Back to Journals » Biologics: Targets and Therapy » Volume 19
IRAK4 Targeting: A Breakthrough Approach to Combat Hidradenitis Suppurativa
Authors Zhang H, Liu Z, Qin B, Cheng D, Chen P, Bi X
Received 26 February 2025
Accepted for publication 21 June 2025
Published 30 June 2025 Volume 2025:19 Pages 387—397
DOI https://doi.org/10.2147/BTT.S525106
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Shein-Chung Chow
Hui Zhang,1,* Zhi Liu,1,* Bozhao Qin,2 Dapeng Cheng,1 Peisheng Chen,1 Xinling Bi1
1Department of Dermatology, The First Affiliated Hospital of Naval Medical University, Shanghai, People’s Republic of China; 2Unit for Drug and Instrument Supervision and Inspection of Wuxi Joint Logistics Support Center, Nanjing, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xinling Bi, Department of Dermatology, The First Affiliated Hospital of Naval Medical University, Shanghai, People’s Republic of China, Email [email protected]
Abstract: Hidradenitis suppurativa (HS), a chronic inflammatory condition, features recurrent, painful lesions in the perineal area, severely impairing patients’ quality of life. Despite its clinical significance, HS pathogenesis remains incompletely understood, and effective treatments are scarce. Interleukin-1 receptor-associated kinase 4 (IRAK4) is located downstream of IL-1R/TLR in the IL-1R/TLR signaling pathway, which is upstream of the end products of the pathway. IRAK4-targeted drugs can potentially block this pathway, reducing cytokine secretion and alleviating HS symptoms. This paper comprehensively reviews IRAK4 and its family members’ physiological functions, systematically examines the IRAK family’s roles in the IL-1R/TLR pathway, with a focus on IRAK4, analyzes IRAK4’s specific role in HS, strengthening the theoretical basis for using IRAK4-targeted drugs. The text also covers representative drugs of the major biologics currently used in the treatment of HS and describes the IRAK4 inhibitor Zimlovisertib and the IRAK4 degrader KT-474, along with a discussion of the current status of drugs that inhibit IRAK4 in the treatment of HS and the challenges they face.
Keywords: Hidradenitis suppurativa, interleukin-1 receptor-associated kinase 4, IL-1R/TLR signalling pathway, cytokines
Introduction
IRAK4, a serine/threonine kinase in the IRAK family, is characterized by a conserved N-terminal death domain (DD) and a central kinase domain (KD). The DD binds to the adapter protein myeloid differentiation factor 88 (MyD88), while the KD is responsible for IRAK4’s catalytic activity.1,2 When IL-1R/TLR is activated, the signal is mediated through MyD88 to form a “Myddosome”. MyD88 fulfils the function of a scaffolding protein, which in turn recruits IL-1R-associated kinases (IRAKs). The process of IRAK4 activation results in the phosphorylation of IRAK1, which subsequently forms a complex with TRAF6, thereby triggering the activation of Nuclear Factor kappa-light-chain-enhancer of activated B cells (NF-κB) and Mitogen-activated protein kinase (MAPK) pathways. This process promotes Th1/Th17 cell-mediated inflammation characterised by increased levels of TNF-α, IL-6 and IL-17.3–5
Clinically, HS presents as nodules, abscesses, sinus tracts, and fistulas, accompanied by pain and inflammation, primarily affecting skin folds in areas like the axillae, groin, buttocks, and perianal region.6–9 (shown in Figure 1) HS patients experience reduced quality of life due to physical discomfort, psychological stress, comorbidities such as metabolic and cardiovascular diseases, and a shorter life expectancy.10–12 The true prevalence of HS may be underestimated due to misdiagnosis, with current estimates ranging from 0.05% to 4.1%.13 Although many studies have investigated HS pathophysiology, its exact mechanisms remain unclear. It is widely believed that HS initiates with hair follicle occlusion and rupture, releasing keratin fibers into the dermis, attracting neutrophils and lymphocytes. In the presence of cytokines, this triggers immune responses, leading to dysregulation and HS progression.13,14 The IL-1R/TLR signaling pathway plays an important role in the development of HS, and it has been shown that the expression of IRAK4 in HS lesions is much higher than that of non-lesional skin, and the role of IRAK4 in the IL-1R/TLR signaling pathway is well recognized. IRAK4 expression increases the secretion of pathogenic cytokines through the relevant signaling pathways, thereby exacerbating disease progression in HS.15,16 Currently, clinical trials of IRAK4 inhibitors are underway. Further investigation of the specific molecular mechanisms is likely to be beneficial for the subsequent development of drug trials and to provide a theoretical foundation for the marketing of IRAK4 inhibitors.17
 |
Figure 1 Typical skin lesions of hidradenitis suppurativa. Representative images of the various lesions that are typically found in patient with hidradenitis suppurativa (HS). (a and b) The patient is a 35-year-old male with an onset of symptoms four years. Large dark brown patch on the left buttock with multiple abscesses, sinus tracts, scar formation, and multiple abscesses penetrating on extrusion. Atrophy, scar formation, and multiple abscesses were seen in the axilla, with yellowish pus coming out on extrusion. |
Physiological Functions of IRAK Family Proteins
The IRAK family, consisting of IRAK1, IRAK2, IRAK3 (IRAKM), and IRAK4, is vital in innate immune system.18 The involvement of IRAKs in the IL-1R/TLR signaling pathway depends on specific ligands and cell types, and each member has distinct functions. IRAK4 is the primary mediator in HS.19
IRAK4
