Back to Journals » Orthopedic Research and Reviews » Volume 15
Knee Pain After Retrograde Intramedullary Nailing with Surgical Implant Generation Network of Femur Shaft Fractures at Public Hospitals in Bahir Dar City, Ethiopia: Analysis of 6-Months Follow-Up Results
Authors Birlie T, Biresaw B, Yadeta E ![]() , Getachew T
, Getachew T ![]() , Debella A
, Debella A ![]() , Eyeberu A
, Eyeberu A ![]()
Received 27 January 2023
Accepted for publication 6 April 2023
Published 12 April 2023 Volume 2023:15 Pages 59—68
DOI https://doi.org/10.2147/ORR.S406176
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Tsegalem Birlie,1 Biniam Biresaw,2 Elias Yadeta,3 Tamirat Getachew,3 Adera Debella,3 Addis Eyeberu3
1School of Medicine, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 2School of Medicine, College of Health and Medical Sciences, Bahir Dar University, Bahir Dar, Ethiopia; 3School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
Correspondence: Elias Yadeta, School of Nursing and Midwifery, College of Health and Medical Sciences, Haramaya University, P.O. Box: 138, Dire Dawa, Ethiopia, Tel +251924899107, Email [email protected]
Background: The incidence of femur fractures in young and elderly people has increased, particularly in countries with limited resources like Ethiopia. Intra-medullary nailing (IM) has been an effective and cost-effective method of treating long bone shaft fractures, but it can lead to complications such as knee pain.
Purpose: This study aimed to evaluate knee pain and its associated factors following retrograde intramedullary nailing for femur fractures.
Patients and Methods: The study followed 110 patients diagnosed with femur fractures and treated with retrograde SIGN Standard Nail or Fin Nail from January 2020 to December 2022 at two hospitals in Ethiopia. The patients were followed up for at least 6 months, and data were collected from medical charts, patient interviews, and phone calls to patients who did not attend the follow-up appointment. Binary logistic regression analysis was used to identify factors associated with knee pain.
Results: The study showed that 40 patients reported knee pain at 6-months follow-up, making a prevalence of 36.4%. Factors significantly associated with knee pain were a time of injury to nailing (AOR=4.23, 95% CI: 1.28– 13.92), use of a screw to the medial cortex (AOR=9.30, 95% CI: 2.90– 12.74), and fracture site (AOR= 2.67, 95% CI: 14.01– 7.03). Specifically, the longer the time from injury to nailing, the higher the risk of knee pain. The use of a longer screw to the medial cortex and a fracture site were also positively associated with knee pain.
Conclusion: This study concludes that although retrograde intramedullary nail fixation is an effective method for femur fractures, it often results in knee pain. Approximately 4 of 10 patients suffered from knee pain in this study. Avoiding delayed surgical management and minimizing the use of prominent metalwork may reduce knee pain.
Keywords: knee pain, intramedullary nailing, Ethiopia
Introduction
In low- and middle-income nations, traumatic injuries are a major cause of morbidity and mortality.1 Femoral shaft fractures have a significant worldwide impact, with up to 2.9 million fractures occurring each year and low- and middle-income countries (LMICs) are disproportionately affected.2 The average annual incidence of femoral shaft fractures inlow- and middle-income nations ranged from 15.7 to 45.5 per 100,000 persons.2 For instance, in Tanzania, the annual incidence of femoral shaft fractures is as high as 18.4 per 100,00.3 Femur fractures are the most common traumatic injury encountered by orthopaedic surgeons and have a bimodal distribution, with younger people typically experiencing high-energy trauma and older people experiencing lower-energy trauma. These fractures are linked to significant mortality and morbidity and can result in severe injuries including nonunion, delayed union, and implant failure, as well as long-term, irreversible impairments.4 The surgical treatment option is more effective than conservative management.5
Since the 1970s, intramedullary nailing has been widely used to repair shaft fractures and has emerged as the gold standard.6 An intramedullary nail is a metal nail that is surgically inserted into the fractured long bone to straighten and hold fractures. The SIGN Nail is an intramedullary nail secured in place by interlocking screws with a 1–1/2-degree bend at the distal end and a 9-degree bend at the proximal end for simpler insertion. However, the SIGN Fin Nail does not require interlocking screws at the distal end, which makes surgery simpler and significantly faster.7 Early definitive therapy within 24 to 48 hours after systemically the patient is stable lowers the risk of pulmonary problems, infection rates, and death. Recently, the practice of retrograde nailing has been growing in acceptance and its main Indications for use include femur and tibia fractures (floating knee injuries), bilateral femur fractures, pregnancy, and morbidly obese individuals.6
Knee discomfort is the most complaint after retrograde nailing Surgical Implant Generation Network (SIGN).6 Even when surgery is technically successful and the union is achieved following femoral fracture, people nevertheless report impairment and discomfort in the knee. Many scholars agree that after a femoral shaft fracture, knee discomfort poses a serious functional challenge.8 Ricci et al reported knee discomfort in as much as 36% of the individuals with femoral shaft fractures.9 Various studies have reported many complications following intramedullary nailings like knee stiffness, implant failure, no-union, infection and protruding nails.10 One of the most common complications identified secondary to intramedullary nailing of the femur was chronic knee pain.11,12 This may significantly hinder the patient’s ability to do his job and other everyday or recreational activities.13 Its prevalence has been observed to reach 16.1%.10 Several studies have indicated a significant occurrence of knee pain with estimates ranging from 20% to 86% and even 17% of the patients may experience moderate-to-severe pain years after surgery.14,15 Brewster,16 in his systematic review, stressed that 40–53% of the individuals who had retrograde intramedullary nailing may experience knee discomfort.
