Back to Journals » Research and Reports in Urology » Volume 15
Is There a Relationship Between Waking Up from Sleep and the Onset of Testicular Torsion?
Authors Alzahrani MA ![]() , Alasmari MM, Altokhais MI, Alkeraithe FW, Alghamdi TA, Aldaham AS, Hakami AH, Alomair S, Hakami BO
, Alasmari MM, Altokhais MI, Alkeraithe FW, Alghamdi TA, Aldaham AS, Hakami AH, Alomair S, Hakami BO ![]()
Received 8 January 2023
Accepted for publication 17 February 2023
Published 22 February 2023 Volume 2023:15 Pages 91—98
DOI https://doi.org/10.2147/RRU.S404073
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Guglielmo Mantica
Meshari A Alzahrani,1 Mishal M Alasmari,2 Moataz I Altokhais,3 Fawaz W Alkeraithe,4 Talal A Alghamdi,4 Abdulaziz S Aldaham,5 Alwaleed H Hakami,6 Saud Alomair,7 Basel O Hakami8
1Department of Urology, College of Medicine, Majmaah University, Al-Majmaah, Saudi Arabia; 2College of Medicine, King Khalid University, Abha, Saudi Arabia; 3Department of Urology, King Khalid University Hospital, Riyadh, Saudi Arabia; 4Department of Urology, King Fahad Medical City, Riyadh, Saudi Arabia; 5College of Medicine, Jouf University, Al Gurayat, Saudi Arabia; 6College of Medicine and Surgery, Jazan University, Jazan, Saudi Arabia; 7College of Medicine, Majmaah University, Al-Majmaah, Saudi Arabia; 8Department of Urology, King Faisal Medical City for Southern Region (KFMC), Abha, Saudi Arabia
Correspondence: Meshari A Alzahrani, Department of Urology, College of Medicine, Majmaah University, Al-Majmaah, 11952, Saudi Arabia, Tel +966569990693, Fax +966164042500, Email [email protected]
Abstract: Testicular torsion is a serious urologic emergency that can present with unusual or atypical history and examination. Classical pain from testicular torsion is of sudden onset, significantly severe, and is accompanied by nausea and vomiting. However, in some patients, the initial scrotal pain appears to considerably subside within the next few hours. In others, testicular torsion tends to occur while sleeping, and many patients recount a history of being woken up from sleep by intense pain. Furthermore, some patients in this subset can resume normal activities and even sleep through the night with little or no discomfort, without a perceived need for pain medications. Other patients initially experience mild pain, which worsens over time. Consequently, these patients are less likely to be evaluated immediately. In view of these atypical cases, the question remains unanswered regarding sleep as a predisposing factor for testicular torsion. This narrative review focuses on exploring the association between sleep and testicular torsion.
Keywords: testicular torsion, torsion of the spermatic cord, acute scrotum, sleep, sleeping, literature review
Introduction
Testicular torsion (TT) is a severe, acute urological emergency that refers to torsion of the spermatic cord structures with subsequent loss of blood supply to the ipsilateral testicle. Torsion of the testes is a critical diagnosis, which unfortunately does not always present with a typical history or examination. Classically, TT pain is described as rapid in onset, instantaneously severe, and often accompanied by nausea and vomiting.1,2 A Nigerian study found that, globally, 1 in 4000 males below 25 years of age is affected annually. This study found that TT contributes to male infertility, accounting for 5.8% of testicular insufficiency.3 TT necessitates immediate diagnosis and treatment. It is widely accepted that irreversible changes will occur after 6 hours, or 4 hours in the case of an extremely twisted spermatic cord.4,5 Thus, time is the most crucial factor in the emergency treatment of TT, with the salvage rate and late outcome relying heavily on it.6–9 Surgical intervention has a 90–100% success rate within 4–8 hours of the onset of symptoms, but only 50% after 12 hours and 10% after 1 day.8 Delay presentation or intervention can be fatal, resulting in impaired fertility and testicular function loss.2
Cold weather, physical exertion, trauma, sleep, and sexual activity have all been documented as precipitating factors.10–15 An Indonesian study indicated that TT could occur during sleep or while engaging in exertional activity.16 A previous study, conducted on 31 patients, compared various factors related to acute TT. When sleep and physical activity were compared, the study found that torsion during sleep was seen in seven patients and in six patients was caused by some form of physical activity.17 In a Japanese study conducted on 70 patients to distinguish TT from torsion of the appendix, a comparison of clinical parameters (age, duration of pain, onset during sleep, and fever) showed that torsion in 33 patients began during sleep. It has been reported that testicular tenderness, testicular swelling, a high-riding testis, pain duration <24 h, and onset during sleep are all positively associated with TT.18 Studies have shown that numerous patients experience TT while sleeping, and many of these patients recount a history of waking up from sleep due to pain. In this study, we aimed to determine whether sleep was a direct cause of TT.
