Back to Journals » Journal of Pain Research » Volume 14
Is ABO Blood Group a Predictive Factor for the Amount of Opioid Consumption in the First 24 Hours After Cesarean Section?
Authors Nimmaanrat S ![]() , Thongkumdee W, Geater AF
, Thongkumdee W, Geater AF ![]() , Oofuvong M
, Oofuvong M ![]() , Benjhawaleemas P
, Benjhawaleemas P
Received 1 July 2021
Accepted for publication 18 October 2021
Published 23 November 2021 Volume 2021:14 Pages 3585—3592
DOI https://doi.org/10.2147/JPR.S327230
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Timothy Atkinson
Sasikaan Nimmaanrat,1 Withaporn Thongkumdee,1 Alan F Geater,2 Maliwan Oofuvong,1 Pannawit Benjhawaleemas1
1Department of Anesthesiology, Faculty of Medicine, Prince of Songkla University, Hatyai, Songkhla, 90110, Thailand; 2Epidemiology Unit, Faculty of Medicine, Prince of Songkla University, Hatyai, Songkhla, 90110, Thailand
Correspondence: Sasikaan Nimmaanrat
Department of Anesthesiology, Faculty of Medicine, Prince of Songkla University, Hatyai, Songkhla, 90110, Thailand
Tel +66 88 790 7842
Fax +66 74 281656
Email [email protected]
Background: Cesarean section is the most common major surgery performed globally. Blood group O has been found as a factor affecting pain severity after cesarean section. We aimed to evaluate the predictive factors, including ABO blood group, for the amount of opioid consumption (measured as milligrams of morphine equivalent [MME]) within the first 24 hrs after cesarean section.
Methods: This retrospective study was done in 1530 pregnant women who had a cesarean section under the same regimen of spinal anesthesia (2.2 mL of 0.5% hyperbaric bupivacaine and morphine 0.2 mg). All were prescribed regular paracetamol and ibuprofen for postoperative pain control. Univariate and multinomial regression analyses were performed to identify the predictive factors for opioid consumption in the first 24 hrs postoperatively.
Results: About 2/5 of them (43.3%) received 0 mg MME, while 25.6%, 23.7% and 7.4% received 1– 5, 6– 10 and > 10 mg MME, respectively. The majority have blood group O (40.6%), while 23.4%, 28% and 8% have blood group A, B and AB, respectively. After univariate and multinomial regression analyses, operation time, opioid consumption in PACU, maximum VNRS within the first 24 hrs and consumption of both paracetamol and ibuprofen were identified as predictive factors for postoperative opioid consumption. ABO blood group exhibited no correlation for opioid requirement postoperatively.
Conclusion: ABO blood group is not a predictive factor for opioid requirement within the first 24 hrs following cesarean section. Duration of operation, opioid given in PACU, maximum VNRS on ward and consumption of both paracetamol and ibuprofen have been found to be predictive factors for postcesarean opioid requirement.
Keywords: ABO blood group, predictive factors, cesarean section, postoperative opioid consumption
Introduction
Cesarean section has become the most frequent surgery performed worldwide.1 It generally leads to moderate to severe postoperative pain in the first 48 hrs.2 The intensity of acute postoperative pain is a substantial predictive factor for the development of chronic pain,3,4 which occurs in 9.2–18% of parturients who undergo cesarean section.5–7 Higher body mass index (BMI) ≥ 30 kg/m2, operation time > 60 minutes, single women, general anesthesia and blood group O have been demonstrated as factors affecting postcesarean section pain severity among Malaysian parturients.8 Preoperative anxiety increased the risk of moderate to severe postoperative pain in cesarean section women, while intrathecal morphine with fentanyl added to bupivacaine was a protective factor against pain.9 A simple three-item questionnaire is a useful tool for predicting the severity of acute postcesarean evoked pain.10 Preoperative electric pain threshold correlates significantly with postcesarean pain scores at 6 and 24 hrs, and with the quantity of paracetamol taken by the patient within 48 hrs after surgery.11 Resting pain after cesarean section can be predicted by 2 factors, thermal pain and unpleasantness, and patient expectations.12
Generally, a number of risk factors for acute postoperative pain have been identified. It is a complex interaction between numerous factors, which roughly can be divided into genetic and environmental factors. Genetic factors such as gender, ethnicity and hair color are also associated with pain sensitivity.13–15 Thus, these factors should be taken into account while planning for postoperative pain control. A less studied factor is the association between postoperative pain and the ABO blood group.
As far as we know, there are studies demonstrating the predictive factors for postcesarean pain intensity but there is no study focusing on contributing factors (including ABO blood group) to postcesarean opioid requirement. Under these circumstances, this study principally aimed to evaluate the association between the ABO blood group and the amount of opioid consumption within the first 24 hrs after cesarean section. The secondary objective was to identify other predictive factors for opioid consumption within the first 24 hrs.
