")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
JAK Inhibitors as Potential Therapeutic Strategy for the Dilemma of Psoriasis Concurrent with Dermatomyositis in the SARS-CoV-2 Era
Received 6 February 2023
Accepted for publication 15 April 2023
Published 20 April 2023 Volume 2023:16 Pages 1059—1062
DOI https://doi.org/10.2147/CCID.S403970
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Qiannan Xu, Nan Xu
Department of Dermatology, Shanghai East Hospital, Tongji University School of Medicine, Shanghai, People’s Republic of China
Correspondence: Nan Xu, Tel +86 38804518, Email [email protected]
Abstract: Dermatomyositis is a rare inflammatory disease with potentially life-threatening systemic involvement that is treated with systemic corticosteroids. However, when psoriasis coexists with dermatomyositis, the administration of corticosteroids may exacerbate psoriasis after withdrawal, posing a treatment dilemma. Our search of the literature revealed 14 cases where various treatments were used, including methotrexate, corticosteroids, cyclosporin, ustekinumab, mycophenolate mofetil, and azathioprine. While methotrexate showed promise, it carries risks, and corticosteroids were used despite their potential to exacerbate psoriasis. Based on transcriptomic data analysis of psoriasis and dermatomyositis, the type II interferon-mediated signaling pathway was enriched in both diseases. Medication targeting this pathway, such as JAK inhibitors, could be a potential solution for the psoriasis concurrent with dermatomyositis dilemma, as JAK inhibitors have been proven effective in treating both dermatomyositis and psoriasis, with some being FDA-approved for treating COVID-19. Therefore, JAK inhibitors may be a potential therapeutic strategy for psoriasis concurrent with dermatomyositis in the SARS-CoV-2 era.
Keywords: psoriasis, dermatomyositis, treatment, JAK, SARS-CoV-2
Dermatomyositis is a rare inflammatory disease that presents distinct cutaneous manifestations and various degrees of potentially life-threatening systemic involvement,1 such as pulmonary diseases or malignancies. The first-line therapy for managing dermatomyositis is systemic corticosteroids. However, in cases where psoriasis coexists with dermatomyositis, the administration of systemic corticosteroids may pose a dilemma due to concerns regarding the potential exacerbation of psoriasis after corticosteroid withdrawal.
In order to figure out the possible solution for this dilemma, we prepared a comprehensive full strategic electronic search of the PubMed, Scopus, Google Scholar and EBSCO databases, using the following keywords ‘psoriasis’, ‘dermatomyositis’ and covering the period 2003–2022. Over 200 articles were found. After reviewing these articles, fourteen cases2–13 were concluded (Table 1). The treatment of these cases concluded methotrexate, corticosteroids, cyclosporin, ustekinumab, mycophenolate mofetil and azathioprine.