Despite the use of the SIGN Standard Nail or Fin Nail for femur fractures being supported by growing evidence, little is known about the associated outcome. To the best of the authors’ knowledge, this is the first study to assess the clinical outcome of retrograde SIGN Standard Nail or Fin Nail femoral nails in Ethiopia. Therefore, the objective of this study was to examine knee pain and its associated factors among patients who underwent retrograde femoral nails at Tibebe Ghion Comprehensive Specialized Referral Hospitals (TGCSH) and Felege Hiwot Comprehensive Specialized Hospitals (FHCSH) over 2 years.
Materials and Methods
Study Setting
The study was carried out at TGCSH and FHCSH’s orthopaedics and trauma surgery department. TGCSH and FHCSH are found in the capital city of Amhara Regional State, Bahir Dar city. It is located 565 km from Addis Ababa to the north direction. It was established to serve 2000 people per day when it was first launched in 2011 E.C./2018 G.C. It mostly provides services at low cost or even at free cost to individuals who cannot afford care elsewhere. The hospital has more than 500 beds in all wards, including more than 67 beds in the ward of surgery with a total of 10 orthopaedic surgeons (1 of them is on fellowship) and 24 residents specializing in orthopaedic surgery.17,18 Operations are performed every day of the week for emergency cases and 4 days a week for elective cases. The department has one large operation room with two operating tables. The hospital has a separate Surgical Implant Generation Network (SIGN) follow-up clinic which is used to offer follow-up services for SIGN patients, and report the surgeries. The study was conducted on SIGN patients in SIGN clinics by reviewing charts from the hospital record rooms and online database records from SIGN online surgical database (SOSD). The study was conducted from January 2020 to December 2022.
Study Design
A hospital-based cross-sectional study was carried out using data that had been collected from patients’ medical records, the SIGN online surgical database (SOSD), and patient interviews.
Populations and Eligibility Criteria
All patients who had been admitted to Tibebe Ghion and Felege Hiwot comprehensive specialized hospital’s Orthopedic surgery department with the diagnosis of femoral bone fractures and treated with either SIGN Standard Nail or SIGN Fin Nail using retrograde surgical approach were the source of the population whereas all patients who had operated for femur fractures with either retrograde SIGN Standard Nail or retrograde SIGN Fin Nail with healed fracture from January 1, 2020, to December 31, 2022, at TGSH and FHSH were the study population.
Inclusion and Exclusion Criteria
All patients with femur fractures who underwent either a retrograde SIGN Standard Nail or SIGN Fin Nail between January 1, 2020, to December 31, 2022, at TGSH and completed 6 months of follow-up post-operation were included and patients with incomplete SIGN database online documentation, patients with non-healed femoral fracture and did not access through phone calls were excluded from the study.
Sample Size and Sampling Technique
All patients who underwent either a retrograde SIGN Standard Nail or SIGN Fin Nail for the treatment of femur fracture from January 1, 2020, to December 31, 2022, at TGSH were included and a convenience sampling technique was used to recruit study participants.
Data Collection Tool and Procedure
Data extraction checklists were developed after reviewing relevant existing literature and prepared in English language. Data collectors have used this checklist to extract data from the patient chart, phone interview and SIGN online database. From medical records and the SIGN online database, a list of all patients who underwent surgical intervention for a femoral shaft or femur fracture at the TGRH trauma centre between January 2020 and December 2022 was generated. Thus, a total of 110 with femur fractures which met all the requirements for inclusion in the study were generated. Using the hospital’s database of patient demographic data, which included phone numbers and emergency contact information, attempts were made to call patients who had undergone either a retrograde SIGN standard nail or SIGN Fin Nail. Patients who were successfully contacted were asked to answer a phone survey on their post-operative experience, including knee pain status and 85 patients were successfully contacted. Medical records were obtained from the department of the card room, and a structured checklist was utilized to gather information on the patient’s diagnosis, types of injury, mechanism of injury, location of fracture, surgical approach, and sociodemographic factors (age, sex, and place of residence). Data were collected by three nurses with one public health professional serving as a supervisor.