Methods
Study Design
This is a retrospective study which was approved by the Ethics Committee of the Faculty of Medicine, Prince of Songkla University, Thailand (REC Number: 61-138-18-4) on 3 August 2018. This retrospective study involved no more than minimal risk to subjects so the patient consent to review their medical records was waived by the Ethics Committee of the Faculty of Medicine, Prince of Songkla University. The data was anonymized, maintained with confidentiality and in compliance with the Declaration of Helsinki.
Participants
Eligibility criteria for study participation included: (1) parturients undergoing cesarean section under successful spinal anesthesia (0.5% hyperbaric bupivacaine 2.2 mL plus morphine 0.2 mg) and (2) regular paracetamol (500 mg every 6 hrs) and ibuprofen (400 mg 3 times per day) were prescribed for postoperative pain control. Exclusion criteria included: (1) parturients receiving general anesthesia either as planned or after a failed/inadequate spinal anesthesia, (2) receiving no intrathecal morphine or other doses of intrathecal morphine, (3) receiving intraoperative supplemental opioid, ketamine or propofol, (4) undergoing other operations in addition to cesarean section, (5) receiving pethidine for shivering in postanesthesia care unit (PACU), (6) receiving no regular paracetamol and ibuprofen postoperatively and (7) incomplete data as per the study’s protocol.
Collected Data
A case record form consisted of 4 parts: (1) general information (age, body weight, height, body mass index [BMI], ABO blood group, ASA classification, elective/emergency case, gravidity [G], parity [P], abortion [A], history of previous cesarean section and history of recurrent Pfannenstiel incision), (2) intraoperative data (successful spinal block, use of intrathecal morphine [0.2 mg], skin incision, operation time, no intraoperative opioid use, no intraoperative ketamine use), (3) PACU data (verbal numerical rating score [VNRS] and amount of opioid used as milligram morphine equivalent [MME])16 and (4) ward data within 24 hrs (minimal and maximum VNRSs, postoperative opioid use as MME, total dose of paracetamol and ibuprofen used, and length of hospital stay).
Statistical Analysis
All data were analyzed with Program R version 3.6.3 (Vienna, Austria) or STATA for Windows version 14.2 (Stata Corporation, College Station, Texas) for both descriptive and inferential statistics with a 5% level of significance. Data were compared between the groups using chi-square test and ANOVA F-test in univariate analysis. Multinomial regression analyses were used to examine the associations between the variables with P-value < 0.2 from univariate analysis and the outcome measures of postoperative opioid requirement within 24 hrs. Adjusted relative risk ratio (RRR) and 95% confidence intervals (CI) were derived.
Sample Size Calculation
The required sample size was estimated based on 2 objectives: testing for a difference in proportions of patients who required opioid and for a difference in the total of opioid between A and O and between B and O blood groups. Given the estimated prevalence of blood groups of 20% A, 34% B, 40% O and 6% AB, there would be insufficient patients of AB group to conduct any meaningful analysis. Preliminary data suggested the prevalence of opioid use in groups A, B and O around 70%, 65% and 50%, respectively. For a power of 80% to detect a significant difference (α = 0.05) between either groups A or B of 60% and O of 50%, and allowing for unusable data from 5% of patients, a total sample of 1530 was required.
Results
We included 1530 parturients having cesarean section under successful spinal anesthesia into this study. Patient demographic data are presented in Table 1. Their ages varied from 14–45 years old. The majority of them have blood group O (40.65%) followed by B (27.97%), A (23.41%) and AB (7.97%). The minority (15.29%) underwent elective cesarean section. Half was multigravida (50.13%).
