference (P= 0.021) was found concerning specialty, where more than half (56.8%) of specialists stated that coronectomy is not a reliable technique (Table 3). Only 40.6% of participants claimed that they could decide whether to do coronectomy or extraction (Table 2), with no significant differences (P> 0.05) between the groups. However, most participants (77.6%) were willing to attend continuing education courses about coronectomy, with no significant differences between the groups except for specialty (P< 0.001), where higher percentages 81.7% of general practitioners were more willing for these courses (Table 3). Less than half of participants (49.4%) claimed that they used 3D imaging for third molar diagnosis (Table 2), with only a significant difference (P= 0.001) between participants concerning the place of work, where a higher percentage (56.5%) of participants in the governmental sector tend to use 3D imaging systems (Table 3).
Only 54 (15%) participants performed coronectomy, with only 5% (n= 18 participants) performing more than 5 cases (Table 2). A significant difference was found between participants with increased age (P= 0.028), with a higher age group performing more cases (Table 2). Also, a significant difference was found in relation to experience (P= 0.018), with more experienced dentists performing more coronectomy procedures (Table 3). Among dentists who performed coronectomy, most of them (86.2%) were satisfied with the results, with no significant differences (P> 0.05) between the groups.
63.6% of the dentists referred the patients having risky mandibular third molars, 28.3% opted to “Leave and wait”, 39.2% opted for “coronectomy”. Surgical removal was advised by only 11.7% participants (Figure 1).
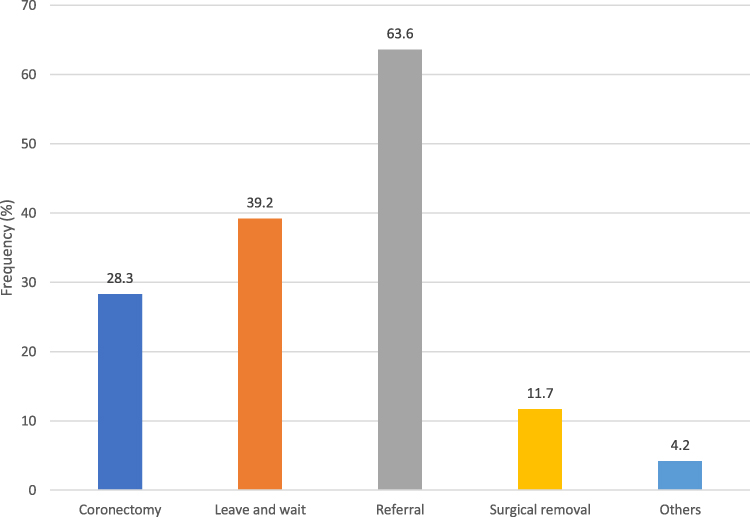 |
Figure 1 Response to the question of the options given to patients having complicated risky mandibular third molars. |
Discussion
The reported prevalence of impacted third molars in Saudi Arabia varied greatly from one region to another, ranging from 5% to 64.87%.46–50 In a study among Saudi subpopulations, Oyebunmi et al51 reported the complications associated with third molar impaction with more frequency of distal root caries of the second molar and pocket formation between the impacted tooth and the second molar. However, Alfadil and Almajed, in their study47 about the reasons for third molars extraction in Saudi Arabia, reported that the most common reason for extraction was for a prophylactic purpose (66.8%), followed by symptomatic pathology (33.2%). On the other hand, studies on coronectomy in Saudi Arabia are rare. A study by Braimah et al39 investigated the sequelae of coronectomy after one year of evaluation and noticed rapid immigration of the remaining roots in most of the study sample.
