Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Is It Possible for Light-Based Hair Removal Home Devices to Induce Ocular Damage? Systematic Review
Authors Al muqarrab FJ ![]() , Alsuwaidan S, Al muqarrab Z, Alajlan A
, Alsuwaidan S, Al muqarrab Z, Alajlan A ![]()
Received 3 October 2023
Accepted for publication 17 December 2023
Published 23 December 2023 Volume 2023:16 Pages 3731—3742
DOI https://doi.org/10.2147/CCID.S442963
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Rungsima Wanitphakdeedecha
Fatimah J Al muqarrab,1 Sami Alsuwaidan,1 Zahraa Al muqarrab,2 Abdulmajeed Alajlan1
1Department of Dermatology, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 2Department of Dermatology, College of Medicine, King Faisal University, Hofuf, Saudi Arabia
Correspondence: Fatimah J Al muqarrab, Department of Dermatology, College of Medicine, King Saud University, Riyadh, Saudi Arabia, Tel +966-545772444, Email [email protected]
Abstract: Light-based hair removal home devices emit intense pulse light (IPL) or Diode laser. While the Food and Drug Administration controls them in the US, Europe continues to classify them as cosmetic products. Emerging concerns are: what if an unprotected eye is inadvertently exposed to light emission? Or if the consumer tries to overcome the protective safety features? We performed this systematic review by searching the Medline, CENTRAL, and Google Scholar databases to investigate the ocular damage reported after exposure to IPL for hair removal. We could not identify any case reported following exposure to home devices; however, a total of 20 patients were identified with iris atrophy, anterior chamber inflammation, and/or retinal pigment epithelium damage following exposure to office IPL or Diode lights. 40% were not using any protective eyewear during the light procedure. The reported fluences were in the range of 20– 24 J/cm2. Although the ocular damage was identified following office devices, the reported fluences were within the home device’s limits. For that, manufacturers should provide clear instructions on the package regarding the ocular hazards, the importance of using protective goggles, and a firm warning not to overcome the contact sensors. Home device-induced ocular damage is still a concern, perhaps under-reported.
Keywords: light-based home devices, IPL, intense pulse light, laser safety, hair removal, ocular damage
Introduction
Home-use light-based device manufacturing has grown exponentially over the last few years. Indeed, their popularity increased as a mean of depilation in the privacy of consumers’ homes at a lower cost than in professional settings. Most of those devices are based on intense pulse light (IPL); however, few laser home devices are available on the market.1,2 The IPL is noncoherent light with a broad wavelength output ranging from 500 to 1200 nm.3 Unlike lasers, pulses are generated from electrical current bursts that stimulate xenon gas-containing chambers. The emitted light is filtered using “cutoff” filters to limit the undesirable lower end of the spectrum minimizing tissue damage.3,4 IPLs emit broad wavelengths within the visible and near-infrared spectrum diminishing the selective photothermolysis of the specified chromophores. Nevertheless, Cohen et al reviewed the literature, and they stated that the grade of evidence as by the Oxford Centre for Evidence-Based Medicine guidelines for the efficacy of home light-based hair removal devices is A.5,6
Those devices are under different regulation systems in the United States compared to European countries. While they are considered medical devices controlled by the Food and Drug Administration (FDA) in the United States, Europe continues to consider them as cosmetic products.2,7 The FDA imposes an obligatory premarket approval (PMA) requisite to make them safe for human use and suitable for consumer use even without healthcare professional supervision. In that term, the FDA is committed to selected laser standards issued by the International Electrotechnical Commission [IEC 60825–1 (Safety of laser products – Part 1: Equipment classification and requirements) and IEC 60601-1-11:2010 (Medical electrical equipment Part 1–11: General requirements for basic safety and essential performance. Collateral standard: Requirements for medical electrical equipment and medical electrical systems used in the home healthcare environment).8 According to the updated IEC 60825–1 Ed. 3.0 b:2014, the international laser standards introduced a new class, class 1 C, designed for laser products requiring contact application to fire.9 The home-use light-based hair removal devices fall into class 1, as claimed by their manufacturers, and they might be reclassified into class 1 C, as most of them incorporate safety contact sensors that minimize inadvertent light emissions when the probe is not in direct contact with the skin.10,11 By that, ocular damage is supposed to be prevented by engineering means. As a result, a good number of IPL home devices are not supplemented with protective eyewear. An emerging concern exists, despite the lower fluence rates of home devices compared to office IPL devices: what if an unprotected eye is inadvertently exposed to light emission? Or what if the consumer tried to overcome the protective safety features? In our experience, some of our patients have already tried to overcome the contact sensors for adjusting the device output window to the curved body parts.
