Back to Journals » Clinical and Experimental Gastroenterology » Volume 17
Jejunal Ectopic Pancreatic Tissue Rest as Lead Point in Patients with Intussusception: A Rare Case Report and Review of Literature
Authors Sefefe WM ![]() , Tesfaw DB, Tebikew AD
, Tesfaw DB, Tebikew AD ![]() , Ayenew AS
, Ayenew AS ![]() , Dencha BA, Abebe TA
, Dencha BA, Abebe TA ![]()
Received 16 December 2023
Accepted for publication 18 April 2024
Published 29 April 2024 Volume 2024:17 Pages 135—139
DOI https://doi.org/10.2147/CEG.S425986
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Vipul Yagnik
Worku Mekonnen Sefefe,1 Destaw Biadgie Tesfaw,2 Andualem Dagne Tebikew,2 Assefa Sisay Ayenew,3 Bereket Amare Dencha,4 Temesgen Agegnehu Abebe1
1Department of Surgery, Debre Markos University (DMU), Debre Markos, Amhara, Ethiopia; 2Department of Surgery, Bahir Dar University, Bahir dar, Amhara, Ethiopia; 3Department of Surgery, Akesta General Hospital, Wollo, Amhara, Ethiopia; 4Department of Pathology, Bahir Dar University, Bahir dar, Amhara, Ethiopia
Correspondence: Worku Mekonnen Sefefe, Department of Surgery, Debre Markos University (DMU), Debre Markos, Amhara, Ethiopia, Tel +251912101424, Email [email protected]
Background: Ectopic pancreas (EP), characterized by pancreatic tissue outside its usual location, poses diagnostic challenges due to its asymptomatic nature in most cases. Gastric lesions are often symptomatic, causing epigastric pain or gastric outlet obstruction. Rarely, jejunal lesions can lead to intestinal obstruction or intussusception. The elusive preoperative diagnosis lacks specific biochemical markers, relying on intraoperative biopsy and histopathology as gold standards.
Case Presentation: We present a unique case of a 37-year-old female with 12-hour crampy abdominal pain, bilious vomiting, blood-mixed diarrhea, abdominal distension, and obstructive symptoms. Imaging revealed jejunojejunal intussusception with a jejunal mass as the lead point. Intraoperatively, also identified jejunal mass as lead point. Resection of mass and end-to-end jejunojejunal anastomosis were performed, resulting in a successful outcome. Histopathological examination identified a type I ectopic pancreas within the muscularis propria. Twelve months postoperatively, the patient exhibited no stricture or recurrence.
Conclusion: Ectopic pancreas, with varied symptoms, poses diagnostic hurdles. Despite the diagnostic challenges, surgical excision remains the optimal treatment for symptomatic cases. This report contributes to the limited literature on ectopic pancreas, emphasizing the importance of considering this entity in the differential diagnosis of gastrointestinal pathology.
Keywords: ectopic pancreas, pancreatic heterotopia, jejunojejunal intussusception, lead point, Ethiopia
Introduction
The ectopic pancreas (EP) denotes pancreatic tissue outside its typical location, lacking anatomical or vascular connection with the normal pancreas. Also termed pancreatic heterotopia, it commonly appears in the upper gastrointestinal (GI) tract, with 70–90% of cases reported in the stomach (25–38%), duodenum (17–36%), and jejunum (15–21%).1–3
The true incidence of EP is uncertain due to its asymptomatic nature, often incidentally discovered during unrelated procedures.1 Autopsy findings indicate an incidence of 1–2% (0.5–13.7%), with a notable male predominance (3:1).2–6
Heterotopic pancreas (HP) spans various age groups, prevalent between 30 and 60 years.7–9 Gastric lesions may cause epigastric pain or gastric outlet obstruction, while rare jejunal lesions can lead to intestinal obstruction or intussusception.1–3,7–9
Diagnostic challenges arise from nonspecific symptoms, small lesion size, and deep submucosal location hindering pathological biopsy.8 Biochemical markers for HP are generally unavailable.1 Preoperative methods include ultrasound, CT, barium studies, and MRI. Intraoperative biopsy and histopathology serve as the gold standard.1,5
EP can be pathologically classified into four subtypes, with Type 1 heterotopia displaying typical pancreatic tissue composition. Histologically, most tumors are in the submucosa, rarely in the muscularis propria, and around 13.5% in the subserosa.1,3
Surgical excision is optimal for symptomatic EP, while managing asymptomatic cases remains debated.8
Jejunal ectopic pancreas is rare.1–3,7–9 This report highlights a 37-year-old female with jejunal ectopic pancreas.
