Back to Journals » Cancer Management and Research » Volume 6
Is extended-field concurrent chemoradiation an option for radiologic negative paraaortic lymph node, locally advanced cervical cancer?
Authors Al Asiri M, Tunio M ![]() , Mohamed R, Bayoumi Y, Alhadab A, Saleh RM, AlArifi M, Alobaid A, Abdulmoniem R
, Mohamed R, Bayoumi Y, Alhadab A, Saleh RM, AlArifi M, Alobaid A, Abdulmoniem R
Received 23 May 2014
Accepted for publication 27 June 2014
Published 9 September 2014 Volume 2014:6 Pages 339—348
DOI https://doi.org/10.2147/CMAR.S68262
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Mushabbab Al Asiri,1 Mutahir A Tunio,1 Reham Mohamed,2 Yasser Bayoumi,2 Abdulrehman Alhadab,1 Rasha M Saleh,3 Muhannad Saud AlArifi,1 Abdelaziz Alobaid4
1Radiation Oncology, Comprehensive Cancer Center, King Fahad Medical City, Riyadh, Saudi Arabia; 2Radiation Oncology, National Cancer Institute, Cairo University, Cairo, Egypt; 3Medical Oncology, Comprehensive Cancer Center, King Fahad Medical City, Riyadh, Saudi Arabia; 4Women's Specialized Hospital, King Fahad Medical City, Riyadh, Saudi Arabia
Background: The aim was to evaluate whether extended-field concurrent chemoradiation (EF-CCRT) leads to results better than those obtained by standard whole-pelvis concurrent chemoradiation (WP-CCRT) in locally advanced cervical cancer with radiologic negative paraaortic lymph nodes (PALNs).
Patients and methods: A total of 102 patients with histopathologically proven squamous cell carcinoma, adenocarcinoma, or adenosquamous cell carcinoma, and radiologic negative PALN locally advanced cervical cancer, stage IIB-IVA, were accrued between July 2007 and April 2008 and were randomly assigned to WP-CCRT (50 patients) or EF-CCRT (52 patients), followed by high-dose rate brachytherapy. Data regarding the safety profile, response rates, and occurrence of local, PALN, or distant failure were recorded.
Results: During a median follow-up time of 60 months (18–66), 74/102 patients completed the treatment protocol and were analyzed. Overall PALN, distant-metastasis control, disease-free survival, and overall survival rates were 97.1%, 86.9%, 80.3%, and 72.4% in EF-CCRT respectively in comparison with WP-CCRT (82.1%,74.7%, 69.1%, and 60.4%), with P-values of 0.02, 0.03, 0.03 and 0.04 respectively. No difference in acute toxicity profile was seen between the groups, and late toxicities were mild and minimal.
Conclusion: Prophylactic EF-CCRT can be a reasonable option in patients with locally advanced cervical cancer with radiologic positive pelvic lymph nodes and radiologic negative PALN.
Keywords: prophylactic extended field radiation therapy, concurrent chemotherapy
Introduction
The incidence of invasive cervical cancer is decreasing in United States.1 However, cervical cancer continues to be a major women’s health issue in many countries because of inadequate cytological screening programs, and many patients present as locally advanced International Federation of Gynecology and Obstetrics (FIGO) stage IIB-IVA, for which surgery is inadequate. The standard treatment for locally advanced cervical cancer is combined chemotherapy and pelvic irradiation, based on results of four randomized trials showing survival benefit of 10%–15% and local and distant recurrence reduction rates of 30%–40%.2–5 However, 15%–25% of patients experience paraaortic lymph nodes (PALN) failures after receiving combined pelvic chemoradiation, in long-term follow up.6 Data suggests that patients with locally advanced cervical cancer harbor 17%–37% paraaortic nodal micrometastases, at the time of diagnosis, just outside of standard radiation fields; therefore, the paraaortic nodal area is a common extrapelvic site of failure, which certainly compromises the distant control and survival.7
Since the last three decades, clinical trials of radiotherapy alone have failed to document the efficacy of prophylactic paraaortic irradiation or extended-field irradiation for biopsy-proven PALNs metastases, PALN failures with 5-year survival rates as low as 29% to 50%.8 Further observations of chemotherapy incorporated with extended-field irradiation for biopsy-proven PALN metastases showed significant gastrointestinal and hematological toxicities and no survival benefit.9
We aimed to evaluate whether prophylactic extended-field irradiation with concurrent chemotherapy leads to results better than those obtained by standard pelvic irradiation with concurrent chemotherapy in patients with locally advanced cervical cancer with radiologic negative PALN status.
Materials and methods
Eligibility
After getting the approval from Institutional (King Fahad Medical City, Riyadh Saudi Arabia) and National ethical review committees (King Abdulaziz City for Science and Technology) and obtaining informed consents from patients for participation in the study in March 2007, consecutive patients with locally advanced cervical cancer, between July 2007 and April 2008, were accrued when they met the following eligibility criteria: 1) histologically proven squamous cell carcinoma, adenocarcinoma or adenosquamous carcinoma of the cervix uteri; 2) clinical and radiologic FIGO stage IIB-IVA, with no other evidence of distant metastasis outside the pelvis; 3) Eastern Cooperative Oncology Group (ECOG) performance status 0–2; 4) negative PALNs on imaging (computed tomography [CT], magnetic resonance imaging [MRI]), or flourodeoxyglucose positron emission tomography (FDG-PET); and 5) normal hematologic, hepatic, and renal functions tests (white blood cell count [WBC] ≥4,000/mm3, absolute neutrophil count [ANC] ≥1,500/mm3, platelets ≥100,000/mm3, total bilirubin ≤1.5 mg/dL, alanine transaminase ≤2 of normal and creatinine ≤1.5 mg/dL).
