Back to Journals » Cancer Management and Research » Volume 13
Is There a Regular Pattern in the Recovery of Parathyroid Function After Thyroid Cancer Surgery?
Authors Yao XY, Zhou Y, Chen SJ, Wu Y, Bian C, Chen H, Liu H
Received 26 June 2021
Accepted for publication 20 August 2021
Published 3 September 2021 Volume 2021:13 Pages 6891—6899
DOI https://doi.org/10.2147/CMAR.S326705
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Xueqiong Zhu
Xi-Yu Yao,1,* Yan Zhou,2,* Shun-Jin Chen,1 Yu Wu,1 Cong Bian,1 Hongbin Chen,1 Hui Liu1
1Department of Head and Neck Surgery, Fujian Cancer Hospital & Fujian Medical University Cancer Hospital, Fuzhou, Fujian, 350011, People’s Republic of China; 2Department of Epidemiology, Fujian Cancer Hospital & Fujian Medical University Cancer Hospital, Fuzhou, Fujian, 350011, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hui Liu
Department of Head and Neck Surgery, Fujian Cancer Hospital & Fujian Medical University Cancer Hospital, Fuzhou, Fujian, 350011, People’s Republic of China
Tel +86 138 0506 9511
Email [email protected]
Purpose: To investigate whether there is a pattern of recovery of parathyroid function after thyroid cancer surgery.
Patients and Methods: The study included 183 patients with papillary thyroid cancer (PTC) who underwent “total thyroidectomy (TT)” plus “unilateral central lymph node dissection (UCLND)” or “bilateral central lymph node dissection (BCLND)”. The intact parathyroid hormone (iPTH) and serum calcium (sCa) were analyzed several times within 1 month after surgery to explore the recovery pattern of parathyroid gland function. Then, these 183 cases were divided into group A (97 cases) with UCLND and group B (86 cases) with BCLND to analyze whether the impairment and recovery of parathyroid function were different between the two subgroups.
Results: Postoperative hypoparathyroidism was seen in 115 out of 183 cases. iPTH values decreased significantly on postoperative day (POD) 1 compared with preoperative values, dropped to the lowest point on POD 3, showed an increasing trend on POD 5 and 14, and increased to 85.0% of preoperative values at POD30, whereas changes in sCa differ from changes in iPTH, which showed the lowest sCa value on POD1, and rebounded on the POD3 with the intervention of calcium supplementation, and continued to rise on the POD5 and POD14, and the sCa value reached 96.6% of the preoperative level at POD30. Subgroup analysis showed that temporary hypoparathyroidism was more pronounced in group B than in group A. SCa and iPTH levels in both subgroups showed the same trend of first decrease and then increase.
Conclusion: The recovery of hypocalcemia and hypo-iPTHemia in the first month after thyroid cancer surgery shows a trend of decreasing and then increasing, and knowing the recovery of parathyroid function at different time points is of great value to surgeons and patients alike.
Keywords: hypoparathyroidism, hypocalcaemia, parathyroid hormone, thyroid carcinoma, thyroidectomy, lymph node dissection
Introduction
In patients with PTC who undergo TT with central zone lymph node dissection (CLND), the most worrisome postoperative complication is impaired parathyroid function in the form of hypo-iPTHemia and/or hypocalcemia. Given the unknown side effects of human recombinant PTH, the need for injections and the high cost, the first line of treatment for post-operative hypoparathyroidism is still calcium supplementation.1 For experienced thyroid specialists, this procedure can be performed with a high degree of confidence that the parathyroid glands will be preserved. Due to the impact on the parathyroid glands and their blood supply, postoperative hypoparathyroidism may occur to varying degrees after this procedure, with most patients recovering parathyroid function within six months and eventually only about 1–3% of patients developing long-term hypoparathyroidism.2 Current research and literature reports are mainly concerned with the prediction and management of hypocalcemia or hypoparathyroidism following thyroid surgery.3–5 There is little literature that specifically summarizes the analysis of how iPTH and sCa change or recover in the short-term postoperative period, especially in the first month after surgery. In this study, we analyzed the sCa and iPTH values of patients who underwent TT with CLND to explore and summarize their recovery patterns, so as to help surgeons to formulate surgical plans and calcium supplementation strategies more rationally, as well as to communicate more effectively with patients about postoperative complications, so that patients can safely survive the perioperative period and improve their quality of life in the long and short term.
