Back to Journals » Risk Management and Healthcare Policy » Volume 11
Is methicillin-resistant Staphylococcus Aureus infection associated with higher mortality and morbidity in hospitalized patients? A cohort study of 551 patients from South Western India
Authors Chatterjee A ![]() , Rai S, Guddattu V, Mukhopadhyay C
, Rai S, Guddattu V, Mukhopadhyay C ![]() , Saravu K
, Saravu K ![]()
Received 6 June 2018
Accepted for publication 10 October 2018
Published 3 December 2018 Volume 2018:11 Pages 243—250
DOI https://doi.org/10.2147/RMHP.S176517
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kent Rondeau
Aparajita Chatterjee,1 Shipra Rai,1 Vasudeva Guddattu,2 Chiranjay Mukhopadhyay,3 Kavitha Saravu1,4
1Department of Medicine, Kasturba Medical College, Manipal Academy of Higher Education (MAHE), Manipal, Madhav Nagar, Karnataka, India; 2Department of Statistics, Prasanna School of Public Health, Manipal Academy of Higher Education (MAHE), Manipal, Madhav Nagar, Karnataka, India; 3Department of Microbiology, Kasturba Medical College Manipal Academy of Higher Education (MAHE), Manipal, Madhav Nagar, Karnataka, India; 4Manipal McGill Center for Infectious Diseases, Prasanna School of Public Health, Manipal Academy of Higher Education (MAHE), Manipal, Madhav Nagar, Karnataka, India
Purpose: To determine morbidity and mortality of methicillin-resistant Staphylococcus aureus (MRSA) and methicillin-sensitive S. aureus (MSSA) infections in a tertiary health care facility.
Methods: A cohort study among hospitalized adult patients with culture proven MRSA or MSSA monoinfection were recruited in a tertiary referral center in South India from November 2011 to December 2012.
Results: Of total 551 subjects, 284 (52%) had MRSA and 267 (48%) MSSA infection. A total of 184 (65%) subjects had health care-associated MRSA (HA-MRSA) and 100 (35%) community-associated MRSA (CA-MRSA). Chronic kidney disease and recent antibiotic use had significant association with MRSA. MRSA patients had significant respiratory infection (OR 2.24 [1.04, 5.16]) and bacteremia (OR 2.24 [10.40, 5.16]), relative to MSSA. MSSA group had better survival function compared to MRSA group (P=0.028). Median duration of ICU stays were 5 days (IQR 4, 8) and 2 days (IQR 2, 2) in MRSA and MSSA, respectively. Complications such as acute kidney injury, sepsis, multiorgan dysfunction, need for supportive measures were more in the MRSA group.
Conclusion: MRSA imposes a huge burden in Indian scenario and HA-MRSA remains the main culprit. Patients with history of chronic kidney disease and recent use of antibiotics were found to be at a higher risk. Patients with MRSA infections tend to have poorer outcomes in terms of longer hospital stay, greater complications, and mortality.
Keywords: methicillin-resistant Staphylococcus aureus, Staphylococcus aureus, risk factors, outcome, mortality, India, prognosis, impact, morbidity
Introduction
Methicillin-resistant Staphylococcus aureus (MRSA) is one of the most commonly implicated agent in nosocomial infections in the US intensive care units. It accounts for more than 60% of all intensive care unit and is one of the leading causes of surgical site infections in tertiary care hospitals in North America.1–4 MRSA is a prominent emerging pathogen in the Indian subcontinent, with incidence varying from 25% in western part to 50% in southern part.5,6 A multicentric study conducted across 15 tertiary care centers in India from 2008 to 2009 showed overall prevalence of MRSA infection to be 41% among S. aureus isolates.7
Over the last decade, there has been an upsurge of community-associated MRSA (CA-MRSA) worldwide.8 CA-MRSA is one of the leading causes of skin and soft tissue infections in the USA.9 Moreover, CA-MRSA is also encroaching on nosocomial settings.10 Furthermore, infections with resistant organisms are notorious to impart significant health and economic consequences. While initial studies that investigated the impact of MRSA on mortality had produced conflicting results, more recent ones have shown increased mortality associated with MRSA infections in various settings.11,12 Although several of these studies have evaluated the difference in mortality between patients with MRSA and methicillin-sensitive S. aureus (MSSA), less is known about the effect of MRSA on other patient outcomes, such as length of hospital stay, length of antibiotics prescribed, and need for supportive measures.13
In this landscape of changing epidemiology of MRSA infections worldwide and dearth of literature on risk factors and outcomes of MRSA infections from the Indian subcontinent, a study addressing this knowledge gap was obligatory. The aims of our study were twofold. The first was to determine the clinical characteristics and risk factors of MRSA and MSSA infections in our tertiary care hospital. The second was to determine the outcomes of patients with MRSA and MSSA infections.
Methods
Study design
We conducted a cohort study to compare the risk factors and outcomes of MRSA and MSSA infections among hospitalized adult patients in a 2030-bed tertiary referral center in Manipal, South India from November 2011 to December 2012. Study group consisted of individuals ≥18 years with culture proven MRSA or MSSA monoinfection, where the organism was isolated from aspirated pus, body fluids, or blood. Only the first S. aureus infection for the individual patient was included. All samples were collected under aseptic conditions following recommended procedures. Individuals with cultures growing any other organism simultaneously along with MRSA/MSSA were excluded. Out of 612 patients with S. aureus infections during the study period, 551 patients fulfilled the inclusion criteria and were analyzed further (Figure 1).