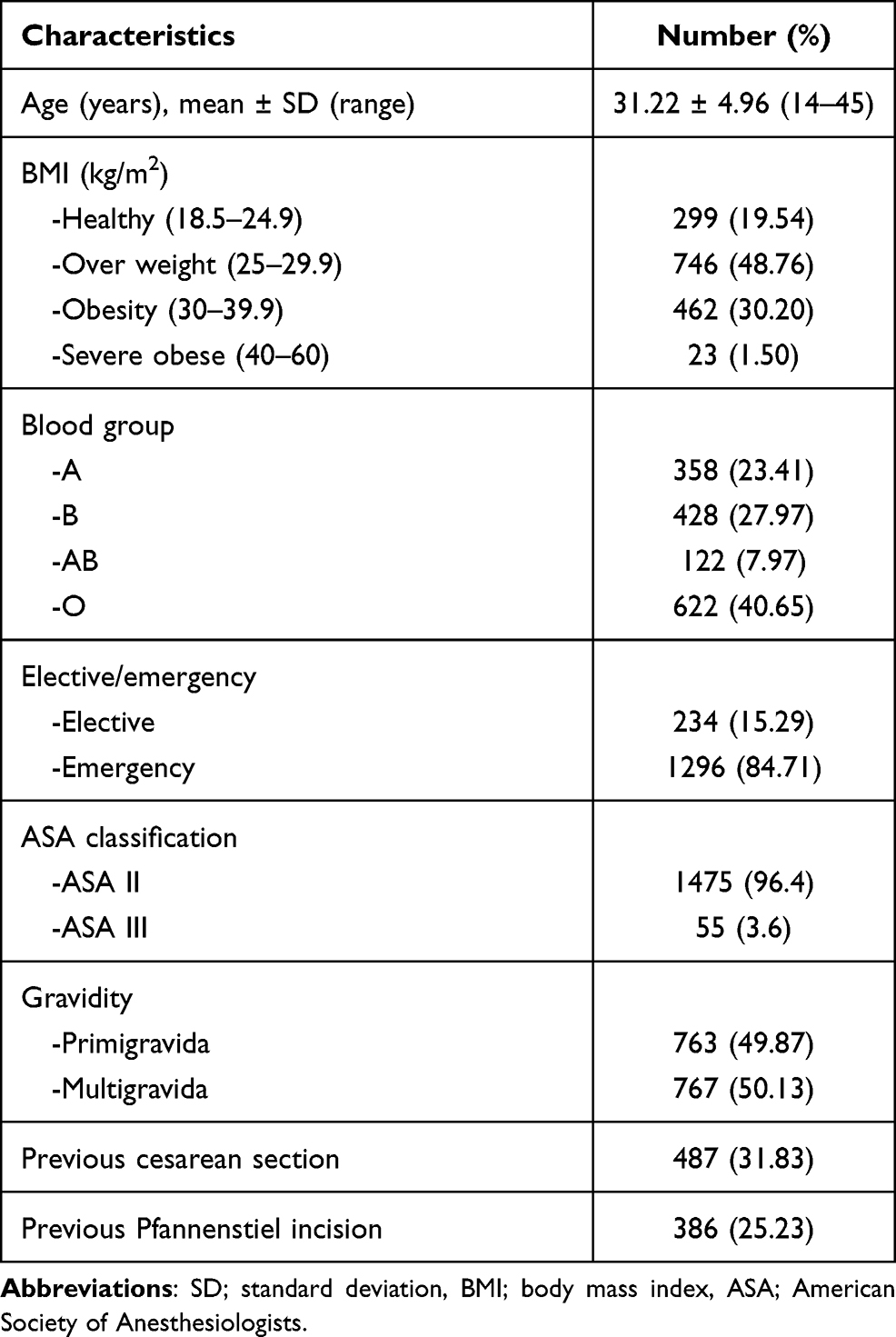 |
Table 1 Patient Demographic Data (n = 1530) |
Intraoperative and postoperative data are presented in Table 2. The majority (74.31%) had Pfannenstiel incision. Mean opioid consumption (MME) at PACU was 0–5 mg. Within 24 hrs on ward, the minimum and maximum VNRSs were 0.54±1 (0–7) and 4.91±1.98 (0–10), respectively. Almost half did not receive any opioid (43.27%). The majority received one dose of paracetamol (60.26%) and ibuprofen (62.68%).
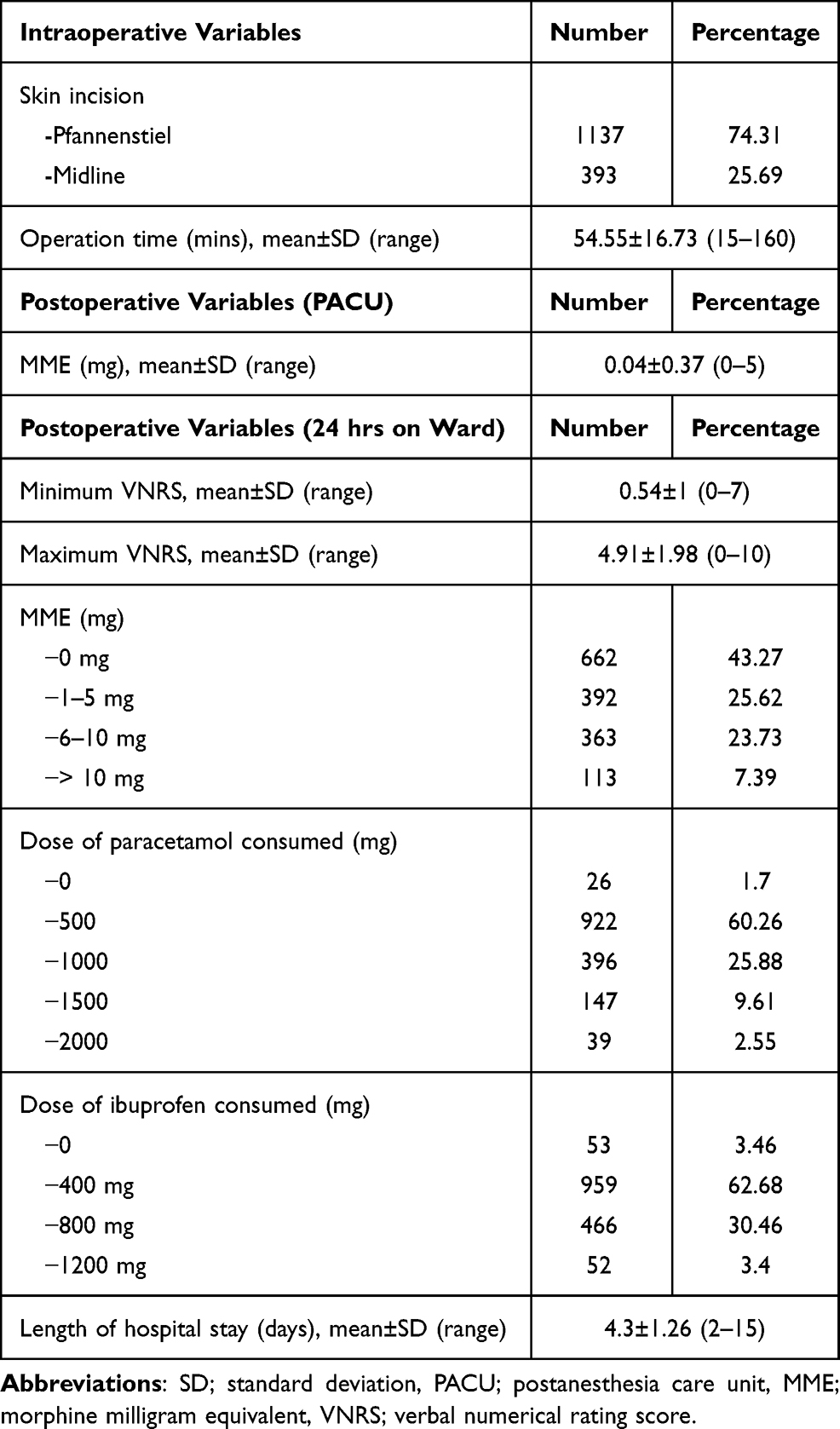 |
Table 2 Intraoperative and Postoperative Variables |
Patients with different blood group did not require statistically different amount of opioid consumption (MME) within the first 24 hrs after cesarean section. [A 3 (0, 6), B 3 (0, 6), AB 3 (0, 6) and O 3 (0, 6), P-value = 0.943]
The univariate analysis was performed to determine the factors associated with postoperative opioid consumption within the first 24 hrs. These variables