Back to Journals » Journal of Pain Research » Volume 14
Is It Necessary to Approach the Severe Osteoporotic Vertebral Biconcave-Shaped Fracture Bilaterally During the Process of PKP?
Authors Tan B ![]() , Yang QY, Fan B, Lei C, Hu ZM
, Yang QY, Fan B, Lei C, Hu ZM
Received 15 December 2020
Accepted for publication 3 May 2021
Published 4 June 2021 Volume 2021:14 Pages 1601—1610
DOI https://doi.org/10.2147/JPR.S293528
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Erika Petersen
Bing Tan,1,2 Qi-Yuan Yang,2 Bin Fan,2 Chao Lei,2 Zhen-Ming Hu1
1Department of Orthopedic, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 2Department of Spine Surgery, The Third Hospital of MianYang, Sichuan Mental Health Center, Mianyang, People’s Republic of China
Correspondence: Zhen-Ming Hu
Department of Orthopedic, The First Affiliated Hospital of Chongqing Medical University, 1 Youyi Road, Chongqing, People’s Republic of China
Tel +8615284041340
Email [email protected]
Qi-Yuan Yang
Department of Spine Surgery, The Third Hospital of MianYang, Sichuan Mental Health Center, 190 Jiannan Road, Mianyang, People’s Republic of China
Tel +8615882889797
Email [email protected]
Purpose: The goal of this study was to explore the outcomes of unilateral and bilateral approach percutaneous kyphoplasty (PKP) using CT-guidance in the treatment of severe osteoporotic single-level vertebral biconcave-shaped fracture.
Methods: We retrospectively reviewed 89 patients with severe osteoporotic single-level vertebral biconcave-shaped fracture who had undergone unilateral and bilateral PKP surgeries using CT-guidance at our hospital between June 2013 and June 2019, and followed for at least 1 year. All patients were divided into unilateral (the transverse process-pedicle approach, n = 49) and bilateral (the pedicle approach, n = 40) groups. We collected the clinical and radiological evaluation results during postoperative and last follow-up periods.
Results: Our findings revealed that the surgery time for the unilateral group was significantly shorter than that of the bilateral group at P < 0.05. The amount of bone cement and radiation exposure of the unilateral group were significantly lesser than that of the bilateral group (P < 0.05). Relative to preoperative data, the values of the VAS score and Oswestry disability index (ODI) were significantly improved at 1 day after surgery and the last follow-up in the two groups (P < 0.05). Notably, the median height of vertebra at 1 day after surgery and the last follow-up in the unilateral group was significantly restored than that of preoperative data (P < 0.05). However, the median height of vertebra at the same time intervals in the bilateral group showed no significant change compared with preoperative data (P > 0.05). Furthermore, the rate of bone cement leakage and incidence of adjacent-level vertebra fracture were not significantly different in the two groups (P > 0.05). Finally, both groups can obtain an asymmetrical distribution of bone cement in the vertebra.
Conclusion: Compared to the bilateral PKP, unilateral PKP using CT-guidance in the treatment of the sOVBFs exhibits significantly shorter operation time, lesser radiation dose, and complications. Moreover, unilateral PKP can restore the median height of the vertebral body and eventually obtain a symmetrical distribution of bone cement in the vertebra.
Keywords: severe biconcave-shaped fracture, percutaneous kyphoplasty, osteoporosis, unilateral/bilateral approach
Introduction
Osteoporosis-related fractures are one of the major complications of osteoporosis especially in people aged over 50, in which the incidence is about 30–50% globally. It is projected that the number of cases will reach 5.99 million cases per year by 2050 in China.1,2 Furthermore, osteoporosis-related fractures primarily include hip, wrist, and vertebral fractures.1 In particular, osteoporotic vertebral fractures (OVFs) cause activity limitation, severe back pain, and reduce the quality of life of patients.2,3 Several studies have characterized OVFs into wedge, biconcave, and compression fractures in the X-ray lateral position.4,5 Biconcave-shaped fractures are predominantly presented as the simultaneous collapse of the upper and lower bony endplates in the middle of the vertebra, while the collapse of both sides of the vertebral body is not obvious or balanced.4 In addition, biconcave fractures are classified into mild, moderate, and severe deformity based on the degree of concavity.4,5 Notably, percutaneous vertebroplasty (PVP) and percutaneous kyphoplasty (PKP) can relieve back pain and subsequently, achieve good clinical values in the treatment of OVFs.6,7 A recent study has demonstrated that PKP holds a greater advantage than PVP, particularly in the restoration of the middle vertebral height and fewer cement leakages for the osteoporotic vertebral biconcave fractures (OVBFs).4
Currently, the approaches of PKP are mainly unilateral and bilateral, and both methods have their advantages and disadvantages.8,9 Specifically, bilateral PKP can obtain better bone cement distribution, lesser risks of puncture, and better recovery of the rigidity and strength of the vertebral body in the treatment of OVFs compared to the unilateral PKP. On the other hand, unilateral PKP requires less radiation dose, operation time, and volume of cement than the bilateral PKP.10,11 Recently, some studies have revealed that the unilateral PKP can restore the height of the vertebral body and distinctively reduce the pain of patients who are suffering from very severe osteoporotic vertebral compression fractures. Of note, its clinical efficacy and safety were comparably satisfactory with that of bilateral PKP.3,6,8 However, it remains unknown which puncture approach should be preferred in the PKP treatment for sOVBFs.