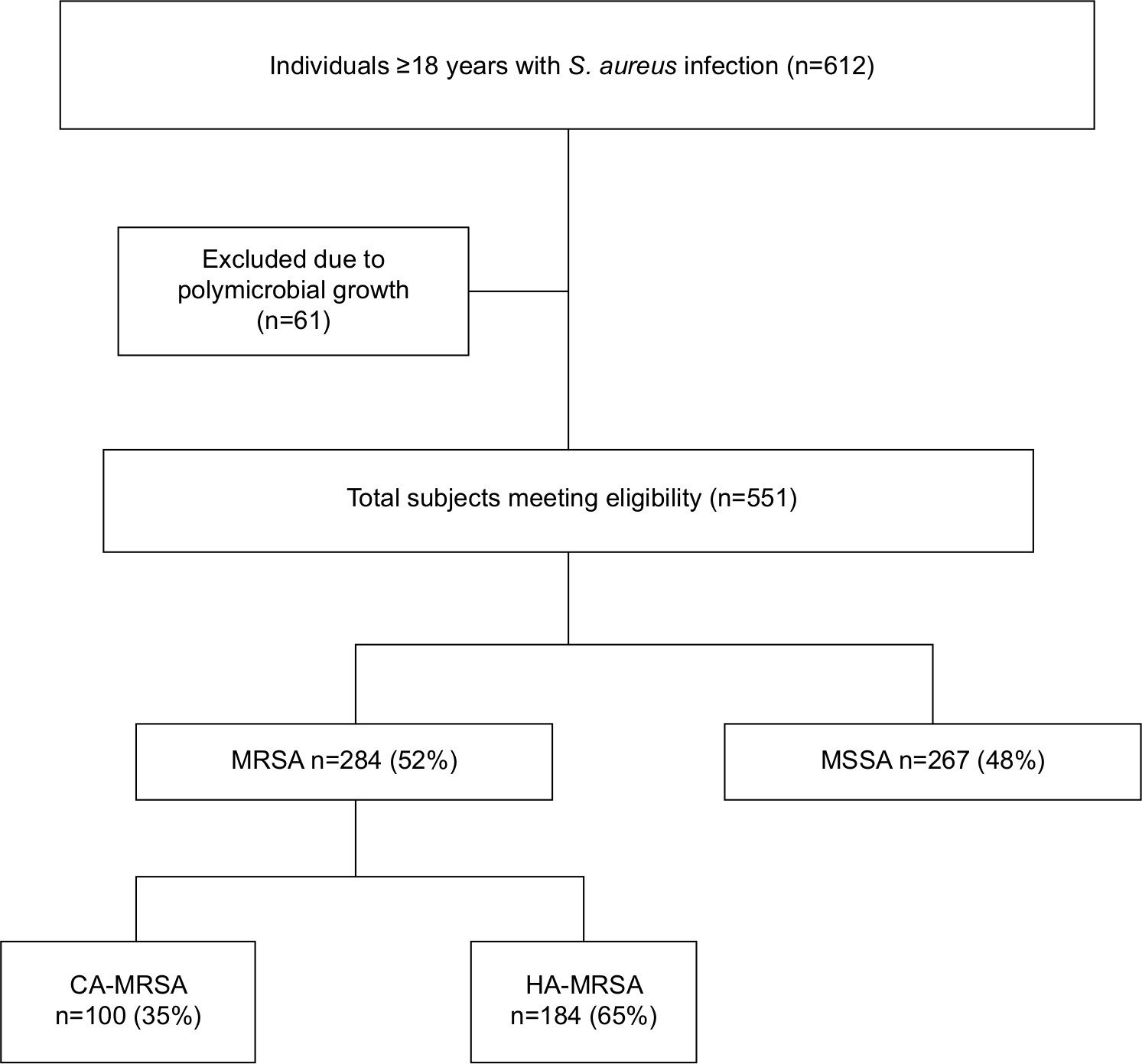 | Figure 1 Flowchart depicting patient enrollment. Abbreviations: HA-MRSA, health care-associated MRSA; MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-sensitive S. aureus. |
Variable definitions
A case (MRSA/MSSA) was defined as a hospitalized patient who had at least one positive culture for MRSA or MSSA. It was considered community-associated (CA-MRSA) when it appeared within 48 hours of admission without any health care risk factors (the presence of invasive device, history of surgery, hospitalization, dialysis, or residence in a long-term care facility within the preceding 12 months) or health care-associated (HA-MRSA) with onset ≥48 hours after admission or with ≥1 health care risk factor.14 Infective endocarditis was defined as per Dukes criteria.15 Acute kidney injury (AKI) was defined by a rise of at least 0.3 mg/dL of creatinine or 50% higher than baseline within a 24- to 48-hour period.15 Gangrene was defined as gray/blackish discoloration of body part/limb with or without line of demarcation. Multiorgan dysfunction syndrome was defined as dysfunction of more than one organ, requiring intervention to maintain homeostasis.15 Septic shock was defined as arterial blood pressure <90 mmHg systolic, or 40 mmHg less than patient’s normal blood pressure for at least 1 hour despite adequate fluid resuscitation or need for vasopressors to maintain systolic blood pressure 90 mmHg or mean arterial pressure 70 mmHg.15 Acute respiratory distress syndrome was defined as PaO2/FiO2 <200 mmHg with bilateral alveolar or interstitial infiltrates and no clinical evidence of increased left atrial pressure.15 Systemic inflammatory response syndrome was defined by two or more of the following conditions, if fulfilled—fever (oral temperature >38°C) or hypothermia (<36°C), tachypnea (>24 breaths/min), tachycardia (heart rate >90 beats/min) and leukocytosis (>12,000/L), leucopenia (<4,000/L) or >10% bands.15 Recent antibiotic use was defined as use of antibiotics for ≥7 days within the preceding 2 months. Adverse outcome was defined as a composite of death and discharge from the hospital against medical advice in a critical condition.