Case Report
A 37-year-old female patient from the rural part of Ethiopia, Amhara ethnicity, presented with crampy abdominal pain every 5 min, which started at a supraumbilical area for 12 h. Associated history of repeated billus vomiting and five to six times producing blood mixed diarrhea followed by abdominal distension, failure to pass feces, and flatus. The patient had no other chronic illnesses or TB treatments. The patient had no history of any trauma. She was referred from the Merawi Primary Hospital for the diagnosis of acute abdomen secondary to small bowel obstruction for further investigation and possible exploration and was brought by ambulance.
Physical examination: general appearance; acute sick looking; vital signs: blood pressure, 110/90 mmHg; pulse rate, 96 beats per minute; respiratory rate, 24 breath per minute; temperature,36.1 °C, oxygen saturation (SpO2) = 95%. Abdominal examination: Distended abdomen with visible bowel loops, non-tenderness, no sign of fluid collection, rectal exam – stool on examination of gloved fingers, no blood.
Laboratory investigations revealed no significant abnormalities and plain abdominal radiography revealed multiple air-fluid levels (See Figure 1). Abdominal ultrasound revealed long-segment telescoping of the bowel loops to another possible jejunal intussusception with multiple mesenteric small lymph nodes. The pancreas appeared normal, with no calcification or mass, and no dilated ducts. No free fluid collection is seen. The conclusion was an intussusception, likely jejunojejunal. On abdominopelvic contrast, enhanced CT scan there was a long segment small bowel intussusceptum into the small bowel giving a mass in the left lower quadrant measuring 5.1 cm × 5.2 cm × 5.8 cm that has a feature of intussusception (doughnut sign). Conclusion: An intra-abdominal bowel mass with marked bowel wall thickening secondary to intussusception with minimal ascites is observed (See Figures 2).
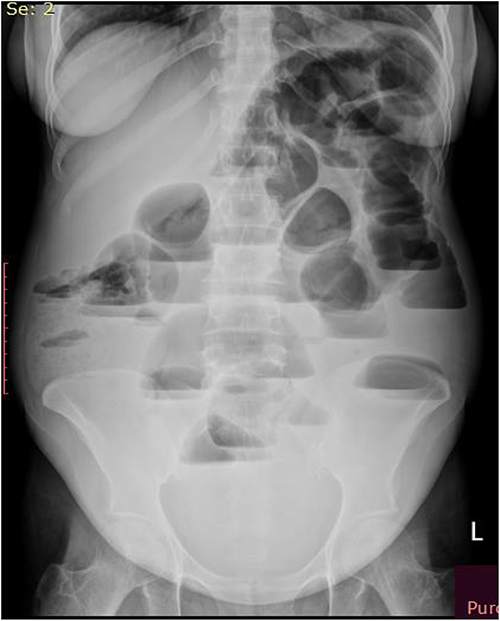 |
Figure 1 On plain abdominal x-ray- there is multiple air fluid level, dilated small bowel, valvulae conniventes are visible and absence of gas in the distal-collapsed bowel. |
 |
Figure 2 Green = intussuscepiens, White = intussusceptum, Black = mesenteric vessels and fat. |
Intraoperative with finding: A 4 cm × 8 cm telescoping of jejunojejunal intussusception with a lead point (both intussuscepiens and intussusceptum were viable). The lead point, which was 3 cm × 4 cm in size, looks jejunal sub-serosal in gross appearance but arose from the mural parts of the bowel upon cut section, had firm consistency, and 30 cm from the ligament of the treitz. The distal jejunum, ileum, and colon collapsed; the proximal jejunum was dilated; and all parts of the bowel were viable. There was 200 mL reactive fluid in the general peritoneum.
Procedure done. Reactive fluid was sucked out, anterograde decompression was performed, intussusception was manually reduced, jejunal mass resected with a 5 cm free margin from the mass, and end-to-end jejunojejunal anastomosis was performed. The mesenteric defect was then closed. Lymph node biopsy was taken from three sites. Biopsies were also obtained from the resected mass. Abdomen was closed in layers (as shown in the intraoperative images Figure 3).
 |
Figure 3 (A) Gross appearance and Cut section of ectopic pancreas as lead point, and (B) blue arrow showed the boundary of pancreatic rest which was lead point. |
Histopathology is done. Gross 12 cm × 4 cm long grey white small bowel tissue segment.
Cut section. Exophytic mucosal lumen 1.5 cm × 1 cm gray-white thickened bowel wall and within muscularis propria mass 4 cm from one of the nearest proximal surgical ends.
Conclusion of histopathology. A confirmed type I ectopic jejunal pancreatic rest (see the pathological slides in Figure 4).
 |
Figure 4 Histologic sections revealed acini, ducts (red arrow) and Islet cells (blue arrow) specific to the pancreas and confirming the diagnosis of pancreatic rest. |
Patient post operatively discharged with improved and also after twelve months postoperatively, the patient exhibited no stricture or recurrence.
