Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
JAK Inhibitors in Psoriatic Disease
Authors Megna M ![]() , Potestio L
, Potestio L ![]() , Ruggiero A
, Ruggiero A ![]() , Cacciapuoti S, Maione F, Tasso M, Caso F
, Cacciapuoti S, Maione F, Tasso M, Caso F ![]() , Costa L
, Costa L ![]()
Received 1 August 2023
Accepted for publication 13 October 2023
Published 31 October 2023 Volume 2023:16 Pages 3129—3145
DOI https://doi.org/10.2147/CCID.S433367
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Anne-Claire Fougerousse
Matteo Megna,1 Luca Potestio,1 Angelo Ruggiero,1 Sara Cacciapuoti,1 Francesco Maione,2 Marco Tasso,3 Francesco Caso,3,* Luisa Costa3,*
1Section of Dermatology, Department of Clinical Medicine and Surgery, University of Naples Federico II, Naples, Italy; 2Immunopharmalab, Department of Pharmacy, School of Medicine and Surgery, University of Naples Federico II, Naples, Italy; 3Rheumatology Research Unit, Department of Clinical Medicine and Surgery, University of Naples Federico II, Naples, Italy
*These authors contributed equally to this work
Correspondence: Angelo Ruggiero, Section of Dermatology, Department of Clinical Medicine and Surgery, University of Naples Federico II, Via Pansini 5, Napoli, 80131, Italy, Tel +39 - 081 – 7462457, Fax +39 - 081 – 7462442, Email [email protected]
Abstract: Psoriasis is now considered to be the cutaneous phenotype of a systemic inflammatory condition, recognized under the term Psoriatic Disease (PsD). PsD has several extracutaneous manifestations, such as inflammatory articular and entheseal involvement, leading to psoriatic arthritis (PsA), and the less frequent intestinal and ocular manifestations with colitis/inflammatory bowel disease and uveitis, respectively. There have also been several reports of an increased frequency of comorbidities such as hypertension, diabetes, dyslipidemia, obesity, metabolic syndrome and cardiovascular manifestations during the course of PsD. The link between psoriasis and related comorbidities is considered a long-term disease sequela, often characterized by an unhealthy lifestyle and a consequence of systemic inflammation; hence, psoriasis requires adequate and prompt treatment, with the aim of controlling not only cutaneous manifestations but also extracutaneous manifestations and systemic inflammation. Pharmacological strategies for PsD have significantly increased over recent years. Recently, the targeted synthetic DMARDs, Janus kinase (JAK) inhibitors, tofacitinib and upadacitinib, were added to the therapeutic armamentarium for treating PsA, and deucravacitinib for psoriasis. These oral agents act directly on inflammatory mechanisms underlining the disease, as antagonists of the intracellular JAK signal pathway and, by STAT phosphorylation, inhibit gene proinflammatory cytokine transcription. JAK inhibitors represent a recent additional treatment strategy for PsD management and, among these, tofacitinib and upadacitinib have recently been approved for PsA, and deucravacitinib for psoriasis. In this review we describe ongoing and recent phase II and III randomized controlled trials (RCTs) evaluating the efficacy and safety of investigational JAK inhibitors in psoriasis and PsA.
Keywords: JAK inhibitors, plaque psoriasis, psoriatic arthritis, TYK2 inhibitors
Introduction
Psoriasis is a chronic inflammatory skin disease, affecting up to 3% of the worldwide population.1,2 The most frequent clinical presentation, accounting for 80–90% of all cases, is plaque psoriasis/psoriasis vulgaris, which is characterized by well-delineated papulo-squamous plaques, involving most commonly the knees, elbows, trunk, scalp and nails.3,4 Psoriatic skin lesions are frequently associated with itching, pain, burning sensation, desquamation and, in its moderate to severe form, may have a significative negative impact on patients’ quality of life (QoL), affecting both social and working aspects.5–7 Of note, psoriasis is now considered to be the cutaneous phenotype of a systemic inflammatory condition, recognized under the term Psoriatic Disease (PsD).8,9 PsD has several extracutaneous manifestations, such as inflammatory articular and entheseal involvement, leading to psoriatic arthritis (PsA), and the less frequent intestinal and ocular manifestations involving colitis/inflammatory bowel disease and uveitis, respectively.10–13
PsA can occur in about one-third of psoriasis patients, showing dactylitis, enthesitis, peripheral and/or axial articular involvement.14 The Toronto Psoriatic Arthritis Screen II (ToPAS II), Psoriatic Arthritis Screening and Evaluation (PASE), Psoriasis Epidemiology Screening Tool (PEST) and Early Arthritis for Psoriatic Patients (EARP) questionnaires represent four useful screening tools for diagnosing PsA in psoriasis subjects.15
There have been sseveral reports of an increased frequency of comorbidities such as hypertension, diabetes, dyslipidemia, obesity, metabolic syndrome and cardiovascular (CV) manifestations in the course of PsD.11–13 The link between psoriasis and related comorbidities is considered a long-term disease sequela often characterized by an unhealthy lifestyle and a consequence of systemic inflammation; hence, psoriasis requires adequate and prompt treatment with the aim of controlling not only cutaneous manifestations but also extracutaneous manifestations and systemic inflammation.16–18
Pharmacological strategies for PsD have significantly increased over recent years. Numerous randomized controlled trials (RCTs) have proven the efficacy and safety of various topical agents for cutaneous involvement, such as conventional synthetic disease-modifying anti-rheumatic drugs (csDMARDs), and biological DMARDs (bDMARDs), and the phosphodiesterase-4 (PDE-4) inhibitor, apremilast, approved both for psoriatic cutaneous and articular manifestations.19–22
Recently, the targeted synthetic DMARDs (tsDMARDs), Janus kinase (JAK) inhibitors (Jakinibs), tofacitinib and upadacitinib, were added to the therapeutic armamentarium for treating PsA, and deucravacitinib for psoriasis. These oral agents act directly on inflammatory mechanisms underlying the disease, as antagonists of the intracellular JAK signal pathway and, by STAT phosphorylation, inhibit gene proinflammatory cytokine transcription.23
JAK inhibitors represent a recent additional treatment strategy for PsD management and, among these, tofacitinib and upadacitinib have recently been approved for PsA, and deucravacitinib for psoriasis. In this review we describe ongoing and recent phase II and III RCTs evaluating the efficacy and safety of investigational JAK inhibitors in psoriasis and PsA.
Psoriatic Disease Etiopathogenesis
PsD shows a complex and still not fully clarified pathophysiology. The hallmark of psoriasis is sustained inflammation with involvement of multiple innate and adaptive cellular pathways that lead to uncontrolled keratinocyte proliferation and dysfunctional differentiation.24,25 The activation of plasmacytoid dendritic cells (pDC) by LL37/cathelicidin released by damaged keratinocytes and complexed with self-genetic material is considered to be the starting key pathogenetic event for the development of the psoriatic plaque. pDC are then able to produce type I IFN promoting myeloid dendritic cell (mDC) phenotypic maturation leading to Th1 and Th17 cell differentiation and activation.24 Several cytokines have been found to play a key role in the development and maintenance of the inflammatory processes behind psoriatic lesions. In particular, the IL-23/Th17 axis is believed to play a central role.26,27 Indeed, IL-23 drives the differentiation and proliferation of Th17 cells, which produce high levels of IL-17 and IL-22, causing keratinocyte proliferation and other typical features of psoriasis.1
The JAK/STAT pathway family is composed of four cytoplasmic tyrosine kinases (JAK1, JAK2, JAK3, and Tyk2),and seven signal transductors (STAT1, STAT2, STAT3, STAT4, STAT5a, STAT 5b, and STAT6) regulating signaling effects of multiple cytokines and growth factor on involved cells.24
Dysregulation of several molecules, including proinflammatory interleukins (ILs), interferons (IFNs), growth factors, and colony-stimulating factors (CSF) act as ligands to receptors connected to intracytoplasmic JAKs. Hence, JAKs activate STAT proteins, which translocate to the nucleus, thus generating expression of inflammatory nuclear factor synthesis. Of note, a key role in psoriatic pathogenesis is played by the IL-23 receptor relying on a heterodimer of JAK2 and TYK2 for signal transduction.28 JAKs are intracellular kinases that mediate signalling of the key cytokines (eg, interleukin [IL]-23 and type I interferons) involved in the pathogenesis of immune-mediated diseases including plaque psoriasis and psoriatic arthritis. JAK/STAT pathway dysfunctions lead to the proliferation and regulation of crucial pathogenetic cells, including keratinocytes, Th17 lymphocytes, and gamma–delta T cells.29,30 Further, JAK/STAT pathways show a central role in the development and pathogenesis of psoriatic-associated inflammatory conditions, as well as in PsA.31–34 Several data have reported an enhanced activation of JAK1/STAT3/STAT1 that may drive the articular inflammatory process, characterized by expansion of Th17 effector cells in the synovial fluid of joints of patients with active PsA.35–38
In this context, understanding of the pro-inflammatory intracellular JAK/STAT pathways involved in PsD has facilitated the identification and development of new therapeutic molecules able to inhibit/reduce the signaling effects of multiple cytokines and growth factor on targeted cells.39,40
Psoriatic Disease Assessment and Therapy
Since psoriasis treatment strictly depends on its severity, disease assessment represents an important issue. Hence, several clinical tools, such as the Psoriasis Area Severity Index (PASI) and Body Surface Area (BSA), are used in clinical practice, as well as in randomized clinical trials (RCTs).41 PASI score is the most widely used tool to evaluate psoriasis severity, and PASI75 (75% or greater reduction in PASI scores from baseline) represents a primary outcome largely used in psoriasis RCTs. It combines the assessment of the severity of lesions and the area affected into a single score ranging from 0 (no disease) to 72 (maximal disease), dividing the body into four sections (head: 10%, arms: 20%, trunk: 30%, and legs: 40%) and scoring any of these areas by itself. Then, the 4 scores are combined into the final PASI. For all sections, the percentage of skin involved is estimated and then converted into a grade from 0 (0% of involved area) to 6 (90–100% of involved area). The severity is estimated by three clinical signs measured on a scale of 0 (none) to 4 maximum): erythema (redness), induration (thickness) and desquamation (scaling). The sum of all three severity parameters is then calculated for each section of skin, multiplied by the area score for that area and multiplied by weight of respective section (0.1 for head, 0.2 for arms, 0.3 for body, and 0.4 for legs).42 BSA represents the arithmetic mean of the affected skin surface based on the assumption that the head presents 10%, the upper extremities 20%, the trunk 30%, and the lower extremities 40% of the total body surface. The formula for the calculation of BSA is: BSA = 0.1 * BSA head + 0.2 * BSA upper extremities + 0.3 * BSA trunk + 0.4 * BSA lower extremities.42 Psoriasis is considered as moderate to severe, hence requiring systemic treatment, when PASI and/or BSA are ≥10. However, psoriasis may be considered as moderate to severe, requiring prompt systemic treatment, even if PASI and/or BSA are less than 10 but the disease involves the so-called difficult to treat areas such as scalp, palmo-plantar area, face, genitals, and nails, which all have a huge impact on quality of life as well as daily life.43 The importance of evaluating disease severity is also displayed by impact on quality of life evaluated through the Dermatology Life Quality Index (DLQI) questionnaire, a simple, self-administered validated questionnaire designed to measure the health-related quality of life of adult patients suffering from a skin disease.44 It consists of 10 questions exploring the impact of the disease in different aspects of life (skin symptoms, embarrassment, influence on choice of clothes to wear, social activities, sport, working activities, sexual activity, etc), showing a score ranging from 0 to 30. The disease is considered moderate to severe for scores of ≥ 10.