IRAK4, a threonine/serine kinase consisting of 460 amino acids, exhibits dual functions of kinase activity and scaffolding.20,21 It is a core mediator in the IL-1R/TLR pathways. Upon the binding of IL-1R/TLRs to DAMPs and PAMPs, IRAK4 is drawn to the MyD88 oligomeric complex. In this complex, IRAK4 serves as a scaffold and displays kinase functions. IRAK4’s kinase activity is crucial for MyD88-dependent cytokine production and plays a key role in Myddosome assembly.22 These roles are indispensable for the downstream signaling processes mediated by NF-κB and MAPK.23–27
Currently, IRAK4-targeted drugs are in clinical trials. These drugs have relieved symptoms in experimental atopic dermatitis (AD) and HS, indicating IRAK4 as a promising target for inflammatory diseases.28 Emavusertib, a selective oral IRAK4 inhibitor, shows safety and efficacy in B-cell non-Hodgkin lymphoma and myeloid malignancies, either as monotherapy or in combination.29–32 Edecesertib, another IRAK4 inhibitor, is being developed for cutaneous lupus erythematosus and rheumatoid arthritis and is well-tolerated and non-toxic.33 Inhibiting IRAK4 kinase activity blocks the NF-κB pathway and reduces chemokine and cytokine production, making IRAK4-targeted drugs a valuable option for HS treatment.22
IRAK1 and IRAK2
IRAK1 and IRAK2 are also members of the IRAK family.34 Unlike IRAK4, under basal conditions, IRAK1 is predominantly in an inactive state and necessitates upstream stimulation to be activated. Serving as a phosphorylation target of IRAK4, IRAK1 experiences extensive ubiquitination and autophosphorylation following the stimulation of IL-1R/TLR.20,35,36 While IRAK1 is not a fundamental component of the Myddosome, it engages in interaction with IRAK4 during the process of Myddosome assembly.18,37 IRAK2, similar to IRAK4, is a crucial Myddosome component and is predicted to be a pseudokinase.38,39 Myddosome formation promotes auto-activation of IRAK4, followed by sequential motivation of IRAK1 and IRAK2.40 Putative binding motifs in IRAK1 and IRAK2 have the capacity to mediate the stimulation of TNF receptor-associated factor 6 (TRAF6) via transient recruitment of the latter to the receptor complex. Upon stimulation, TRAF6 is secreted into the cytoplasm, where it stimulates the NF-κB pathway. Moreover, TRAF6 signalling initiates the MAPK pathway, which in turn leads to the stimulation of activator protein 1 (AP-1) and cAMP-responsive element-binding proteins, leading to the production of proinflammatory cytokines and chemokines.22,41,42
Pacritinib, a highly effective kinase inhibitor, exhibits selective targeting of JAK2/FLT3 and IRAK1.43,44 It suppresses the proliferation of acute myeloid leukemia (AML) cells harboring gene mutations. Primarily, it is utilized in the treatment of hematological malignancies such as primary myelofibrosis.45–47
IRAK3
Like other IRAKs, IRAK3 has an N-terminal death domain and a C-terminal TRAF6 binding site.41 While certain IRAKs play a positive role in regulating the IL-1R/TLR pathway, IRAK3 functions as a negative modulator.48,49 It downregulates the inflammatory response by impeding the dissociation of IRAK1 or IRAK2 from Myddosome complexes. Reduced IRAK3 expression is associated with increased NF-κB activity and elevated inflammatory cytokines.50,51 It downregulates the inflammatory response by impeding the dissociation of IRAK1 or IRAK2 from Myddosome complexes. This inhibitory mechanism of IRAK3 is distinct from the positive regulatory effects of other IRAKs in the IL-1R/TLR signaling cascade. Reduced IRAK3 expression is associated with increased NF-κB activity and elevated inflammatory cytokines.39
The Pivotal Function of IRAK4 in Triggering the IL-1R/TLR Pathway within HS
When a ligand binds to IL-1R/TLR, IRAK4 is attracted to the MyD88 oligomerization complex. Here, it serves dual functions as both a scaffolding molecule and a kinase.17,52 There are two main pathways for IL-1/TLR signaling, the MyD88-dependent pathway and the Toll-IL-1 receptor (TIR)-containing structural domain articulin-induced interferon-β (TRIF) pathway. In the MyD88-dependent pathway, the ligand mediates initial activation, which results in the recruitment of MyD88 to the TIR, followed by the recruitment of IRAK4 to the complex and binding to MyD88 and consequent activation of IRAK1.53 Activation of IRAK1 results in its binding to TRAF6. Subsequently, IRAK1 and TRAF6 are released from the receptor complex and bind to TGF-β-activated kinase 1 (TAK1) and the TAK1-binding protein (TAB) complexes.54 At this point, the inhibitor of κB kinase (IKK) complex promotes the degradation of IκB (NF-κB inhibitor), which in turn translocates the dissociated NF-κB to the nucleus to induce target gene transcription. On the other hand, TAK1 activates MAPK, which further activates AP-1 (a heterodimer of c-Jun), which translocates to the nucleus and coordinates with NF-κB to initiate transcription of various inflammatory cytokines, chemokines, and co-stimulators. The TRIF signaling pathway manifests itself in the binding of TLRs and ligands to activate TRAF3 and TBK1, resulting in the transcription of interferons.55,56 It has been established that, in the presence of TLR3, activation of downstream signalling is initiated through the MyD88 non-dependent pathway.57 Conversely, TLR4 has been demonstrated to activate both MyD88-dependent and non-dependent signalling pathways.58
