Back to Journals » Clinical Interventions in Aging » Volume 19
Is There an Association Between Inflammation and Serum-Vitamin D? – Results of a Retrospective Analysis of Hospitalized Geriatric Patients
Authors Funk L, Trampisch US ![]() , Pourhassan M, Wirth R
, Pourhassan M, Wirth R ![]()
Received 1 November 2023
Accepted for publication 9 April 2024
Published 9 May 2024 Volume 2024:19 Pages 763—768
DOI https://doi.org/10.2147/CIA.S447678
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Lukas Funk, Ulrike Sonja Trampisch, Maryam Pourhassan, Rainer Wirth
Department of Geriatric Medicine, Marien Hospital Herne, Herne, Germany
Correspondence: Lukas Funk Marien Hospital Herne, Universitätsklinikum der Ruhr-Universität Bochum, Herne, Hölkeskampring, 4044629, Deutschland, Tel +49 (0) 2323 499 5822, Email [email protected]
Purpose: Vitamin D deficiency is a common finding in geriatric patients. The ESPEN micronutrient guideline states that vitamin D serum levels significantly decrease in the presence of inflammation and should be interpreted with caution. This is of great interest for hospital care and would imply a significant change to the current approach to hospitalized patients with suspected vitamin D deficiency.
Patients and methods: To evaluate the association of vitamin D and inflammation, we reanalyzed the data set of serum 25(OH)D-Levels of 687 consecutive geriatric hospitalized patients of a previously published study.
Results: We found that vitamin D deficiency (< 20 ng/dl) was prevalent in 78.0% and vitamin D insufficiency (20– 30 ng/dl) in 9.9% of patients. Sperman’s correlation showed a significant but very weak correlation (R = − 0.100, P < 0.01) of serum vitamin D and C-reactive protein. However, linear regression with the inclusion of age and gender revealed no significant association (beta-coefficient − 0.070; p=0.067).
Conclusion: In this study, we could not confirm a significant and clinically relevant association between serum vitamin D levels and inflammation, contrasting with a previous study. However, longitudinal studies need to be performed to draw a final conclusion.
Keywords: Vitamin D, 25-hydroxyvitamin D, inflammation, older, C-reactive protein, geriatric
Introduction
We read with great interest the ESPEN micronutrient guideline, which is an important contribution to nutritional medicine.1 However, in the chapter on vitamin D, the authors reported a significant drop in serum-vitamin D levels in the context of inflammation. They report that in the presence of C-reactive protein (CRP) >4 mg/dl, nearly all values are below the reference range, which may complicate the interpretation of such measurements. The authors based this statement on the study of Duncan et al from 2012.2 In this study, the authors examined the correlation between serum CRP and serum vitamin D, utilizing a cross-sectional methodology applied to 5154 blood samples drawn from a cohort of 3676 patients. Furthermore, the exploration extended to assess the interactions with other micronutrients. The authors observe a pronounced reduction in serum vitamin D levels, quantified at 41%, if serum CRP concentrations exceeded 8 mg/dl. Considering the routine assessment of serum vitamin D levels in geriatric patients with acute illnesses, we have questioned the validity of these measurements as an accurate reflection of vitamin D stores. The question then arises as to whether we need to modify our method by adjusting these measures for the degree of inflammation or restrict vitamin D testing to periods devoid of inflammation.
However, the study by Duncan et al is the only large study investigating this association, and using a cross-sectional approach cannot prove causality. CRP is an acute-phase protein and is used as one of the main laboratory markers for inflammation. It is very sensitive to inflammation, increasing within hours of new-onset inflammation and reaching its peak after 48 hours. Thereby, it is lacking specificity regarding the type of inflammation, as infection, trauma, and surgery or rheumatic diseases will all lead to an increase in CRP levels.
Vitamin D is almost completely synthesized by the body and only small amounts are supplied through food. 25-hydroxyvitamin D [25(OH)D] or calcidiol is synthesized in the liver from the precursor steroid cholecalciferol and is then converted in the kidneys to the biologically active form, the steroid hormone calcitriol. Measuring 25(OH)D concentrations in the serum is used to determine the total body stores of vitamin D. Though the limit values of 25(OH)D from which insufficiency or deficiency of vitamin D should be defined are still under discussion, there is agreement that vitamin D deficiency is common in older persons3,4 and is associated with several negative consequences5 eg, bone loss, falls and fractures.6 However, the effect on the immune system is debated.7 The prevalence of vitamin D deficiency varies widely depending on the criteria, location of the survey (natural sun exposure), and the cohort that is studied (eg, older patients hospitalized or institutionalized patients, etc.).