Materials and Methods
This review was conducted using a predefined protocol. Medline/PubMed and Google Scholar were used to identify related articles on testicular torsion and sleep available at literature published in the English language. The following keywords were used to search through articles: “Testicular Torsion”, AND “Sleep”, AND “Sleeping”. We searched for articles from the date of inception of the database until May 2022. Two senior authors (M.A.A. and B.O.H) were assigned to independently collect relevant information, including authors’ names, publication year, region of study, study design, sample size, study inclusion, and exclusion criteria, and reported association of sleep with TT presentation. In cases of disagreement, a third reviewer was asked to resolve the matter with a consensus. We considered no limitations in publication time of articles.
We found a total of 434 related articles (422 from Google Scholar and 12 from PubMed) and included articles on pediatric and adult studies that reported a relationship between testicular torsion and sleep. We excluded articles from non-English literature, nonrelevant articles, duplicate articles, abstract-only articles, no full-text articles, and books. After finding the relevant articles, the reference lists of them and also recent reviews were reviewed to avoid missing any articles.
Based on our predefined inclusion and exclusion criteria, 420 articles were excluded for not meeting our criteria; 14 articles met our criteria and had a clear relationship between testicular torsion and sleep, which we used in our review. A flow chart of the article selection process is shown in Figure 1.
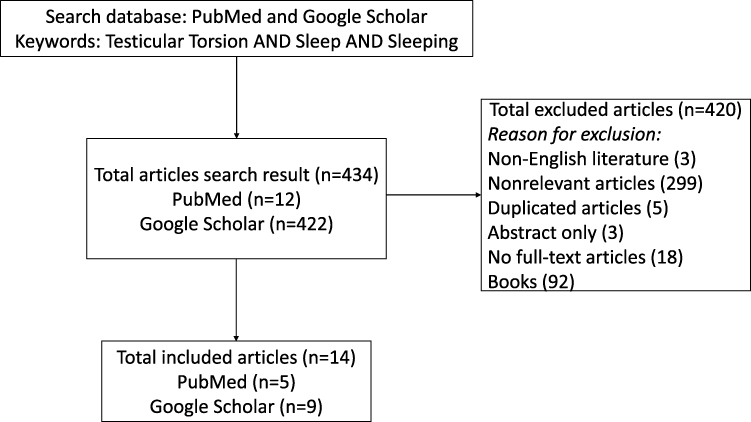 |
Figure 1 Flow diagram representing the study articles selection. |
Results
We found 14 articles that reported sleep as an associated risk factor for TT between 1926 and 2022. Most studies that reported an association between sleep and TT have been conducted in the United States. Majority of studies featured Cohort design (n = 6) including Prospective (n = 1) and Retrospective (n = 5) studies. Among studies included in this review, most of the patients with were slightly younger were ranged between newborn to elderly age group. The duration of TT presentation ranged between <1 hour to 30 days. Nine out of 14 studies did not report type of TT, remaining reported intravaginal TT (n = 39), torsion of appendix testis (n = 61). However, one study reported extravaginal TT (n = 6), 5 at neonatal period and one case 4-year-old boy (Table 1).
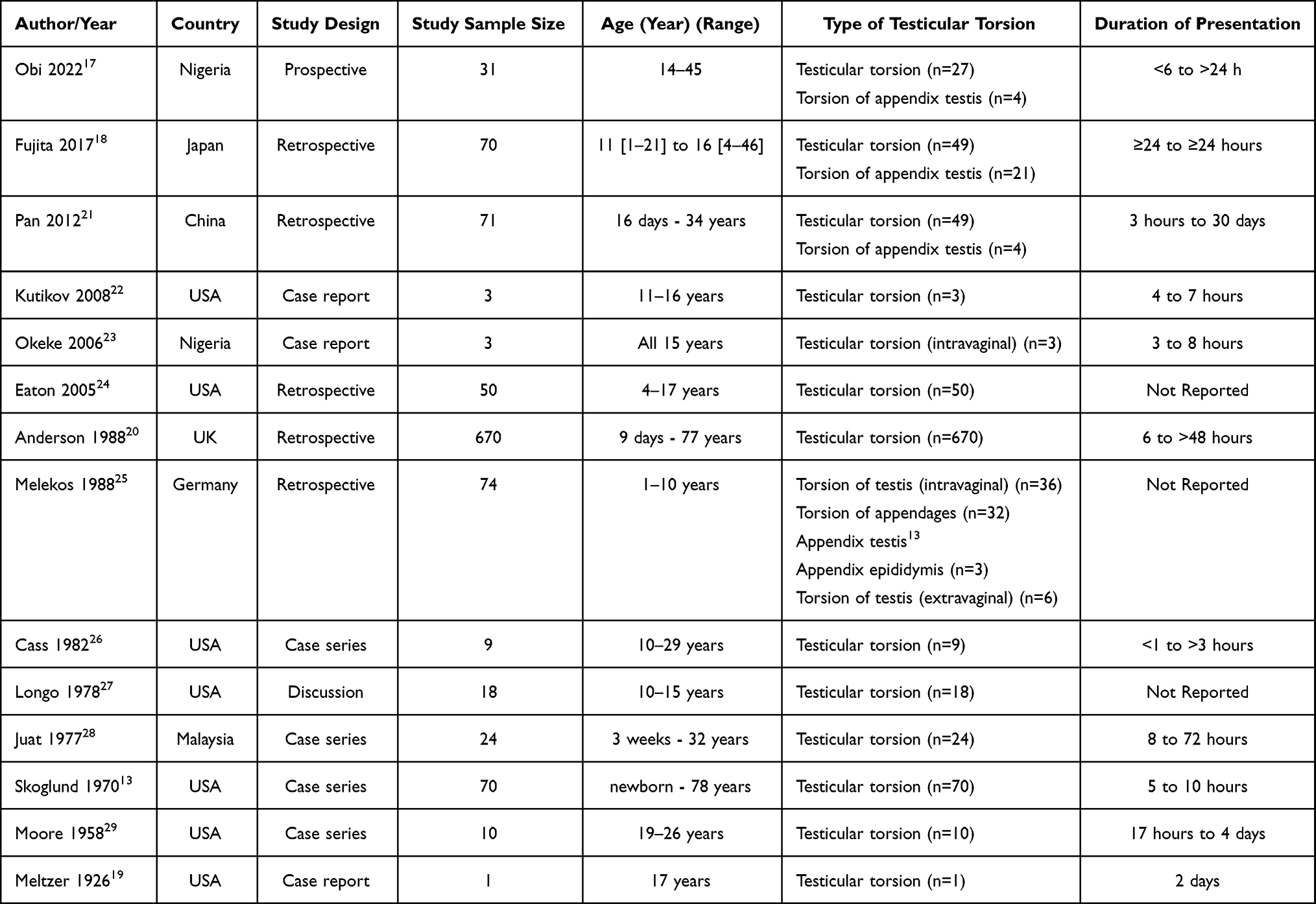 |
Table 1 Studies Reported Sleep as an Associated or Risk Factor for Testicular Torsion |