Cytokines secreted by the IL-1/TLR signaling pathway, in which IRAK4 is involved, such as IL-36, IL-17, TNF-α, IFN-γ, and IL-1β, assume important roles in the pathogenesis of HS. IRAK4 oligomerizes through MyD88 to form the “Myddosome” complex, a central platform for IL-1R/TLR signaling, and phosphorylated IRAK4 activates downstream IRAK1, which together promote activation of the TRAF6/NF-κB pathway.59,60 IL-1β and TNF-α, which are directly upregulated by NF-κB, activate hair follicle epithelial cells and immune cells (such as macrophages), leading to an increase in local vascular permeability and resulting in redness, swelling and pruritus.61 IL-8 (CXCL8) and CXCL1/CXCL2 attract neutrophils to gather around the follicle, and a chemokine gradient directs neutrophils to penetrate the follicle wall, releasing toxic substances such as elastase and myeloperoxidase.62 AP-1 and MAPK synergistically upregulate the transcription of matrix metalloproteinases,63,64 which degrade the follicular basement membrane (eg collagen type IV) and extracellular matrix (ECM), weakening the mechanical stability of the hair follicle and leading to follicular rupture. In skin lesion tissues of HS patients, IRAK4 protein levels were significantly higher than in non-lesion areas and positively correlated with disease severity. Preclinical models showed that IRAK4 inhibitors reduced NF-κB p65 expression,65 neutrophil marker MPO levels and abscess diameter in skin lesion areas.28 This provides substantial evidence in support of the utilisation of IRAK4 inhibitors as a therapeutic intervention for HS. (shown in Figure 2)
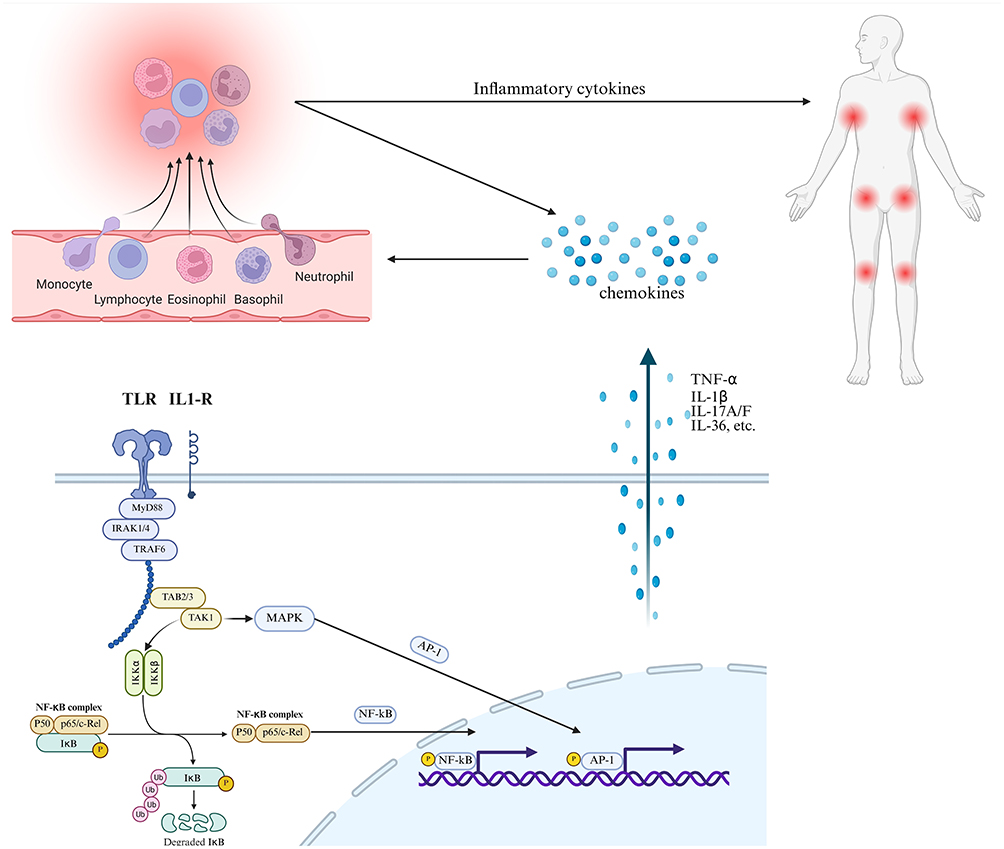 |
Figure 2 Mechanisms of IRAK4 involvement in IL-1R/TLR signaling pathways. |
Current Treatments for Hidradenitis Suppurativa
Current HS treatments are mainly pharmacological and surgical. Pharmacological treatments range from local and intra-lesional therapies for mild cases to systemic medications, including antibiotics, hormones, retinoids, immunosuppressants, and biologics, for moderate to severe cases.66,67 The development of biopharmaceuticals has enabled innovative therapeutic strategies.68
Surgical Treatment for HS
Improved reconstructive surgical techniques are changing the role of surgery in HS treatment from a last resort to an early option. Reconstructing larger defects is now more straightforward, facilitating complete excision of diseased areas. Surgical techniques encompass “de-roofing”, “local excision”, “wide excision”, and “radical excision”, along with the utilization of fascia post-excision.69,70 The application of local regional flaps, perforator flaps, and propeller flaps composed of fascial skin tissue can lead to superior cosmetic and functional results.71–75 However, in cases with tunnels and deep nodules, insufficient excision may lead to local recurrence. Combining biological therapy with surgery is recommended, as it has a higher probability of reducing active nodules by 75%.76
Biological Agents Currently used in the Treatment of HS
Adalimumab
Adalimumab, a TNF-α inhibitor, is the first approved biologic for moderate-to-severe HS. It is a human-derived recombinant IgG1 monoclonal antibody. Its mechanism lies in impeding the interaction between TNF-α and its receptors.77–80 By doing so, it effectively alleviates painful nodules and abscesses, thereby enhancing the skin’s condition.81 However, only 50% of HS patients respond to treatment.82 The most common side effects of Adalimumab include injection site reactions, upper respiratory tract infections, and headache, in addition to the risk of infection (eg, recurrence of tuberculosis) and the risk of potential malignancy, similar to other TNF-α inhibitors.83–85
Secukinumab
Secukinumab, a human monoclonal antibody, selectively blocks the binding of IL-17A to its receptor and is the first approved anti-IL-17A drug for HS.86–88 Secukinumab had a favorable safety profile in Phase III trials, with common side effects of nasopharyngitis, headache, and upper respiratory tract infections,89,90 and no increased risk of serious infections or Candida infections compared to placebo.91 Long-term use (52 weeks) maintained efficacy and a stable safety profile.87
Bimekizumab
Bimekizumab, a humanized antibody binding to IL-17A, IL-17F, and their heterodimers, may block the activation of the IL-17 receptor A and C heterodimer complex. It has a favorable safety profile and provides symptomatic improvement for moderate-to-severe HS patients.82,92–95 Bimekizumab is currently undergoing a review process with the FDA to determine its suitability as a treatment for HS. Bimekizumab showed common side effects of oral candidiasis and mild gastrointestinal reactions in Phase III clinical trials, with a favorable safety profile, rapid onset of action, and significant improvement in HiSCR over 48 weeks.92,95,96
Povorcitinib
Povorcitinib, a selective JAK1 inhibitor, has shown a 29.30% improvement in the dermatological quality of life index in patients, but its efficacy is still under investigation.86,97 Povorcitinib had a manageable safety profile in Phase II clinical trials in the 15–75 mg dose group, with common side effects of mild infections (eg, nasopharyngitis) and dyslipidemia, and was administered orally with dose-dependent inhibition of the JAK1 pathway, which resulted in significant reductions in inflammatory markers over 16 weeks.98,99
Guselkumab
Guselkumab is a fully human IgG1λ monoclonal antibody that selectively targets the p19 subunit of IL-23.100 It has demonstrated encouraging efficacy, primarily in the treatment of psoriasis, and is currently being investigated for potential use in other chronic inflammatory skin diseases. The present study reports on the ongoing clinical trials of the drug in HS. Although case reports and series have demonstrated positive results with Guselkumab, Phase 2 studies have yet to confirm this encouraging trend.101 Guselkumab has demonstrated its efficacy in the treatment of paradoxical HS, as well as cases of HS in patients with paradoxical psoriasis-like reactions following adalimumab treatment. In addition, evidence has demonstrated the efficacy of guselkumab in the treatment of HS patients who also suffer from other comorbidities, such as Crohn’s disease.102 Guselkumab 200 mg subcutaneously every 4 weeks was well tolerated in phase II trials, with side effects comparable to placebo (eg, injection site reactions), and some patients achieved HiSCR at 16 weeks, but efficacy data are more limited.101,103