Data Quality Control
Before the actual data collection, the checklist was pretested and adjusted based on the results. Data collectors received intensive training for 2 days on how to collect the data and keep to keep patients’ information confidentiality.
Outcome Variable
Knee pain: In this study, patient self-report data on knee pain were assessed during follow-up at 6 months and through a phone call if the patient did not come at 6 months of post-operation.
Data Processing and Analysis
EpiData version 3.1 was used to enter the obtained data before being exported to SPSS version 25 for analysis. Microsoft Office Excel was used to draw some figures. Descriptive statistics were used to determine the frequencies and percentages of patients’ characteristics. Tables, figures, and frequency were used to display the results. To examine the association between knee pain and its associated factors, biavirable and multivariable logistic regression analyses were performed. A P-value of 0.05 or below was deemed statistically significant.
Results
Socio-Demographic Characteristics of Study Participants
A follow-up evaluation of 110 patients and their medical records over 6 months was done, with a response rate of 95.6%. Five study participants were excluded because they were not accessed through a phone call to assess knee pain status following retrograde SIGN nail. Regarding the age of the study participants, the mean age was 31.74±13.3 SD years, with ages ranging from 17 to 75 years. The majority of study participants (64.5%) were between 15 and 30 years. In terms of sex, the majority of the cases 87 (79.1%) were male patients (Table 1).
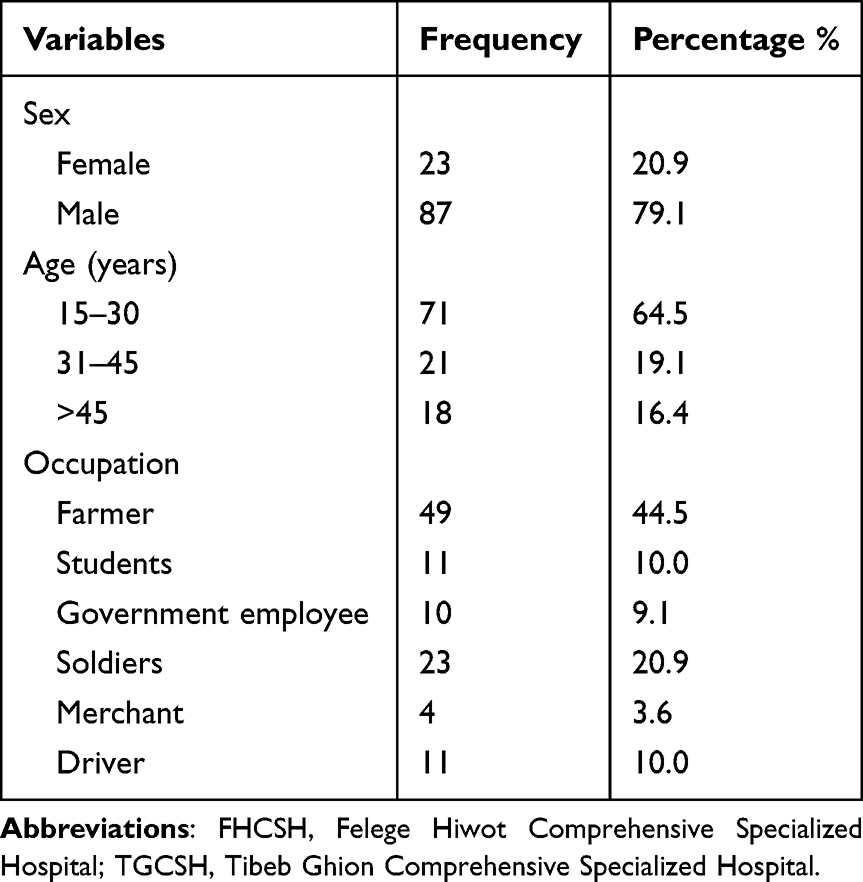 |
Table 1 Socio-Demographic Characteristics of Study Participants at TGCSH and FHCSH, Bahir Dar City, Amhara Region State, Northern Ethiopia, from January 2020 to December 2022, 2022 (n=110) |
Patient-Related Characteristics
A total of 110 patients with femur fractures were treated with either a SIGN Standard Nail or SIGN Fin Nail using a retrograde surgical approach during the study period. The majority of the patients who had femur shaft fractures were farmers. All fractures were reduced and reamed manually. The fractures were either in the middle third (60.9%) or lower (30.1%) of the femoral shaft. Fifty-six (50.9%) of the femur fractures treated with retrograde SIGN Nail were closed. The most common cause of femur fracture was a road traffic accident 54 (49.1%) and mainly affected the middle shaft 66 (60%) followed by distal femoral shaft fracture 44 (40%) (Table 2).
