Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Isolated Palmoplantar Lentiginosis
Authors Alghubaywi F ![]() , AlJasser MI
, AlJasser MI ![]() , Alfadhel M
, Alfadhel M ![]() , Almohanna HM
, Almohanna HM
Received 4 April 2023
Accepted for publication 21 June 2023
Published 27 June 2023 Volume 2023:16 Pages 1653—1657
DOI https://doi.org/10.2147/CCID.S415686
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Faisal Alghubaywi,1,2 Mohammed I AlJasser,1– 3 Majid Alfadhel,1,3,4 Hind M Almohanna5
1College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 2Division of Dermatology, King Abdulaziz Medical City, Ministry of National Guard Health Affairs, Riyadh, Saudi Arabia; 3King Abdullah International Medical Research Center, Riyadh, Saudi Arabia; 4Genetics and Precision Medicine Department, King Abdullah Specialized Children Hospital, Riyadh, Saudi Arabia; 5Department of Dermatology and Dermatologic Surgery, Prince Sultan Military Medical City, Riyadh, Saudi Arabia
Correspondence: Faisal Alghubaywi, Division of Dermatology, King Abdulaziz Medical City, Ministry of National Guard Health Affairs, P.O. Box 3660, Riyadh, 11481, Saudi Arabia, Tel +966-11-801 1111 ext. 15626, Fax +966-11-801 1111 Ext. 80-14229, Email [email protected]
Abstract: The distribution of lentigines offers great insight into the multitude of potential-associated genetic or acquired conditions. In this report, we described a unique presentation of lentigines limited to the palms and soles in a healthy individual. Personal and familial history, clinical examination, serological testing, and whole-genome sequencing were all unremarkable. The benign clinical features and absence of associated medical conditions support the likely lentigo simplex with an isolated palmoplantar distribution. To date, no similar distribution has been reported. This case extends the breadth of view into all possible presentations of lentigines.
Keywords: lentiginosis, palmoplantar, isolated, case report
Introduction
Lentigines are small, well-circumscribed, hyperpigmented macules that can present anywhere on the skin and/or mucous membranes.1 They can develop slowly over the years or they may erupt in a sudden manner.1 Their appearance is owed to an increase in the number or activity of epidermal melanocytes.1 Lentigines are typically a clinical diagnosis, while dermoscopy and histologic examinations are reserved for equivocal cases.1 They can be a separate entity (ie, lentigo simplex) or a feature of an associated disorder.1 Acral distribution of lentigines can be associated with several genetic or acquired conditions with or without systemic abnormalities.2 Patients with acral lentigines usually have involvement of other body sites (such as lip lentigines in Peutz-Jeghers syndrome or Laugier-Hunziker syndromes).3,4 This report describes a distinct case of lentigines predominately on the palms and soles with no involvement of other body sites. The presentation did not match any other reported cases of palmoplantar lentiginosis.
Case Report
A 35-year-old middle eastern female presented for evaluation of hyperpigmented lesions over her palms and soles. The lesions appeared unprovoked at the age of 16 years. Over time, they increased in number but remained confined to the palms and soles. No associated symptoms, aggravating or relieving factors were noted. The past drug, medical, family, and social history were unremarkable. On examination, she had numerous, sharply demarcated, round-to-oval, 1–5 mm macules with different shades of brown, affecting mainly the palmoplantar surface with some extension to the periungual areas (Figure 1). Dermoscopic examination showed a parallel furrow and lattice-like pattern (Figure 2). Mucous membranes, hair, and nails were spared. The remainder of the physical examination revealed no neurological, cardiac, or gastrointestinal (GI) abnormalities. Laboratory work-up including serum complete blood count with differentials, liver function test, renal function test, cortisol, adrenocorticotropic hormone, vitamin B12, thyroid stimulating hormone, anti-nuclear antibody, lactate dehydrogenase hormone, and immunoglobulins were all normal. Whole-genome sequencing was performed but was negative. The patient was reassured and was offered a trial of laser therapy.