It is essential that IPL home device consumers are well informed regarding the presumed ocular hazards, the precautions that must be taken during the procedure, and the clinical signs of varying ocular complications. We conducted this review to describe the reported ocular complications following IPL exposure, the most common ocular segment that has been damaged, and how the damage was presented clinically.
Methodology
We followed the PRISMA methodology in our search, i.e., Preferred Reporting Items for Systematic Review and Meta-Analysis. Initially, we searched the PROSPERO database to detect duplicate works; however, we did not find any ongoing or published similar reviews. Subsequently, this review was registered in PROSPERO, with an ID number CRD42023429287. Our search strategy is summarized in the study flow chart. An electronic search of the Medline, CENTRAL, Cochrane, and Google Scholar databases was conducted using the terms ocular complication, ocular damage, intense pulse light, and IPL home devices. Furthermore, cited references from the ResearchGate database were further explored to identify any relevant articles. We included articles if they met our inclusion criteria: case reports of ocular damage following exposure to IPL used for dermatologic indications, written in English or in a language reliably translated to English. Papers were excluded if they described ocular injuries after laser exposure other than IPL if the exposure occurred in nonclinical settings or for non-dermatologic indications.
Data were extracted by one investigator and cross-checked by a second reviewer. At the same time, papers were critically appraised using the Critical Appraisal Tools, Joanna Briggs Institute, 2020.12 The quality checks the adequacy of the patients and their clinical condition description, the presence of conclusive evidence of the diagnosis provided, a clear description of the intervention given and the post-intervention outcomes. Generated data are summarized in an Excel sheet and subsequently tabulated. Dichotomous variables were descriptively calculated using frequencies and percentages.
Results
A total of 18 articles13–30 including 20 patients were identified in the literature, describing ocular complications following exposure to an IPL source (60%) or to a diode laser (40%) [Figure 1]. Most patients (95%) were female; their mean age was 40 (St. deviation 12). Of those reporting the usage of protective eyewear or not, 40% did not use any protective measure, an additional 30% shifted the protective eyewear during the procedure, and one patient was wearing cosmetic contact lenses during the procedure.22 Three patients reported that they directly looked at the IPL probe while it was fired up.15,24,27 Eighteen patients (90%) received facial IPL treatment, and 17 of their procedures were performed in a periocular location. Of those reported laser parameters, the fluence used was in the range of 20–24 J/cm2.
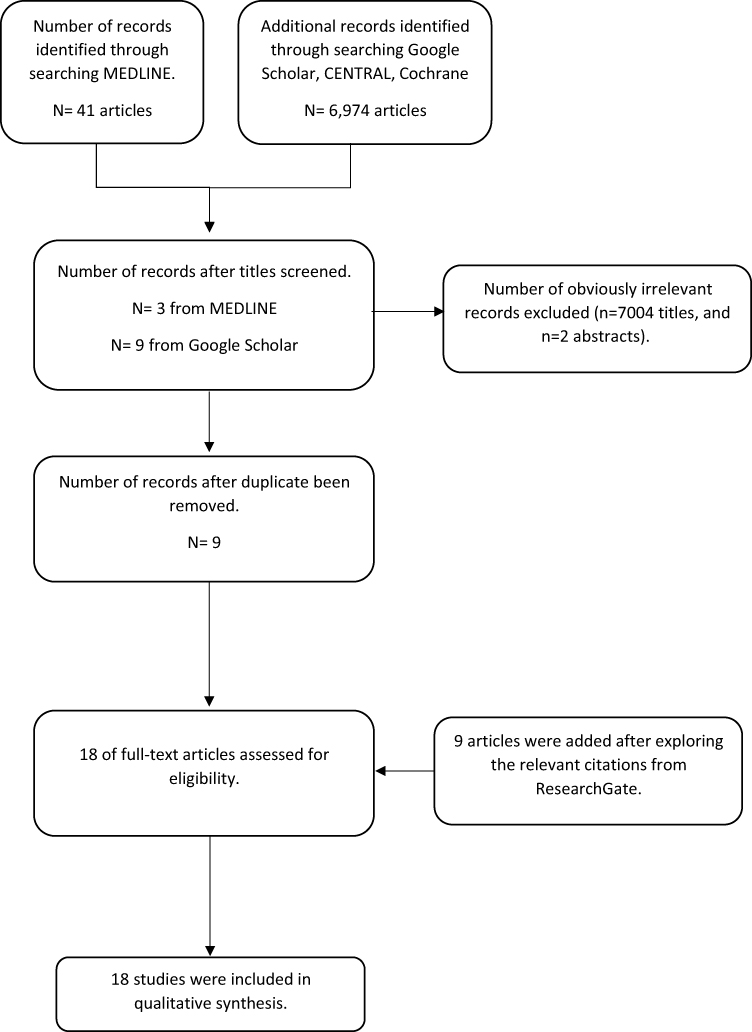 |
Figure 1 PRISMA chart flow. |
Clinically (Table 1), the symptoms of ocular complications started during the procedure in 7 (35%) patients, a few hours after the procedure in 4 (20%) patients, and within two days after the procedure in 6 (30%) patients. The most reported symptom was photophobia (75%), followed by ocular pain and visual disturbances (60%). Thirty percent of the patients reported eye redness as their presenting symptom. Half of the patients reported left laterality of the injury, 20% reported bilateral complications, and 30% reported right laterality. The most common complication reported was iris atrophy (65%) caused by IPL exposure in 61% of the cases and by diode laser in an additional 38%. Anterior chamber inflammation was the second most common complication, reported in 60% of the cases (Figure 2). Interestingly, the retinal pigment epithelium was damaged in four patients (20%), equally experienced following IPL or diode exposure. In one case,22 where the patient was wearing cosmetic contact lenses during the IPL procedure, the lens pigment was deposited over the cornea, which was corrected surgically using a No. 15 blade.