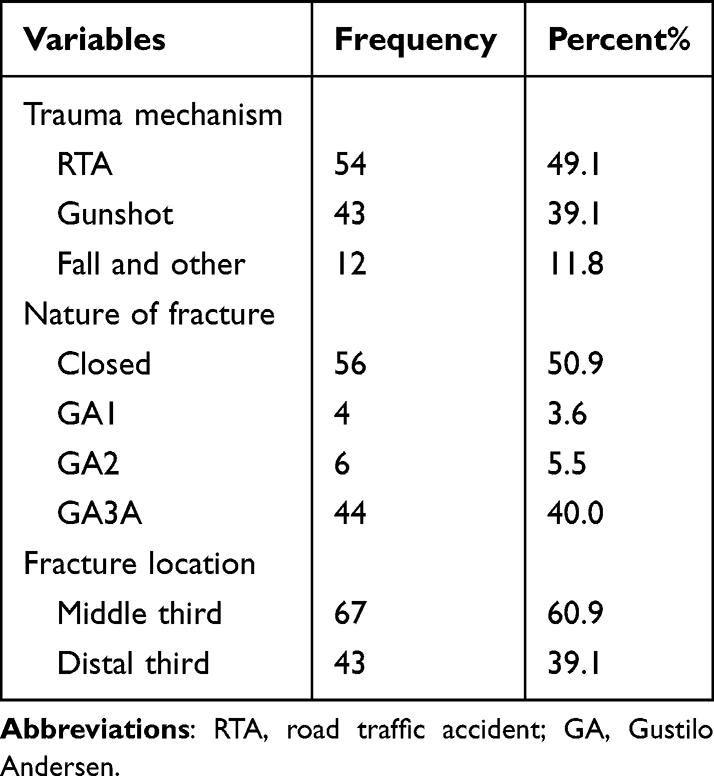 |
Table 2 Injury-Related Characteristics of the Study Participant at TGCSH and FHCSH, Bahir Dar City, Northern Ethiopia, from January 1, 2020, to December 31, 2022 (n=110) |
Treatment-Related Characteristics
The mean interval between fracture and intramedullary nail (IMN) was 9.84±12.15 days. Concerning nail entry (51.80%) of femoral nails were inserted through the medial para patellar (16.40%) lateral para patellar and (31.80%) patellar tendon splitting (Table 3).
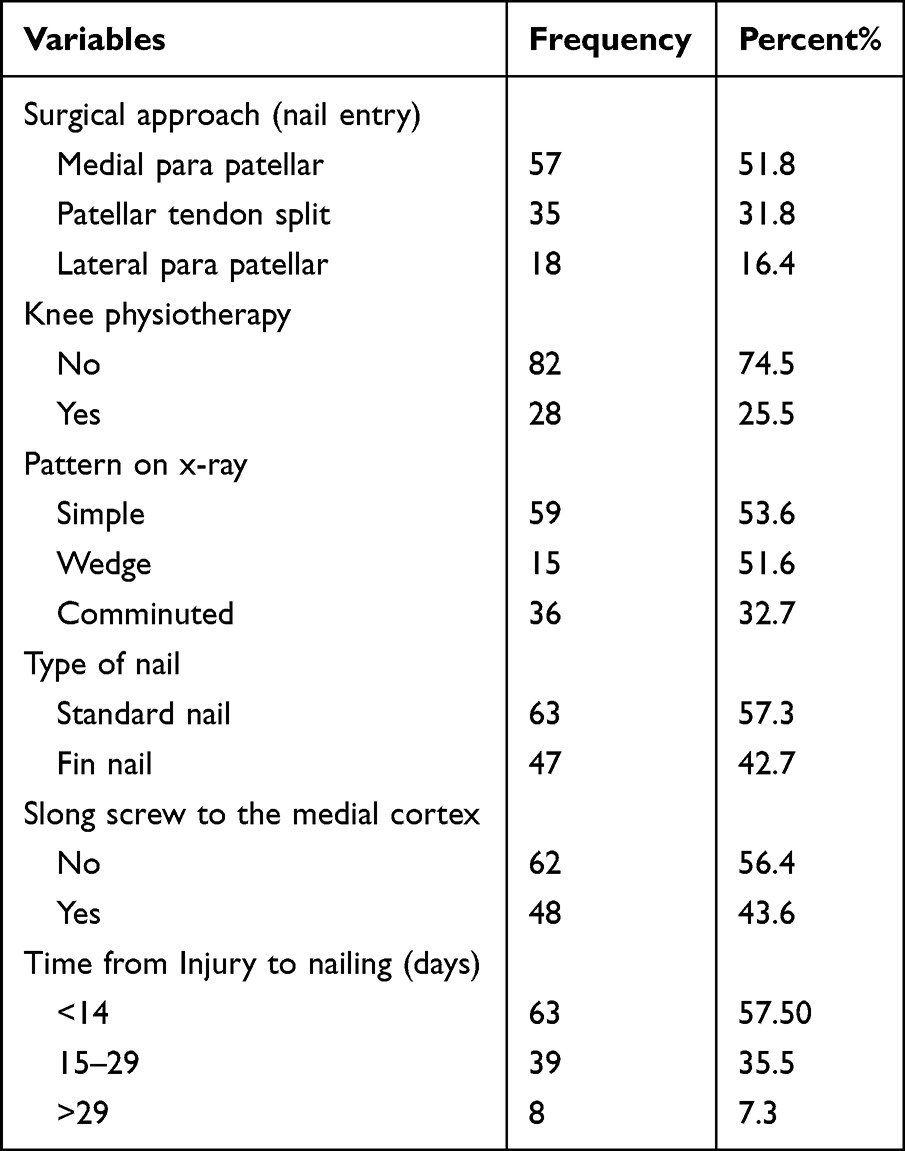 |
Table 3 Treatment-Related Characteristics of the Study Participant at TGCSH and FHCSH, Bahir Dar City, Amhara Regional State, Northern Ethiopia, from January 1, 2020, to December 31, 2022 (n=110) |
Prevalence of Knee Pain
During the follow-up period, we identified 110 cases of femur fracture treated with retrograde SIGN nail from January 2020 to December 2022 and there were 40 cases of knee pain among 110 patients included in the study. This makes the prevalence of knee pain 36.4% (95% CI: 31.36–39.54) among the total patients. The majority of the patients complained of knee pain while walking up/down (34%), squatting (33%) and after long-distance walking (26.4) (Figure 1).