Patients and Methods
This study is a retrospective study. 222 patients with PTC who underwent TT with CLND in our unit throughout 2019 were collected, and all cases are performed by the same team of surgeons. The criteria for inclusion: age 18–70 years, all PTC cases were confirmed by preoperative puncture cytology combined with intraoperative cryopathology. 39 of the 222 cases were excluded: 1, age did not meet the inclusion criteria (4 cases); 2, unexplained preoperative hypocalcemia (1 case); 3, usual oral calcium (2 cases); 4, combined hyperthyroidism (2 cases); 5, combined parathyroid disease (combined hyperparathyroidism 2 cases); 6, previous history of thyroid surgery (18 cases); 7, previous history of neck radiotherapy (3 cases); 8, previous history of major gastrectomy (1 case); 9, bilateral lateral lymph node dissection (LND) during the same period (3 cases); 10, CLND was not performed because malignancy was not confirmed preoperatively and intraoperatively, but postoperative pathology confirmed PTC (2 cases); 11, 1 case of lost to follow-up. The remaining 183 cases were included in the study.During hospitalization, electrolytes and iPTH were tested on the morning of POD1 and POD3, and if postoperative hypocalcemia (sCa <2.0 mmol/L, normal reference value 2.10–2.70 mmol/L) or hypo-PTHemia (iPTH <1.3 pmol/L, normal reference value 1.3–9.3 pmol/L) was present, then electrolytes and iPTH were retested in the morning on POD5 and POD14 (range12-16, median 14), and discharged patients had their blood drawn at the outpatient clinic for retesting. No calcium was given on the day of surgery, and oral calcium carbonate 600 mg/dose twice/day after meals was routinely started on the first POD, and oral calcium carbonate 600 mg/dose three times/day with calcitriol (0.5ug QD) was added for those with combined hypo-PTHemia.Additional intravenous calcium (10% calcium gluconate, 2–4 g/day) will be administered when sCa is less than 1.75 mmol/L or when symptomatic hypocalcemia or Chvostek’s sign is strongly positive.4,5 According to the monitored iPTH and sCa, the intravenous