Psoriasis management is challenging, particularly for moderate-to-severe forms of the disease, defined as PASI >10 or BSA >10 and DLQI > 10, or PASI or BSA <10 with involvement of visible and/or difficult to treat areas (scalp, face, genitals, nails with onycholysis or onychodystrophy of at least two fingernails, and palmo-plantar area), and/or presence of itching leading to scratching and the presence of recalcitrant plaques.45,46
When articular involvement is verified, several composite disease activity measures (Composite Psoriatic Disease Activity Index [CPDAI], PsA Impact of Disease [PsAID], Psoriatic Arthritis Disease Activity Score [PASDAS], Disease Activity Index for Psoriatic Arthritis [DAPSA]) assess contemporaneously multiple domains, such as axial and peripheral involvement, responses to the Health Assessment Questionnaire (HAQ), pain, enthesis and dactylitis. The rates of ACR20 response (≥ 20% improvement from baseline in the number of tender and swollen joints and at least three of five other important domains) and mean change from baseline in Health Assessment Questionnaire-Disability Index (HAQ-DI) score (scores range from 0 to 3, with higher scores indicating greater disability) are the main outcomes used in PsA trials.47,48
Psoriatic Disease Treatment
Even if mild psoriasis is often controlled with topical therapies, systemic treatments are required for moderate-to-severe forms. Conventional systemic drugs include cyclosporine, acitretin, methotrexate, and fumarates. However, their use is often limited by contraindications (eg, cardiovascular disease, hepatic or renal failure, etc.) and the risk of adverse events (AEs).45,46 For example, cyclosporine is contraindicated in patients with hypertension and renal failure and also has several drug interactions; acitretin is teratogen and may cause lipid level alteration; and methotrexate may determine blood count or transaminase alterations, limiting their use, especially for patients with other comorbidities and polypharmacy use.49–52
Phototherapy may be a valuable alternative option, despite being limited by logistic concerns (the patient should attend the phototherapy center three times weekly).45,46
In this scenario, bDMARDs and oral small molecules have revolutionized psoriasis management. Indeed, they combine a greater efficacy profile rather than conventional systemic treatments, together with a more desirable safety profile. To date, several bDMARD classes have been approved for the management of psoriasis, including anti-TNFs, anti-IL-12/23, anti-IL-17s, and anti-IL-23s, and they are able to achieve a fast and sustained clinical response, with an even, generally safe profile.53 In PsA, bDMARDs targeting TNF-α and IL-17A are highly recommended for predominant axial, and entheseal phenotypes and peripheral arthritis refractory to methotrexate.54–56
However, although generally safe, bDMARds have several concerns to be considered before starting the treatment, such as the risk of reactivation of latent tuberculosis infection (especially for anti-TNF and anti-IL12/23), or onset or worsening of inflammatory bowel diseases (anti-IL-17s).57,58 Moreover, bDMARDs are administered by subcutaneous injection, or intravenously in case of infliximab, which may represent a partial limit in some patients. Of note, bDMARDS were also shown to be safe during the COVID-19 pandemic.59,60 Hence, oral small molecules, such as the PDE-4 inhibitor, Apremilast, may represent a valuable alternative for moderate to severe forms of psoriasis and for patients with mild PsA refractory to therapy with at least one csDMARD, and contraindications to bDMARD or JAK inhibitor use.45,46,61,62
JAK inhibitors represent a recent additional treatment strategy for PsD management, and among these, tofacitinib and upadacitinib have recently been approved for PsA, and deucravacitinib for psoriasis. In this review we describe ongoing and recent phase II and III RCTs evaluating the efficacy and safety of investigational JAK inhibitors in psoriasis and PsA.
As previously described, PsD pathophysiology relies on JAK/STAT signaling and JAK-inhibitors, tofacitinib and upadacitinib, are yet to be approved for psoriatic articular phenotype, as well deucravacitinib for the cutaneous phenotype.63,64 Inhibition of this pathway seems be a promising treatment for PsD management and several RCTs are ongoing for other JAK inhibitors.
Aim of the Study
The aim of our study was to review current literature on the use of JAK inhibitors in PsD in order to offer a wide perspective on their efficacy and safety and investigate their potential applications.
Materials and Methods
A search of the current literature on the PubMed, Embase, Cochrane Skin, Google Scholar, and clinicaltrials.gov databases (until June 30, 2023) was performed using the following terms: “psoriasis”, “psoriatic arthritis”, “JAK inhibitors”, “tofacitinib”, “upadacitinib”, “filgotinib”, “itacitinib”, “abrocitinib”, “solcitinib”, “ivarmacitinib”, “baricitinib”, “pefcitinib”, “deucravacitinib”, “BMS-986165”, “brepocitinib”, “PF-06700841”, “ropsacitinib”, and “PF-06826647”. The following types of article were considered in our review: metanalyses, reviews, clinical trials, case reports and series, and real-life experiences. The most relevant articles were selected. The texts and abstracts of designated manuscripts were reviewed to refine the research. References were also analyzed to avoid missing some relevant articles. The current article is based on previously performed studies and does not contain any studies with animal or human participants carried out by any of the authors.
JAK Inhibitors Approved for PsA and Under Investigation for Psoriasis
Results of our research are summarized in Table 1.