were found to be correlative factors (P-value < 0.2) including age (P-value = 0.168), BMI (P-value = 0.09), elective/emergency (P-value = 0.137), history of previous cesarean section (P-value = 0.148), type of skin incision (P-value < 0.001), operation time (P-value = 0.001), opioid consumption in PACU (P-value = 0.002), maximum VNRS on ward (P-value < 0.001) as well as the analgesics (paracetamol ± ibuprofen) used on ward (P-value < 0.001). There was no significant correlation between ABO blood group and postoperative opioid consumption within the first 24 hrs. (P-value = 0.683) (Table 3).
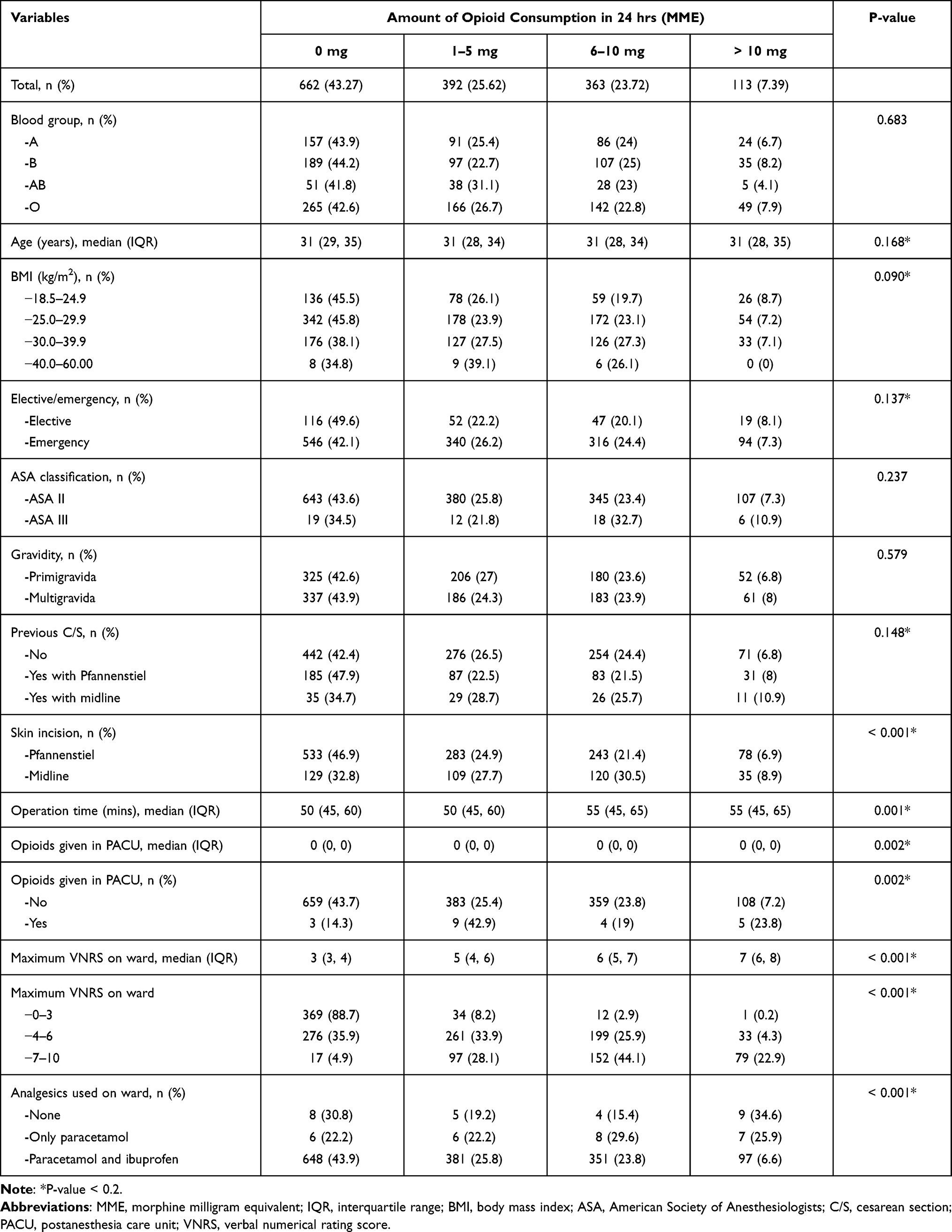 |
Table 3 Univariate Analysis of Variables Which Might Be Related to the Amount of Opioid Consumption in the First 24 Hours After Cesarean Section |
Finally, multinomial analysis was conducted to identify the relationship between each variable with each group of outcomes (comparison by pair). Our study found 4 variables (operation