Patients with a previous history of hysterectomy, retroperitoneal surgery, abdominal or pelvic radiotherapy, prior chemotherapy, pregnancy, or positive paraaortic nodes on imaging or biopsy proven were excluded.
The pretreatment workup consisted of a complete history and physical examination; bimanual examination; CT and MRI of chest, abdomen, and pelvis; complete hematology, hepatic, renal, and electrolytes studies; bone scan; and cystoscopy and sigmoidoscopy when necessary.
Treatment protocol
External beam radiation therapy (EBRT)
All patients were scanned, for simulation, on a CT simulator, from epigastrium to midthighs, and noncontrast and contrast images were obtained. After the data acquisition, all patients were randomized into two groups according to radiation therapy techniques. In the first group, whole-pelvis concurrent chemoradiation (WP-CCRT), the following were delineated: gross tumor volume (GTV); uterus; the presacral, common iliac, internal iliac, and external iliac lymph nodes; initial clinical target volume (CTV-1), covering GTV and the uterus, with 1 cm margins, and the presacral, common iliac, internal iliac, and external iliac lymph nodes; initial planning target volume (PTV)-1, with 0.5 to 1 cm margins around CTV-1; boost clinical target volume (CTV-2), covering the positive lymph nodes and parametria; PTV-2 (4 cm midline block and 0.5 cm margins to CTV2); and organs at risk, including kidneys, small bowel, bladder, rectum, and femoral heads. For the majority of patients; equally spaced, coplanar three-dimensional chemoradiation (3D-CRT) field plans (box-field) were generated; however, intensity-modulated radiation therapy (IMRT) was also generated for some cases, to achieve better dose distribution. Radiation (3D-CRT) was delivered with anteroposterior, posteroanterior, and opposed lateral beams of 18-MV photons. The borders of (anteroposterior/posteroanterior) fields were kept, cranially, at the junction of L3/L4; caudally, 3 cm below the most inferior vaginal involvement (as marked by golden seeds); and laterally, 2 cm lateral to the pelvic brim. The borders of lateral fields were kept, anteriorly, 1 cm anterior to the symphysis pubis, and posteriorly, were extended to the sacrum hollow. The prescribed radiation doses were 45–50.4 Gy/25–28 fractions to PTV-1, and 54– 59.4 Gy/30–33 fractions to PTV-2, 5 days per week, and up to 7% variation was considered acceptable (Figures 1 and 2A). Radiologic positive lymph nodes were boosted to a dose of 50.4–54 Gy. During planning, the mean dose to the rectum was constrained to <50 Gy, and the total doses to the small bowel, kidneys, and bladder were constrained to <45 Gy, <20 Gy, and <60 Gy respectively. In the second group, receiving prophylactic extended-field concurrent chemoradiation (EF-CCRT), the pelvis was treated similarly as for the WP-CCRT group, and additional paraaortic fields were added as a continuous area or with a half-beam block, with a superior field border at the junction of T12/L1, to cover PALNs up to the level of the renal hila. In no cases were anteroposterior or posteroanterior fields allowed, to minimize the toxicity. The prescribed radiation dose to PALNs was 45 Gy (up to 7% variation was considered acceptable). All patients in the EF-CCRT arm were given routine antiemetics before planned radiotherapy sessions.