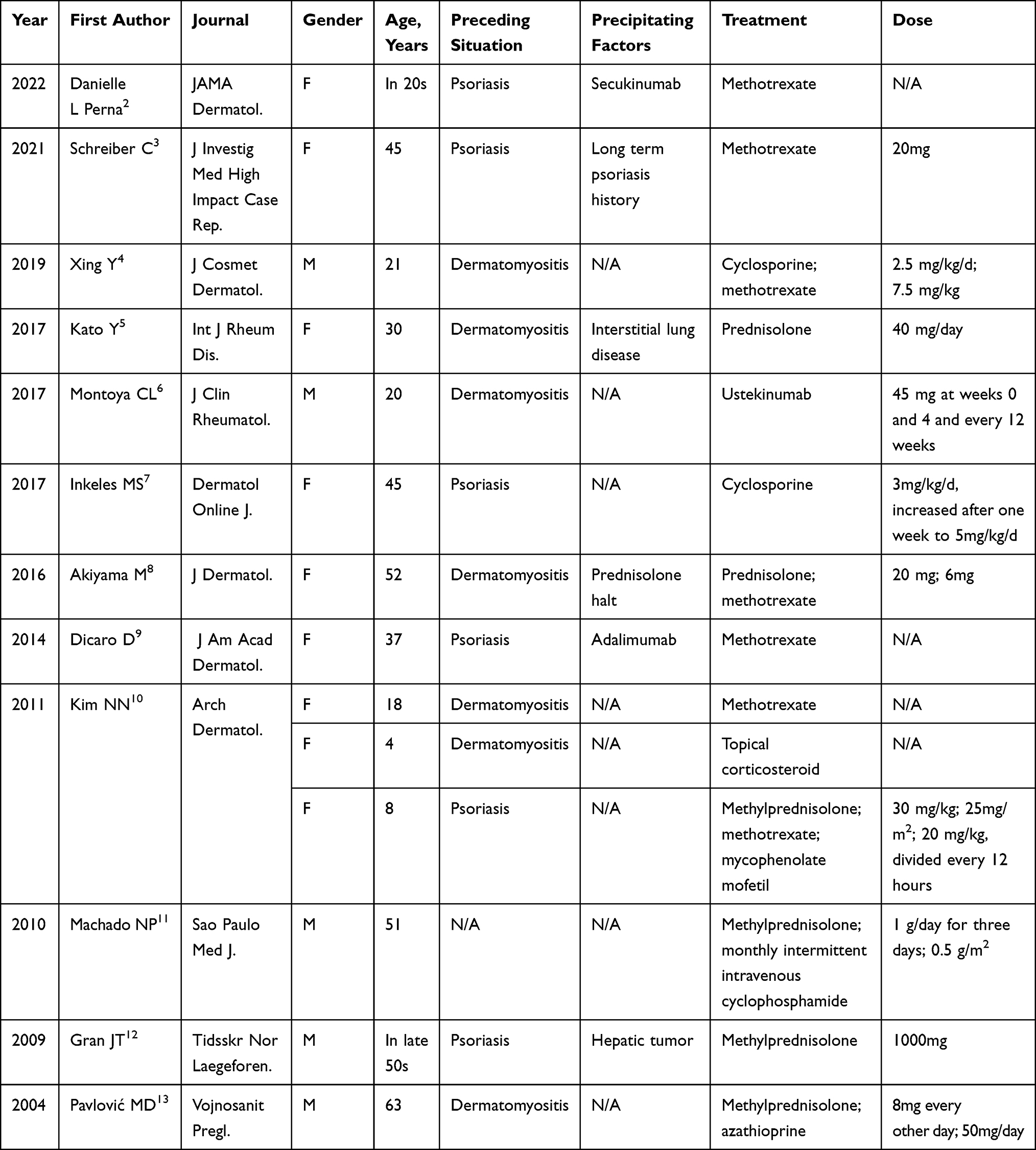 |
Table 1 Cases of Psoriasis Concurrent with Dermatomyositis |
Among the available treatments for psoriasis concurrent with dermatomyositis, methotrexate has shown promise and was utilized in seven out of fourteen cases. However, the use of methotrexate to treat this condition carries certain risks, such as the potential for interstitial lung disease, which raises concerns that the treatment may trigger or exacerbate the interstitial lung disease associated with dermatomyositis. In some cases, corticosteroids were used in the treatment of psoriasis concurrent with dermatomyositis, despite their known potential to exacerbate psoriasis. Of the six cases in which corticosteroids were used, four were administered concomitantly with other immunosuppressants, including methotrexate, cyclosporin, mycophenolate mofetil, and azathioprine. However, the possibility of psoriasis exacerbation remained. Inkeles MS reported the effectiveness of cyclosporine monotherapy in the treatment of psoriasis concurrent with dermatomyositis, noting that its selection was based on its documented efficacy and safety in treating dermatomyositis, as well as its FDA-approved status for treating psoriasis. Nonetheless, limitations exist, such as the concern that during the SARS-CoV-2 pandemic, immunosuppressants like cyclosporine may increase the risk of infection. Furthermore, biologics such as ustekinumab, which target Interleukin(IL)-12/23p40 and are effective in treating psoriasis, have shown promise in treating psoriasis concurrent with dermatomyositis. However, there have been reports of secukinumab, an interleukin 17 antagonist, acting as a precipitating factor for psoriasis concurrent with dermatomyositis, which has led to caution in using biologics that target the IL23-IL17 pathway in the treatment of this condition.