A review of the available literature on TT associated with sleep revealed 192 reported cases, the characteristics of the patients with testicular torsion related to sleep are summarized in (Table 2). The first study by Meltzer et al reported TT during sleep in patients in 1926. Most studies that reported a large number of patients presenting with TT associated with sleep originated in Japan authored by Fujita et al (40 patients), followed by Anderson et al (39 patients). Many of these studies have found that the incidence of TT involvement per testicular unit was higher on the left side than on the right side. No study reported the type of sleep, sleep duration related to TT presentation among included studies. Only three studies reported the timing of TT related to sleep, Pan et al reported TT mostly occurs late in the night or early evening, while Okeke et al report all cases developed TT during the night and Longo et al reported TT occurs at night or early morning. Suggested mechanisms attributed to TT-related sleep reported by studies included in our review as follows: sudden body movement during sleep or change of posture, sharp cremasteric muscle contraction or cremasteric muscle spasm during the sexual dream or penile erection, low ambient temperature, testis activities caused by increased nocturnal vagal excitability, high testosterone level, concomitant, or coexisting bell-clapper deformity (Table 2).
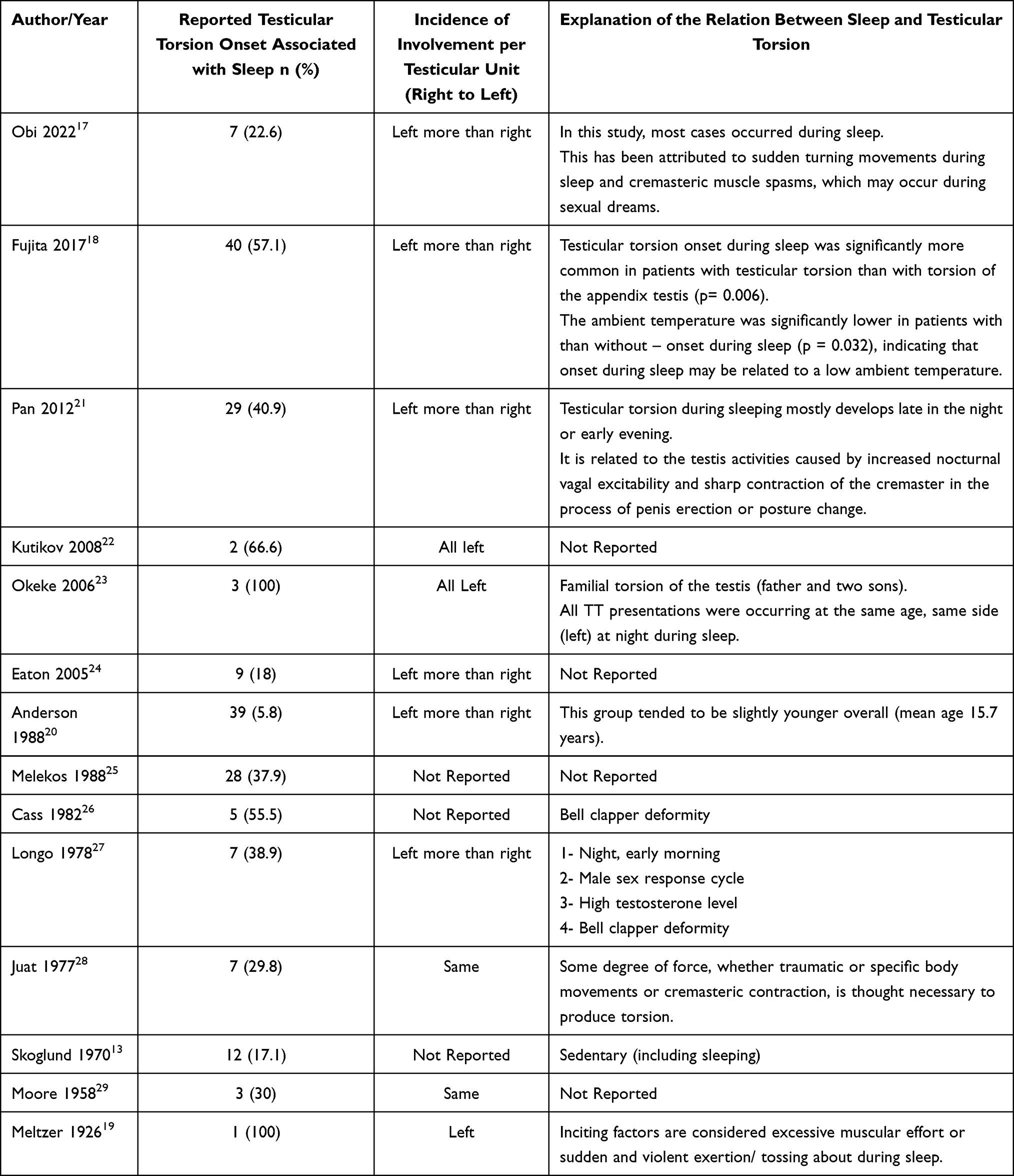 |
Table 2 Patient Characteristics with Testicular Torsion Associated with Sleep |
Discussion
Our review shares available English literatures report TT-related sleep between 1926 to November 2022.
Delasiauve first described TT in 1840.30 In our review, the first case of TT after waking from sleep was reported by Meltzer et al19 in 1926 (Table 1). Intravaginal TT is common in older men and adolescents. This type of torsion occurs frequently during sleep. This causes a bell-clapper anomaly characterized by increased testicular mobility.30,31 Cass et al highlighted various TT mechanisms in 1990.32 He reported that the testis appears to be affected by two factors, either bell-clapper deformity or the muscle that twists and holds the testes in place.
Association Between Sleep and Testicular Torsion
The causes of TT are unknown, but it could be related to cold temperatures10,33,34 or to diurnal temperature changes,35 activation of the cremasteric reflex, and/or rapid testicular growth at puberty. However, torsion can also occur at rest or during sleep.
In the literature, data elucidating the causality of the relationship between sleep and TT is scarce. Current comprehensive reviews of TT based on recently published articles, including etiology, risk factors, diagnosis, treatment, and outcome, either lacked or failed to discuss any relationship between TT and sleep.2,36 Deep sleep as a predisposing factor, along with other factors such as violent injury and strenuous exercise, can increase scrotal peristalsis and induce excessive torsion, causing the lower spermatic