time, amount of opioid consumption in PACU, maximum VNRS within the first 24 hrs and consumption of both paracetamol and ibuprofen) to have statistically significant influences on postoperative opioid consumption within the first 24 hrs after cesarean section, as shown in Table 4.
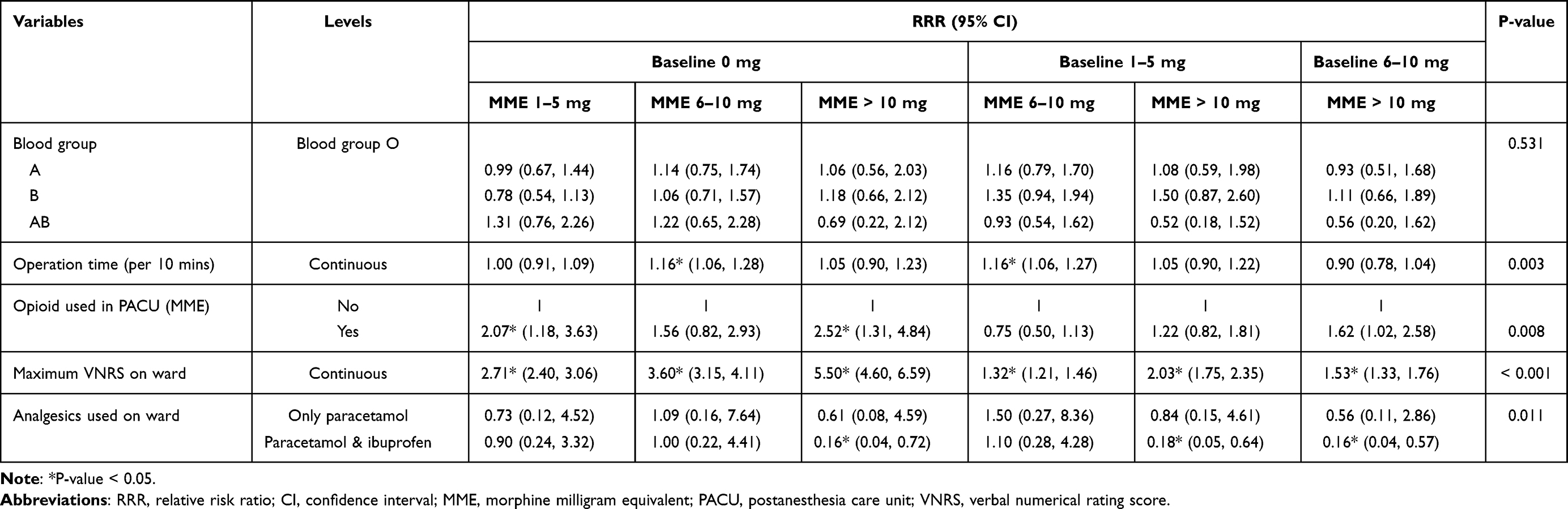 |
Table 4 Multinomial Analysis of Variables Carried from the Univariate Analysis |
Discussion
This retrospective study in 1530 parturients has found 4 predictive factors for opioid requirement (measured by MME) in the first 24 hrs after cesarean section. Longer operation time, larger amount of opioid consumption in PACU and maximum VNRS within the first 24 hrs were shown as predictive factors for higher opioid consumption. On the other hand, consumption of both paracetamol and ibuprofen postoperatively was found as a predictive factor for lower opioid requirement. ABO blood group has not been demonstrated as a contributing factor.