The median height of the sOVBFs’ vertebra has collapsed to less than one-third of its original height. Therefore, the unilateral approach exhibits extreme risk and asymmetric distribution of bone cement in the vertebra under the C-arm guidance.12 However, a question remains: can we only choose a bilateral approach in the treatment of the sOVBFs with PKP? To answer this question, we herein analyzed the clinical data of 89 patients with single-level thoracolumbar sOVBF between September 2013 and September 2019 at our hospital. We also investigated the clinical effects and security of unilateral PKP under CT-guidance in the treatment of sOVBFs compared with the bilateral PKP.
Materials and Methods
Study Population Selection
We performed a retrospective case-control study on 89 patients (including 23 men, 66 women; the age range, 65–93 years, mean, 71.6±5.4 years) with sOVBFs from the authors’ hospital between June 2013 and June 2019. All patients received PKP surgery under CT-guidance and were divided into two groups: 49 cases received unilateral puncture at the transverse process-pedicle approach (unilateral group), while 40 cases received bilateral pedicle approach (bilateral group). The intraoperative CT scan of the vertebral was feasible using digital subtraction angiography (DSA) (Digital Subtraction Angiography, Siemens, US). The procedures were performed in the hybrid operating room. The detailed general information of the patients in the two groups, which are comparable (P > 0.05) is summarized in Table 1. All patients enrolled in this study met the following inclusion criteria: (1) bone mineral density (BMD) T ≤ − 2.5; (2) no prior history of PKP or PVP surgery; (3) the patients who had a history of trauma and suffered from single level sOVBF; (4) the vertebra that was hyperintense on T2-weighted images, and hypointense on T1-weighted images. Then, we related patients with stubborn and increasing back pain to postural changes. However, herein the patients who met the following exclusion criteria were excluded: (1) pathological fractures caused by metastatic tumors, primary tumors, and infectious diseases such as tuberculosis; (2) fracture blocks that compressed the spinal cord or nerve roots and caused neurological dysfunction; (3) the patients who had a history of PKP or PVP operation; (4) the patients suffering from severe coagulopathy. The function of cardiopulmonary was so weak that it cannot tolerate surgery. This study was performed in conformity with the Declaration of Helsinki and approved by the ethics committee of the Third Hospital of Mianyang (2020, Reviewed, No.22). Finally, due to the retrospective design of this work, there is no need to obtain informed consent from patients. All data were collected and analyzed anonymously.