cord to twist.37 Previous research has found a link between frequent occasions of testicular pain that begin during sleep or shortly after waking up from deep sleep among patients with TT.6,23 One study asserted that a clinical diagnosis of TT can be definitively made when a patient experiences testicular pain when at rest or asleep.38 Another study reported that onset of TT occurs while the patient is sleeping, causing sudden awakening.39 However, these reports did not provide further details about the number of cases or the relationship between TT and sleep.
From our review, it appears that TT frequently occurs during sleep at night or after waking up from sleep. TT was reported during or after sleep in 192 cases (Table 2) in three studies reported TT mostly occurs early evening, during the night or late night or early morning.21,23,27 The explanation could be based on the theory proposed by Longo et al,27 which attributes TT in young boys to a complex sex cycle extending to a deep plateau phase during sleep under the effect of the erection reflex response during REM sleep and peak testosterone levels in the early morning, which is remarkably high among newborns and adolescents.27 The consequence of this in contemporary society, where finding transportation to the hospital at night is frequently challenging, is that patients may present to the hospital later than necessary, perhaps risking testis loss.23
From our review, TT during or after sleep happen more frequently on the left side than on the right side (Table 2). Most studies suggest that TT is more common on the left side.11,13,40–42 This is because the left spermatic cord is often slightly longer than the right, making the left testis more mobile and consequently more susceptible to torsion. This anatomical difference has been linked to the left-sided preponderance of the TT.11,13
Based on our review, most sleep-related TT patients were slightly younger (Table 2). Although intravaginal TT can occur at any age, in most instances, it peaks between 12 and 16 years of age; often occurring after the age of 10.43–48
Our review also documented the familial incidence of TT as reported by Okeke et al in a father and two of his sons who all experienced incidences of TT related to sleep23 (Table 2). There is evidence that TT runs through families,49–51 although it is unclear how this is transmitted. Approximately 10% of probands have a family history (in different relatives), and one family has three generations of torsion according to Cubillos et al.51
One study reported low ambient temperature as a cause of TT during sleep, as reported by Fujita et al,18 stating that the ambient temperature was significantly lower around patients with TT onset during sleep than around those without TT (p = 0.032), suggesting that low ambient temperature may cause the onset of TT during sleep.