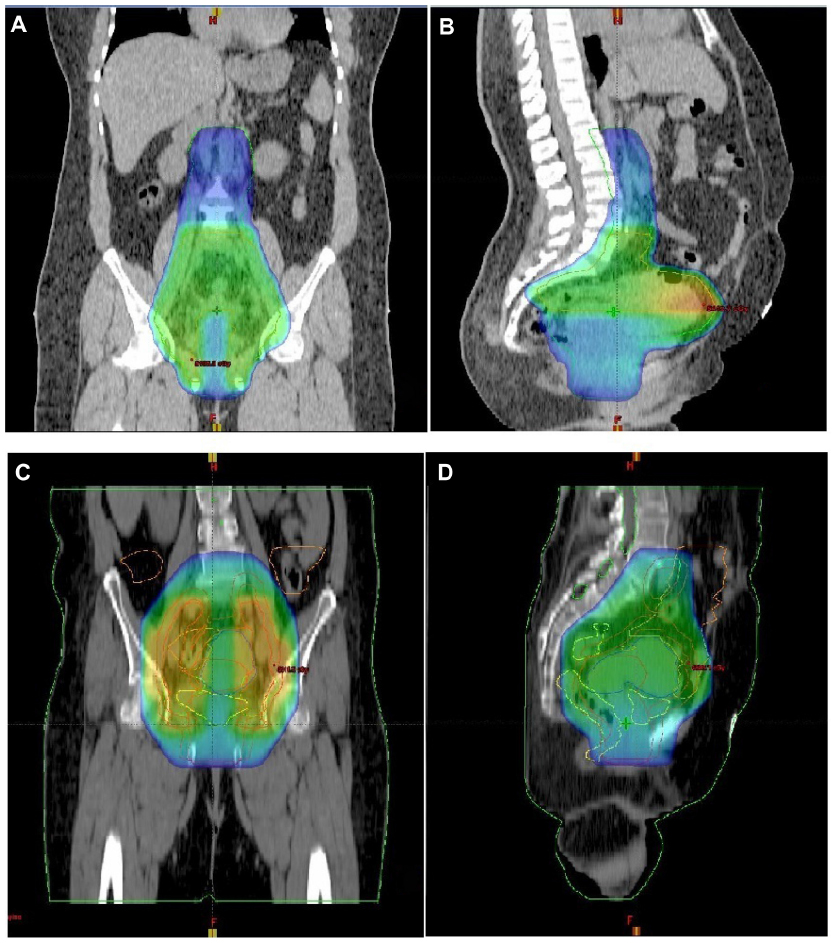 | Figure 1 Initial-phase radiotherapy: (A,B) extended-field and (C,D) three-dimensional conformal radiation therapy (3D-CRT) plans showing 45 Gy to planning target volume (PTV)-1, in coronal (A,C) and sagittal views (B,D). |
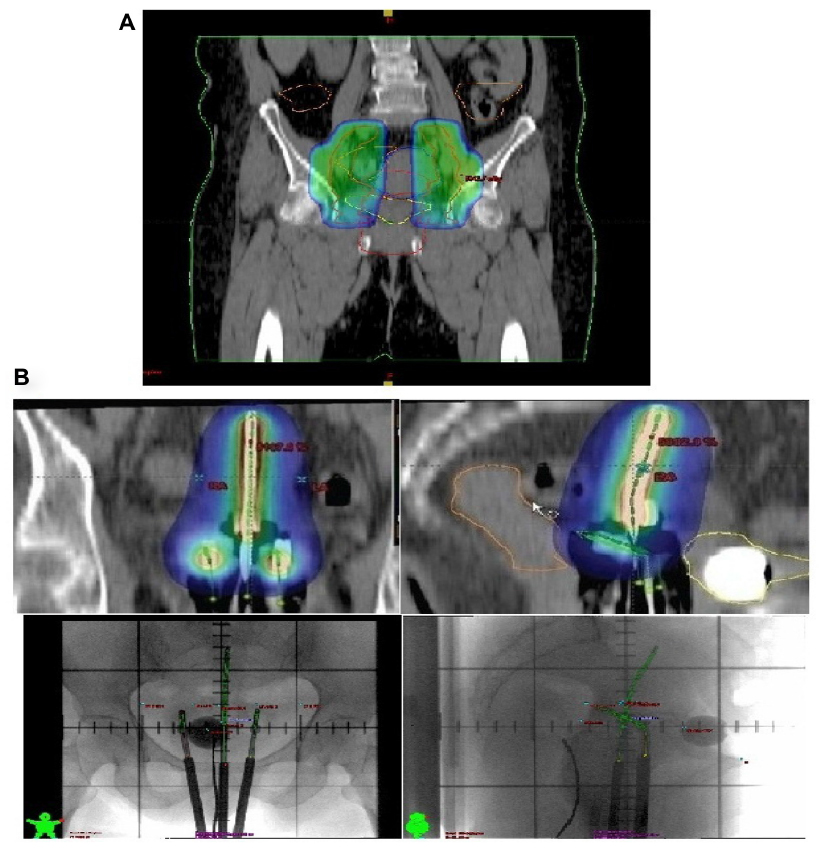 | Figure 2 (A) Parametrial boost (planning target volume [PTV]-2) of 5.4-9 Gy with midline shielding, followed by (B) high-dose rate brachytherapy of 21 Gy in three sessions, in the two treatment groups (rectum on the left and bladder on the right). |
Concurrent chemotherapy
Both groups of patients received weekly cisplatin 40 mg/m2 before the administration of radiotherapy for six doses. During CCRT, the doses were modified on a weekly basis. If the WBC count was below 2,000/mm3 or the platelet count was below 50,000/mm3, all chemotherapy for that week was omitted. If the WBC count was below 1,000/mm3 or the platelet count was below 25,000/mm3, CCRT was withheld until the WBC count and the platelet count recovered to 1,000/mm3 or greater and 25,000/mm3 or greater, respectively. If the serum creatinine level was above 1.8 mg/dL, the cisplatin was withheld. Patients were deemed unsuitable for further chemotherapy if the delay to resume treatment was longer than 2 weeks.
High-dose rate (HDR) brachytherapy
Fletcher–Suit tandem and ovoids afterloading applicators were used for HDR-brachytherapy with iridium-192 sources, once a week under conscious sedation, after 45 Gy of EBRT. A dose of 7 Gy per fraction, using three insertions to point A with a total dose of 21 Gy, was delivered, based on the dose limit derived from the treatment plan for the rectum and bladder. The dose constraints were 75 Gy and 80 Gy for the rectum and bladder, respectively (Figure 2B).
Toxicity scoring
During CCRT, patients were evaluated every week for weight, performance status, pelvic examination, hematologic and blood chemistry determinations, and other related characteristics. The National Cancer Institute Common Toxicity Criteria (NCI-CTC) version 2.0 were used to score acute radiation and chemotherapy toxicity (<90 days from the start of radiation therapy).
After completion of the CCRT, patients were seen every 3 months for the first 2 years, and every 6 months thereafter, at radiation oncology and gynecology oncology clinics. Response evaluation consisted of physical and pelvic examination; Pap smear; hematology, hepatic, and renal function tests; and CT chest, and abdomen and pelvic MRI every 6 months for the first 2 years. The Radiation Therapy Oncology Group (RTOG) Late Radiation Morbidity Scoring Criteria were used to score radiation toxicity persisting beyond 90 days from the completion of radiotherapy.