calcium was gradually reduced or stopped, and patients were discharged from the hospital only when they could maintain serum calcium >1.75 mmol/L with no obvious hypocalcemia symptoms with only oral calcium ± calcitriol, otherwise they continued to stay in the hospital for observation. At POD1, 3, 5, and 14 monitoring, patients with sCa≥2.0 mmol/l and iPTH ≥1.3 mmol/L on two consecutive monitoring were discontinued from calcium ± calcitriol, otherwise they continued to take it. All patients had their electrolytes, iPTH and thyroid function checked 1 month after surgery and returned to our outpatient clinic for follow-up. Subsequent follow-ups were generally once every 3–6 months for 5 years and once a year after 5 years. Parathyroidism can be classified as biochemical or symptomatic, temporary or permanent, and is defined according to the American Association of Clinical Endocrinologists (AACE).5
First, sCa and iPTH values monitored several times during 1 month after surgery were analyzed in 183 patients to understand the changes of the two values, draw the change curve and explore the regularity.Then, the 183 cases were analyzed by subgroups, and 97 cases of “TT + UCLND ± unilateral LND” were classified as group A, and 86 cases of “TT + BCLND ± unilateral LND” were classified as group B. The clinical data of the two subgroups were compared to analyze whether the impaired parathyroid function and recovery were different in the two subgroups. UCLND means dissection of the paratracheal, pre-tracheal, and anterior laryngeal lymph nodes on the side of the thyroid lesion. BCLND means dissection of bilateral paratracheal, pre-tracheal and anterior laryngeal lymph nodes. Central zone boundaries were defined according to the American Thyroid Association (ATA).6
Statistical analysis of the data was performed with the SPSS 20.0 software package. The student t test (normal distribution) or Mann–Whitney U-test (non-normal distribution) was used for the measurement data. The χ2 test or Fisher’s exact probability method was used for the count data. p < 0.05 was considered statistically different.
