Back to Journals » Clinical Interventions in Aging » Volume 19
Is Shock Wave Application Effective on Various Chronic Wounds in the Geriatric Population? Preliminary Clinical Study
Authors Dymarek R ![]() , Kuberka I, Walewicz K
, Kuberka I, Walewicz K ![]() , Taradaj J
, Taradaj J ![]() , Rosińczuk J, Sopel M
, Rosińczuk J, Sopel M ![]()
Received 5 November 2023
Accepted for publication 1 April 2024
Published 30 April 2024 Volume 2024:19 Pages 665—679
DOI https://doi.org/10.2147/CIA.S448298
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Robert Dymarek,1 Izabela Kuberka,2 Karolina Walewicz,3 Jakub Taradaj,4 Joanna Rosińczuk,5 Mirosław Sopel6
1Department of Physiotherapy, Wroclaw Medical University, Wroclaw, Poland; 2Division of Anaesthetic and Surgical Nursing, Wroclaw Medical University, Wroclaw, Poland; 3Medical Institute, Jan Grodek State University in Sanok, Sanok, Poland; 4Institute of Physiotherapy and Health Sciences, The Jerzy Kukuczka Academy of Physical Education in Katowice, Katowice, Poland; 5Division of Internal Medicine Nursing, Wroclaw Medical University, Wroclaw, Poland; 6Faculty of Medicine, Wrocław University of Science and Technology, Wroclaw, Poland
Correspondence: Robert Dymarek, Department of Physiotherapy, Wroclaw Medical University, Chałubińskiego 3, Wroclaw, 50-368, Poland, Tel +48 71 784 28 15, Email [email protected]
Purpose: Extracorporeal shock wave therapy (ESWT) is a beneficial adjunct modality for chronic wounds. Limited research has been conducted on pressure ulcers (PUs), while the majority of studies have focused on diabetic foot ulcers (DFUs) and venous leg ulcers (VLUs). This study aimed to evaluate the short-term effects of radial ESWT in older adults with chronic wounds.
Patients and Methods: This study involved a total of 31 wounds: PUs (n=22), VLUs (n=7), and DFUs (n=2). A single radial ESWT was performed with 300 + 100 shocks per cm2, pressure of 2.5 bar, energy of 0.15 mJ/mm2, and frequency of 5 Hz. Assessments using digital planimetry and clinical methods, utilizing the Wound Bed Score (WBS) and the Bates-Jansen Wound Assessment Tool (BWAT) were performed before the radial ESWT application (M0) and one week after (M1).
Results: A significant wound decrease in planimetry was noted (pre-ESWT vs post-ESWT), with wound area from 9.4 cm2 to 6.2 cm2, length from 6.4 cm to 3.9 cm, and width from 2.8 cm to 2.1 cm (p< 0.001). Additionally, a substantial clinical improvement was noted in both the WBS with a 31.25% increase and the BWAT with a 20.00% increase (p< 0.001). It was also found a significant correlation between the planimetric and clinical outcomes for both tools: WBS (r=− 0.446, p=0.012) and BWAT (r=0.327, p=0.073).
Conclusion: The ESWT application yields substantial immediate clinical effects that support the healing of chronic wounds in older adults. Even a single ESWT session can prove to be clinically effective and beneficial in the management of chronic wounds.
Keywords: extracorporeal shockwave therapy, wound healing, older adults, clinical assessment, pressure ulcer, venous ulcer, diabetic foot ulcer
Introduction
Chronic wounds are characterized by impaired healing and delayed tissue repair resulting in long-term anatomical and functional disturbances within the skin.1 Chronic wounds result in severe impairment of recovery and disruption of the normal sequence of healing phases and are persistent to the use of conventional treatments.2 According to the etiological classification, diabetic foot ulcers (DFUs), venous leg ulcers (VLUs) and pressure ulcers (PUs) are most common chronic wounds of the skin and soft tissue.3
Patient suffering from chronic wounds may lose independent functioning and experience a significant deterioration in quality of life.4,5 These problems become more significant in patients with chronic wounds and can lead to several complications resulting in disability, loss of independent functioning, the need for institutional care and, in extreme cases, even premature death.6 The cost to health systems of medical care and inability to work for people with chronic wounds is about $10 billion a year, and it is likely that most of this cost is attributable to wound care for the older population over the age of 65.7
The vast majority of chronic wounds are associated with conditions more typically found in the elderly, such as arteriosclerosis, venous insufficiency, hypertension, or diabetes and metabolic disorders. In addition, a growing number of older adults are at risk due to surgical procedures, with potential complications in wound healing or immobilization causing pressure injury.8,9
According to available data, 60–70% of all reported PUs occur in older adults over the age of 65 years, including especially geriatric ward patients with an incidence of 8–20%.10 It should be emphasized that VLUs are most common chronic wounds among elderly people with associated chronic venous insufficiency and represent 60–80% of all lower leg ulcers in the course of venous disease.11 DFUs are one of the diabetic complications and its worldwide prevalence among diabetic patients ranges between 3–13%.12 Moreover, the 5-year mortality rate for the presence of DFUs and ischemic ulcers is higher than for some cancers.13
The management of chronic wounds is a complex process dependent on the intricate synergy of many highly regulated factors which is focused tissue remodelling and regeneration based on promotion of re-epithelialization process.9 The therapeutic management and systematic approach for assessing chronic wounds is still based on the TIME principles.14
Contemporary wound care modalities and strategies being the gold standard for the treatment chronic wounds, can be effectively enhanced by a variety of biophysical methods.15,16 The comprehensive wound care team includes physicians, nurses, podiatrists, certified diabetes educators, registered dietitians and prosthetists or orthotists as well as specialized physiotherapists.17 Physiotherapeutic modalities have some potential to be implemented to comprehensive and interprofessional wound care management.18,19
The clinical utility of a few biophysical methods including electrical stimulation or ultrasound therapy has been confirmed.20 However, the effects of low-level laser therapy for improving healing process has not been proved.21 The remaining methods with documented experience-based efficiency can be involved, such as pulsed lavage with suction, concurrent optical and magnetic stimulation, hyperbaric oxygen therapy, ultraviolet C therapy, polarized light therapy or far-infrared therapy.22–25
One of potentially valuable biophysical agent is extracorporeal shock wave therapy (ESWT). It harnesses the mechanical energy generated by acoustic waves to induce biological responses within the treated tissues.26 One of the primary mechanisms of action involves generating mechanical stress that triggers cellular responses. The mechanical forces generated by ESWT are believed to activate various cellular signaling pathways, leading to increased production of growth factors, cytokines, and other molecules involved in tissue repair and regeneration as mechanotransduction phenomena.27 Additionally, ESWT is thought to modulate inflammation, enhance neovascularization, and promote the recruitment of cells proliferation to the injured site. The mechanical impact of shock waves on cellular structures may trigger cellular processes that contribute to tissue healing, making ESWT a promising therapeutic approach for conditions ranging from musculoskeletal injuries to chronic wound healing.28
Previous studies demonstrated that ESWT may be implemented for treating wounds, specifically of those with chronic etiology like DFUs and VLUs.29,30 The fact is that the usefulness of the ESWT for PU’s remains poorly documented. There is only one cross-over randomized controlled trial (RCT) study by Larking et al31 who involved a limited group of nine patients and our previous RCT among 40 patients.32 Also, two case reports published in 2020 by Duan et al33 and Kang et al34 which reported a beneficial effect after ESWT on PUs can be found.
Therefore, this prospective uncontrolled interventional study was performed to observe short-term clinical outcomes after one session of radial ESWT delivered to etiologically different chronic wounds. Also, the correlations between the planimetric and clinical assessments as well as comparisons of study outcomes between groups in terms of wound etiology and location were conducted.