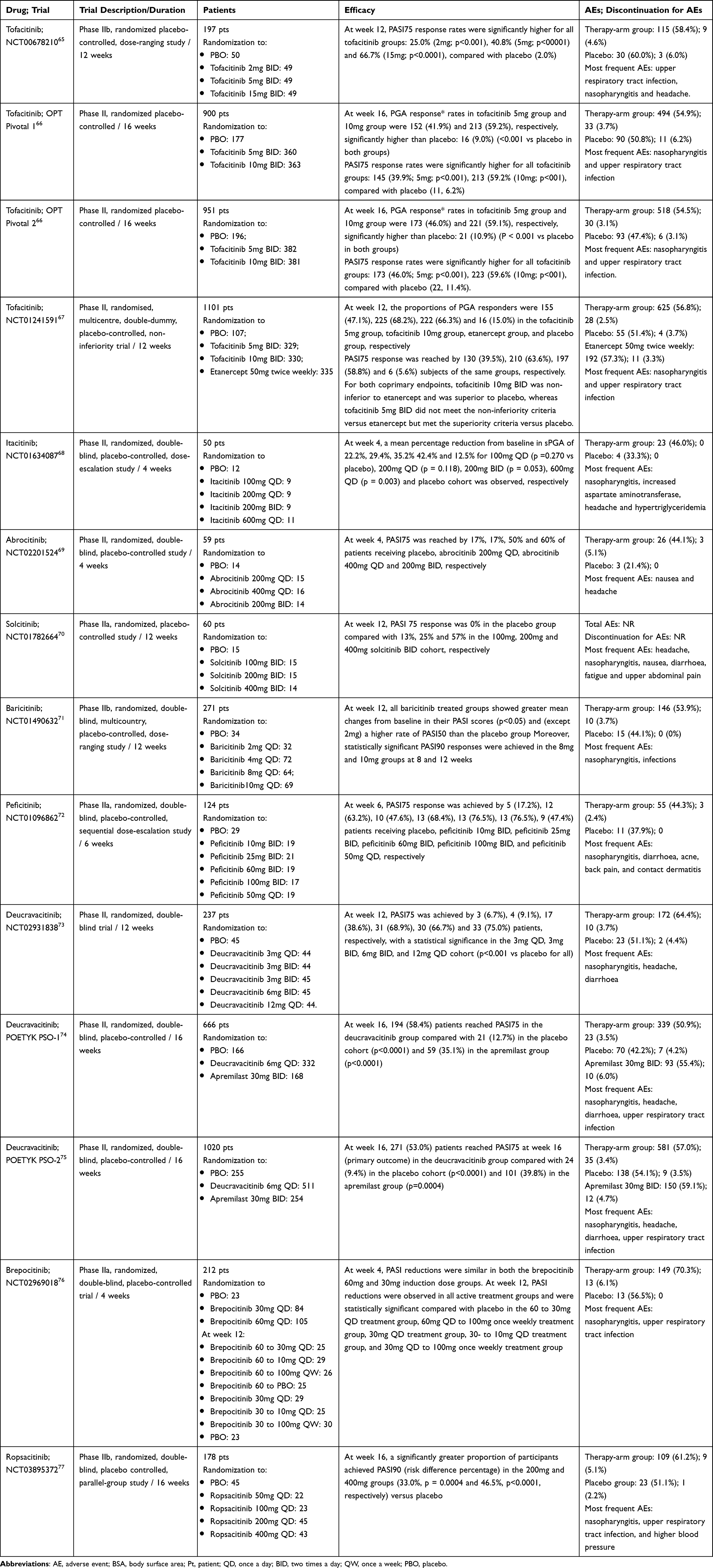 |
Table 1 JAK Inhibitors in Psoriatic Disease |
JAK Inhibitors Approved for PsA
Tofacitinib
Tofacitinib is a pan-JAK inhibitor that effectively blocks JAK1 and JAK3. It is approved at the dose of 5mg twice daily (BID) combined with MTX for the treatment of moderate-to-severe active PsA in adult patients with an intolerance or inadequate response to csDMARDs.78,79
Two double-blind, placebo-controlled phase III RCTs (Oral Psoriatic Arthritis triaL [OPAL] and Broaden and Oral Psoriatic Arthritis triaL [OPAL Beyond])79,80 and a long-term extension analysis up to 48 months during these trials (OPAL Balance) have reported efficacy and an acceptable safety profile in PsA.80
These trials have shown a significant improvement in term of ACR20 response rates and mean change from baseline in HAQ-DI score (primary outcomes), at month 3 and over time (48 months) in tofacitinib (5mg and 10mg BID) patients, as compared with placebo.80–82
Significant improvements were also reported for secondary outcomes and, among those, for skin outcomes, PASI75 response rates and changes from baseline in PGA-PsO.81,83–86
In particular, a greater proportion of patients on tofacitinib 5 and 10mg BID achieved PASI75 vs placebo at month 3. PASI75 response further improved at month 6. Improvements in skin outcomes were also maintained over time.80
Although tofacitinib is not indicated for psoriasis treatment, the efficacy and safety of tofacitinib have been investigated in numerous RCTs enrolling patients with moderate-to-severe plaque psoriasis.
In a 2012 phase IIb, 12-week, dose-ranging study, PASI75 response rates were significantly higher for all tofacitinib groups (25.0% (2mg; p<0.001), 40.8% (5mg; p<00001) and 66.7% (15mg; p<0.0001) compared with placebo (2.0%).65
In two successive phase III RCTs (Oral-treatment Psoriasis Trial [OPT] Pivotal 1 and OPT Pivotal 2), at week 16, a greater proportion of patients achieved PGA responses of 0/1 with tofacitinib 5- and 10mg BID vs placebo. Similarly, significantly higher PASI75 responses were reported with tofacitinib vs placebo. In these RCTs, at week 16, all placebo patients were re-randomized to tofacitinib 5mg and followed up for 52 weeks. From week 16 to 28, the proportion of patients achieving PASI75 increased further with both tofacitinib doses and results were maintained up to week 52 in 74–79% of patients.66,87
Tofacitinib has also been evaluated in a phase III non-inferiority trial. It compared tofacitinib (5mg and 10mg BID) to both etanercept (50mg twice weekly) and placebo over 12 weeks. At week 12, PASI75 responses were achieved in 39%, 63%, 59% and 6% of patients receiving tofacitinib 5mg, 10mg, etanercept, and placebo, respectively. Similarly, a PGA 0/1 response was achieved by 47.1%, 68.2%, 66% and 15% of patients.67
Finally, an open-label extension study on the use of tofacitinib for psoriasis enrolled patients who had completed phase II/III tofacitinib trials and showed that the improvement in patient-reported treatment outcomes were maintained for up to 54 months.88
Concerning tofacitinib’s safety, it has shown an acceptable profile with, in most cases, mild to moderate AEs, mainly nasopharyngitis, upper respiratory tract infection, headache, and gastrointestinal symptoms (diarrhea, nausea, vomiting, and constipation).65,66,87 In psoriasis RCTs, although a dose-response was observed for serious infections, herpes zoster (HZ) and nonmelanoma skin cancer (NMSC), the 95% CIs for each incidence rate overlapped and the incidence rate difference was small between dose groups; no dose response was observed for malignancies (excluding NMSC). Over 33 months, 10.1% of patients experienced SAEs and 10.7% of patients discontinued because of AEs. The incidence rates for HZ were higher for the total tofacitinib exposure versus the first 52 weeks; however, most HZ cases resolved without complications.66,87
In the non-inferiority trial by Bachelez et al, AE rate was similar across tofacitinib 5mg, tofacitinib 10mg, etanercept, and placebo cohorts. Globally, 1%, 3%, 3% and 4% patients in the tofacitinib 5mg, tofacitinib 10mg, etanercept, and placebo cohort, respectively, discontinued their assigned treatment because of AEs.67
In contrast to RA trials, in which major adverse cardiovascular events and thromboembolic events have been reported in patients aged over 50 or with cardiovascular risk factors at enrollment,89–91 in PsD, long-term data demonstrated rare cases of major cardiovascular problems.65,66,87 However, caution when using tofacitinib is required in elderly patients at increased cardiovascular risk.
Upadacitinib
Upadacitinib is a selective oral inhibitor of JAK1 and, to a lesser extent, JAK2. The agent has been evaluated in two main phase III trials (SELECT-PsA 1 and SELECT-PsA 2) and it is approved for the treatment of PsA.92,93
The SELECT-PsA 1 phase III RCT (24-week) compared upadacitinib at different dosages (15mg or 30mg once daily [QD]) with adalimumab (40mg subcutaneously every other week) and placebo (1:1:1:1) in about 1700 adult patients with active PsA and an inadequate response to at least one csDMARD.92 At week 12, in both upadacitinib groups, ACR20 response rates swere similar to adalimumab and higher when compared with placebo.92
Select-PsA1 also showed upadacitinib efficacy in skin outcomes. Improvements in PASI75/90/100 and Static Investigator Global Assessment of Psoriasis of 0 or 1 (sIGA 0/1) response rates, and change from baseline in Self-Assessment of Psoriasis Symptoms were maintained over time. In patients randomized to placebo, the proportion of patients reaching PASI75/90/100 and sIGA 0/1 increased after switching to upadacitinib, and responses were similar to the groups on upadacitinib at week 56.94,95
In a SELECT-PsA2 trial, 642 PsA patients with inadequate response or intolerance to at least one bDMARD were randomized (2:2:1:1) to upadacitinib 15mg or 30mg QD, and two placebo groups shifting either to upadacitinib 15mg or upadacitinib 30mg at week 24.93 At week 12, when compared to placebo (24%), a significant proportion of patients on upadacitinib 15mg (57%) and 30mg (64%) achieved ACR20 (primary outcome). At week 56, the efficacy of upadacitinib, in terms of PASI75/90/100, PROs and MDA, was maintained over time.96–99
At week 56, the proportions of patients achieving PASI75/90/100 using non-responder imputation (NRI) were 52/41/27% with upadacitinib 15mg, and 59/47/35% with upadacitinib 30mg. In both placebo to upadacitinib groups, PASI75/90/100 responses at week 56 were similar to those for patients who received upadacitinib from baseline, with the exception of PASI100 in the placebo to upadacitinib 15mg group. Numerically, greater proportions of patients on upadacitinib from baseline than placebo subjects switching to upadacitinib groups for each of the doses achieved sIGA 0 or 1 and ≥ 2 point improvement from baseline.96
Upadacitinib RCTs have shown an acceptable safety profile of this agent comparable to adalimumab. Rates of serious infection, HZ, anemia, neutropenia, lymphopenia, and elevated creatine phosphokinase remained numerically higher with upadacitinib versus adalimumab. Rates of malignancies excluding NMSC, major adverse cardiovascular events, and venous thromboembolism were similar across groups; rates of NMSC were higher with upadacitinib versus adalimumab.94,95
Data from upadacitinib clinical trials specifically investigating PASI75 as the primary outcome are lacking, but it seems a potentially valid therapeutic strategy for treating psoriasis, as well as other cutaneous diseases.100,101
JAK Inhibitors Under Investigation for Psoriatic Disease
JAK1 Inhibitors
Filgotinib is a selective JAK1 inhibitor with minimal JAK2 selectivity. Approved for rheumatoid arthritis, it has been investigated in a phase II trial placebo-controlled RCT (EQUATOR trial).102
In the EQUATOR trial, 131 active PsA patients with insufficient response or intolerance to at least one csDMARD were randomized to filgotinib 200mg (n: 65) or placebo (n: 66) orally QD for 16 weeks.96 At week 16, a significant proportion of patients on filgotinib achieved ACR20 (primary outcome), as well as ACR50 and ACR70 responses when compared with the placebo cohort.102,103 Cutaneous improvement in terms of PASI75 at week 16 was also verified in more patients on filgotinib.102,103 More frequent AEs were mild, occurring in 57% of treated patients and represented by nasopharyngitis and headache. No statistical significance in AE frequency was found in the comparison with the placebo group (59%).102
Itacitinib, abrocitinib solcitinib and ivarmacitinib are oral selective JAK1 inhibitors, investigated in psoriasis phase II RCTs.68–70
In a phase II, 28-day dose-escalation RCT, at 4 weeks itacitinib proved efficacious in mean sPGA percentage reduction from baseline of 22%, 29%, 35%, and 42% for 100mg QD, 200mg QD, 200mg BID, and 600mg cohorts, respectively. Finally, itacitinib was generally well tolerated, with nasopharyngitis the most common AE reported (18.4%).68
At week 4, PASI75 was reached by 17%, 17%, 50% and 60% of patients receiving placebo, abrocitinib 200mg QD, abrocitinib 400mg QD and 200mg BID, respectively. No serious infections or bleeding events related to neutropenia or thrombocytopenia, respectively, were reported.69
At week 12, a PASI 75 response of 0% in the placebo group was compared with 13%, 25% and 57% in the 100mg, 200mg and 400mg solcitinib BID cohort, respectively. Of note, improvement in itching and quality of life were observed at all doses relative to placebo, with the greatest improvement seen in the 400mg dose group. Globally, the incidence of AEs was similar across treatment groups, and no relationship between frequency of AE and solcitinib dose was identified.70
For ivarmacitinib (SHR0302), investigated in a phase III study to evaluate the efficacy and safety of different doses in PsA patients (estimated participants: 444) (NCT04957550), data are not available.104
JAK Inhibitors with Preferential JAK1/JAK2 (Baricitinib) or JAK3 Selectivity (Peficitinib)
