Back to Archived Journals » Open Access Journal of Sports Medicine » Volume 16
Knee-Spanning External Fixation in the Management of Knee Dislocations and Multiligamentous Knee Injuries: A Narrative Review
Authors Ayhan EM ![]() , Nair M, Levitt SJ
, Nair M, Levitt SJ ![]() , Levy BA, Medvecky MJ
, Levy BA, Medvecky MJ ![]()
Received 5 July 2025
Accepted for publication 8 October 2025
Published 15 October 2025 Volume 2025:16 Pages 131—149
DOI https://doi.org/10.2147/OAJSM.S523319
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Andreas Imhoff
Ekrem Melih Ayhan,1,2 Meghana Nair,1,2 Sarah J Levitt,1,2 Bruce A Levy,3 Michael J Medvecky2
1Frank H. Netter MD School of Medicine, Quinnipiac University, North Haven, CT, USA; 2Department of Orthopaedics & Rehabilitation, Yale School of Medicine, New Haven, CT, USA; 3Orlando Health Jewett Orthopedic Institute, Orlando, FL, USA
Correspondence: Michael J Medvecky, Department of Orthopaedics and Rehabilitation, Yale School of Medicine, New Haven, CT, USA, Tel +1 203 737-6323, Email [email protected]
Abstract: Knee dislocations (KD) and multiligamentous knee injuries (MLKI) are challenging injuries to manage due to the high incidence of associated neurovascular compromise, extensive peri-articular soft-tissue trauma, and long-term functional deficits. Knee-spanning external fixation (KSEF) is occasionally utilized in the acute management of these injuries with the aim of maintaining alignment, protecting vascular repairs, allowing soft-tissue recovery prior to definitive treatment, and protecting freshly reconstructed or repaired ligaments. Despite its use in 5% of MLKIs and up to 50% of KDs, the clinical indications, outcomes, and complications associated with KSEF in the setting of KD/MLKI remain incompletely defined. Furthermore, KD/MLKI treatment algorithms incorporating decision-making related to KSEF application are limited both institutionally and within the literature. Thus, the purpose of this study was to consolidate the existing evidence related to the use of KSEF in the setting of KD/MLKI to support clinical decision-making and identify avenues for future investigation. Following a narrative review of the literature, the identified indications for KSEF in the setting of KD/MLKI were vascular injury, knee fracture-dislocation, extensive soft-tissue injury, persistent instability following reduction, open KDs, and when bracing is not feasible due to patient factors such as morbid obesity. Both rigid and hinged KSEF constructs have been described, with hinged fixators potentially permitting early motion while providing joint stability. Reported complications of KSEF include arthrofibrosis, infection, heterotopic ossification, and compartment syndrome, though available data are primarily retrospective and heterogeneous. Other topics that have been addressed in the literature include biomechanics, cost, magnetic resonance imaging (MRI) compatibility, and psychological impact. However, further research is needed to clarify its specific role, define standardized indications, and compare outcomes with non-invasive or alternative fixation and immobilization strategies.
Plain Language Summary: Knee dislocations and multiple ligament knee injuries are serious injuries that can cause damage to blood vessels, nerves, and soft tissues around the knee, leading to long-term challenges with movement. Doctors sometimes use a device called a knee-spanning external fixator to treat these injuries, which is a metal frame that surgeons place outside of the leg to hold the knee stable This article summarizes what doctors and researchers currently know about knee-spanning external fixators, including their risks and benefits, and explains why more research is needed to guide treatment decisions related to the use of these devices in the management of severe knee injuries. This device is mainly used when the knee is too unstable for a brace, when there is a blood vessel injury, when the skin around the knee is severely damaged, and when the patient has multiple other injuries that need to be managed before their knee injury. While knee-spanning external fixators can help protect the knee and allow it to heal, they also carry several risks like stiffness, infections where the pins enter the skin, unwanted bone growth in the knee, and excessive pressure build-up within the leg. There are also psychological and cost-related concerns associated with the use of these devices. Despite being used frequently, doctors and researchers have not reached a clear agreement about exactly when to use or avoid these devices.
Keywords: multiligament knee injury, knee dislocation, external fixation, external fixator, knee-spanning external fixator, polytrauma
Introduction
Multiligamentous knee injuries (MLKI) are defined as injury to two or more of the major knee ligaments comprising the anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), posteromedial corner (PMC) (including the medial collateral ligament (MCL)) and posterolateral corner (PLC) (including the lateral (fibular) collateral ligament) (Table 1). Knee dislocations (KD), which are not to be equated with MLKI unless a true tibiofemoral dislocation is confirmed, are defined as total disruption of the tibiofemoral joint verified clinically or radiographically (Table 2).1,2 These injuries are often associated with substantial injury to other musculoskeletal and neurovascular structures of the knee and therefore pose significant challenges for the healthcare system.3,4 Patients can experience significant deterioration of clinical outcomes over time, particularly when the PCL is involved.5 Out of 11 million orthopedic injuries from 2004–2009, Arom et al identified 8050 KDs, representing an incidence of 0.072 events per 100 patient-years.6 Around 28–37% of patients with KD/MLKI require a second knee surgery, with readmission more likely in patients with a documented KD.7,8 Furthermore, KDs are associated with concomitant vascular injury in up to 38% of cases, which is potentially limb-threatening.9
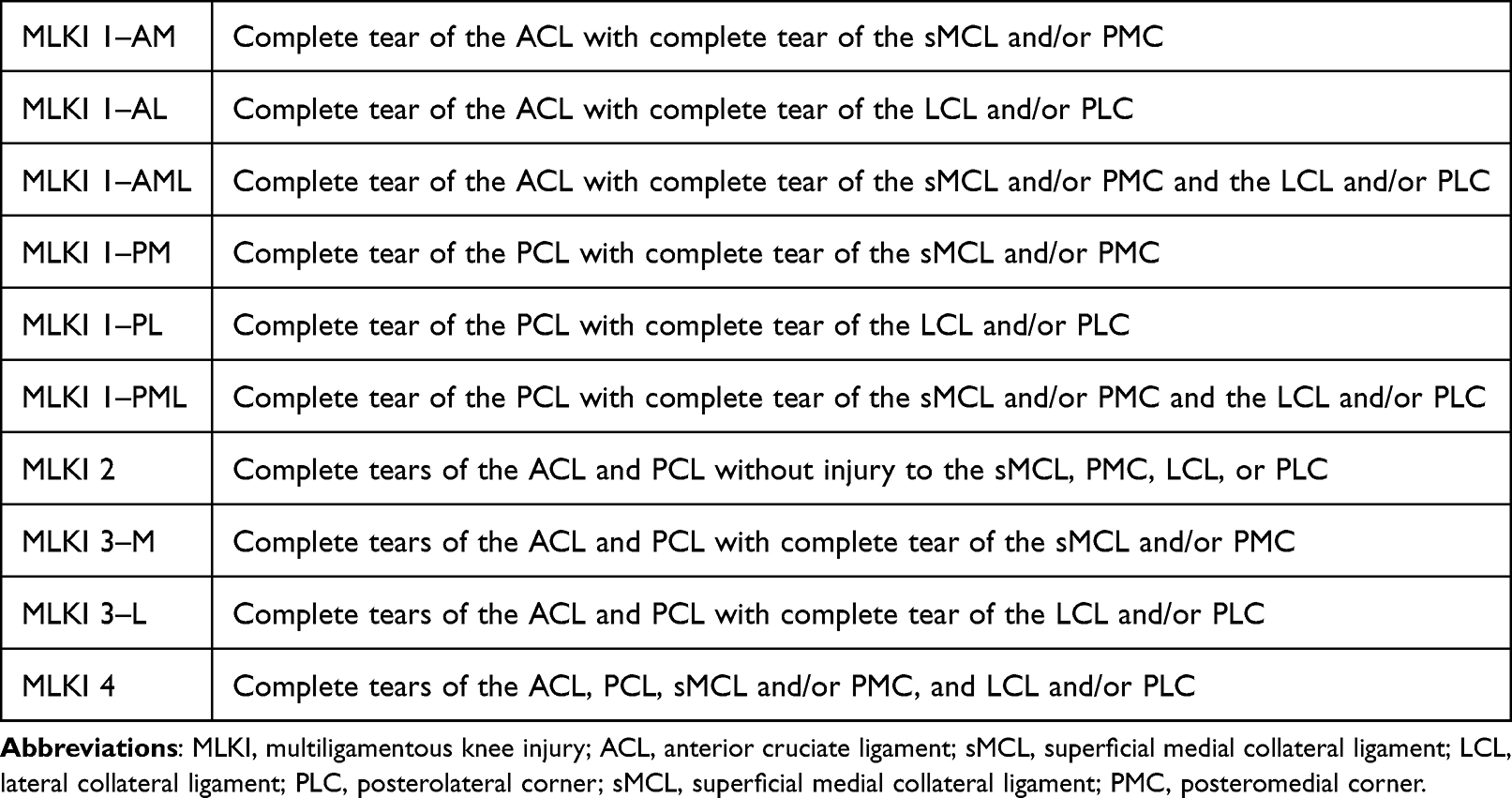 |
Table 1 Anatomic Classification of Multiple Ligament Knee Injuries3 |
 |
Table 2 Schenck Classification Criteria for Knee Dislocations |
Compared to non-dislocated MLKI, KDs are much more likely to be treated with knee-spanning external fixation (KSEF) (Figure 1).10 This temporary immobilization technique, which can be in the form of a rigid or hinged construct, is utilized in approximately 5% of MLKIs but up to 50% of KDs, which increases to 72% when vascular injury is present.9–11 Knee-spanning external fixation, which aims to maintain joint length and alignment while supporting soft-tissue healing, is applied across various fracture and soft-tissue pathologies of the knee. Typically, the decision to use KSEF depends on injury severity, the need to manage existing or potential complications, and the evaluation of knee instability.12–17 KSEF may also be applied due to practical considerations related to patient characteristics such as morbid obesity, eligibility for surgery, anticipated non-adherence to bracing protocols, or polytrauma.18 However, the selective application of pre- and postoperative KSEF represents a significant controversy in the management of KD/MLKI, as KSEF is also associated with several postoperative complications.19–21
 |
Figure 1 Anteriorly placed knee-spanning external fixator for an open knee dislocation. |
Despite the existence of KD/MLKI treatment algorithms that incorporate KSEF, their application in clinical practice remains inconsistent. This variability is likely due to the absence of standardized, evidence-based application criteria. The result is that KSEF may be overutilized in stable injuries or underutilized in scenarios where it could be limb-saving. Thus, the purpose of this narrative review was to clarify the role of KSEF in existing KD/MLKI treatment algorithms. We review the published indications for KSEF, compare how they are applied across studies, highlight key controversies, and describe the spectrum of reported complications. The findings provide new insight by synthesizing the literature into a clearer framework to guide clinical decision-making and future research on the use of KSEF for the treatment of KD/MLKI.