Zimlovisertib
Zimlovisertib, an IRAK4 inhibitor, has completed Phase II clinical trials and shows promise for HS treatment, though further verification of its clinical efficacy is needed.104,105
KT-474
KT-474 is a highly selective degrader of IRAK4 among proteolysis-targeting chimeras (PROTAC) degraders. It is composed of three key components: a ligand for Cereblon (CRBN), a linker, and a ligand for IRAK4. This unique composition endows KT-474 with its selectivity in targeting IRAK4 for degradation, which is a significant feature in the realm of PROTAC-based molecular regulation.106 It leads to IRAK4 ubiquitylation and proteasomal degradation. In early clinical trials, it exhibited anti-inflammatory properties, was more effective than IRAK4 inhibitors, and had a favorable safety profile, reducing lesion severity and cytokine release in moderate-to-severe HS and AD patients.15,107 (shown in Table 1)
 |
Table 1 Small Molecule Drugs for the Treatment of HS |
Expectations for IRAK4-Targeted Drugs in Therapeutic Management of HS
Possibility of IRAK4-Targeted Drugs for HS Treatment
Multiple immune pathways are upregulated in lesion tissues, including IFN-γ, IL-36, IL-1, IL17A, IL17F, IL-3/IL-5/GM-CSF, etc. In HS skin, notable responses are observed towards IFN-γ and IL-36. However, it fails to respond to Th2 cytokines such as IL-4, as well as to IL-17A or TNF stimulation. In contrast to AD and psoriasis, HS lacks a dominant Th cytokine axis. Distinct cytokine response pattern in HS may reflect unique immunological mechanisms underlying the disease, setting it apart from AD and psoriasis in terms of cytokine-mediated immune regulation. This may explain the limited efficacy of some targeted drugs in HS.108,109 In skin samples from patients with HS, the levels of IRAK4 protein are elevated. Additionally, an increase in the infiltration of IRAK4-positive immune cells is associated with the severity of the disease. In HS lesions, there is an upregulation of inflammatory mediators, which is correlated with the overexpression of IRAK4.15,17 In clinical trials of IRAK4 inhibitors targeting HS, the IRAK4 degrader KT-474 significantly reduced IRAK4 levels in immune cells from PBMCs of healthy volunteers and HS patients and inhibited the production of inflammatory cytokines (eg, TNF-α, IL-6), which may reduce inflammatory infiltration and cytokine release, improve skin lesion severity, and possibly affect the fibrosis process.15,16,110 The mechanism involves the regulation of the MyD88/IRAK4 signaling pathway, but the specific clinical efficacy still needs to be verified in further trials.
Challenges Faced by IRAK4-Targeted Drugs
Despite the potential of IRAK4-targeted drugs, obstacles exist. The KD amino-acid sequences of IRAK1 and IRAK4 exhibit a high degree of homology. As a result, inhibitors designed for IRAK4 might inadvertently act on IRAK1 as well. Although there is currently no reported resistance data, the potential for drug resistance due to active-site mutations exists. Traditional IRAK4 inhibitors cannot fully inhibit all IRAK4 functions due to its dual kinase and scaffolding roles. IRAK4 degraders may address this issue, and the development and application of these drugs will be a focus in the coming years.
Conclusion
HS affects the quality of life of patients and causes considerable psychological and physical distress. However, the existing treatment options, which include various medications and surgical interventions, have been ineffective or recurrent in a substantial proportion of patients with HS. IRAK4 has emerged as a prominent research focus, with its potential as a therapeutic target for inflammatory skin diseases being a key area of investigation. Clinical trials of IRAK4-targeted drugs, including inhibitors and degraders, are underway, showing early promise in alleviating AD and HS symptoms with satisfactory safety. KT-474, the most advanced IRAK4-selective degrader, significantly reduced IRAK4 levels in immune cell types from healthy volunteers and HS patients. Despite the significant clinical potential of IRAK4-targeted therapeutics, several challenges remain. However, it is important to note that a range of issues, including drug resistance, may emerge in the future. The integration of genomic or proteomic profiles of HS patients has the potential to facilitate the personalisation of IRAK4-targeted therapies and to address the challenges posed by emerging resistance mechanisms.
Data Sharing Statement
There are no additional data available.
Author Contributions
Conceptualization: HZ, ZL, XB; Data Curation: HZ, ZL; Formal Analysis: BQ, DC, PC; Validation: HZ, ZL; Supervision and Project Administration: XB; Writing-Review and Editing: HZ, ZL, BQ, DC, PC, XB. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the National Key R&D Program of China (Key Special Project for Marine Environmental Security and Sustainable Development of Coral Reefs 2022-2.4), Clinical Research Plan of SHDC (SHDC22022302) and General Project Incubation Fund of Naval Medical University (2022MS015).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Wesche H, Gao X, Li X, et al. IRAK-M is a novel member of the Pelle/interleukin-1 receptor-associated kinase (IRAK) family. J Biol Chem. 1999;274(27):19403–19410. doi:10.1074/jbc.274.27.19403