We have found that longer operation time is a predictive factor for higher demand for postoperative opioid in the first 24 hrs after cesarean section. This finding is in accordance with the previous study in cesarean section patients.8 A long operation time was demonstrated to correlate with more postoperative analgesic requirement.17,18
The majority of our patients did not receive any opioid in PACU. However, we have discovered that the amount of opioid consumption in PACU is also a predictive factor; the higher the dose of opioid consumed in PACU, the higher the dose of opioid consumed in the first 24 hrs. As we usually discharge patients receiving spinal anesthesia when the block level is at L1 or L2 level, it may reflect that those who experience pain and request analgesic earlier have lower pain threshold and tolerance leading to higher postoperative opioid consumption on ward. Heat pain threshold12 and pressure pain tolerance,19 were found to be related to postoperative analgesic use. Both factors displayed negative correlation with the amount of analgesics used following surgery.20 In children, doses of morphine titration in PACU was found to be a strong predictor for postoperative morphine consumption by the 3rd day.21
From this study, maximum VNRS within the first 24 hrs has been found as a predictive factor for postoperative opioid consumption after cesarean section. It seems to be straight forward that patients with higher acute postoperative pain intensity require higher dose of analgesics. It has been demonstrated that higher pain scores are associated with higher morphine consumption via patient-controlled analgesia on the first postoperative day.18 Early maximum pain score has also been revealed to associate with opioid administration in PACU.21
Multimodal analgesia combining of drugs with different mechanisms of action22 such as utilizing regular non-opioid analgesic23,24 and opioid as needed, is a standard recommendation for treating postoperative pain.25 In general, paracetamol reduces the use of postoperative opioid, so called opioid sparing effect.26 Conversely, a Cochrane review found that paracetamol did not reduce a requirement for addition postcesarean pain relief.27 Ibuprofen is certainly beneficial for managing mild to moderate postoperative pain and may provide a longer duration of action than paracetamol.28 For dental surgery, NSAIDs were found to be obviously more effective than paracetamol.29 However, a combination of paracetamol and an NSAID may offer better analgesic effect in comparison to either drug alone.23 From this study, patients who took both paracetamol and ibuprofen required less postoperative opioid compared to those who took only paracetamol.
For our primary objective of this study, we have found that ABO blood group is not a predictive factor for postoperative opioid requirement after cesarean section. The previous study in cesarean section patients exhibited that blood group O was a factor affecting postoperative pain severity.8 Result from a study in patients having anterior cruciate ligament reconstruction displayed that different blood types were not related to postoperative analgesic consumption. However, blood group O patients showed a tendency for higher postoperative analgesic consumption in comparison to non-O blood types.30 From an experimental study, blood group B participants showed the lowest mechanical pain sensitivity while AB participants had the strongest conditioned pain modulation effect.31 ABO blood group is influenced by genetics. Up to date, the correlation between ABO blood group and pain intensity or analgesic requirement is inconclusive. Further experimental and clinical investigations are mandatory to explore the truth.