Retrospective data analysis by our working group8 with 679 geriatric hospitalized patients, was able to show that 78.0% of participants demonstrated a vitamin D deficiency, defined as a vitamin D serum concentration <20 ng/mL.
Given the particular characteristics of an acute care geriatric hospital department, a significant proportion of patients are in the midst of or have recently undergone an acute-phase reaction, exhibiting inflammation and correspondingly elevated CRP levels.
If indeed inflammation plays a substantial role in reducing vitamin D levels, it would compel us, along with others in the field, to rethink our diagnostic approach. Hence, in pursuit of clarity, we reassessed our data, exploring the interrelationship between CRP and vitamin D levels with the aim of confirming the findings of Duncan et al.
Methods
Participants
In this study, we performed a retrospective analysis of the dataset from Pourhassan et al (8), who originally also retrospectively examined the 25(OH)D concentration of 679 patients regarding a possible seasonal variation in 25(OH)D levels in frail older hospitalized patients.
The patients in that previous study were consecutively hospitalized to a geriatric acute care ward at Marien Hospital, Herne, Germany, and the study protocol had been approved by the ethical committee of Ruhr-University Bochum (No. 16–6001). Of that original cohort all patients with available CRP and 25(OH)D levels from the same day were included in our analysis, encompassing the original cohort. As our focus was solely on analyzing vitamin D and CRP levels, the need for exclusions was reduced compared to the previous study. Consequently, this accounts for the slightly larger cohort of 687 patients observed in this secondary analysis. As in the original paper, we also investigated subgroups of patients who were not on vitamin D supplementation, those who were on supplementation and those for whom this information was not available.
Serum vitamin 25(OH)D concentrations and CRP levels
The measurement of vitamin 25(OH)D levels was conducted using an electro-chemiluminescence immunoassay (ECLIA) on the Cobas 8000 (e602) analyzer, manufactured by Roche in Mannheim, Germany. In contrast, CRP measurements, which were not addressed in the original study, were performed using the Cobas Pro (c503)/Cobas Pure (C303) analyzer, also developed by Roche in Mannheim, Germany. The local laboratory is certified according to DIN ISO 9001 and internal and external (ring tests) QC checks are three monthly done according to the guidelines of the German Medical Association.
For statistical analysis, Vitamin D Levels <3 ng/mL (lower limit of the laboratory test) were set at a level of 2.9 mg/dl, which explains the gap in the statistical analysis and on the x-axis of the correlation graph (Figure 1).
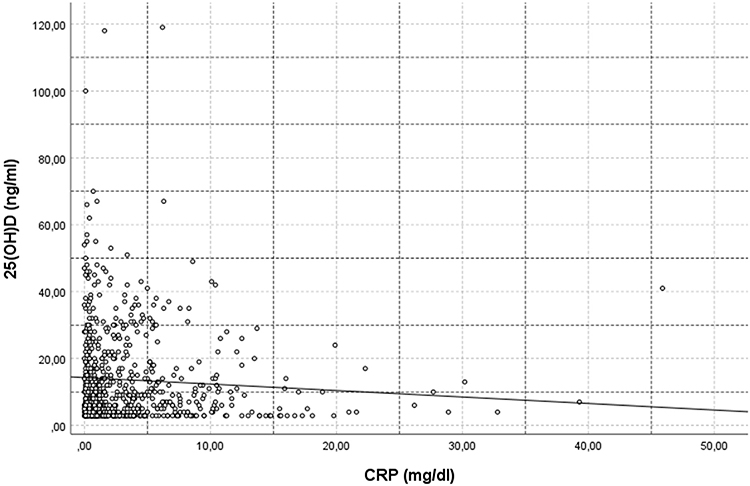 |
Figure 1 Scatter plot showing the relationship of 25(OH)D and CRP. |
Data analysis
The statistical analysis was performed with SPSS statistical software (SPSS Statistics for Windows, IBM Corp, Version 27.0, Armonk, NY, USA). Continuous variables are reported by their means (age and CRP) and standard deviations (SDs) for normally distributed variables, 25(OH)D-levels, which were not normally distributed were also expressed as P50 (P25 – P75). Categorical variables are expressed as absolute numbers and relative frequencies (%). The correlation of 25(OH)D levels compared with CRP was expressed as the Spearman correlation coefficient for the entire cohort and for the three subgroups.