2. Bahia MS, Kaur M, Silakari P, et al. Interleukin-1 receptor associated kinase inhibitors: potential therapeutic agents for inflammatory- and immune-related disorders. Cell Signal. 2015;27(6):1039–1055. doi:10.1016/j.cellsig.2015.02.025
3. Edmondson SD. Discovery of the first clinical protein degrader for the treatment of autoimmune indications: orally bioavailable and selective IRAK4 degrader KT-474. J Med Chem. 2024;67(20):18017–18021. doi:10.1021/acs.jmedchem.4c02264
4. Lowe MM, Naik HB, Clancy S, et al. Immunopathogenesis of hidradenitis suppurativa and response to anti-TNF-α therapy. JCI Insight. 2020;5(19). doi:10.1172/jci.insight.139932
5. Witte-Händel E, Wolk K, Tsaousi A, et al. The IL-1 pathway is hyperactive in hidradenitis suppurativa and contributes to skin infiltration and destruction. J Invest Dermatol. 2019;139(6):1294–1305. doi:10.1016/j.jid.2018.11.018
6. Almukhadeb E, Almudimeegh A, Nagshabandi KN, et al. The efficacy and safety of biosimilars in hidradenitis suppurativa: a comprehensive review. Clin Cosmet Investig Dermatol. 2024;17:1841–1851. doi:10.2147/CCID.S478840
7. Sabat R, Jemec GBE, Matusiak Ł, et al. Hidradenitis suppurativa. Nat Rev Dis Primers. 2020;6(1):18. doi:10.1038/s41572-020-0149-1
8. Ghias MH, Hyde MJ, Tomalin LE, et al. Role of the complement pathway in inflammatory skin diseases: a focus on hidradenitis suppurativa. J Invest Dermatol. 2020;140(3):531–536.e531. doi:10.1016/j.jid.2019.09.009
9. Chu CB, Yang CC, Tsai SJ. Hidradenitis suppurativa: disease pathophysiology and sex hormones. Chin J Physiol. 2021;64(6):257–265. doi:10.4103/cjp.cjp_67_21
10. McDonald A, Karnik R, Campbell V, et al. Interleukin 1 receptor-associated kinase 4 is overexpressed in hidradenitis suppurativa skin and correlates with inflammatory biomarkers. J Invest Dermatol. 2024;145(2):323–333.e10. doi:10.1016/j.jid.2024.04.035
11. Sy SMT, Eder L, Jerome D, et al. Prevalence and predictors of inflammatory arthritis in hidradenitis suppurativa. Exp Dermatol. 2024;33(10):e15194. doi:10.1111/exd.15194
12. Almuhanna N, Tobe SW, Alhusayen R. Risk of chronic kidney disease in hospitalized patients with hidradenitis suppurativa. Dermatology. 2023;239(6):912–918. doi:10.1159/000531960
13. Elzawawi KE, Elmakaty I, Habibullah M, et al. Hidradenitis suppurativa and its association with obesity, smoking, and diabetes mellitus: a systematic review and meta-analysis. Int Wound J. 2024;21(9):e70035. doi:10.1111/iwj.70035
14. Campbell C, Mayatra JM, Neve AJ, et al. Inflammasomes: emerging therapeutic targets in hidradenitis suppurativa?. Br J Dermatol. 2024;191(5):670–679. doi:10.1093/bjd/ljae262
15. Ackerman L, Acloque G, Bacchelli S, et al. IRAK4 degrader in hidradenitis suppurativa and atopic dermatitis: a Phase 1 trial. Nat Med. 2023;29(12):3127–3136. doi:10.1038/s41591-023-02635-7
16. McDonald A, Karnik R, Campbell V, et al. IRAK4 is overexpressed in hidradenitis suppurativa skin and correlates with inflammatory biomarkers. J Invest Dermatol. 2025;145(2):323–333.e310.
17. Shirley SN, Watson AE, Yusuf N. Pathogenesis of inflammation in skin disease: from molecular mechanisms to pathology. Int J Mol Sci. 2024;25(18):10152. doi:10.3390/ijms251810152
18. Cao Z, Xiong J, Takeuchi M, et al. TRAF6 is a signal transducer for interleukin-1. Nature. 1996;383(6599):443–446. doi:10.1038/383443a0
19. Moon AM, Singal AG, Tapper EB. Contemporary epidemiology of chronic liver disease and cirrhosis. Clin Gastroenterol Hepatol. 2020;18(12):2650–2666. doi:10.1016/j.cgh.2019.07.060
20. Li S, Strelow A, Fontana EJ, et al. IRAK-4: a novel member of the IRAK family with the properties of an IRAK-kinase. Proc Natl Acad Sci U S A. 2002;99(8):5567–5572. doi:10.1073/pnas.082100399
21. Cushing L, Stochaj W, Siegel M, et al. Interleukin 1/Toll-like receptor-induced autophosphorylation activates interleukin 1 receptor-associated kinase 4 and controls cytokine induction in a cell type-specific manner. J Biol Chem. 2014;289(15):10865–10875. doi:10.1074/jbc.M113.544809
22. De Nardo D, Balka KR, Cardona Gloria Y, et al. Interleukin-1 receptor-associated kinase 4 (IRAK4) plays a dual role in myddosome formation and toll-like receptor signaling. J Biol Chem. 2018;293(39):15195–15207. doi:10.1074/jbc.RA118.003314
23. Dinarello CA. Overview of the IL-1 family in innate inflammation and acquired immunity. Immunol Rev. 2018;281(1):8–27. doi:10.1111/imr.12621
24. Cushing L, Winkler A, Jelinsky SA, et al. IRAK4 kinase activity controls toll-like receptor-induced inflammation through the transcription factor IRF5 in primary human monocytes. J Biol Chem. 2017;292(45):18689–18698. doi:10.1074/jbc.M117.796912
25. Navrazhina K, Frew JW, Gilleaudeau P, et al. Epithelialized tunnels are a source of inflammation in hidradenitis suppurativa. J Allergy Clin Immunol. 2021;147(6):2213–2224. doi:10.1016/j.jaci.2020.12.651
26. Pereira M, Gazzinelli RT. Regulation of innate immune signaling by IRAK proteins. Front Immunol. 2023;14:1133354. doi:10.3389/fimmu.2023.1133354
27. Sun J, Li N, Oh KS, et al. Comprehensive RNAi-based screening of human and mouse TLR pathways identifies species-specific preferences in signaling protein use. Sci Signal. 2016;9(409):ra3. doi:10.1126/scisignal.aab2191
28. Yue C, Hu Y, Yu J, et al. IL-38 aggravates atopic dermatitis via facilitating migration of Langerhans cells. Int J Biol Sci. 2024;20(8):3094–3112. doi:10.7150/ijbs.93843
29. Choudhary GS, Pellagatti A, Agianian B, et al. Activation of targetable inflammatory immune signaling is seen in myelodysplastic syndromes with SF3B1 mutations. Elife. 2022;11. doi:10.7554/eLife.78136