Data collection
All the isolates were identified as MRSA or MSSA based on the culture sensitivity reports. Blood culture was done using BacT-ALERT 3D automated microbial detection system (bioMérieux, Marcy l’Etoile, France), and growth of S. aureus was identified according to standard laboratory procedures. Antimicrobial susceptibility was tested in accordance with Clinical and Laboratory Standards Institute guidelines by Kirby–Bauer disk diffusion method.16 Cefoxitin disk diffusion was used to categorize S. aureus isolates as MRSA or MSSA. Once the subject was identified data including the demographic details, type of infection, risk factors, complications, treatment given, and outcomes were collected in a standard proforma after obtaining written informed consent from the patient or his/her relatives. Patients were initiated with empiric antibiotic therapy followed by specific therapy as per drug susceptibility reports along with surgical interventions wherever indicated, as per the treating clinicians’ judgment. All patients were followed up till discharge from the hospital or death.
Statistical analyses
Categorical variables are summarized by frequency and percentage. Continuous variables are summarized using mean and SD (for normally distributed variables) or median and IQR (for non-normally distributed variables). Chi-squared test was used as test of association between two categorical variables whereas OR with 95% CI was used to report the strength of association between them. Mann–Whitney U-test was used to compare medians across binary variable. Log rank test was used to compare survival function between two groups. All the data were analyzed using SPSS 15 and Stata 13. A P-value <0.05 was considered statistically significant.
Ethical approval/statement
The study was approved by Kasturba Medical College and Kasturba Hospital Ethics committee. Written informed consent was obtained from all participants. Patients’ data were anonymized to maintain confidentiality.
Results
Profile of MRSA and MSSA infections
Out of 551 subjects, 284 (52%) individuals were infected with MRSA, whereas 267 (48%) had MSSA infection. A 184 (65%) of the subjects were classified as having HA-MRSA as compared to the 100 (35%) who had CA-MRSA infections (Figure 1). Of the MRSA patients who were classified as having HA-MRSA infection, 162 (88%) had hospitalization within 12 months, 86 (47%) of them grew MRSA from cultures drawn 48 hours after admission, 102 (55%) had surgery in the past 12 months, 18 (10%) had a percutaneous device in situ, and 15 (8%) patients had undergone hemodialysis in the last 12 months.
Mean age of the MRSA group was 46.39±16.08 and in MSSA was 44.77±14.31. The number of males in MRSA and MSSA groups were 197 (70%) and 175 (66%), respectively. The distribution of participants across age group and gender was homogeneous between the two groups.
Spectrum of infections produced by MRSA/MSSA are summarized in Table 1. Skin and soft tissue infections predominated the clinical presentations in both the groups without any difference. However, MRSA was associated with significantly higher odds of respiratory infections (OR 2.24 [1.04, 5.16]) and bacteremia (OR 2.24 [10.40, 5.16]) than MSSA and had inverse association with deep abscesses (OR 0.51 [0.31, 0.81]) and septic arthritis (OR 0.30 [0.08, 0.89]).
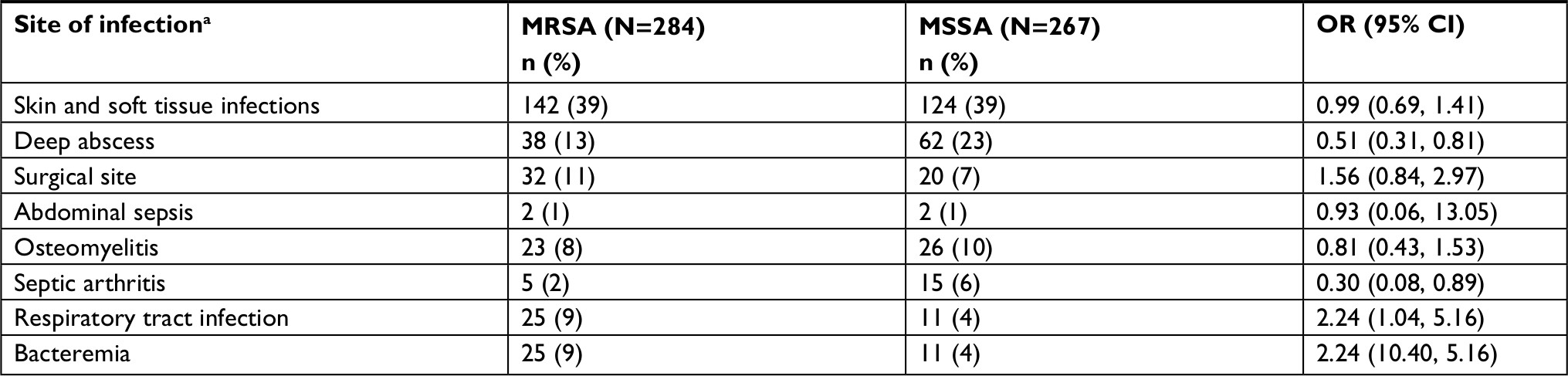 | Table 1 Distribution of sites of MRSA and MSSA infections Notes: aDifferent subgroups are not mutually exclusive. Abbreviations: MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-sensitive S. aureus. |
Distribution of clinical characteristics of MRSA and MSSA infections
The distribution of risk factors and comorbidities associated with infections are depicted in Table 2. Chronic kidney disease (OR 7.60 [2.90, 25.25]) and recent use of antibiotics (OR 1.74 [1.13, 2.68]) showed significant association with MRSA infection as compared to MSSA.