An analysis of variance (ANOVA) was performed to assess for differences in age and CRP levels between 25(OH)D deficient patients and those with insufficient (defined as a 25(OH)D concentration below 20 ng/mL), insufficient (25(OH)D concentration between 20 and 30 ng/mL), and normal 25(OH)D levels. A stepwise binary logistic regression model was performed to assess the simultaneous effects of age and gender on serum 25(OH)D deficiency. A P-value of <0.05 was considered as the limit of significance.
Results
The study group comprised 687 participants, predominantly females (67.3%), with a mean age of 82.1 ± 8.2 (age range between 61 and 99 years). Of the 687 participants 504 were on no previous vitamin D supplementation, 118 were on some kind of vitamin D supplementation and for 118 participants the supplementation status was not known. The mean 25(OH)D serum level was 12.4 ng/mL (range, 0–70 ng/mL), the median value was 8 ng/mL (IQR 4–17). The proportion of vitamin D deficiency was 77.6%, 9.9%, and 12.5%, respectively. The mean CRP-Level was 3.6 mg/dl (range 0.0–45.9 mg/dl).
The baseline characteristics of study participants stratified by different serum vitamin 25(OH)D concentrations are shown in Table 1.
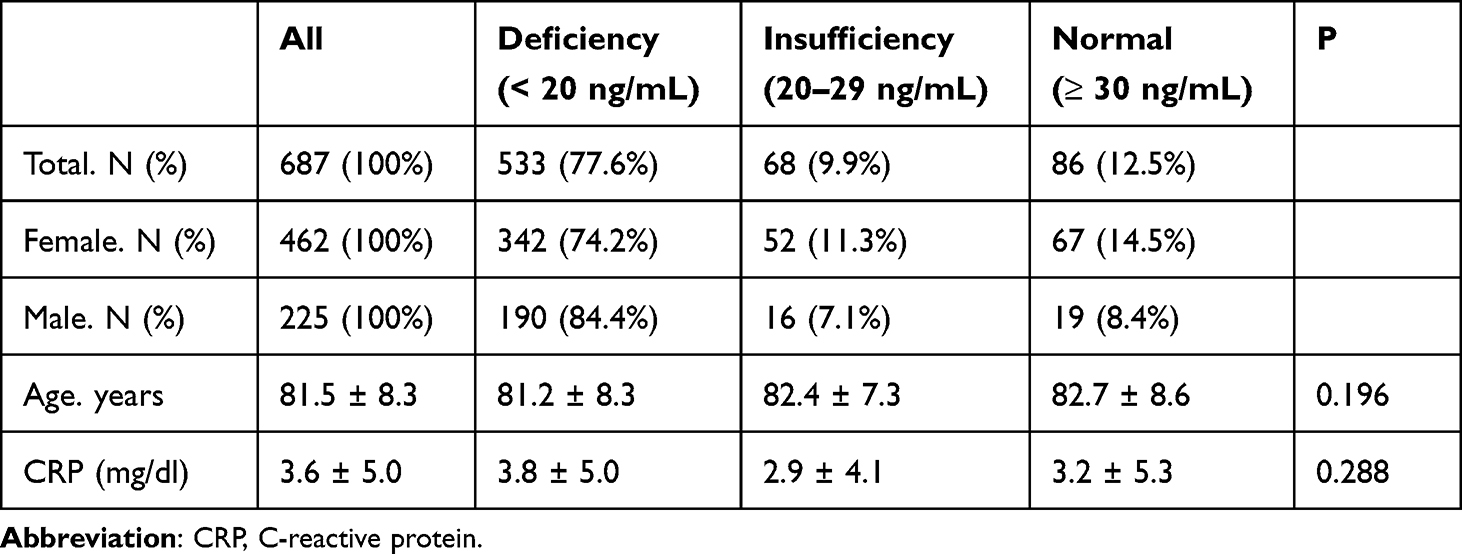 |
Table 1 Characteristics of Study Participants Stratified According to Different Serum 25(OH)D Levels |
As for the ESPEN micronutrient guideline mention, that in the presence of a CRP >4.0 mg/dl, nearly all values of vitamin D are below the reference ranges, we did a comparison of these two groups. In the 194 participants with a CRP of >4.0 mg/dl, mean vitamin D levels were 12.9 ng/mL with a median of 8 ng/mL, while in the 493 participants with a CRP of 0 to 4 mg/dl, the mean vitamin D levels were 13.9 ng/mL with a median of 9 ng/mL.