Materials and Methods
Design and Settings
The study protocol received approval from the Bioethics Committee of Wroclaw Medical University in Poland (approval no. KB–632/2016). The study was conducted in accordance with Good Clinical Practice guidelines and the 2004 revision of the Declaration of Helsinki. The study project was prospectively registered at the Clinical Trials Registry Platform (no. ACTRN12617000075381).
This prospective interventional study was carried out between January 2017 and December 2020 in two facilities: an inpatient center for long-term care and an outpatient clinic specializing in wound care, both located in Wroclaw, Poland. The study is identified by the acronym SHOWN (SHOck Waves in wouNds).
Qualification Procedure
This study included patients who met all of the following criteria: (1) skin wounds with pressure, venous, or diabetic etiology; (2) wounds with a duration exceeding 3 months; (3) wounds classified as class II or III according to the Centers for Disease Control and Prevention (CDC); (4) the absence of health conditions contraindicating the application of ESWT; and (5) patient’s informed consent obtained prior to the study commencement. Patients were excluded if they met any of the following criteria: (1) clinical wound infection confirmed in microbiological tests; (2) wounds classified as class I or IV according to CDC; (3) patient non-compliance with the study protocol; and (4) patients with existing contraindications to ESWT were also excluded from participation in the study.
Patients’ Characteristics
At the outset, the study group comprised 33 patients; however, 14 patients were excluded from the study for not meeting the inclusion criteria. Ultimately, 19 patients with a total of 31 chronic wounds (22 PUs, 7 VLUs, and 2 DFUs) were included in the study and qualified for ESWT treatment. Detailed general and clinical characteristics of the study participants are provided in Tables 1 and 2, respectively.
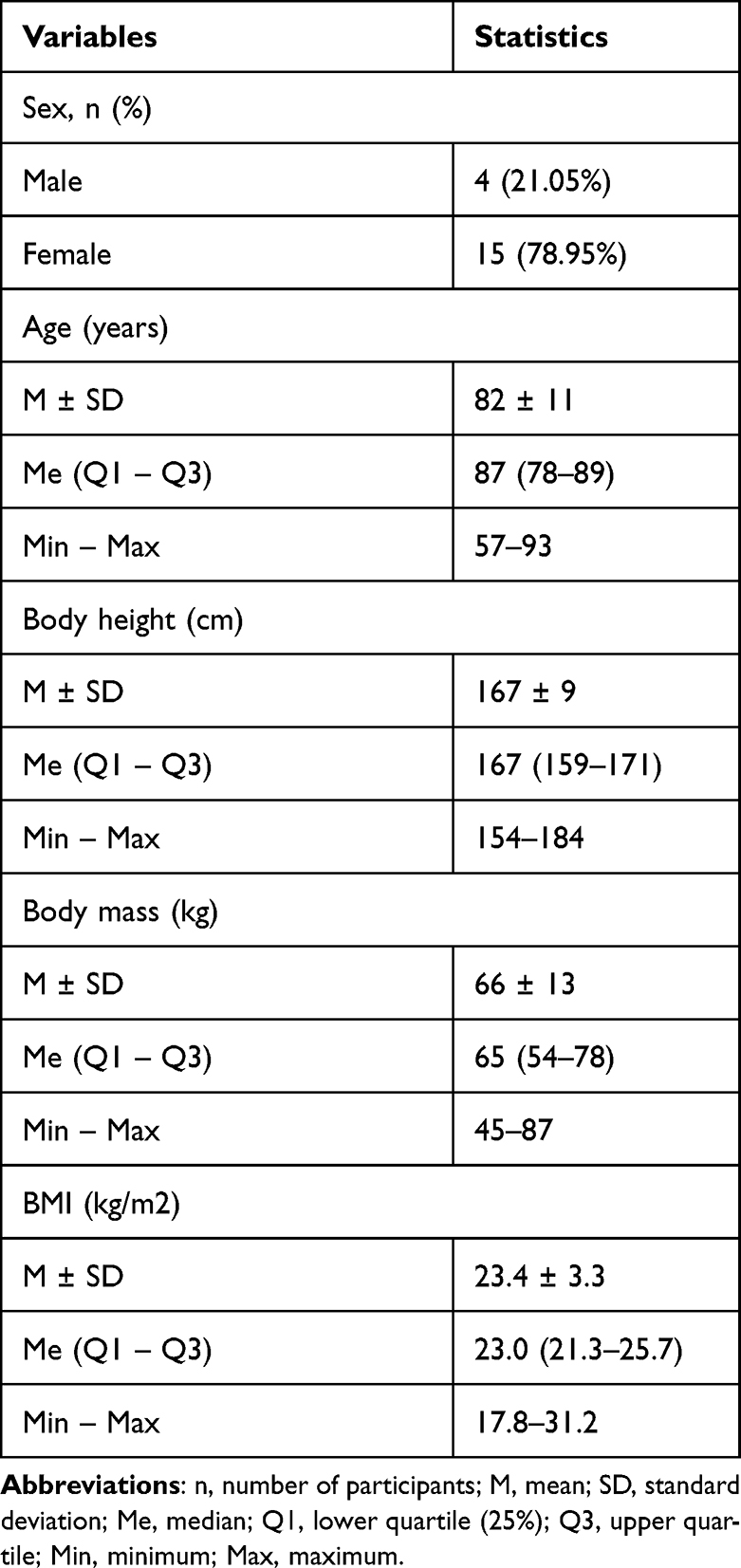 |
Table 1 Patients’ Characteristics Including Demographic Items (n=19) |
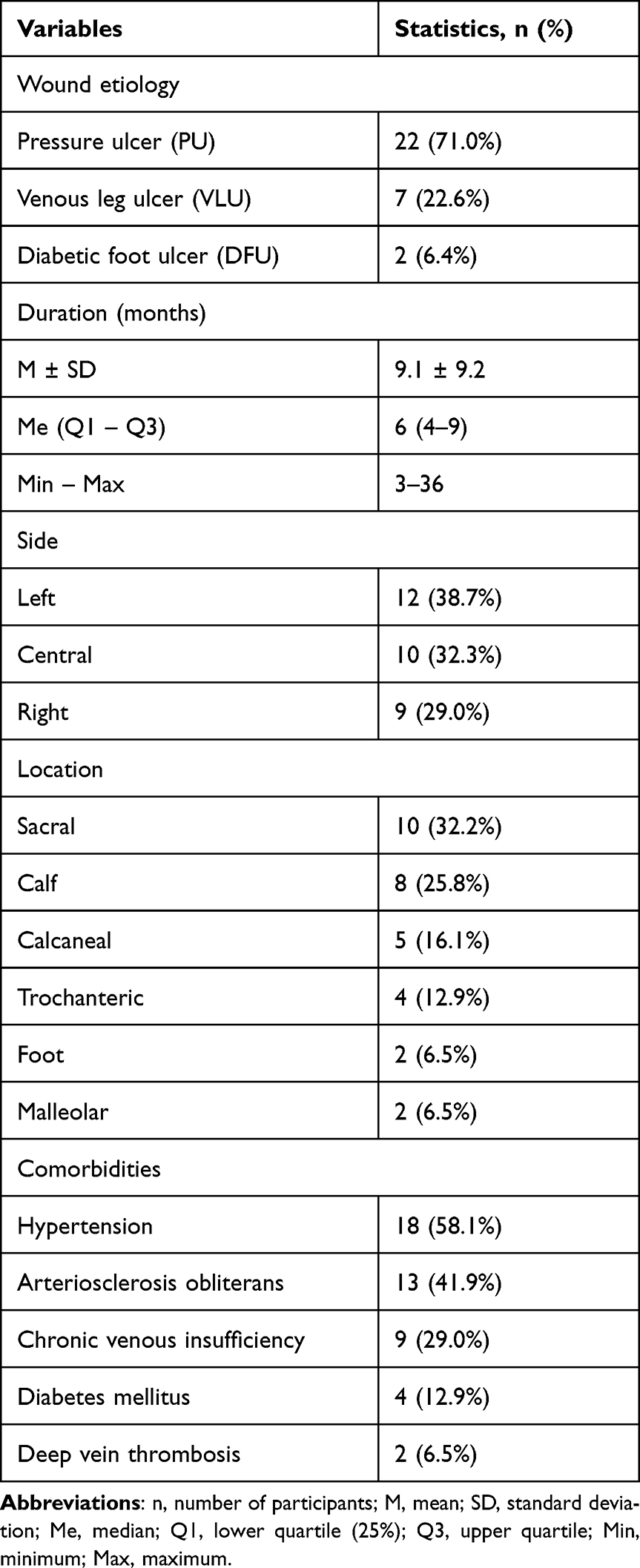 |
Table 2 Patients’ Characteristics Including Clinical Items (n=19) |
Therapeutic Intervention
The therapeutic session was conducted using a radial ESWT applicator (Cellactor® SC1, Storz Medical, Switzerland). The methodology for ESWT ensured safe and sterile conditions as follows: (1) a sterile ultrasound gel was used as a contact medium directly on the entire wound surface and its edges, (2) a sterile barrier in the form of polyurethane film was placed directly over the wound, previously covered by the ultrasound gel, and (3) the same ultrasound gel was applied on top of the film as a second layer to ensure full contact of the ESWT transducer with the tissues.