Baricitinib is an oral JAK1/JAK2 inhibitor. Its efficacy and safety for psoriasis has been investigated in a randomized phase IIb trial enrolling 271 patients randomized to receive placebo (n=34), baricitinib 2mg (n=32), baricitinib 4mg (n=72), baricitinib 8mg (n=64), and baricitinib 10mg (n=69). At week 12, all baricitinib treated groups showed greater mean changes from baseline in their PASI scores (p<0.05) and (except 2mg) a higher rate of PASI50 than the placebo group. Moreover, statistically significant PASI90 responses were achieved in the 8mg and 10mg groups at 8 and 12 weeks.71 Peficitinib (ASP015K) is a novel oral JAK inhibitor, with a higher selectivity for JAK3 over JAK1 and JAK2. The efficacy and safety of peficitinib has been investigated in a phase IIa multicentre, double-blind, randomized, placebo-controlled study enrolling 124 patients with moderate-to-severe plaque psoriasis randomized to receive peficitinib 10mg BID (n=19), 25mg BID (n=21), 60mg BID (n =19), 100mg BID (n=17), 50 mg QD (n=19) or placebo (n=29) for 6 weeks. Improvements in PASI score were demonstrated over the course of peficitinib treatment, with a statistically significant profile (overall treatment effect p<0·001). Similarly, the secondary endpoints (PGA and BSA) also improved with peficitinib vs placebo (p<0.001 for both). ASP015K was generally well tolerated, with no serious AEs reported.72
TYK-2 Inhibitors (Deucravacitinib; BMS-986165, Brepocitinib; PF-06700841 and Ropsacitinib; PF-06826647)
Deucravacitinib (BMS-986165) is an oral allosteric and a selective inhibitor of TYK2, approved for the treatment of adult patients with moderate-to-severe plaque psoriasis.105,106 Deucravacitinib has shown its efficacy first in a phase II RCT, in which PASI75 was achieved in groups on therapy, with a statistical significance in the 3mg QD, 3mg BID, 6mg BID, and 12mg QD groups in terms of improvement in QoL vs placebo.73,107
Subsequently, the efficacy and safety of deucravacitinib were also investigated in a 52-week, phase III RCT (POETYK PSO-1) in which 58% of patients reached PASI75 at week 16 (primary outcome) in the deucravacitinib group compared with 13% in the placebo cohort, and 35% in the apremilast group. Similarly, sPGA 0/1 was reached in 54% of the patients on deucravacitinib compared with 7% and 32% of patients on placebo and apremilast, respectively. Moreover, PASI75 response and sPGA 0/1 continued to improve up to week 24 and these responses were maintained to week 52 in patients receiving deucravacitinib.74
These outcomes were verified also in another 52-week, phase III RCT (POETYK PSO-2), in which, at week 16, 53% of patients reached PASI75 at week 16 (primary outcome) in the deucravacitinib group compared with 9% of patients on placebo (p<0.0001) and 40% on apremilast. Similarly, sPGA 0/1 was reached by 49.5%, 9% and 34% of patients on deucravacitinib, placebo and apremilast, respectively.75
In an open-label, long-term extension trial, POETYK PSO-LTE, deucravacitinib efficacy in relation to cutaneous outcomes were reported to persist over time (up to 2 years).108
More recently, Imafuku et al confirmed the efficacy of deucravacitinib in psoriasis patients, with the proportion of patients achieving PASI75 being numerically higher with deucravacitinib versus placebo and apremilast at week 16 (78.1% vs 11.8% and 23.5%, respectively) and versus apremilast at week 24 (78.1% vs 29.4%). Results were maintained over time (52 weeks).109
Deucravacitinib is also in development for PsA (NCT03881059) and recent results from a phase III RCT with randomization of 203 active PsA patients to deucravacitinib at the dosages of 6mg and 12mg QD and placebo have shown a significant difference in ACR 20 response rate at week 16 for both treatment groups (53% and 63%, respectively) when compared to placebo (32%). Further, higher articular and cutaneous responses were verified in both groups on deucravacitinib vs placebo.110 Both in psoriasis and PsA RCTs, deucravacitinib was generally well tolerated, with nasopharyngitis, headache, diarrhea, nausea, and upper respiratory tract infection representing the most common AEs. No cases of herpes zoster infection, opportunistic infections, malignancies or thromboembolic events were verified on deucravacitinib.73–75,110
Brepocitinib (PF-06700841) is another oral inhibitor of TYK2, as well as of JAK1 and JAK2, in development for psoriasis and PsA.111 In a phase IIb RCT (NCT03963401) enrolling 218 PsA patients with inadequate response or intolerance to NSAIDs/DMARDs, brepocitinib at doses of 30 and 60mg QD showed superior efficacy (ACR20/50/70, MDA, dactylitis, enthesitis, fatigue, HAQ-DI and PASI 75/90) vs placebo at week 16. Responses were maintained over time (52 weeks).76 In the 16-week treatment period, AEs were mild in severity (165/250 [66%]) through week 16 and seven serious AEs (SAEs) were verified.76 At week 52, no major adverse cardiovascular events, venous thromboembolic events, serious infections, or deaths occurred.76
In psoriasis patients on brepocitinib, improvement of cutaneous manifestations with inhibition of synthesis of several proinflammatory cytokines (IL-17A, IL-17F and IL-12B mRNA) involved in TYK2 and JAK1 pathways have been reported.112,113 Brepocitinib at dosages of 30mg QD and 60mg QD was generally effective and well tolerated in patients with moderate-to-severe plaque psoriasis.114,115
In a phase I trial, a PGA 0/1 response was achieved in 57%, 100%, and 0% of 30 psoriasis patients receiving 30mg or 100mg orally or placebo once daily for 28 days, respectively.116
In a phase II RCT, 212 psoriasis patients were randomized to PF-06700841 30mg QD, 60mg QD, or placebo (4-week induction), followed by 10mg QD, 30mg QD, 100mg once weekly, or placebo (8-week maintenance), showing that decreases in PASI at week 12 were statistically significant compared with placebo in five treatment groups. Overall, 136 patients experienced AEs, and 13 AE-related discontinuations were reported in treated patients. No herpes zoster cases, or major adverse cardiac events and thromboembolic events occurred.114
Topical brepocitinib recently tested in a phase IIb trial in patients with mild to moderate psoriasis did not result in statistically significant changes from respective controls in the primary or key secondary endpoints for any dosage group (brepocitinib 0·1% QD, 0.3% QD or BID, 1% QD or BID, 3% QD, or vehicle QD or BID).115
Ropsacitinib (PF-06826647) is another TYK2 inhibitor, which was investigated in a phase IIb RCT (NCT03895372) enrolling 178 patients with moderate-to-severe plaque psoriasis. Patients were randomized to oral, once-daily PF-06826647 (1:1:2:2:2) 50:100:200:400mg: placebo (16 weeks), then 200 or 400mg (24 weeks).77 At week 16, a significantly greater proportion of patients achieved PASI90 in the 200mg and 400mg groups versus placebo. At week 40, significant increases in comparison to placebo were observed for all secondary endpoints (PASI50/75/90/100; Physician’s Global Assessment). PF-06826647 was well tolerated over 40 weeks and most treatment-emergent adverse events were mild/moderate. Eighteen participants discontinued due to treatment-emergent adverse events.77
Phase II trials are ongoing for other novel TYK2 allosteric inhibitors, such as ESK-001 in patients with moderate-to-severe plaque psoriasis and NDI-034858 in patients with PsA. Primary outcomes of these studies are represented by PASI-75 and ACR20 response rate, respectively.117,118
Discussion
PsD is an inflammatory condition, characterized by heterogenous manifestations, mainly involving cutaneous and articular domains. Recently, the introduction of new drugs selectively targeting pathogenetic mechanisms has led to the development of selective drugs.119–121
In particular, the approval of the TYK2 inhibitor, deucravacitinib, for psoriasis and the pan-JAK inhibitor, tofacitinib, and the JAK1 inhibitor, upadacitinib, for PsA, has represented an additional therapeutic strategy in moderate to severe phenotypes.122 Further, deucravacitinib, has been reported to be efficacious in treating PsA as measured by ACR20, and tofacitinib and upadacitinib in treating psoriasis as measured by PASI75 and sPGA. These agents have also shown an acceptable safety profile. Of note, numerous trials are ongoing for new JAK inhibitors and preliminary data for several of these are available for these molecules. In particular, the investigational JAK1 inhibitors, filgotinib, itacitinib, abrocitinib and solcitinib, have been shown to be efficacious in the cutaneous domain in terms of PASI75, and sPGA percentage reduction from baseline. Further, filgotinib has also shown good efficacy for the articular domain in terms of ACR 20 response. Of note, these agents appear to be very safe, with only mild AEs, more often represented by nasopharyngitis and headache, with no statistical differences in AE frequency in comparison with placebo groups.68–70
RCTs focused on investigational JAK inhibitors with preferential JAK1/JAK2 (Baricitinib) or JAK3 selectivity (Peficitinib) have shown improvements in cutaneous outcomes in terms of PASI score (PASI75 and PASI90) for baricitinib, PGA and BSA, with no serious AEs reported.71,72
Among investigational TYK2 inhibitors, brepocitinib (PF-06700841) and ropsacitinib (PF-06826647) appear promising due to their efficacy in terms of articular (ACR20 response rate) and cutaneous outcomes (PASI50/75/90/100 and PGA 0/1 response) (up to 52 weeks and 40 weeks, respectively).76,77,123–125
In both psoriasis and PsA RCTs, investigational TYK2 inhibitors were generally well-tolerated, with mild AEs (nasopharyngitis, headache, diarrhea, nausea, and upper respiratory tract infection) and no major adverse cardiovascular events, venous thromboembolic events, serious infections, or deaths occurred.110
An increasing number of JAK inhibitors for treating PsD is being investigated, and preliminary results from phase II and III trials show promising results. However, further investigation of these molecules is needed to evaluate their efficacy and safety in PsD patients.
