Back to Journals » Advances in Medical Education and Practice » Volume 17
Knowledge Acquisition, Self-Assessed Competence, and Simulator-Based Performance in a Structured Laparoscopic VR Curriculum for Obstetrics and Gynecology Residents: A Single-Center Observational Study
Authors Sierant A ![]() , Bijok J, Pirozynski M
, Bijok J, Pirozynski M
Received 28 April 2026
Accepted for publication 8 July 2026
Published 10 July 2026 Volume 2026:17 618836
DOI https://doi.org/10.2147/AMEP.S618836
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Antoni Sierant, Julia Bijok, Michal Pirozynski
Centre for Endoscopy Simulation, Centre of Postgraduate Medical Education, Warsaw, Poland
Correspondence: Antoni Sierant, Centre for Endoscopy Simulation, Centre of Postgraduate Medical Education, Marymoncka 99/103, Warsaw, 01-813, Poland, Tel +48 609170302, Email [email protected]
Introduction: Simulation enables safe, structured practice of laparoscopic skills outside the operating room, yet objective, threshold-referenced performance data from mandatory postgraduate curricula in Central and Eastern Europe remain scarce. We report the educational outcomes of a structured, multi-level virtual-reality (VR) laparoscopy curriculum delivered at a single national simulation center.
Methods: We conducted a single-center prospective observational study of 29 obstetrics and gynecology residents who completed a four-module laparoscopic course (Basic 1– 2, Advanced 1– 2) at the Centre for Endoscopy Simulation, Centre of Postgraduate Medical Education (CMKP), Warsaw. Outcomes comprised pre- and post-course single-choice knowledge tests, self-assessed competence, satisfaction, and simulator-based performance evaluated against a priori, criterion-referenced passing thresholds. Technical metrics were simulator-generated (Simbionix LAP Mentor); no human global rating scales were used. Demographic and training-related variables (gender, residency year, training-center referral level, prior endoscopic experience) were analyzed with non-parametric statistics.
Results: Knowledge scores improved from 20.9 (SD = 2.70) to 29.2 (SD = 1.01) (Wilcoxon, p < 0.05). Self-assessed competence increased significantly across all domains (p < 0.05). Satisfaction was uniformly high (mean 4.7/5, SD = 0.45) but did not correlate with objective performance (all p > 0.05). Outcomes did not differ by gender or training-center referral level; residency year was associated with performance only in colpotomy (ρ = – 0.37, p =0.047), and prior experience predicted performance mainly in basic camera manipulation (e.g. 30° navigation distance, ρ = – 0.50, p =0.005), consistent with a learning-curve effect.
Conclusion: A structured, multi-modular VR laparoscopy course significantly improved theoretical knowledge and self-assessed competence among OB-GYN residents. Within this single-center cohort, measured outcomes did not differ by gender or training-center referral level. High satisfaction diverged from objective performance, underscoring the need for balanced, criterion-referenced evaluation. A priori passing thresholds enabled transparent, proficiency-oriented assessment.
Keywords: laparoscopy/education, gynecology/education, simulation/training, clinical competence
Introduction
Minimally invasive surgery has transformed gynecological practice by reducing postoperative pain, length of hospital stay, and recovery time. However, these benefits come at the cost of a steep learning curve: laparoscopic surgery requires advanced visuospatial, psychomotor, and cognitive skills that are difficult to acquire in traditional apprenticeship models. Concerns about patient safety, variability of training opportunities, and limited operative exposure during residency have created strong impetus for structured alternatives to operating room learning.
Simulation-based training has emerged as one of the most effective innovations to address these challenges. Modern platforms—including physical box trainers, virtual reality (VR), and augmented reality systems—provide risk-free environments where learners can practice technical tasks repeatedly, receive structured feedback, and develop competence in a stepwise fashion.1,2 Systematic reviews and meta-analyses consistently confirm that simulation improves technical performance, accelerates learning curves, and reduces intraoperative errors.2–5 Importantly, simulation-trained surgeons demonstrate improved efficiency and safety in the operating room, supporting the transferability of skills to clinical practice.6,7
Despite strong evidence for its effectiveness, simulation has not been universally implemented. Surveys highlight an implementation gap, with many institutions possessing simulators but lacking structured, mandatory programs.8 As a result, objective, threshold-referenced performance data from mandatory postgraduate laparoscopy curricula remain limited, particularly in Central and Eastern Europe, where structured simulation has historically been less embedded than traditional apprenticeship. Recent innovations—such as telesimulation, asynchronous feedback systems, and low-cost portable platforms—have demonstrated that simulation can be scaled across countries and resource settings, including low- and middle-income countries.9–12
Several structured curricula and proficiency frameworks have been developed to standardize laparoscopic training and assessment. The Fundamentals of Laparoscopic Surgery (FLS) program provides a validated, proficiency-based curriculum and certification standard for core laparoscopic skills.13 In gynecology specifically, the European Society for Gynaecological Endoscopy and the European Academy of Gynaecological Surgery have established the GESEA program (eg., the LASTT and SUTT modules) for structured skill acquisition and certification.14 These frameworks share an emphasis on proficiency-based progression, in which trainees must reach predefined performance criteria before advancing, rather than completing a fixed time or number of repetitions.4,15,16 The curriculum evaluated here adopts the same proficiency-based logic through criterion-referenced passing thresholds, while differing in its delivery as a mandatory, multi-level national course within a postgraduate OB-GYN program.
Scientific societies and professional organizations have recognized simulation as a cornerstone of modern surgical education. International calls now advocate for its integration at all stages of training, standardization of curricula, and accreditation of programs.9,10,17 Recommendations include embedding simulation in residency curricula, ensuring funding and institutional support, promoting low-cost scalable solutions, and establishing quality standards for training and certification.