Discussion
The occurrence of ectopic pancreas at diverse sites within the gastrointestinal (GI) tract, with majority, estimated at 70–90%, upper GI tract and but jejunum (15–21%).1–3 In our patients, the ethereal presence of ectopic jejunal pancreas unfolded, adding a unique chapter to this enigmatic narrative.1 The true incidence and prevalence of EP remain unknown but from autopsy specimens ranging from 1% to 2%.2–6
Heterotopic pancreas spans diverse age groups but predominantly surfaces between 30 and 60 years,7–9 aligning with our patient’s age of 37 years.
Symptoms of ectopic pancreas (EP) are largely absent; however, when present, manifestations vary based on lesion size and location. Gastric lesions, particularly symptomatic, may induce epigastric pain or symptoms of gastric outlet obstruction attributed to a prepyloric mass.1–3,7–9
Conversely, jejunal lesions, though rare, can lead to intestinal obstruction or intussusception.1–3,7–9 In our case, the patient presented with symptoms and signs of small bowel obstruction.
Diagnosing heterotopic pancreatic tissue poses significant challenges due to nonspecific symptoms and no established biochemical markers for the diagnosis.1
Ectopic pancreas exhibits four pathological subtypes. Type 1 heterotopia embodies typical pancreatic tissue with acini, ducts, and islet cells. The remaining subtypes: pancreatic ducts alone (Type II), acinar tissue alone representing the exocrine pancreas (Type III), and islet cells alone comprising the endocrine pancreas (Type IV).1,3 Histologically, tumors predominantly reside in the submucosa, with rare occurrences in the muscularis propria.1,3 Our diagnosis, confirmed through histopathological scrutiny of the jejunal mass, identified ectopic pancreatic tissue at the muscularis propria (Type I), devoid of malignant transformations.1
The optimal management symptomatic cases, surgical excision stands as the preferred treatment, offering symptomatic relief.8 Our patient also managed with surgically.
Conclusions
Ectopic pancreas, characterized by pancreatic tissue outside its usual location, presents diagnostic challenges due to its asymptomatic nature and diverse clinical manifestations. Surgical excision, guided by histopathological examination, remains the optimal treatment for symptomatic cases, providing relief and preventing potential complications. This case contributes valuable insights to the understanding of ectopic pancreas and emphasizes its consideration in the differential diagnosis of gastrointestinal pathology.
Ethical and Consent Statements
Institutional approval letter from Bahir Dar Comprehensive Specialized Hospital for publishing this case report is provided.
Written informed consent for the case report was taken from the patient to obtain images and other clinical information to be reported in the journal for publication. The patient understands that her name and initial will not be published and due efforts will be made to conceal her identity. Our institution also witnessed that the consent taken from the patient.
Disclosure
The authors report that no known competing financial interests or personal relationships that could have influenced the work reported in this study.
References
1. Saeed MF, Verhagen KR, Albinali S, Juma IM. A case report and literature review: incidental jejunal ectopic pancreatic tissue in an emergency bowel exploration for suspected intussusception. AME Case Rep. 2019;3:24. doi:10.21037/acr.2019.07.05
2. Dhruv S, Polavarapu A, Asuzu I, Andrawes S, Mukherjee I. Jejunal Ectopic Pancreas: a Rare Cause of Small Intestinal Mass. Cureus. 2021;13(6):657.
3. Swarnkar M, Jain SC. Heterotopic subserosal pancreatic tissue in Jejunum-an incidental rare finding. J Krishna Institute Med Sci Univ. 2017;6:105–108.
4. Masoodi I, Al-Lehibi A, Almohaimeed K, Hussain S. Pancreatic Rest - An Unusual Cause of Dyspepsia: a Case Report with Literature Review. Saudi J Med Sci. 2016;4(3):225–228. doi:10.4103/1658-631X.188261
5. Watanabe M, Shiozawa K, Kishimoto Y, et al. Heterotopic Pancreas of the Jejunum Incidentally Detected by Preoperative Abdominal CT: report of Two Cases and Review of the Literature. Case Rep Gastroenterol. 2012;6(3):576–582. doi:10.1159/000343093
6. Paramythiotis D, Kollatou AS, Simou T, et al. Ectopic pancreatic tissue in stomach: a case report. Ann Med Surg. 2022;79:104005. doi:10.1016/j.amsu.2022.104005
7. Zhang P, Wang M, Bai L, Zhuang W. A unique case of ectopic pancreas presenting as jejunal malignance. J Surgical Case Rep. 2019;2019(7):rjz217. doi:10.1093/jscr/rjz217
8. Li J, Huang H, Huo S, et al. Ectopic pancreatic tissue in the wall of the small intestine: two rare case reports. Medicine. 2017;96(35):e7986. doi:10.1097/MD.0000000000007986
9. Daniel NE, Rampersad FS, Naraynsingh V, Barrow S, David S. Jejunal Intussusception Due to Heterotopic Pancreas: a Case Report. Cureus. 2021;13(4):e14586. doi:10.7759/cureus.14586
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.