30. Parrondo RD, Iqbal M, Von Roemeling R, et al. IRAK-4 inhibition: emavusertib for the treatment of lymphoid and myeloid malignancies. Front Immunol. 2023;14:1239082. doi:10.3389/fimmu.2023.1239082
31. Guidetti F, Arribas AJ, Sartori G, et al. Targeting IRAK4 with Emavusertib in lymphoma models with secondary resistance to PI3K and BTK inhibitors. J Clin Med. 2023;12(2):399. doi:10.3390/jcm12020399
32. Seipel K, Mandhair H, Bacher U, et al. FLT3 and IRAK4 inhibitor emavusertib in combination with BH3-mimetics in the treatment of acute myeloid leukemia. Curr Issues Mol Biol. 2024;46(4):2946–2960. doi:10.3390/cimb46040184
33. Bai YR, Yang WG, Hou XH, et al. The recent advance of Interleukin-1 receptor associated kinase 4 inhibitors for the treatment of inflammation and related diseases. Eur J Med Chem. 2023;258:115606. doi:10.1016/j.ejmech.2023.115606
34. Flannery S, Bowie AG. The interleukin-1 receptor-associated kinases: critical regulators of innate immune signalling. Biochem Pharmacol. 2010;80(12):1981–1991. doi:10.1016/j.bcp.2010.06.020
35. Emmerich CH, Ordureau A, Strickson S, et al. Activation of the canonical IKK complex by K63/M1-linked hybrid ubiquitin chains. Proc Natl Acad Sci U S A. 2013;110(38):15247–15252. doi:10.1073/pnas.1314715110
36. Kollewe C, Mackensen AC, Neumann D, et al. Sequential autophosphorylation steps in the interleukin-1 receptor-associated kinase-1 regulate its availability as an adapter in interleukin-1 signaling. J Biol Chem. 2004;279(7):5227–5236. doi:10.1074/jbc.M309251200
37. Vollmer S, Strickson S, Zhang T, et al. The mechanism of activation of IRAK1 and IRAK4 by interleukin-1 and Toll-like receptor agonists. Biochem J. 2017;474(12):2027–2038. doi:10.1042/BCJ20170097
38. Janssens S, Beyaert R. Functional diversity and regulation of different interleukin-1 receptor-associated kinase (IRAK) family members. Mol Cell. 2003;11(2):293–302. doi:10.1016/S1097-2765(03)00053-4
39. Wang ZY, Gao ST, Gou XJ, et al. IL-1 receptor-associated kinase family proteins: an overview of their role in liver disease. Eur J Pharmacol. 2024;978:176773. doi:10.1016/j.ejphar.2024.176773
40. Kawagoe T, Sato S, Matsushita K, et al. Sequential control of toll-like receptor-dependent responses by IRAK1 and IRAK2. Nat Immunol. 2008;9(6):684–691. doi:10.1038/ni.1606
41. Ye H, Arron JR, Lamothe B, et al. Distinct molecular mechanism for initiating TRAF6 signalling. Nature. 2002;418(6896):443–447. doi:10.1038/nature00888
42. Takaoka A, Yanai H, Kondo S, et al. Integral role of IRF-5 in the gene induction programme activated by Toll-like receptors. Nature. 2005;434(7030):243–249. doi:10.1038/nature03308
43. Masarova L, Chifotides HTD. How I individualize selection of JAK inhibitors for patients with myelofibrosis. Blood. 2024;2024:1.
44. Kim KM, Hwang NH, Hyun JS, et al. Recent advances in IRAK1: pharmacological and therapeutic aspects. Molecules. 2024;29(10). doi:10.3390/molecules29102226
45. Hosseini MM, Kurtz SE, Abdelhamed S, et al. Inhibition of interleukin-1 receptor-associated kinase-1 is a therapeutic strategy for acute myeloid leukemia subtypes. Leukemia. 2018;32(11):2374–2387. doi:10.1038/s41375-018-0112-2
46. Oh ST, Mesa RA, Harrison CN, et al. Pacritinib is a potent ACVR1 inhibitor with significant anemia benefit in patients with myelofibrosis. Blood Adv. 2023;7(19):5835–5842. doi:10.1182/bloodadvances.2023010151
47. Nair PC, Piehler J, Tvorogov D, et al. Next-generation JAK2 inhibitors for the treatment of myeloproliferative neoplasms: lessons from structure-based drug discovery approaches. Blood Cancer Discov. 2023;4(5):352–364. doi:10.1158/2643-3230.BCD-22-0189
48. Zhou H, Yu M, Fukuda K, et al. IRAK-M mediates toll-like receptor/IL-1R-induced NFκB activation and cytokine production. EMBO j. 2013;32(4):583–596. doi:10.1038/emboj.2013.2
49. Kobayashi K, Hernandez LD, Galán JE, et al. IRAK-M is a negative regulator of toll-like receptor signaling. Cell. 2002;110(2):191–202. doi:10.1016/S0092-8674(02)00827-9
50. Liu ZJ, Yan LN, Li XH, et al. Up-regulation of IRAK-M is essential for endotoxin tolerance induced by a low dose of lipopolysaccharide in Kupffer cells. J Surg Res. 2008;150(1):34–39. doi:10.1016/j.jss.2007.12.759
51. Srivastav S, Saha A, Barua J, et al. IRAK-M regulates the inhibition of TLR-mediated macrophage immune response during late in vitro Leishmania donovani infection. Eur J Immunol. 2015;45(10):2787–2797. doi:10.1002/eji.201445336
52. Rosi E, Fastame MT, Scandagli I, et al. Insights into the pathogenesis of HS and therapeutical approaches. Biomedicines. 2021;9(9):1168. doi:10.3390/biomedicines9091168
53. Li Y, Shah RB, Sarti S, et al. A noncanonical IRAK4-IRAK1 pathway counters DNA damage-induced apoptosis independently of TLR/IL-1R signaling. Sci Signal. 2023;16(816):eadh3449. doi:10.1126/scisignal.adh3449
54. Shen H, Yuan J, Tong D, et al. Regulator of G protein signaling 16 restrains apoptosis in colorectal cancer through disrupting TRAF6-TAB2-TAK1-JNK/p38 MAPK signaling. Cell Death Dis. 2024;15(6):438. doi:10.1038/s41419-024-06803-6
55. Lee CS, Hwang G, Nam YW, et al. IKK-mediated TRAF6 and RIPK1 interaction stifles cell death complex assembly leading to the suppression of TNF-α-induced cell death. Cell Death Differ. 2023;30(6):1575–1584. doi:10.1038/s41418-023-01161-w
56. Talreja J, Bauerfeld C, Wang X, et al. MKP-1 modulates ubiquitination/phosphorylation of TLR signaling. Life Sci Alliance. 2021;4(12):e202101137. doi:10.26508/lsa.202101137
57. Yin Y, Liu Z, Li Q, et al. Identification and evolution of PDK-1-like involving lamprey innate immunity. Mol Immunol. 2024;172:47–55. doi:10.1016/j.molimm.2024.06.001