 |
Figure 1 Showing different conditions in which patients noticed knee pain at TGCSH and FHCSH, Bahir Dar city, Amhara Regional state, northern Ethiopia, January 1, 2020 to December 31, 2022 (n=40). |
Associated Factors of Knee Pain
In the binary logistic regression analysis, age of study participants, screw to the medial cortex, time of injury to nailing, and fracture site were associated with knee pain at p-value <0.05.
In multivariable binary logistic regression analysis, time interval from injury to SIGN nail fixation, fracture site and screw penetration to medial cortex were found to be significantly associated with the occurrence of knee pain with a p-value ˂0.05. Those patients treated with retrograde femur SIGN nail and screw penetrate medial cortex has 9 times (AOR=9.30, 95% CI: 2.90–12.74) likely to develop knee pain than the medial cortex is intact. The odds of developing knee pain in cases with fixation done between 15 and 29 days after injury were 4.2 times (AOR=4.23, 95% CI: 1.28–13.92) higher than those cases treated before 15 days. Furthermore, the odds of developing knee pain among patients with distal femur shaft fracture was 2.671 times (AOR=2.67, 95% CI: 14.01–7.03) higher than those patients with middle shaft fracture (Table 4).
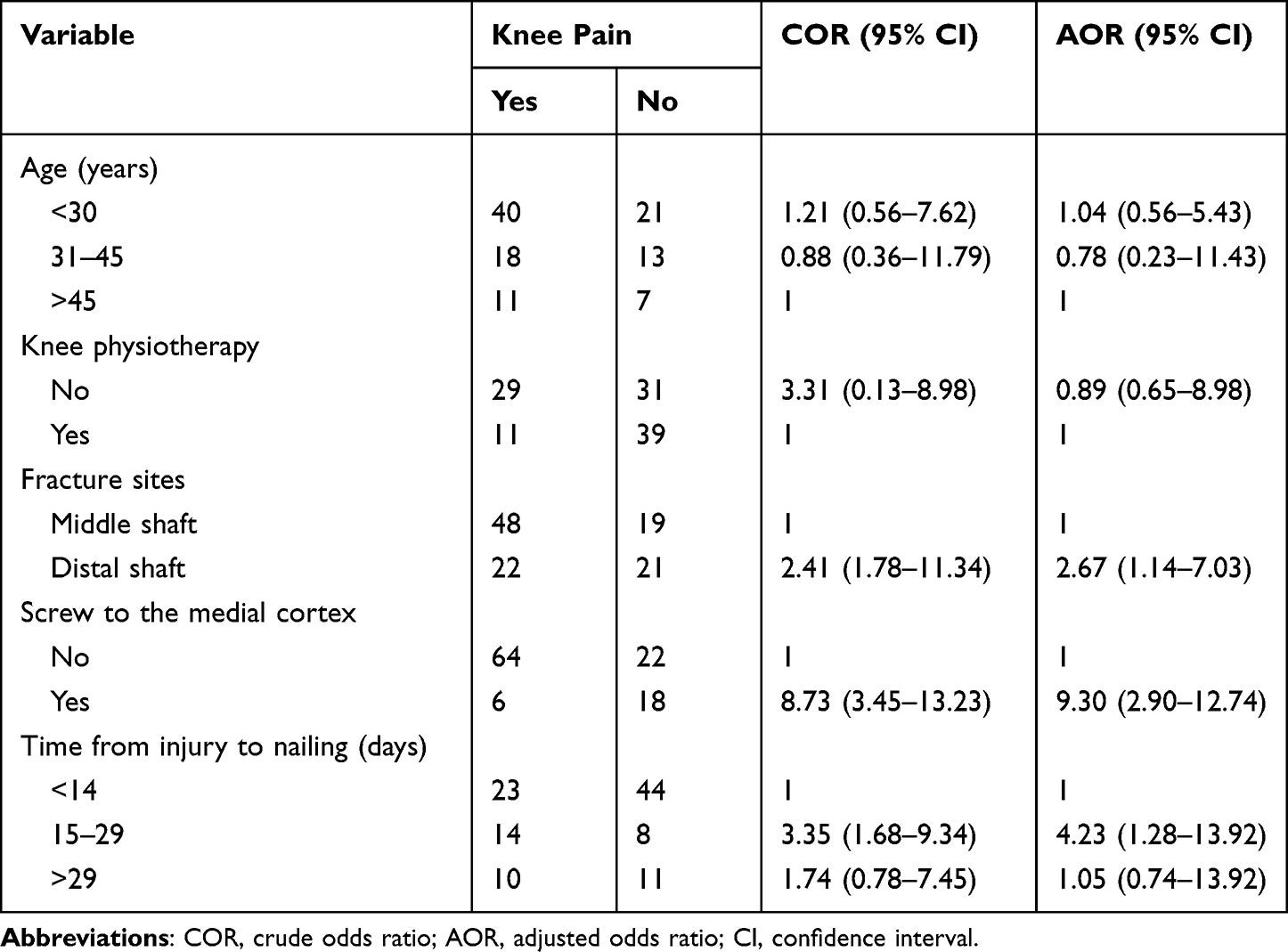 |
Table 4 Bivariable and Multivariable Logistic Regression Analyses of Factors Associated with Knee Pain at TGCSH and FHCSH, Bahir Dar City, Amhara Regional State, Northern Ethiopia, from January 1, 2020 to December 31, 2022 (N=110) |
Discussion
This is the first study conducted in Ethiopia to assess knee pain after retrograde SIGN nail is done for a patient with a femur fracture. After retrograde intramedullary nailing, knee discomfort is one of the most often reported complications. Accordingly, the frequency of knee pain secondary to retrograde SIGN nail treatment for femur fracture in this study was relatively high (36.4%), which implies knee pain remains to be a therapeutic challenge. This finding agreed with the result of the meta-analysis of postoperative complications of retrograde intramedullary nailing in distal femoral fractures,19 which reports knee pain frequently occurs following retrograde intramedullary nailing more than other alternatives. However, the current finding is lower than the reports of Acharya.20 He concluded that up to 70% of the patients have knee pain after a retrograde nail. The possible reason for this discrepancy might be due to variations in the study setting, sample size, study period and socioeconomic status among the study population.