In the current study, Saudi dentists’ level of knowledge and readiness regarding the coronectomy procedure were assessed. Generally, the participants’ knowledge about coronectomy was good (71.9%). However, fewer numbers (68.9%) were aware of its main purpose. The available literature on this subject is still scarce; hence, the comparison to other studies is limited. A study done in Brazil31 found similar findings of awareness (71.8%) among professionals, and 64.10% indicated that the main benefit of the procedure is to lower the risk of IAN injury. The authors of the Brazilian study concluded that a third of the participants rejected coronectomy. Our results, however, revealed that most of the participants (61.1%) found coronectomy a reliable technique. This finding is also higher than that observed in the study by Cameri et al in Switzerland,29 in which only 42.6% indicated that coronectomy is a reliable technique. These differences might be related to the fact that our study is more recent, where coronectomy became more popular in recent years.12,15,19,28,52
About half (49.4%) of the participants would recommend 3D imaging in case of the risky positional relationship of impacted mandibular molars with IAN. This result is lower than that reported by Devine et al30 in the UK (73%) and that reported by Cameri et al29 in Switzerland (97.4%). These differences might be related to the limited access to 3D imaging systems in Saudi Arabia or the relatively high cost for the patient53,54. However, most of our participants were willing to attend continuous education courses about coronectomy, which is higher than that reported by Cameri et al29 in Switzerland (47.7%). This might be explained by the fact that the study by Cameri et al was carried among practitioners who are already aware of coronectomy. Moreover, in our study, most participants cannot decide to entirely remove the risky impacted third molars or perform a coronectomy.
In the current study, only 15% of participants performed coronectomy. This is actually a low number compared to the study by Cameri et al29 among professionals in Switzerland, where 43.8% reported that they performed at least one coronectomy procedure. These differences might be related to the fact that part of our participants was not aware of the procedure, and most of them were not specialists. However, the satisfaction with the results of the coronectomy was almost similar in both studies (87.0% in the current study vs 88.6% in the Switzerland study). The frequency of coronectomy recommended by our participants for risky impacted third molars was lower (28.3%) than that reported by Cameri et al29 in Switzerland (40.6%), Devine et al30 in the UK (73%), and Martin et al31 in Brazil (38.46%). On the other hand, Richards et al33 and Beaumont et al28 reported a wide variation in the number of coronectomies offered. These differences might be related, in part, to the lack of knowledge and attitude,31 or the lack of experience in reading the radiographic features that show possible risky involvement with the IAN.28,30,33
Even though the surgical removal of impacted third molars is a complicated procedure, Manor et al55 observed no significant difference between surgical removal compared to coronectomy groups in quality-of-life scores during the first post-operative week and no complications were reported in this period. This, in turn, makes coronectomy a better option than surgical removal. Furthermore, surgeons with better capability produce a lower prevalence of post-operative complications. For coronectomy success, the roots must be left entirely enclosed by a mucosa to prevent any localized infection56. During the clinical and radiographic evaluation, the dentist ought to contemplate the advantages and disadvantages of complete removal or coronectomy to indicate the greatest alternative for the patient57. Additionally, it is essential to enlighten the patients about the benefits and justifications for coronectomy procedure as many patients are still hesitant to agree to leave the roots.
Regardless of the indication from various studies that coronectomy is a harmless method in the long-term and involves the least injuries, even in low-risk cases of injuring the IAN, researchers are against it. In clinical facilities with the advantage of 3D imaging, it will most probably lessen the recommendation of coronectomy procedure in cases with roots demonstrating more risky signs on OPG radiograph where they are shown to be above the inferior alveolar canal.30,33 Even after the full removal of the tooth or a coronectomy procedure, sensory disruption might be noticed to the IAN, which is based on the operator and not on the radiographic method58,59. Nevertheless, the option of executing coronectomy or complete extraction of lower wisdom molar is still upon the decision made between the surgeon and the patient.60
Although the response rate in the current study was high, some limitations should be acknowledged. The study’s cross-sectional nature with only self-reported (subjective) responses is considered a limitation. Another limitation is that the questionnaire did not include radiographic images for impacted mandibular third molars, which can help explore the participants’ ability to assess the risk of impacted molars with IAN and advise complete removal or coronectomy. Therefore, future studies with a larger sample, radiographic images, and more related questions are highly recommended.
Conclusion
Within the limitation of this study, it can be concluded that the knowledge of Saudi dentists towards coronectomy is good, while their attitude is still low. The dental curriculum should include more details about coronectomy, and continuous education courses in this issue should be implemented.