Biomechanics
The primary biomechanical goal of external fixation in the trauma setting is stability restoration. KSEF can neutralize varus-valgus, shear, and torsional loads while preserving limb length, assist in resolution of soft-tissue edema, and protect reconstructed ligaments during early rehabilitation.22,23 Thus, the stability of the mechanical construct largely determines whether the reduction is maintained and/or grafts are protected. KSEF devices are typically constructed using two femoral pins placed anterior or anterolateral and two tibial pins connected by rods/bars, with the knee in full extension to slight flexion (20–30 degrees).24 Stability of KSEF constructs can be enhanced by increasing the pin diameter, number of pins, and distance between pins and bars, as well as reducing the pin-to-fracture and bar-to-bone distances.24–27 Multiplanar configurations can further enhance rigidity.23,28 Several configurations have been assessed biomechanically to optimize stiffness (Figure 2). Mercer et al demonstrated that constructs utilizing anterolateral femoral pin placement coupled with dual connecting rods provided superior stiffness in varus, valgus, and anterior-posterior shear when compared to single monotube or anterior pin placements.22 Similarly, Desai et al found that using pin-to-bar clamps with two crossbars significantly increased stiffness compared to multipin clamps or single crossbar configurations.29
 |
Figure 2 Rigid knee-spanning external fixator construct variations. Reproduced from Morandi MM, Simoncini A, Hays C et al. Optimal configuration for stability and magnetic resonance imaging quality in temporary external fixation of tibial plateau fractures. Orthop Traumatol Surg Res. 2020;106(7):1405–1412. doi:10.1016/j.otsr.2019.12.025,30 with permission from Elsevier. Copyright ©2020. Elsevier Masson SAS. All rights reserved. |
In addition to rigid KSEF constructs, hinged KSEF devices have been increasingly recognized for their ability to permit controlled knee motion postoperatively, thereby minimizing joint stiffness while protecting ligament repairs.31 Hinged external fixators typically consist of two rigid segments connected via a hinge joint, permitting primarily flexion-extension movements (Figure 3). Biomechanical studies highlight their capacity to reduce stress on ligament reconstructions and stabilize anteroposterior translation post-operatively, with minimal adverse loading of periarticular structures.32,33 Fitzpatrick et al demonstrated that hinged KSEF devices significantly reduce tibiofemoral translation in cruciate-deficient knees and decrease cruciate ligament strain in intact or reconstructed knees, indicating their utility in KD/MLKI. However, proper alignment and precise axis placement of hinges are critical for avoiding abnormal loading patterns on the knee joint. Hinge axis alignment is typically manually identified via radiographic landmarks, which requires careful technique to prevent misalignment and potential kinematic complications.33,34 For cases where early controlled knee motion is desirable, hinged KSEF devices offer the advantage of balancing joint stability and mobility, which may be particularly useful following ligament reconstruction.31 Proper surgical technique and appropriate construct selection can significantly enhance clinical outcomes in managing KDs and MLKIs.
 |
Figure 3 Hinged knee-spanning external fixator constructs demonstrating (a) unilateral assembly and (b) compass knee hinge. Reproduced from Fitzpatrick DC, Sommers MB, Kam BC, Marsh JL, Bottlang M. Knee stability after articulated external fixation. Am J Sports Med. 2005;33(11):1735–1741. doi:10.1177/0363546505275132,32 with permission from SAGE Publications. © 2005 SAGE Publications, Inc. All rights reserved. |
History and Rationale
Traumatic KD/MLKI has long been recognized as a limb-threatening emergency, primarily due to the high risk of popliteal artery disruption, as a missed vascular injury can be catastrophic.35 Early reports document alarmingly high amputation rates of up 57%.36 Management strategies have evolved substantially over time and require a careful approach to evaluation and treatment to balance the dichotomous demands of stability and mobility. Until the 1970s, nonsurgical management with closed reduction followed by prolonged cast immobilization was common, with inconsistent outcomes.37 As surgical techniques and postoperative care improved, surgeons began to favor operative treatment, which can be early or delayed and may include temporizing KSEF.17,38,39 While surgical timing has been investigated extensively, there remains no consensus on the optimal strategy, including KSEF use, as systematic reviews have yielded mixed results for MLKI40–47 and KD.48 This is likely due to the wide range of injury patterns, severity levels, and patient factors, necessitating a tailored approach for each individual scenario. Factors that influence the timing of surgery include vascular injuries, fractures, irreducible dislocations, open injuries, surrounding soft-tissue condition, extensor mechanism disruption, stability of the reduction, head trauma, and visceral injuries.49
A staged protocol that involves immediate temporizing KSEF followed by delayed (2–3 weeks) multiligament reconstruction, achieving satisfactory range of motion (ROM) and functional outcomes, was described by Levy et al.17 This work emphasized the idea that temporizing KSEF can improve limb salvage and overall outcomes following KD/MLKI. In the staged/delayed scenario, temporizing KSEF aims to provide immediate mechanical stability for severely unstable knees that cannot maintain joint reduction through bracing alone, thereby protecting the integrity of neurovascular structures. By delaying definitive ligamentous repair/reconstruction, this approach allows soft-tissue recovery, inflammation reduction, and resolution of any concurrent traumatic injuries in the case of a polytraumatized patient. Thus, the delayed/staged approach with immediate temporizing KSEF aims to balance the urgency of addressing ligament injuries against the practical constraints posed by severe soft-tissue and/or systemic injuries. This is compared to early, single-stage reconstruction without the use of temporizing KSEF, which offers the theoretical advantages of decreased cost, decreased risk of osteoarthritis, and decreased risk of altered knee biomechanics and subsequent meniscal and cartilage damage.50–54
As for hinged KSEF, several authors have described its use in various scenarios, primarily for postoperative stabilization and graft protection following acute and chronic KD.55–60 Hinged KSEF has also been described in the setting of acute fracture-dislocation,61 recurrent tibiofemoral subluxation,62 extensor mechanism disruption,63,64 and status-post extensive capsular release and ligament reconstruction for chronic, fixed KDs.65–67
Treatment Algorithms
While there is no universal KD/MLKI treatment algorithm, several authors have described algorithms that incorporate the use of temporizing KSEF.16,17,68,69 The staged protocol described by Levy et al begins with immediate vascular assessment, followed by temporizing KSEF if there is vascular injury, gross instability after reduction, open dislocation, or an inability to safely mobilize the patient in a brace (Figure 4). Definitive ligament reconstruction is subsequently performed after soft-tissue recovery, typically 3–6 weeks post-injury, with simultaneous repair of all affected ligaments.
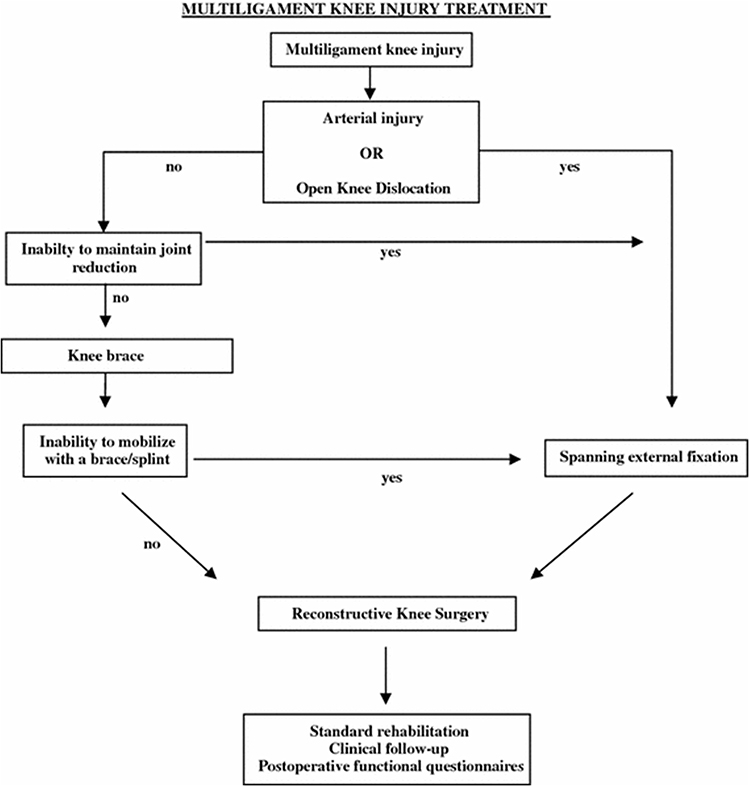 |
Figure 4 Multiligament knee injury treatment algorithm with temporizing knee-spanning external fixation. Reproduced from Levy BA, Krych AJ, Shah JP, Morgan JA, Stuart MJ. Staged protocol for initial management of the dislocated knee. Knee Surg Sports Traumatol Arthrosc. 2010;18(12):1630–1637. doi:10.1007/s00167-010-1209-y,17 with permission from John Wiley & Sons. © 2010 John Wiley & Sons, Inc. All rights reserved. |
Maslaris et al describe a similar systematic algorithm emphasizing an initial rapid vascular assessment and stabilization guided by damage-control orthopedics (Figure 5).16 Immediate joint reduction is followed by neurovascular examination via ankle-brachial indices (ABI). Temporizing KSEF is applied if there is vascular injury, open injury, compartment syndrome, fracture-dislocation, persistent instability in a brace or other closed means, or polytrauma.