The correlation analysis for the entire cohort showed a significant but weak correlation (Spearman-Rho (R) = −0.100, Sig. (2-tailed) = 0.009) between CRP levels and vitamin D levels. In the subgroup analysis, the correlation could only be seen in the group without previous vitamin D supplementation (N = 504, Spearman-Rho (R) = −0.133, Sig. (2-tailed) = 0.003), not in patients on supplementation (N = 118, Spearman-Rho (R) = −0.099, Sig. (2-tailed) = 0.295) or when previous supplementation was unknown (N = 65, Spearman-Rho (R) = −0.081, Sig. (2-tailed) = 0.538).
Figure 1 presents the scatter plot analysis showing the relationship between 25(OH)D and CRP.
Adjusting for age and gender, an additional logistic regression analysis, as presented in Table 2, revealed no significant association between Vitamin D and CRP, age, or gender.
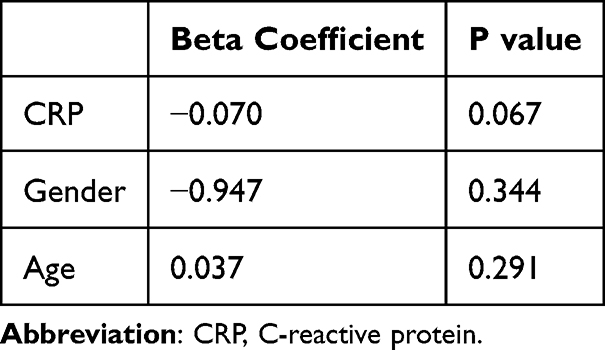 |
Table 2 Linear Regression Analysis of Factors Associated with Serum 25(OH)D Deficiency |
Discussion
To the best of our knowledge, there are currently only a few studies that have examined vitamin D concentration in the context of acute inflammation.9,10 Both studies reported a significant decrease in 25(OH)D levels after surgery. Other studies reported no significant decrease in acute inflammation in malaria infection11 or myocardial infarction.12 However, due to the nature of these conditions, the first 25(OH)D-levels in these studies were measured after the inflammatory insults. As reported by Waldron et al9 after inflammatory insult vitamin D levels decrease rapidly and persist to be low for weeks to months before increasing again while CRP will normalize within days. Therefore, measurement of 25(OH)D and CRP days to a few weeks after an inflammatory stimulus as is regularly the case in geriatric rehabilitation will tend to find patients with already normalized CRP but still decreased 25(OH)D.
Young et al13 retrospectively analyzed the data of 9880 preschool children and 14,749 nonpregnant females from nutrition surveys and correlated inflammation biomarkers with 25(OH)D concentration without finding a significant association.
All these findings support our current practice of not adjusting for inflammation biomarkers when interpreting 25(OH)D levels in hospitalized older patients.
In our current study, involving a retrospective analysis of nearly 700 older patients admitted to a geriatric ward, we found no significant correlation between vitamin D levels and the degree of inflammation, as indicated by CRP levels using linear regression analysis. And though we observed a significant correlation, using the Spearman Correlation analysis, Spearman’s rho showed only a negligible to weak correlation (r = −0.100). The subgroup analysis showed that correlation could only be seen in patients without previous vitamin D supplementation, but not in patients on supplementation or in the group of patients where previous supplementation status was unknown.
These findings are similar to those reported by Duncan et al (r = −0.16, P < 0.01), which led to the recommendation in the ESPEN micronutrient guideline cautioning the interpretation of vitamin D levels in the presence of inflammation.
In both analyses, the one Duncan et al did and the one we did in our study the correlation coefficients show only a very weak correlation. As the correlation coefficient (r) has no obvious interpretation, r² or the “coefficient of determination” is sometimes reported. The “coefficients of determination” are 0.026 (Duncan et al) and 0.01 (our study), suggesting that only about 1 to 3% of a decrease in 25(OH)D levels can be “explained” by an increase in CRP levels. This states the question if that is of sufficient clinical significance to warrant a recommendation of caution when interpreting vitamin D levels in inflammation which could possibly lead to doctors not starting to supplement people with insufficiency or deficiency in case of an elevated CRP.
As for the cohorts, some significant differences need to be addressed. In our study, the mean age of our cohort was 82 years, representing a substantially older population compared to the cohort examined by Duncan et al (mean age of 49 years). While specific details about the Duncan cohort are not provided, it is worth noting that our study group comprises older frail patients requiring inpatient treatment or early rehabilitation, reflecting an acute care setting. Older, multimorbid, and notably frail patients are often underrepresented in large-scale studies,14 despite having the highest prevalence of vitamin D deficiency and related secondary diseases.3 Our study highlights the limited generalizability of results obtained from specific cohorts to other populations. There are several potential reasons for these different findings, including variations in study design and differences among the cohorts under investigation. Also there was no information regarding the vitamin D supplementation status in the study by Duncan et al.