It is hypothesized that the asymmetrical contraction of cremasteric muscle fibers occurs at low temperatures.10,34,52 In contrast, some authors found no statistically significant differences in the seasonal occurrence of TT.36,53
Szymusiak et al explore the relationship between sleep and body temperature.54 Sleep in mammals is associated with a reduction in core body temperature (CBT). The circadian clock in the hypothalamic suprachiasmatic nucleus regulates daily rhythms in both CBT and arousal states, and these rhythmic patterns are normally combined.54 Decreased metabolic heat production due to behavioral quiescence and decreased muscle tone, as well as changes in autonomic nervous system activity and thermoeffector activity, all contribute to the sleep-related decline in CBT.54 Reduced sympathetic tone to the peripheral vasculature, resulting in heat loss through the skin, is reflected in a sleep-related increase in distal skin temperature, which is a significant feature of sleep onset in humans.54 Patterns of the autonomic nervous system and thermoeffector activity, as well as the ability to defend against heat and cold exposure, differ during nonrapid eye movement (NREM) and rapid eye movement (REM) sleep.54 Warm-sensing neurons in the preoptic/anterior hypothalamus, which are implicated in CBT regulation, are spontaneously activated during sleep onset and NREM sleep compared to waking, and this may explain sleep-related changes in the autonomic nervous system and thermoeffector activity.54
In our review, three studies, Obi et al,17 Pan et al,21 and Juat et al28 have reported that TT associated with sleep was due to cremasteric muscle spasms or contractions. The bell-clapper deformity associated with TT-related sleep was reported in two studies26,27 (Table 2). The most common explanation for intravaginal torsion is excessive testicular mobility within a bell-clapper deformity in which the tunica vaginalis abnormally attaches proximally to the spermatic cord. The bell-clapper deformity is a congenital failure of the gubernaculum to posteriorly attach to the testis, resulting in increased testicular mobility within the tunica vaginalis and a predisposition to TT.55
Recent results from a systematic review identified strong evidence of the association between sleep quality, sleep duration, and muscle strength among middle-aged and older adults.56 Sleep disruptions may have an effect on muscle function because sleep interferes with catabolic and anabolic hormonal pathways. Reduced sleep quality and duration may have an effect on hormone secretion, resulting in an imbalance in muscle metabolism (ie between protein synthesis and degradation).57 The same conclusion is reached by Dattilo et al, who show that sleep debt causes physiological alterations such as an increase in cortisol and a decrease in testosterone and growth factor. These alterations may cause muscular atrophy and muscle fiber loss.58 Strong evidence exists that the circadian clock is essential for the physiology and operation of muscles.59 A sign of declining physiologic function, prolonged sleep duration is comparable to impaired neuromuscular function. Long periods spent in bed while sleeping could immediately result in diminished muscle strength. On the other hand, excessive sleep or time in bed may be caused by inactivity, which is related to limited muscle power.60,61 According to a study, testosterone levels rose as sleep time increased up to 9.9 hours. In addition to the testosterone effect, unknown mechanisms also link muscle strength and sleep duration in men.62 The circadian rhythm of testosterone is characterized by a trough in the late evening (8 PM), an increase during sleep, and a peak in the morning (8 AM).63,64 However, it has also been found that its elevation may be linked to sleeping rather than sleep timing. Even during the daytime, testosterone levels rose, but remained low at night.65 As a result, sleep may be one of the major determinants of testosterone production or secretion.
From previous literature, it is clear that sleep quality, duration, and muscle function may be critically related as risk factor associated with TT especially cremasteric muscle spasms or contractions or associated with the bell-clapper deformity. Further future clinical studies among individual with a history of TT or risk factors for TT is important to identify the relationship between their muscle function and risk for developing TT.
Recommendation and Future Direction
The Testicular Workup for Ischemia and Suspected Torsion (TWIST) score is a 7-point tool to evaluate acute scrotal pain, introduced by Barbosa et al.66 The parameters for evaluation include testicular swelling (2 points), hard testis (2 points), high-riding testis (1 point), absent cremasteric reflex (1 point), and nausea/vomiting (1 point).66 A recent systematic review and meta-analysis showed that TWIST is a valuable technique for detecting possible TT and is suitable for widespread use, suggesting that it is a helpful tool for making treatment decisions in cases of acute scrotal presentation.67 Based on our review, we suggested adding one more point to the TWIST score for TT presentation concomitant with sleep. Adopting this upgrade in the TWIST score to confirm the association of sleep as a risk factor for TT requires further investigation through future studies.
Limitations
The strength of this review is for the first time and to our knowledge, this review highlighted TT-related sleep in English literature. Due to lack of homogeneity of studies, it was difficult to conduct a systematic review. Narrative reviews may be broader in scope than systematic reviews but have been criticized for lacking synthesis and rigor.