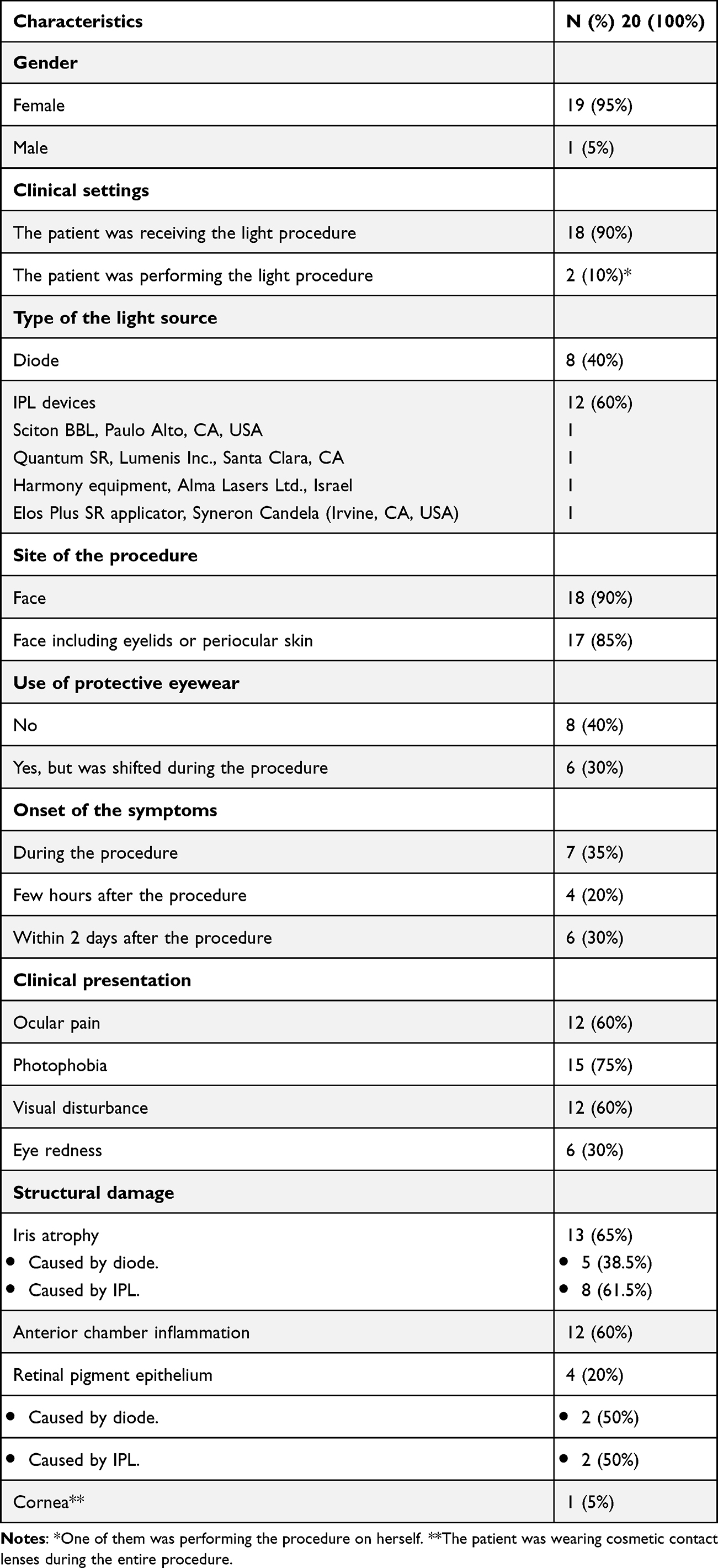 |
Table 1 Patient Characteristics, Clinical Settings and Ocular Structural Damages Induced by Intense Pulse Light/Diode Laser |
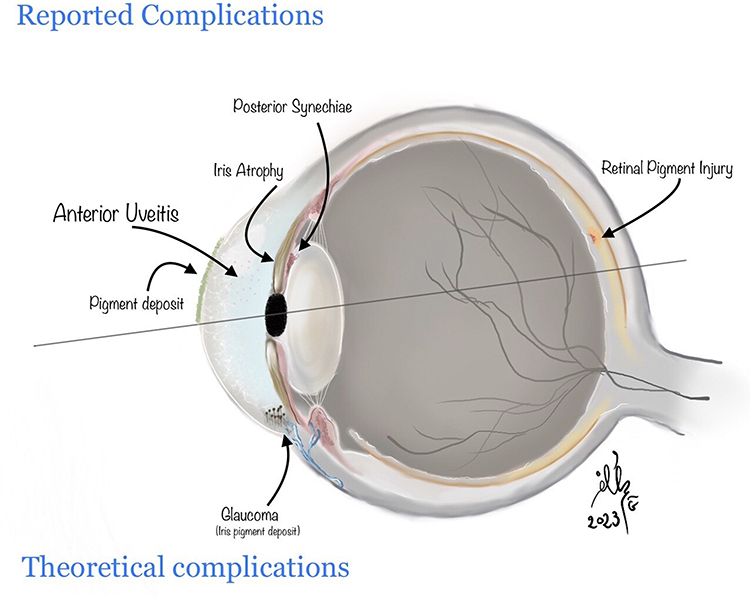 |
Figure 2 Ocular complications reported following exposure to IPL or Diode laser. |
All the reported cases of anterior chamber inflammation improved completely; however, iris atrophy did not. All 14 reported cases of iris atrophy were permanent at the follow-up visits: 6 weeks to 3 years from the injury. Of those 14 cases, 6 cases developed additional ocular complications in the follow-up visits: 3 cases had permanent posterior iris synechiae,17,19,23 one case developed transient glaucoma that improved after stopping the topical steroid,20 an additional case developed persistent posterior subcapsular cataract,14 and another case was complicated with persistent peripheral visual field defects.30 In the same context, the three reported cases of retinal damage persisted for months. While a case of retinal detachment and choroidal neovascularization improved after medical treatment, a case that developed a macular hole was partially corrected surgically with a remnant persistent retinal pigment epithelium defect, and a further case of persistent retinal pigment epithelium interruption was reported (Table 2).
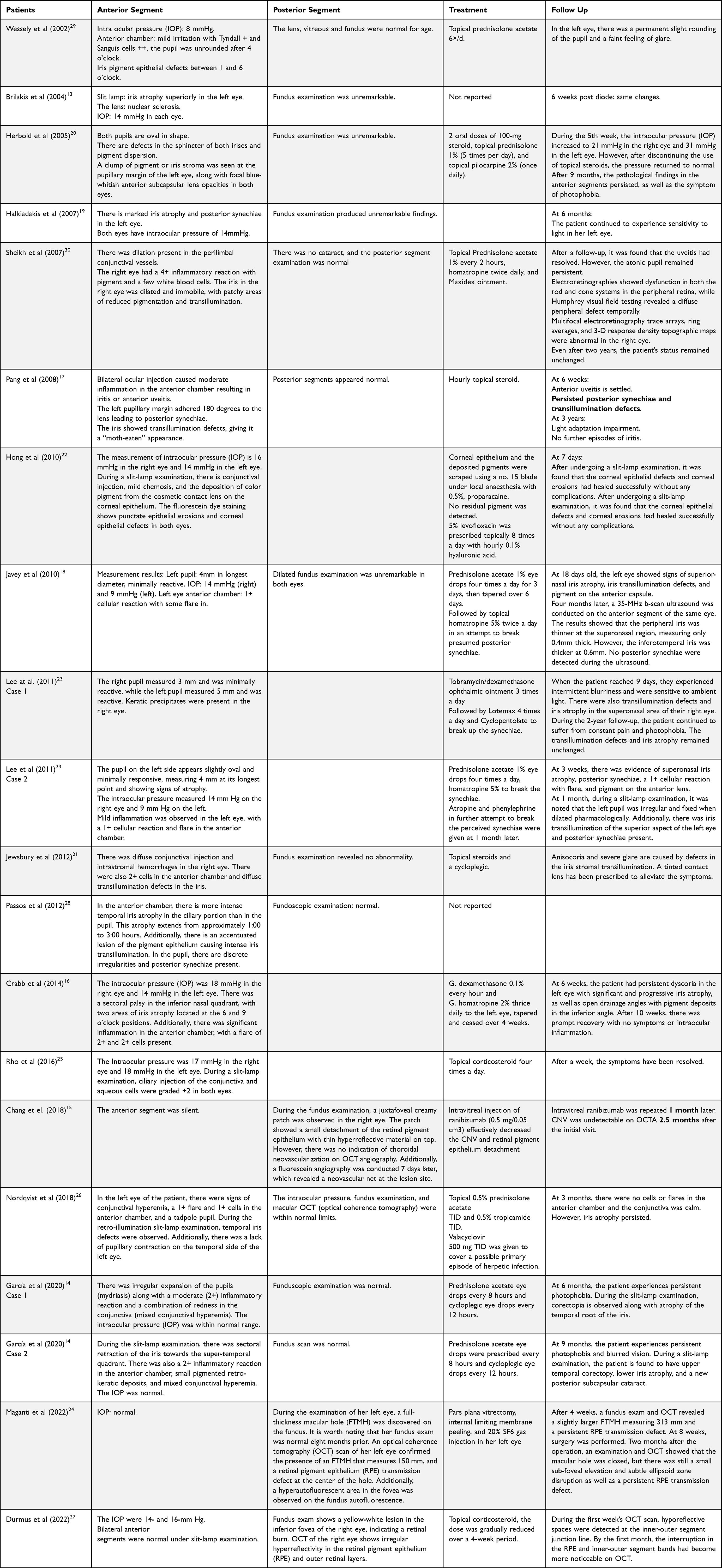 |
Table 2 Clinical Course of the Ocular Complications Induced by Intense Pulse Light/Diode Laser and the Undertaken Treatment Measures |
Discussion