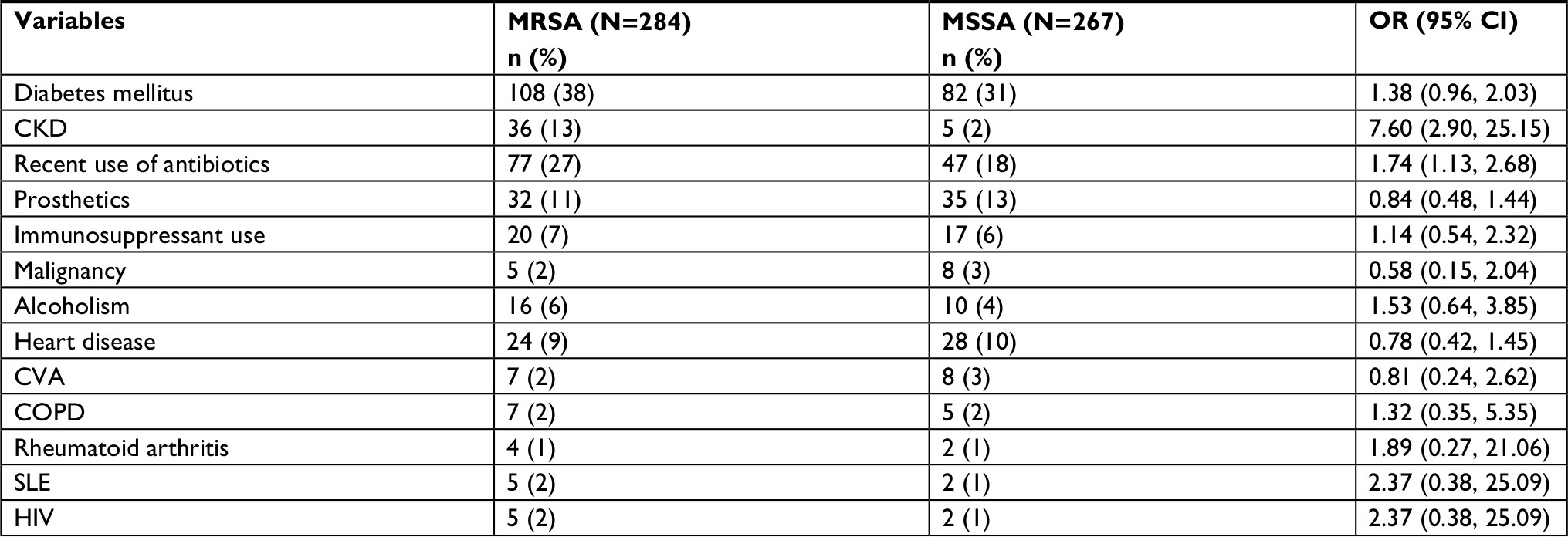 | Table 2 Distribution of risk factors and comorbidities associated with MRSA and MSSA infections Abbreviations: CKD, chronic kidney disease; CVA, cerebrovascular accident; HD, hemodialysis; MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-sensitive S. aureus; SLE, systemic lupus erythematosus. |
Treatment of MRSA and MSSA infections
In both the groups, 96% of the patients were empirically started on antimicrobial therapy. Notably, in the MRSA group, only 83/284 (29%) patients received empirical antibiotics that were effective against MRSA, as compared to 215/267 (80%) of MSSA patients who received antibiotics that the organism was sensitive to. The most commonly used empirical antibiotic was amoxicillin–clavulanic acid in both the MRSA (151/284 [53%]) and MSSA (148/267 [55%]) groups. Subsequent to culture reports, while the empiric antibiotic treatment was continued in 137/267 (51%) of MSSA patients, antibiotics were changed in 212/284 (75%) of MRSA patients. As specific anti-MRSA regimen, linezolid was initiated in 145/284 (51%), whereas 36/284 (13%) were given co-trimoxazole, 17/284 (6%) received vancomycin, and 14/284 (5%) received teicoplanin. Moreover, 33/267 (12%) of the MSSA patients were changed over to clindamycin, 32/267 (12%) to co-trimoxazole, and 21/267 (8%) to linezolid. Surgical debridement and removal of focus of infection were required in 204/267 (76%) of the MSSA patients as compared to 180/284 (63%) of MRSA patients.