 |
Figure 1 Clinical images showing numerous macules with different shades of brown affecting mainly the palmoplantar surfaces with some extension to the periungual areas. |
 |
Figure 2 Polarized dermoscopic images showing a parallel furrow and lattice-like pattern. |
Discussion
Lentigines can be seen in association with a wide range of conditions. The diagnosis of the associated condition usually depends on the overall combination of cutaneous, systemic, and investigative findings. Table 1 summarizes a selected group of conditions that present with acral pigmentation and compares them to the findings in our patient. The findings in our patient did not match any of the previously described conditions with acral pigmentation as they typically present with the involvement of other body parts and/or associated non-dermatological findings. Peutz-Jeghers syndrome (PJS) is an autosomal dominant disorder presenting with the external hallmark of macular pigmentation on the lips (94%), palms (74%), buccal mucosa (66%), and soles (62%).3 The macules typically appear in the first year of life, increase in size and number over time, then eventually fade away after puberty. The internal cardinal finding in PJS is diffused hamartomatous GI polyposis, which becomes symptomatic and potentially malignant for most patients by the age of 30 years. Laugier-Hunziker syndrome (LHS) is a sporadic condition that is thought to have no systemic involvement.4 The clinical feature of LHS is lenticular mucocutaneous macules that distinctively affect the lip and oral cavity but can be seen in the palmoplantar region. Associated with dotted macular melanosis of the fingertips and longitudinal melanonychia in 50–60% of the patients but without nail dystrophy.4,5
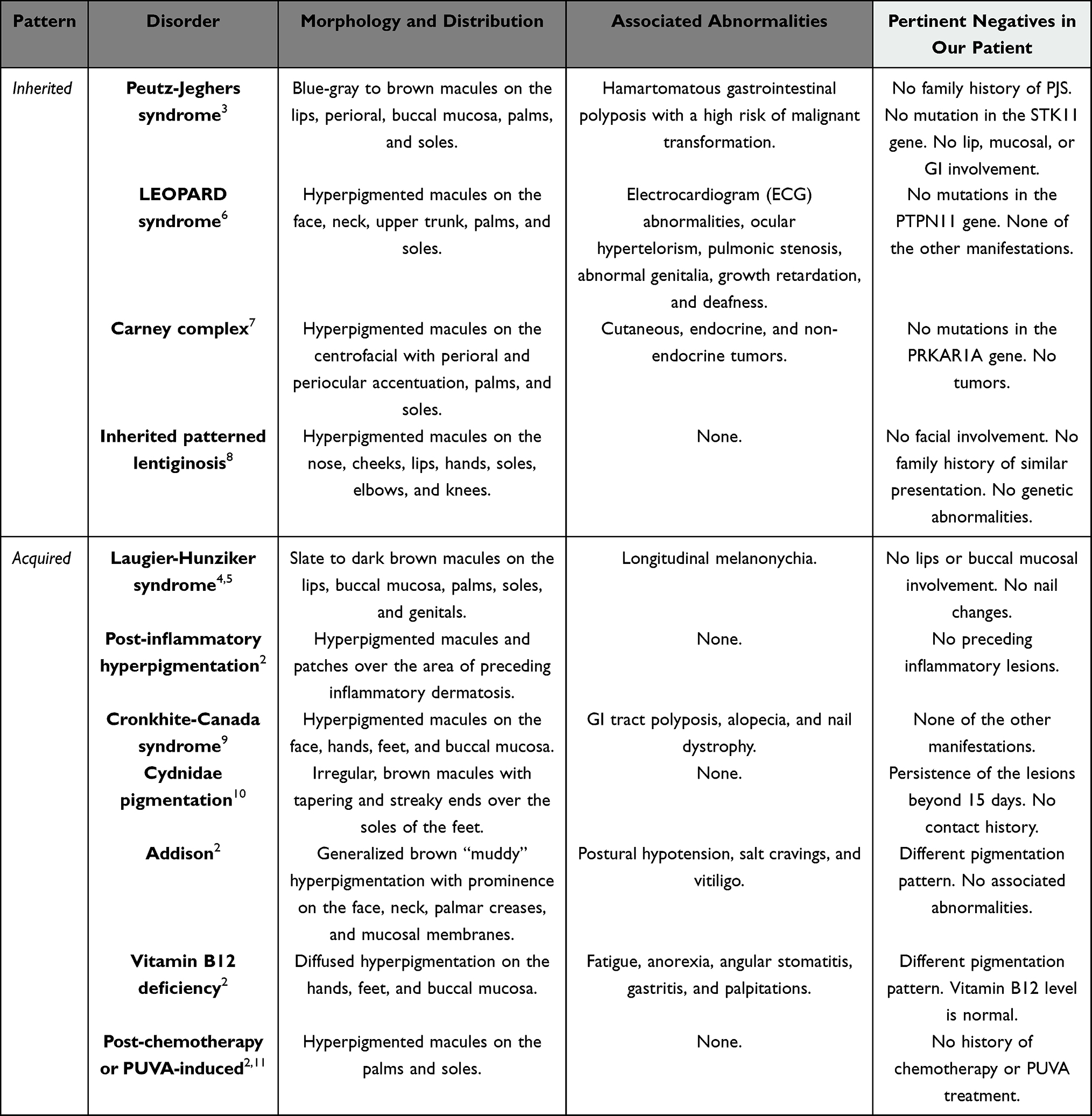 |
Table 1 Features of Selected Disorders Associated with Acral Pigmentation |
LEOPARD syndrome (multiple lentiginosis, ECG conduction irregularities, ocular hypertelorism, pulmonic stenosis, abnormal genitalia, retardation of growth, and deafness) is a rare autosomal dominant disorder.6 The pathognomonic presence of multiple lentigines is typically found on the face, neck, and upper trunk but can be seen anywhere, including the palmoplantar. The diagnosis requires the presence of multiple lentigines and two other prominent features. Carney complex is an autosomal dominant disease with major features such as mucocutaneous