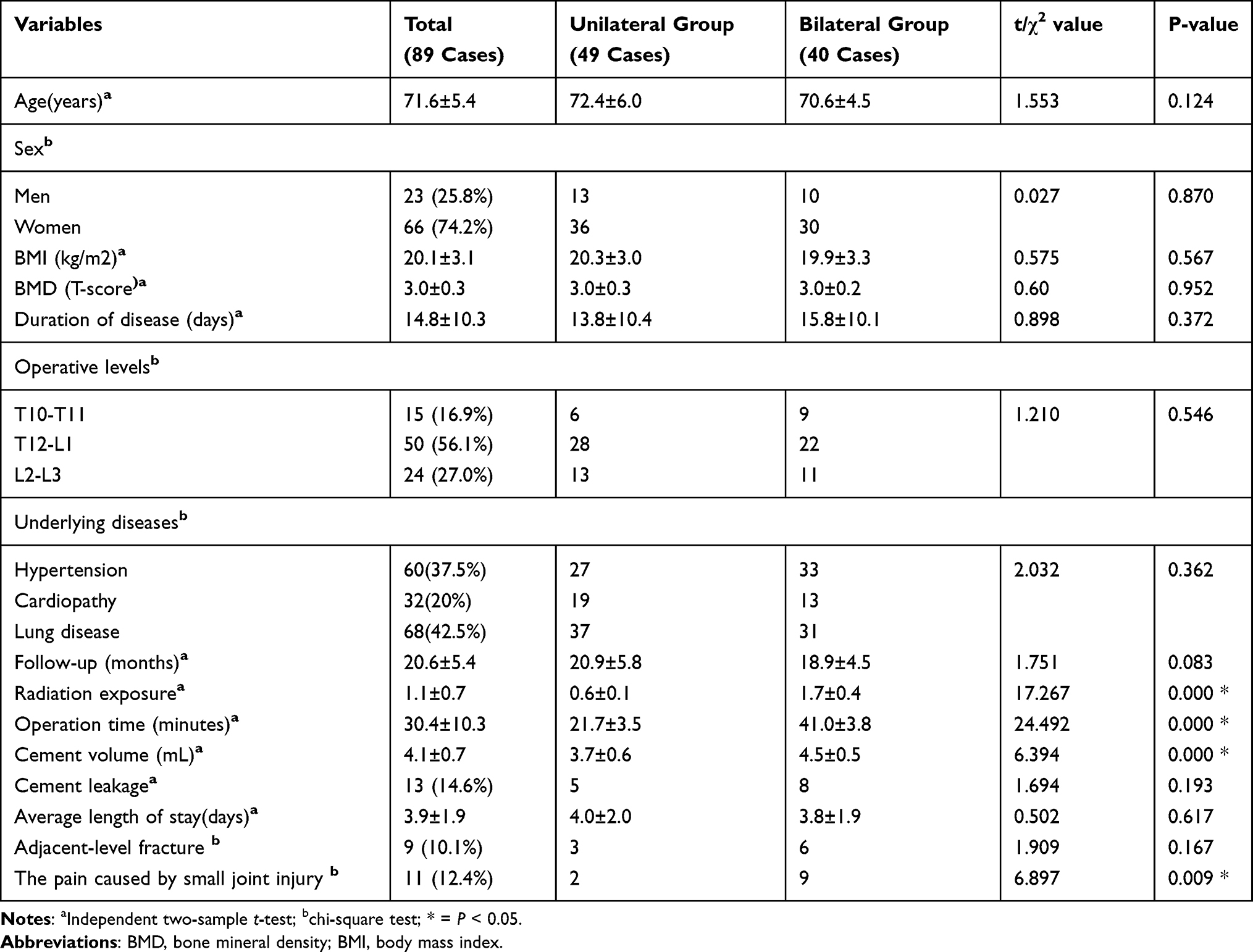 |
Table 1 Patient Demographics of the Two Groups (Unilateral and Bilateral Groups) |
Surgical Management
The same senior surgeon performed the surgery for all patients. The patients who received local anesthesia were laid in a prone position on the radiolucent operating table and subsequently, placed a radiometer on their waist that was used to record the amount of radiation exposure. Afterward, a special mesh marker was placed on the skin of the patient’s back, the pedicle of the responsible vertebra was located under DSA fluoroscopy, while the incision location was marked based on the preoperative computed tomography (CT, including sagittal reconstruction). Using a CT scan obtained with DSA, we identified the entry point of a puncture during operation. In the unilateral group (Figure 1), taking a surgical incision about 0.5 cm, we identified the position of the puncture needle using DSA. Moreover, we adjusted the puncture needle position based on CT images under DSA. This prevents damages to the upper and lower endplates (Figure 2). After the puncture needle tip passed through the pedicle, we then increased the camber angle to ensure the needle gets in the right place (Figure 3). Finally, we established a working channel on the posterior 1/3 of the vertebral body by inserting a fine drill through the working channel. Subsequently, we carefully expanded the medulla to the front 1/3~ 1/4 of the vertebral body under lateral position, insert a balloon, and eventually, inject a contrast agent to expand the balloon (Figure 4). Then, the balloon was removed. Consequently, bone cement was injected at a suitable time. In the bilateral group (Figure 5); we first determined the puncture point using the Magerl method13 (Figure 6) and simultaneous bilateral puncture by using CT-guidance. We then adjusted the puncture needle position based on CT images under DSA. At last, we established a working channel, expanded with balloons on both sides, and injected bone cement at a suitable period. Notably, we observed dynamically the injection and leakage of bone cement using a CT scan during the surgery. We noted that patients can walk by themselves after postoperative for four to six hours. All patients were treated with zoledronate, calcium carbonate, and vitamin D after the surgery.