Against this background, the present study evaluates the educational impact of a structured, multi-level VR laparoscopy course delivered at a single national training center. We assessed four complementary domains chosen to span the lower levels of the Kirkpatrick framework and established validity dimensions: learner satisfaction (reaction/face validity), knowledge acquisition (learning/content validity), self-assessed competence (self-efficacy), and simulator-based technical performance (objective construct validity). We additionally explored the influence of demographic and training-related factors and examined the feasibility of transparent, criterion-referenced assessment using a priori passing thresholds. The present objective performance data complement our previously reported survey of residents’ subjective perceptions of the same training program.18
Methods
Study Design and Participants
This single-center prospective observational study was conducted between November 2019 and March 2021 at the Centre for Endoscopy Simulation, Centre of Postgraduate Medical Education (Warsaw, Poland). Twenty-nine obstetrics and gynecology residents at various stages of training participated. Eligibility required ongoing residency training and submission of an online application to the course, which was offered within the CMKP national project (see Ethics statement). Participation was voluntary; the cohort was therefore self-selected, a point considered in the Limitations. Participant demographics and training-related characteristics are presented in Table 1.
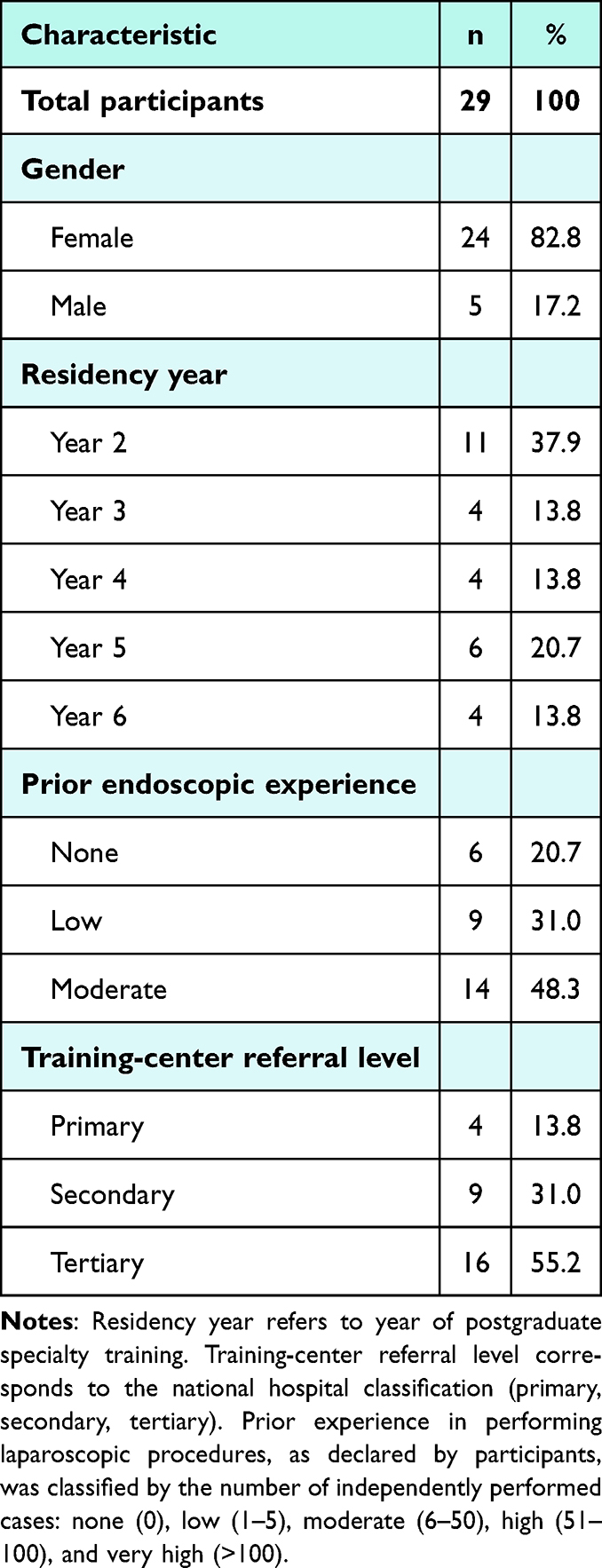 |
Table 1 Participant Characteristics |
Ethics Statement
Data were collected as part of the project conducted by the Centre of Postgraduate Medical Education (CMKP), titled “Development of specialty training of physicians in fields relevant to the epidemiological and demographic needs of the country, using endoscopic simulation techniques”. The study was approved by the Bioethics Committee of the Centre of Postgraduate Medical Education (approval No. 102/PB/2019). The study was conducted in accordance with the Declaration of Helsinki and with applicable institutional and national ethical standards. It involved secondary analysis of fully anonymized educational data, with no clinical intervention or access to identifiable personal information. All participants had previously provided written informed consent to participate in the project, including consent for the use of their anonymized evaluation data for research purposes.
Course Structure
The training program consisted of four progressive modules, designed to build skills from basic manual tasks to advanced surgical procedures and team-based training:
- Basic 1: fundamental laparoscopic skills, including camera manipulation with 0° and 30° optics, peg transfer, shape cutting, and electrocautery.
- Basic 2: applied basics and simple clinical procedures, such as anatomy table exercises, ultrasound-based diagnostic training, navigation tasks, laparoscopic tubal occlusion, and ectopic pregnancy surgery on virtual reality simulators.
- Advanced 1: laparoscopic suturing techniques, including needle positioning, continuous sutures, simple and surgical knots, and the C-loop technique.
- Advanced 2: advanced procedures and team training, covering laparoscopic hysterectomy, multidisciplinary exercises using the LAP Express system, VR operating room scenarios, and emergency simulations (eg., resuscitation protocols).