Statistical analysis
The study was initially designed to be able to detect an improvement of approximately 10% in the 5-year locoregional control (LRC), with a statistical power of 80% and a two-sided significance level of 0.05. To detect such a difference, we predicted that we would need to enroll 163 women in the study over a 2-year period and then follow them for an additional 4 years. We estimated that 50% (86) women would have died by the time of the analysis. The primary end point was the LRC (pelvic and paraaortic control). Secondary end points were distant metastatic control, disease-free survival (DFS), and the overall survival (OS) for each group. DFS was defined as the duration between the completion of CCRT and the date of documented disease recurrence, death resulting from the cancer, and/or last follow-up visit (censored). OS was defined as the duration between the completion of CCRT and the date of patient death or last follow-up visit (censored). The probabilities of LRC, distant metastatic control, DFS, and OS were determined with the Kaplan–Meier method. The comparisons for various end points were performed using the log-rank test. The Student’s unpaired t test was used to determine the significance of the difference between two groups. A P-value of 0.05 was considered statistically significant. Statistical analyses were performed using the computer program SPSS (Statistical Package for the Social Sciences, Version 17.0; IBM Corp, Chicago, IL, USA).
Results
Characteristics of the patients
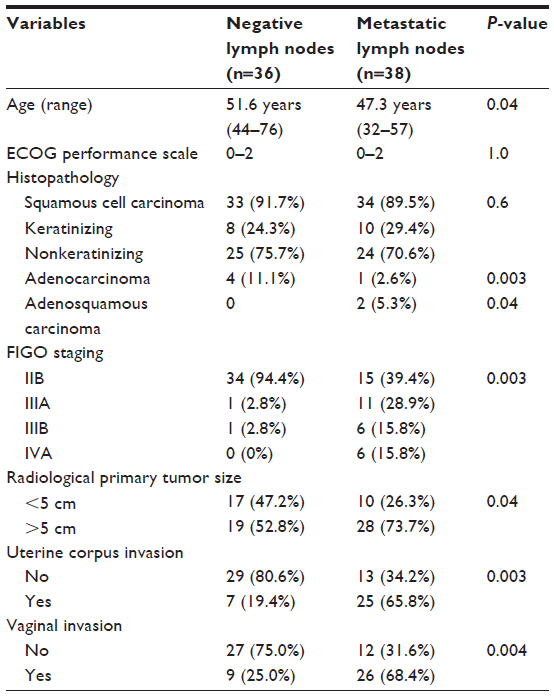