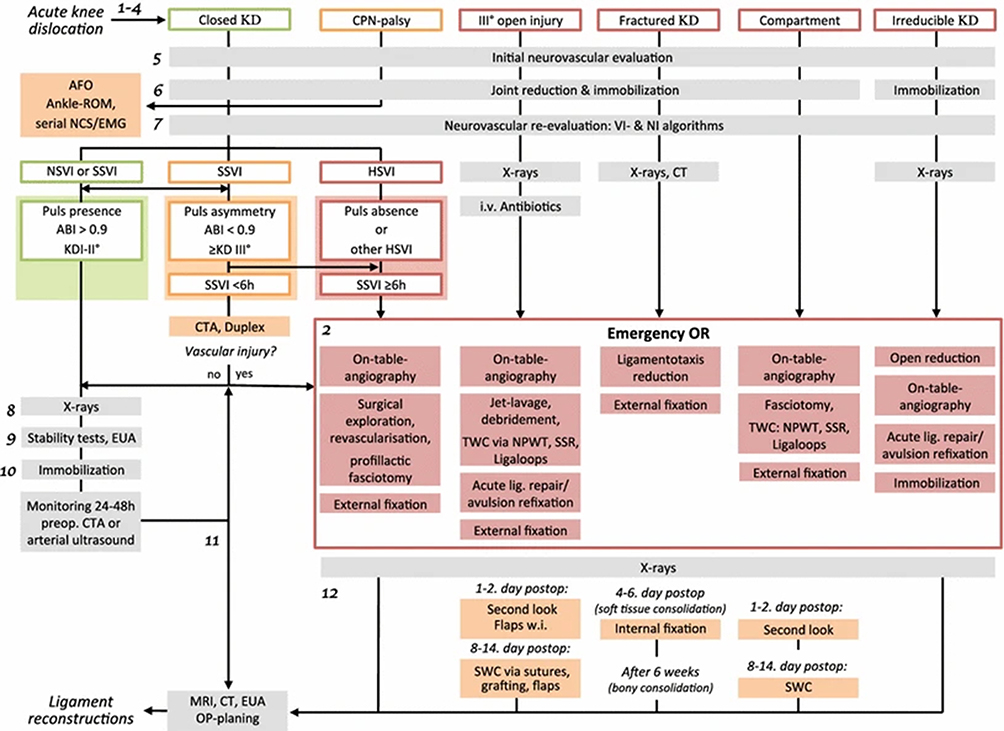 |
Figure 5 Acute knee dislocation treatment algorithm with temporizing knee-spanning external fixation. KD, knee dislocation; CPN, common peroneal nerve; AFO, ankle-foot orthosis; ROM, range of motion; NCS/EMG, nerve conduction study/electromyography; NSVI, no signs of vascular injury; SSVI, soft signs of vascular injury; HSVI, hard signs of vascular injury; EUA; examination under anesthesia: CTA: CT angiogram; TWC, traditional wound care; NPWT, negative pressure wound therapy; SSR, secondary surgical revision; SWC, secondary wound closure. Reproduced from Maslaris A, Brinkmann O, Bungartz M, Krettek C, Jagodzinski M, Liodakis E. Management of knee dislocation prior to ligament reconstruction: What is the current evidence? Update of a universal treatment algorithm. Eur J Orthop Surg Traumatol. 2018;28(6):1001–1015. doi:10.1007/s00590-018-2148-4,16 with permission from Springer Nature. © 2018 Springer Nature, Inc. All rights reserved. |
Indications
While KSEF remains a critical intervention for managing KD and MLKI, the indications remain poorly standardized within the literature. Commonly recognized indications include vascular injury, knee fracture-dislocation, persistent instability, open dislocation, severe soft-tissue injury, and specific patient characteristics such as morbid obesity.9,14–17,70 Vascular injuries are particularly emphasized, with KSEF being utilized largely to prevent redislocation, protect vascular repairs, monitor and manage fasciotomy sites, and enable continued assessment of soft-tissue swelling.9,17 Likewise, complex fracture-dislocations of the distal femur or tibial plateau, irreducible or redislocating KDs, and chronically subluxated joints are repeatedly listed as absolute indications because they require rigid alignment control prior to definitive osseous or ligamentous reconstruction.13,17,71 Additionally, several authors emphasize indications driven by the condition of the soft-tissue envelope. Open KDs, degloving injuries, or extensive abrasions benefit from temporary external stabilization that permits serial debridement and wound access while preventing further cartilage or neurovascular injury.13,15–17 Additionally, in patients with morbid obesity, particularly following ultra-low-velocity KDs, commercial braces often fail to maintain concentric reduction, making KSEF the only reliable means to prevent early recurrence.14,15,72 Patients with obesity with ultra-low velocity injuries also have higher rates of concomitant neurovascular injuries and postoperative complications following ligament reconstruction, which further justifies definitive management with KSEF in these patients.73,74 Overall, precise clinical scenarios such as vascular compromise, open fractures, irreducible subluxations, fracture-dislocations, and morbid obesity should guide the selective application of KSEF to minimize morbidity, resource utilization, and potential complications. Further clarification and validation of standardized criteria is warranted to refine the utilization of this important orthopedic intervention.
A Note on Polytrauma
“Polytrauma” is also frequently cited as a clinical indication for KSEF in the setting of KD/MLKI.12,15,16,75,76 This term is most recently defined in the 2014 Berlin consensus statement as an injury with an Abbreviated Injury Scale (AIS) score ≥ 3 in at least two distinct body regions, plus ≥ 1 of the following admission criteria: hypotension (systolic blood pressure ≤ 90 mmHg), unconsciousness (Glascow Coma Scale (GCS) score ≤ 8), acidosis (base deficit ≤ −6.0), coagulopathy (PTT ≥ 40 seconds or INR ≥ 1.4), and age (≥ 70 years).77 Up to a third of patients with KD/MLKI present with head, chest, or abdominal injuries, and up to 60% sustain an associated fracture.75,78,79 While the injury severity score (ISS) and new injury severity score (NISS) are available for quantitatively assessing polytrauma, specific KSEF application criteria in the setting of polytrauma are not available. If polytrauma is to be used as a primary indication for KSEF application following KD/MLKI, additional guidelines and protocols based on the NISS are needed.80,81 This raises concern that KSEF may be applied more broadly than needed in the setting of polytrauma, specifically for knees that are sufficiently stable post-reduction in a brace or splint. A case series by Darabos et al highlights this controversy by demonstrating worse clinical outcomes in polytraumatized patients undergoing prolonged, staged management with KSEF compared to patients managed with shorter, more direct surgical interventions without KSEF.82 In 14 polytraumatized patients with KDs, KSEF was applied selectively in three cases specifically in the setting of hemothorax, reflecting a more conservative approach aimed at reducing avoidable complications due to KSEF.82 Thus, if there is no trauma-associated neurovascular injury and the reduction can be maintained non-invasively, a single-stage treatment protocol in the subacute phase without the use of KSEF may be sufficient in the polytraumatized patient with a KD. Ng et al provide a set of indications for KSEF in the setting of MLKI that does not include polytrauma and is instead based on vascular injury, open KD, fracture-dislocation, or an inability to non-invasively maintain reduction.13 Thus, for KDs that are isolated or stable after reduction, alternative management strategies should be considered to avoid additional patient morbidity, overutilization of healthcare resources, and potential complications, even in the setting of polytrauma. Table 3 displays studies in the current literature that provide a set of indications for KSEF following KD/MLKI.
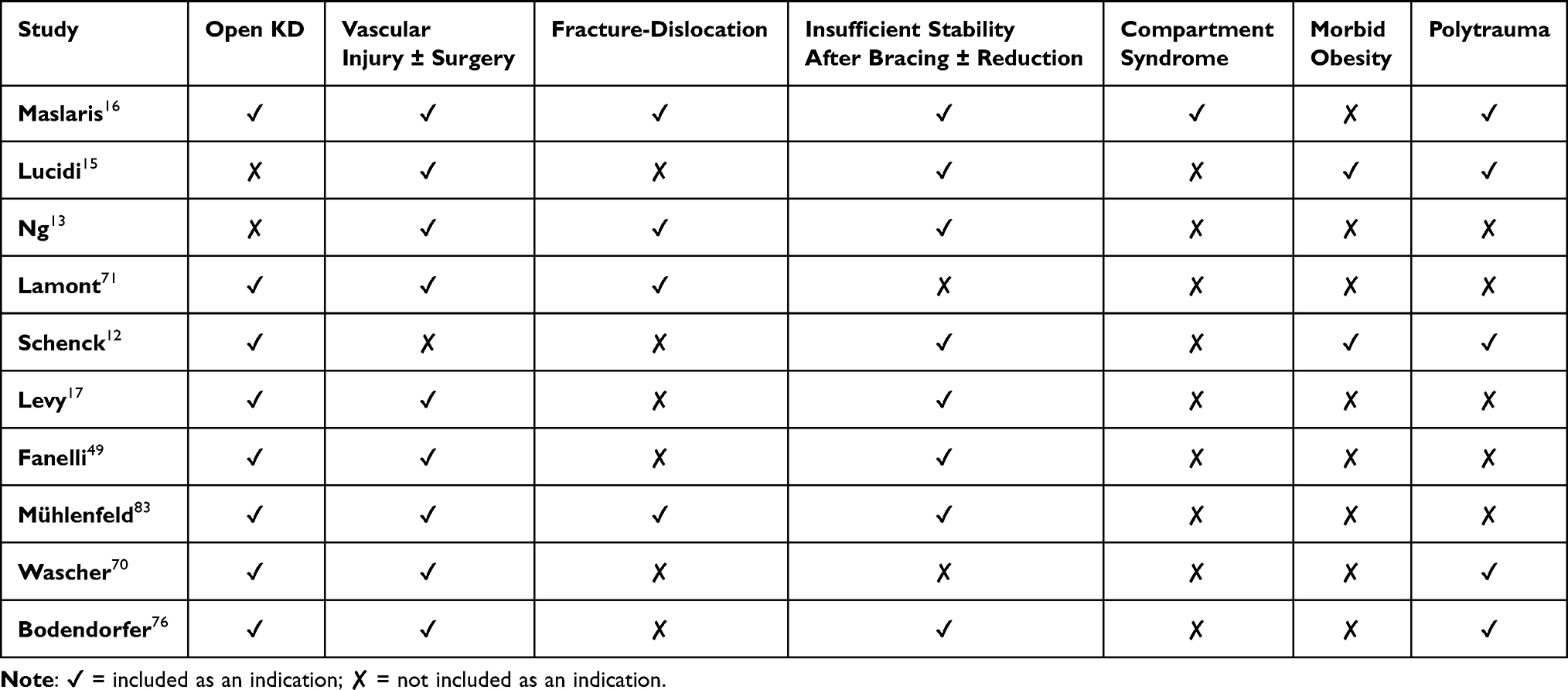 |
Table 3 Studies Describing Indications for KSEF After KD/MLKI |
Outcomes
Few comparative studies have directly assessed outcomes of temporizing KSEF in the setting of KD/MLKI, which may be attributable to the wide range of possible injury patterns and subsequent difficulty controlling for confounding variables, as well as the rarity of this injury and treatment modality at baseline. While there are no studies directly comparing outcomes of KD/MLKI managed with temporizing KSEF to those managed without temporizing KSEF, there have been several retrospective studies within the past 15 years that have indirectly or secondarily assessed outcomes associated with temporizing KSEF (Table 4). The outcomes related to temporizing KSEF assessed in these studies include stiffness/arthrofibrosis/motion loss in seven studies, infection in three, compartment syndrome in two, heterotopic ossification in two, and ROM in two. Other variables that have been assessed include obesity, return to duty, MRI image quality, Oxford Knee Score, IKDC, Lysholm, SF-12 Mental and Physical components, and ligament stability.