We would like to shed some light on some interesting variables which were statistically significant from univariate analysis but not from multinomial analysis. We did not discover that BMI was correlated with postoperative opioid requirement even the previous study found that BMI was one of the most significant predictors of pain after cesarean section and claimed that it might be associated with insufficient opioid dose in comparison to patients with lower BMI.8 From our study, emergent cesarean section has not been demonstrated as a predictive factor for higher postoperative opioid requirement despite the fact that emergent patients have less time for emotional preparation. Anxiety is more common in patients undergoing emergent surgeries.32 Emergency surgery was found to be a predictive factor for opioid consumption in early postoperative period.17 This study has revealed that skin incision (Pfannenstiel or midline) is not correlated with postoperative opioid consumption. It has been reported that in primary cesarean section, pain score of midline incision group was more than Pfannenstiel incision group in the first 24 hrs but with repeated cesarean section, the result was reverse.33
This study is retrospective in nature so some data were missing. However, we solved this problem by selecting only patients with all the required data in records. The power of this study was calculated to determine significance of ABO blood group on postcesarean opioid consumption so the variables which were not identified as the predictive factors might be due to inadequate power. The strength is this study evaluated the relationship between ABO blood group and postcesarean opioid consumption in a large scale of patients.
Conclusions
ABO blood group is not a predictive factor for opioid requirement within the first 24 hrs following cesarean section. Duration of operation, opioid given in PACU, maximum VNRS on ward and consumption of both paracetamol and ibuprofen have been found to be predictive factors for postcesarean opioid requirement.
Acknowledgments
The authors thank Walailuk Jitpiboon for her assistance in statistical analysis.
Funding
This work was solely supported by Faculty of Medicine, Prince of Songkla University, Hatyai, Songkhla 90110, Thailand.
Disclosure
The authors declare no conflicts of interest for this work.
References
1. Villar J, Valladares E, Wojdyla D, et al. Caesarean delivery rates and pregnancy outcomes: the 2005 WHO global survey on maternal and perinatal health in Latin America. Lancet. 2006;367:1819–1829. doi:10.1016/S0140-6736(06)68704-7
2. Bonnet MP, Mignon A, Mazoit JX, Ozier Y, Marret E. Analgesic efficacy and adverse effects of epidural morphine compared to parenteral opioids after elective caesarean section: a systematic review. Eur J Pain. 2010;14:894–e1. doi:10.1016/j.ejpain.2010.03.003
3. Eisenach JC, Pan PH, Smiley R, Lavand’homme P, Landau R, Houle TT. Severity of acute pain after childbirth, but not type of delivery, predicts persistent pain and postpartum depression. Pain. 2008;140:87–94. doi:10.1016/j.pain.2008.07.011
4. Niklasson B, Georgsson Ohman S, Segerdahl M, Blanck A. Risk factors for persistent pain and its influence on maternal wellbeing after cesarean section. Acta Obstet Gynecol Scand. 2015;94:622–628. doi:10.1111/aogs.12613
5. Kainu JP, Sarvela J, Tiippana E, Halmesmaki E, Korttila KT. Persistent pain after caesarean section and vaginal birth: a cohort study. Int J Obstet Anesth. 2010;19:4–9. doi:10.1016/j.ijoa.2009.03.013
6. Nikolajsen L, Sorensen HC, Jensen TS, Kehlet H. Chronic pain following caesarean section. Acta Anaesthesiol Scand. 2004;48:111–116. doi:10.1111/j.1399-6576.2004.00271.x
7. Sng BL, Sia AT, Quek K, Woo D, Lim Y. Incidence and risk factors for chronic pain after caesarean section under spinal anaesthesia. Anaesth Intensive Care. 2009;37:748–752. doi:10.1177/0310057X0903700513
8. Jasim HH, Sulaiman SA, Khan AH, Rajah UA. Factors affecting post caesarean pain intensity among women in the northern peninsular of Malaysia. J Clin Diagn Res. 2017;11:IC07–IC11.
9. Borges NC, Pereira LV, de Moura LA, Silva TC, Pedroso CF. Predictors for moderate to severe acute postoperative pain after cesarean section. Pain Res Manag. 2016;2016:5783817. doi:10.1155/2016/5783817
10. Pan PH, Tonidandel AM, Aschenbrenner CA, Houle TT, Harris LC, Eisenach JC. Predicting acute pain after cesarean delivery using three simple questions. Anesthesiology. 2013;118:1170–1179. doi:10.1097/ALN.0b013e31828e156f
11. Buhagiar L, Cassar OA, Brincat MP, et al. Predictors of post-caesarean section pain and analgesic consumption. J Anaesthesiol Clin Pharmacol. 2011;27:185–191. doi:10.4103/0970-9185.81822
12. Pan PH, Coghill R, Houle TT, et al. Multifactorial preoperative predictors for postcesarean section pain and analgesic requirement. Anesthesiology. 2006;104:417–425. doi:10.1097/00000542-200603000-00007
13. Edwards CL, Fillingim RB, Keefe F. Race, ethnicity and pain. Pain. 2001;94:133–137. doi:10.1016/S0304-3959(01)00408-0
14. Fillingim RB, Wallace MR, Herbstman DM, Ribeiro-Dasilva M, Staud R. Genetic contributions to pain: a review of findings in humans. Oral Dis. 2008;14:673–682. doi:10.1111/j.1601-0825.2008.01458.x
15. Gradwohl SC, Aranake A, Addallah AB, et al. Intraoperative awareness risk, anesthetic sensitivity, and anesthetic management for patients with natural red hair: a matched cohort study. Can J Anaesth. 2015;62:345–355. doi:10.1007/s12630-014-0305-8
16. Padjen K, Maddalo S, Milord P, Goldfeiz C, Otterbeck R, Gharibo C. Opioids. In: Khelemsky Y, Malhotra A, Gritsenko K, editors. Academic Pain Medicine. Cham: Springer; 2019:63–67.