lentigines, cardiac and noncardiac myxomatous tumors, and endocrine neoplasia.7 The lentigines can be located anywhere, but a rather classic distribution is observed over the face, lips, genitals, and mucosal membranes. Other common cutaneous findings include epithelioid blue nevus and myxomas, usually on the eyelids, external ear canal, breast, and genitals. The diagnosis is established if two major features are present. O’Neill et al described 10 cases of inherited patterned lentiginosis in black patients.8 All had centrofacial and lip distribution but sparing the oral mucosa. Six of the patients had palmoplantar involvement as well as the dorsum. Similar to our patient, 5 of the 6 were healthy, one had hypertension, and all were Fitzpatrick skin phototype IV. Even so, our patient’s lentigines are limited to the palms and soles, while theirs were predominantly on the face.
Cronkhite-Canada syndrome (CCS) is a rare, nonhereditary disorder that affects individuals in their sixth decade with a male-to-female ratio of 3:2.9 Two-thirds of the patients (75%) are Japanese. CCS manifests with diffused GI polyposis, nail dystrophy (described in 98% of the patients), non-scarring alopecia, and macular hyperpigmentation, mainly on the face, neck, palms, and soles. Cydnidae pigmentation occurs after direct contact with the fluids secreted from an insect known as Cydnidae (burrowing bug).10 The rural-residing insect causes irregular, brown macules with tapering and streak-like ends to erupt over the soles of the feet with quick resolution of the lesions (10–15 days). Post-inflammatory hyperpigmentation (eg, lichen planus) can present as violaceous, macular, or papular melanotic lesions over the palms and soles.2 Acquired causes of lentiginosis are relatively easier to detect and may potentially be reversible. In our patient, the past medical and drug history are unremarkable. The laboratory results regarding a variety of endocrine and nutritional deficiencies, such as vitamin B12 deficiency, and Addison disease are normal. In addition, post-chemotherapy or PUVA-induced hyperpigmentation is less likely since both conditions are lacking in our case.2,11 Our patient’s benign clinical features and absence of associated medical conditions support the likely lentigo simplex with an isolated palmoplantar distribution. This report is limited by the short follow-up duration since the first clinic visit was 1-year ago.