Conclusion
This review emphasized that a better understanding of the onset of testicular torsion during sleep may aid in distinguishing testicular torsion from other acute scrotum presentations. Testicular torsion-related sleep lends credence to the notion that suspected testicular torsion based on symptoms and other confirmatory tests necessitates immediate surgical intervention. More research into the relationship between sleep and testicular torsion is required.
Acknowledgments
The authors would like to thank the Deanship of Scientific Research at Majmaah University for supporting this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mellick LB, Sinex J. Testicular torsion pain honeymoons. Pediatr Emerg Care. 2019;35(12):e241–e244. doi:10.1097/PEC.0000000000001286
2. Fehér ÁM, Bajory Z. A review of main controversial aspects of acute testicular torsion. J Acute Dis. 2016;5(1):1–8. doi:10.1016/j.joad.2015.06.017
3. Oseni TI. Testicular torsion in a 17 year old boy: role of school health education. J Contracept Stud. 2018;3:12.
4. Yang C, Song B, Tan J, Liu X, Wei GH. Testicular torsion in children: a 20-year retrospective study in a single institution. ScientificWorldJournal. 2011;11:362–368. doi:10.1100/tsw.2011.39
5. Drlík M, Kočvara R. Torsion of spermatic cord in children: a review. J Pediatr Urol. 2013;9(3):259–266. doi:10.1016/j.jpurol.2012.05.016
6. DaJusta DG, Granberg CF, Villanueva C, Baker LA. Contemporary review of testicular torsion: new concepts, emerging technologies and potential therapeutics. J Pediatr Urol. 2013;9(6Pt A):723–730. doi:10.1016/j.jpurol.2012.08.012
7. Gatti JM, Patrick Murphy J. Current management of the acute scrotum. Semin Pediatr Surg. 2007;16(1):58–63. doi:10.1053/j.sempedsurg.2006.10.008
8. Sharp VJ, Kieran K, Arlen AM. Testicular torsion: diagnosis, evaluation, and management. Am Fam Physician. 2013;88(12):835–840.
9. Crawford P, Crop JA. Evaluation of scrotal masses. Am Fam Physician. 2014;89(9):723–727.
10. Srinivasan AK, Freyle J, Gitlin JS, Palmer LS. Climatic conditions and the risk of testicular torsion in adolescent males. J Urol. 2007;178(6):2585–2588. doi:10.1016/j.juro.2007.08.049
11. Williamson RC. Torsion of the testis and allied conditions. Br J Surg. 1976;63(6):465–476. doi:10.1002/bjs.1800630618
12. Lindsey D, Stanisic TH. Diagnosis and management of testicular torsion: pitfalls and perils. Am J Emerg Med. 1988;6(1):42–46. doi:10.1016/0735-6757(88)90204-5
13. Skoglund RW, McRoberts JW, Ragde H. Torsion of the spermatic cord: a review of the literature and an analysis of 70 new cases. J Urol. 1970;104(4):604–607. doi:10.1016/s0022-5347(17)61792-0
14. Nöske HD, Kraus SW, Altinkilic BM, Weidner W. Historical milestones regarding torsion of the scrotal organs. J Urol. 1998;159(1):13–16. doi:10.1016/s0022-5347(01)63997-1
15. Ugwu BT, Dakum NK, Yiltok SJ, et al. Testicular torsion on the Jos plateau. West Afr J Med. 2003;22(2):120–123. doi:10.4314/wajm.v22i2.27929
16. Zamzami Z, Yunfaista Y. Characteristics of testicular torsion in arifin achmad regional general hospital, Pekanbaru, Riau Province, Indonesia. Natl J Med Res. 2018;8(01):36–38.
17. Obi AO, Okeke CJ, Ugwuidu EI. Acute testicular torsion: a critical analysis of presentation, management and outcome in southeast Nigeria. Niger J Clin Pract. 2020;23(11):1536–1541. doi:10.4103/njcp.njcp_188_20
18. Fujita N, Tambo M, Okegawa T, Higashihara E, Nutahara K. Distinguishing testicular torsion from torsion of the appendix testis by clinical features and signs in patients with acute scrotum. Res Rep Urol. 2017;9:169–174. doi:10.2147/RRU.S140361
19. Meltzer M. Torsion of the testicle. J Urol. 1926;15(6):601–610. doi:10.1016/S0022-5347(17)73486-6
20. Anderson JB, Williamson RC. Testicular torsion in Bristol: a 25-year review. J Br Surg. 1988;75(10):988–992. doi:10.1002/bjs.1800751015
21. Pan F, Zhu Z, Li B, Pang Z, Xiao Y, Zeng F. Emergency treatment of testicular torsion and postoperative follow-up: a 71 case report. J Huazhong Univ Sci Technol Med Sci. 2012;32(5):704–706. doi:10.1007/s11596-012-1021-7
22. Kutikov A, Casale P, White MA, et al. Testicular compartment syndrome: a new approach to conceptualizing and managing testicular torsion. Urology. 2008;72(4):786–789. doi:10.1016/j.urology.2008.03.031
23. Okeke LI, Ikuerowo OS. Familial torsion of the testis. Int Urol Nephrol. 2006;38(3–4):641–642. doi:10.1007/s11255-006-0049-7
24. Eaton SH, Cendron MA, Estrada CR, et al. Intermittent testicular torsion: diagnostic features and management outcomes. J Urol. 2005;174(4 Pt 2):1532–1535. doi:10.1097/01.ju.0000177726.84913.cc
25. Melekos MD, Asbach HW, Markou SA. Etiology of acute scrotum in 100 boys with regard to age distribution. J Urol. 1988;139(5):1023–1025. doi:10.1016/s0022-5347(17)42756-x
26. Cass AS. Elective orchiopexy for recurrent testicular torsion. J Urol. 1982;127(2):253–254. doi:10.1016/S0022-5347(17)53727-1