The delivery of the procedure should be conducted meticulously and with the use of sterile materials. During the ESWT session, the applicator head makes direct contact with the wound, facilitated by sterile ultrasound gel and a sterile polyurethane film. ESWT application should commence from the wound’s edges, moving gently towards the center while meticulously treating the entire wound surface. Special attention is necessary when working near any bone structure, which should be avoided. Figure 1 provides an illustration of a treatment session employing radial ESWT. The ESWT parameters were as follows: 300 baseline pulses + 100 additional pulses per square centimeter, a pulse pressure of 2.5 bars, a pulse energy of 0.15 mJ/mm2, and a pulse frequency of 5 Hz. Local anesthesia was not used, and the procedure was conducted without causing pain. Any adverse events and side effects were carefully observed and reported during the ESWT procedures.
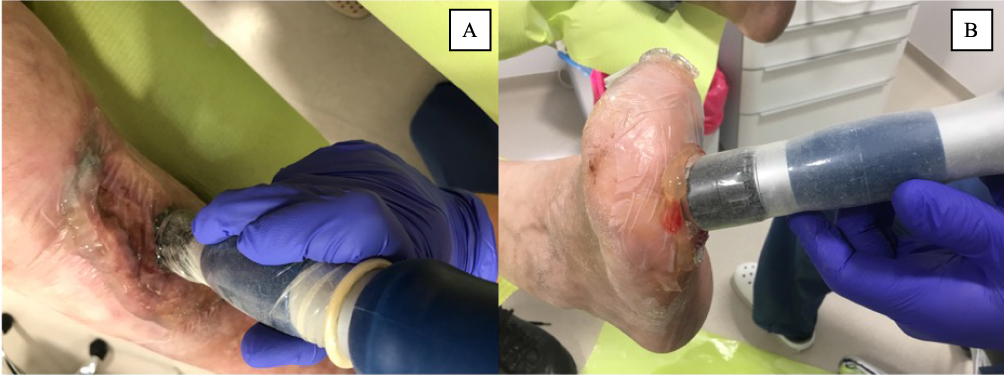 |
Figure 1 Example of a treatment session using radial ESWT for a VLU (A) and DFU (B). Abbreviations: ESWT, extracorporeal shockwave therapy; VLU, venous leg ulcer; DFU, diabetes foot ulcer. |
All patients continued their standard wound care procedures, including proper wound care and hygiene, individually selected and standardized dressings, using pressure relief mattresses and appropriate positioning to optimize healing conditions. These standardized and evidence-based practices adhered to the European Pressure Ulcer Advisory Panel (EPUAP) recommendations for PUs management.
Outcomes Measurements
The primary objective of this study was to demonstrate an objective improvement in selected parameters of chronic wounds through planimetric assessment. The secondary goal was to observe enhancements in the clinical properties of chronic wounds using validated tools. The tertiary aim was to establish the relationship between wound parameters and clinical evaluation and to compare study outcomes between groups based on wound etiology and location. Both planimetric and clinical measurements were conducted immediately before the ESWT application (M0) and one week following the ESWT procedure (M1).
A digital planimetry method using the Swift Wound application on an iPhone 7 Plus (Apple Inc., Cupertino, California, United States) smartphone was employed to measure the metric parameters of chronic wounds. This application is known for its accuracy and reliability in creating comprehensive documentation of the wound healing process.35 The wound measurements exhibit a very low error level (less than 0.5%), and high inter-rater reliabilities (ICC = 0.97–1.00).35
The Wound Bed Score (WBS) is a standardized questionnaire used to evaluate the clinical status of soft tissue wounds. It comprises eight components represented by the acronym BEDSCORE, which assess the following wound parameters: Black eschar, Eczema or dermatitis, Depth, Scarring, Color, Edema or swelling, Resurfacing epithelium, and Exudate amount. Each component is assigned a score within the 0–2 range, resulting in a total score that falls between 0 and 16 points. A higher WBS score signifies a more favorable clinical condition of the wound. The WBS serves as a valuable tool in both research and clinical settings, aiding in the optimization of treatments and the exploration of new treatment options.36
The Bates-Jansen Wound Assessment Tool (BWAT) is another standardized instrument comprising 13 components. It assesses various wound parameters, encompassing nine factors: Size, Depth, Edges, Undermining, Type of necrotic tissue, Amount of necrotic tissue, Exudate type, Exudate amount, Skin color around the wound, as well as Peripheral tissue edema, Tissue sclerosis around the wound, Granulation tissue, and Epithelialization. The first nine items are scored within a range of 1–5 points, while the last four items are scored from 0 to 5 points each. The total BWAT score falls between 9 and 65 points, with a lower score indicating a more favorable clinical wound condition. The BWAT demonstrates a level of reliability ranging from moderate to high.37
Statistical Analysis
Statistical analysis was performed using STATISTICA v. 13.3 (TIBCO Software Inc., Tulsa, USA). For all quantitative parameters (age, wound area, etc.), the normal distribution was checked using the Shapiro–Wilk test. The level of significance was set at p < 0.05. The mean (M), standard deviation (SD), median (Me), lower (Q1), and upper (Q3) quartiles and minimum (Min) and maximum (Max) were calculated for all measurable parameters. The significance of differences in the mean values of quantitative variables in two independent groups (PU vs VLU+DFU) for parameters with a distribution significantly different from normal or with heterogeneous variances was tested using the Mann–Whitney U-test. For dependent variables (pre-ESWT and post-ESWT), the Wilcoxon test was applied. Parametric correlations (Pearson’s r) were used to assess the significance and strength of relationships between quantitative variables. The results were considered significant for p < 0.05 and highly significant for p < 0.001.
Results
Patients’ Characteristics
The study population consisted of 19 patients (15 females and 4 males) with a mean age of 82 ± 11 years and a mean body mass index (BMI) of 23.4 ± 3.3 kg/m2. Detailed general patient characteristics are provided in Table 1. A total of 31 chronic wounds were identified (22 PUs, 7 VLUs, and 2 DFUs). The mean wound duration was 9.1 ± 9.2 months. Most of the wounds were located on the left side (n=12, 38.7%), with a majority situated on the sacral region (n=10, 32.2%). All patients had comorbidities, including hypertension (n=18, 58.1%), arteriosclerosis obliterans (n=13, 41.9%), chronic venous insufficiency (n=9, 29.0%), diabetes mellitus (n=4, 12.9%), and deep vein thrombosis (n=2, 6.5%). Detailed patient clinical characteristics are presented in Table 2.