The distribution of lentigines can help delineate the multitude of underlying etiologies. In this report, we described a unique presentation of lentigines limited to the palms and soles in a healthy individual without associated findings. The case will add to the understanding of all the possible clinical appearances of lentigines. Physicians should be aware of this atypical distribution after carefully evaluating associated medical conditions.
Abbreviation
GI, gastrointestinal; PJS, Peutz-Jeghers syndrome; LHS, Laugier-Hunziker syndrome; CCS, Cronkhite-Canada syndrome.
Ethical Statement
No institutional approval is required for case reports and the patient cannot be identified from the images.
Informed Consent Statement
Patient consented in writing for the publication of her case/photographs both online and in-print and understood that it will be publicly available and was sent a copy of the article to read.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ber Rahman S, Bhawan J. Lentigo. Int J Dermatol. 1996;35(4):229–239. PMID: 8786179. doi:10.1111/j.1365-4362.1996.tb02994.x
2. Bhalla M, Garg S. Acral melanosis. Pigment Int. 2018;5(1):14–27. doi:10.4103/Pigmentinternational.Pigmentinternational_15_17
3. Utsunomiya J, Gocho H, Miyanaga T, Hamaguchi E, Kashimure A. Peutz-Jeghers syndrome: its natural course and management. Johns Hopkins Med J. 1975;136(2):71–82. PMID: 1117595.
4. Lampe AK, Hampton PJ, Woodford-Richens K, Tomlinson I, Lawrence CM, Douglas FS. Laugier-Hunziker syndrome: an important differential diagnosis for Peutz-Jeghers syndrome. J Med Genet. 2003;40(6):e77. PMID: 12807976; PMCID: PMC1735508. doi:10.1136/jmg.40.6.e77
5. Nayak RS, Kotrashetti VS, Hosmani JV. Laugier-Hunziker syndrome. J Oral Maxillofac Pathol. 2012;16(2):245–250. PMID: 22923898; PMCID: PMC3424942. doi:10.4103/0973-029X.99079
6. Sarkozy A, Digilio MC, Dallapiccola B. Leopard syndrome. Orphanet J Rare Dis. 2008;3(13). doi:10.1186/1750-1172-3-13
7. Correa R, Salpea P, Stratakis CA. Carney complex: an update. Eur J Endocrinol. 2015;173(4):M85–M97. PMID: 26130139; PMCID: PMC4553126. doi:10.1530/EJE-15-0209
8. O’Neill JF, James WD. Inherited patterned lentiginosis in blacks. Arch Dermatol. 1989;125(9):1231–1235. doi:10.1001/archderm.1989.01670210069009
9. Shah KR, Boland CR, Patel M, Thrash B, Menter A. Cutaneous manifestations of gastrointestinal disease: part I. J Am Acad Dermatol. 2013;68(2):189.e1–21; quiz 210. PMID: 23317980. doi:10.1016/j.jaad.2012.10.037
10. Poojary S, Baddireddy K. Demystifying the stinking reddish brown stains through the dermoscope: cydnidae pigmentation. Indian Dermatol Online J. 2019;10(6):757–758. doi:10.4103/idoj.IDOJ_346_18
11. Stewart CJ, Hawkins CN. Eruptive acral nevi secondary to treatment with chemotherapy. JAMA Dermatol. 2023. doi:10.1001/jamadermatol.2022.6543
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.