 |
Figure 1 A 80-year-old male patient who suffered from L2 serve OVBF caused by minor trauma, and CT-guided unilateral approach PKP was performed 15 days after the injury; (A) preoperative X-ray showed serve biconcave-shaped fracture of L2 vertebra. (B) Preoperative CT showed mid-height of L2 vertebra with severe collapse. (C) Preoperative T2 sagittal MRI indicated an acute recent fracture of L2 vertebra. (D) Plain lateral radiography showed mid-height of fractured vertebrae which was significantly restored at postoperative day 8. (E) The mid-height of fractured vertebrae, which was improved and maintained at the last follow-up. |
 |
Figure 2 The lumbar sagittal via CT scan. |
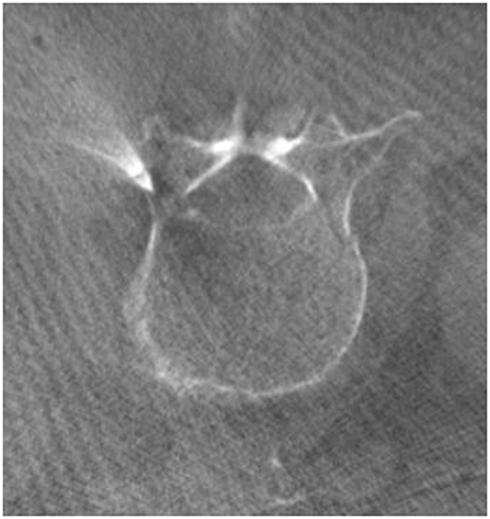 |
Figure 3 The lumbar cross-section via CT scan (the unilateral approach). |
 |
Figure 4 Balloon dilation and reduction in the X-ray lateral view (the unilateral approach). |
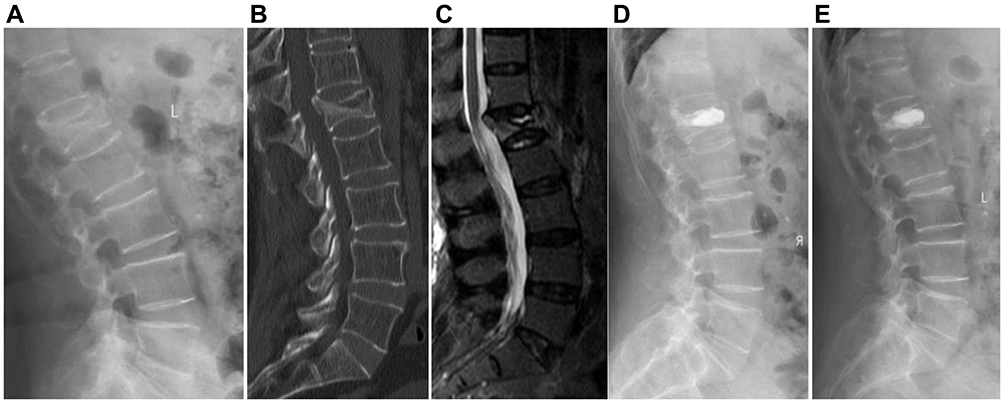 |
Figure 5 A 76-year-old female patient who suffered from L1 serve OVBF caused by trauma, and CT-guided bilateral approach PKP was performed 20 days after the injury; (A) preoperative X-ray showed serve biconcave-shaped fracture of L1 vertebra. (B) Preoperative CT showed mid-height of L1 vertebra with severe collapse; (C) Preoperative T2 sagittal MRI showed an acute recent fracture of L1 vertebra. (D) Plain lateral radiography showed mid-height of fractured vertebrae that was significantly restored at postoperative day 8. (E) The mid-height of fractured vertebrae, which was improved and maintained at the last follow-up. |
 |
Figure 6 The lumbar cross-section using CT scan (the bilateral approach). |
Evaluation Criteria
For this study, three independent authors collected the clinical data, which included clinical and radiological evaluation results before the operation, on postoperative day 1, and at the last follow-up. We used a same Dual-Energy X-Ray Absorptiometry (General Electric Company, America) to measure BMD. All patients were followed up for more than 1 year after surgery. We recorded data on operation time, radiation exposure, and bone cement injection in the two groups. To evaluate the clinical efficacy and recovery of spinal function on postoperative day 1 and during the last follow-up, we used the visual analog scale (VAS) and Oswestry Disability Index (ODI). The mid-heights of the injured vertebrae as well as the mid-height of the upper and lower vertebrae of the injured vertebrae were measured using lateral X-rays before the operation,1 day after the operation, and at the last follow-up. The calculating formula was as follows: The value of mid-height of the injured vertebra = (The mid-height of the injured vertebra/Average height of upper and lower vertebral bodies) × 100%. Lastly, we divided the vertebral body into six areas to assess the mechanical properties of the vertebral body after the operation, and each area can be further subdivided into left and right areas14 (Figure 7).
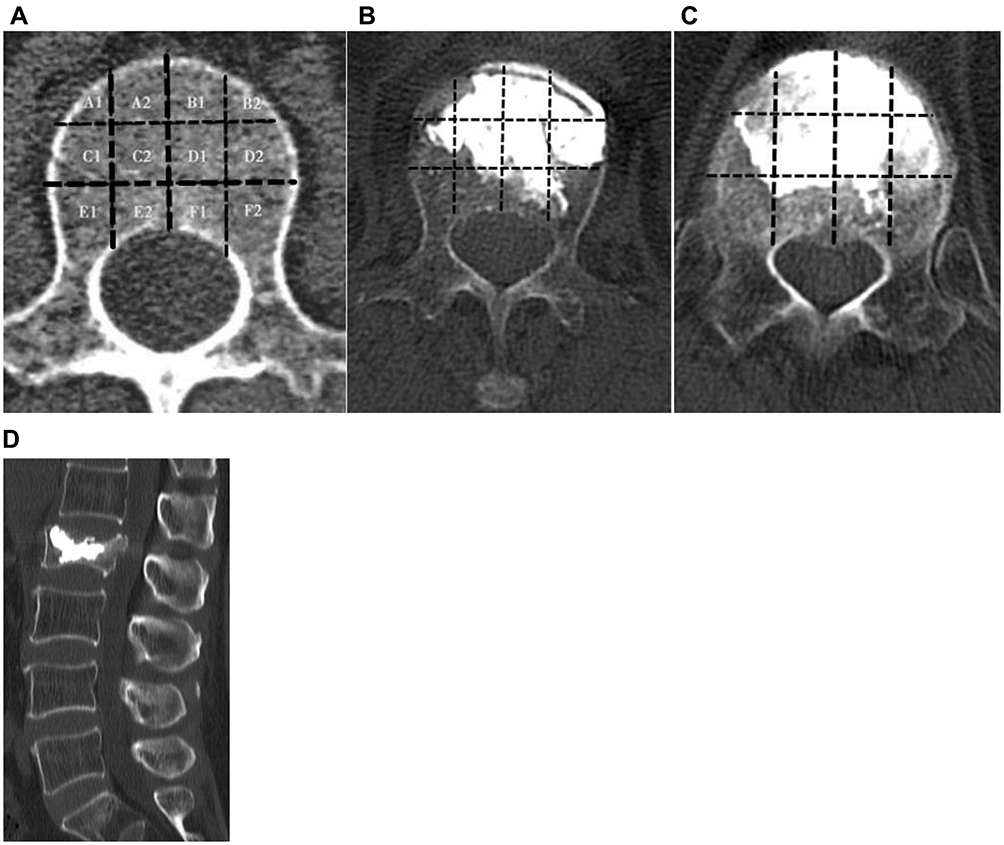 |
Figure 7 Comparison of the distribution of bone cement in the vertebra between the two groups. (A) Dividing the vertebral cross-section into 12 regions and we used the A1, A2, B1, B2, C1, C2, D1, D2, E1, E2, F1, F2 to represent each area. (B) The unilateral group with bone cement primarily distributed in areas A2, B, C2, and D. (C) The bilateral group with bone cement mainly distributed in areas A, B, C, and D. (D) The unilateral group with bone cement distributed well on sagittal spinal. |
Statistical Analysis