Wounds’ Size
After completing the study, it was observed that a single ESWT session led to a significant and immediate improvement in wound healing parameters. There was a significant reduction in wound metric parameters: a reduction in the mean wound area from 9.4 ± 9.1 cm2 to 6.2 ± 7.1 cm2 (a difference of 3.2 ± 2.6 cm2, p<0.001), a reduction in the mean wound length from 6.4 ± 2.7 cm to 3.9 ± 2.8 cm (a difference of 0.7 ± 0.6 cm, p<0.001), and a reduction in the mean wound width from 2.8 ± 1.7 cm to 2.1 ± 1.5 cm (a difference of 0.7 ± 0.4 cm, p<0.001). Similar improvements were observed for PUs in all tested planimetric parameters (p<0.001). Detailed results are presented in Table 3. Examples of radial ESWT application effects using planimetric assessment are summarized in Figure 2.
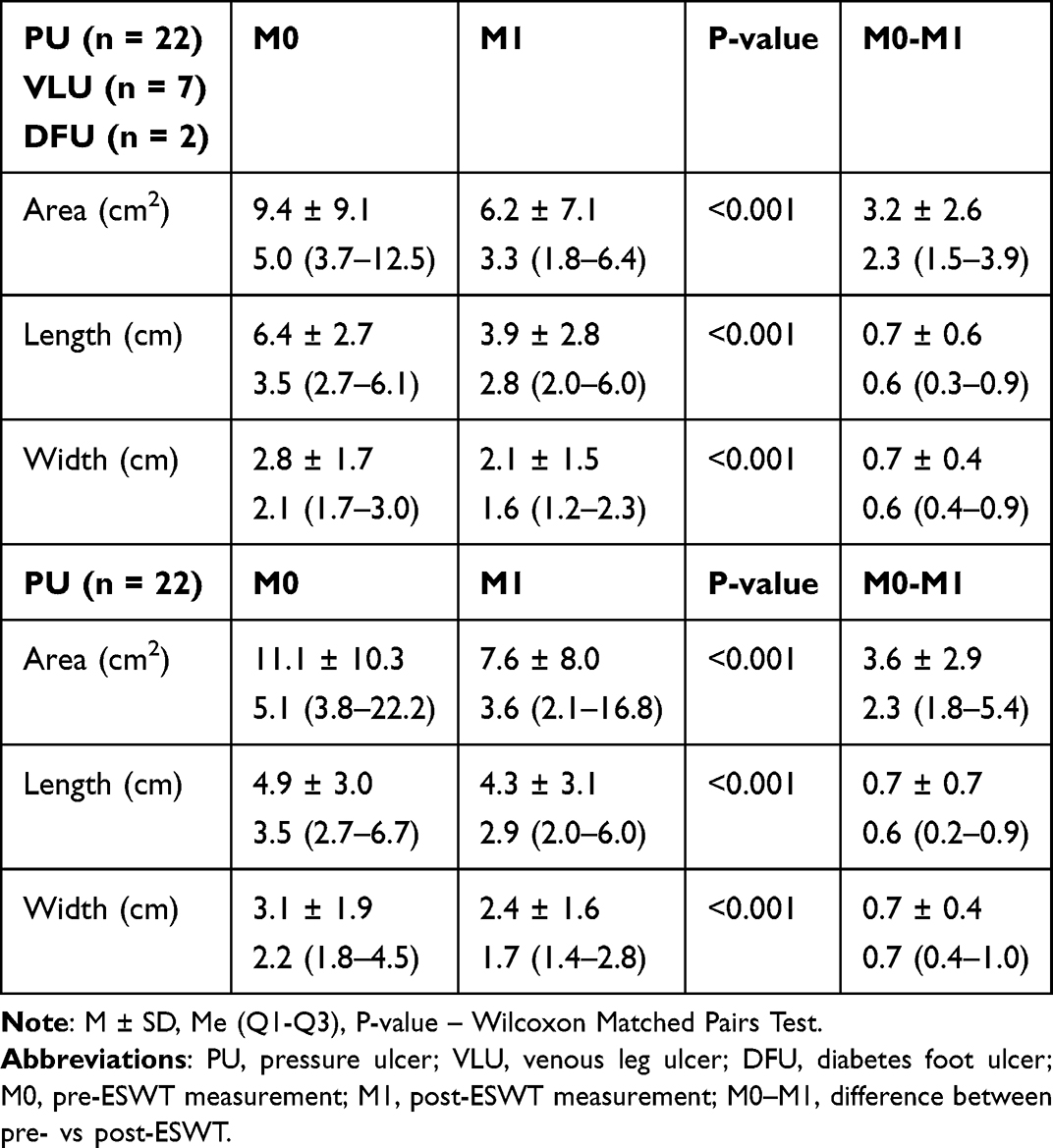 |
Table 3 Planimetric Results Prior-ESWT and Post-ESWT for All Wounds (n=31) and PUs Alone (n=22) |
 |
Figure 2 Example of planimetric effects of radial ESWT for a patient with a PU (A), VLU (B), and DFU (C). Abbreviations: ESWT, extracorporeal shockwave therapy; PU, pressure ulcer; VLU, venous leg ulcer; DFU, diabetes foot ulcer. |
Wounds’ Condition
There was a significant beneficial effect on the clinical condition of the wound when considering the pre- and post-ESWT comparison. The WBS score improved significantly from 4.6 ± 2.8 to 10.4 ± 3.6 points, indicating a better clinical condition of the wound, with an improvement of 31.25% (p<0.001). The BWAT score also showed a significant enhancement, improving from 43.8 ± 7.9 to 30.7 ± 7.5 points, representing a better clinical condition by 20.00% (p<0.001). Similar improvements were observed for PUs in terms of clinical evaluation, with significant improvements in both the WBS (p<0.001) and BWAT (p<0.001) scores. Detailed results are presented in Table 4.
 |
Table 4 Clinical Results Using the WBS and BWAT Results Prior-ESWT and Post-ESWT for All Wounds (n = 31) and PUs Alone (n=22) |
Selected Correlations
The strongest positive correlation was observed between the wound width parameter and the BWAT assessment (r=0.472, p<0.001). Both wound assessment models—the WBS and BWAT—demonstrate relatively weak correlations for small wounds up to 5 cm2 but provide better estimations for larger wounds above 5 cm2. Detailed results are presented in Table 5.
 |
Table 5 Correlations Between Clinical Wound Assessment Using the WBS and BWAT and Their Metric Parameters Following the Planimetric Assessment |
A statistically significant correlation was observed between the changes in the wound surface area and the clinical assessment for both WBS and BWAT scores. There was a strong negative correlation between the wound area and WBS score (r=−0.367, p=0.003), as well as a strong positive correlation between the wound surface area and BWAT score (r=0.368, p=0.003). Similar results were obtained for correlations after ESWT treatment for both the WBS (r=−0.446, p=0.012) and BWAT (r=0.327, p=0.073). Detailed results are provided in Figure 3.