Patient-specific factors may also contribute significantly to the differences observed in study results. Older patients exhibit heightened levels of inflammation markers. In our cohort of frail and elderly inpatients, the presence of chronic inflammation, stemming from multimorbidity such as chronic kidney disease, heart failure, COPD, rheumatic diseases, chronic infections, chronic wounds, and others, could have influenced the observed correlation and potentially contributed to chronically elevated CRP levels.15
Additionally, it is known that the immune system itself is subject to changes with age (immunosenescence). For example, it is shown that the inflammation-associated increase in CRP is reduced in the older population.16 Suppose there was a decrease in 25(OH)D levels in inflammation there might be a less pronounced increase in CRP accompanying this change. Or similar to the smaller increase in the CRP concentration, there may be a less pronounced decrease of the 25(OH)D in the context of acute inflammation in an older age compared to the changes expected at a younger age. Conversely, in cohorts with chronic diseases, such as COPD it may also be the fact that disease severity and inflammation lead to less mobility and sun exposure and therefore a decrease in vitamin D.17 Finally, it may also be possible that a drop in the 25(OH)D levels caused by inflammation is less pronounced in pre-existing vitamin D insufficiency or deficiency which are both more often found in older subjects.
This study has some limitations though. First, the study was performed in a group of older hospitalized patients with a high probability of frailty and a high burden of acute and chronic illnesses and can therefore not be generalized. Second, our data analysis is a retrospective and not a prospective cohort analysis. Based on the available data, only limited information was available about previous vitamin D therapy, total burden of illnesses and therefore no clear conclusion could be drawn regarding recent inflammation eg, infections or surgery and chronic illnesses. As CRP is a fast-reacting acute-phase marker, its levels could in some patients have already been normalized while 25(OH)D could have still been suppressed. Other inflammatory markers (white blood count, procalcitonin or IL-6) were not available.
Conclusion
In this retrospective cross-sectional study analyzing 25(OH)D levels in 687 frail and elderly inpatients, we found no indication for a clinically relevant association of serum-vitamin D with serum-CRP as an inflammatory marker in older hospitalized patients. Longitudinal research is needed to elucidate a possible association and possible differences between different types of inflammation.
Ethical Standard
The authors declare that the study procedures comply with current ethical standards for research involving human participants in Germany. The study protocol had been approved by the ethical committee of Ruhr-University Bochum. Patient consent was waived due to the retrospective nature of this study, all data was anonymized and maintained with confidentially and all data accessed complied with relevant data protection and privacy regulations.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
We acknowledge support by the Open Access Publication Funds of the Ruhr-Universität Bochum.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Berger MM, Shenkin A, Schweinlin A, et al. ESPEN micronutrient guideline. Clin Nutr. 2022;41(6):1357–1424. doi:10.1016/j.clnu.2022.02.015
2. Duncan A. Quantitative data on the magnitude of the systemic inflammatory response and its effect on micronutrient status based on plasma measurements. Am J Clin Nutr. 2012;95(1):64–71.