58. Chen Z, Chen X, Zou Y, et al. The immune function of TLR4-1 gene in octopus sinensis revealed by RNAi and RNA-seq. Fish Shellfish Immunol. 2024;154:109899. doi:10.1016/j.fsi.2024.109899
59. Choudhary SA, Patra D, Sinha A, et al. A small molecule potent IRAK4 inhibitor abrogates lipopolysaccharide-induced macrophage inflammation in-vitro and in-vivo. Eur J Pharmacol. 2023;944:175593. doi:10.1016/j.ejphar.2023.175593
60. Najjar MK, Khan MS, Zhuang C, et al. Interleukin-1 receptor-associated kinase 1 in cancer metastasis and therapeutic resistance: mechanistic insights and translational advances. Cells. 2024;13(20):1690. doi:10.3390/cells13201690
61. Molinelli E, Gioacchini H, Sapigni C, et al. New insight into the molecular pathomechanism and immunomodulatory treatments of hidradenitis suppurativa. Int J Mol Sci. 2023;24(9):8428. doi:10.3390/ijms24098428
62. Wang Q, Zhang X, Han C, et al. Immunodynamic axis of fibroblast-driven neutrophil infiltration in acute pancreatitis: NF-κB-HIF-1α-CXCL1. Cell Mol Biol Lett. 2025;30(1):57. doi:10.1186/s11658-025-00734-6
63. Woessner JF Jr. Matrix metalloproteinases and their inhibitors in connective tissue remodeling. FASEB j. 1991;5(8):2145–2154. doi:10.1096/fasebj.5.8.1850705
64. Wang Y, Mou C, Huang L, et al. The ethanolic extract of Rhaphidophora peepla prevents inflammation by inhibiting the activation of Syk/AKT/NF-κB and TAK1/MAPK/AP-1. Phytomedicine. 2025;136:156339. doi:10.1016/j.phymed.2024.156339
65. Zhaohua Z, Rong L, Nana DU, et al. Efficacy of Sishen Wan on dinitrobenzene sulfonic acid-induced ulcerative colitis and its effect on toll-like receptor 2/interleukin-1 receptor-associated kinase-4/nuclear factor-κB signal pathway. J Tradit Chin Med. 2022;42(4):565–575. doi:10.19852/j.cnki.jtcm.20220608.001
66. Taylor EM, Hamaguchi R, Kramer KM, et al. Plastic surgical management of hidradenitis suppurativa. Plast Reconstr Surg. 2021;147(3):479–491. doi:10.1097/PRS.0000000000007677
67. Zouboulis CC, Desai N, Emtestam L, et al. European S1 guideline for the treatment of hidradenitis suppurativa/acne inversa. J Eur Acad Dermatol Venereol. 2015;29(4):619–644. doi:10.1111/jdv.12966
68. Świerczewska Z, Lewandowski M, Surowiecka A, et al. Immunomodulatory drugs in the treatment of hidradenitis suppurativa-possibilities and limitations. Int J Mol Sci. 2022;23(17):9716. doi:10.3390/ijms23179716
69. Bouazzi D, Chafranska L, Saunte DML, et al. Systematic review of complications and recurrences after surgical interventions in hidradenitis suppurativa. Dermatol Surg. 2020;46(7):914–921. doi:10.1097/DSS.0000000000002323
70. Mehdizadeh A, Hazen PG, Bechara FG, et al. Recurrence of hidradenitis suppurativa after surgical management: a systematic review and meta-analysis. J Am Acad Dermatol. 2015;73(5 Suppl 1):S70–77. doi:10.1016/j.jaad.2015.07.044
71. Clark SR, Soti V. Effectiveness of surgical deroofing and carbon dioxide laser in moderate-to-severe hidradenitis suppurativa patients. Cureus. 2024;16(3):e56959. doi:10.7759/cureus.56959
72. Krajewski A, Alsayed A, Capek A, et al. Surgical management of hidradenitis suppurativa. Plast Reconstr Surg Glob Open. 2024;12(6):e5860. doi:10.1097/GOX.0000000000005860
73. Manfredini M, Garbarino F, Bigi L, et al. Hidradenitis suppurativa: surgical and postsurgical management. Skin Appendage Disord. 2020;6(4):195–201. doi:10.1159/000507297
74. Wong HS, Jiang JY, Huang SD, et al. A review of surgical and reconstructive techniques for hidradenitis suppurativa. Arch Dermatol Res. 2024;316(6):270. doi:10.1007/s00403-024-03000-5
75. Riddle A, Westerkam L, Feltner C, et al. Current surgical management of hidradenitis suppurativa: a systematic review and meta-analysis. Dermatol Surg. 2021;47(3):349–354. doi:10.1097/DSS.0000000000002892
76. Shanmugam VK, Mulani S, McNish S, et al. Longitudinal observational study of hidradenitis suppurativa: impact of surgical intervention with adjunctive biologic therapy. Int J Dermatol. 2018;57(1):62–69. doi:10.1111/ijd.13798
77. Ingram JR, Burton T. NICE approval of Adalimumab for moderate-to-severe hidradenitis suppurativa: the end of the beginning for hidradenitis suppurativa therapeutics? Br J Dermatol. 2017;176(2):281–282. doi:10.1111/bjd.15255
78. Khosravi H, Anderson AM, Kettering C, et al. Real-world experience of Adalimumab in the treatment of hidradenitis suppurativa. J Am Acad Dermatol. 2021;84(5):1406–1409. doi:10.1016/j.jaad.2020.12.012
79. Murdaca G, Colombo BM, Puppo F. Adalimumab for the treatment of immune-mediated diseases: an update on old and recent indications. Drugs Today. 2011;47(4):277–288. doi:10.1358/dot.2011.47.4.1576692
80. Sahl RE, Poggi AI, Nielsen VW, et al. Adalimumab treatment effects on inflammation and adipose tissue mitochondrial respiration in hidradenitis suppurativa. Endocrinol Diabetes Metab. 2024;7(6):e70002. doi:10.1002/edm2.70002
81. Kyriakou A, Trigoni A, Galanis N, et al. Efficacy of adalimumab in moderate to severe hidradenitis suppurativa: real life data. Dermatol Reports. 2018;10(2):7859. doi:10.4081/dr.2018.7859
82. Malvaso D, Calabrese L, Chiricozzi A, et al. IL-17 inhibition: a valid therapeutic strategy in the management of hidradenitis suppurativa. Pharmaceutics. 2023;15(10):2450. doi:10.3390/pharmaceutics15102450
83. Sabat R, Alavi A, Wolk K, et al. Hidradenitis suppurativa. Lancet. 2025;405(10476):420–438. doi:10.1016/S0140-6736(24)02475-9
84. Charrow A, Santiago-Soltero K, Porter M. Biologics in hidradenitis suppurativa: progress and new directions. J Am Acad Dermatol. 2024;91(6s):S27–s30. doi:10.1016/j.jaad.2024.09.027
85. Heidari A, Ghane Y, Heidari N, et al. Golimumab and certolizumab pegol for the treatment of hidradenitis suppurativa: a literature review and future perspective. Ther Adv Chronic Dis. 2024;15:20406223241257342. doi:10.1177/20406223241257342