All statistical data analyses were executed using SPSS software, version 23.0 (SPSS Inc, Chicago, IL, USA). Data are expressed as mean ± SD. The significant difference between preoperative and postoperative measurements of VAS score, ODI index, and mid-height of fractured vertebrae for each group was confirmed using paired-samples t-test. Additionally, an independent two-sample t-test was used to test a significant difference between the two groups, whereas the chi-squared test (Fisher’s exact test for small samples) was employed to analyze the categorical data in the two groups. For all analyses, a level of P < 0.05 was considered statistically significant.
Results
Overall, 89 patients were enrolled in this study who comprised of 23 men and 66 women (age range, 65–93 years, mean 71.6±5.4 years). All patients were followed up for 12–31 months, with an average of 20.6±5.3 months. We observed no significant differences in age, sex, BMI, BMD, duration of disease, operative levels, the average length of stay, underlying diseases, follow-up and average length of stay between unilateral and bilateral groups (P > 0.05, Table 1). The operation time of the unilateral group (21.7±3.5 minutes) was significantly shorter compared to that of the bilateral group (41.0±3.8 minutes) at P < 0.05. Besides, the amount of bone cement (3.7±0.6 mL) and radiation exposure (0.6±0.1 mSv) of the unilateral group was significantly lower than that of the bilateral group (4.5±0.5 mL, 1.7±0.4 mSv), respectively (P < 0.05, Table 1). The rate of cement leakage was 14.6% (in total 13 cases with 5 cases in the unilateral and 8 cases in the bilateral groups), without the symptoms of spinal cord injury and pulmonary embolism. Additionally, the rate of bone cement leakage was not significantly different in the two groups (c2 = 1.694, P > 0.05, Table 1). The incidence of adjacent-level fracture was 10.1% (overall, 9 cases, with 3 cases in the unilateral and 6 cases in the bilateral groups) during the follow-up period, whereas that of vertebra fracture revealed no significant differences in the two groups (c2 = 1.909, P > 0.05). The pain caused by small joint injury during operation occurred in 11 cases (rate, 12.4%, with 2 cases in the unilateral group and 9 cases in the bilateral group), and was significantly different in the two groups (c2 = 6.897, P < 0.05). Subsequently, patients received physical therapy to relieve their symptoms.
Relative to preoperative data, the values of the VAS score and Oswestry disability index (ODI) were significantly improved at 1 day after surgery and the last follow-up in the two groups (P < 0.05, Table 2) and there was no statistical difference between unilateral and bilateral groups (P > 0.05, Table 2). The median height of vertebra at 1 day after surgery and the last follow-up in the unilateral group was significantly restored than that of preoperative data (P < 0.05, Table 2). However, the median height of vertebra at the same time intervals in the bilateral group showed no significant change compared with preoperative data (P > 0.05, Table 2).
 |
Table 2 Comparison of Surgical Results Between Unilateral and Bilateral Groups in Patients with Severe OVBF |
In comparison, the bone cement of the unilateral group was primarily distributed in the front and middle of the vertebral body (A2, B1, C2, D1), while that of the bilateral group was prevalent in the front 2/3 area of the vertebral body (A, B, C, D). In summary, after the operation, there were no serious adverse events such as infection, the displacement, or abscission of bone cement in these patients in the two groups.