After accrual, 83 patients with locally advanced cervical cancer were randomly assigned to WP-CCRT (50 patients) and EF-CCRT (52 patients), as shown in Figure 3. The characteristics of remaining 74 patients are given in Table 1. The majority of the cohort was presented with FIGO stage IIB (66.2%) and with radiologic positive pelvic lymph nodes (51.4%). FIGO stage IIIB with hydronephrosis/ nonfunctioning kidneys was seen in three cases (4.05%), and for these patients, percutaneous nephrostomy or JJ stenting was performed prior to starting CCRT. The median follow-up time was 60 months (range, 18–66). The histopathologic characteristics of patients with positive pelvic lymph nodes are shown in Table 2.
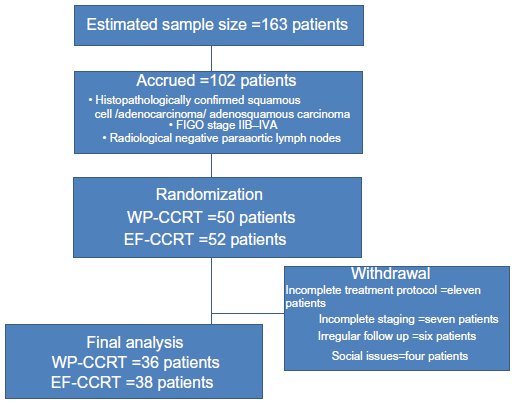 | Figure 3 Treatment algorithm. |
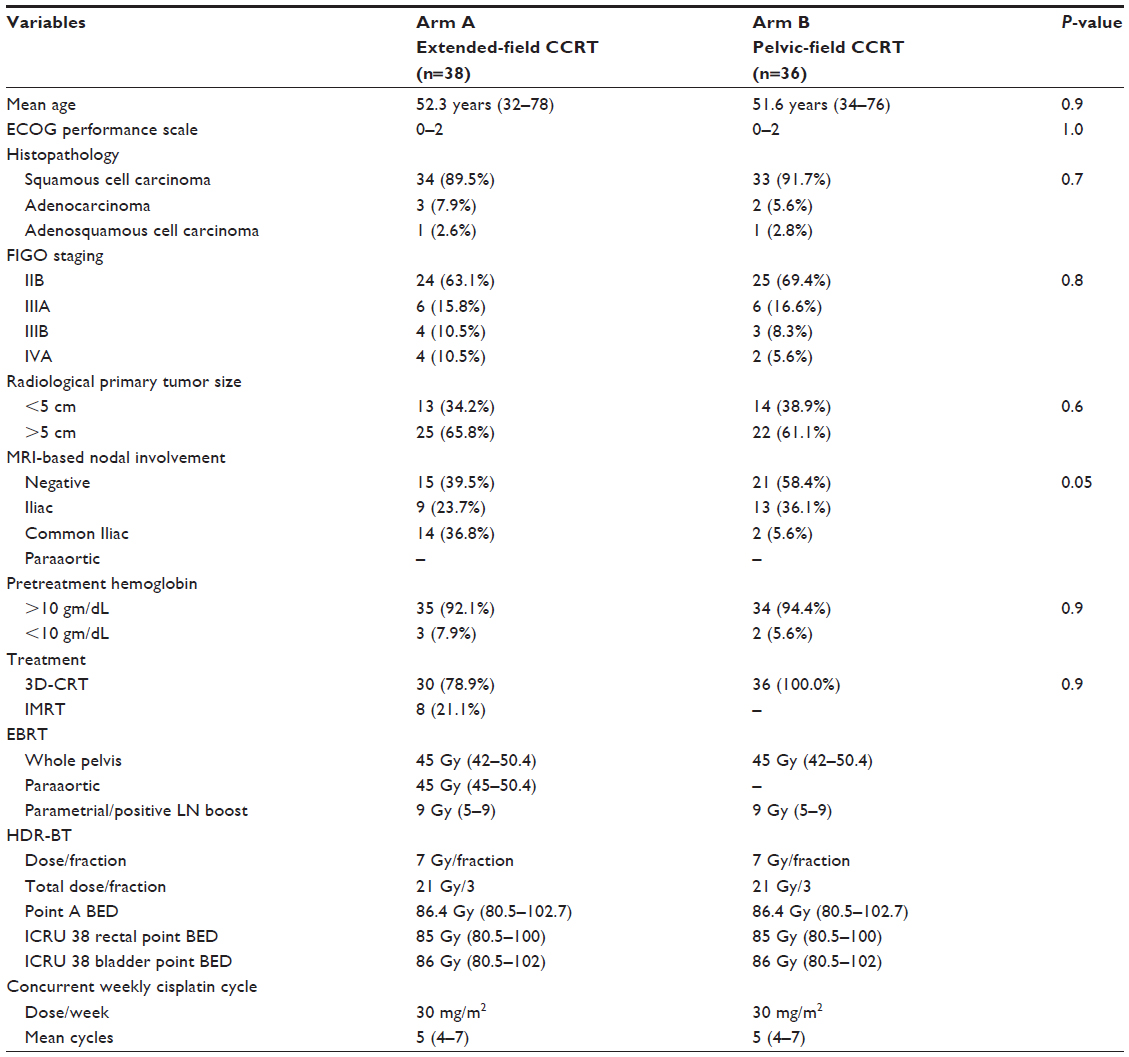 | Table 1 Patients characteristics |
 | Table 2 Clinicopathological findings variation in cervical patients with positive lymph nodes |
Among all 74 patients who received CCRT, the treatment protocol completion rate was 90% (95% confidence interval [CI]: 85–100) in the WP-CCRT group and 88.4% (95% CI: 90–100) in the EF-CCRT group (P=0.8). Weekly concurrent cycles of cisplatin, in both treatment arms, were completed in all 74 (100%) patients, with no interruption. The median duration of radiation therapy (including EBRT and HDR-brachytherapy) in both arms was 55.5 days (7.8 weeks) with 95% CI: 48–58.
Toxicity profile
The overall incidence of the grade 3 or 4 acute hematological and nonhematological toxicities was 5.2% and 2.6%, respectively, in the EF-CCRT arm and 5.4% and 2.7%, respectively, in the WP-CCRT arm (P=0.7). Both treatment arms had similar grade 3 or 4 acute gastrointestinal toxicity (Table 3).
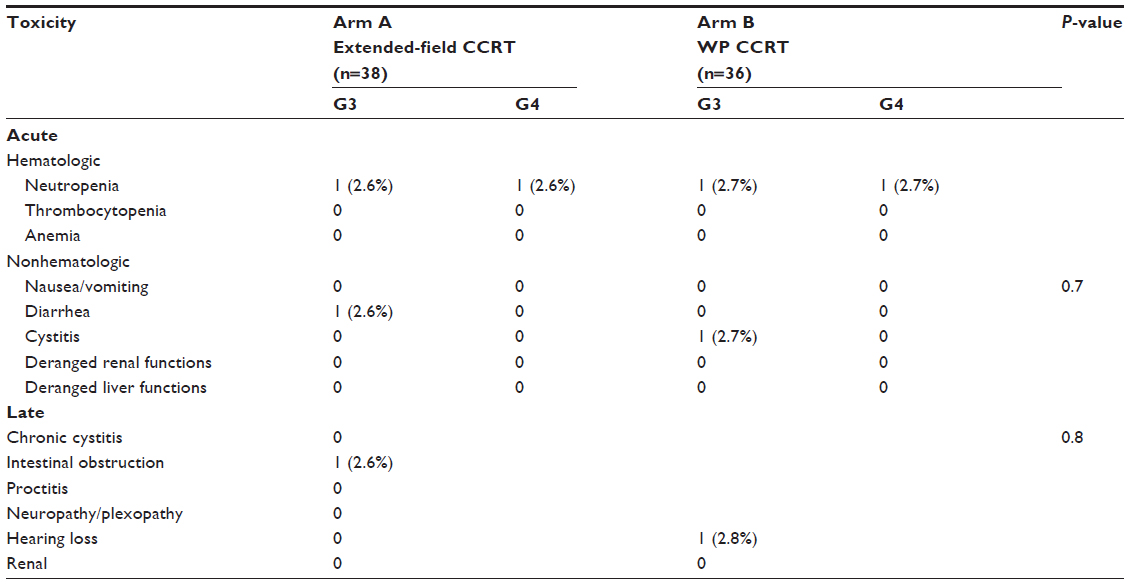 | Table 3 Acute and late treatment related toxicity profile |
During the follow-up time of 60 months, in the EF-CCRT group, one patient (2.6%) experienced subacute intestinal obstruction. No patient in either arm underwent surgery for radiation-induced damage or died because of treatment-related side effects.