Data Sharing Statement
The authors confirm that the data supporting the findings of this study are available within the article.
Ethical Approval
Local Ethics Committee, University of Naples Federico II, 408/19.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Boehncke WH, Schön MP. Psoriasis. Lancet. 2015;386(9997):983–994. doi:10.1016/S0140-6736(14)61909-7
2. Napolitano M, Caso F, Scarpa R, et al. Psoriatic arthritis and psoriasis: differential diagnosis. Clin Rheumatol. 2016;35(8):1893–1901. doi:10.1007/s10067-016-3295-9
3. Ruggiero A, Potestio L, Cacciapuoti S, et al. Tildrakizumab for the treatment of moderate to severe psoriasis: results from a single center preliminary real-life study. Dermatol Ther. 2022;35(12):e15941. doi:10.1111/dth.15941
4. Megna M, Ruggiero A, Battista T, Marano L, Cacciapuoti S, Potestio L. Long-term efficacy and safety of risankizumab for moderate to severe psoriasis: a 2-year real-life retrospective study. J Clin Med. 2023;12(9):3233. doi:10.3390/jcm12093233
5. Bhosle MJ, Kulkarni A, Feldman SR, Balkrishnan R. Quality of life in patients with psoriasis. Health Qual Life Outcomes. 2006;4:35. doi:10.1186/1477-7525-4-35
6. Potestio L, Camela E, Cacciapuoti S, et al. Biologics for the management of erythrodermic psoriasis: an updated review. Clin Cosmet Investig Dermatol. 2023;16:2045–2059. doi:10.2147/CCID.S407813
7. Megna M, Camela E, Ruggiero A, et al. Use of biological therapies for the management of pustular psoriasis: a new era? Clin Cosmet Investig Dermatol. 2023;16:1677–1690. doi:10.2147/CCID.S407812
8. Chimenti MS, Caso F, Alivernini S, et al. Amplifying the concept of psoriatic arthritis: the role of autoimmunity in systemic psoriatic disease. Autoimmun Rev. 2019;18(6):565–575. doi:10.1016/j.autrev.2018.11.007
9. Scarpa R, Caso F, Costa L, Peluso R, Del Puente A, Olivieri I. Psoriatic Disease 10 Years Later. J Rheumatol. 2017;44(9):1298–1301. doi:10.3899/jrheum.161402
10. Megna M, Ocampo-Garza SS, Potestio L, et al. New-onset psoriatic arthritis under biologics in psoriasis patients: an increasing challenge? Biomedicines. 2021;9(10):1482. doi:10.3390/biomedicines9101482
11. Toussirot E, Gallais-Sérézal I, Aubin F. The cardiometabolic conditions of psoriatic disease. Front Immunol. 2022;13:970371. doi:10.3389/fimmu.2022.970371
12. Caso F, Del Puente A, Oliviero F, et al. Metabolic syndrome in psoriatic arthritis: the interplay with cutaneous involvement. Evidences from literature and a recent cross-sectional study. Clin Rheumatol. 2018;37(3):579–586. doi:10.1007/s10067-017-3975-0
13. Caso F, Chimenti MS, Navarini L, et al. Metabolic Syndrome and psoriatic arthritis: considerations for the clinician. Expert Rev Clin Immunol. 2020;16(4):409–420. doi:10.1080/1744666X.2020.1740593
14. Ogdie A, Gelfand JM. Clinical risk factors for the development of psoriatic arthritis among patients with psoriasis: a review of available evidence. Curr Rheumatol Rep. 2015;17(10):64. doi:10.1007/s11926-015-0540-1
15. Mishra S, Kancharla H, Dogra S, Sharma A. Comparison of four validated psoriatic arthritis screening tools in diagnosing psoriatic arthritis in patients with psoriasis (COMPAQ Study). Br J Dermatol. 2017;176(3):765–770. doi:10.1111/bjd.14929
16. Caso F, Postiglione L, Covelli B, et al. Pro-inflammatory adipokine profile in psoriatic arthritis: results from a cross-sectional study comparing PsA subset with evident cutaneous involvement and subset “sine psoriasis”. Clin Rheumatol. 2019;38(9):2547–2552. doi:10.1007/s10067-019-04619-w
17. Tashiro T, Sawada Y. Psoriasis and Systemic Inflammatory Disorders. Int J Mol Sci. 2022;23(8):4457. doi:10.3390/ijms23084457
18. Campanati A, Marani A, Martina E, Diotallevi F, Radi G, Offidani A. Psoriasis as an immune-mediated and inflammatory systemic disease: from pathophysiology to novel therapeutic approaches. Biomedicines. 2021;9(11):1511. doi:10.3390/biomedicines9111511
19. Ruggiero A, Camela E, Potestio L, Fabbrocini G, Megna M. Drug safety evaluation of tildrakizumab for psoriasis: a review of the current knowledge. Expert Opin Drug Saf. 2022;21(12):1445–1451. doi:10.1080/14740338.2022.2160447
20. Megna M, Potestio L, Fabbrocini G, Cinelli E. Tildrakizumab: a new therapeutic option for erythrodermic psoriasis? Dermatol Ther. 2021;34:e15030. doi:10.1111/dth.15030
21. Megna M, Potestio L, Camela E, Fabbrocini G, Ruggiero A. Ixekizumab and brodalumab indirect comparison in the treatment of moderate to severe psoriasis: results from an Italian single-center retrospective study in a real-life setting. Dermatol Ther. 2022;35:e15667. doi:10.1111/dth.15667
22. Yang F, Lu C, Wang Y, Liu H, Leng X, Zeng X. Efficacy and safety of Janus kinase inhibitors in patients with psoriasis and psoriatic arthritis: a systematic review and meta-analysis. Clin Rheumatol. 2023;42(6):1593–1605. doi:10.1007/s10067-023-06529-4
23. Caso F, Costa L, Triggianese P, et al. Recent developments for new investigational JAK inhibitors in psoriatic arthritis. Expert Opin Investig Drugs. 2023;32(5):361–371. doi:10.1080/13543784.2023.2207737
24. Rendon A, Schäkel K. Psoriasis Pathogenesis and Treatment. Int J Mol Sci. 2019;20(6):1475. doi:10.3390/ijms20061475
25. Harden JL, Krueger JG, Bowcock AM. The immunogenetics of Psoriasis: a comprehensive review. J Autoimmun. 2015;64:66–73. doi:10.1016/j.jaut.2015.07.008
26. Camela E, Potestio L, Fabbrocini G, Pallotta S, Megna M. The holistic approach to psoriasis patients with comorbidities: the role of investigational drugs. Expert Opin Investig Drugs. 2023;1–16. doi:10.1080/13543784.2023.2219387
27. Cacciapuoti S, Potestio L, Guerrasio G, et al. Effectiveness of brodalumab in patients with moderate-to-severe plaque psoriasis located in difficult-to-treat areas. Clin Cosmet Investig Dermatol. 2023;16:2637–2644. doi:10.2147/CCID.S423234
28. Singh S, Pradhan D, Puri P, et al. Genomic alterations driving psoriasis pathogenesis. Gene. 2019;683:61–71. doi:10.1016/j.gene.2018.09.042
29. Komine M, Freedberg IM, Blumenberg M. Regulation of epidermal expression of keratin K17 in inflammatory skin diseases. J Invest Dermatol. 1996;107(4):569–575. doi:10.1111/1523-1747.ep12582820
30. Zeng R, Spolski R, Casas E, Zhu W, Levy DE, Leonard WJ. The molecular basis of IL-21-mediated proliferation. Blood. 2007;109(10):4135–4142. doi:10.1182/blood-2006-10-054973
31. Ishizaki M, Muromoto R, Akimoto T, et al. Tyk2 is a therapeutic target for psoriasis-like skin inflammation. Int Immunol. 2014;26(5):257–267. doi:10.1093/intimm/dxt062
32. Azuaga AB, Ramírez J, Cañete JD. Psoriatic arthritis: pathogenesis and targeted therapies. Int J Mol Sci. 2023;24(5):4901. doi:10.3390/ijms24054901
33. Caso F, Costa L, Chimenti MS, Navarini L, Punzi L. Pathogenesis of Psoriatic Arthritis. Crit Rev Immunol. 2019;39(5):361–377. doi:10.1615/CritRevImmunol.2020033243
34. Marasca C, Ruggiero A, Napolitano M, et al. May COVID-19 outbreaks lead to a worsening of skin chronic inflammatory conditions? Med Hypotheses. 2020;143:109853. doi:10.1016/j.mehy.2020.109853
35. Fiocco U, Accordi B, Martini V, et al. JAK/STAT/PKCδ molecular pathways in synovial fluid T lymphocytes reflect the in vivo T helper-17 expansion in psoriatic arthritis. Immunol Res. 2014;58(1):61–69. doi:10.1007/s12026-013-8481-0
36. Fiocco U, Martini V, Accordi B, et al. Transcriptional network profile on synovial fluid T cells in psoriatic arthritis. Clin Rheumatol. 2015;34(9):1571–1580. doi:10.1007/s10067-015-3002-2
37. Fiocco U, Martini V, Accordi B, et al. Ex vivo signaling protein mapping in t lymphocytes in the psoriatic arthritis joints. J Rheumatol Suppl. 2015;93:48–52. doi:10.3899/jrheum.150636
38. Caso F, Saviano A, Tasso M, et al. Analysis of rheumatoid- vs psoriatic arthritis synovial fluid reveals differential macrophage (CCR2) and T helper subsets (STAT3/4 and FOXP3) activation. Autoimmun Rev. 2022;21(12):103207. doi:10.1016/j.autrev.2022.103207