Each module was delivered as a one-day course (8 hours) with a maximum of six participants under the supervision of a multidisciplinary faculty consisting of gynecologist, simulation experts, and emergency medicine instructors. The overall structure and progression of modules are summarized in Table 2, outlining the key practical exercises, lecture topics, and assessment components included at each course level. Figure 1 illustrates representative virtual reality exercises included in the curriculum, such as laparoscopic hysterectomy. Training methods included multimedia lectures, box trainers (Karl Storz), high-fidelity laparoscopic VR simulators (Simbionix LAP Mentor), ultrasound simulators (Simbionix U/S Mentor), and anatomical tables.
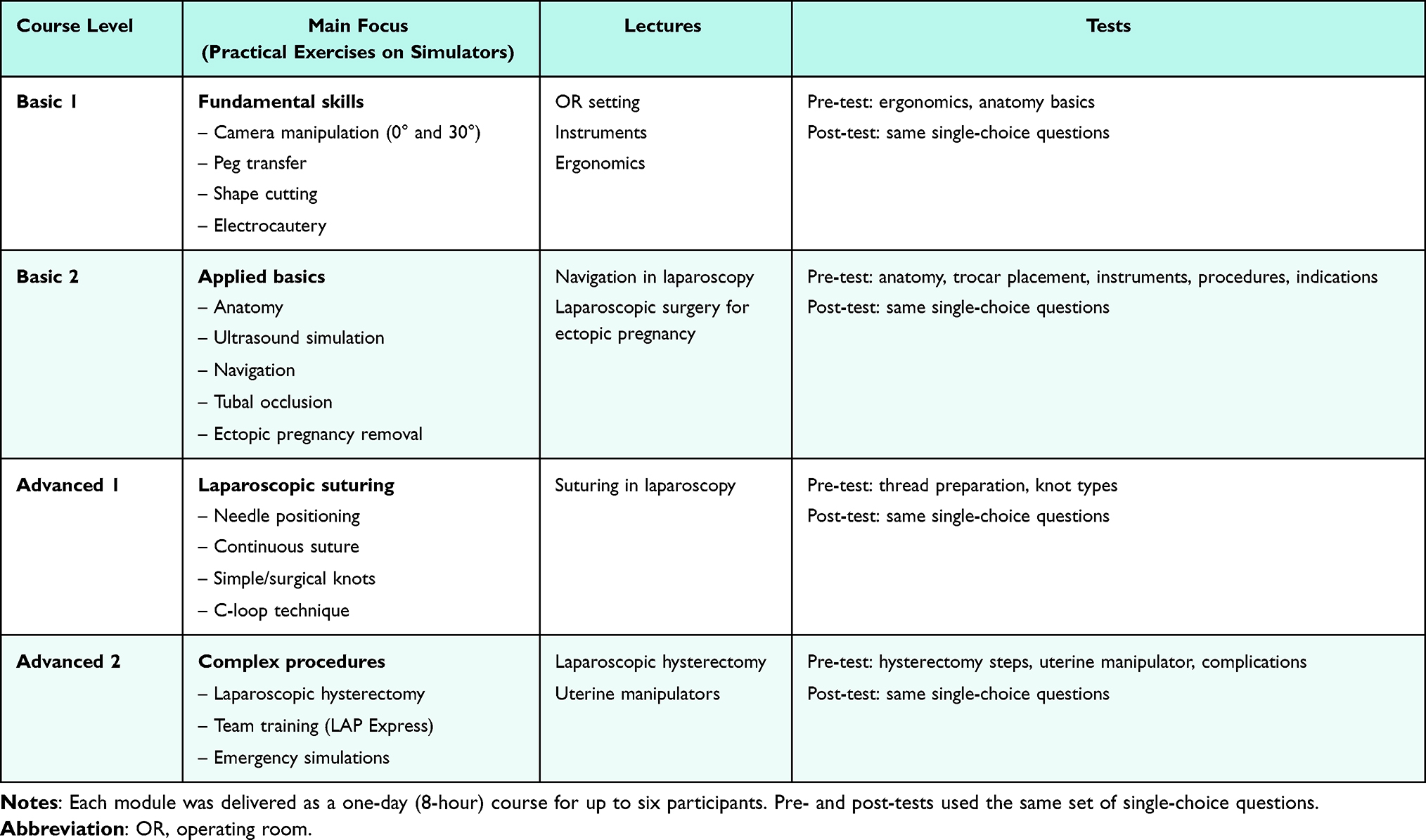 |
Table 2 Training Pathway in the Gynecological Laparoscopy Course |
 |
Figure 1 Example of laparoscopic training tasks used in the simulation curriculum, including camera navigation (0° and 30° optics), peg transfer, precision cutting, electrocautery, and procedural modules (ectopic pregnancy surgery, suturing, and hysterectomy). |
Assessment Tools
Assessment comprised four complementary components, mapped to the validity domains defined above.
- Knowledge acquisition was measured with a single-choice pre-test and post-test covering principles of laparoscopy, ergonomics, anatomy, and perioperative management. The test items were developed by the authors, who are experts in minimally invasive gynecologic surgery, to assess the fundamentals of minimally invasive surgery and to establish each resident’s baseline level. The instrument was author-developed for institutional educational evaluation and was not formally piloted or externally validated prior to this cohort.
- Satisfaction (face validity) was assessed with a Likert-scale survey (“To what extent did the training meet your expectations?”).
- Technical performance (construct validity) was evaluated exclusively using metrics generated automatically by the VR simulator (Simbionix LAP Mentor) — including task time, distance travelled, accuracy, errors, and task completion — across exercises spanning camera manipulation, peg transfer, electrocautery, ectopic pregnancy removal, laparoscopic suturing, and colpotomy. No human expert global rating scales (eg., GOALS, OSATS) were applied; consequently, inter-rater reliability is not applicable to this assessment.