Ocular injury following laser or light-based devices is not an uncommon devastating complication that can be minimized by proper training and adherence to safety protocols. Investigating a legal national resource in the US identified 174 cases of litigation involving laser procedures; more than half of them were performed for hair removal. A total of 2.2% of those cases were related to ocular injuries. More than 50% of the cases were associated with a lack of informed consent, and an additional 0.5% were related to a lack of goggles.31 In parallel, more than three-quarters of the reported IPL-induced ocular injuries we identified were secondary to the improper use of protective eyewear.
Although all the reported cases we identified were office-based devices, home-based devices can induce a similar pattern of injuries. For illustration, Town et al32 measured 18 IPL medical and nonmedical CE devices and 36 applicator parameters; they identified up to 10% higher emitted fluence from the applicators compared to the claimed fluence by the manufacturers, and 9 out of the 18 devices exceeded the medical Class 4 laser standards (> +20%). Additionally, 65.5% of the devices they tested showed inaccurate cutoff filters by more than 20 nm, as claimed by the manufacturers. Considering the lack of strict wide-nation regulations over light-based home device manufacturing and commercial pressures, discrepancies between the measured and manufacturers’ claimed parameters are also possible for home devices. As an instance, Eadie et al33 examined one IPL home device for ocular safety hazards, and