17. Dahmani S, Dupont H, Mantz J, Desmonts JM, Keita H. Predictive factors of early morphine requirements in the post-anaesthesia care unit (PACU). Br J Anaesth. 2001;87:385–389. doi:10.1093/bja/87.3.385
18. Gagliese L, Gauthier LR, Macpherson AK, Jovellanos M, Chan VW. Correlates of postoperative pain and intravenous patient-controlled analgesia use in younger and older surgical patients. Pain Med. 2008;9:299–314. doi:10.1111/j.1526-4637.2008.00426.x
19. Hsu YW, Somma J, Hung YC, Tsai PS, Yang CH, Chen CC. Predicting postoperative pain by preoperative pressure pain assessment. Anesthesiology. 2005;103:613–618. doi:10.1097/00000542-200509000-00026
20. Abrishami A, Chan J, Chung F, Wong J, Warner DS. Preoperative pain sensitivity and its correlation with postoperative pain and analgesic consumption: a qualitative systematic review. Anesthesiology. 2011;114:445–457. doi:10.1097/ALN.0b013e3181f85ed2
21. Silins V, Brasher C, Antus F, et al. Predicting postoperative morphine consumption in children. Anaesth Crit Care Pain Med. 2017;36:179–184. doi:10.1016/j.accpm.2016.08.005
22. Gritsenko K, Khelemsky Y, Kaye AD, Vadivelu N, Urman RD. Multimodal therapy in perioperative analgesia. Best Pract Res Clin Anaesthesiol. 2014;28:59–79. doi:10.1016/j.bpa.2014.03.001
23. Ong CK, Seymour RA, Lirk P, Merry AF. Combining paracetamol (Acetaminophen) with nonsteroidal antiinflammatory drugs: a qualitative systematic review of analgesic efficacy for acute postoperative pain. Anesth Analg. 2010;110:1170–1179. doi:10.1213/ANE.0b013e3181cf9281
24. Alexander L, Hall E, Eriksson L, Rohlin M. The combination of non-selective NSAID 400 mg and paracetamol 1000 mg is more effective than each drug alone for treatment of acute pain. A systematic review. Swed Dent J. 2014;38:1–14.
25. American Society of Anesthesiologists Task Force on Acute Pain Management. Practice guidelines for acute pain management in the perioperative setting: an updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management. Anesthesiology. 2012;116:248–273. doi:10.1097/ALN.0b013e31823c1030
26. Remy C, Marret E, Bonnet F. Effects of Acetaminophen on morphine side-effects and consumption after major surgery: meta-analysis of randomized controlled trials. Br J Anaesth. 2005;94:505–513. doi:10.1093/bja/aei085
27. Mkontwana N, Novikova N. Oral analgesia for relieving post-caesarean pain. Cochrane Database Syst Rev. 2015;(3):CD010450. doi:10.1002/14651858.CD010450.pub2
28. Slavic-Svircev V, Heidrich G, Kaiko RF, Rusy BF. Ibuprofen in the treatment of postoperative pain. Am J Med. 1984;77:84–86. doi:10.1016/S0002-9343(84)80024-8
29. Hyllested M, Jones S, Pedersen JL, Kehlet H. Comparative effect of paracetamol, NSAIDs or their combination in postoperative pain management: a qualitative review. Br J Anaesth. 2002;88:199–214. doi:10.1093/bja/88.2.199
30. Lausten MB, Rasmussen S, Gazerani P. Association between the ABO blood types and post-operative pain. Eur Neurol Rev. 2018;13:38–43. doi:10.17925/ENR.2018.13.1.38
31. Simoni AH, Jerwiarz A, Randers A, Gazerani P. Association between ABO blood types and pain perception. Somatosens Mot Res. 2017;34:258–264. doi:10.1080/08990220.2018.1425675
32. Latif A, Shamsher khan RM, Nawaz K. Depression and anxiety in patients undergoing elective and emergency surgery: cross-sectional study from Allama Iqbal Memorial Teaching Hospital, Sialkot. J Pak Med Assoc. 2017;67:884–888.
33. Suwannarurk K, Kasemsin P, Pongrojpaw D, et al. Post-cesarean pain associated with skin incision: vertical versus Pfannenstiel. J Med Assoc Thai. 2017;100:162.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.