Results
Outcome 1: The clinical data of 183 patients with PTC are shown in Table 1, of which 115 patients had hypoparathyroidism and the perioperative values are shown in Table 2. It can be seen that iPTH and sCa show a curve of decrease and then increase over time. The specific changes were as follows: iPTH levels decreased significantly on POD1 compared to preoperative day, continued to decrease to the lowest point on POD3, started to increase on POD5, continued to increase on POD14 and increased to 85.0% (3.23/3.80, mmol/l) of preoperative levels on POD30. The change in sCa was different from iPTH, showing the lowest sCa on POD1 and then rebounded on the POD3 with the intervention of calcium supplementation, continued to rise on the POD5 and POD14,and reaching 96.6% of the preoperative levels on POD30.
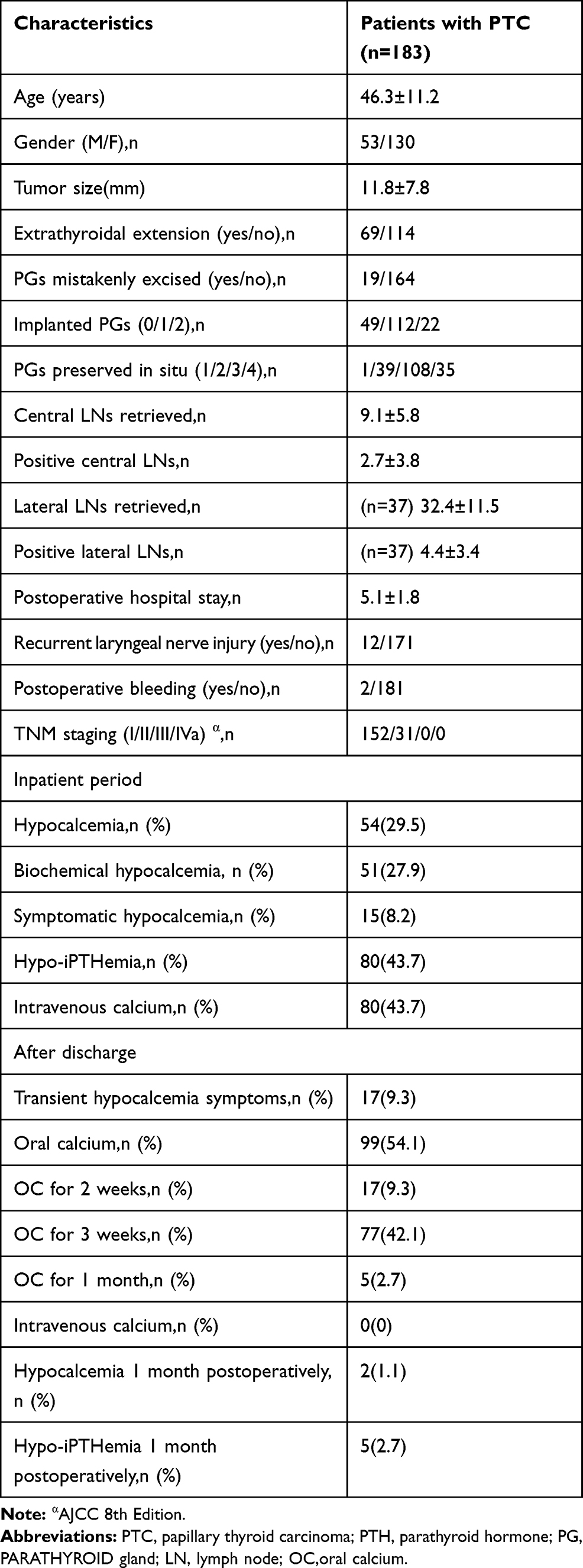 |
Table 1 Clinical Characteristics of 183 Patients with PTC |
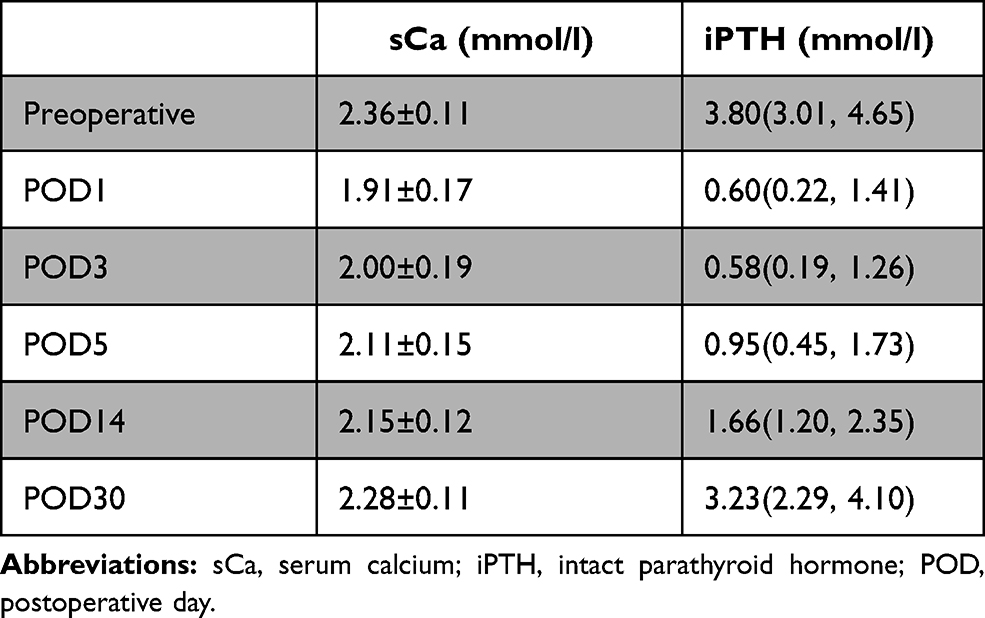 |
Table 2 Serum Calcium and iPTH in 115 Patients |
Outcome 2: The perioperative clinical data of groups A and B are compared in Tables 3–5.
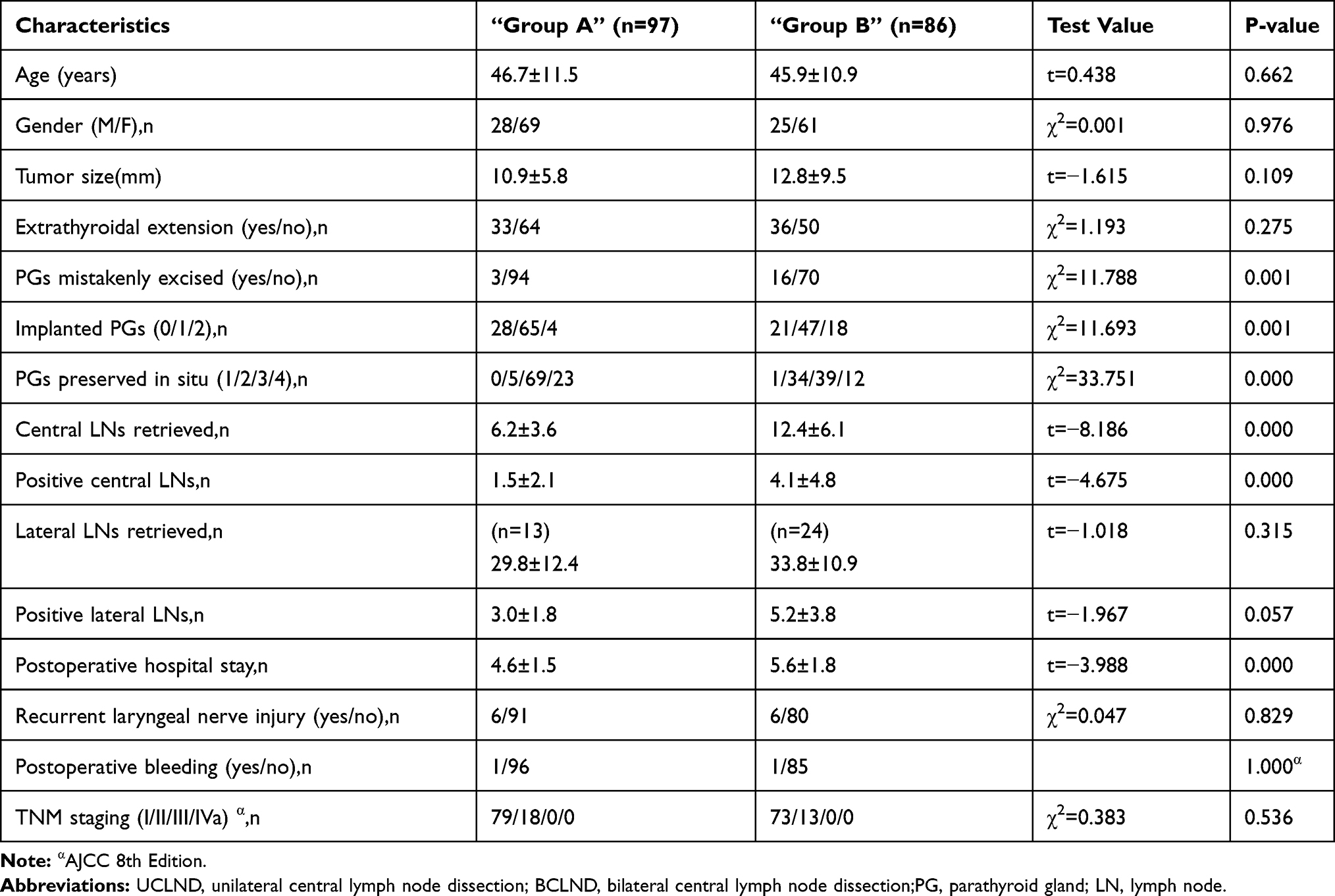 |
Table 3 Comparison of Clinical Data Between “Group A (Uclnd)” and “Group B (Bclnd) “ |
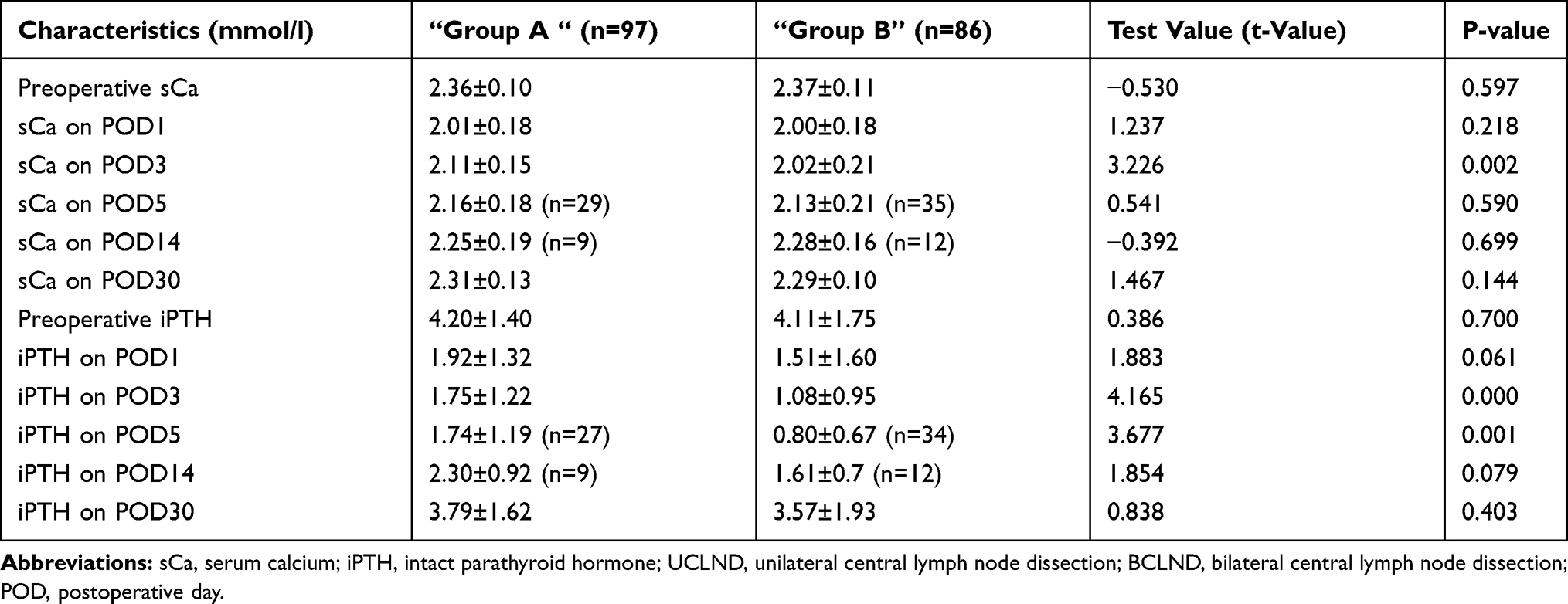 |
Table 4 Comparison of Serum Calcium and iPTH In “Group A (Uclnd)” and “Group B (Bclnd) “ |
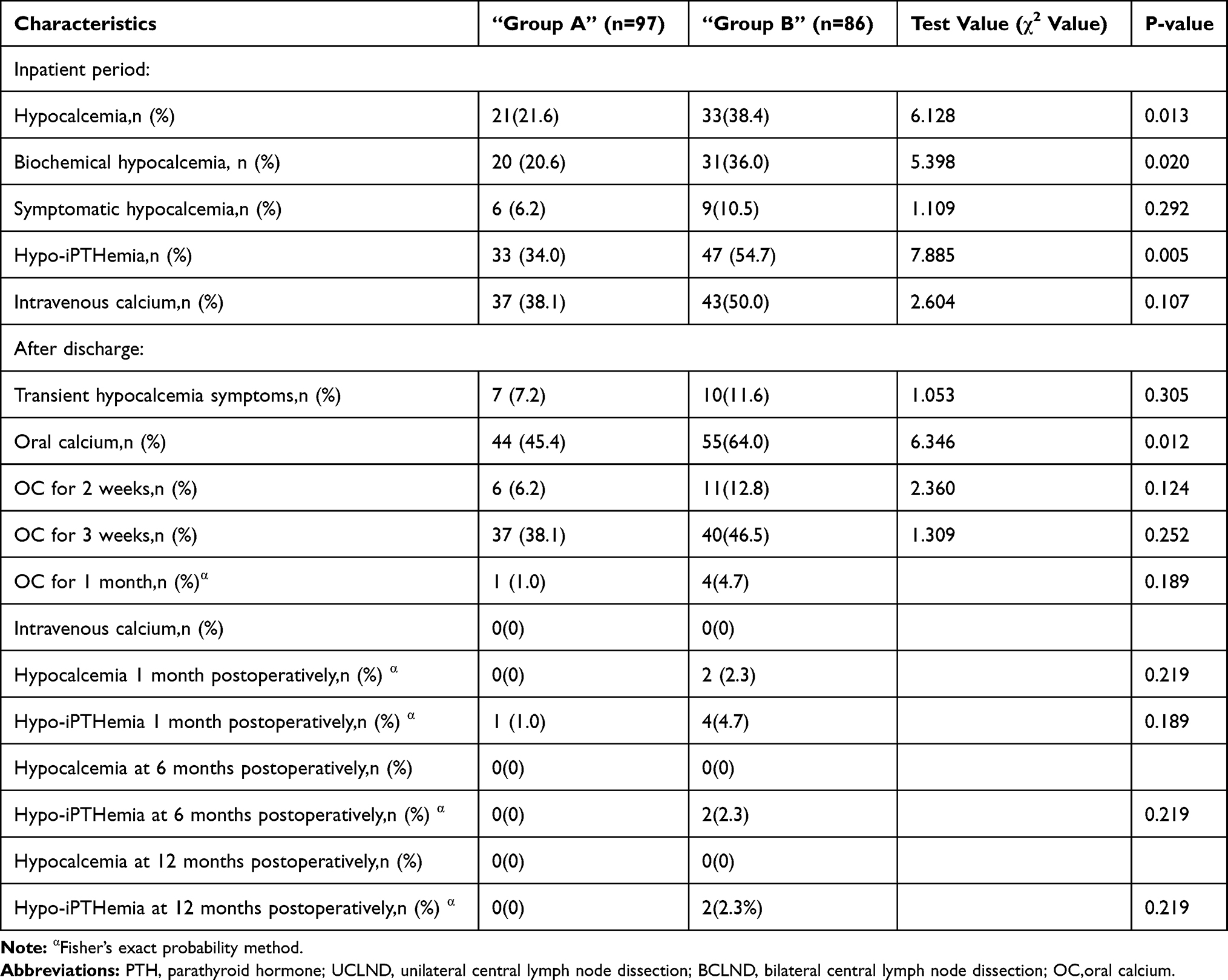 |
Table 5 Comparison of Postoperative Data Between “Group A (Uclnd)” and “Group B (Bclnd)” |
As can be seen in Tables 3 and 4, there were no significant differences in gender, age, tumor size, extraperitoneal invasion, tumor TNM stage (AJCC 8th edition),7 preoperative sCa value, and preoperative iPTH value between group A and group B. No postoperative complications such as wound infection and lymphatic fistula occurred in both groups, and there was no statistical difference in the incidence of damage to the recurrent laryngeal nerve and postoperative bleeding between the two groups (p>0.05).