- Self-assessment of skills was collected through a structured post-course questionnaire covering six domains: knowledge of principles, anatomical knowledge, practical skills, patient preparation, theoretical understanding of techniques, and manual preparation.
- Demographic and training-related factors (gender, residency year, training-center referral level, and prior endoscopic experience) were explored as potential moderators of these outcomes, in order to (i) examine whether a standardized curriculum yields comparable outcomes irrespective of trainee background and (ii) assess construct validity by testing whether simulator metrics discriminate according to prior experience.
Passing Thresholds
Technical performance was judged against criterion-referenced passing thresholds defined a priori by the expert faculty for each exercise and metric (Table 3). Trainees repeated each task until the corresponding threshold was met. During practice, guidance was provided as immediate, task-oriented feedback; structured debriefing was not used, in keeping with the focus on technical-skills acquisition, where feedback is the appropriate instructional modality, as distinct from the scenario- and team-based debriefing characteristic of crisis-resource-management simulation.19–21
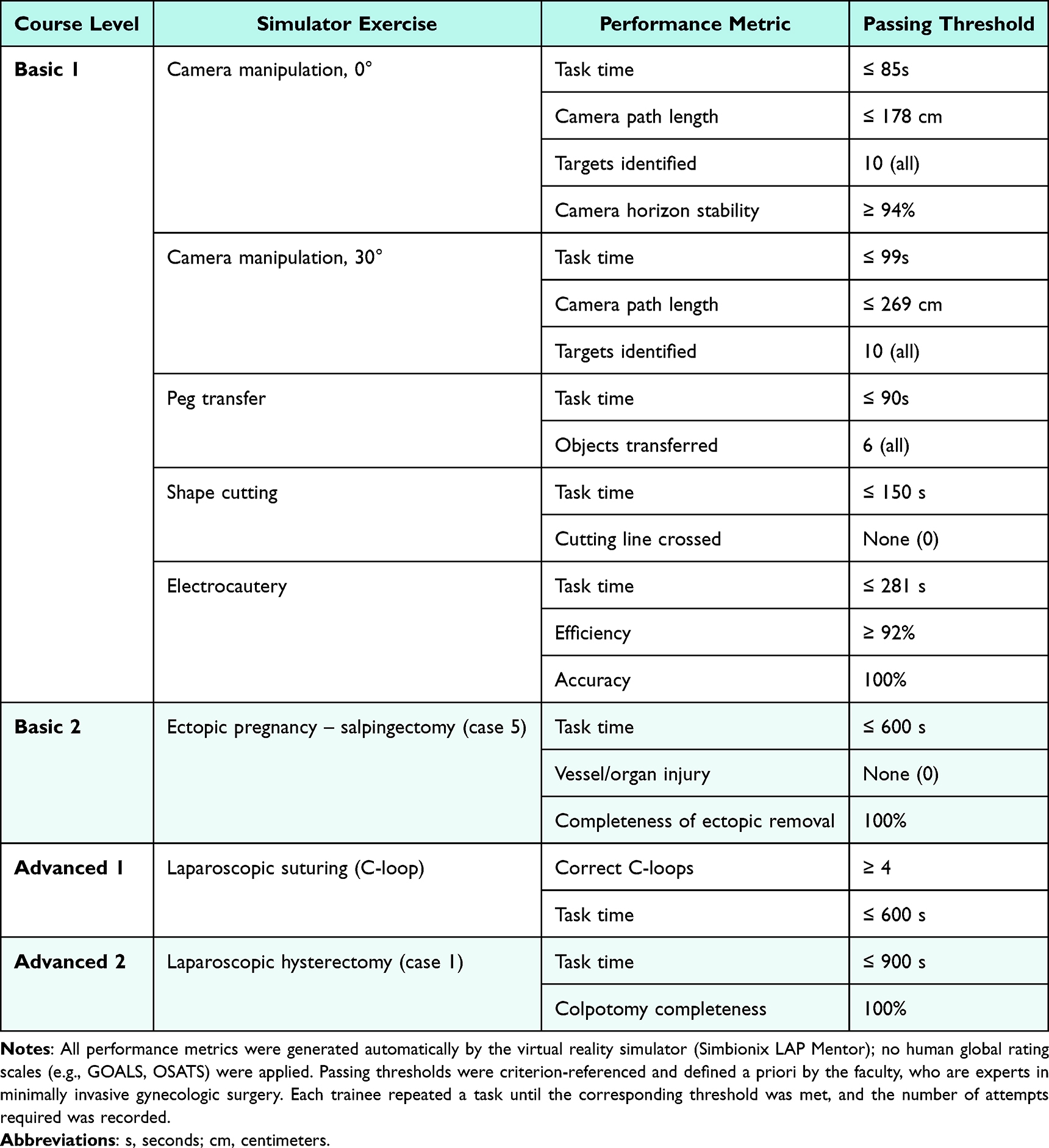 |
Table 3 Proficiency-Based Passing Thresholds Applied to the Simulator Exercises |
Statistical Analysis
Data were analyzed using non-parametric tests due to the small sample size and non-normal distribution of variables. Between-group comparisons were performed using the Mann–Whitney U-test. Correlations with residency year, prior experience, and training center referral level (primary, secondary, tertiary) were examined using Spearman’s rho. Pre- and post-test as well as pre- and post-course self-assessment scores were compared using the Wilcoxon signed-rank test. The level of significance was set at p <0.05. Given the sample size, all analyses were exploratory and hypothesis-generating; no multivariable modelling was performed.