Then, what could be a solution for this treatment dilemma of psoriasis concurrent with dermatomyositis? We thought the same pathogenetic pathway might give us a hint. Thus, we download the skin transcriptomic data of psoriasis14 (GSM5216154, GSM5216170, GSM5216195, GSM5216211, GSM5216226, GSM5216244, GSM5216272 as lesion samples and GSM5216067, GSM5216071, GSM5216086, GSM5216102, GSM5216106, GSM5216114, GSM5216118 as control samples) and dermatomyositis15 (GSM3671281, GSM3671282, GSM3671285, GSM3671287 as lesion samples and GSM3671288, SM3671289, GSM3671290, GSM3671291, GSM3671292 as control samples). We used R studio in the analyses of the downloaded psoriasis (DESeq2 and clusterProfiler package) and dermatomyositis data (limma and clusterProfiler package). We found type II interferon-mediated signaling pathway (GO: 0060333) was enriched in both psoriasis (P = 0.003144649) and dermatomyositis (P = 1.37E-07).
Based on our data above, the medication targeting type II interferon-mediated signaling pathway could be a potential solution for the psoriasis concurrent with dermatomyositis dilemma. Type II interferon-mediated signaling pathway is controlled by Janus Kinase (JAK) 1 and JAK2 which several JAK inhibitors targeting this pathway including tofacitinib,16 ruxolitinib,17 baricitinib,16 abrocitinib18 and etc. There were several JAK inhibitors proved effective in the treatment of dermatomyositis. Meanwhile, these JAK inhibitors were also used in the treatment of psoriasis. These facts made JAK inhibitors eligible for the treatment of psoriasis concurrent with dermatomyositis. As mentioned above, in the SARS-CoV-2 era whether a treatment might aggravate SARS-CoV-2 should be taken into consideration. Baricitinib, one of the JAK inhibitors was approved by FDA for the treatment of adult patients hospitalized with COVID-19. While another JAK inhibitor, tofacitinib were also appeared to benefit attenuating SARS-CoV-2 infection. Thus, based on the psoriasis and dermatomyositis transcriptomic data as well as the lines above, we believe that JAK inhibitors could be the potential therapeutic strategy for the dilemma of psoriasis concurrent with dermatomyositis in the SARS-CoV-2 era.
Funding
National Natural Science Foundation of China 82202018.
Disclosure
The authors have declared that no conflict of interest exists. None of the authors has any financial interest in any products, devices or drugs used in the manuscript. There is also no conflict of interest related to any commercial associations or financial relationships.