Ethical Approval
The study was approved by the Institutional Review Board of Riyadh Elm University (Ref#: FUGRP/2020/149/97/98).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Agbaje JO, Heijsters G, Salem AS, et al. Coronectomy of Deeply Impacted Lower Third Molar: incidence of Outcomes and Complications after One Year Follow-Up. J Oral Maxillofacial Res. 2015;6(2):e1.
2. Cheung LK, Leung YY, Chow LK, et al. Incidence of neurosensory deficits and recovery after lower third molar surgery: a prospective clinical study of 4338 cases. Int J Oral Maxillofac Surg. 2010;39(4):320–326.
3. Céspedes-Sánchez JM, Ayuso-Montero R, Marí-Roig A, et al. The importance of a good evaluation in order to prevent oral nerve injuries: a review. Acta Odontol Scand. 2014;72(3):161–167.
4. Cunha-Cruz J, Rothen M, Spiekerman C, et al. Recommendations for third molar removal: a practice-based cohort study. Am J Public Health. 2014;104(4):735–743.
5. Bailey E, Kashbour W, Shah N, et al. Surgical techniques for the removal of mandibular wisdom teeth. Cochrane Database Sys Rev. 2020;7(7):Cd004345.
6. Ali AS, Benton JA, Yates JM. Risk of inferior alveolar nerve injury with coronectomy vs surgical extraction of mandibular third molars-A comparison of two techniques and review of the literature. J Oral Rehabil. 2018;45(3):250–257.
7. Bui CH, Seldin EB, Dodson TB. Types, frequencies, and risk factors for complications after third molar extraction. J Oral Amaxillofacial Surg. 2003;61(12):1379–1389.
8. Loescher AR, Smith KG, Robinson PP. Nerve damage and third molar removal. Dent Update. 2003;30(7):375–380, 382.
9. Kandasamy S, Rinchuse DJ, Rinchuse DJ. The wisdom behind third molar extractions. Aust Dent J. 2009;54(4):284–292.
10. Zuniga JR. Management of third molar-related nerve injuries: observe or treat? Alpha Omegan. 2009;102(2):79–84.
11. Savi A, Manfredi M, Pizzi S, et al. Inferior alveolar nerve injury related to surgery for an erupted third molar. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103(2):e7–9.
12. Chen YW, Chi LY, Lee OK. Revisit incidence of complications after impacted mandibular third molar extraction: a nationwide population-based cohort study. PLoS One. 2021;16(2):e0246625.
13. Patel V, Moore S, Sproat C. Coronectomy - oral surgery’s answer to modern day conservative dentistry. Br Dent J. 2010;209(3):111–114.
14. O’Riordan B. Uneasy lies the head that wears the crown. Br J Oral Maxillofac Surg. 1997;3(35):209.
15. Póvoa RCS, Mourão C, Geremias TC, et al. Does the Coronectomy a Feasible and Safe Procedure to Avoid the Inferior Alveolar Nerve Injury during Third Molars Extractions? A Systematic Review. Healthcare. 2021;9:6.
16. Knutsson K, Lysell L, Rohlin M. Postoperative status after partial removal of the mandibular third molar. Swed Dent J. 1989;13(1–2):15–22.
17. Frafjord R, Renton T. A review of coronectomy. Oral Surgery. 2010;3(1–2):1–7.
18. Dhanrajani P, Smith M. Coronectomy: a recognised procedure? Oral Surgery. 2018;11(4):273–281.
19. Abu-Mostafa N, AlRejaie LM, Almutairi FA, et al. Evaluation of the Outcomes of Coronectomy Procedure versus Surgical Extraction of Lower Third Molars Which Have a High Risk for Inferior Alveolar Nerve Injury: a Systematic Review. Int J Dent. 2021;2021:9161606.
20. Blaeser BF, August MA, Donoff RB, et al. Panoramic radiographic risk factors for inferior alveolar nerve injury after third molar extraction. J Oral Amaxillofacial Surg. 2003;61(4):417–421.