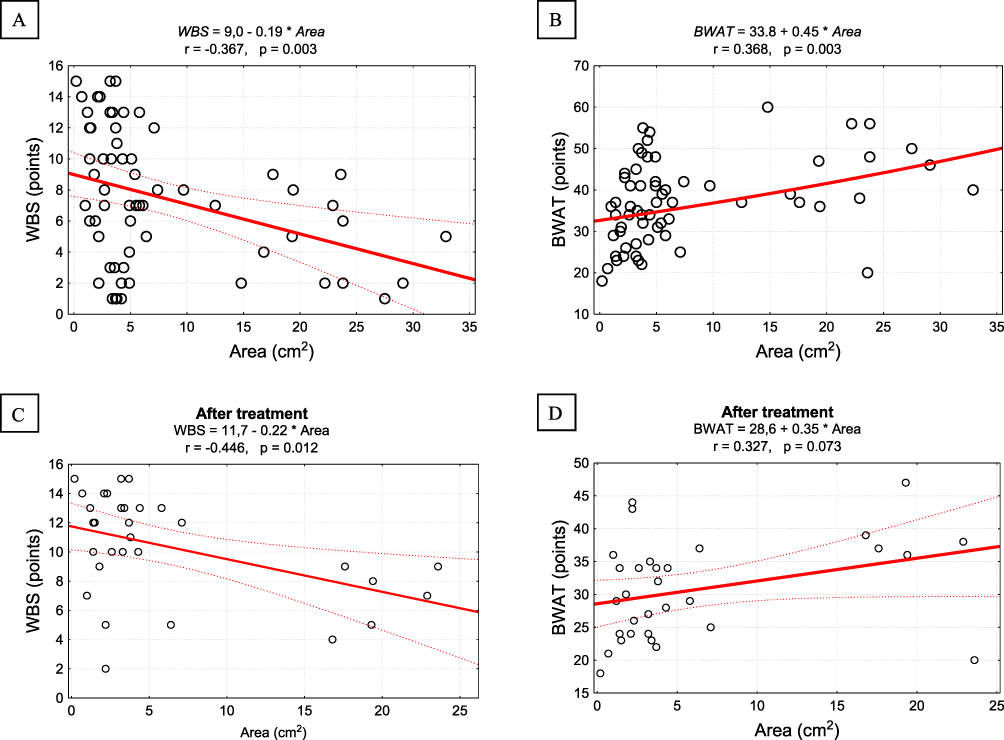 |
Figure 3 Correlation diagrams for clinical wound assessment using the WBS and BWAT with the wound area before and after ESWT (A and B) and separately after ESWT only (C and D). Abbreviations: WBS, Wound Bed Score; BWAT, Bates-Jansen Wound Assessment Tool. Notes: Pearson r correlation coefficients and linear regression equations. |
A statistically significant and strong negative correlation was observed for both the WBS and BWAT in terms of clinical wound evaluation (r=−0.892, p<0.001). This correlation was also confirmed for the WBS and BWAT during the pre-ESWT (r=−0.807, p<0.001) and post-ESWT (r=−0.825, p<0.001) assessments. Detailed results are shown in Figure 4.
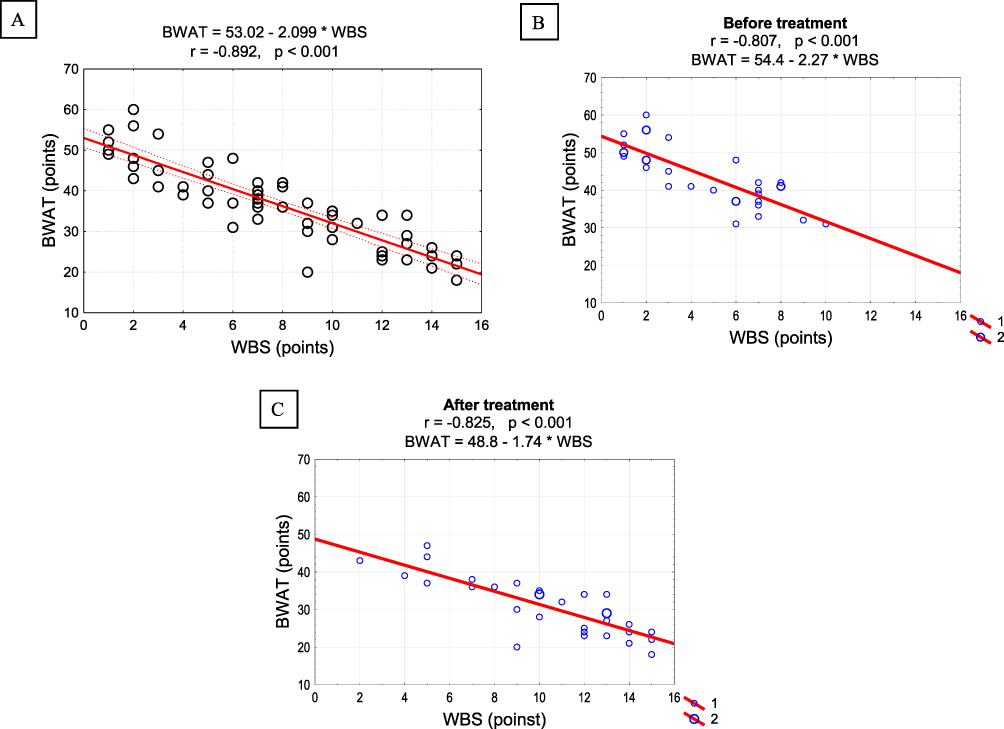 |
Figure 4 Correlation diagram for clinical wound assessment using the WBS and BWAT overall (A) and separately before and after ESWT (B and C). Abbreviations: WBS, Wound Bed Score; BWAT, Bates-Jansen Wound Assessment Tool. Notes: Pearson r correlation coefficients and linear regression equations. |
Selected Comparisons
It was observed that the therapeutic effect of ESWT (the difference between M0 and M1) for wounds with different etiologies (PU vs VLU+DFU) was statistically significant only for the BWAT score (14 vs 9 points, p<0.031). The differences in the WBS were found to be statistically insignificant (p=0.913). Detailed results are presented in Figure 5. Furthermore, there was no statistically significant difference in the changes in the therapeutic effect of ESWT (the difference between M0 and M1) with respect to the anatomical location of the wound in terms of clinical evaluation using both the WBS (p=0.187) and BWAT (p=0.215). Detailed results are provided in Figure 6.