Thyroidectomy is performed using fine envelope dissection. Intraoperatively, parathyroid glands were routinely identified and preserved in situ as much as possible. When parathyroid glands were judged to have lost blood supply or when the success rate of in situ preservation was estimated to be low, autologous transplantation was used, in which parathyroid glands were cut into homogenates and injected into the deltoid muscle of the upper arm. Intraoperatively, the isolated specimen including the thyroid gland and the central region tissues were carefully examined, and if suspicious parathyroid tissue was found, a small portion of it was cut out and confirmed by frozen pathology for autografting. If parathyroid tissue was found on postoperative paraffin pathology, it was defined as a parathyroid gland that had been mistakenly excised. Intraoperative parathyroid gland identification, preservation and autologous transplantation were recorded faithfully in the surgical record, and unidentified parathyroid glands were not included in the data of this study.Only one of the 183 cases in group B had one parathyroid gland preserved in situ, while the remaining 182 cases had at least two parathyroid glands preserved in situ.Compared with group A, group B had fewer parathyroid glands preserved in situ than group A (p<0.05) and more parathyroid glands autologously transplanted (p<0.05), while group B also had more cases of parathyroid glands mistakenly excised than group A (p<0.05).
As shown in Table 5: The incidence of both hypocalcemia or hypo-PTHemia was higher in group B than in group A (p<0.05). The whole group showed symptoms of hypocalcemia in 15 cases (6 cases in group A and 9 cases in group B), of which 10 cases (4 cases in group A and 6 cases in group B) showed numbness of the face and/or limbs, and the remaining 5 cases (2 cases in group A and 3 cases in group B) showed twitching of the hands in addition to the above symptoms, which were controlled by additional intravenous calcium and did not occur twice. The whole group of patients did not show any clinical manifestations of severe hypocalcemia such as respiratory distress and cardiac arrhythmia.