Results
Knowledge Gain
Theoretical knowledge significantly improved after the course. Mean test scores increased from 20.9 (SD = 2.70) in the pre-test to 29.2 (SD = 1.01) in the post-test, representing a significant gain (Wilcoxon test, W = 0, p <0.05). When analyzed by subgroups, improvements were consistent. There were no significant differences in knowledge gains by gender, residency year, center referral level, or prior endoscopic experience (all p >0.05). Overall, the results confirm that the simulation-based curriculum produced a substantial and broadly distributed knowledge gain, reinforcing its effectiveness in delivering theoretical content.
Satisfaction (Face Validity)
Participants rated the course very highly, with a mean satisfaction score of 4.7 out of 5 (SD = 0.45). The training was consistently perceived as meeting expectations across all participant groups. No significant differences were observed when comparing responses by gender (U = 65.50, p =0.709), residency year (ρ = –0.17, p =0.376), or center referral level. Similarly, prior endoscopic experience did not influence satisfaction (ρ = –0.18, p =0.359). Descriptive analyses indicated uniformly high evaluations: female participants (n = 24) reported a mean score of 4.71 (SD = 0.46), while male participants (n = 5) reported 4.80 (SD = 0.45). Satisfaction scores across residency years ranged from 4.33 (SD = 0.52) in year 5 to 5.00 (SD = 0.00) in year 6, without statistical significance. With respect to prior endoscopic experience, mean satisfaction scores were 4.83 (SD = 0.41) for those without experience, 4.78 (SD = 0.44) for those with low experience, and 4.64 (SD = 0.50) for those with moderate experience. Overall, these findings confirm the face validity of the program.
Demographics and Exercise Outcomes
Analyses showed that gender and center referral level did not significantly influence exercise performance. No differences were observed between male and female participants across any of the assessed tasks (all p >0.05). Similarly, no significant associations were found between center referral level and performance metrics. Residency year showed an effect only in colpotomy: participants in higher years completed the procedure in shorter times (ρ = –0.37, p =0.047). For all other exercises, no significant associations with residency year were identified.
Prior endoscopic experience had a partial influence on technical performance. Residents with greater experience demonstrated better results in selected tasks, particularly camera manipulation (0° and 30°) and distance travelled during 30° camera navigation (ρ = –0.50, p =0.005). However, experience did not significantly affect outcomes in more complex tasks such as peg transfer, electrocautery, ectopic pregnancy surgery, or colpotomy completion.In summary, while demographic variables such as gender and center referral level showed no effect, residency year influenced performance in colpotomy only, and prior experience improved selected basic tasks but not advanced exercises.
Self-Assessed Skills
Participants reported significant improvements in all domains of self-assessed competence following the course. Median scores increased across knowledge of endoscopic principles, anatomical knowledge, practical endoscopic skills, patient preparation, theoretical knowledge of techniques, and manual preparation. In each domain, the Wilcoxon test confirmed statistically significant gains (all W = 0, p <0.05). For example, mean scores in knowledge of endoscopic principles rose from 2.48 (SD = 0.78) before the course to 4.41 (SD = 0.50) afterwards, while manual preparation increased from 2.45 (SD = 0.87) to 4.34 (SD = 0.55). Similar patterns were observed across all other domains, with consistent shifts from moderate pre-course ratings to high post-course ratings. Subgroup analyses revealed no significant differences in self-assessed improvement by gender or center referral level. Some isolated differences emerged for residency year and prior experience, but these did not alter the overall trend of marked skill enhancement across the cohort.
Course Satisfaction and Skill Performance
Correlation analyses revealed no significant associations between participants’ satisfaction ratings and their objective performance in simulation exercises. Across all measured tasks—including camera manipulation (0° and 30°), peg transfer, shape cutting, electrocautery, ectopic pregnancy surgery, suturing, and colpotomy—satisfaction scores did not correlate with time, accuracy, or error metrics (all p >0.05). Descriptive data confirmed this pattern: despite uniformly high satisfaction (mean 4.7/5), participants varied widely in technical performance. For example, satisfaction did not predict faster times in basic camera navigation nor higher accuracy in advanced procedures such as colpotomy or ectopic pregnancy removal. These results suggest that while residents valued the course structure and delivery, subjective satisfaction did not align with objective measures of skill acquisition.
Experience and Construct Validity
Declared endoscopic experience showed partial, task-specific associations with performance. Stronger experience correlated with improved camera navigation metrics—most notably shorter distance travelled in 30° camera manipulation (ρ = –0.50, p =0.005), with similar trends for 0° navigation (near-significant). In contrast, no significant differences by experience were detected for peg transfer, shape cutting, electrocautery, ectopic pregnancy surgery, or colpotomy completion metrics. These results indicate partial construct validity: the simulator can distinguish experience levels in foundational visuomotor tasks (camera work), but advanced or composite tasks appear less sensitive to prior exposure—suggesting a levelling effect of the standardized simulation protocol. Importantly, even residents with substantial prior clinical experience required initial familiarization, indicating a learning curve effect inherent to simulator-based training. However, experienced participants tended to reach the established passing criteria more quickly, consistent with accelerated progression along the simulator learning curve. A summary of key educational outcomes, including knowledge gains, self-assessed competence, satisfaction, and simulator-based performance, is provided in Table 4.