 |
Figure 5 Summary of therapeutic effect for clinical wound assessment using the WBS (A) and BWAT (B) in terms of the groups of wounds of different etiology. Abbreviations: PU, pressure ulcer; VLU, venous leg ulcer; DFU, diabetes foot ulcer; WBS, Wound Bed Score; BWAT, Bates-Jansen Wound Assessment Tool. Notes: P-value: Mann–Whitney U-test; Wound etiology: PUs (n=22) and VLUs with DFUs (n=9).WBS PU: Me = 5; Q1 = 3; Q3 = 9 BWAT PU: Me = 14; Q1 = 9; Q3 = 19.WBS VLU+DFU: Me = 5; Q1 = 5; Q3 = 6 BWAT VLU+DFU: Me = 8; Q1 = 7; Q3 = 12. |
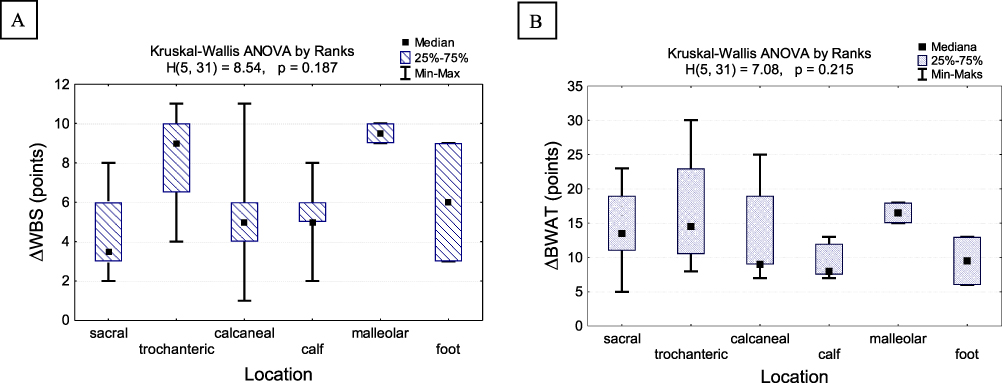 |
Figure 6 Summary of therapeutic effect for clinical wound assessment using the WBS (A) and BWAT (B) in terms of the groups of wounds with different anatomical locations. Abbreviations: PU, pressure ulcer; VLU, venous leg ulcer; DFU, diabetes foot ulcer; WBS, Wound Bed Score; BWAT, Bates-Jansen Wound Assessment Tool. Notes: Kruskal–Wallis ANOVA test; Wound location: sacral (n=10), calf (n=8), calcaneal (n=5), trochanteric (n=4), foot (n=2), and malleolar (n=2).WBS sacral: Me = 3.5; Q1 = 3; Q3 = 6 BWAT sacral: Me = 13.5; Q1 = 11; Q3 = 19WBS trochanteric: Me = 9; Q1 = 6.5; Q3 = 10 BWAT trochanteric: Me = 14.5; Q1 = 10.5; Q3 = 23WBS calcaneal: Me = 5; Q1 = 4; Q3 = 6 BWAT calcaneal: Me = 9; Q1 = 9; Q3 = 19WBS calf: Me = 5; Q1 = 5; Q3 = 6 BWAT calf: Me = 8; Q1 = 7.5; Q3 = 1WBS malleolar: Me = 9.5; Q1 = 9; Q3 = 10 BWAT malleolar: Me = 16.5; Q1 = 15; Q3 = 18WBS foot: Me = 6; Q1 = 3; Q3 = 9 BWAT foot: Me = 9.5; Q1 = 6; Q3 = 13. |
Discussion
This study highlights the potential for favorable effects following just one session of radial ESWT, indicating a rapid onset of benefits. Immediate reductions in key planimetric parameters, such as wound area, length, and width, were observed. Additionally, there was a notable enhancement in the clinical status of the wounds, as assessed by validated scales like WBS and BWAT. Furthermore, the study establishes a correlation between wound surface area and clinical assessment using WBS and BWAT. A strong negative correlation was noted between wound surface area and WBS score, while a robust positive correlation was identified between wound surface area and BWAT score. This implies that a decrease in wound surface area is associated with an improvement in the clinical condition of the wound, reflected by a higher WBS score and a lower BWAT score.
So far, there have been limited reports on the use of ESWT in wound management. The majority of studies with well-documented RCT designs have focused on DFUs,38–44 with only one study addressing VLUs45 and PUs.31 Furthermore, in the aforementioned trials, both focused and defocused (planar) ESWT were applied as treatment interventions. Drawing comparisons with prevailing literature highlights the scarcity of rigorous RCTs focused on ESWT in PUs.31 Our earlier parallel RCT demonstrated the superiority of radial ESWT, presenting not just improvements but significant strides in planimetric measures and clinimetric outcomes. In contrast to the conventional, our study stands as a torchbearer, injecting a much-needed jolt of evidence into the relatively unexplored realm of radial ESWT in wound care.32
Considering anecdotal evidence from case reports, particularly those emanating from Chinese researchers,33,34 lends weight to our unconventional approach. While these narratives remain anecdotal, they echo our findings of rapid wound closure and effective management. Our study, in the face of skepticism, emerges as a bold protagonist, providing tangible, real-world evidence of the impact of radial ESWT on chronic wounds.
Aligning our results with prior clinical studies and case series brings forth a defiance echoing the positive trends observed by pioneers like Porso et al46 and Saggini et al.47 These studies, while suggesting the need for more research, could not anticipate the disruptiveness of our study, diving into chronic wounds of varied etiologies and unraveling the potential of radial ESWT in diverse clinical scenarios. The authors suggested that additional research is necessary before considering the clinical implementation of ESWT for chronic wounds.
Comparisons with the grand narrative of expansive trials, such as Schaden et al48 which encompassed a myriad of chronic wounds treated with defocused ESWT, direct the spotlight back to radial ESWT, particularly in the context of pressure ulcers. In this clash of narratives, our study emerges as the radical underdog, insisting that the unique characteristics of radial ESWT deserve a distinct place in the annals of wound healing. The authors concluded that additional clinical trials are essential to assess the biophysical characteristics of ESWT and to establish a standardized ESWT protocol for chronic ulcers.
In substantiating our audacious claims, our study presents concrete evidence. A single session of radial ESWT yielded significant reductions in wound area, length, and width, transcending the confines of conventional wound care. The clinical condition of the wounds, assessed through Wound Bed Score (WBS) and Bates-Jansen Wound Assessment Tool (BWAT), witnessed remarkable enhancements. WBS scores soared from 4.6 ± 2.8 to 10.4 ± 3.6 points, showcasing a staggering 31.25% improvement. The BWAT score, a testament to the comprehensive clinical evaluation, exhibited a parallel rise from 43.8 ± 7.9 to 30.7 ± 7.5 points, marking a substantial 20.00% improvement. In this aspect, study by Wolf et al49 identified a significant correlation between the initial WBS and wound area, a finding consistent with our own study (including post-ESWT evaluation). The authors advocate for further research to elucidate the mechanisms by which ESWT promotes wound healing.
The timing of assessments is crucial in understanding the dynamics of wound healing. In this study, evaluations were conducted at two specific time-points: before the initiation of ESWT treatment (M0) and one week after the treatment (M1). These time-points were strategically chosen to capture the baseline condition of wounds and to assess the immediate impact of ESWT. The one-week interval allows for a relatively short-term observation of changes in wound parameters, providing insights into the early response to shockwave therapy. However, it’s important to note that longer-term follow-ups could offer a more comprehensive understanding of the sustained effects and overall progress in wound healing over time.
In the realm of ESWT parameters and sessions, our study aligns with the grand narrative only to the extent that it prompts evaluation in controlled clinical trials. However, our exclusive focus on radial ESWT in the context of pressure ulcers redefines the discourse. With specific parameters — 300 baseline pulses + 100 additional pulses per square centimeter, a pulse pressure of 2.5 bars, a pulse energy of 0.15 mJ/mm2, and a pulse frequency of 5 Hz — our study sets a benchmark for future investigations. Notably, our study hints at the transformative potential of radial ESWT, challenging the status quo and paving the way for a more targeted, nuanced approach in chronic wound management.
Study Limitations
This paper has certain potential limitations. First of all, it is recommended to validate the experiment through the inclusion of a control group within the protocol. It is important to note that ESWT treatment applications may require 3-5-10 sessions for stronger results, or treatment may need to continue until complete wound closure is achieved. Additionally, follow-up observations should be considered to assess long-term effects and the comprehensive journey of wound healing from intervention to closure.
Clinical Implications
This study offers compelling evidence endorsing the practicality of utilizing radial ESWT applications in the treatment of chronic wounds among geriatric patients. This finding holds potential benefits for both researchers and clinical practitioners in their pursuit of safe and efficient treatment approaches to facilitate wound healing of such demanding group of patients. It is important to take into account the essential methodological factors associated with the ESWT procedure, with particular attention to maintaining aseptic conditions throughout. The delivery of the procedure should be conducted meticulously and with the use of sterile materials. During the ESWT session, the applicator head makes direct contact with the wound, facilitated by sterile ultrasound gel and a sterile polyurethane film. ESWT application should commence from the wound’s edges, moving gently towards the center while meticulously treating the entire wound surface. Special attention is necessary when working near any bone structure, which should be avoided. Figure 6 provides an illustration of a treatment session employing radial ESWT. The potential complications, such as general discomfort during ESWT application, local pain sensations, transient increase in wound drainage, and the rare risk of infection, tissue damage or the possibility of local bleeding, should be thoroughly considered and reported to ensure the comprehensive understanding of the therapy’s impact on patients and to prevent any deterioration in their clinical condition.