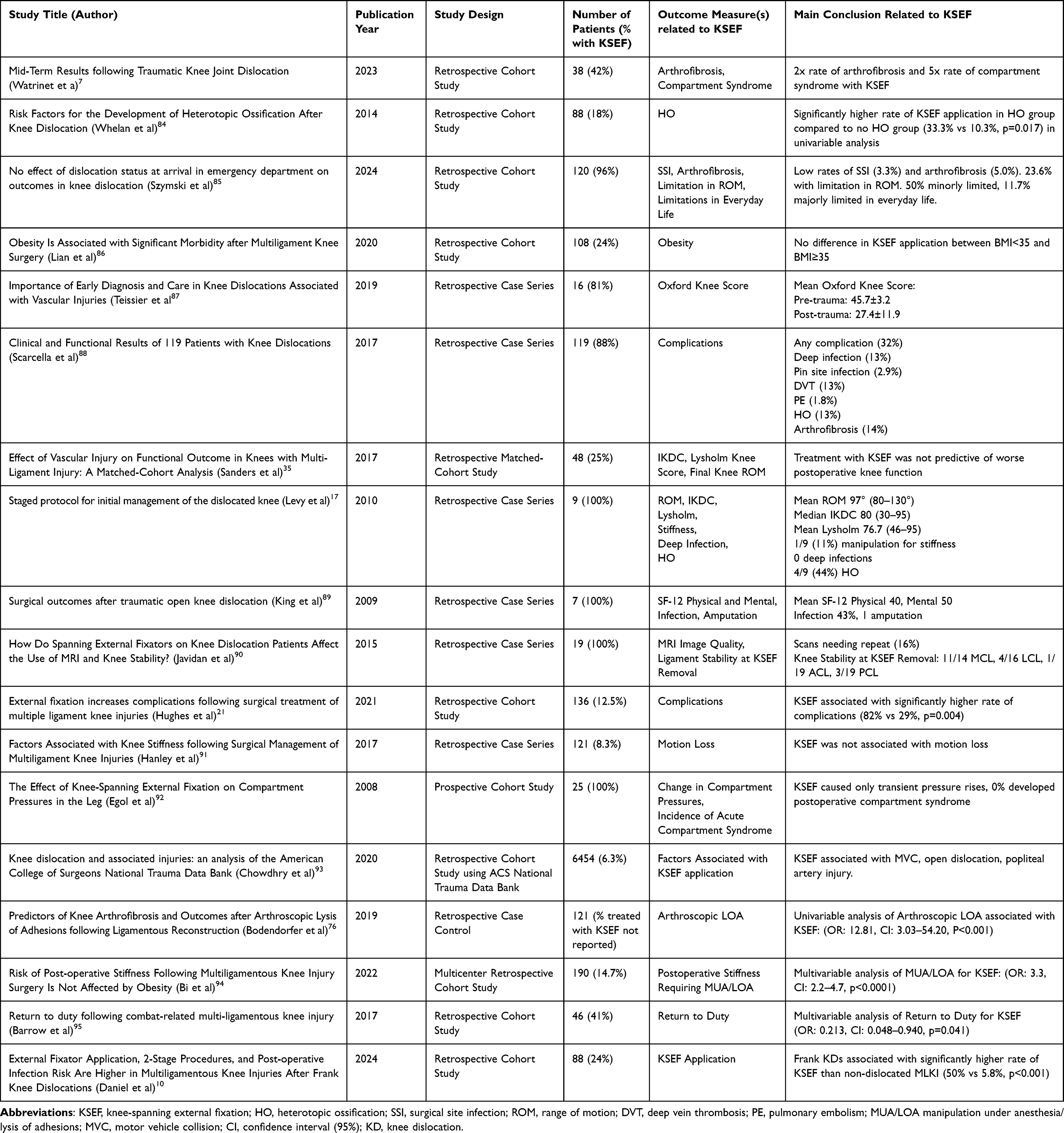 |
Table 4 Studies Assessing Outcomes Related to KSEF Following KD/MLKI |
There are also a few studies that have investigated the use of hinged KSEF as an adjunct following ligament reconstruction.55–57,96 The goal of hinged KSEF in this scenario would be to minimize the risk of motion loss and potential arthrofibrosis that may result from rigid casts, braces, and immobilization, as this can be associated with significant pain and poor functional outcomes.7,97 Angelini et al demonstrated in a randomized controlled trial (RCT) that the use of hinged KSEF for subacute and chronic KD provides the same ligament stability and improved ROM and patient-reported outcomes (PROs) compared to rigid knee bracing in extension.57 Stannard et al demonstrated in two prospective studies that hinged KSEF following KD is associated with significantly lower rates of ligament failure following repair/reconstruction.55,56 Lastly, Sobrado et al found a high prevalence of osteoarthritis (64.5%) in patients with chronic KD, with no significant difference between the hinged KSEF and rigid knee brace groups.96 These studies suggest that, overall, hinged KSEF following KD/MLKI to supplement ligament repair/reconstruction can be utilized safely and effectively, particularly when multiple ligaments are repaired at once.57
Complications
Infection
One of the most cited complications of KSEF is device-related infection, which occurs most frequently at the interface of the pin, bar and clamps.18,98–104 Studies investigating the risk of infection associated with KSEF are largely in the setting of tibial plateau fractures rather than KD/MLKI.105 Infection rates following KSEF for tibial plateau fractures range from 6.0% to 26.9% depending upon sterilization methods.100,101,106 Various contributing factors have been described, including clamp/bar adjustment post sterilization, increased time in the operating room, and overlapping pin sites.101,104,107–109 However, it has also been suggested that KSEF is not associated with infection.110 While there is a lack of consensus regarding the standard protocol for pin site care, it has been encouraged to adopt a consistent approach until further high-quality evidence is established.102,104,111–114 Specific strategies for minimizing the risk of infection due to KSEF include changing gloves after device manipulation, protecting soft tissues with drill sleeves, using sharp drill bits, and avoiding thermal and ischemic necrosis of the bone and skin.104
Arthrofibrosis
A recent systematic review by de Fortuny et al found that arthrofibrosis is the most common complication following surgically treated MLKI, with an incidence of 8.4%.115 This complication can have devastating consequences for the patient.7,97,116 Notably, KSEF application has been found to be associated with an increased risk of arthrofibrosis.7,76,94 Thus, prolonged KSEF use may contribute to arthrofibrosis, although it remains unclear whether this is due to the device itself or to injury severity.10 Arthrofibrosis following KD/MLKI may be prevented with the use of immediate knee motion, shorter surgery time, minimizing soft tissue damage, and utilization of HEF.58,116,117 If arthrofibrosis does result, arthroscopic arthrolysis of adhesions can be performed, as this has been demonstrated to be a safe and effective way to restore ROM following acute KD.118,119
Heterotopic Ossification
Heterotopic ossification (HO) is one of the most common complications after KD/MLKI, affecting 21–43% of patients.11,120–122 Heterotopic ossification in the knee can lead to significant pain, stiffness, arthrofibrosis, and mechanical block, often requiring surgical excision.11,84,120–127 While trauma-induced HO has been studied, very little is known regarding the risk factors and pathophysiology of HO following KD/MLKI, including its anatomical distribution and functional impact.128–135 Available evidence suggests HO commonly forms in the medial and posterior compartments of the knee, particularly following posterior cruciate ligament (PCL) reconstruction or extensive soft tissue trauma.84,121,122,136–140 Additionally, surgical factors such as tunnel drilling, reamed tibial nailing, or KSEF application use may contribute to HO by leaving behind bone debris or hematoma that stimulate bone formation.84,139,141–143 The association between HO and KSEF may result from both mechanical limitations in joint motion and the underlying severity of the injury and/or surgery.21 It is unknown whether trauma from the initial injury, subsequent surgery and management, or a synergistic effect yields a greater risk of HO following KD/MLKI. KSEF is often applied in the setting of polytrauma, which makes it challenging to isolate its specific contribution to HO from other potentially contributory factors.15,16 For example, injury severity score (ISS) ≥ 26 has been shown to significantly increase the risk of severe HO, possibly due to a more intense systemic inflammatory response.120 Additionally, motion loss, which is frequently observed in patients with prolonged KSEF use, is strongly associated with HO.21 Therefore, the observed association between KSEF and HO may not be directly related to KSEF itself.
Compartment Syndrome
Few studies have investigated the risk of compartment syndrome associated with KSEF application, primarily in the setting of tibial plateau fractures. Watrinet et al found that compartment syndrome occurred in 25% of patients with KDs treated with KSEF compared to 5% in those treated without KSEF.7 Stark et al found an incidence of 53% in 17 tibial plateau fracture-dislocations treated with temporizing KSEF, suggesting that KSEF placement itself may precipitate compartment syndrome following severe knee injuries.144 The authors recommended careful monitoring of tibial plateau fracture-dislocations for compartment syndrome after KSEF placement. However, a prospective series that included KDs found only transient pressure spikes and no postoperative compartment syndrome after immediate KSEF, suggesting the KSEF itself is not a primary driver when applied correctly.92
Deep Vein Thrombosis
Patients undergoing KSEF in the setting of KD/MLKI may also face increased risk of deep vein thrombosis (DVT) and pulmonary embolism (PE).145–148 This risk may be further exacerbated by prolonged immobility following these injuries.149 A prospective study by Sems et al evaluated 148 external fixation devices applied for lower extremity trauma, including 10 KDs, instituting low-molecular-weight heparin (LMWH) prophylaxis and early mobilization.147 Duplex ultrasonography performed 1–3 days prior to frame removal revealed a 2.1% incidence of DVT, with no hemorrhagic complications, which aligns with DVT rates seen in historical controls. Similar findings were reported in a study of elective KSEF use, with an overall thromboembolic event incidence of less than 1% when patients at high risk were treated with thromboprophylaxis.148 These findings suggest that early restoration of limb length, alignment, and stability to enable early joint mobilization may contribute to the prevention of thromboembolic events when combined with the appropriate prophylactic measures.
Other Considerations
Psychological Impact
It is important to also consider the potential for KSEF to create psychological distress and aesthetic concerns for patients, which may affect adherence to treatment and overall quality of life during the recovery period following KD.150 It has been demonstrated that patients with strong social support can better manage the stressors of external fixation.151 It has also been demonstrated that patients who experience psychological distress may have less adherence to their rehabilitation protocols, impacting recovery.152 When there are no definitive indications for KSEF, the added patient morbidity and hospitalization costs and time as well as the psychological impact of KSEF should be a primary consideration in management. The necessity for stability must be carefully weighed against the risks of morbidity, complications, and their effects on patient comfort and adherence.