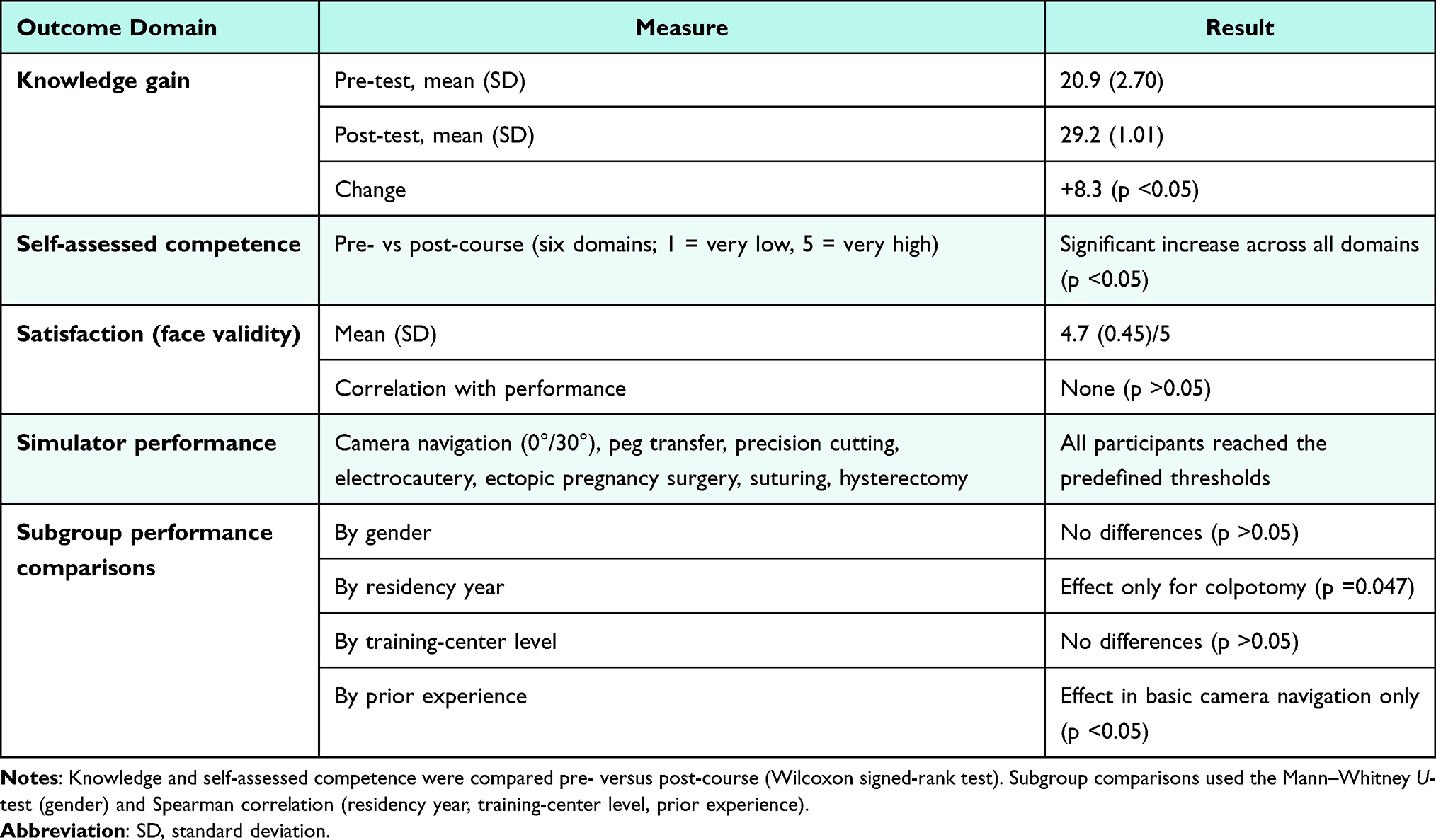 |
Table 4 Summary of Outcomes in Simulation-Based Training (N = 29) |
Discussion
Main Findings
This study demonstrates that a structured simulation-based course in gynecological laparoscopy was highly acceptable, produced significant pre–post gains in theoretical knowledge, and enhanced self-assessed competence across multiple domains. Objective performance outcomes were largely independent of gender and training center referral level, with residency year associated only in colpotomy performance and prior laparoscopic experience affecting primarily basic visuospatial tasks (camera manipulation). The use of standardized passing thresholds provided a transparent, criterion-referenced evaluation aligned with the philosophy of proficiency-based learning.
Effectiveness and Skill Acquisition
Our results are consistent with robust evidence demonstrating the effectiveness of simulation-based training. Multiple systematic reviews and meta-analyses confirm that simulation leads to substantial improvements in knowledge, technical skills, and task efficiency compared to traditional instruction or no intervention.2,4,15,22 These improvements extend to both basic and advanced laparoscopic tasks, with simulation-trained participants demonstrating faster procedure times, fewer errors, and higher global assessment scores in the operating room.2,4–6,22
Our study further supports the finding that simulation is particularly effective for novices and participants with low prior exposure. Meta-analyses report that such learners show large improvements in surgical skills, shorter operative times, and fewer errors following structured training.7 Recent evidence also demonstrates that even medical students with no prior laparoscopic experience can reach performance levels comparable to more experienced peers after simulator-based training.23 These observations indicate that structured simulation is particularly beneficial for novices and trainees with limited prior exposure, who show the largest gains.