they discovered that the retinal thermal hazard was exceeded at a fluence of 11 J/cm2 and 20 cm viewing distance following firing the IPL home device they tested. It is worth mentioning that the maximum available energy from IPL home devices is between 7.5 and 30 Joules (J) delivered over a spot size of 2–6 cm2 over 2.5–60 milliseconds (Ms). On the other hand, home-based laser devices such as (Tria Beauty, Dublin, CA 94568, USA) deliver up to 22 J/cm2 over a spot size of 0.79 cm2 and a pulse duration of 600 ms.1,2,7 Nevertheless, we identified the reported ocular injuries following exposure to a similar fluence range to the home devices. Moreover, the increasing reports of ocular damage following exposure to low-energy laser sources, such as toy laser pointers, warrant the hazardous possibility of such events following exposure to low-energy home-based light sources.34
Interestingly, authors of a recent surveillance-based study investigated the post marketing voluntary reports of adverse events noticed following exposure to home-IPL devices, they detected 34 cases of eye pain of unknown clinical significance.35 Equally concerning, we randomly searched online market engines such as Amazon.com to identify the available hair removal light-based home devices. Predictably, out of 20 randomly detected devices searched for FDA clearance at 510(k) Premarket Notification (fda.gov),36 10 market-available devices are not FDA cleared. Eight out of the 20 randomly selected devices lack supplementary goggles with the device’s package (Table 3).