86. Gao JL, Otto TS, Porter ML, et al. Hidradenitis suppurativa: new targets and emerging treatments. Am J Clin Dermatol. 2024;25(5):765–778. doi:10.1007/s40257-024-00880-1
87. Roccuzzo G, Repetto F, Giordano S, et al. Anti-IL17 secukinumab in hidradenitis suppurativa: a long-term drug survival analysis. Exp Dermatol. 2024;33(7):e15140. doi:10.1111/exd.15140
88. Stergianou D, Kanni T, Damoulari C, et al. An evaluation of secukinumab for the treatment of moderate-to-severe hidradenitis suppurativa. Expert Opin Biol Ther. 2024;24(4):225–232. doi:10.1080/14712598.2024.2343112
89. Snyder CL, Gibson RS, Porter ML, et al. Secukinumab in the treatment of hidradenitis suppurativa. Immunotherapy. 2023;15(17):1449–1457. doi:10.2217/imt-2023-0103
90. Kimball AB, Jemec GBE, Alavi A, et al. Secukinumab in moderate-to-severe hidradenitis suppurativa (SUNSHINE and SUNRISE): week 16 and week 52 results of two identical, multicentre, randomised, placebo-controlled, double-blind Phase 3 trials. Lancet. 2023;401(10378):747–761. doi:10.1016/S0140-6736(23)00022-3
91. Tsai YC, Hung CY, Tsai TF. Efficacy and safety of biologics and small molecules for moderate-to-severe hidradenitis suppurativa: a systematic review and network meta-analysis. Pharmaceutics. 2023;15(5):1351. doi:10.3390/pharmaceutics15051351
92. Molinelli E, De Simoni E, Simonetti O. Expanding the frontiers of therapeutic options in hidradenitis suppurativa: the valid contribution of bimekizumab. Med. 2024;5(10):1197–1199. doi:10.1016/j.medj.2024.08.005
93. Molinelli E, Simonetti O. Bimekizumab: dual inhibition as a promising tool in the management of hidradenitis suppurativa. Lancet. 2024;403(10443):2457–2459. doi:10.1016/S0140-6736(24)00591-9
94. Guermazi D, Shah A, Yumeen S, et al. The use of biologics and JAK inhibitors in the management of moderate to severe hidradenitis suppurativa treatment: a scoping review. Arch Dermatol Res. 2024;316(6):259. doi:10.1007/s00403-024-03121-x
95. Kimball AB, Jemec GBE, Sayed CJ, et al. Efficacy and safety of bimekizumab in patients with moderate-to-severe hidradenitis suppurativa (BE HEARD I and BE HEARD II): two 48-week, randomised, double-blind, placebo-controlled, multicentre phase 3 trials. Lancet. 2024;403(10443):2504–2519. doi:10.1016/S0140-6736(24)00101-6
96. Shams RB, Sayed CJ. Bimekizumab for the treatment of hidradenitis suppurativa. Immunotherapy. 2024;16(16–17):1005–1013. doi:10.1080/1750743X.2024.2401308
97. Liu H, Santos LL, Smith SH. Modulation of disease-associated pathways in hidradenitis suppurativa by the janus kinase 1 inhibitor povorcitinib: transcriptomic and proteomic analyses of two phase 2 studies. Int J Mol Sci. 2023;24(8):7185.
98. Kirby JS, Okun MM, Alavi A, et al. Efficacy and safety of the oral Janus kinase 1 inhibitor povorcitinib (INCB054707) in patients with hidradenitis suppurativa in a phase 2, randomized, double-blind, dose-ranging, placebo-controlled study. J Am Acad Dermatol. 2024;90(3):521–529. doi:10.1016/j.jaad.2023.10.034
99. Heidari A, Ghane Y, Heidari N, et al. A systematic review of janus kinase inhibitors and spleen tyrosine kinase inhibitors for hidradenitis suppurativa treatment. Int Immunopharmacol. 2024;127:111435. doi:10.1016/j.intimp.2023.111435
100. Orzan OA, Țieranu CG, Olteanu AO, et al. An insight on the possible association between inflammatory bowel disease and biologic therapy with IL-17 inhibitors in psoriasis patients. Pharmaceutics. 2023;15(8):2171. doi:10.3390/pharmaceutics15082171
101. Kimball AB, Podda M, Alavi A, et al. Guselkumab for the treatment of patients with moderate-to-severe hidradenitis suppurativa: a phase 2 randomized study. J Eur Acad Dermatol Venereol. 2023;37(10):2098–2108. doi:10.1111/jdv.19252
102. Bubna AK, Viplav V. Guselkumab - In Psoriasis and Beyond. Dermatol Pract Concept. 2024;14(3):e2024181.
103. Dudink K, Bouwman K, Chen Y, et al. Guselkumab for hidradenitis suppurativa: a Phase II, open-label, mode-of-action study. Br J Dermatol. 2023;188(5):601–609. doi:10.1093/bjd/ljad010
104. Kimball AB, Peeva E, Forman S, et al. Brepocitinib, Zimlovisertib, and Ropsacitinib in Hidradenitis Suppurativa. NEJM Evid. 2024;3(3):EVIDoa2300155. doi:10.1056/EVIDoa2300155
105. Wright SW, Farley KA, Han S, et al. In retrospect: root-cause analysis of structure-activity relationships in IRAK4 inhibitor zimlovisertib (PF-06650833). ACS Med Chem Lett. 2024;15(4):540–545. doi:10.1021/acsmedchemlett.4c00036
106. Yifan Feng CC, Shao A, Lei W, Haiyu H, Zhang T, Zhang T. Emerging interleukin-1 receptor-associated kinase 4 (IRAK4) inhibitors or degraders as therapeutic agents for autoimmune diseases and cancer. Acta Pharmaceutica Sinica B. 2024;14(12):5091–5105. doi:10.1016/j.apsb.2024.09.008
107. Zheng X, Ji N, Campbell V, et al. Discovery of KT-474─a Potent, Selective, and Orally Bioavailable IRAK4 Degrader for the Treatment of Autoimmune Diseases. J Med Chem. 2024;67:18022–37.
108. Ben Abdallah H, Bregnhøj A, Iversen L, et al. Transcriptomic analysis of hidradenitis suppurativa: a unique molecular signature with broad immune activation. Int J Mol Sci. 2023;24(23):17014. doi:10.3390/ijms242317014
109. Silverberg JI, Thyssen JP, Fahrbach K, et al. Comparative efficacy and safety of systemic therapies used in moderate-to-severe atopic dermatitis: a systematic literature review and network meta-analysis. J Eur Acad Dermatol Venereol. 2021;35(9):1797–1810. doi:10.1111/jdv.17351
110. Lavazais S, Jargosch M, Dupont S, et al. IRAK4 inhibition dampens pathogenic processes driving inflammatory skin diseases. Sci Transl Med. 2023;15(683):eabj3289. doi:10.1126/scitranslmed.abj3289
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.