The current finding is, however, higher than what is reported in a study conducted by Shah et al,21 which states that 23% of the patients had complained of knee pain following retrograde SIGN nail treatment. The knee pain has reportedly been attributed to surgical technique and the placement of distal screws.22 Papadokostakis et al23 in their systematic review described knee pain as a common complication of retrograde femoral nailing; however, they observed a statistical variation in the incidence of knee pain between femoral shaft fractures and distal femur fractures. They found that 16.5% of the patients with distal femur fractures treated with a retrograde nail have knee pain, compared to 24.5% of the patients with femoral shaft fractures. The possible reason for the higher prevalence in the present study might be due to the utilization of large sample size and a short follow-up period (6 months) to assess knee status compared to the studies conducted by Shah et al.21
In a study conducted in Tanzania, the most common cause of femur fracture was motor accidents, likewise in the present study the most common cause of femur fracture was a road traffic accident. The most common type of fracture seen was middle shaft fracture which was similar to the finding of Tanzanian studies.24 It has been stated that there are a number of causes for the sharp increase in death rates have attributed to increase in urbanization, bad road conditions, irresponsible driving, ineffective law enforcement and regulation of road safety, and the use of alcohol and recreational drugs while driving.25 For instance, a study from Tanzania concluded that the increases in death rates have been attributed to an increase in the number of motorbikes on the road, especially motorbike-taxi drivers, as well as the lack of legal driving licenses and safety equipment for these vehicles.26 In this study, the mean time from injury to intervention or surgery was 9.8 days. Approximately a similar finding was reported from Uganda which states the mean time to surgery was 13.2 days.27
Shah et al21 demonstrated that use of long screw has significantly associated with the presence of knee pain and they report that 19% of patients desired the removal of symptomatic screws after the union. Brewster, M.16 also reported in his systematic review, 37% of knee discomfort experienced after surgery was related to the use of prominent metal-work and a majority of the cases were resolved if the metal was removed. Similarly, the present study also reported that screwing to the medial cortex was significantly associated with higher odds of developing knee pain. Furthermore, our results were in line with Ostrum et al22 as they note that 21% of patients wanted the removal of e distal screws following union. So interlocking screws of the proper length should be inserted at the knee, and internal rotation oblique radiographs should be taken to confirm the screw’s length in light of the distal femur’s rhomboid shape anatomy. This will help to keep these patients from having to return to the operating room to have their hardware removed because of prominent screws.28
In this study, we observed that fracture site was significantly associated with higher odds of knee pain. The patients who sustained an injury to the distal shaft were more likely to experience knee pain than one who sustained an injury to a middle shaft. In contrast Shah et al21 reported no association between knee pain and fracture site.