The incidence of transient hypocalcemia symptoms was not high in both groups A and B after discharge, 7.2% and 11.6%, respectively, and the patients described the symptoms as mild numbness in the hands or (and) feet, or (and) face, and no twitching or respiratory distress. Patients were discharged from the hospital with weekly monitoring of sCa and iPTH values as prescribed by the surgeon. In the absence of symptoms of hypocalcemia and when sCa and iPTH were normal on two consecutive occasions within 1 month after surgery, it was recommended that calcium and calcitriol could be discontinued. All 94 of the 99 patients who developed hypocalcemia or hypo-PTHemia discontinued calcium with calcitriol at 2–3 weeks after discharge, 17.2% (17/99) at 2 weeks and 77.8% (77/99) at 3 weeks. Only 5 cases (1 in group A and 4 in group B) still had hypoparathyroidism at 1 month postoperatively, and 2 of them (belonging to group B) had sCa values below 2 mmol/l, while the remaining 3 cases had normal sCa values. These 5 patients continued to take oral calcium carbonate 600 mg/dose 2–3 times/day, and sCa and iPTH were rechecked at 2–4 week intervals, and oral calcium was adjusted in conjunction with the recheck results. At 6 months of follow-up, two cases of long-term hypoparathyroidism with occasional transient terminal limb numbness appeared in group B. They required long-term oral calcium carbonate (600 mg/dose, 2–3 times/day) and were unable to restore normal sCa and iPTH at 1 year of follow-up, during which sCa values of 1.8–2.0 mmol/l and iPTH values of 0.8–1 mmol/l were monitored.
Discussion
PTC is prone to lymph node metastasis and the central region is often the first site of metastasis, with a 33% rate of metastasis in the central region even in microscopic papillary carcinomas with cN0.8 Aggressive CLND significantly reduces the rate of local recurrence, but may increase postoperative complications such as hypoparathyroidism as manifested by hypocalcemia and/or hypo-iPTHemia.9,10 Current studies have focused on The time frame of iPTH changes is mainly focused on intraoperative to 24 hours postoperatively3–5,11 and few studies have addressed how iPTH and sCa change within 1 month postoperatively. The data and graphs in this study suggest that there is a pattern of recovery of iPTH and sCa after TT+CLND. The iPTH decreased significantly on the POD1 compared with the preoperative level, continued to decrease to the lowest point on the POD3, and showed an increasing trend on POD5 and POD14, with most patients recovering close to preoperative levels on POD30. Because of the intervention of oral ± intravenous calcium, postoperative sCa did not change in line with iPTH, with the lowest values occurring on POD1, rising steadily on POD 3–5, and continuing to rise at POD14, also on POD30 when most patients approached preoperative levels.Most patients had mild or no symptoms of hypocalcemia during hospitalization and were safely discharged in the short term. The four main time points of POD 1, 3–5 days, 2–3 weeks and 1 month are further elaborated below.
Both iPTH and sCa decreased significantly on POD1 relative to the preoperative period. The significant decrease in iPTH was mainly due to impaired parathyroid function caused by surgery, whereas the decrease in calcium was mainly related to the decrease in iPTH, but may also be related to other factors outside of surgery, such as female gender, preoperative vitamin D deficiency, combined Grave’s disease or Hashimoto’s thyroiditis.12 The overall incidence of hypocalcemia ranges from 1.6 to 50%.13 The incidence of transient hypocalcemia in this study was 29.5% (Table 1), which is slightly higher than the results reported in a multicenter study with a large sample, which reported a 27.9% incidence of hypocalcemia after total or near-total thyroidectomy.14 A reasonable explanation is that the patients in this study had increased CLND, which is an independent risk factor for the development of hypocalcemia.9,10,14 The significant decrease in sCa compared to the preoperative period can often induce clinical signs of hypocalcemia in patients, so the morning check-up on the POD1 is particularly important, and patients should be asked about the presence of numbness in the end extremities or around the mouth, must be checked for facial nerve percussion signs (ie Chvostek’s sign), and the feedback of electrolyte and iPTH should be noted. As described in the previous methods section, when patients have sCa ≤1.75 mmol/L or symptomatic hypocalcemia or strong positive Chvostek’s sign, they should be treated with intravenous calcium to minimize exacerbation on top of regular oral calcium + calcitriol. Because intravenous calcium can rapidly increase the sCa levels, 43.7% (80/183) of the patients in this study used intravenous calcium according to the above criteria. The aim was to minimize the symptoms of severe hypocalcemia such as hand and foot twitching, respiratory distress or cardiac arrhythmia, and to maximize patient safety and comfort in the perioperative period. In contrast, the ATA and AACE have an uncertain attitude toward aggressive intravenous calcium4,5 presumably because of the fear of triggering hypercalcemia or increasing the burden of infusion, whereas the results of multiple reviews in this group of patients reveal that not a single case of hypercalcemia has occurred.
There are also few studies reporting the time point at which the nadir of iPTH and serum calcium occurs. Because of the short half-life of iPTH, which is only 3–5 minutes,15 it may be misleading to believe that a trough value of iPTH will occur within 24 hours after surgery.However, this study shows that the lowest value of iPTH after TT+CLND occurs at 3–5 days postoperatively. The implication is that a significant proportion of patients discharged 1–2 days postoperatively will have significant out-of-hospital hypo-iPTHemia if discharge is evaluated on the basis of iPTH and/or calcium values measured intraoperatively or within 24 hours postoperatively. Even if these patients are routinely given oral calcium, they may still be at risk for severe hypocalcemia at about 3–5 days postoperatively, including the aforementioned torsades de pointes, laryngospasm, diaphragmatic spasm, and even arrhythmias affecting cardiac output. This is the main reason why patients seek help in the emergency department or are readmitted to the hospital. Therefore, in patients at high risk of hypoparathyroidism after TT+CLND, it is necessary to extend the hospital stay for observation and monitoring while intensifying calcium supplementation therapy. If the patient chooses to be discharged for observation 1–2 days after the procedure, adequate education and communication should be provided to the patient at the time of discharge. The education should include a high calcium and low phosphorus diet, regular oral calcium, and recognition of signs and clinical manifestations of hypocalcemia. Communication should include how to seek medical help in case of hypocalcemic emergencies, and a good emergency plan to help patients to be informed and avoid doctor-patient disputes.