Distribution of complications and outcomes of MRSA vs MSSA infections
The distribution of complications, supportive measures, durations of ICU stay, hospital stay, and antibiotic prescription in MRSA and MSSA group is presented in Tables 3 and 4. The occurrence of complications such as sepsis, AKI, and multiorgan dysfunction were significantly higher in the MRSA group as compared to MSSA group (Table 3). The median (IQR) duration of hospital stay in the MRSA group was 14 days (8.0–18.75 days) as compared to 8 days (4–16 days) in the MSSA group. The total duration of hospital stay was significantly longer in the MRSA group (P<0.001) (Table 4). A total of 112 (40%) of MRSA patients required ICU care in contrast to 38 (14%) of MSSA patients. Among patients requiring ICU care, the median IQR duration of ICU stays were 5 days (4, 8) and 2 days (2, 2) in MRSA and MSSA, respectively, which was statistically significant (P<0.001). The median (IQR) duration of antibiotics received in MRSA was 20 days (14–27 days); in MSSA, it was 14 days (10–24 days). Overall, the duration of antibiotic therapy was significantly longer in MRSA patients compared to MSSA patients. Likewise, the need for supportive measures were significantly higher in MRSA patients compared to MSSA patients (Table 4).
 | Table 3 Distribution of complications in MRSA vs MSSA infections Abbreviations: ARDS, acute respiratory distress syndrome; MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-sensitive S. aureus; MODS, multiorgan dysfunction; SIRS, systemic inflammatory response syndrome. |
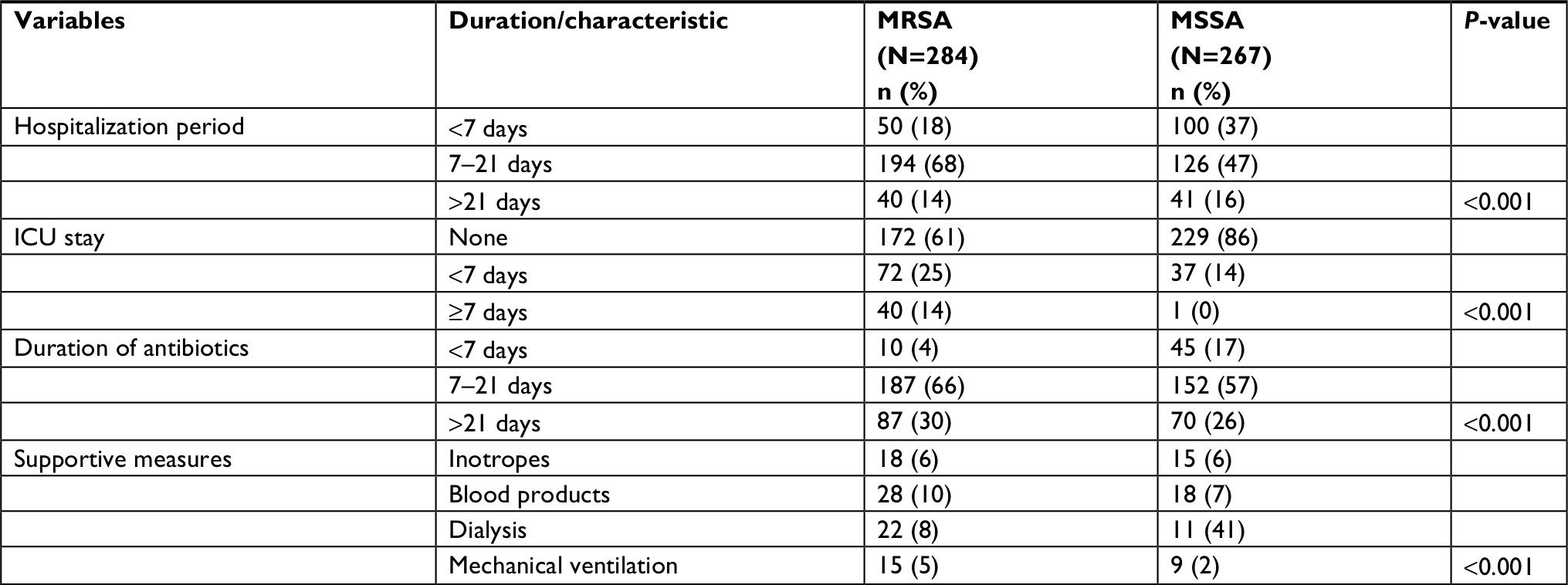 | Table 4 Distribution of supportive measures, durations of ICU stay, hospital stay, and antibiotic prescription with MRSA vs MSSA infection Abbreviations: MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-sensitive S. aureus. |
Case fatality rates were 7 (2%) and 3 (1%) for MRSA and MSSA infections, respectively; 18(6%) MRSA patients took discharge against medical advice (worse at discharge) in view of poor prognosis and lack of affordability of further health care as compared to 6 (2%) of MSSA patients. Of the 34 patients who had an adverse outcome, 24 patients had received inappropriate empirical antibiotics. Inappropriate empiric antibiotic therapy had significant (P=0.006) association with adverse outcome. The mean survival time for MSSA group is significantly higher as compared to MRSA group.
Discussion
The present study aimed to determine the distribution of risk factors and outcomes of MRSA infection in an Indian tertiary health care facility. A high proportion (52%) of MRSA infections was in concordance with other studies from India and the USA.2,7 In Europe, however, the prevalence of MRSA varies considerably, ranging from 0.4% in Sweden to 48.4% in Belgium.17 We further classified the MRSA patients as health care-associated MRSA (HA-MRSA) or community-associated MRSA (CA-MRSA). In the MRSA sub-group, 184 (65%) HA-MRSA. These findings are consistent with other studies conducted in India and elsewhere.7 However, this is in contrast to a study from South India that had reported a prevalence of 74% of CA-MRSA.18 This difference was probably due to the lone criterion used for CA-MRSA in their study with all positive cultures drawn within 48 hours of hospitalization being taken as community acquired.
Skin and soft tissue infections predominated in both the groups, proportions being 46% for MSSA and 49% for MRSA, in concurrence with other studies.7 However, MRSA was associated with significantly higher odds of respiratory infections and bacteremia (OR 2.24 [95% CI 1.04, 5.16]), which reiterate the findings of previous studies.19 Notably, there was no case of infective endocarditis due to S. aureus.