39. Navarini L, Currado D, Costa L, Tasso M, Chimenti MS, Caso F. Experimental and investigational pharmacotherapy for psoriatic arthritis: drugs of the future. J Exp Pharmacol. 2020;12:487–502. doi:10.2147/JEP.S265633
40. Caso F, Navarini L, Ruscitti P, et al. Targeted synthetic pharmacotherapy for psoriatic arthritis: state of the art. Expert Opin Pharmacother. 2020;21(7):785–796. doi:10.1080/14656566.2020.1726317
41. Mattei PL, Corey KC, Kimball AB. Psoriasis area severity index (PASI) and the dermatology life quality index (DLQI): the correlation between disease severity and psychological burden in patients treated with biological therapies. J Eur Acad Dermatol Venereol. 2014;28(3):333–337. doi:10.1111/jdv.12106
42. Fernández-Torres RM, Paradela S, Fonseca E. Long-term response to etanercept monotherapy in moderate to severe psoriasis: assessment in daily practice by the maintenance of low values of PASI and BSA. J Dermatolog Treat. 2014;25(1):54–56. doi:10.3109/09546634.2012.755254
43. Gisondi P, Fargnoli MC, Amerio P, et al. Italian adaptation of EuroGuiDerm guideline on the systemic treatment of chronic plaque psoriasis. Ital J Dermatology Venereol. 2022;157(Suppl. 1 to No. 1):1–78. doi:10.23736/S2784-8671.21.07132-2
44. Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI)--a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19(3):210–216. doi:10.1111/j.1365-2230.1994.tb01167.x
45. Nast A, Smith C, Spuls PI, et al. EuroGuiDerm Guideline on the systemic treatment of Psoriasis vulgaris - Part 2: specific clinical and comorbid situations. J Eur Acad Dermatol Venereol. 2021;35(2):281–317. doi:10.1111/jdv.16926
46. Nast A, Smith C, Spuls PI, et al. EuroGuiDerm Guideline on the systemic treatment of Psoriasis vulgaris - Part 1: treatment and monitoring recommendations. J Eur Acad Dermatol Venereol. 2020;34(11):2461–2498. doi:10.1111/jdv.16915
47. Scarpa R, Caso F. Spondyloarthritis: which composite measures to use in psoriatic arthritis? Nat Rev Rheumatol. 2018;14(3):125–126. doi:10.1038/nrrheum.2018.15
48. Tucker LJ, Coates LC, Helliwell PS. Assessing Disease Activity in Psoriatic Arthritis: a Literature Review. Rheumatol Ther. 2019;6(1):23–32. doi:10.1007/s40744-018-0132-4
49. Megna M, Camela E, Battista T, et al. Efficacy and safety of biologics and small molecules for psoriasis in pediatric and geriatric populations. Part I: focus on pediatric patients. Expert Opin Drug Saf. 2023:1–17. doi:10.1080/14740338.2023.2173170
50. Megna M, Camela E, Battista T, et al. Efficacy and safety of biologics and small molecules for psoriasis in pediatric and geriatric populations. Part II: focus on elderly patients. Expert Opin Drug Saf. 2023:1–16. doi:10.1080/14740338.2023.2173171
51. Costa L, Lubrano E, Ramonda R, et al. Elderly psoriatic arthritis patients on TNF-α blockers: results of an Italian multicenter study on minimal disease activity and drug discontinuation rate. Clin Rheumatol. 2017;36(8):1797–1802. doi:10.1007/s10067-017-3697-3
52. Caso F, Tasso M, Chimenti MS, et al. Late-onset and elderly psoriatic arthritis: clinical aspects and management. Drugs Aging. 2019;36(10):909–925. doi:10.1007/s40266-019-00688-3
53. Jiang Y, Chen Y, Yu Q, Shi Y. Biologic and small-molecule therapies for moderate-to-severe psoriasis: focus on psoriasis comorbidities. BioDrugs. 2023;37(1):35–55. doi:10.1007/s40259-022-00569-z
54. Caso F, Lubrano E, Del Puente A, et al. Progress in understanding and utilizing TNF-α inhibition for the treatment of psoriatic arthritis. Expert Rev Clin Immunol. 2016;12(3):315–331. doi:10.1586/1744666X.2016.1117941
55. Caso F, Del Puente A, Peluso R, et al. Emerging drugs for psoriatic arthritis. Expert Opin Emerg Drugs. 2016;21(1):69–79. doi:10.1517/14728214.2016.1146679
56. Coates L, Gossec L. The updated GRAPPA and EULAR recommendations for the management of psoriatic arthritis: similarities and differences. Jt Bone Spine. 2023;90(1):105469. doi:10.1016/j.jbspin.2022.105469
57. Costa L, Perricone C, Chimenti MS, et al. Switching between biological treatments in psoriatic arthritis: a review of the evidence. Drugs R D. 2017;17(4):509–522. doi:10.1007/s40268-017-0215-7
58. Chimenti MS, Triggianese P, De Martino E, et al. An update on pathogenesis of psoriatic arthritis and potential therapeutic targets. Expert Rev Clin Immunol. 2019;15(8):823–836. doi:10.1080/1744666X.2019.1627876
59. Zagaria O, Villani A, Ruggiero A, et al. New-onset lichen planus arising after COVID-19 vaccination. Dermatol Ther. 2022;35(5):e15374. doi:10.1111/dth.15374
60. Ruggiero A, Martora F, Picone V, et al. The impact of COVID-19 infection on patients with psoriasis treated with biologics: an Italian experience. Clin Exp Dermatol. 2022;47(12):2280–2282. doi:10.1111/ced.15336
61. Keating GM. Apremilast: a review in psoriasis and psoriatic arthritis. Drugs. 2017;77(4):459–472. doi:10.1007/s40265-017-0709-1
62. Costa L, Del Puente A, Peluso R, et al. Small molecule therapy for managing moderate to severe psoriatic arthritis. Expert Opin Pharmacother. 2017;18(15):1557–1567. doi:10.1080/14656566.2017.1378343
63. Martora F, Scalvenzi M, Ruggiero A, Potestio L, Battista T, Megna M. Hidradenitis suppurativa and JAK inhibitors: a review of the published literature. Medicina. 2023;59(4). doi:10.3390/medicina59040801
64. Martora F, Scalvenzi M, Battista T, et al. Guselkumab, risankizumab, and tildrakizumab in the management of hidradenitis suppurativa: a review of existing trials and real-life data. Clin Cosmet Investig Dermatol. 2023;16:2525–2536. doi:10.2147/CCID.S418748
65. Papp KA, Menter A, Strober B, et al. Efficacy and safety of tofacitinib, an oral Janus kinase inhibitor, in the treatment of psoriasis: a Phase 2b randomized placebo-controlled dose-ranging study. Br J Dermatol. 2012;167(3):668–677. doi:10.1111/j.1365-2133.2012.11168.x
66. Papp KA, Menter MA, Abe M, et al. Tofacitinib, an oral Janus kinase inhibitor, for the treatment of chronic plaque psoriasis: results from two randomized, placebo-controlled, phase III trials. Br J Dermatol. 2015;173(4):949–961. doi:10.1111/bjd.14018
67. Bachelez H, van de Kerkhof PCM, Strohal R, et al. Tofacitinib versus etanercept or placebo in moderate-to-severe chronic plaque psoriasis: a phase 3 randomised non-inferiority trial. Lancet. 2015;386(9993):552–561. doi:10.1016/S0140-6736(14)62113-9
68. Bissonnette R, Luchi M, Fidelus-Gort R, et al. A randomized, double-blind, placebo-controlled, dose-escalation study of the safety and efficacy of INCB039110, an oral janus kinase 1 inhibitor, in patients with stable, chronic plaque psoriasis. J Dermatolog Treat. 2016;27(4):332–338. doi:10.3109/09546634.2015.1115819
69. Schmieder GJ, Draelos ZD, Pariser DM, et al. Efficacy and safety of the Janus kinase 1 inhibitor PF-04965842 in patients with moderate-to-severe psoriasis: phase II, randomized, double-blind, placebo-controlled study. Br J Dermatol. 2018;179(1):54–62. doi:10.1111/bjd.16004
70. Ludbrook VJ, Hicks KJ, Hanrott KE, et al. Investigation of selective JAK1 inhibitor GSK2586184 for the treatment of psoriasis in a randomized placebo-controlled phase IIa study. Br J Dermatol. 2016;174(5):985–995. doi:10.1111/bjd.14399
71. Papp KA, Menter MA, Raman M, et al. A randomized phase 2b trial of baricitinib, an oral Janus kinase (JAK) 1/JAK2 inhibitor, in patients with moderate-to-severe psoriasis. Br J Dermatol. 2016;174(6):1266–1276. doi:10.1111/bjd.14403
72. Papp K, Pariser D, Catlin M, et al. A phase 2a randomized, double-blind, placebo-controlled, sequential dose-escalation study to evaluate the efficacy and safety of ASP015K, a novel Janus kinase inhibitor, in patients with moderate-to-severe psoriasis. Br J Dermatol. 2015;173(3):767–776. doi:10.1111/bjd.13745
73. Papp K, Gordon K, Thaçi D, et al. Phase 2 Trial of Selective Tyrosine Kinase 2 Inhibition in Psoriasis. N Engl J Med. 2018;379(14):1313–1321. doi:10.1056/NEJMoa1806382