Pelvic, paraaortic, distant control, and survival rates
At the time of the last follow-up visit, three (7.9%) patients had pelvic recurrences (one vaginal and two pelvic nodal) in the EF-CCRT arm, and three (8.3%) patients had local recurrences (pelvic nodal) in the WP-CCRT arm (P=0.8). Isolated vaginal recurrence in the EF-CCRT group was successfully salvaged with surgery, and pelvic nodal recurrences were treated with salvage chemotherapy. First pelvic recurrence was manifested within 24 months of completion of CCRT in both arms.
Paraaortic nodal failures were seen in five (13.9%) patients in the WP-CCRT arm and one (2.6%) patient in EF-CCRT arm (P=0.02) (Figure 3A). In the WP-CCRT arm, three (60%) of five paraaortic nodal failures were seen at the level of junction L2 and L3 vertebrae and two (40%) at the level of L1 vertebrae; and in the EF-CCRT arm, one paraaortic nodal failure was seen at the junction of T12 and L1 vertebrae. In both arms, paraaortic nodal failures were seen within 20 months of completion of CCRT. Distant failures were seen in seven (19.4%) patients in the WP-CCRT and in four (10.5%) patients from the EF-CCRT arm (P=0.02) (Figure 4B). The common sites of distant failure were: lungs (four patients), mediastinal (three patients), and supraclavicular nodes (one patient), and thoracic spine (one patient). Combined distant and paraaortic nodal failures were observed in four (11.4%) in the WP-CCRT and one (2.6%) in the EF-CCRT group. All distant and PALN were treated with salvage chemotherapy ± radiotherapy for bony lesions. Important prognostic factors for PALN were positive pelvic nodes on imaging (CT/MRI), the FIGO stage >IIB, and prolonged treatment time >55 days (P=0.001, 0.001 and 0.03, respectively) (Table 4). At the time of analysis, 32 patients in the EF-CCRT and 27 patients in the WP-CCRT group were found without evidence of disease (Figure 4C and D).
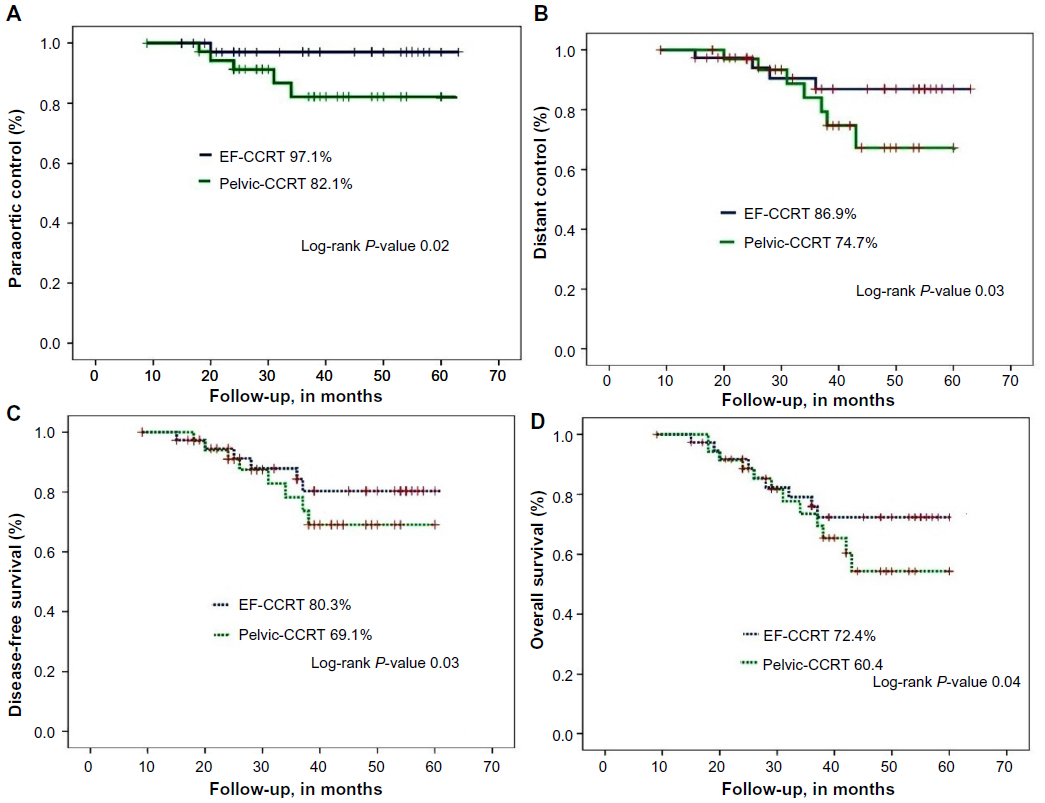 | Figure 4 Five year (A) paraaortic control, (B) distant control, (C) disease-free survival, and (D) overall survival, after extended-field chemoradiation and WP-CCRT. |
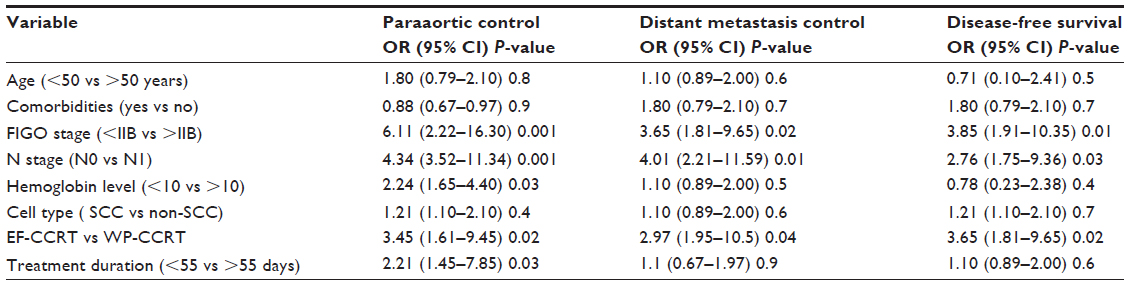 | Table 4 Multivariate analysis of variables on paraaortic, distant control, and disease-free survival rates |
Discussion
WP-CCRT is deemed the standard treatment, by many North American and European teams, for treatment of locally advanced cervical cancer, which has resulted in survival gain but also, 10%–25% paraaortic nodal failures.10 The 10-year results of a RTOG (RTOG-97-20) trial, which compared pelvic irradiation with paraaortic plus pelvic radiotherapy alone, have shown an improvement in survival gain of 11% in the prophylactic paraaortic plus pelvic irradiation group but no difference in LRC.11,12 A subsequent other RTOG trial (RTOG 90-01) compared prophylactic extended-field radiotherapy versus pelvic irradiation with chemotherapy in locally advanced cervical cancer patients; the study showed that 5-year OS rates for patients treated with pelvic irradiation and concurrent chemotherapy was significantly greater than for patients treated with extended-field radiation alone (67% vs 41% at 8 years), and pelvic irradiation with concurrent chemotherapy resulted in a 51% reduction in the risk of recurrence and a 52% reduction in the risk of death but no difference in the incidence of paraaortic failures (7% in pelvic irradiation with concurrent chemotherapy vs 4% in extended-field irradiation [P-value 0.15]).6