MRI Safety
Studies focusing on the MRI safety of KSEF indicate that MRI can be performed safely with these devices in place under the proper conditions.153,154 This is important because all patients with suspected MLKI should undergo MRI, and the urgent placement of a KSEF device can prevent this if MRI safety is not clearly understood.1 A recent systematic review of 358 MRIs found zero cases of serious patient harm, with no burns or instability, and a 1.1% rate of minor patient discomfort that resolved without injury.155 Additionally, while the presence of a KSEF device does introduce artifact and signal noise on MRI, literature suggests high-quality images are usually still achievable.156,157 However, significant variability exists regarding institutional policies and clinician comfort levels with performing MRI in patients with external fixators.153 A survey study by Marcel et al revealed a lack of consensus and widespread absence of formal institutional guidelines, contributing to delayed imaging and potentially impacting clinical outcomes negatively.153 Given these findings, clinicians are encouraged to perform thorough risk assessments, reference manufacturer guidelines as a baseline, and closely coordinate with their medical and radiological teams. The broader consensus in current literature indicates that while definitive universal guidelines remain elusive due to configuration variability, MRI can and should be utilized safely and effectively in the management of patients with a KSEF for KD/MLKI, provided proper precautions and multidisciplinary collaboration are observed.153,155,156
Cost
A US national database study found that the average total charges associated with KD were $63,138, which increase significantly in patients with obesity and morbid obesity to $72,608.158 Furthermore, staged surgical treatment, which often includes temporizing KSEF, is significantly more expensive than a single-stage repair.159 Notably, one Level I trauma center analysis found that hardware alone for an external fixator frame costs approximately $5,900 per case in the US, compared to $50 in low-income countries.160,161 Furthermore, in developing countries, external fixators are reused up to 10 times.161 While there are important ethical considerations regarding the reuse of external fixators, Dirschl et al demonstrated that reducing costs via device reuse can be implemented safely and effectively.162 Overall, KSEF is a costly intervention in the US with significant cost variability, which presents a unique opportunity for cost savings in trauma care.163
Conclusion
Knee-spanning external fixation is a commonly used tool in the acute and postoperative management of knee dislocations and multiligament knee injuries. Current evidence broadly supports its use in scenarios involving vascular compromise, knee fracture-dislocations, severe soft-tissue trauma, difficulty with maintaining reduction via non-invasive means, morbid obesity, postoperative graft protection, and potentially polytrauma. Despite its widespread application, controversy persists regarding its precise indications, optimal timing, and associated complications, necessitating judicious utilization and individualized decision-making. Further high-quality studies and updated guidelines are needed to clarify these considerations, refine treatment algorithms, and improve outcomes.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this study.
Disclosure
M.J.M. serves as a speaker for educational symposia sponsored by DePuy Mitek and Smith & Nephew.
B.A.L. received royalties from Arthrex, Inc., is a Paid Consultant for Arthrex, Inc, received stock from COVR Medical LLC, is on the Editorial or Governing board of Journal of Knee Surgery, Knee Surgery, Sports Traumatology, Arthroscopy, Orthopedics Today.
The authors declare no other conflicts of interest.
References
1. Murray IR, Makaram NS, Geeslin AG, et al. Multiligament knee injury (MLKI): an expert consensus statement on nomenclature, diagnosis, treatment and rehabilitation. Br J Sports Med. 2024;58(23):1385–1400. doi:10.1136/bjsports-2024-108089
2. Makaram NS, Murray IR, Geeslin AG, Chahla J, Moatshe G, LaPrade RF. Diagnosis and treatment strategies of the multiligament injured knee: a scoping review. Br J Sports Med. 2023;57(9):543–550. doi:10.1136/bjsports-2022-106425
3. Poploski KM, Lynch AD, Burns TC, et al. Presentation and surgical management of multiple ligament knee injuries: a multicenter study from the Surgical Timing and Rehabilitation (STaR) Trial for MLKIs Network [published correction appears in. J Bone Joint Surg Am. 2023;21(12):e33. doi:10.2106/JBJS.ER.20.02051
4. Kim SH, Park YB, Kim BS, Lee DH, Pujol N. Incidence of associated lesions of multiligament knee injuries: a systematic review and meta-analysis. Orthop J Sports Med. 2021;9(6):23259671211010409. doi:10.1177/23259671211010409
5. Klasan A, Maerz A, Putnis SE, Ernat JJ, Ollier E, Neri T. Outcomes after multiligament knee injury worsen over time: a systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2025;33(4):1281–1298. doi:10.1002/ksa.12442
6. Arom GA, Yeranosian MG, Petrigliano FA, et al. The changing demographics of knee dislocation: a retrospective database review. Clin Orthop Relat Res. 2014;472(9):2609–2614. PMID: 24214822; PMCID: PMC4117912. doi:10.1007/s11999-013-3373-0
7. Watrinet J, von Rüden C, Regenbogen S, et al. Mid-term results following traumatic knee joint dislocation. J Clin Med. 2022;12(1):266. doi:10.3390/jcm12010266
8. Wilson SM, Mehta N, Do HT, Ghomrawi H, Lyman S, Marx RG. Epidemiology of multiligament knee reconstruction. Clin Orthop Relat Res. 2014;472(9):2603–2608. PMID: 24777729; PMCID: PMC4117876. doi:10.1007/s11999-014-3653-3
9. Ramírez-Bermejo E, Gelber PE, Pujol N. Management of acute knee dislocation with vascular injury: the use of the external fixator. A systematic review. Arch Orthop Trauma Surg. 2022;142(2):255–261. doi:10.1007/s00402-020-03684-0
10. Daniel AV, Johnson TA, Druskovich KF, Williams WA, Miller D, Kupiszewski SJ. External fixator application, 2-stage procedures, and postoperative infection risk are higher in multiligamentous knee injuries after frank knee dislocations. Arthrosc Sports Med Rehabil. 2024;7(2):101070. doi:10.1016/j.asmr.2024.101070
11. Randall ZD, Strok MJ, Mazzola JW, Agrawal R, Yaeger LH, Berkes MB. The known and unknown reality of knee dislocations: a systematic review. Injury. 2024;55(11):111904. doi:10.1016/j.injury.2024.111904
12. Schenck RC, Richter DL, Wascher DC. Knee dislocations: lessons learned from 20-year follow-up. Orthop J Sports Med. 2014;2(5):2325967114534387. doi:10.1177/2325967114534387
13. Ng JW, Myint Y, Ali FM. Management of multiligament knee injuries. EFORT Open Rev. 2020;5(3):145–155. doi:10.1302/2058-5241.5.190012
14. Fanelli GC. Timing of repair or reconstruction after knee dislocation. J Knee Surg. 2020;33(4):335–338. doi:10.1055/s-0039-1700573
15. Lucidi GA, Grassi A, Cucurnia I, Macchiarola L, Zaffagnini S. Use of external fixator pre- and postreconstruction in the multiligament injured knee. Annals of Joint. 2018;3.
16. Maslaris A, Brinkmann O, Bungartz M, Krettek C, Jagodzinski M, Liodakis E. Management of knee dislocation prior to ligament reconstruction: what is the current evidence? Update of a universal treatment algorithm. Eur J Orthop Surg Traumatol. 2018;28(6):1001–1015. doi:10.1007/s00590-018-2148-4
17. Levy BA, Krych AJ, Shah JP, Morgan JA, Stuart MJ. Staged protocol for initial management of the dislocated knee. Knee Surg Sports Traumatol Arthrosc. 2010;18(12):1630–1637. doi:10.1007/s00167-010-1209-y
18. Encinas-Ullán CA, Martínez-Diez JM, Rodríguez-Merchán EC. The use of external fixation in the emergency department: applications, common errors, complications and their treatment. EFORT Open Rev. 2020;5(4:204–214. doi:10.1302/2058-5241.5.190029.
19. Mosquera MF, Jaramillo A, Gil R, Gonzalez Y. Controversies in acute multiligamentary knee injuries (MLKI). J Exp Orthop. 2020;7(1):56. doi:10.1186/s40634-020-00260-8
20. Levy BA, Fanelli GC, Whelan DB, et al. Controversies in the treatment of knee dislocations and multiligament reconstruction. J Am Acad Orthop Surg. 2009;17(4):197–206. doi:10.5435/00124635-200904000-00001
21. Hughes JD, Lynch AD, Smith CN, Musahl V, Irrgang JJ. External fixation increases complications following surgical treatment of multiple ligament knee injuries. Knee Surg Sports Traumatol Arthrosc. 2022;30(1):161–166. doi:10.1007/s00167-021-06508-9
22. Mercer D, Firoozbakhsh K, Prevost M, Mulkey P, DeCoster TA, Schenck R. Stiffness of knee-spanning external fixation systems for traumatic knee dislocations: a biomechanical study. J Orthop Trauma. 2010;24(11):693–696. doi:10.1097/BOT.0b013e3181e3cd4b
23. Fragomen AT, Rozbruch SR. The mechanics of external fixation. HSS J. 2007;3(1):13–29. doi:10.1007/s11420-006-9025-0
24. Morshed S, Malik A, Lim Z. External fixators for lower extremity fractures. In: von Keudell AG, Weaver MJ, editors. Operative Techniques in Orthopedic Trauma. Cham: Springer; 2025. doi:10.1007/978-3-031-80825-8_10.
25. Behrens F. General theory and principles of external fixation. Clin Orthop Relat Res. 1989;241:15–23. doi:10.1097/00003086-198904000-00004
26. Behrens F, Johnson W. Unilateral external fixation. Methods to increase and reduce frame stiffness. Clin Orthop Relat Res. 1989;241:48–56. doi:10.1097/00003086-198904000-00007
27. Behrens F, Johnson WD, Koch TW, Kovacevic N. Bending stiffness of unilateral and bilateral fixator frames. Clin Orthop Relat Res. 1983;178:103–110. doi:10.1097/00003086-198309000-00014
28. Moss DP, Tejwani NC. Biomechanics of external fixation: a review of the literature. Bull NYU Hosp Jt Dis. 2007;65(4):294–299.
29. Desai MJ, Reisman WM, Hutton WC. Improving spanning-knee external fixator stiffness: a biomechanical study. Am J Orthop. 2016;45(2):E42–E45.