21. Issrani R, Prabhu N, Sghaireen M, et al. Comparison of Digital OPG and CBCT in Assessment of Risk Factors Associated with Inferior Nerve Injury during Mandibular Third Molar Surgery. Diagnostics. 2021;11:12.
22. Leung YY, Cheung LK. Safety of coronectomy versus excision of wisdom teeth: a randomized controlled trial. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108(6):821–827.
23. Dolanmaz D, Yildirim G, Isik K, et al. A preferable technique for protecting the inferior alveolar nerve: coronectomy. J Oral Maxillofacial Surg. 2009;67(6):1234–1238.
24. Patel V, Gleeson CF, Kwok J, et al. Coronectomy practice. Br j oral maxillofacial surg. 2013;51(4):347–352.
25. Cilasun U, Yildirim T, Guzeldemir E, et al. Coronectomy in patients with high risk of inferior alveolar nerve injury diagnosed by computed tomography. J Oral Amaxillofacial Surg. 2011;69(6):1557–1561.
26. Pogrel MA, Lee JS, Muff DF. Coronectomy: a technique to protect the inferior alveolar nerve. J Oral Amaxillofacial Surg. 2004;62(12):1447–1452.
27. Long H, Zhou Y, Liao L, et al. Coronectomy vs. J Dental Res. 2012;91(7):659–665.
28. Beaumont I, Richards JA, Coyle MJ, et al. Counselling by general dental practitioners for coronectomy before referral – is it always appropriate? Oral Surgery. 2021;14(2):122–126.
29. Crameri M, Kuttenberger JJ. Application and evaluation of coronectomy in Switzerland. Swiss Dental j. 2018;128(7–8):582–586.
30. Devine M, Gerrard G, Renton T. Current practice in mandibular third molar surgery. Br Assoc Oral Surgeons Membership Oral Surgery. 2017;10(1):11–19.
31. Martins LS, Sartori B, Giongo CC, et al. Perception of oral maxillofacial surgeons from Rio Grande do Sul on coronectomy. RFO UPF. 2015;20(1):75–80.
32. O’Riordan BC. Coronectomy (intentional partial odontectomy of lower third molars). Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;98(3):274–280.
33. Richards JA, Coyle MJ, Kalyanapu P, et al. Variance in interpretation of plain radiographs for the assessment of third molars for coronectomy: our solution. Br J Oral Maxillofac Surg. 2018;56(7):644.
34. Sarwar H, Mahmood-Rao S. Coronectomy; Good or Bad? Dent Update. 2015;42(9):824–826.
35. Leung YY, Cheung LK. Can coronectomy of wisdom teeth reduce the incidence of inferior dental nerve injury? Ann R Australas Coll Dent Surg. 2008;19:50–51.
36. Alves FA, Serpa MS, Delgado-Azañero W, et al. Coronectomy - An alternative approach to remove impacted teeth in oncological patients. J Clin Exp Dentistry. 2018;10(10):e992–e995.
37. Martin A, Perinetti G, Costantinides F, et al. Coronectomy as a surgical approach to impacted mandibular third molars: a systematic review. Head Face Med. 2015;11:9.
38. Geisler S. Coronectomy is an effective strategy for treating impacted third molars in close proximity to the inferior alveolar nerve. J Am Dent Assoc. 2013;144(10):1172–1173.
39. Braimah RO, Ali-Alsuliman D, Taiwo AO, et al. Coronectomy of deeply impacted mandibular third molars: socio-demographics and sequelae after one year evaluation in a Saudi Arabian Sub-population. J Oral Maxillofacial Surg. 2021;1:65.
40. Cervera-Espert J, Pérez-Martínez S, Cervera-Ballester J, et al. Coronectomy of impacted mandibular third molars: a meta-analysis and systematic review of the literature. Med Oral Patol Oral Cir Bucal. 2016;21(4):e505–513.
41. Cosola S, Kim YS, Park YM, et al. Coronectomy of Mandibular Third Molar: four Years of Follow-Up of 130 Cases. Medicina. 2020;56:12.