The role of incorporating concurrent chemotherapy with prophylactic extended-field irradiation to reduce the paraaortic nodal failures and promote a survival gain is not well known; due to lack of Phase III trials to pursue this question, Malfetano et al used weekly cisplatin concomitant with prophylactic extended-field radiation, followed by low-dose rate brachytherapy, in a Phase II study in which 67 women were enrolled, of whom 54 had radiologic negative paraaortic nodes. Treatment was well tolerated, with high efficacy, and at a median follow up of 47.5 months, 75% of patients were alive without evidence of disease and with no paraaortic failures.13 However, this trial was criticized for nonrandomization, selection bias, and use of older conventional external beam and low-dose rate radiation techniques. Another Phase II study by Chung et al treated 63 locally advanced cervical cancers with concurrent cisplatin during the first and fifth weeks of extended-field irradiation, followed by two adjuvant cycles of cisplatin- and 5-flouro-uracil-based chemotherapy; results showed that toxicity was minimal, with paraaortic nodal failures in only 4.5% and an OS rate of 81% at 3 years.14 Advanced FIGO stage, parametrial invasion, elevated CEA, and SCC-Ag are all associated with increased risk of PALN failure.
To the best of our knowledge, our single institutional study is the first randomized, prospective study to compare prophylactic EF-CCRT plus HDR brachytherapy with standard WP-CCRT plus HDR brachytherapy, in patients with locally advanced cervical cancer with radiologic negative PALNs. We used radiologic (CT/MRI) staging along with clinical FIGO staging, as tumor size and lymph node involvement are also important prognostic factors that influence the LRC and survival.17,18 For such patients, CT/PET imaging would be superior to other imaging modalities to assess the lymph node status and distant metastasis;19 however, our study can be criticized for not performing baseline CT/PET in all patients. Possible explanation was the nonavailability of PET imaging in our institute at the time of accrual of patients (and later on, only 16% of patients had routine follow-up CT/PET imaging). The course of treatment was well tolerated in our patients, and hematological and nonhematological toxicities were minimal or even better than those reported in other trials of EF-CCRT.4,5 Further, EF-CCRT resulted in excellent 5-year paraaortic distant control rates and better DFS and OS rates, in comparison with WP-CCRT, in the present study, especially in patients with radiologic gross pelvic lymphadenopathy; however, we did not see any difference in pelvic control between the two groups.
Possible explanation for the lower toxicity profile and better outcomes (LRC and distant control) in the EF-CCRT group may be that: a) the majority of our patients (90%) had gross pelvic nodes >1 cm on imaging, which enhances the risk of paraaortic nodal micrometastasis, and these were eradicated by prophylactic EF-CCRT; b) surgical staging causes more intestinal fibrosis which results in more gastrointestinal toxicity; c) moderate doses of weekly cisplatin were used than elsewhere; d) use of better radiation techniques in our study (CT simulation, 3D-CRT/IMRT and HDR brachytherapy); and e) treatment duration was 55 days for the majority of patients.
Although our study showed encouraging treatment outcomes and low morbidity, limitations of the present study were: a) the low sample size; b) poor randomization to study treatment and selection bias as many patients with common iliac lymphadenopathy were included in the EF-CCRT arm; c) lack of baseline FDG-PET-based staging; and e) the lack of baseline carcinoembryonic antigen and SCC-Ag levels.