30. Morandi MM, Simoncini A, Hays C, et al. Optimal configuration for stability and magnetic resonance imaging quality in temporary external fixation of tibial plateau fractures. Orthop Traumatol Surg Res. 2020;106(7):1405–1412. doi:10.1016/j.otsr.2019.12.025
31. Ayhan EM, Levitt S, Abrams GD, Stannard JP, Medvecky MJ. The role of hinged external fixation in the treatment of knee dislocation, subluxation and fracture-dislocation: a systematic review of indications. J Exp Orthop. 2025;
32. Fitzpatrick DC, Sommers MB, Kam BC, Marsh JL, Bottlang M. Knee stability after articulated external fixation. Am J Sports Med. 2005;33(11):1735–1741. doi:10.1177/0363546505275132
33. Gatti G, Shweiki S, Lupinacci G, Fragomeni G, Danieli G (2014). Hinged external fixators for knee rehabilitation - kinematic concept of a two degree-of-freedom system In
34. Nuelle CW, Stannard JP. Placement of a compass knee hinge: surgical technique. JBJS Essent Surg Tech. 2014;4(1):e2. doi:10.2106/JBJS.ST.M.00062
35. Sanders TL, Johnson NR, Levy NM, et al. Effect of vascular injury on functional outcome in knees with multi-ligament injury: a matched-cohort analysis. J Bone Joint Surg Am. 2017;99(18):1565–1571. doi:10.2106/JBJS.16.01540
36. Lefrak EA. Knee dislocation. An illusive cause of critical arterial occlusion. Arch Surg. 1976;111(9):1021–1024. doi:10.1001/archsurg.1976.01360270093018
37. Rihn JA, Groff YJ, Harner CD, Cha PS. The acutely dislocated knee: evaluation and management. J Am Acad Orthop Surg. 2004;12(5):334–346. doi:10.5435/00124635-200409000-00008
38. Harner CD, Waltrip RL, Bennett CH, Francis KA, Cole B, Irrgang JJ. Surgical management of knee dislocations. J Bone Joint Surg Am. 2004;86(2):262–273. doi:10.2106/00004623-200402000-00008
39. Levy BA, Dajani KA, Whelan DB, et al. Decision making in the multiligament-injured knee: an evidence-based systematic review. Arthroscopy. 2009;25(4):430–438. doi:10.1016/j.arthro.2009.01.008
40. Vermeijden HD, Yang XA, Rademakers MV, et al. Early and delayed surgery for isolated ACL and multiligamentous knee injuries have equivalent results: a systematic review and meta-analysis. Am J Sports Med. 2023;51(4):1106–1116. doi:10.1177/03635465211069356
41. Kim SH, Han SJ, Park YB, Kim DH, Lee HJ, Pujol N. A systematic review comparing the results of early vs delayed ligament surgeries in single anterior cruciate ligament and multiligament knee injuries. Knee Surg Relat Res. 2021;33(1):1. doi:10.1186/s43019-020-00086-9
42. Vicenti G, Solarino G, Carrozzo M, et al. Major concern in the multiligament-injured knee treatment: a systematic review. Injury. 2019;50(Suppl 2):S89–S94. doi:10.1016/j.injury.2019.01.052
43. Marder RS, Poonawala H, Pincay JI, et al. Acute versus delayed surgical intervention in multiligament knee injuries: a systematic review. Orthop J Sports Med. 2021;9(10):23259671211027855. doi:10.1177/23259671211027855
44. Hohmann E, Glatt V, Tetsworth K. Early or delayed reconstruction in multi-ligament knee injuries: a systematic review and meta-analysis. Knee. 2017;24(5):909–916. doi:10.1016/j.knee.2017.06.011
45. Vaishya R, Patralekh MK, Vaish A, Tollefson LV, LaPrade RF. Effect of timing of surgery on the outcomes and complications in multi-ligament knee injuries: an overview of systematic reviews and a meta-analysis. Indian J Orthop. 2024;58(9):1175–1187. doi:10.1007/s43465-024-01224-1
46. Sheth U, Sniderman J, Whelan DB. Early surgery of multiligament knee injuries may yield better results than delayed surgery: a systematic review. Journal of ISAKOS. 2019;4(1):26–32. doi:10.1136/jisakos-2015-000021
47. Mook WR, Miller MD, Diduch DR, Hertel J, Boachie-Adjei Y, Hart JM. Multiple-ligament knee injuries: a systematic review of the timing of operative intervention and postoperative rehabilitation. J Bone Joint Surg Am. 2009;91(12):2946–2957. doi:10.2106/JBJS.H.01328
48. Jiang W, Yao J, He Y, Sun W, Huang Y, Kong D. The timing of surgical treatment of knee dislocations: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2015;23(10):3108–3113. doi:10.1007/s00167-014-3435-1
49. Fanelli GC, Fanelli DG. Multiple ligament knee injuries. J Knee Surg. 2018;31(5):399–409. doi:10.1055/s-0038-1636910
50. Goyal A, Kumar S, Mishra P, Mehta N, Joshi D, Sinha S. Long term outcome of early single stage surgery in multi-ligamentous injuries of knee. J Clin Orthop Trauma. 2020;11(Suppl 4):S650–S656. doi:10.1016/j.jcot.2020.05.018
51. Mather RC 3rd, Hettrich CM, Dunn WR, et al. Cost-effectiveness analysis of early reconstruction versus rehabilitation and delayed reconstruction for anterior cruciate ligament tears. Am J Sports Med. 2014;42(7):1583–1591. doi:10.1177/0363546514530866
52. Hoit G, Chahal J, Khan R, Rubacha M, Nauth A, Whelan DB. Early compared with delayed reconstruction in multiligament knee injury: a retrospective propensity analysis. J Bone Joint Surg Am. 2024;106(20):1903–1909. doi:10.2106/JBJS.23.00795
53. Mescher PK, Anderson AB, Dekker TJ, Pav V, Dickens JF. Characterization of cartilage injury and associated treatment at the time of primary anterior cruciate ligament reconstruction. J Knee Surg. 2022;35(11):1175–1180. doi:10.1055/s-0042-1748173
54. Dekker TJ, et al. “early compared with delayed reconstruction in multiligament knee injury. a retrospective propensity analysis”. J Bone Joint Surg Am. 2024;106(20):e44. doi:10.2106/JBJS.24.00742
55. Stannard JP, Nuelle CW, McGwin G, Volgas DA. Hinged external fixation in the treatment of knee dislocations: a prospective randomized study. J Bone Joint Surg Am. 2014;96(3):184–191. doi:10.2106/JBJS.L.01603
56. Stannard JP, Sheils TM, McGwin G, Volgas DA, Alonso JE. Use of a hinged external knee fixator after surgery for knee dislocation. Arthroscopy. 2003;19(6):626–631. doi:10.1016/s0749-8063(03)00125-7
57. Angelini FJ, Helito CP, Bonadio MB, et al. External fixator for treatment of the sub-acute and chronic multi-ligament-injured knee. Knee Surg Sports Traumatol Arthrosc. 2015;23(10):3012–3018. doi:10.1007/s00167-015-3719-0
58. Angelini FJ, Helito CP, Bonadio MB, Pecora JR, Camanho GL. Surgical management of knee dislocations with ligament reconstruction associated with a hinged external fixator. Orthop Traumatol Surg Res. 2015;101(1):77–81. doi:10.1016/j.otsr.2014.11.001
59. Marcacci M, Zaffagnini S, Bonanzinga T, Pizzoli A, Manca M, Caiaffa E. Surgical technique: articulated external fixator for treatment of complex knee dislocation. Clin Orthop Relat Res. 2012;470(3):869–876. doi:10.1007/s11999-011-2062-0
60. Zaffagnini S, Iacono F, Lo Presti M, et al. A new hinged dynamic distractor, for immediate mobilization after knee dislocations: technical note. Arch Orthop Trauma Surg. 2008;128(11):1233–1237. doi:10.1007/s00402-007-0515-4
61. Stannard J. Fracture Dislocation of the Knee. J Knee Surg. 2016;29(4):300–302. doi:10.1055/s-0036-1583177
62. Geiger EJ, Arzeno AH, Medvecky MJ.Hinged-knee external fixator used to reduce and maintain subacute tibiofemoral coronal subluxation. Am J. 2016;45(7):E497–E502.
63. Liu CC, Gao X, Xu M, Kong ZG. Surgical management of posterior knee dislocation associated with extensor apparatus rupture. Knee. 2017;24(5):940–948. doi:10.1016/j.knee.2017.05.023
64. Takahashi T, Matsumura T, Ishihara K, Hiyama S, Takeshita K. Open knee dislocation with a patellar tendon rupture: result of staged surgical repair. SAGE Open Med Case Rep. 2019;7:2050313X18823102. doi:10.1177/2050313X18823102
65. Pardiwala DN, Subbiah K, Rao N, Yathiraj BR. Chronic irreducible knee dislocations: outcomes following open reduction and reconstructive surgery. J Knee Surg. 2023;36(11):1116–1124. doi:10.1055/s-0042-1750062
66. Simonian PT, Wickiewicz TL, Hotchkiss RN, Warren RF. Chronic knee dislocation: reduction, reconstruction, and application of a skeletally fixed knee hinge. A report of two cases. Am J Sports Med. 1998;26(4):591–596. doi:10.1177/03635465980260042201
67. Richter M, Lobenhoffer P. Chronic posterior knee dislocation: treatment with arthrolysis, posterior cruciate ligament reconstruction and hinged external fixation device. Injury. 1998;29(7):546–549. doi:10.1016/s0020-1383(98)00095-3
68. Anazor FC, Baryeh K, Davies NC. Knee joint dislocation: overview and current concepts. Br J Hosp Med. 2021;82(12):1–10. doi:10.12968/hmed.2021.0466
69. Bryant BJ, Musahl, V, Harner, CD, et al. Insall & Scott Surgery of the Knee. 2012:565–581.
70. Wascher DC. High-velocity knee dislocation with vascular injury. Treatment principles. Clin Sports Med. 2000;19(3):457–477. doi:10.1016/s0278-5919(05)70218-0
71. Lamont J. external fixation of the knee. In: Siliski JM, editor. Traumatic Disorders of the Knee. New York, NY: Springer; 1994.