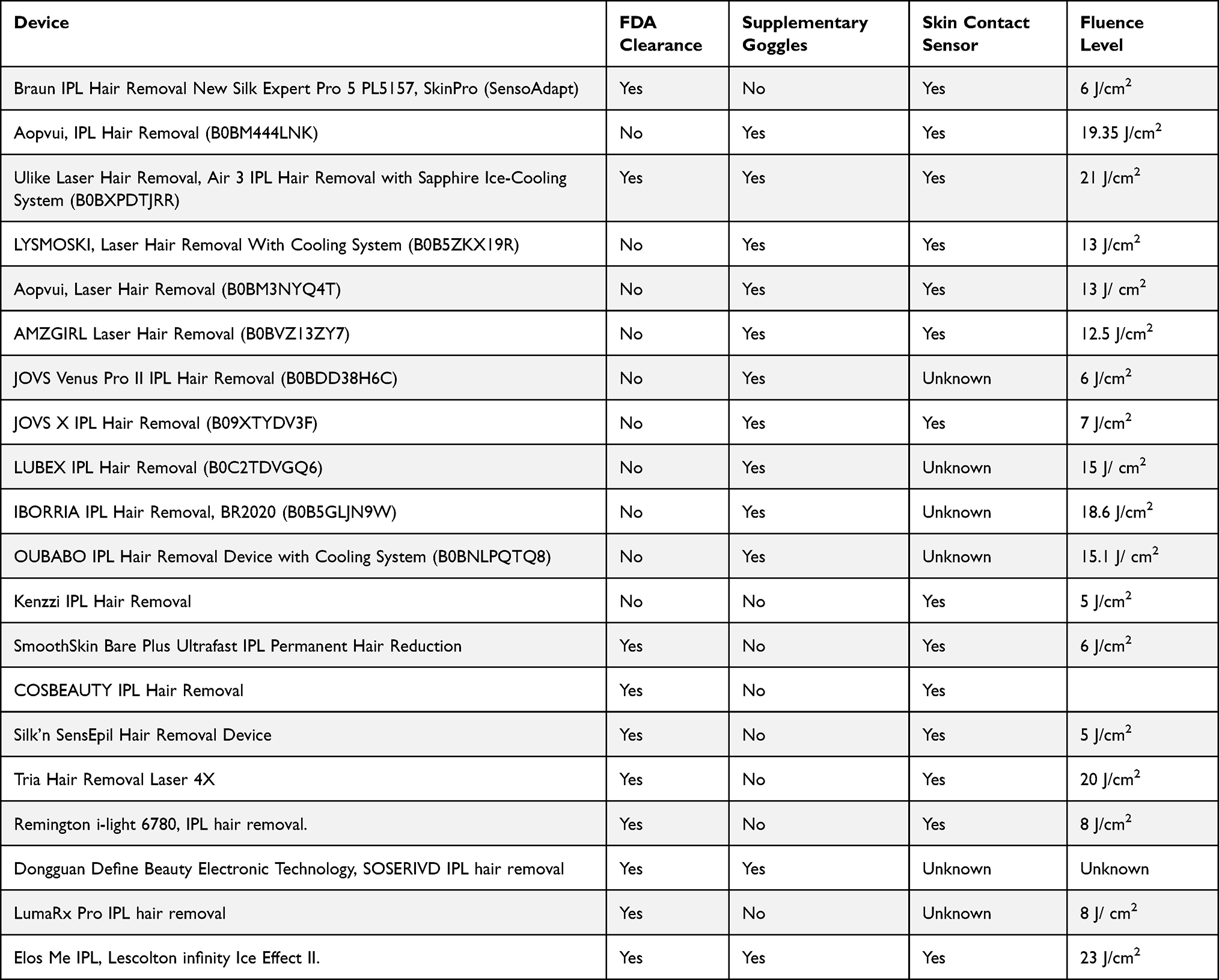 |
Table 3 Randomly Picked Online Available Light-Based Hair Removal Home Devices Manufacturing Properties |
Clinically, IPL-induced ocular injuries most commonly present with photophobia and most widely cause iris atrophy. Ocular pain, pupil irregularities, and visual disturbances are additional concerning symptoms. Early identification of the signs and symptoms is equally essential for both physicians and home device consumers to prevent further ocular damage and complications such as iris pigment flakes and subsequent glaucoma formation. Thought-provoking, in parallel with the reported laser-induced ocular injuries,37 IPL-induced ocular injuries showed left-side laterality as well, which might be triggered by the patient’s position during the procedure in relation to the operator’s dominant hand.