Validity, Transferability, and Retention
High satisfaction ratings in our cohort support the face validity of the program, while significant knowledge gains confirm its content validity. Construct validity was partially supported: prior experience differentiated performance only in camera manipulation, whereas advanced tasks demonstrated less discriminatory ability. Such a levelling effect has been reported in other studies, likely reflecting standardized task design and the equalizing influence of simulation.7,16
Most importantly, simulation-based skills are transferable to the operating room. Evidence from systematic reviews and randomized controlled trials confirms that simulation-trained participants perform laparoscopic cholecystectomy and endoscopy with fewer errors, faster times, and higher global assessment scores.4–6,22,24 While skill retention is generally robust, some studies report modest decline over time, especially in VR-based tasks, highlighting the need for refresher practice.25
Demographics, Residency Year, and Performance
We found no association of gender or training-center referral level with performance within this cohort. This should be interpreted cautiously: in a single-center sample of 29 self-selected volunteers, the absence of detectable subgroup differences reflects comparability of measured outcomes within a standardized curriculum and must not be read as evidence of systemic equity of access or reduced regional training disparities, which this design cannot address. Residency year was associated with outcomes only in colpotomy, a task requiring broader surgical context, while prior experience was predictive mainly for camera navigation, mirroring evidence that performance gaps between novices and experienced trainees narrow after repetition in more complex tasks.7,16
Technology and Curriculum Design
Simulation technology has advanced rapidly, incorporating physical, virtual, and augmented reality systems. Modern simulators integrate high-fidelity visualization, haptic feedback, and automated performance metrics, improving realism and learning efficiency.1,15 VR simulators are as effective as, or superior to, traditional box trainers for both skill acquisition and transfer.4,15 Immersive technologies such as head-mounted displays and 360° video further enhance engagement and presence, with encouraging levels of learner satisfaction.26
Curriculum design is equally important. Reviews recommend proficiency-based progression, individualized feedback, and validated assessment tools as best practices to maximize training outcomes.4,15,16 Our program’s use of passing thresholds reflects this approach and ensured a fair, transparent benchmark across participants.
Assessment, Proficiency, and Stress
By applying standardized thresholds instead of fixed time or repetition counts, our program aligns with proficiency-based learning, where learners must demonstrate competence before progressing.4,15,16 Our results confirm that this model was feasible. Although stress was not measured directly, existing literature suggests that high-stakes examinations can increase anxiety, impair concentration, and widen performance variability, while threshold-based designs reduce variability and support deliberate practice.23,25,27
Implementation and Broader Context
Beyond the present data, the literature describes innovative delivery models — remote and asynchronous simulation, and low-cost portable platforms — that may extend structured training to settings with constrained resources, including low- and middle-income countries.9–12 These approaches are promising but lie outside the scope of the present single-center study; our findings neither demonstrate nor test scalability or equity of access, and we therefore frame these possibilities as context and directions for future work rather than as outcomes of this study.
Cost-Effectiveness and Resource Use
Simulation is increasingly recognized as a cost-effective strategy. By reducing operative times, errors, and complications, simulation training can offset the initial costs of equipment and improve system-wide efficiency.2,3 Low-cost, reusable models and remote training networks further reduce costs and make simulation feasible for a broader range of institutions.10–12
Limitations and Future Directions
This study has several limitations. It was conducted at a single, well-resourced national simulation center using high-fidelity VR simulators, and the cohort comprised 29 self-selected volunteers; both factors limit generalizability and introduce potential selection bias. Because all available participants were included, no a priori power analysis was performed, and the analyses are exploratory and hypothesis-generating. We did not fit a multivariable regression model: with this sample size, the number of events per variable falls well below the conventionally accepted minimum (~10 per predictor), so adjustment for baseline clinical volume and center referral level would be statistically unstable; accordingly, residual confounding by baseline clinical exposure cannot be excluded.28 The passing thresholds were defined a priori by the faculty and were not empirically validated against a normative expert benchmark. Technical performance relied solely on automated simulator metrics, without expert global rating scales (GOALS/OSATS). Self-assessed competence and satisfaction are subject to response and self-report bias. Finally, we lacked trial-level trajectory data and long-term follow-up, precluding assessment of skill retention. Future research should empirically validate the thresholds against expert performance, incorporate expert global rating alongside automated metrics, employ adequately powered multi-center designs permitting adjusted analyses, and link simulator performance to operating-room performance and patient outcomes.
Conclusion
This study demonstrates that a structured, proficiency-oriented laparoscopic simulation course significantly improved theoretical knowledge and self-assessed competence among obstetrics and gynecology residents. Within this single-center cohort, measured outcomes did not differ by gender or training-center referral level, and the influence of prior experience was limited to basic visuospatial tasks. High satisfaction diverged from objective performance, reinforcing the value of criterion-referenced assessment over subjective evaluation alone. A priori passing thresholds supported a transparent, learner-centered evaluation framework. These findings should be regarded as exploratory; confirmation will require adequately powered, multi-center studies linking simulator performance to operating-room performance, skill retention, and clinical outcomes.
Funding
No funding was obtained for this study.
Disclosure
The authors declare that there are no conflicts of interest associated with this article.