72. Held M, Schenck RC, Khanduja V, et al. Prioritised challenges in the management of acute knee dislocations are stiffness, obesity, treatment delays and associated limb-threatening injuries: a global consensus study. J ISAKOS. 2021;6(4):193–198. doi:10.1136/jisakos-2020-000565
73. Werner BC, Gwathmey FW, Higgins ST, Hart JM, Miller MD. Ultra-low velocity knee dislocations: patient characteristics, complications, and outcomes. Am J Sports Med. 2014;42(2):358–363. doi:10.1177/0363546513508375
74. Burrus MT, Werner BC, Griffin JW, Gwathmey FW, Miller MD. Diagnostic and management strategies for multiligament knee injuries: a critical analysis review. JBJS Rev. 2016;4(2):e1. doi:10.2106/JBJS.RVW.O.00020
75. Wascher DC, Dvirnak PC, DeCoster TA. Knee dislocation: initial assessment and implications for treatment. J Orthop Trauma. 1997;11(7):525–529. doi:10.1097/00005131-199710000-00011
76. Bodendorfer BM, Keeling LE, Michaelson EM, et al. Predictors of knee arthrofibrosis and outcomes after arthroscopic lysis of adhesions following ligamentous reconstruction: a retrospective case-control study with over two years’ average follow-up. J Knee Surg. 2019;32(6):536–543. doi:10.1055/s-0038-1655741
77. Pape HC, Lefering R, Butcher N, et al. The definition of polytrauma revisited: an international consensus process and proposal of the new ‘Berlin definition’. J Trauma Acute Care Surg. 2014;77(5):780–786. doi:10.1097/TA.0000000000000453
78. Burrus MT, Werner BC, Cancienne JM, Miller MD. Simultaneous bilateral multiligamentous knee injuries are associated with more severe multisystem trauma compared to unilateral injuries. Knee Surg Sports Traumatol Arthrosc. 2015;23(10):3038–3043. doi:10.1007/s00167-015-3720-7
79. Woodmass JM, Johnson NR, Mohan R, Krych AJ, Levy BA, Stuart MJ. Poly-traumatic multi-ligament knee injuries: is the knee the limiting factor? Knee Surg Sports Traumatol Arthrosc. 2018;26(9):2865–2871. doi:10.1007/s00167-017-4784-3
80. Smith BP, Goldberg AJ, Gaughan JP, Seamon MJ. A comparison of injury severity score and new injury severity score after penetrating trauma: a prospective analysis. J Trauma Acute Care Surg. 2015;79(2):269–274. doi:10.1097/TA.0000000000000753
81. Sutherland AG, Johnston AT, Hutchison JD. The new injury severity score: better prediction of functional recovery after musculoskeletal injury. Value Health. 2006;9(1):24–27. doi:10.1111/j.1524-4733.2006.00077.x
82. Darabos N, Gusic N, Vlahovic T, Darabos A, Popovic I, Vlahovic I. Staged management of knee dislocation in polytrauma injured patients. Injury. 2013;44(Suppl 3):S40–S45. doi:10.1016/S0020-1383(13)70196-7
83. Mühlenfeld N, Berthold DP, Münch LN, et al. Epidemiology of complete knee dislocations: an updated classification system. Arch Orthop Trauma Surg. 2022;142(10):2711–2718. doi:10.1007/s00402-021-04079-5
84. Whelan DB, Dold AP, Trajkovski T, Chahal J. Risk factors for the development of heterotopic ossification after knee dislocation. Clin Orthop Relat Res. 2014;472(9):2698–2704. doi:10.1007/s11999-014-3730-7
85. Szymski D, Huber L, Riedl M, Rupp M, Alt V, Weber J. No effect of dislocation status at arrival in emergency department on outcome of knee joint dislocations. Knee Surg Sports Traumatol Arthrosc. 2024;32(6):1376–1383. doi:10.1002/ksa.12154
86. Lian J, Patel NK, Nickoli M, et al. Obesity is associated with significant morbidity after multiligament knee surgery [published correction appears in. J Knee Surg. 2020;33(6):e1. doi:10.1055/s-0039-1681027
87. Teissier V, Tresson P, Gaudric J, et al. Importance of early diagnosis and care in knee dislocations associated with vascular injuries. Ann Vasc Surg. 2019;61:238–245. doi:10.1016/j.avsg.2019.04.016
88. Scarcella NR, Weinberg DS, Bowen S, Vallier HA. Clinical and functional results of 119 patients with knee dislocations. J Orthop Trauma. 2017;31(7):380–386. doi:10.1097/BOT.0000000000000839
89. King JJ 3rd, Cerynik DL, Blair JA, Harding SP, Tom JA. Surgical outcomes after traumatic open knee dislocation. Knee Surg Sports Traumatol Arthrosc. 2009;17(9):1027–1032. doi:10.1007/s00167-009-0721-4
90. Javidan P, Owen J, Cutuk A, Watson T, Kaar S. How do spanning external fixators on knee dislocation patients affect the use of MRI and knee stability? J Knee Surg. 2015;28(3):247–254. doi:10.1055/s-0034-1386579
91. Hanley J, Westermann R, Cook S, et al. Factors associated with knee stiffness following surgical management of multiligament knee injuries. J Knee Surg. 2017;30(6):549–554. doi:10.1055/s-0036-1593624
92. Egol KA, Bazzi J, McLaurin TM, Tejwani NC. The effect of knee-spanning external fixation on compartment pressures in the leg. J Orthop Trauma. 2008;22(10):680–685. doi:10.1097/BOT.0b013e31818afbdb
93. Chowdhry M, Burchette D, Whelan D, Nathens A, Marks P, Wasserstein D. Knee dislocation and associated injuries: an analysis of the American College of Surgeons National Trauma Data Bank. Knee Surg Sports Traumatol Arthrosc. 2020;28(2):568–575. doi:10.1007/s00167-019-05712-y
94. Bi AS, Mojica ES, Markus DH, et al. Risk of postoperative stiffness following multiligamentous knee injury surgery is not affected by obesity: a multicenter study. Arthroscopy. 2022;38(12):3175–3181. doi:10.1016/j.arthro.2022.06.017
95. Barrow AE, Sheean AJ, Burns TC. Return to duty following combat-related multi-ligamentous knee injury. Injury. 2017;48(4):861–865. doi:10.1016/j.injury.2017.02.019
96. Sobrado MF, Giglio PN, Bonadio MB, et al. High incidence of osteoarthritis observed in patients at short- to midterm follow-up after delayed multiligament knee reconstruction. J Knee Surg. 2022;35(10):1147–1152. doi:10.1055/s-0040-1722348
97. Lawrance SE, Shelbourne KD. Treatment and Rehabilitation of Arthrofibrosis of the Knee.
98. Balato G, Rizzo M, Ascione T, Smeraglia F, Mariconda M. Re-infection rates and clinical outcomes following arthrodesis with intramedullary nail and external fixator for infected knee prosthesis: a systematic review and meta-analysis. BMC Musculoskelet Disord. 2018;19(1):361. doi:10.1186/s12891-018-2283-4
99. Salar M, Dougherty PJ. Infections associated with temporary external fixation. J Surg Orthop Adv. 2020;29(2):73–76.
100. Stenquist DS, Yeung CM, Guild T, Weaver MJ, Harris MB, Von Keudell AG. Is It safe to prep the external fixator in situ during staged ORIF of bicondylar tibial plateau fractures? a retrospective comparative cohort study. J Orthop Trauma. 2022;36(8):382–387. doi:10.1097/BOT.0000000000002334
101. Moon TJ, Haase L, Haase D, Ochenjele G, Wise B, Napora J. Are infection rates increased after sterilization of the external fixator during staged internal fixation of high-energy tibial plateau fractures? J Orthop Trauma. 2022;36(10):530–534. doi:10.1097/BOT.0000000000002371
102. Kazmers N, Fragomen A, Rozbruch S. Prevention of pin site infection in external fixation: a review of the literature. Strategies in Trauma and Limb Reconstruction. 2016;11(2):75–85. doi:10.1007/s11751-016-0256-4
103. Zych G. Complications of External Fixation. In: Seligson D, Mauffrey C, Roberts C, editors. External Fixation in Orthopedic Traumatology. London: Springer London; 2012:173–184.
104. Hodel S, Link BC, Babst R, et al. Perioperative management of external fixation in staged protocols: an international survey. Eur J Orthop Surg Traumatol. 2018;28(4):565–572. doi:10.1007/s00590-018-2135-9
105. Risitano S, Rea A, Garofalo G, et al. Impact of surgical timing, fasciotomy, and external fixation on infection risk in tibial plateau fractures. J Pers Med. 2025;15(3):108. doi:10.3390/jpm15030108
106. Hardeski D, Gaski G, Joshi M, et al. Can applied external fixators be sterilized for surgery? A prospective cohort study of orthopaedic trauma patients. Injury. 2016;47(12):2679–2682. doi:10.1016/j.injury.2016.07.009
107. Stinner DJ, Beltran MJ, Masini BD, Wenke JC, Hsu JR. Bacteria on external fixators: which prep is best? J Trauma Acute Care Surg. 2012;72(3):760–764. doi:10.1097/TA.0b013e31823c97f5
108. Hak DJ, Wiater PJ, Williams RM, Pierson CL. The effectiveness of standard povidone iodine surgical preparation in decontaminating external fixator components. Injury. 2005;36(12):1449–1452. doi:10.1016/j.injury.2005.05.006
109. Parameswaran AD, Roberts CS, Seligson D, Voor M. Pin tract infection with contemporary external fixation: how much of a problem? J Orthop Trauma. 2003;17(7):503–507. doi:10.1097/00005131-200308000-00005
110. Acklin YP, Potocnik P, Sommer C. Compartment syndrome in dislocation and non-dislocation type proximal tibia fractures: analysis of 356 consecutive cases. Arch Orthop Trauma Surg. 2012;132(2):227–231. doi:10.1007/s00402-011-1408-0
111. Lethaby A, Temple J, Santy‐Tomlinson J.Pin site care for preventing infections associated with external bone fixators and pins.Cochrane Database of Systematic Reviews.2013;12.PubMed PMID: CD004551. doi:10.1002/14651858.CD004551.pub3
112. Roth F, Cagienard F, Link BC, et al. Primary or secondary wound healing of the pin sites after removal of the external fixator: study protocol for a prospective, randomized controlled, monocenter trial. Trials. 2020;21(1):205. doi:10.1186/s13063-020-4087-8
113. Tudu L. Betadine dressing versus surgical spirit dressing in prevention of pin site infection among the patients with external skeletal fixators. International Journal of Nursing Care. 2019;7(1):30–38. doi:10.37506/ijonc.v7i1.7655
114. Makhdoom A, Baloch R, Sheikh T, et al. The role of chlorhexidine in the prevention of pin tract infection as compared to povidone-iodine in patients managed by ilizarov circular fixator. PJMHS. 2021;15(5):1751–1754. doi:10.53350/pjmhs211551751
115. de Fortuny LM, Santoli A, Giovanoulis V, et al. How do surgically treated multiligamentous knee injuries affect overall complication rate and especially stiffness? A systematic review. Knee Surg Relat Res. 2025;37(1):18. doi:10.1186/s43019-025-00270-9
116. Fahlbusch H, Krivec L, Müller S, Reiter A, Frosch KH, Krause M. Arthrofibrosis is a common but poorly defined complication in multiligament knee injuries: a systematic review. Arch Orthop Trauma Surg. 2023;143(8):5117–5132. doi:10.1007/s00402-022-04730-9
117. Noyes FR, Berrios-Torres S, Barber-Westin SD, Heckmann TP. Prevention of permanent arthrofibrosis after anterior cruciate ligament reconstruction alone or combined with associated procedures: a prospective study in 443 knees. Knee Surg Sports Traumatol Arthrosc. 2000;8(4):196–206. doi:10.1007/s001670000126
118. Fahlbusch H, Neumann M, Frings J, Frosch KH, Krause M. Surgically treated acute knee dislocations with knee stiffness perform equally as well as non-stiff knees when treated with arthroscopic arthrolysis. Knee. 2024;51:114–119. doi:10.1016/j.knee.2024.08.017
119. Lamba A, Boos AM, Krych AJ, Stuart MJ, Hevesi M, Levy BA. Satisfactory outcomes and improved range of motion with arthroscopic lysis of adhesions and manipulation for arthrofibrosis after multiligamentous knee reconstruction. Arthrosc Sports Med Rehabil. 2023;5(5):100784. doi:10.1016/j.asmr.2023.100784
120. Mills WJ, Tejwani N. Heterotopic ossification after knee dislocation: the predictive value of the injury severity score. J Orthop Trauma. 2003;17(5):338–345. doi:10.1097/00005131-200305000-00004
121. Stannard JP, Wilson TC, Sheils TM, G M Jr, Volgas DA, Alonso JE. Heterotopic ossification associated with knee dislocation. Arthroscopy. 2002;18(8):835–839. doi:10.1053/jars.2002.32842
122. Zhang J, Song GY, Feng H. Development of heterotopic ossification after multiple-ligament reconstruction of the knee joint: incidence and explanatory factor analysis. Knee. 2020;27(3):642–648. doi:10.1016/j.knee.2020.04.012
123. Almangour W, Schnitzler A, Salga M, Debaud C, Denormandie P, Genêt F. Recurrence of heterotopic ossification after removal in patients with traumatic brain injury: a systematic review. Ann Phys Rehabil Med. 2016;59(4):263–269. doi:10.1016/j.rehab.2016.03.009
124. Charnley G, Judet T, Garreau de Loubresse C, Mollaret O. Excision of heterotopic ossification around the knee following brain injury. Injury. 1996;27(2):125–128. doi:10.1016/0020-1383(95)00180-8
125. Furia JP, Pellegrini VD. Heterotopic ossification following primary total knee arthroplasty. J Arthroplasty. 1995;10(4):413–419. doi:10.1016/s0883-5403(05)80139-1
126. Gosselin RA, Belzer JP, Contreras DM. Heterotopic ossification of the patellar tendon following intramedullary nailing of the tibia: report on two cases. J Trauma. 1993;34(1):161–163. doi:10.1097/00005373-199301000-00033
127. Tornetta P 3rd, Barbera C. Severe heterotopic bone formation in the knee after tibial intramedullary nailing. J Orthop Trauma. 1992;6(1):113–115.