Discussion
With the advent of an aging society, the incidence of OVBFs also shows a rising trend. Based on the examination of preoperative lateral X-ray, OVBFs are graded on the basis of the extent of central vertebrae collapse: mild (20%-25%), moderate (25%-40%), and severe (>40%) deformity.5 On the other hand, PKP and PVP are the primary surgical approaches for the treatment of OVFs.14,15 Gan M et al4 found that PKP holds a greater advantage than PVP, particularly in the restoration of the middle vertebral height and fewer cement leakages for the OVBFs. However, it remains unknown which puncture approach should be preferred in the PKP treatment for sOVBFs. Our study demonstrated that unilateral PKP under CT-guidance is more safe and effective than bilateral PKP in the treatment of sOVBFs.
The surgical approach of PKP for the treatment of OVBFs is mainly bilateral pedicle puncture and previous reports highlight that bilateral PKP can obtain good bone cement distribution and restore the strength of the vertebral body.4 Compared with the unilateral PKP, bilateral PKP needed longer operation time, more X-ray exposure, and increased occurrence risk of cardiovascular and cerebrovascular events.16 It also significantly increased the incidence of puncture complications.17 The abduction angle of the bilateral PKP was smaller, and the balloon cannot reach the middle of the vertebral body, hence leading to failure to restore the middle height of the vertebra.16,17 The sOVBFs occurred more frequently especially in elderly people with poor cardiopulmonary function and who cannot maintain a prone position for a long time. Therefore, the treatment of sOVBFs with bilateral PKP remains controversial. Some scholars have suggested the use of unilateral PKP to treat mild and moderate OVBFs.4,8 However, sOVBFs exhibit less residual bone in the middle of the vertebral body, which requires extreme puncture accuracy that is difficult to achieve when using the unilateral PKP under the guidance of C-arm. As a result, this may damage the upper and lower bone endplates and increase the incidence of bone cement leakage.12,17 The angle of the unilateral PKP is too small to reach or pass through the mid-line of the vertebra and resulting in an asymmetric distribution of bone cement.18 However, if we increased the angle between the puncture needle and the sagittal plane, it is easy to penetrate the spinal canal and damage the spinal cord or nerve roots, leading to serious consequences.19 Thus, the question remains: How can we reduce the risk of unilateral PKP treatment for sOVBFs, accurately puncture, restore the middle height of the vertebral body and obtain excellent bone cement distribution? To address this problem, we selected the junction of the transverse process and superior articular process as the unilateral PKP puncture point and did the precise puncture of the vertebral body using CT guidance during operation.20 This technique avoids damage to the upper and lower endplates of sOVBFs, and the position of the balloon was beyond the mid-line of the vertebral body in unilateral PKP cases. After the balloon was expanded and formed, the middle height of the vertebral body was clearly restored. Our finding that the postoperative median height of vertebra in the unilateral group (62.3±7.4%) was significantly restored than that of preoperative data (37.7±9.7%, P < 0.05). However, the median height of vertebra at the same time intervals in the bilateral group (37.5±9.3) showed no significant change compared with preoperative data (37.7±9.2, P > 0.05). The present data confirmed that unilateral PKP is more advantageous for the restoration of the median height of vertebral body than that of bilateral PKP. The results of this study show that compared to the bilateral PKP, the unilateral PKP via CT-guidance for the treatment of sOVBFs has lesser radiation exposure and significantly shorter operation time. It can also reduce the number of puncture tools, surgical costs, and complications. Thus, this technology is essential particularly to elderly people who have poor cardiorespiratory function and cannot tolerate long-term beds. The present data shown that relative to preoperative data, the values of the VAS score and Oswestry disability index (ODI) were significantly improved at 1 day after surgery and the last follow-up in the two groups (P < 0.05) and there was no statistical difference between unilateral and bilateral groups. This demonstrated that both unilateral and bilateral PKP can relieve back pain and increase the quality of life. For bone defects in the middle of the vertebral body measured using CT was less than 5 mm, hence we did not recommend doing the unilateral PKP. In addition, if there is a bone defect in the middle of the vertebral body, unilateral PKP will inevitably cause bone cement leakage into the intervertebral space, increasing the risk of re-fracture after surgery. Because of the puncture needle (Aide, Suzhou, China) which was used in our hospital with a minimum diameter of 3.5 mm, if the middle height of the vertebral body is less than 5 mm, the upper and lower endplates are easily damaged during the puncture process, causing bone cement leakage into the intervertebral space.