74. Armstrong AW, Gooderham M, Warren RB, et al. Deucravacitinib versus placebo and apremilast in moderate to severe plaque psoriasis: efficacy and safety results from the 52-week, randomized, double-blinded, placebo-controlled phase 3 POETYK PSO-1 trial. J Am Acad Dermatol. 2023;88(1):29–39. doi:10.1016/j.jaad.2022.07.002
75. Strober B, Thaçi D, Sofen H, et al. Deucravacitinib versus placebo and apremilast in moderate to severe plaque psoriasis: efficacy and safety results from the 52-week, randomized, double-blinded, phase 3 Program fOr Evaluation of TYK2 inhibitor psoriasis second trial. J Am Acad Dermatol. 2023;88(1):40–51. doi:10.1016/j.jaad.2022.08.061
76. Mease P, Helliwell P, Silwinska-Stanczyk P, et al. Efficacy and safety of brepocitinib (tyrosine kinase 2/janus kinase 1 inhibitor) for the treatment of active psoriatic arthritis: results from a phase 2b randomized controlled trial. Arthr Rheu. 2021;73:1009–1011.
77. Tehlirian C, Singh RSP, Pradhan V, et al. Oral tyrosine kinase 2 inhibitor PF-06826647 demonstrates efficacy and an acceptable safety profile in participants with moderate-to-severe plaque psoriasis in a phase 2b, randomized, double-blind, placebo-controlled study. J Am Acad Dermatol. 2022;87(2):333–342. doi:10.1016/j.jaad.2022.03.059
78. Berekmeri A, Mahmood F, Wittmann M, Helliwell P. Tofacitinib for the treatment of psoriasis and psoriatic arthritis. Expert Rev Clin Immunol. 2018;14(9):719–730. doi:10.1080/1744666X.2018.1512404
79. Leung YY, Korotaeva T, Candia L, et al. Management of peripheral arthritis in patients with psoriatic arthritis: an updated literature review informing the 2021 GRAPPA treatment recommendations. J Rheumatol. 2022;49(12):1. doi:10.3899/jrheum.220315.C1
80. Mease P, Hall S, FitzGerald O, et al. Tofacitinib or Adalimumab versus Placebo for Psoriatic Arthritis. N Engl J Med. 2017;377(16):1537–1550. doi:10.1056/NEJMoa1615975
81. Gladman D, Rigby W, Azevedo VF, et al. Tofacitinib for psoriatic arthritis in patients with an inadequate response to TNF inhibitors. N Engl J Med. 2017;377(16):1525–1536. doi:10.1056/NEJMoa1615977
82. Nash P, Coates LC, Kivitz AJ, et al. Safety and efficacy of tofacitinib in patients with active psoriatic arthritis: interim analysis of OPAL balance, an open-label, long-term extension study. Rheumatol Ther. 2020;7(3):553–580. doi:10.1007/s40744-020-00209-4
83. Strand V, de Vlam K, Covarrubias-Cobos JA, et al. Effect of tofacitinib on patient-reported outcomes in patients with active psoriatic arthritis and an inadequate response to tumour necrosis factor inhibitors in the Phase III, randomised controlled trial: OPAL Beyond. RMD Open. 2019;5(1):e000808. doi:10.1136/rmdopen-2018-000808
84. Nash P, Coates LC, Fleischmann R, et al. Efficacy of tofacitinib for the treatment of psoriatic arthritis: pooled analysis of two phase 3 studies. Rheumatol Ther. 2018;5(2):567–582. doi:10.1007/s40744-018-0131-5
85. Strand V, de Vlam K, Covarrubias-Cobos JA, et al. Tofacitinib or Adalimumab versus placebo: patient-reported outcomes from OPAL Broaden-a phase III study of active psoriatic arthritis in patients with an inadequate response to conventional synthetic disease-modifying antirheumatic drugs. RMD Open. 2019;5(1):e000806. doi:10.1136/rmdopen-2018-000806
86. van der Heijde D, Gladman DD, FitzGerald O, et al. Radiographic progression according to baseline c-reactive protein levels and other risk factors in psoriatic arthritis treated with tofacitinib or Adalimumab. J Rheumatol. 2019;46(9):1089–1096. doi:10.3899/jrheum.180971
87. Papp KA, Krueger JG, Feldman SR, et al. Tofacitinib, an oral Janus kinase inhibitor, for the treatment of chronic plaque psoriasis: long-term efficacy and safety results from 2 randomized phase-III studies and 1 open-label long-term extension study. J Am Acad Dermatol. 2016;74(5):841–850. doi:10.1016/j.jaad.2016.01.013
88. Valenzuela F, Korman NJ, Bissonnette R, et al. Tofacitinib in patients with moderate-to-severe chronic plaque psoriasis: long-term safety and efficacy in an open-label extension study. Br J Dermatol. 2018;179(4):853–862. doi:10.1111/bjd.16798
89. Winthrop KL, Cohen SB. Oral surveillance and JAK inhibitor safety: the theory of relativity. Nat Rev Rheumatol. 2022;18(5):301–304. doi:10.1038/s41584-022-00767-7
90. Burmester GR, Nash P, Sands BE, et al. Adverse events of special interest in clinical trials of rheumatoid arthritis, psoriatic arthritis, ulcerative colitis and psoriasis with 37 066 patient-years of tofacitinib exposure. RMD Open. 2021;7(2):e001595. doi:10.1136/rmdopen-2021-001595
91. Ytterberg SR, Bhatt DL, Mikuls TR, et al. Cardiovascular and Cancer Risk with Tofacitinib in Rheumatoid Arthritis. N Engl J Med. 2022;386(4):316–326. doi:10.1056/NEJMoa2109927
92. McInnes IB, Anderson JK, Magrey M, et al. Trial of upadacitinib and adalimumab for psoriatic arthritis. N Engl J Med. 2021;384(13):1227–1239. doi:10.1056/NEJMoa2022516
93. Mease PJ, Lertratanakul A, Anderson JK, et al. Upadacitinib for psoriatic arthritis refractory to biologics: SELECT-PsA 2. Ann Rheum Dis. 2021;80(3):312–320. doi:10.1136/annrheumdis-2020-218870
94. McInnes IB, Kato K, Magrey M, et al. Upadacitinib in patients with psoriatic arthritis and an inadequate response to non-biological therapy: 56-week data from the phase 3 SELECT-PsA 1 study. RMD Open. 2021;7(3):e001838. doi:10.1136/rmdopen-2021-001838
95. McInnes IB, Kato K, Magrey M, et al. Efficacy and safety of upadacitinib in patients with psoriatic arthritis: 2-year results from the phase 3 SELECT-PsA 1 study. Rheumatol Ther. 2023;10(1):275–292. doi:10.1007/s40744-022-00499-w
96. Mease PJ, Lertratanakul A, Papp KA, et al. Upadacitinib in patients with psoriatic arthritis and inadequate response to biologics: 56-week data from the randomized controlled phase 3 SELECT-PsA 2 study. Rheumatol Ther. 2021;8(2):903–919. doi:10.1007/s40744-021-00305-z
97. Strand V, Mease PJ, Soriano ER, et al. Improvement in patient-reported outcomes in patients with psoriatic arthritis treated with upadacitinib versus placebo or adalimumab: results from SELECT-PsA 1. Rheumatol Ther. 2021;8(4):1789–1808. doi:10.1007/s40744-021-00379-9
98. Strand V, Van den Bosch F, Ranza R, et al. Patient-reported outcomes in psoriatic arthritis patients with an inadequate response to biologic disease-modifying antirheumatic drugs: SELECT-PsA 2. Rheumatol Ther. 2021;8(4):1827–1844. doi:10.1007/s40744-021-00377-x
99. Mease P, Kavanaugh A, Gladman D, et al. Disease control with upadacitinib in patients with psoriatic arthritis: a post hoc analysis of the randomized, placebo-controlled SELECT-PsA 1 and 2 phase 3 trials. Rheumatol Ther. 2022;9(4):1181–1191. doi:10.1007/s40744-022-00449-6
100. Megna M, Caiazzo G, Parisi M, et al. Eczematous drug eruption in patients with psoriasis under anti-interleukin-17A: does interleukin-22 play a key role? Clin Exp Dermatol. 2022;47(5):918–925. doi:10.1111/ced.15052
101. Gargiulo L, Ibba L, Pavia G, et al. Upadacitinib for the treatment of concomitant psoriasis and atopic dermatitis: a case series. J Dermatolog Treat. 2023;34(1):2183729. doi:10.1080/09546634.2023.2183729
102. Mease P, Coates LC, Helliwell PS, et al. Efficacy and safety of filgotinib, a selective Janus kinase 1 inhibitor, in patients with active psoriatic arthritis (EQUATOR): results from a randomised, placebo-controlled, phase 2 trial. Lancet. 2018;392(10162):2367–2377. doi:10.1016/S0140-6736(18)32483-8
103. Orbai AM, Ogdie A, Gossec L, et al. Effect of filgotinib on health-related quality of life in active psoriatic arthritis: a randomized phase 2 trial (EQUATOR). Rheumatology. 2020;59(7):1495–1504. doi:10.1093/rheumatology/kez408
104. To evaluate the efficacy and safety of shr0302 tablet in subjects of active psoriatic arthritis. Available from: https://classic.clinicaltrials.gov/ct2/show/NCT04957550.