128. Agarwal S, Loder SJ, Breuler C, et al. Strategic targeting of multiple BMP receptors prevents trauma-induced heterotopic ossification. Mol Ther. 2017;25(8):1974–1987. doi:10.1016/j.ymthe.2017.01.008
129. Dey D, Wheatley BM, Cholok D, et al. The traumatic bone: trauma-induced heterotopic ossification. Transl Res. 2017;186:95–111. doi:10.1016/j.trsl.2017.06.004
130. Gugala Z, Olmsted-Davis EA, Xiong Y, Davis EL, Davis AR. Trauma-induced heterotopic ossification regulates the blood-nerve barrier. Front Neurol. 2018;9:408. doi:10.3389/fneur.2018.00408
131. Hwang CD, Pagani CA, Nunez JH, et al. Contemporary perspectives on heterotopic ossification. JCI Insight. 2022;7(14):e158996. doi:10.1172/jci.insight.158996
132. Kraft CT, Agarwal S, Ranganathan K, et al. Trauma-induced heterotopic bone formation and the role of the immune system: a review. J Trauma Acute Care Surg. 2016;80(1):156–165. doi:10.1097/TA.0000000000000883
133. Lawand J, Loeffelholz Z, Khurshid B, Barcak E. Heterotopic ossification after trauma. Orthop Clin North Am. 2023;54(1):37–46. doi:10.1016/j.ocl.2022.08.007
134. Martin EC, Qureshi AT, Llamas CB, et al. Trauma induced heterotopic ossification patient serum alters mitogen activated protein kinase signaling in adipose stem cells. J Cell Physiol. 2018;233(9):7035–7044. doi:10.1002/jcp.26504
135. Ohlmeier M, Krenn V, Thiesen DM, Sandiford NA, Gehrke T, Citak M. Heterotopic ossification in orthopaedic and trauma surgery: a histopathological ossification score. Sci Rep. 2019;9(1):18401. doi:10.1038/s41598-019-54986-2
136. Berndt C, Ganko A, Whitehouse SL, Crawford RW. Heterotopic ossification within an arthroscopic portal after uneventful partial meniscectomy. Knee. 2008;15(5):416–418. doi:10.1016/j.knee.2008.05.003
137. Kumar SNL, Ravi S, Subramaniam KN, Kumar SNJ, Sowmya Priya A. Heterotopic ossification after knee surgery, arthroscopy is not an exception!!!! J Orthop Case Rep. 2021;11(1):41–44. doi:10.13107/jocr.2021.v11.i02.2018
138. Li C, Huang Z, Anil KC, Lao C, Wu Q, Jiang H. Heterotopic ossification in the post cruciate ligament of the knee: a case report and literature review. BMC Musculoskelet Disord. 2021;22(1):304. doi:10.1186/s12891-021-04176-x
139. Patton WC, Tew WM. Periarticular heterotopic ossification after multiple knee ligament reconstructions. A report of three cases. Am J Sports Med. 2000;28(3):398–401. doi:10.1177/03635465000280032001
140. Zhou L, Gee SM, Hansen JA, Posner MA. Heterotopic ossification after arthroscopic procedures: a scoping review of the literature. Orthop J Sports Med. 2022;10(1):23259671211060040. doi:10.1177/23259671211060040
141. Chalmers J, Gray DH, Rush J. Observations on the induction of bone in soft tissues. J Bone Joint Surg Br. 1975;57(1):36. doi:10.1302/0301-620X.57B1.36
142. Jones CA, Seilern Und Aspang J, Homes JS, et al. Incidence and risk factors of hetertopic ossification in the knee after reamed tibial nailing. J Am Acad Orthop Surg Glob Res Rev. 2024;8(2):
143. Ogilvie-Harris DJ, Sekyi-Otu A. Periarticular heterotopic ossification: a complication of arthroscopic anterior cruciate ligament reconstruction using a two-incision technique. Arthroscopy. 1995;11(6):676–679. doi:10.1016/0749-8063(95)90108-6
144. Stark E, Stucken C, Trainer G, Tornetta P. Compartment syndrome in Schatzker type VI plateau fractures and medial condylar fracture-dislocations treated with temporary external fixation. J Orthop Trauma. 2009;23(7):502–506. doi:10.1097/BOT.0b013e3181a18235
145. Lee JK, Koo JW, Jeong SY, Choi S, Park KC, Hwang KT. Perioperative symptomatic venous thromboembolism after immediate chemoprophylaxis in patients with pelvic and lower-extremity fractures. Sci Rep. 2020;10(1):5431. doi:10.1038/s41598-020-62333-z
146. Niikura T, Sakai Y, Lee SY, Iwakura T, Kuroda R, Kurosaka M. Rate of venous thromboembolism after complex lower-limb fracture surgery without pharmacological prophylaxis. J Orthop Surg. 2015;23(1):37–40. doi:10.1177/230949901502300109
147. Sems SA, Levy BA, Dajani K, Herrera DA, Templeman DC. Incidence of deep venous thrombosis after temporary joint spanning external fixation for complex lower extremity injuries. J Trauma. 2009;66(4):1164–1166. doi:10.1097/TA.0b013e318183801e
148. Roberts DJ, Panagiotidou A, Sewell M, Calder P, Goodier D. The incidence of deep vein thrombosis and pulmonary embolism with the elective use of external fixators. Strategies Trauma Limb Reconstr. 2015;10(2):67–71. doi:10.1007/s11751-015-0219-1
149. Bahloul M, Dlela M, Bouchaala K, et al. Post-traumatic pulmonary embolism: incidence, physiopathology, risk factors of early occurrence, and impact outcome. A narrative review. Am J Cardiovasc Dis. 2020;10(4):432–443.
150. Jia Q, Peng Z, Huang A, et al. Is fracture management merely a physical process? Exploring the psychological effects of internal and external fixation. J Orthop Surg Res. 2024;19(1):231. doi:10.1186/s13018-024-04655-6
151. Richard HM, Nguyen DC, Birch JG, Roland SD, Samchukov MK, Cherkashin AM. Clinical implications of psychosocial factors on pediatric external fixation treatment and recommendations. Clin Orthop Relat Res. 2015;473(10):3154–3162. doi:10.1007/s11999-015-4276-z
152. Abulaiti A, Yilihamu Y, Yasheng T, Alike Y, Yusufu A. The psychological impact of external fixation using the Ilizarov or Orthofix LRS method to treat tibial osteomyelitis with a bone defect. Injury. 2017;48(12):2842–2846. doi:10.1016/j.injury.2017.10.036
153. Marcel AJ, Alaia EF, Alaia MJ, Katz LD, Medvecky MJ, Porrino J. Perspectives and institutional policies on patient safety and image quality regarding the use of knee-spanning external fixators in MRI: a survey study of the society of skeletal radiology. Skeletal Radiol. 2024;53(3):525–536. doi:10.1007/s00256-023-04445-x
154. Lo L, Jubouri S, Mulligan ME. MRI of traumatic knee dislocation: a study to evaluate safety and image quality for patients with knee-spanning stabilization devices. Curr Probl Diagn Radiol. 2022;51(3):317–322. doi:10.1067/j.cpradiol.2021.04.002
155. Box MW, Marsh L, Major J, Puga TB, Poffenbarger MC, Riehl JT. Safety and utility of magnetic resonance imaging of patients with external fixators: a systematic review. OTA Int. 2025;8(2):e403. doi:10.1097/OI9.0000000000000403
156. Marcel AJ, Green JS, Alaia EF, Alaia MJ, Katz LD, Medvecky MJ. Patient Safety in MRI with the use of a joint-spanning external fixator for knee dislocation: a critical analysis review. JBJS Rev. 2023;11(8):
157. Elsissy P, Akpolat YT, Chien A, Cheng WK. MRI evaluation of the knee with non-ferromagnetic external fixators: cadaveric knee model. Eur J Orthop Surg Traumatol. 2015;25(5):933–939. doi:10.1007/s00590-015-1655-9
158. Johnson JP, Kleiner J, Klinge SA, McClure PK, Hayda RA, Born CT. Increased incidence of vascular injury in obese patients with knee dislocations. J Orthop Trauma. 2018;32(2):82–87. doi:10.1097/BOT.0000000000001027
159. Lau BC, Varsheya K, Morriss N, Wickman J, Kirkendall D, Abrams G. Single-stage surgical treatment of multi-ligament knee injuries results in lower cost and fewer complications and unplanned reoperations compared with staged treatment. Arthrosc Sports Med Rehabil. 2022;4(5):e1659–e1666. doi:10.1016/j.asmr.2022.06.012
160. Chaus GW, Dukes C, Hak DJ, Mauffrey C, Mark Hammerberg E. Analysis of usage and associated cost of external fixators at an urban level 1 trauma centre. Injury. 2014;45(10):1611–1613. doi:10.1016/j.injury.2014.04.031
161. Padhi NR, Padhi P. Use of external fixators for open tibial injuries in the rural third world: panacea of the poor? Injury. 2007;38(2):150–159. doi:10.1016/j.injury.2006.08.053
162. Dirschl DR, Smith IJ. Reuse of external skeletal fixator components: effects on costs and complications. J Trauma. 1998;44(5):855–858. doi:10.1097/00005373-199805000-00018
163. Hayek KR, Parikh HR, McCreary DL, et al. Cost variation in temporizing external fixation of tibial plateau fractures. J Orthop Trauma. 2019;33(Suppl 7):S5–S10. doi:10.1097/BOT.0000000000001620
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.