Based on data from this study, we herein summarize the advantages of the unilateral PKP via CT-guidance for the treatment of sOVBFs including (1) during operation, the position of the puncture needle can be precisely adjusted using CT images to avoid the puncture needle from damaging the upper and lower endplates, thus making the working channel reach or exceed the mid-line of the vertebra. All cases are adjusted to satisfaction at one time and this can reduce the number of punctures and radiation exposure. Additionally, it reduced puncture complications and operation time. (2) The unilateral PKP via CT-guided is safe and efficient, which rarely causes complications of the spinal cord, nerve, and surrounding important blood vessels. Furthermore, it is easier for young physicians to study. (3) We dynamically observed the distribution of bone cement, then adjust the direction of bone cement injection using a CT scan. The bone cement leakage can be revealed on time, in which we can reduce the occurrence of bone cement leakage. (4) The biggest hindrance of unilateralPKP is the asymmetric distribution of bone cement in the vertebra. The biomechanical effect of the vertebrae is different with the distribution of bone cement in different areas of the vertebral body. The best distribution of bone cement was in the front 2/3 (A, B, C, D area) of the vertebral body.21,22 In this study, the distribution of bone cement in the vertebral body in the unilateral group was close to the anterior 2/3 of the vertebral body (A2, B, C2, and D area), which achieved an ideal distribution of bone cement in the vertebral body. In comparison, this distribution in the unilateral group was equivalent to the ideal distribution of the bilateral group. Complications of PKP surgery primarily included bone cement leakage, puncture damage to surrounding structures (facet joints, spinal cord, and blood vessels), and pulmonary embolism.23 The rate of bone cement leakage was not significantly different in the two groups. This supported the fact that the rate of bone cement leakage is not associated with the puncture approach of PKP. In this study, we recorded that the rate of bone cement leakage was primarily associated with higher fracture severity grade, speed of bone cement injection, and larger volume of bone cement.24 Postoperative pain in the puncture site of the unilateral group was lesser than that of the bilateral group. The main reason is that the precise unilateral puncture through CTguidance does not need repeated adjustments. Compared to the bilateral group, the unilateral puncture point was outside the articular process, which significantly reduces the damage to the facet joints. Elsewhere, a study reported that the incidence of adjacent vertebral body fractures after PKP was about 7–19%, which may be caused by the progress of osteoporosis and the bone cement fusion harden the vertebrae after PKP and adjacent vertebra fractures after PKP may be associated with reducing spinal mobility and increasing stress on adjacent vertebral bodies.25 In this work, adjacent vertebral body fractures occurred in 9 cases after PKP. In particular, the 9 patients did not take anti-osteoporosis drugs and calcium regularly and thus osteoporosis was not controlled. The measurement of bone density demonstrated that the degree of osteoporosis was worse than before. A study by Scholten et al26 concluded that regular anti-osteoporosis drugs and calcium after PKP can reduce the incidence of adjacent vertebral fractures. Therefore, we hereby recommend that patients be routinely given regular anti-osteoporosis treatment after PKP and supervised throughout the process.
Conclusion
In summary, this study shows that both unilateral and bilateral PKP can significantly alleviate the pain of patients with sOVBFs. We also noted that the rate of bone cement leakage is not associated with the puncture approach of PKP. Compared to the bilateral PKP, unilateral PKP via CT-guided techniques in the treatment of the sOVBFs exhibited significantly shorter operation time, lesser radiation dose, and complications. Moreover, unilateral PKP can restore the median height of the vertebral body and obtain a symmetrical distribution of bone cement in the vertebra. However, this study was only a retrospective study with limited data because of the small sample size. Therefore, a large sample multicenter study is required so as to confirm these promising results.
Acknowledgments
The study was not supported by any financial funding. No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no competing interests in this work.
References
1. Si L, Winzenberg TM, Jiang Q, et al. Projection of osteoporosis-related fractures and costs in China: 2010–2050. Osteoporos Int. 2015;26(7):1929–1937. doi:10.1007/s00198-015-3093-2
2. Wu CH, Tu ST, Chang YF, et al. Fracture liaison services improve outcomes of patients with osteoporosis-related fractures: a systematic literature review and meta-analysis. Bone. 2018;111(7):92–100. doi:10.1016/j.bone.2018.03.018
3. Wang F, Wang LF, Miao DC, et al. Which one is more effective for the treatment of very severe osteoporotic vertebral compression fractures: PVP or PKP? J Pain Res. 2018;28(11):2625–2631. doi:10.2147/JPR.S179022
4. Gan M, Zou J, Song D, et al. Is balloon kyphoplasty better than percutaneous vertebroplasty for osteoporotic vertebral biconcave-shaped fractures? Acta Radiol. 2014;55(8):985–991. doi:10.1177/0284185113511603
5. Genant HK, Wu CY, van Kuijk C, et al. Vertebral fracture assessment using a semiquantitative technique. J Bone Miner Res. 1993;8(9):1137–1148. doi:10.1002/jbmr.5650080915
6. Wu AM, Li XL, Li XB, et al. The outcomes of percutaneous kyphoplasty in treatment of the secondary osteoporotic vertebral compression factures: a case-control study. Ann Transl Med. 2018;6(6):107–113. doi:10.21037/atm.2018.02.17
7. Herad M, Rosengren BE, Hasserius R, et al. Low clinical relevance of a prevalent vertebral fracture in elderly men–the MrOs Sweden study. Spine J. 2015;15(2):281–289. doi:10.1016/j.spinee.2014.09.016
8. Liu MX, Xia L, Zhong J, et al. Is it necessary to approach the compressed vertebra bilaterally during the process of PKP? J Spinal Cord Med. 2020;43(2):201–205. doi:10.1080/10790268.2018.1451238
9. Wang H, Sribastav SS, Ye F, et al. Comparison of Percutaneous Vertebroplasty and Balloon Kyphoplasty for the Treatment of Single Level Vertebral Compression Fractures: a Meta-analysis of the Literature. Pain Physician. 2015;18(3):209–222.