Figures 1 and 2 show that the iPTH and sCa values at 2 weeks postoperatively did not reach preoperative levels, and both values were still in a period of continued increase. Table 5 shows that of the 99 patients who continued oral calcium at discharge, the percentages of calcium discontinued at 2 weeks, 3 weeks, and 1 month were 17.2% (17/99), 77.8% (77/99), and 5.1% (5/99), respectively, indicating that more than three-quarters of patients discontinued oral calcium at about 3 weeks postoperatively. From the monitored sCa data, oral calcium ± calcitriol for more than 2–3 weeks postoperatively can maintain sCa levels to the maximum extent without either hypocalcemia resulting in emergency events or hypercalcemia. There are currently two views on postoperative calcium supplementation, namely “ parathyroid splinting” and “ parathyroid stress testing”.5 The former emphasizes active calcium supplementation, while the latter advocates no active calcium supplementation without significant hypocalcemia. We believe that both approaches should be implemented in stages, rather than choosing one over the other, as we have done above.The initial period (especially within 2–3 weeks postoperatively) may be a critical period for recovery of impaired parathyroid function, and splinting during this period may not only avoid symptoms of hypocalcemia, but also reduce ischemic and hypoxic damage by reducing the secretory load of the parathyroid glands, which may reduce the risk of long-term hypoparathyroidism.16 The “ parathyroid stress testing” method is started only after 2–3 weeks postoperatively, when the hormone secretion of the parathyroid glands is stimulated by the reduction of exogenous calcium to restart and revive parathyroid function. Of course, the benefits of this approach need to be confirmed by additional studies.It should be mentioned that the autologous parathyroid gland also starts its secretory function only 2–4 weeks after surgery,17 which means that it cannot be relied upon to participate in the regulation of the body’s parathyroid hormones during this period, supporting this staged calcium supplementation strategy.
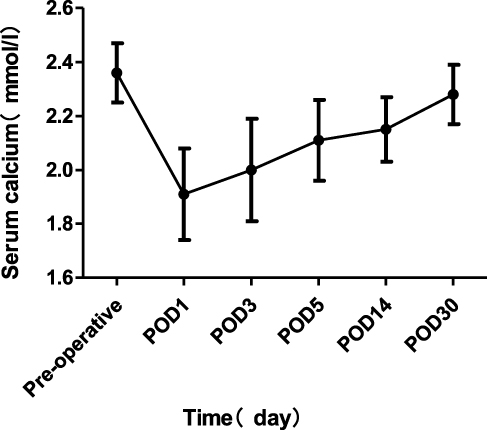 |
Figure 1 Changes in perioperative serum calcium in 115 patients. |
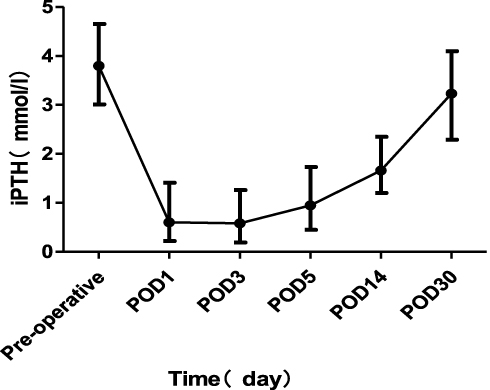 |
Figure 2 Changes in perioperative iPTH in 115 patients. |
By 1 month postoperatively, the vast majority (95%) of patients had stopped taking calcium, and the data showed that both iPTH and sCa were close to preoperative levels. The recovery of iPTH levels meant that maintenance of calcium was not dependent on exogenous calcium. The physician needs to emphasize with the patient the importance of returning to the clinic for follow-up 1 month after surgery. The purpose is multiple: to observe wound recovery; to counsel on the presence or absence of post-discharge hypocalcemia; to learn about regularly monitored sCa, iPTH, and calcium adjustments; to adjust the follow-up calcium and monitoring regimen based on sCa and iPTH at the 1-month postoperative review; to assess whether to supplement iodine 131 nuclear therapy; and to adjust the dose of TSH-suppressing medication. Thereafter, if oral calcium is required for long-term maintenance of TSH suppression therapy, especially in postmenopausal women, its purpose is mainly to prevent osteoporosis,18 which is different from the previous purpose of calcium supplementation.
The subgroup data showed the same trend of decreasing and then increasing calcium and iPTH levels in both subgroups, and the time axis of change was similar to that of the previous large group. However, BCLND is associated with a higher incidence of transient hypoparathyroidism, an increased proportion of patients requiring intravenous calcium, a longer hospital stay, and a higher proportion of patients requiring oral calcium at discharge compared with UCLND. Although there was no statistical difference in the incidence of long-term parathyroidism between the two subgroups, the 2 cases of permanent hypoparathyroidism (PH) were both seen in the BCLND group. The incidence of PH after bilateral thyroid surgery has been reported in the literature to be in the range of 1-3% and in experienced surgeons to be in the range of 1%-2%,2 which in this study was 1.1% (2/183). Therefore, “TT + BCLND” is a high-risk procedure even for experienced specialists. It is recommended that at least 2 parathyroid glands should be identified and preserved during bilateral thyroid surgery to avoid hypoparathyroidism.19 In this study, 99.5% (182/183) of patients had 2 or more parathyroid glands preserved in situ, which is the key to ensure safe implementation of “TT+CLND”.
This study is a retrospective study, and selection bias and recall bias inevitably interfere. In addition, for patients presenting with hypoparathyroidism, there are few data on iPTH test values between 5 and 14 days postoperatively, and this study failed to clarify the specific time point at which iPTH began to rise. It would be more helpful and informative for the dynamic management of patients if prospective studies could be promoted to clarify the time of inflection point appearance.