Research Directions
It should be pointed out that ESWT currently lacks widespread adoption in routine clinical practice. Our study, along with others in this domain, seeks to provide evidence supporting the effectiveness and feasibility of ESWT in wound healing. These investigations are essential for developing practical guidelines and facilitating the integration of ESWT into routine wound care protocols. We value the chance to offer valuable insights into this emerging therapeutic approach. Future studies should be focused into optimizing treatment protocols, such as shockwave intensity, frequency, and duration, through iterative studies can help identify the optimal parameters for maximizing therapeutic benefits. Collectively, these future research directions aim to establish ESWT as a reliable and effective modality in the holistic management of wounds, providing evidence-based guidelines for its incorporation into clinical practice. Also, mechanistic studies at the molecular and cellular levels can deepen our understanding of how ESWT influences wound healing processes and explaining the biological mechanism of its action.
Conclusion
The ESWT may potentially serve as a clinically effective, non-invasive, and safe adjunctive biophysical therapy to enhance the healing of chronic wounds in older adults. Nonetheless, the outcomes of this initial clinical study should be approached with caution, and further well-designed RCTs involving a larger patient cohort, including placebo ESWT sessions, should be considered, particularly for PUs.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, [R.D.], upon reasonable request.
Acknowledgments
There were no other contributors to the article than the authors as well as there was no writing assistance regarding our paper.
Funding
This research project was supported by the Ministry of Health subventions for young researchers of the Wroclaw Medical University (no. STM.E020.20.100). The article processing charge was funded by the Ministry of Science and Higher Education of Poland as a part of a statutory grant of the Wroclaw Medical University for maintaining research potential (no. SUBZ.E250.23.020). The project was supported by the Wroclaw Academic Hub as part of MOZART programs number BWU-26/2017/M6 and BWU-20/2018/M7.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Järbrink K, Ni G, Sönnergren H, et al. The humanistic and economic burden of chronic wounds: a protocol for a systematic review. Syst Rev. 2017;6. doi:10.1186/s13643-016-0400-8
2. Frykberg RG, Banks J. Challenges in the treatment of chronic wounds. Adv Wound Care. 2015;4(9):560–582. doi:10.1089/wound.2015.0635
3. Darwin E, Tomic-Canic M. Healing chronic wounds: current challenges and potential solutions. Curr Dermatol Rep. 2018;7(4):296–302. doi:10.1007/s13671-018-0239-4
4. Raeder K, Jachan DE, Müller‐Werdan U, Lahmann NA. Prevalence and risk factors of chronic wounds in nursing homes in Germany. Int Wound J. 2020;17(5):1128–1134. doi:10.1111/iwj.13486
5. Kapp S, Miller C, Santamaria N. The quality of life of people who have chronic wounds and who self-treat. J Clin Nurs. 2018;27(1–2):182–192. doi:10.1111/jocn.13870
6. Sen CK, Gordillo GM, Roy S, et al. Human skin wounds: a major and snowballing threat to public health and the economy. Wound Repair Regen. 2009;17(6):763–771. doi:10.1111/j.1524-475X.2009.00543.x
7. Bickers DR, Lim HW, Margolis D, et al. The burden of skin diseases: 2004 a joint project of the American Academy of Dermatology Association and the Society for Investigative Dermatology. J Am Acad Dermatol. 2006;55(3):490–500. doi:10.1016/j.jaad.2006.05.048
8. Gould L, Abadir P, Brem H, et al. Chronic wound repair and healing in older adults: current status and future research. Wound Repair Regen. 2015;23(1):1–13. doi:10.1111/wrr.12245
9. Han G, Ceilley R. Chronic wound healing: a review of current management and treatments. Adv Ther. 2017;34(3):599–610. doi:10.1007/s12325-017-0478-y
10. Campbell C, Parish LC. The decubitus ulcer: facts and controversies. Clin Dermatol. 2010;28(5):527–532. doi:10.1016/j.clindermatol.2010.03.010
11. Probst S, Weller CD, Bobbink P, et al. Prevalence and incidence of venous leg ulcers—a protocol for a systematic review. Syst Rev. 2021;10:148. doi:10.1186/s13643-021-01697-3
12. Zhang P, Lu J, Jing Y, Tang S, Zhu D, Bi Y. Global epidemiology of diabetic foot ulceration: a systematic review and meta-analysis †. Ann Med. 2017;49(2):106–116. doi:10.1080/07853890.2016.1231932
13. Armstrong DG, Wrobel J, Robbins JM. Guest Editorial: are diabetes-related wounds and amputations worse than cancer? Int Wound J. 2007;4(4):286–287. doi:10.1111/j.1742-481X.2007.00392.x
14. Harries RL, Bosanquet DC, Harding KG. Wound bed preparation: TIME for an update. Int Wound J. 2016;13(Suppl 3):8–14. doi:10.1111/iwj.12662
15. Khan I, Arany P. Biophysical approaches for oral wound healing: emphasis on photobiomodulation. Adv Wound Care. 2015;4(12):724–737. doi:10.1089/wound.2014.0623
16. Kloth LC. Roles of physical therapists in wound management, part III: select biophysical technologies and management of patients with diabetic foot ulceration. J Am Coll Certif Wound Spec. 2009;1(3):80–83. doi:10.1016/j.jcws.2009.05.001
17. Kloth LC. The role of physical therapy in wound management - part one. J Am Coll Certif Wound Spec. 2009;1(1):4–5. doi:10.1016/j.jcws.2008.08.001
18. Heerschap C, Nicholas A, Whitehead M. Wound management: investigating the interprofessional decision‐making process. Int Wound J. 2018;16(1):233–242. doi:10.1111/iwj.13017
19. Korzendorfer H, Hettrick H. Biophysical technologies for management of wound bioburden. Adv Wound Care. 2014;3(12):733–741. doi:10.1089/wound.2013.0432
20. Taradaj J, Franek A, Blaszczak E, et al. Using physical modalities in the treatment of venous leg ulcers: a 14-year comparative clinical study. Wounds Compend Clin Res Pract. 2012;24(8):215–226.