105. Lé AM, Puig L, Torres T. Deucravacitinib for the treatment of psoriatic disease. Am J Clin Dermatol. 2022;23(6):813–822. doi:10.1007/s40257-022-00720-0
106. Burke JR, Cheng L, Gillooly KM, et al. Autoimmune pathways in mice and humans are blocked by pharmacological stabilization of the TYK2 pseudokinase domain. Sci Transl Med. 2019;11(502). doi:10.1126/scitranslmed.aaw1736
107. Thaçi D, Strober B, Gordon KB, et al. Deucravacitinib in moderate to severe psoriasis: clinical and quality-of-life outcomes in a phase 2 trial. Dermatol Ther. 2022;12(2):495–510. doi:10.1007/s13555-021-00649-y
108. Warren RB, Sofen H, Imafuku S, et al. POS1046 deucravacitinib long-term efficacy and safety in plaque psoriasis: 2-year results from the phase 3 poetyk PSO program. Ann Rheum Dis. 2022;81:841. doi:10.1136/annrheumdis-2022-eular.2445
109. Imafuku S, Tada Y, Hippeli L, Banerjee S, Morita A, Ohtsuki M. Efficacy and safety of the selective TYK2 inhibitor, deucravacitinib, in Japanese patients with moderate to severe plaque psoriasis: subgroup analysis of a randomized, double-blind, placebo-controlled, global phase 3 trial. J Dermatol. 2023;50(5):588–595. doi:10.1111/1346-8138.16740
110. Mease PJ, Deodhar AA, van der Heijde D, et al. Efficacy and safety of selective TYK2 inhibitor, deucravacitinib, in a phase II trial in psoriatic arthritis. Ann Rheum Dis. 2022;81(6):815–822. doi:10.1136/annrheumdis-2021-221664
111. Calabrese L, Malvaso D, Antonelli F, Mannino M, Peris K, Chiricozzi A. Investigational systemic drugs for moderate to severe plaque psoriasis: what’s new? Expert Opin Investig Drugs. 2023;32(3):229–243. doi:10.1080/13543784.2023.2184684
112. Martin G. Novel therapies in plaque psoriasis: a review of tyrosine kinase 2 inhibitors. Dermatol Ther (Heidelb). 2023;13(2):417–435. doi:10.1007/s13555-022-00878-9
113. Page KM, Suarez-Farinas M, Suprun M, et al. Molecular and cellular responses to the TYK2/JAK1 Inhibitor PF-06700841 reveal reduction of skin inflammation in plaque psoriasis. J Invest Dermatol. 2020;140(8):1546–1555.e4. doi:10.1016/j.jid.2019.11.027
114. Forman SB, Pariser DM, Poulin Y, et al. TYK2/JAK1 inhibitor PF-06700841 in patients with plaque psoriasis: phase iia, randomized, double-blind, placebo-controlled trial. J Invest Dermatol. 2020;140(12):2359–2370.e5. doi:10.1016/j.jid.2020.03.962
115. Landis MN, Smith SR, Berstein G, et al. Efficacy and safety of topical brepocitinib cream for mild-to-moderate chronic plaque psoriasis: a phase IIb randomized double-blind vehicle-controlled parallel-group study. Br J Dermatol. 2023;189(1):33–41. doi:10.1093/bjd/ljad098
116. Banfield C, Scaramozza M, Zhang W, et al. The safety, tolerability, pharmacokinetics, and Pharmacodynamics of a TYK2/JAK1 Inhibitor (PF-06700841) in healthy subjects and patients with plaque psoriasis. J Clin Pharmacol. 2018;58(4):434–447. doi:10.1002/jcph.1046
117. Alumis Inc. A study to evaluate the efficacy and safety of ESK-001 in patients with plaque psoriasis. Available from: https://clinicaltrials.gov/study/NCT05600036?cond=Plaque%20Psoriasis&term=esk-001&rank=2.
118. Takeda. A Study to Evaluate the Efficacy, Safety, and Tolerability of NDI-034858 in Subjects With Active Psoriatic Arthritis. https://clinicaltrials.gov/study/NCT05153148?cond=Psoriatic%20Arthritis&term=NDI-034858&rank=1.
119. Megna M, Battista T, Potestio L, et al. A case of erythrodermic psoriasis rapidly and successfully treated with Bimekizumab. J Cosmet Dermatol. 2023;22(3):1146–1148. doi:10.1111/jocd.15543
120. Gargiulo L, Narcisi A, Ibba L, et al. Effectiveness and safety of bimekizumab for the treatment of plaque psoriasis: a real-life multicenter study-IL PSO (Italian landscape psoriasis). Front Med. 2023;10:1243843. doi:10.3389/fmed.2023.1243843
121. Ruggiero A, Potestio L, Martora F, Villani A, Comune R, Megna M. Bimekizumab treatment in patients with moderate to severe plaque psoriasis: a drug safety evaluation. Expert Opin Drug Saf. 2023;22:355–362. doi:10.1080/14740338.2023.2218086
122. Camela E, Potestio L, Fabbrocini G, Ruggiero A, Megna M. New frontiers in personalized medicine in psoriasis. Expert Opin Biol Ther. 2022;1–3. doi:10.1080/14712598.2022.2113872
123. Marasca C, Ruggiero A, Annunziata MC, Fabbrocini G, Megna M. Face the COVID-19 emergency: measures applied in an Italian dermatologic clinic. J Eur Acad Dermatol Venereol. 2020;34(6):e249. doi:10.1111/jdv.16476
124. Martora F, Marasca C, Fabbrocini G, Ruggiero A. Strategies adopted in a southern Italian referral centre to reduce Adalimumab discontinuation: comment on ‘Can we increase the drug survival time of biologic therapies in hidradenitis suppurativa?’. Clin Exp Dermatol. 2022;47(10):1864–1865. doi:10.1111/ced.15291
125. Ruggiero A, Megna M, Fabbrocini G, Martora F. Video and telephone teledermatology consultations during COVID-19 in comparison: patient satisfaction, doubts and concerns. Clin Exp Dermatol. 2022;47(10):1863–1864. doi:10.1111/ced.15286
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effectiveness and Safety of Deucravacitinib for the Management of Psoriasis: A Review of the Current Literature
Potestio L, Ruggiero A, Fabbrocini G, Martora F, Megna M
Psoriasis: Targets and Therapy 2023, 13:19-26
Published Date: 4 May 2023
The Impact of Targeted Therapies on the Bone-Vascular Axis in Psoriasis: A Narrative Review
Zeng H, Chen Y, Yang L
Clinical, Cosmetic and Investigational Dermatology 2026, 19:595065
Published Date: 1 April 2026