Risk factors found to be statistically significant for MRSA were chronic kidney disease and recent use of antibiotics.20 Prior receipt of antibiotics is an established risk factor that selects for drug-resistant MRSA and facilitates colonization and infection. However, we could not assign a particular class of antibiotics; the data could not be ascertained with certainty in all patients as available prescription prior to the hospitalization was uniformly poor in the study setting. Older age, diabetes mellitus, and chronic kidney disease were significantly associated with MRSA surgical site infections compared to MSSA.21 In another study among 13,796 adult ICU patients, MRSA was associated with cancer and chronic renal failure.22 Remarkably, in the present study, no patient had history of intravenous drug abuse.
There was a significant increase in survival function of MSSA group as compared to MRSA group (P=0.028) (Figure 2). These results are in conformity with those observed by Hanberger et al in critically ill patients and Engemann et al among surgical site infection patients.21,22 Moreover, in critically ill patients, MRSA bacteremia was found to have a higher attributable mortality than MSSA bacteremia after adjusting for disease severity and acute illness and additionally a meta-analysis has ascertained higher mortality with MRSA bacteremia compared to MSSA bacteremia.11,12 The number of hospital days, the need and duration of ICU stay, and the total duration of antibiotics prescription were also longer for MRSA patients than MSSA patients, as observed by others.22 The above-noted findings can be expounded on the basis that MRSA patients had more invasive infections, had more co-morbidities and complications as compared to the MSSA sub-group, and they tended to receive appropriate antibiotic therapy at a later date, all delaying their recovery.
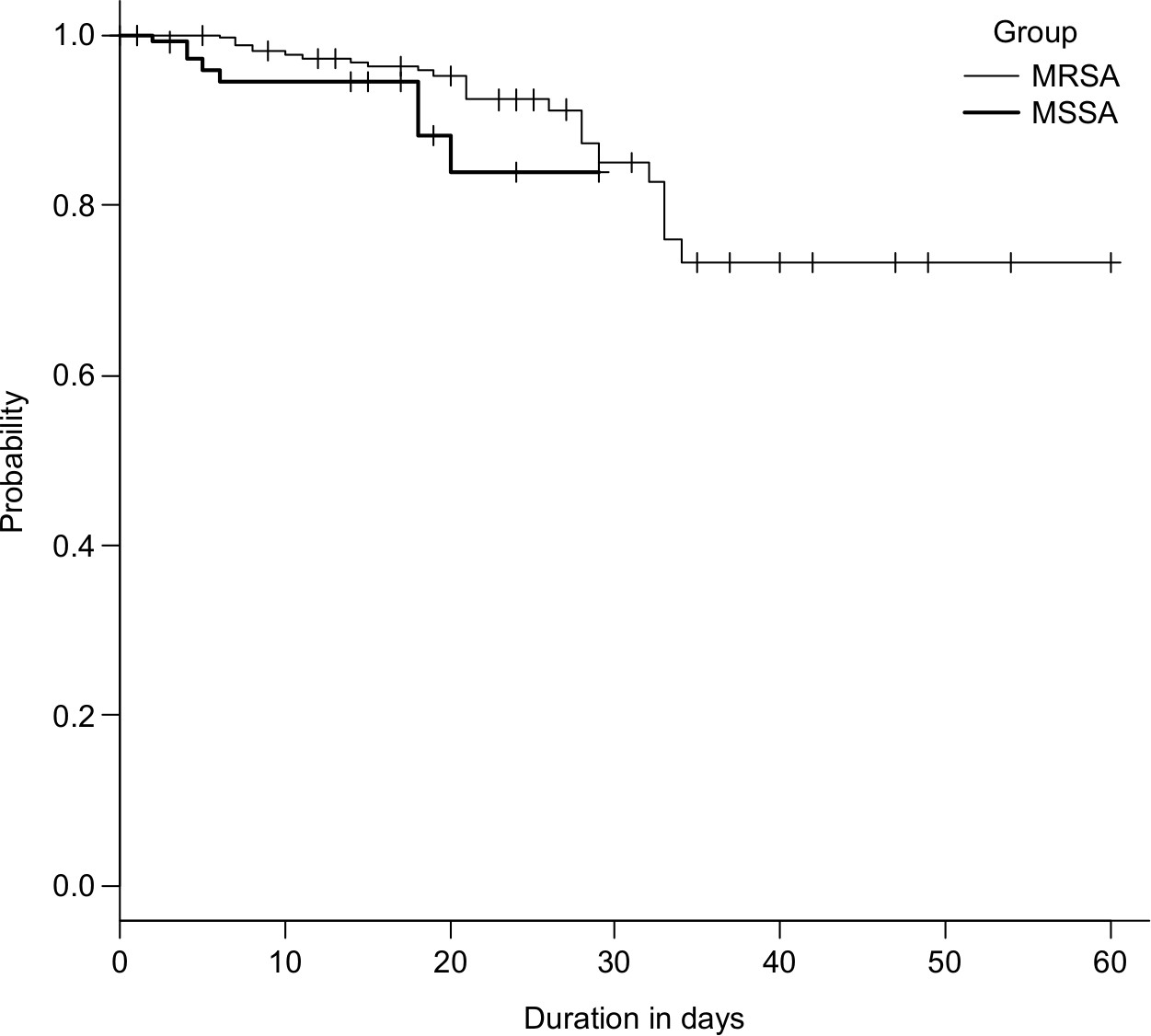 | Figure 2 Kaplan–Meier graph depicting survival function across the groups. Abbreviations: MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-sensitive S. aureus. |
There has been no evidence hitherto to suggest that MRSA strains are more virulent than MSSA strains.12 However, MRSA-associated increased mortality is accounted for by SCCmec type II in a study that adjusted for source of infection, comorbid conditions, illness severity, and treatment type.23 A notable feature in the present study was that only 29% of MRSA patients received antibiotics that the organism was sensitive to, whereas the vast majority of MSSA patients (81%) received appropriate empirical antibiotics. Similar findings were also noted by Soriano et al and Eshwara et al in their studies.18,24 Only one-third of MRSA patients had received appropriate empiric treatment and three-fourth of MRSA patients received a change in prescription post cultures. Notably, failure to receive early appropriate antibiotic in MRSA group was a major contributing factor for increased mortality and supportive requirements. A delay in receiving effective antibiotic therapy was associated significantly with all cause and attributable mortality in a study from Thailand.25
The present study has significant strengths. To the best of our knowledge, this is one of the largest clinical studies on MRSA infection in a non-outbreak setting from India, which prospectively recruited patients across all departments and thus gives us an idea about the wide spectrum of infections that can be caused by this versatile microbe. This study has sought to identify the risk factors and has used standard definition of CA-MRSA. In addition to mortality, the study has also addressed lesser studied outcomes such as length of hospital stay, ICU requirement, need for supportive care, and duration of antibiotics prescribed giving a useful surrogate metric of resource utilization and economic consequences. Outcomes of infections with susceptible vs resistant organisms is affected by the severity of underlying illness, as this by itself may influence the length of hospitalization and mortality/morbidity profiles. In the present study, as we did not adjust for underlying diseases or severity of clinical condition, there is a possibility that the association of MRSA with mortality and adverse outcomes has been overestimated. The standard scoring systems that are in use for ICU patients were not applicable for all our patients with S. aureus infections across the departments and hence could not be used. Although MSSA can be hospital or community acquired, this distinction was not assigned in the present study and hence could not be compared. Definition of sepsis and septic shock has changed since the study; however, this would not change the results of the present study.