Conclusion
Light-based home devices are widely available in the market, in most of the world, their manufacturing process is not under strict medical safety regulations, and they are widely available in the markets. The available home devices are emitting IPL or diode lasers under the control of skin contact sensors, making the manufacturers of a good number of them not supplying the package with protective eyewear. Although the ocular damage identified in our paper was reported following IPL office-based devices, home devices can induce a similar pattern of injury that might be underreported. Given the cumulative evidence of the inaccurate light energy levels delivered by different in-office and home-based systems and the reported damage following exposure to 20–24 J/cm2 fluence levels, which are within the home-based device’s energy levels, the possible severe permanent consequences of the damage cannot be ignored. IPL-induced ocular damage most commonly affects the iris, causing permanent atrophy with devastating photophobia. Awareness of the ocular hazards of IPL devices must be raised, and protective eyewear should be supplied to consumers’ hands. Manufacturers should provide clear instructions on the device package regarding ocular hazards, the importance of using protective goggles, and a firm warning for consumers not to try to overcome the protective safety features of the sensors. Both practitioners and consumers must be aware of the signs and symptoms of possible ocular damage to seek prompt medical care.
Acknowledgement
We would like to thank Dr. Fatimah Almuqarrab for the figure 2 illustration artwork she painted.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Town G, Ash C, Dierickx C, Fritz K, Bjerring P, Haedersdal M. Guidelines on the safety of light-based home-use hair removal devices from the European society for laser dermatology. J Eur Acad Dermatol Venereol. 2012;26(7):799–811. doi:10.1111/j.1468-3083.2011.04406.x
2. Juhász MLW, Levin MK, Marmur ES. A review of available laser and intense light source home devices: a dermatologist’s perspective. J Cosmet Dermatol. 2017;16(4):438–443. doi:10.1111/jocd.12371
3. Lyngå C, Urban D. Non-Ionizing Radiation Protection: Summary of Research and Policy Options. First. (Wood AW, Karipidis K, Eds). John Wiley & Sons, Inc.; 2017.
4. Town G, V. BN, Uzunbajakava NE, et al. Light-based home-use devices for hair removal: why do they work and how effective they are? Lasers Surg Med. 2019;51(6):481–490. doi:10.1002/lsm.23061
5. Cohen M, Austin E, Masub N, Kurtti A, George C, Jagdeo J. Home-based devices in dermatology: a systematic review of safety and efficacy. Arch Dermatol Res. 2022;314(3):239–246. doi:10.1007/s00403-021-02231-0
6. Howick J, Chalmers I, Glasziou P, et al. Explanation of the 2011 Oxford Centre for Evidence-Based Medicine (OCEBM) levels of evidence (background document). Available from: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/explanation-of-The-2011-ocebm-levels-of-evidence/.
7. Thaysen-Petersen D, Bjerring P, Dierickx C, Nash JF, Town G, Haedersdal M. A systematic review of light-based home-use devices for hair removal and considerations on human safety. J Eur Acad Dermatol Venereol. 2012;26(5):545–553. doi:10.1111/j.1468-3083.2011.04353.x
8. FDA. Laser products and instruments. radiation-emitting products; 2023. Available from: https://www.fda.gov/radiation-emitting-products/home-business-and-entertainment-products/laser-products-and-instruments.
9. IEC. Safety of laser products - part 1: equipment classification and requirements. IEC 60825-1, international standard; 2014. Available from: https://webstore.iec.ch/publication/3587.
10. Kelechava B. Laser safety: class 1, 1C, 1M, 2, 2M, 3R, 3B, and 4. Available from: https://blog.ansi.org/2018/09/laser-class-safety-1-1c-1m-2-2m-3r-3b-4/#gref.
11. Malayanur D, Mysore VN. Laser safety eyewear. CosmoDerma. 2022;2:24. doi:10.25259/CSDM_15_2022
12. JBI. JBI’s critical appraisal tools, checklist for case reports. Available from: https://jbi.global/critical-appraisal-tools.