References
1. Hornung T, Ko A, Tüting T, Bieber T, Wenzel J. Efficacy of low-dose methotrexate in the treatment of dermatomyositis skin lesions. Clin Exp Dermatol. 2012;37(2):139–142. doi:10.1111/j.1365-2230.2011.04188.x
2. Perna DL, Callen JP, Schadt CR. Association of treatment with secukinumab with exacerbation of dermatomyositis in a patient with psoriasis. JAMA Dermatol. 2022;158(4):454–456. doi:10.1001/jamadermatol.2021.6011
3. Schreiber C, Khamlong M, Raza N, Huynh BQ. Overlap of psoriatic arthritis and dermatomyositis. J Investig Med High Impact Case Rep. 2021;9:23247096211057702. doi:10.1177/23247096211057702
4. Xing Y, Xie J, Jiang S, Upasana M, Song J. Co-existence of Juvenile dermatomyositis and psoriasis vulgaris with fungal infection: a case report and literature review. J Cosmet Dermatol. 2019;18(5):1560–1563. doi:10.1111/jocd.12869
5. Kato Y, Yamamoto T. Development of psoriasis with relapse of dermatomyositis-associated interstitial lung disease. Int J Rheum Dis. 2017;20(5):660–661. doi:10.1111/1756-185X.13084
6. Montoya CL, Gonzalez ML, Ospina FE, et al. Case of amyopathic juvenile dermatomyositis associated with psoriasis successfully treated with ustekinumab. J Clin Rheumatol. 2017;23(2):129–130. doi:10.1097/RHU.0000000000000430
7. Inkeles MS, No D, Wu JJ. Clinical improvement of a patient with both amyopathic dermatomyositis and psoriasis following treatment with cyclosporine. Dermatol Online J. 2017;23(8). doi:10.5070/D3238036019
8. Akiyama M, Ueno T, Kanzaki A, Kuwana M, Nagao M, Saeki H. Association of psoriasis with Hashimoto’s thyroiditis, Sjögren’s syndrome and dermatomyositis. J Dermatol. 2016;43(6):711–712. doi:10.1111/1346-8138.13265
9. Dicaro D, Bowen C, Dalton SR. Dermatomyositis associated with anti-tumor necrosis factor therapy in a patient with psoriasis. J Am Acad Dermatol. 2014;70(3):e64–5. doi:10.1016/j.jaad.2013.11.012
10. Kim HJ, Choi EW, Choi EJ, et al. Non-thermal plasma promotes hair growth by improving the inter-follicular macroenvironment. RSC Adv. 2021;11(45):27880–27896.
11. Machado NP, Camargo CZ, Oliveira AC, Buosi AL, Pucinelli ML, Souza AW. Association of anti-glomerular basement membrane antibody disease with dermatomyositis and psoriasis: case report. Sao Paulo Med J. 2010;128(5):306–308. doi:10.1590/S1516-31802010000500012
12. Gran JT, Gunnarsson R, Mørk NJ. En mann med erytrodermi, muskelsvakhet og vekttap [A man with erythrodermia, muscle weakness and weight loss]. Tidsskr nor Laegeforen. 2009;129(21):2240–2241. Norwegian. doi:10.4045/tidsskr.09.0184
13. Pavlović MD, Zecević RD, Zolotarevski L. Psoriasis in a patient with dermatomyositis. Vojnosanit Pregl. 2004;61(5):557–559. doi:10.2298/VSP0405557P
14. Liu J, Chang HW, Grewal R, et al. Transcriptomic profiling of plaque psoriasis and cutaneous T-cell subsets during treatment with secukinumab. JID Innovations. 2022;2(3):100094. doi:10.1016/j.xjidi.2021.100094
15. Cassius C, Amode R, Delord M, et al. MDA5(+) dermatomyositis is associated with stronger skin type I interferon transcriptomic signature with upregulation of IFN-κ transcript. J Invest Dermatol. 2020;140(6):1276–1279.e7. doi:10.1016/j.jid.2019.10.020
16. Dillon KL. A comprehensive literature review of JAK inhibitors in treatment of alopecia areata. Clin Cosmet Investig Dermatol. 2021;14:691–714. doi:10.2147/CCID.S309215
17. Appeldoorn TYJ, Munnink THO, Morsink LM, Hooge MNL, Touw DJ. Pharmacokinetics and pharmacodynamics of ruxolitinib: a review. Clin Pharmacokinet. 2023;62:559–571. doi:10.1007/s40262-023-01225-7
18. Fougerousse AC, Jacobzone C, Mery-Bossard L, et al. Use of systemic medications for treating adult atopic dermatitis in France: results of a practice survey. Clin Cosmet Investig Dermatol. 2021;14:179–183. doi:10.2147/CCID.S300402
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.