Furthermore, the current study identified that the time of injury to nailing is another factor significantly associated with knee pain. We found no study supporting these findings. However, the possible justification by the fact that some activities like running, long-distance walking, squatting, and rising from sitting before the successful union of bones may worsen knee discomfort.
Conclusions
This study concluded that although retrograde intramedullary nail fixation is an effective method for femur fracture, it frequently results in knee pain. In this study, we observed that approximately 4 of 10 patients suffered from knee pain. Time from injury to nailing, use of screw to the medial cortex and fracture site was significantly associated with knee pain. Therefore, knee pain may be prevented by applying early surgical intervention as soon as an accident occurs and avoiding the use of prominent metalwork.
Abbreviations
AOR, adjusted odds ratio; COR, crude odds ratio; FHCSH, Felege Hiwot Comprehensive Specialized Hospital; GA, Gustilo Andersen; IMN, intramedullary nail; LMICs, low-and middle-income countries; RTA, road traffic accident; SIGN, surgical implant generation network; SOSD, SIGN online surgical database; TGCSH, Tibebe Ghion Comprehensive Specialized Hospital.
Data Sharing Statement
The data set supported the results reported in the manuscript are accessible on the reasonable request from the corresponding author.
Ethics Approval and Informed Consent
Ethical clearance was obtained from the Ethical review committee of the faculty of medicine and health sciences of Bahir Dar University (CMHS/IRB 01 with protocol number 499/2020). Before collecting the data, permission was sought from Tibebe Ghion and Felege Hiwot comprehensive specialized hospital and the regional health research bureau. The checklists did not contain any names or other identifying information, and confidentiality was secured throughout the study. The study was carried out following the Declaration of Helsinki.
Consent for Publication
The study did not include images or videos relating to an individual, but concerning other collected and used data in the study, consent information was obtained from the study participants.
Acknowledgments
The authors would like to thank Bahir Dar University for providing the opportunity to conduct this study. We would also like to thank Felege Hiwot and Tibebe Ghion Hospital staff and administration for their assistance during the collection of data, and for providing valuable data about the patients. The authors extend their appreciation to the study participant and data collectors for their contribution.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no funding support for this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Liu Y, Dong Y, Yan X, et al. Global trends and regional differences in non-transport unintentional injuries mortality among children and adolescents, 1990 to 2019: results from the global burden of disease 2019 study. Chin Med J. 2022;135(17):2056–2065. doi:10.1097/CM9.0000000000002315
2. Agarwal-Harding KJ, Meara JG, Greenberg SL, Hagander LE, Zurakowski D, Dyer GS. Estimating the global incidence of femoral fracture from road traffic collisions: a literature review. JBJS. 2015;97(6):e31. doi:10.2106/JBJS.N.00314
3. Conway D, Albright P, Eliezer E, Haonga B, Morshed S, Shearer DW. The burden of femoral shaft fractures in Tanzania. Injury. 2019;50(7):1371–1375. doi:10.1016/j.injury.2019.06.005
4. Henderson CE, Kuhl LL, Fitzpatrick DC, Marsh J. Locking plates for distal femur fractures: is there a problem with fracture healing? J Orthop Trauma. 2011;25:S8–S14. doi:10.1097/BOT.0b013e3182070127
5. Ergün T, Bayraktar MK, Karslioglu B, et al. Evaluating the results of retrograde intramedullary nailing for distal femur fractures: a level 3 trauma center retrospective study. Duzce Med J. 2022;24(1):44–48.
6. Afsari MDA. Femoral shaft fractures. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK556057/.
7. Liu MB, Ali SH, Haonga BT, et al. Surgical Implant Generation Network (SIGN) fin nail versus SIGN standard intramedullary nail for distal diaphyseal femur fractures treated via retrograde approach. Injury. 2019;50(10):1725–1730. doi:10.1016/j.injury.2019.09.009
8. Sanders DW, MacLeod M, Charyk-Stewart T, Lydestad J, Domonkos A, Tieszer C. Functional outcome and persistent disability after isolated fracture of the femur. Can J Surg. 2008;51(5):366–370.
9. Ricci WM, Bellabarba C, Evanoff B, Herscovici D, DiPasquale T, Sanders R. Retrograde versus antegrade nailing of femoral shaft fractures. J Orthop Trauma. 2001;15(3):161–169. doi:10.1097/00005131-200103000-00003
10. Yogi LK, Mahi G, Lokhande M. Evaluation of short term complications following use of retrograde intramedullary femoral interlocking nail for fractures of distal femur. Int J Orthop. 2020;6(3):149–152.