However, the results of our study recommend use prophylactic EF-CCRT in patients with locally advanced cervical cancer with radiologic positive pelvic lymph nodes. Further, our results warrant a multicenter, Phase III trial using IMRT with prophylactic EF-CCRT in FDG-PET negative PALN locally advanced cervical patients, to evaluate whether the outcomes of EF-CCRT are truly better than those of WP-CCRT.
Acknowledgment
We thank Laura Stanciu Gabriella, medical physicist, who did manuscript language editing on behalf of the authors.
Disclosure
The authors report no conflicts of interest in this work.
References
Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62(1):10–29. | |
Keys HM, Bundy BN, Stehman FB, et al. Cisplatin, radiation, and adjuvant hysterectomy compared with radiation and adjuvant hysterectomy for bulky stage IB cervical carcinoma. N Engl J Med. 1999;340(15):1154–1161. | |
Rose PG, Bundy BN, Watkins EB, et al. Concurrent cisplatin based radiotherapy and chemotherapy for locally advanced cervical cancer. N Eng J Med. 1999;340(15):1144–1153. | |
Whitney CW, Sause W, Bundy BN, et al. Randomized comparison of fluorouracil plus cisplatin versus hydroxyurea as an adjunct to radiation therapy in stage IIB-IVA carcinoma of the cervix with negative para-aortic lymph nodes: a Gynecologic Oncology Group and Southwest Oncology Group study. J Clin Oncol. 1999;17(5):1339–1348. | |
Peters WA III, Liu PY, Barrett RJ, et al. Cisplatin and 5-Flourouracil plus radiation therapy are superior to radiation therapy as adjunctive in high risk early stage carcinoma of the cervix after radical hysterectomy and pelvic lymphadenectomy: report of a phase III intergroup study. J Clin Oncol. 2000;18:1606–1613. | |
Eifel PJ, Winter K, Morris M, et al. Pelvic irradiation with concurrent chemotherapy versus pelvic and para-aortic irradiation for high-risk cervical cancer: an update of radiation therapy oncology group trial (RTOG) 90-01. J Clin Oncol. 2004;22(5):872–880. | |
Berman ML, Keys H, Creasman W, DiSaia P, Bundy B, Blessing J. Survival and patterns of recurrence in cervical cancer metastatic to periaortic lymph nodes (a Gynecologic Oncology Group study). Gynecol Oncol. 1984;19(1):8–16. | |
Morris M, Eifel PJ, Lu J, et al. Pelvic radiation with concurrent chemotherapy compared with pelvic and para-aortic radiation for high-risk cervical cancer. N Engl J Med. 1999;340(15):1137–1143. | |
Small W, Winter K, Levenback C, et al. Extended-field irradiation and intracavitary brachytherapy combined with cisplatin chemotherapy for cervical cancer with positive para-aortic or high common iliac lymph nodes: results of ARM 1 of RTOG 0116. Int J Radiat Oncol Biol Phys. 2007;68(4):1081–1087. | |
Gouy S, Morice P, Narducci F, et al. Nodal-staging surgery for locally advanced cervical cancer in the era of PET. Lancet Oncol. 2012;13(5):e212–e220. | |
Rotman M, Choi K, Guse C, et al. Prophylactic irradiation of the para-aortic lymph node chain in stage IIB and bulky stage IB carcinoma of the cervix, initial treatment results of RTOG 7920. Int J Radiat Oncol Biol Phys. 1990;19(3):513–521. | |
Rotman M, Pajak TF, Choi K, et al. Prophylactic extended-field irradiation of para-aortic lymph nodes in stages IIB and bulky IB and IIA cervical carcinomas. Ten-year treatment results of RTOG 79-20. JAMA. 1995;274(5):387–393. | |
Malfetano JH, Keys H, Cunningham MJ, Gibbons S, Ambros R. Extended field radiation and cisplatin for stage IIB and IIIB cervical carcinoma. Gynecol Oncol. 1997;67(2):203–207. | |
Chung YL, Jian JJ, Cheng SH, et al. Extended-field radiotherapy and high-dose-rate brachytherapy with concurrent and adjuvant cisplatin-based chemotherapy for locally advanced cervical cancer: a phase I/II study. Gynecol Oncol. 2005;97(1):126–135. | |
Huang EY, Huang YJ, Chanchien CC, et al. Pretreatment carcinoembryonic antigen level is a risk factor for para-aortic lymph node recurrence in addition to squamous cell carcinoma antigen following definitive concurrent chemoradiotherapy for squamous cell carcinoma of the uterine cervix. Radiat Oncol. 2012;7:13. | |
Jeong BK, Choi DH, Huh SJ, Park W, Bae DS, Kim BG. The role of squamous cell carcinoma antigen as a prognostic and predictive factor in carcinoma of uterine cervix. Radiat Oncol J. 2011;29(3):191–198. | |
Kodaira T, Fuwa N, Toita T, et al. Comparison of prognostic value of MRI and FIGO stage among patients with cervical carcinoma treated with radiotherapy. Int J Radiat Oncol Biol Phys. 2003;56(3):769–777. | |
Scheidler J, Hricak H, Yu KK, Subak L, Segal MR. Radiological evaluation of lymph node metastases in patients with cervical cancer. A meta-analysis. JAMA. 1997;278(13):1096–1101. | |
Herrera FG, Prior JO. The role of PET/CT in cervical cancer. Front Oncol. 2013;3:34. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.