13. Brilakis HS, Holland EJ. Diode-laser–induced cataract and iris atrophy as a complication of eyelid hair removal. Am J Ophthalmol. 2004;137(4):762–763. doi:10.1016/j.ajo.2003.09.043
14. Carrancho García A, Garrote Llordén A, Cordero Coma M. Ocular complications secondary to diode laser-assisted eyebrow epilation. Arch Soc Esp Oftalmol. 2022;97(3):172–175. doi:10.1016/j.oftal.2020.09.006
15. Chang CY, Sheu SJ. Choroidal neovascularization secondary to intense pulsed light injury. Ophthalmic Plast Reconstr Surg. 2018;34(4):e129–e131. doi:10.1097/IOP.0000000000001142
16. Crabb M, Chan WO, Taranath D, Huilgol SC. Intense pulsed light therapy (IPL) induced iritis following treatment for a medial canthal capillary malformation. Australas J Dermatol. 2014;55(4):289–291. doi:10.1111/ajd.12137
17. Pang ALY, Wells K. Bilateral anterior uveitis after intense pulsed light therapy for pigmented eyelid lesions. Dermatol Surg. 2008;34(9):1276–1279. doi:10.1111/j.1524-4725.2008.34274.x
18. Javey G, Schwartz SG, Albini TA. Ocular complication of intense pulsed light therapy: Iris photoablation. Dermatol Surg. 2010;36(9):1466–1468. doi:10.1111/j.1524-4725.2010.01661.x
19. Halkiadakis I, Skouriotis S, Stefanaki C, et al. Iris atrophy and posterior synechiae as a complication of eyebrow laser epilation. J Am Acad Dermatol. 2007;57(2):S4–S5. doi:10.1016/j.jaad.2006.07.024
20. Herbold TM, Busse H, Uhlig CE. Bilateral cataract and corectopia after laser eyelid epilation. Ophthalmology. 2005;112(9):1634–1635. doi:10.1016/j.ophtha.2005.03.032
21. Jewsbury H, Morgan F. Uveitis and iris photoablation secondary to intense pulsed light therapy. Can J Ophthalmol. 2012;47(4):e13–e14. doi:10.1016/j.jcjo.2012.01.019
22. Hong S, Lee JR, Lim T. Pigment deposition of cosmetic contact lenses on the cornea after intense pulsed-light treatment. Korean J Ophthalmol. 2010;24(6):367. doi:10.3341/kjo.2010.24.6.367
23. Lee WW, Murdock J, Albini TA, O’Brien TP, Levine ML. Ocular damage secondary to intense pulse light therapy to the face. Ophthalmic Plast Reconstr Surg. 2011;27(4):263–265. doi:10.1097/IOP.0b013e31820c6e23
24. Maganti N, Kalbag NS, Gill MK. Macular hole formation associated with intense pulsed light therapy. Retin Cases Brief Rep. 2022;16(2):161–164. doi:10.1097/ICB.0000000000000947
25. Rho NK, Sa HS. Bilateral acute anterior uveitis after intense pulsed light treatment. Med Lasers. 2016;5(2):101–103. doi:10.25289/ML.2016.5.2.101
26. Nordqvist C, Fracheboud S, Guex-Crosier Y. Intense pulsed light eyebrow epilation and Iris lesion. Klin Monbl Augenheilkd. 2018;235(04):450–452. doi:10.1055/s-0043-124468
27. Durmus Ece BS. Macular burn secondary to diode laser epilation. Can J Ophthalmol. 2023;58(2):e95–e97. doi:10.1016/j.jcjo.2022.07.011
28. Passos ÂF, Borges DF. Iris atrophy after aesthetic treatment with intense pulsed light. Rev Bras Oftalmol. 2012;71(3):191–193. doi:10.1590/S0034-72802012000300010
29. Wessely D, Lieb W. Okuläre Komplikationen bei Diodenlaserepilation im Gesichtsbereich [Ocular complications of diode laser epilation in the area of the face. Loss of pupillary symmetry and pigment layer defect as well as coagulation of the ciliary body with intraocular inflammation caused by laser treatment]. Der Ophthalmologe. 2002;99(1):60–61. doi:10.1007/PL00007119
30. Sheikh A, Hodge W, Coupland S. Diode laser-induced uveitis and visual field defect. Ophthalmic Plast Reconstr Surg. 2007;23(4):321–323. doi:10.1097/IOP.0b013e3180a6f296
31. Jalian HR, Jalian CA, Avram MM. Common causes of injury and legal action in laser surgery. JAMA Dermatol. 2013;149(2):188. doi:10.1001/jamadermatol.2013.1384
32. Town G, Ash C, Eadie E, Moseley H. Measuring key parameters of intense pulsed light (IPL) devices. J Cosmet Laser Ther. 2007;9(3):148–160. doi:10.1080/14764170701435297
33. Eadie E, Miller P, Goodman T, Moseley H. Assessment of the optical radiation hazard from a home-use intense pulsed light (IPL) source. Lasers Surg Med. 2009;41(7):534–539. doi:10.1002/lsm.20801
34. Birtel J, Harmening WM, Krohne TU, Holz FG, Charbel Issa P, Herrmann P. Retinal injury following laser pointer exposure. Dtsch Arztebl Int. 2017;114(49):831–837. doi:10.1016/j.ajo.2003.09.043
35. Hattersley AM, Kiernan M, Goldberg D, et al. Assessment of adverse events for a home‐use intense pulsed light hair removal device using postmarketing surveillance. Lasers Surg Med. 2023;55(4):414–422. doi:10.1002/lsm.23650
36. FDA. 510(k) premarket notification; 2023. Available from: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfPMN/pmn.cfm.
37. Juhasz M, Zachary C, Cohen JL. Ocular complications after laser or light-based therapy—dangers dermatologists should know. Dermatologic Surg. 2021;47(5):624–629. doi:10.1097/DSS.0000000000002974
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.