27. Longo VJ. Point of view--torsion of testis: a new twist. Urology. 1978;12(6):743. doi:10.1016/0090-4295(78)90450-8
28. Juat WT, Hin OT, Somasundaram K. Torsion of the testes: a review of 24 cases. Med J Malaysia. 1977;32(2):168–171.
29. Moore CA. Torsion of the spermatic cord: a review of ten cases. J Urol. 1958;80(4):260–262. doi:10.1016/s0022-5347(17)66175-5
30. Underhill BM. Torsion of the testicle. Lancet. 1955;268(6855):129–130. doi:10.1016/s0140-6736(55)91702-5
31. Kapoor S. Testicular torsion: a race against time. Int J Clin Pract. 2008;62(5):821–827. doi:10.1111/j.1742-1241.2008.01727.x
32. Cass AS. Torsion of the testis. Postgrad Med. 1990;87(1):69–74. doi:10.1080/00325481.1990.11704522
33. Lyronis ID, Ploumis N, Vlahakis I, Charissis G. Acute scrotum -etiology, clinical presentation and seasonal variation. Indian J Pediatr. 2009;76(4):407–410. doi:10.1007/s12098-009-0008-2
34. Chiu B, Chen CS, Keller JJ, Lin CC, Lin HC. Seasonality of testicular torsion: a 10-year nationwide population based study. J Urol. 2012;187(5):1781–1785. doi:10.1016/j.juro.2011.12.104
35. Chen JS, Lin YM, Yang WH. Diurnal temperature change is associated with testicular torsion: a nationwide, population based study in Taiwan [published correction appears in J Urol. 2018 Jan 29]. J Urol. 2013;190(1):228–232. doi:10.1016/j.juro.2013.02.013
36. Xue E, Yu Y, Lin L, Li Z, Su H. Application value of real-time shear wave elastography in differential diagnosis of testicular torsion. Med Ultrason. 2020;22(1):43–48. doi:10.11152/mu-2200
37. King H, Whelan P. Treatment of acute scrotal pain. Br Med J. 1984;288(6430):1576–1577. doi:10.1136/bmj.288.6430.1576-A
38. Hricak H, Lue T, Filly RA, Alpers CE, Zeineh SJ, Tanagho EA. Experimental study of the sonographic diagnosis of testicular torsion. J Ultrasound Med. 1983;2(8):349–356. doi:10.7863/jum.1983.2.8.349
39. Shergill IS, Foley CL, Arya M, Bott SR, Mundy AR. Testicular torsion unravelled. Hosp Med. 2002;63(8):456–459. doi:10.12968/hosp.2002.63.8.1964
40. Bello JO. Burden and seasonality of testicular torsion in tropical Africa: analysis of incident cases in a Nigerian community. Afr J Urol. 2018;24(1):79–82. doi:10.1016/j.afju.2017.10.001
41. Takure AO, Shittu OB, Adebayo SA, Okeke LO, Olapade-Olaopa EO. Torsion of the testis and factors that determine the choice of orchiectomy and unilateral orchidopexy. Niger Postgrad Med J. 2013;20(3):197–202.
42. Jones DJ, Macreadie D, Morgans BT. Testicular torsion in the armed services: twelve year review of 179 cases. Br J Surg. 1986;73(8):624–626. doi:10.1002/bjs.1800730813
43. Mansbach JM, Forbes P, Peters C. Testicular torsion and risk factors for orchiectomy. Arch Pediatr Adolesc Med. 2005;159(12):1167–1171. doi:10.1001/archpedi.159.12.1167
44. Murphy FL, Fletcher L, Pease P. Early scrotal exploration in all cases is the investigation and intervention of choice in the acute paediatric scrotum. Pediatr Surg Int. 2006;22(5):413–416. doi:10.1007/s00383-006-1681-0
45. Mäkelä E, Lahdes-Vasama T, Rajakorpi H, Wikström S. A 19-year review of paediatric patients with acute scrotum. Scand J Surg. 2007;96(1):62–66. doi:10.1177/145749690709600112
46. Mushtaq I, Fung M, Glasson MJ. Retrospective review of paediatric patients with acute scrotum. ANZ J Surg. 2003;73(1–2):55–58. doi:10.1046/j.1445-2197.2003.02612.x
47. Sidler D, Brown RA, Millar AJ, Rode H, Cywes S. A 25-year review of the acute scrotum in children. S Afr Med J. 1997;87(12):1696–1698.