21. Glazov G, Yelland M, Emery J. Low-level laser therapy for chronic non-specific low back pain: a meta-analysis of randomised controlled trials. Acupunct Med J Br Med Acupunct Soc. 2016;34(5):328–341. doi:10.1136/acupmed-2015-011036
22. Feehan J, Burrows SP, Cornelius L, et al. Therapeutic applications of polarized light: tissue healing and immunomodulatory effects. Maturitas. 2018;116:11–17. doi:10.1016/j.maturitas.2018.07.009
23. Lin YH, Li TS. The application of far-infrared in the treatment of wound healing. J Evid-Based Complement Altern Med. 2017;22(1):186–188. doi:10.1177/2156587215623436
24. Reinboldt-Jockenhöfer F, Traber J, Liesch G, Bittner C, Benecke U, Dissemond J. Concurrent optical and magnetic stimulation therapy in patients with lower extremity hard-to-heal wounds. J Wound Care. 2022;31(Sup6):S12–S21. doi:10.12968/jowc.2022.31.Sup6.S12
25. Kranke P, Bennett MH, Martyn-St James M, Schnabel A, Debus SE, Weibel S. Hyperbaric oxygen therapy for chronic wounds. Cochrane Database Syst Rev. 2015;(6):CD004123. doi:10.1002/14651858.CD004123.pub4
26. Rosińczuk J, Taradaj J, Dymarek R, Sopel M. Mechanoregulation of wound healing and skin homeostasis. BioMed Res Int. 2016;2016:3943481. doi:10.1155/2016/3943481
27. d’Agostino MC, Craig K, Tibalt E, Respizzi S. Shock wave as biological therapeutic tool: from mechanical stimulation to recovery and healing, through mechanotransduction. Int J Surg Lond Engl. 2015;24(Pt B):147–153. doi:10.1016/j.ijsu.2015.11.030
28. Sopel M, Kuberka I, Szczuka I, Taradaj J, Rosińczuk J, Dymarek R. Can shockwave treatment elicit a molecular response to enhance clinical outcomes in pressure ulcers? The SHOck waves in wounds project. Biomedicines. 2024;12(2):359. doi:10.3390/biomedicines12020359
29. Zhang L, Fu XB, Chen S, Zhao ZB, Schmitz C, Weng CS. Efficacy and safety of extracorporeal shock wave therapy for acute and chronic soft tissue wounds: a systematic review and meta-analysis. Int Wound J. 2018;15(4):590–599. doi:10.1111/iwj.12902
30. Dymarek R, Halski T, Ptaszkowski K, Slupska L, Rosinczuk J, Taradaj J. Extracorporeal shock wave therapy as an adjunct wound treatment: a systematic review of the literature. Ostomy Wound Manage. 2014;60(7):26–39.
31. Larking AM, Duport S, Clinton M, Hardy M, Andrews K. Randomized control of extracorporeal shock wave therapy versus placebo for chronic decubitus ulceration. Clin Rehabil. 2010;24(3):222–229. doi:10.1177/0269215509346083
32. Dymarek R, Kuberka I, Rosińczuk J, Walewicz K, Taradaj J, Sopel M. The immediate clinical effects following a single radial shock wave therapy in pressure ulcers: a preliminary randomized controlled trial of the SHOWN project. Adv Wound Care. 2023;12(8):440–452. doi:10.1089/wound.2021.0015
33. Duan H, Li H, Liu H, et al. Extracorporeal shockwave therapy combined with alginate dressing for treatment of sacroiliac decubital necrosis in older adults: a case report. Medicine. 2020;99(19):e19849. doi:10.1097/MD.0000000000019849
34. Kang N, Yu X, Ma Y. Radial extracorporeal shock wave therapy in a patient with decubitus ulcer after spinal cord injury: a case report. Am J Transl Res. 2020;12(5):2093–2098.
35. Wang SC, Anderson JAE, Evans R, et al. Point-of-care wound visioning technology: reproducibility and accuracy of a wound measurement app. PLoS One. 2017;12(8):e0183139. doi:10.1371/journal.pone.0183139
36. Falanga V, Saap LJ, Ozonoff A. Wound bed score and its correlation with healing of chronic wounds. Dermatol Ther. 2006;19(6):383–390. doi:10.1111/j.1529-8019.2006.00096.x
37. Bates-Jensen BM, McCreath H, Patlan A, Harputlu D. Reliability of the Bates-Jensen Wound Assessment Tool (BWAT) for pressure injury assessment: the pressure ulcer detection study. Wound Repair Regen. 2019;27(4):386–395. doi:10.1111/wrr.12714
38. Galiano R, Snyder R, Mayer P, Rogers LC, Alvarez O; Sanuwave Trial Investigators. Focused shockwave therapy in diabetic foot ulcers: secondary endpoints of two multicentre randomised controlled trials. J Wound Care. 2019;28(6):383–395. doi:10.12968/jowc.2019.28.6.383
39. Jeppesen SM, Yderstraede KB, Rasmussen BSB, Hanna M, Lund L. Extracorporeal shockwave therapy in the treatment of chronic diabetic foot ulcers: a prospective randomised trial. J Wound Care. 2016;25(11):641–649. doi:10.12968/jowc.2016.25.11.641
40. Moretti B, Notarnicola A, Maggio G, et al. The management of neuropathic ulcers of the foot in diabetes by shock wave therapy. BMC Musculoskelet Disord. 2009;10:54. doi:10.1186/1471-2474-10-54
41. Omar MTA, Alghadir A, Al-Wahhabi KK, Al-Askar AB. Efficacy of shock wave therapy on chronic diabetic foot ulcer: a single-blinded randomized controlled clinical trial. Diabet Res Clin Pract. 2014;106(3):548–554. doi:10.1016/j.diabres.2014.09.024
42. Snyder R, Galiano R, Mayer P, Rogers LC, Alvarez O; Sanuwave Trial Investigators. Diabetic foot ulcer treatment with focused shockwave therapy: two multicentre, prospective, controlled, double-blinded, randomised Phase III clinical trials. J Wound Care. 2018;27(12):822–836. doi:10.12968/jowc.2018.27.12.822
43. Wang CJ, Kuo YR, Wu RW, et al. Extracorporeal shockwave treatment for chronic diabetic foot ulcers. J Surg Res. 2009;152(1):96–103. doi:10.1016/j.jss.2008.01.026
44. Wang CJ, Wu RW, Yang YJ. Treatment of diabetic foot ulcers: a comparative study of extracorporeal shockwave therapy and hyperbaric oxygen therapy. Diabet Res Clin Pract. 2011;92(2):187–193. doi:10.1016/j.diabres.2011.01.019
45. Dolibog P, Dolibog P, Franek A, et al. Randomized, controlled clinical pilot study of venous leg ulcers treated with using two types of shockwave therapy. Int J Med Sci. 2018;15(12):1275–1285. doi:10.7150/ijms.26614
46. Porso M, Loreti S, Nusca SM, et al. Defocused shock wave therapy for chronic soft tissue wounds in the lower limbs: a pilot study. Ultrasound Med Biol. 2017;43(1):362–369. doi:10.1016/j.ultrasmedbio.2016.08.038
47. Saggini R, Figus A, Troccola A, Cocco V, Saggini A, Scuderi N. Extracorporeal shock wave therapy for management of chronic ulcers in the lower extremities. Ultrasound Med Biol. 2008;34(8):1261–1271. doi:10.1016/j.ultrasmedbio.2008.01.010
48. Schaden W, Thiele R, Kölpl C, et al. Shock wave therapy for acute and chronic soft tissue wounds: a feasibility study. J Surg Res. 2007;143(1):1–12. doi:10.1016/j.jss.2007.01.009
49. Wolff KS, Wibmer A, Pusch M, et al. The influence of comorbidities and etiologies on the success of extracorporeal shock wave therapy for chronic soft tissue wounds: midterm results. Ultrasound Med Biol. 2011;37(7):1111–1119. doi:10.1016/j.ultrasmedbio.2011.04.007
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patient-Reported Outcomes and Wound-Related Quality of Life in Adults with Diabetic Foot Ulcers Treated with Silicone Superabsorbent Polymer Dressings: Exploratory Results from a Prospective Multicenter Nonrandomized Cohort Study
Armstrong DG, Mikosinski J, Panczak K, Wegrzynowski A, Piechota D, Kotala M, Lipinski P, Rybolowicz K, Lipinska A, Velickovic V, Bil J, Szenk T, Buczak P, Pitchika A, Probst S
Medical Devices: Evidence and Research 2026, 19:619815
Published Date: 15 June 2026
Host Susceptibility Phenotypes and Construction of an Inflammation–Vascular–Metabolic (IVM) Integrated Score for Hard-to-Heal Wounds After Low-Energy Foot Trauma in Older Adults
Xiu L, Liu T, Ji Z, Zhang X, Yuan G, Li J, Yang P
Clinical Interventions in Aging 2026, 21:604608
Published Date: 30 June 2026