11. Becher S, Ziran B. Retrograde intramedullary nailing of open femoral shaft fractures: a retrospective case series. J Trauma Acute Care Surg. 2012;72(3):696–698. doi:10.1097/TA.0b013e31823cc5ae
12. El Moumni M, Schraven P, ten Duis HJ, Wendt K. Persistent knee complaints after retrograde unreamed nailing of femoral shaft fractures. Acta Orthop Belg. 2010;76(2):219.
13. Katsoulis E, Court-Brown C, Giannoudis P. Incidence and aetiology of anterior knee pain after intramedullary nailing of the femur and tibia. J Bone Joint Surg Br. 2006;88(5):576–580. doi:10.1302/0301-620X.88B5.16875
14. Çepni Ş, Veizi E, Erdoğan Y, Şahin A, Fırat A, Kılıçarslan K. Closure of the femoral medullary canal after retrograde nailing using an in-situ osteochondral autograft–technical trick and a case series. Injury. 2022;53(2):798–801. doi:10.1016/j.injury.2021.10.030
15. El Moumni M, Voogd EH, ten Duis HJ, Wendt KW. Long-term functional outcome following intramedullary nailing of femoral shaft fractures. Injury. 2012;43(7):1154–1158. doi:10.1016/j.injury.2012.03.011
16. Brewster M. Does fixation of femoral fractures using retrograde intramedullary nailing cause long-term knee pain: a systematic review of the literature. Eur J Orthop Surg Traumatol. 2009;19(1):27–31. doi:10.1007/s00590-008-0371-0
17. Tewabe T, Mohammed S, Tilahun Y, et al. Clinical outcome and risk factors of neonatal sepsis among neonates in Felege Hiwot referral hospital, Bahir Dar, Amhara Regional State, North West Ethiopia 2016: a retrospective chart review. BMC Res Notes. 2017;10(1):265. doi:10.1186/s13104-017-2573-1
18. Ferede B, Ayenew A, Belay W. Pelvic fractures and associated injuries in patients admitted to and treated at emergency department of Tibebe Ghion Specialized Hospital, Bahir Dar University, Ethiopia. Orthop Res Rev. 2021;13:73–80. doi:10.2147/orr.s311441
19. Moed BR, Watson JT. Complications of retrograde intramedullary nailing of the femur. Tech Orthop. 2001;16(4):361–371. doi:10.1097/00013611-200112000-00005
20. Acharya K, Rao M. Retrograde nailing for distal third femoral shaft fractures: a prospective study. J Orthop Surg. 2006;14(3):253–258. doi:10.1177/230949900601400305
21. Shah S, Desai P, Mounasamy V. Retrograde nailing of femoral fractures: a retrospective study. Eur J Orthop Surg Traumatol. 2015;25(6):1093–1097. doi:10.1007/s00590-015-1658-6
22. Ostrum RF, DiCicco J, Lakatos R, Poka A. Retrograde intramedullary nailing of femoral diaphyseal fractures. J Orthop Trauma. 1998;12(7):464–468. doi:10.1097/00005131-199809000-00006
23. Papadokostakis G, Papakostidis C, Dimitriou R, Giannoudis P. The role and efficacy of retrograding nailing for the treatment of diaphyseal and distal femoral fractures: a systematic review of the literature. Injury. 2005;36(7):813–822. doi:10.1016/j.injury.2004.11.029
24. Hollis AC, Ebbs SR, Mandari FN. The epidemiology and treatment of femur fractures at a northern Tanzanian referral centre. Pan Afr Med J. 2015;22(1). doi:10.11604/pamj.2015.22.338.8074
25. Clelland SJ, Chauhan P, Mandari FN. The epidemiology and management of tibia and fibula fractures at Kilimanjaro Christian Medical Centre (KCMC) in Northern Tanzania. Pan Afr Med J. 2016;25:51. doi:10.11604/pamj.2016.25.51.10612
26. Sumner SA, Pallangyo AJ, Reddy EA, et al. Effect of free distribution of safety equipment on usage among motorcycle–taxi drivers in Tanzania—a cluster randomised controlled trial. Injury. 2014;45(11):1681–1686. doi:10.1016/j.injury.2014.04.034
27. Sekimpi P, Okike K, Zirkle L, Jawa A. Femoral fracture fixation in developing countries: an evaluation of the Surgical Implant Generation Network (SIGN) intramedullary nail. JBJS. 2011;93(19):1811–1818. doi:10.2106/jbjs.j.01322
28. Lucas SE, Seligson D, Henry SL. Intramedullary supracondylar nailing of femoral fractures: a preliminary report of the GSH supracondylar nail. Clin Orthop Relat Res. 1993;296:200–206. doi:10.1097/00003086-199311000-00034
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.