48. Anderson PA, Giacomantonio JM. The acutely painful scrotum in children: review of 113 consecutive cases. Can Med Assoc J. 1985;132(10):1153–1155.
49. Cunningham RF. Familial occurrence of testicular torsion. JAMA. 1960;174(10):1330–1331. doi:10.1001/jama.1960.63030100018026b
50. Collins K, Broecker BH. Familial torsion of the spermatic cord. J Urol. 1989;141(1):128–129. doi:10.1016/s0022-5347(17)40618-5
51. Cubillos J, Palmer JS, Friedman SC, Freyle J, Lowe FC, Palmer LS. Familial testicular torsion. J Urol. 2011;185(6 Suppl):2469–2472. doi:10.1016/j.juro.2011.01.022
52. Korkes F, Cabral PR, Alves CD, Savioli ML, Pompeo AC. Testicular torsion and weather conditions: analysis of 21,289 cases in Brazil. Int Braz J Urol. 2012;38(2):222–229. doi:10.1590/s1677-55382012000200010
53. Cost NG, Bush NC, Barber TD, Huang R, Baker LA. Pediatric testicular torsion: demographics of national orchiopexy versus orchiectomy rates. J Urol. 2011;185(6 Suppl):2459–2463. doi:10.1016/j.juro.2011.01.016
54. Szymusiak R. Body temperature and sleep. Handb Clin Neurol. 2018;156:341–351. doi:10.1016/B978-0-444-63912-7.00020-5
55. Nassiri N, Zhu T, Asanad K, Vasquez E. Testicular torsion from bell-clapper deformity. Urology. 2021;147:275. doi:10.1016/j.urology.2020.06.045
56. Pana A, Sourtzi P, Kalokairinou A, Pastroudis A, Chatzopoulos ST, Velonaki VS. Association between muscle strength and sleep quality and duration among middle-aged and older adults: a systematic review. Eur Geriatr Med. 2021;12(1):27–44. doi:10.1007/s41999-020-00399-8
57. Piovezan RD, Abucham J, Dos Santos RV, Mello MT, Tufik S, Poyares D. The impact of sleep on age-related sarcopenia: possible connections and clinical implications. Ageing Res Rev. 2015;23(Pt B):210–220. doi:10.1016/j.arr.2015.07.003
58. Dattilo M, Antunes HK, Medeiros A, et al. Sleep and muscle recovery: endocrinological and molecular basis for a new and promising hypothesis. Med Hypotheses. 2011;77(2):220–222. doi:10.1016/j.mehy.2011.04.017
59. Chatterjee S, Ma K. Circadian clock regulation of skeletal muscle growth and repair. F1000Res. 2016;5:1549. doi:10.12688/f1000research.9076.1
60. Chen HC, Hsu NW, Chou P. The association between sleep duration and hand grip strength in community-dwelling older adults: the Yilan study, Taiwan. Sleep. 2017;40(4). doi:10.1093/sleep/zsx021
61. Fu L, Jia L, Zhang W, et al. The association between sleep duration and physical performance in Chinese community-dwelling elderly. PLoS One. 2017;12(3):e0174832. doi:10.1371/journal.pone.0174832
62. Auyeung TW, Kwok T, Leung J, et al. Sleep duration and disturbances were associated with testosterone level, muscle mass, and muscle strength--a cross-sectional study in 1274 older men. J Am Med Dir Assoc. 2015;16(7):630.e1–630.e6306. doi:10.1016/j.jamda.2015.04.006
63. de Lacerda L, Kowarski A, Johanson AJ, Athanasiou R, Migeon CJ. Integrated concentration and circadian variation of plasma testosterone in normal men. J Clin Endocrinol Metab. 1973;37(3):366–371. doi:10.1210/jcem-37-3-366
64. Tenover JS, Matsumoto AM, Clifton DK, Bremner WJ. Age-related alterations in the circadian rhythms of pulsatile luteinizing hormone and testosterone secretion in healthy men. J Gerontol. 1988;43(6):M163–M169. doi:10.1093/geronj/43.6.m163
65. Axelsson J, Ingre M, Akerstedt T, Holmbäck U. Effects of acutely displaced sleep on testosterone. J Clin Endocrinol Metab. 2005;90(8):4530–4535. doi:10.1210/jc.2005-0520
66. Barbosa JA, Tiseo BC, Barayan GA, et al. Development and initial validation of a scoring system to diagnose testicular torsion in children [published correction appears in J Urol. 2014 Aug;192(2):619]. J Urol. 2013;189(5):1859–1864. doi:10.1016/j.juro.2012.10.056
67. Qin KR, Qu LG. Diagnosing with a TWIST: systematic review and meta-analysis of a testicular torsion risk score. J Urol. 2022;208(1):62–70. doi:10.1097/JU.0000000000002496
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.