10. Huang Z, Wan S, Ning L, et al. Is unilateral kyphoplasty as effective and safe as bilateral kyphoplasties for osteoporotic vertebral compression fractures? A meta-analysis. Clin Orthop Relat Res. 2014;472(9):2833–2842. doi:10.1007/s11999-014-3745-0
11. Zhuang Y, Yang L, Li H, et al. A novel technique of unilateral percutaneous kyphoplasty achieves effective biomechanical strength and reduces radiation exposure. Am J Transl Res. 2016;8(2):1172–1179.
12. Cheng X, Long HQ, Xu JH, et al. Comparison of unilateral versus bilateral percutaneous kyphoplasty for the treatment of patients with osteoporosis vertebral compression fracture (OVCF): a systematic review and meta-analysis. Eur Spine J. 2016;25(11):3439–3449. doi:10.1007/s00586-016-4395-6
13. Magerl FP. Stabilization of the lower thoracic and lumbar spine with external skeletal fixation. Clin Orthop Relat Res. 1984;18(9):125–141.
14. Pelletier MH, Lau AC, Smitham PJ, et al. Pore distribution and material properties of bone cement cured at different temperatures. Acta Biomater. 2010;6(3):886–891. doi:10.1016/j.actbio.2009.09.016
15. Li YX, Guo DQ, Zhang SC, et al. Risk factor analysis for re-collapse of cemented vertebrae after percutaneous vertebroplasty (PVP) or percutaneous kyphoplasty (PKP). Int Orthop. 2018;42(9):2131–2139. doi:10.1007/s00264-018-3838-6
16. He X, Li H, Meng Y, et al. Percutaneous Kyphoplasty Evaluated by Cement Volume and Distribution: an Analysis of Clinical Data. Pain Physician. 2016;19(7):495–506.
17. Zhiyong C, Yun T, Hui F, et al. Unilateral Versus Bilateral Balloon Kyphoplasty for Osteoporotic Vertebral Compression Fractures: a Systematic Review of Overlapping Meta-analyses. Pain Physician. 2019;22(1):15–28.
18. Lee JH, Lee DO, Lee JH, et al. Comparison of radiological and clinical results of balloon kyphoplasty according to anterior height loss in the osteoporotic vertebral fracture. Spine J. 2014;14(10):2281–2289. doi:10.1016/j.spinee.2014.01.028
19. Wang H, Zhang Z, Liu Y, et al. Percutaneous kyphoplasty for the treatment of very severe osteoporotic vertebral compression fractures with spinal canal compromise. J Orthop Surg Res. 2018;13(1):13. doi:10.1186/s13018-018-0719-z
20. Wang H, Hu P, Wu D, et al. Anatomical feasibility study of unilateral percutaneous kyphoplasty for lumbar through the conventional transpedicular approach: an observational study using 3D CT analysis. Medicine. 2018;97(37):e12314. doi:10.1097/MD.0000000000012314
21. Zhang L, Wang Q, Wang L, et al. Bone cement distribution in the vertebral body affects chances of recompression after percutaneous vertebroplasty treatment in elderly patients with osteoporotic vertebral compression fractures. Clin Interv Aging. 2017;12:431–436. doi:10.2147/CIA.S113240
22. Baorong HE, Zhengwei XU, Ha DJ, et al. Biomechanical effect of bone cement volume and distribution on lumbar vertebral body with osteoporotic fracture. Chin J Orthop. 2012;32(8):768–773.
23. Yilmaz A, Çakir M, Yücetaş CŞ, et al. Percutaneous Kyphoplasty: is Bilateral Approach Necessary? Spine. 2018;43(14):977–983. doi:10.1097/BRS.0000000000002531
24. Zhu SY, Zhong ZM, Wu Q, et al. Risk factors for bone cement leakage in percutaneous vertebroplasty: a retrospective study of four hundred and eighty-five patients. Int Orthop. 2016;40(6):1205–1210. doi:10.1007/s00264-015-3102-2
25. Zhang H, Xu C, Zhang T, et al. Does Percutaneous Vertebroplasty or Balloon Kyphoplasty for Osteoporotic Vertebral Compression Fractures Increase the Incidence of New Vertebral Fractures? A Meta-Analysis. Pain Physician. 2017;20(1):E13–E28. doi:10.36076/ppj.2017.1.E13
26. Scholten DJ, Bray JK, Wang KY, et al. Implementation of a fracture liaison service and its effects on osteoporosis treatment adherence and secondary fracture at a tertiary care academic health system. Arch Osteoporos. 2020;15(1):80. doi:10.1007/s11657-020-00736-1
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.