References
1. Hong M, Rozenblit JW, Hamilton AJ. Simulation-based surgical training systems in laparoscopic surgery: a current review. Virtual Reality. 2021;25:491–11. doi:10.1007/s10055-020-00469-z
2. Zendejas B, Brydges R, Hamstra SJ, Cook DA. State of the evidence on simulation-based training for laparoscopic surgery: a systematic review. Ann Surg. 2013;257(4):586–593. doi:10.1097/SLA.0b013e318288c40b
3. Aggarwal R, Ward J, Balasundaram I, Sains P, Athanasiou T, Darzi A. Proving the effectiveness of virtual reality simulation for training in laparoscopic surgery. Ann Surg. 2007;246(5):771–779. doi:10.1097/SLA.0b013e3180f61b09
4. Larsen CR, Oestergaard J, Ottesen BS, Soerensen JL. The efficacy of virtual reality simulation training in laparoscopy: a systematic review of randomized trials. Acta Obstet Gynecol Scand. 2012;91(9):1015–1028. doi:10.1111/j.1600-0412.2012.01482.x
5. Spiliotis AE, Spiliotis PM, Palios IM. Transferability of Simulation-Based Training in Laparoscopic Surgeries: a Systematic Review. Minim Invasive Surg. 2020;2020:5879485. doi:10.1155/2020/5879485
6. Dawe SR, Windsor JA, Broeders JA, Cregan PC, Hewett PJ, Maddern GJ. A systematic review of surgical skills transfer after simulation-based training: laparoscopic cholecystectomy and endoscopy. Ann Surg. 2014;259(2):236–248. doi:10.1097/sla.0000000000000245
7. Sarmiento-Altamirano D, Ormaza F, Arroyo MR, et al. Optimizing laparoscopic and robotic skills through simulation in participants with limited or no prior experience: a systematic review and meta-analysis. J Gastrointest Surg. 2024;28(4):566–576. doi:10.1016/j.gassur.2024.01.027
8. Fjørtoft K, Konge L, Gögenur I, Thinggaard E. The Implementation Gap in Laparoscopic Simulation Training. Scand J Surg. 2019;108(2):109–116. doi:10.1177/1457496918798201
9. Asfaw ZK, Todd R, Abasi U, et al. Use of virtual platform for delivery of simulation-based laparoscopic training curriculum in LMICs. Surg Endos Other Interventl Techniq. 2023;37(2):1528–1536. doi:10.1007/s00464-022-09438-w
10. Gaete MI, Belmar F, Cortés M, et al. Remote and asynchronous training network: from a SAGES grant to an eight-country remote laparoscopic simulation training program. Surg Endos Other Interventl Techniq. 2023;37(2):1458–1465. doi:10.1007/s00464-022-09386-5
11. Ulrich AP, Cho MY, Lam C, Lerner VT. A Low-Cost Platform for Laparoscopic Simulation Training. Obstetrics Gynecol. 2020;136(1):77–82. doi:10.1097/aog.0000000000003920
12. Schmitt EM, Randall B, White L, Penick E. Low-Budget Laparoscopic Entry Simulation. Obstet Gynecol. 2025;145(4):e135. doi:10.1097/aog.0000000000005867
13. Fried GM. FLS assessment of competency using simulated laparoscopic tasks. J Gastrointest Surg. 2008;12(2):210–212. doi:10.1007/s11605-007-0355-0
14. Campo R, Wattiez A, Tanos V, et al. Gynaecological endoscopic surgical education and assessment. A diploma programme in gynaecological endoscopic surgery. Gynecol Surg. 2016;13:133–137. doi:10.1007/s10397-016-0957-1
15. Alaker M, Wynn GR, Arulampalam T. Virtual reality training in laparoscopic surgery: a systematic review & meta-analysis. Int J Surg. 2016;29:85–94. doi:10.1016/j.ijsu.2016.03.034
16. Toale C, Morris M, Kavanagh DO. Training and assessment using the LapSim laparoscopic simulator: a scoping review of validity evidence. Surg Endosc. 2023;37(3):1658–1671. doi:10.1007/s00464-022-09593-0
17. Charokar K, Modi JN. Simulation-based structured training for developing laparoscopy skills in general surgery and obstetrics & gynecology postgraduates. J Educ Health Promot. 2021;10(1):387. doi:10.4103/jehp.jehp_48_21
18. Sierant A, Bijok J, Pirozynski M. VR Simulation-Based vs Traditional Apprenticeship Training in Gynecological Laparoscopy: a Comparative Survey of Residents’ Expectations, Skills Acquisition, and Training Structure. Adv Med Educ Pract. 2026;17:570702. doi:10.2147/amep.S570702
19. Sawyer T, Eppich W, Brett-Fleegler M, Grant V, Cheng A. More Than One Way to Debrief: a Critical Review of Healthcare Simulation Debriefing Methods. Simul Healthc. 2016;11(3):209–217. doi:10.1097/sih.0000000000000148
20. Rudolph JW, Simon R, Rivard P, Dufresne RL, Raemer DB. Debriefing with good judgment: combining rigorous feedback with genuine inquiry. Anesthesiol Clin. 2007;25(2):361–376. doi:10.1016/j.anclin.2007.03.007
21. Issenberg SB, McGaghie WC, Petrusa ER, Lee Gordon D, Scalese RJ. Features and uses of high-fidelity medical simulations that lead to effective learning: a BEME systematic review. Med Teach. 2005;27(1):10–28. doi:10.1080/01421590500046924
22. Humm G, Mohan H, Fleming C, et al. The impact of virtual reality simulation training on operative performance in laparoscopic cholecystectomy: meta-analysis of randomized clinical trials. BJS Open. 2022;6(4):86. doi:10.1093/bjsopen/zrac086
23. Zhang W, Qu L, Zilundu PLM, et al. Advancing surgical education: an evaluation of laparoscopic simulation training for medical students. J Eval Clin Pract. 2025;31(1):e14225. doi:10.1111/jep.14225
24. Vanderbilt AA, Grover AC, Pastis NJ, et al. Randomized controlled trials: a systematic review of laparoscopic surgery and simulation-based training. Glob J Health Sci. 2014;7(2):310–327. doi:10.5539/gjhs.v7n2p310
25. Stefanidis D, Korndorffer Jr JR, Sierra R, Touchard C, Dunne JB, Scott DJ. Skill retention following proficiency-based laparoscopic simulator training. Surgery. 2005;138(2):165–170. doi:10.1016/j.surg.2005.06.002
26. Huber T, Paschold M, Hansen C, Wunderling T, Lang H, Kneist W. New dimensions in surgical training: immersive virtual reality laparoscopic simulation exhilarates surgical staff. Surg Endosc. 2017;31(11):4472–4477. doi:10.1007/s00464-017-5500-6
27. Yiannakopoulou E, Nikiteas N, Perrea D, Tsigris C. Virtual reality simulators and training in laparoscopic surgery. Int J Surg. 2015;13:60–64. doi:10.1016/j.ijsu.2014.11.014
28. Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373–1379. doi:10.1016/s0895-4356(96)00236-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.