Conclusion
In patients with hypoparathyroidism after TT with CLND for PTC, iPTH and sCa levels tend to decrease and then increase at different time points within 1 month after surgery, and this trend can be interpreted as a pattern of recovery of parathyroid function. Understanding this pattern is of great value to the surgeon in choosing the surgical procedure, individualizing calcium supplementation, and communicating effectively with the patient, which will help the patient to pass the perioperative period safely and comfortably and improve the quality of life in the short and long term. In addition, compared to “TT + UCLND”, “TT + BCLND” increases the risk of hypoparathyroidism and requires more aggressive postoperative monitoring and calcium supplementation in the short term.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The protocol of this research was approved by the ethics committee of the Cancer Hospital of FuJian Medical University. All methods were performed in accordance with the Helsinki Declaration. All data were used retrospectively, so the committee waived the need for written informed consent. All clinical data were anonymized for analysis.
Disclosure
Xi-Yu Yao and Yan Zhou are co-first authors for this study. The authors declare no financial or non-financial competing interests.
References
1. Bollerslev J, Rejnmark L, Marcocci C, et al. European Society of Endocrinology Clinical Guideline: treatment of chronic hypoparathyroidism in adults. Eur J Endocrinol. 2015;173(2):G1–G20. doi:10.1530/EJE-15-0628
2. Barczyński M, Gołkowski F, Nawrot I. Parathyroid transplantation in thyroid surgery. Gland Surg. 2017;6(5):530–536. doi:10.21037/gs.2017.06.07
3. Chang JW, Park KW, Jung SN, Liu L, Kim SM, Koo BS. The most reliable time point for intact parathyroid hormone measurement to predict hypoparathyroidism after total thyroidectomy with central neck dissection to treat papillary thyroid carcinoma: a prospective cohort study. Eur Arch Otorhinolaryngol. 2020;277(2):549–558. doi:10.1007/s00405-019-05693-1
4. Orloff LA, Wiseman SM, Bernet VJ, et al. American thyroid association statement on postoperative hypoparathyroidism: diagnosis, prevention, and management in adults. Thyroid. 2018;28(7):830–841. doi:10.1089/thy.2017.0309
5. Stack BC
6. Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association Management Guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American thyroid association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26(1):1–133. doi:10.1089/thy.2015.0020
7. Shaha AR, Migliacci JC, Nixon IJ, et al. Stage migration with the new American Joint Committee on Cancer (AJCC) staging system (8th edition) for differentiated thyroid cancer. Surgery. 2019;165(1):6–11. doi:10.1016/j.surg.2018.04.078
8. Liu LS, Liang J, Li JH, et al. The incidence and risk factors for central lymph node metastasis in cN0 papillary thyroid microcarcinoma: a meta-analysis. Eur Arch Otorhinolaryngol. 2017;274(3):1327–1338. doi:10.1007/s00405-016-4302-0
9. Zhao W, You L, Hou X, et al. The effect of prophylactic central neck dissection on locoregional recurrence in papillary thyroid cancer after total thyroidectomy: a systematic review and meta-analysis: pCND for the locoregional recurrence of papillary thyroid cancer. Ann Surg Oncol. 2017;24(8):2189–2198. doi:10.1245/s10434-016-5691-4
10. Chen L, Wu YH, Lee CH, Chen HA, Loh EW, Tam KW. Prophylactic central neck dissection for papillary thyroid carcinoma with clinically uninvolved central neck lymph nodes: a systematic review and meta-analysis. World J Surg. 2018;42(9):2846–2857. doi:10.1007/s00268-018-4547-4
11. Mazotas IG, Wang TS. The role and timing of parathyroid hormone determination after total thyroidectomy. Gland Surg. 2017;6(Suppl1):S38–S48. doi:10.21037/gs.2017.09.06
12. Edafe O, Antakia R, Laskar N, Uttley L, Balasubramanian SP. Systematic review and meta-analysis of predictors of post-thyroidectomy hypocalcaemia. Br J Surg. 2014;101(4):307–320. doi:10.1002/bjs.9384
13. Reeve T, Thompson NW. Complications of thyroid surgery: how to avoid them, how to manage them, and observations on their possible effect on the whole patient. World J Surg. 2000;24(8):971–975. doi:10.1007/s002680010160
14. Puzziello A, Rosato L, Innaro N, et al. Hypocalcemia following thyroid surgery: incidence and risk factors. A longitudinal multicenter study comprising 2631 patients. Endocrine. 2014;47(2):537–542. doi:10.1007/s12020-014-0209-y
15. Leiker AJ, Yen TW, Eastwood DC, et al. Factors that influence parathyroid hormone half-life: determining if new intraoperative criteria are needed. JAMA Surg. 2013;148(7):602–606. doi:10.1001/jamasurg.2013.104
16. Sitges-Serra A. The PGRIS and parathyroid splinting concepts for the analysis and prognosis of protracted hypoparathyroidism. Gland Surg. 2017;6(Suppl1):S86–S93. doi:10.21037/gs.2017.07.16
17. Lo CY, Tam SC. Parathyroid autotransplantation during thyroidectomy: documentation of graft function. Arch Surg. 2001;136(12):1381–1385. doi:10.1001/archsurg.136.12.1381
18. Grani G, Ramundo V, Verrienti A, Sponziello M, Durante C. Thyroid hormone therapy in differentiated thyroid cancer. Endocrine. 2019;66(1):43–50. doi:10.1007/s12020-019-02051-3
19. Thomusch O, Machens A, Sekulla C, Ukkat J, Brauckhoff M, Dralle H. The impact of surgical technique on postoperative hypoparathyroidism in bilateral thyroid surgery: a multivariate analysis of 5846 consecutive patients. Surgery. 2003;133(2):180–185. doi:10.1067/msy.2003.61
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.