Rates of nasal carriage of MRSA have been studied by various investigators in India, and they range from 7.7% in school children, 3%–10% in predominantly outpatient population to 7.5%–25% in health care workers, highlighting the potential role of health care workers in the transmission.26–29 However, the present study lacks MRSA carrier status estimation, molecular characterization, and panton-valentine leukocidin toxin carriage status. Future multicentric studies that adequately adjust for the severity of underlying illness and treatment instituted are needed to better clarify the risk factors for mortality and improve the treatment outcomes.
Conclusion
More than half of all the staphylococcal infections in the present study were due to methicillin-resistant strains. Of these, the majority were health care associated. Risk factors associated with MRSA infections were chronic kidney disease and recent antibiotic use. These findings thus highlight the problem of MRSA in the Indian scenario. Our study reiterates that MRSA is associated with increased mortality and prolonged hospitalization. They were also more likely to have received inappropriate antibiotics at the onset. Hence, a greater degree of suspicion for MRSA in clinical setting, early detection of MRSA by rapid tests from blood stream infection by automated methods, along with timely prescription of appropriate antibiotics and source control are needed to improve the outcomes in these patients. Also, restricted use of antimicrobials, antibiotic stewardship, and infection control can help prevent further spread of these deadly multidrug-resistant organisms.
Disclosure
The authors report no conflicts of interest in this work.
References
National Nosocomial Infections Surveillance System. National Nosocomial Infections Surveillance (NNIS) System Report, data summary from January 1992 through June 2004, issued October 2004. Am J Infect Control. 2004;32(8):470. | ||
Anderson DJ, Sexton DJ, Kanafani ZA, Auten G, Kaye KS. Severe surgical site infection in community hospitals: epidemiology, key procedures, and the changing prevalence of methicillin-resistant Staphylococcus aureus. Infect Control Hosp Epidemiol. 2007;28(9):1047–1053. | ||
Hidron AI, Edwards JR, Patel J, et al; National Healthcare Safety Network Team; Participating National Healthcare Safety Network Facilities. NHSN annual update: antimicrobial-resistant pathogens associated with healthcare-associated infections: annual summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2006-2007. Infect Control Hosp Epidemiol. 2008;29(11):996–1011. | ||
Dukic VM, Lauderdale DS, Wilder J, Daum RS, David MZ. Epidemics of community-associated methicillin-resistant Staphylococcus aureus in the United States: a meta-analysis. PLoS One. 2013;8(1):e52722. | ||
Patel AK, Patel KK, Patel KR, Shah S, Dileep P. Time trends in the epidemiology of microbial infections at a tertiary care center in west India over last 5 years. J Assoc Physicians India. 2010;58(Suppl):37–40. | ||
Gopalakrishnan R, Sureshkumar D. Changing trends in antimicrobial susceptibility and hospital acquired infections over an 8 year period in a tertiary care hospital in relation to introduction of an infection control programme. J Assoc Physicians India. 2010;58(Suppl):25–31. | ||
Joshi S, Ray P, Manchanda V, Bajaj J, Chitnis D, Gautam V, Goswami P et al. Methicillin resistant Staphylococcus aureus (MRSA) in India: prevalence & susceptibility pattern. Indian J Med Res. 2013;137(2):363. | ||
Alvarez-Uria G, Reddy R. Prevalence and antibiotic susceptibility of community-associated methicillin-resistant Staphylococcus aureus in a rural area of India: is MRSA replacing methicillin-susceptible Staphylococcus aureus in the community? ISRN Dermatol. 2012;2012(21):1–5. | ||
Moran GJ, Krishnadasan A, Gorwitz RJ, et al. Methicillin-resistant S. aureus infections among patients in the emergency department. N Engl J Med. 2006;355(7):666–674. | ||
Popovich KJ, Weinstein RA, Hota B. Are community-associated methicillin-resistant Staphylococcus aureus (MRSA) strains replacing traditional nosocomial MRSA strains? Clin Infect Dis. 2008;46(6):787–794. | ||