3. Marcos-Perez D, Sánchez-Flores M, Proietti S, et al. Low Vitamin D Levels and Frailty Status in Older Adults: a Systematic Review and Meta-Analysis. Nutrients. 2020;12(8). doi:10.3390/nu12082286
4. Boettger SF. Prevalence and predictors of vitamin D-deficiency in frail older hospitalized patients. BMC Geriatr. 2018;18(1):219. doi:10.1186/s12877-018-0919-8
5. Hossein-nezhad A, Holick MF. Vitamin D for health: a global perspective. Mayo Clin Proc. 2013;88(7):720–755. doi:10.1016/j.mayocp.2013.05.011
6. Bischoff HA, Stähelin HB, Dick W, et al. Effects of vitamin D and calcium supplementation on falls: a randomized controlled trial. J Bone Miner Res. 2003;18(2):343–351. doi:10.1359/jbmr.2003.18.2.343
7. Martens PJ, Gysemans C, Verstuyf A, et al. Vitamin D’s effect on immune function. Nutrients. 2020;12(5). doi:10.3390/nu12051248
8. Pourhassan M, Wirth R. Seasonal variation in vitamin d status among frail older hospitalized patients. J Frailty Aging. 2018;7(2):95–99. doi:10.14283/jfa.2018.10
9. Waldron JL, Ashby HL, Cornes MP, et al. Vitamin D: a negative acute phase reactant. J Clin Pathol. 2013;66(7):620–622. doi:10.1136/jclinpath-2012-201301
10. Reid D, Toole BJ, Knox S, et al. The relation between acute changes in the systemic inflammatory response and plasma 25-hydroxyvitamin D concentrations after elective knee arthroplasty. Am J Clin Nutr. 2011;93(5):1006–1011. doi:10.3945/ajcn.110.008490
11. Newens K, Filteau S, Tomkins A. Plasma 25-hydroxyvitamin D does not vary over the course of a malarial infection. Trans R Soc Trop Med Hyg. 2006;100(1):41–44. doi:10.1016/j.trstmh.2005.06.022
12. Barth JH, Field HP, Mather AN, et al. Serum 25 hydroxy-vitamin D does not exhibit an acute phase reaction after acute myocardial infarction. Ann Clin Biochem. 2012;49(Pt 4):399–401. doi:10.1258/acb.2011.011195
13. Young MF, Ou J, Duong C, et al. Assessment of Vitamin D status and association with inflammation: Biomarkers reflecting inflammation and nutritional determinants of anemia (BRINDA) project. Am J Clin Nutr. 2023;117(1):175–181. doi:10.1016/j.ajcnut.2022.10.018
14. Ju SY, Lee JY, Kim DH. Low 25-hydroxyvitamin D levels and the risk of frailty syndrome: a systematic review and dose-response meta-analysis. BMC Geriatr. 2018;18(1):206. doi:10.1186/s12877-018-0904-2
15. Walston J. Frailty and activation of the inflammation and coagulation systems with and without clinical comorbidities: results from the cardiovascular health study. Arch Intern Med. 2002;162(20):2333–2341. doi:10.1001/archinte.162.20.2333
16. Liu A, Bui T, Van Nguyen H, et al. Serum C-reactive protein as a biomarker for early detection of bacterial infection in the older patient. Age Ageing. 2010;39(5):559–565. doi:10.1093/ageing/afq067
17. Jorde I, Stegemann-Koniszewski S, Papra K, et al. Association of serum vitamin D levels with disease severity, systemic inflammation, prior lung function loss and exacerbations in a cohort of patients with chronic obstructive pulmonary disease (COPD). J Thorac Dis. 2021;13(6):3597–3609. doi:10.21037/jtd-20-3221
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Associations of High-Sensitivity C-Reactive Protein and Interleukin-6 with Depression in a Sample of Italian Adolescents During COVID-19 Pandemic
Serra M, Presicci A, Quaranta L, Achille M, Caputo E, Medicamento S, Margari F, Croce F, Margari L
Neuropsychiatric Disease and Treatment 2022, 18:1287-1297
Published Date: 29 June 2022
Vitamin D Ameliorates Apoptosis and Inflammation by Targeting the Mitochondrial and MEK1/2-ERK1/2 Pathways in Hyperoxia-Induced Bronchopulmonary Dysplasia
Hu J, Wu Z, Wang H, Geng H, Huo J, Zhu X, Zhu X
Journal of Inflammation Research 2022, 15:4891-4906
Published Date: 25 August 2022
The Inhibition of Evolocumab on Non-Infarct-Related Artery Disease in Patients with ST-Elevation Myocardial Infarction
Zhao Q, Sun S, Zhou F, Yue J, Luo X, Qu X
International Journal of General Medicine 2023, 16:2771-2781
Published Date: 30 June 2023
A Synergistic Effect of Remnant Cholesterol and C-Reactive Protein on Predicting the Severity of Coronary Artery Disease
Zhang Z, Chen Q, Chen Q, Hou J, Li X, Fu J, Luo Y, Su H, Long Y, Feng Q, Peng X, Jiang M, Wu D, Liu H, Cai L, Xiong S
Journal of Inflammation Research 2024, 17:11291-11303
Published Date: 19 December 2024
The Prognostic Value of CRP/Alb Ratio in Predicting Overall Survival for Hepatocellular Carcinoma Treated with Transcatheter Intra-Arterial Therapy Combined with Molecular-Targeted Agents and PD-1/PD-L1 Inhibitors
Huang X, Peng G, Kong Y, Cao X, Zhou X
Journal of Inflammation Research 2025, 18:203-217
Published Date: 8 January 2025