42. Kouwenberg AJ, Stroy LP, Rijt ED, et al. Coronectomy of the mandibular third molar: respect for the inferior alveolar nerve. J Cranio-Maxillo-Facial Surg. 2016;44(5):616–621.
43. Pogrel MA. Coronectomy to prevent damage to the inferior alveolar nerve. Alpha Omegan. 2009;102(2):61–67.
44. Monaco G, de Santis G, Gatto MR, et al. Coronectomy: a surgical option for impacted third molars in close proximity to the inferior alveolar nerve. J Am Dent Assoc. 2012;143(4):363–369.
45. Kang F, Xue Z, Zhou X, et al. Coronectomy: a Useful Approach in Minimizing Nerve Injury Compared with Traditional Extraction of Deeply Impacted Mandibular Third Molars. J Oral Maxillofacial Surg. 2019;77(11):
46. Al-Dajani M, Abouonq AO, Almohammadi TA, et al. A Cohort Study of the Patterns of Third Molar Impaction in Panoramic Radiographs in Saudi Population. Open Dent J. 2017;11:648–660.
47. Alfadil L, Almajed E. Prevalence of impacted third molars and the reason for extraction in Saudi Arabia. Saudi Dental j. 2020;32(5):262–268.
48. Hassan AH. Pattern of third molar impaction in a Saudi population. Clin Cosmet Investig Dent. 2010;2:109–113.
49. Alfergani SM, Latif K, Alanazi YM. Pattern of impacted mandibular third molars in a Saudi population. Pak Oral Dental J. 2017;37(3):407–410.
50. Syed KB, Zaheer KB, Ibrahim M, et al. Prevalence of Impacted Molar Teeth among Saudi Population in Asir Region, Saudi Arabia - A Retrospective Study of 3 Years. J Int Oral Health. 2013;5(1):43–47.
51. Oyebunmi BR, Ali-Alsuliman D, Alsalah Y, et al. Complications associated with the occurrence of impacted mandibular third molars in Saudi Arabian sub-population: najran province experience. Am J Biomed Sci Res. 2019;1:54.
52. Ouassime K, Rachid A, Amine K, et al. The wisdom behind the third molars removal: a prospective study of 106 cases. Ann Med Surg. 2021;68:102639.
53. Zain-Alabdeen E, El Khateeb S. Comparison of knowledge and perspectives toward cone-beam computed tomography among dentists in three Middle East regions: a cross-sectional study. Saudi J Oral Sci. 2018;5(1):3–10.
54. Aljuhani A, Dutta S, Mandorah A. Evaluation of Knowledge and Perspective of Endodontic Residents and General Dentist Towards the Endodontic Application of CBCT in Saudi Arabia. J Res Med Dent Sci. 2020;8(7):459–464.
55. Manor Y, Bader A, Chaushu G, et al. How Patients Percept Their Recovery Following Impacted Mandibular Third Molar Coronectomy. J Craniofac Surg. 2016;27(3):671–674.
56. Nishimoto RN, Moshman AT, Dodson TB, et al. Why Is Mandibular Third Molar Coronectomy Successful Without Concurrent Root Canal Treatment? J Oral Amaxillofacial Surg. 2020;78(11):1886–1891.
57. Gleeson CF, Patel V, Kwok J, et al. Coronectomy practice. Paper 1. Technique and troubleshooting. Br j oral maxillofacial surg. 2012;50(8):739–744.
58. Matzen LH, Christensen J, Hintze H, et al. Influence of cone beam CT on treatment plan before surgical intervention of mandibular third molars and impact of radiographic factors on deciding on coronectomy vs surgical removal. Dentomaxillofac Radiol. 2013;42(1):98870341.
59. Matzen LH, Villefrance JS, Nørholt SE, et al. Cone beam CT and treatment decision of mandibular third molars: removal vs. Dentomaxillofac Radiol. 2020;49(3):20190250.
60. Leung YY, Cheung LK. Long-term morbidities of coronectomy on lower third molar. Oral Surg Oral Med Oral Pathol Oral Radiol. 2016;121(1):5–11.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.