Blot SI, Vandewoude KH, Hoste EA, Colardyn FA. Outcome and attributable mortality in critically Ill patients with bacteremia involving methicillin-susceptible and methicillin-resistant Staphylococcus aureus. Arch Intern Med. 2002;162(19):2229–2235. | ||
Cosgrove SE, Sakoulas G, Perencevich EN, Schwaber MJ, Karchmer AW, Carmeli Y. Comparison of mortality associated with methicillin-resistant and methicillin-susceptible Staphylococcus aureus bacteremia: a meta-analysis. Clin Infect Dis. 2003;36(1):53–59. | ||
Wang JL, Chen SY, Wang JT, et al. Comparison of both clinical features and mortality risk associated with bacteremia due to community-acquired methicillin-resistant Staphylococcus aureus and methicillin-susceptible S. aureus. Clin Infect Dis. 2008;46(6):799–806. | ||
Klevens RM, Morrison MA, Nadle J, et al. Invasive methicillin-resistant Staphylococcus aureus infections in the United States. J Am Med Assoc. 2007;298(15):1763–1771. | ||
Fauci AS, Braunwald E, Kasper DL, Hauser SL, Longo DL, Jameson JL. Harrison’s Principles of Internal Medicine. 17th ed. New York: McGraw-Hill Education; 2008. | ||
Clinical Laboratory Standards Institute. Performance Standards for Antimicrobial Disk Susceptibility Tests; Approved Standard. Wayne, PA: Laboratory Standard Institute; 2012. | ||
Sader HS, Farrell DJ, Jones RN. Antimicrobial susceptibility of Gram-positive cocci isolated from skin and skin-structure infections in European medical centres. Int J Antimicrob Agents. 2010;36(1):28–32. | ||
Eshwara VK, Munim F, Tellapragada C, et al. Staphylococcus aureus bacteremia in an Indian tertiary care hospital: observational study on clinical epidemiology, resistance characteristics, and carriage of the Panton-Valentine leukocidin gene. Int J Infect Dis. 2013;17(11): e1051–e1055. | ||
Filice GA, Nyman JA, Lexau C, et al. Excess costs and utilization associated with methicillin resistance for patients with Staphylococcus aureus infection. Infect Control Hosp Epidemiol. 2010;31(4):365–373. | ||
Hershow RC, Khayr WF, Smith NL. A comparison of clinical virulence of nosocomially acquired methicillin-resistant and methicillin-sensitive Staphylococcus aureus infections in a university hospital. Infection Control. 1992;13(10):587–593. | ||
Engemann JJ, Carmeli Y, Cosgrove SE, et al. Adverse clinical and economic outcomes attributable to methicillin resistance among patients with Staphylococcus aureus surgical site infection. Clin Infect Dis. 2003;36(5):592–598. | ||
Hanberger H, Walther S, Leone M, et al. Increased mortality associated with methicillin-resistant Staphylococcus aureus (MRSA) infection in the intensive care unit: results from the EPIC II study. Int J Antimicrob Agents. 2011;38(4):331–335. | ||
Ganga R, Riederer K, Sharma M, et al. Role of SCCmec type in outcome of Staphylococcus aureus bacteremia in a single medical center. J Clin Microbiol. 2009;47(3):590–595. | ||
Soriano A, Martínez JA, Mensa J, et al. Pathogenic significance of methicillin resistance for patients with Staphylococcus aureus bacteremia. Clin Infect Dis. 2000;30(2):368–373. | ||
Nickerson EK, Wuthiekanun V, Wongsuvan G, et al. Factors predicting and reducing mortality in patients with invasive Staphylococcus aureus disease in a developing country. PLoS One. 2009;4(8):e6512. | ||
Singh AK, Agarwal L, Kumar A, Sengupta C, Singh RP. Prevalence of nasal colonization of methicillin-resistant Staphylococcus aureus among schoolchildren of Barabanki district, Uttar Pradesh, India. J Family Med Prim Care. 2018;7(1):162–166. | ||
Sharma Y, Jain S, Singh H, Govil V. Staphylococcus aureus: screening for nasal carriers in a community setting with special reference to MRSA. Scientifica. 2014;2014(3):1–5. | ||
Singh S, Malhotra R, Grover P, et al. Antimicrobial resistance profile of methicillin-resistant Staphylococcus aureus colonizing the anterior nares of health-care workers and outpatients attending the remotely located tertiary care hospital of North India. J Lab Physicians. 2017;9(4):317–321. | ||
Patwardhan V, Kumar D, Goel V, Singh S, Sarman S. Changing prevalence and antibiotic drug resistance pattern of pathogens seen in community-acquired pediatric urinary tract infections at a tertiary care hospital of North India. J Lab Physicians. 2017;9(4):264–268. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.