Back to Journals » Drug Design, Development and Therapy » Volume 20
Investigation of Esketamine Administration During Surgical Procedures for the Alleviation of Postoperative Anxiety and Depression in Adolescent Patients: A Randomized Controlled Trial
Authors Li Y, Zhao K ![]() , Cao P
, Cao P ![]() , Wang Q
, Wang Q ![]() , Li K, Zhou J
, Li K, Zhou J ![]()
Received 10 December 2025
Accepted for publication 26 May 2026
Published 3 June 2026 Volume 2026:20 587626
DOI https://doi.org/10.2147/DDDT.S587626
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Anastasios Lymperopoulos
Yanhong Li,1 Kuangyu Zhao,2 Peipei Cao,2 Qian Wang,2 Kairui Li,2 Jun Zhou2
1School of Medicine, Zhengzhou University of Industrial Technology, Zhengzhou, Henan, People’s Republic of China; 2Department of Anaesthesiology and Perioperative Medicine, Henan Provincial People’s Hospital, Zhengzhou, Henan, People’s Republic of China
Correspondence: Jun Zhou, Department of Anaesthesiology and Perioperative Medicine, Henan Provincial People’s Hospital, Zhengzhou, Henan, 450000, People’s Republic of China, Email [email protected]
Background: Surgical stress can lead to postoperative anxiety and depression, especially in adolescents. These complications reduce quality of life and increase medical burdens, but perioperative psychological interventions for adolescents are limited, and related mechanisms remain unclear. Esketamine (S-ketamine), an N-methyl-D-aspartate receptor (NMDAR) antagonist, has analgesic, sedative, antidepressant, and anxiolytic effects, yet its efficacy and safety in adolescent surgical patients have not been systematically studied.
Purpose: This study seeks to investigate the prophylactic efficacy of subanesthetic-dose S-ketamine in mitigating postoperative anxiety and depression among adolescent patients.
Methods: In this prospective double-blind randomized placebo-controlled trial, 92 American Society of Anesthesiologists (ASA) I–II adolescents aged 13– 18 years undergoing elective surgery were randomly assigned to receive intravenous esketamine (0.25 mg/kg) or normal saline at skin incision. Anxiety and depression were assessed with the Hospital Anxiety and Depression Scale (HADS); serum C-reactive protein (CRP) and interleukin-6 (IL-6) were measured; pain was evaluated using the NRS. Adverse events were recorded.
Results: Eighty patients completed the study. The esketamine group had significantly lower anxiety scores on postoperative days 1, 3, 7, and 14 (P < 0.05). Depression scores differed significantly only on day 14 (P = 0.043). There were no significant between‑group differences in inflammatory markers or adverse events. Esketamine was a protective factor against postoperative anxiety (OR = 0.38, P < 0.05).
Conclusion: Subanesthetic-dose esketamine during surgery effectively reduces postoperative anxiety and partially alleviates depressive symptoms in adolescents with acceptable safety. Limited by sample size and single‑center design, multicenter studies with longer follow‑up are warranted.
Keywords: postoperative anxiety and depression in adolescents, S-ketamine, inflammatory markers, postoperative pain
Introduction
Surgery acts as a physiological stressor, activating the hypothalamic-pituitary-adrenal (HPA) axis and triggering a systemic stress response. This process induces substantial secretion of cortisol and glucocorticoids, thereby disrupting homeostasis and causing significant alterations in the internal environment. Such physiological perturbations frequently manifest as postoperative complications, including inflammatory responses, nociceptive pain perception, and circadian rhythm disturbances. Furthermore, these pathophysiological changes often precipitate psychological comorbidities, particularly anxiety and depressive disorders. Anxiety represents a maladaptive emotional state characterized by excessive apprehension regarding potential future threats, typically accompanied by both somatic and cognitive symptoms. Depression constitutes a mood disorder marked by persistent anhedonia, dysphoria, and psychomotor retardation, frequently associated with impaired cognitive function and behavioral alterations1,2 Anxiety and depression represent distinct yet frequently comorbid psychiatric disorders, characterized by overlapping clinical manifestations, behavioral patterns, and shared genetic and environmental etiological pathways. Consequently, these conditions are commonly investigated as comorbid entities, which are associated with both acute and chronic detrimental health consequences. The emergence or persistence of anxiety and depression following surgical procedures not only elevates healthcare expenditures but also substantially diminishes patients’ quality of life.3,4 Research indicates that the prevalence of postoperative anxiety symptoms surpasses 20%, with this condition frequently co-occurring with elevated rates of additional postoperative complications.5 Anxiety and depression represent distinct mental disorders; however, they frequently co-occur as comorbid conditions. These disorders exhibit overlapping clinical manifestations, behavioral traits, and shared genetic and environmental etiological mechanisms. Consequently, they are commonly investigated as comorbid entities and are linked to both acute and chronic adverse health outcomes. Adolescents, in contrast to adults, exhibit unique physiological characteristics. The ventromedial prefrontal cortex (vmPFC), a key region for emotional regulation, undergoes incomplete maturation, reaching only approximately 60% of its developmental capacity by age 15. This delayed neurodevelopment contributes to heightened emotional reactivity in adolescents, as evidenced by elevated amygdala activity levels compared to adults;6–9 Furthermore, the expression density of the glutamate N-methyl-D-aspartate (NMDA) receptor subunit 2C (GluN2C) exhibits a significant peak during adolescence, demonstrating approximately 40% higher levels compared to adult stages. This heightened receptor expression may predispose individuals to excessive neuronal excitation, potentially increasing vulnerability to anxiety and depressive disorders.10,11 The synergistic interaction of these factors significantly elevates the risk of postoperative anxiety and depression among adolescent populations. These psychiatric conditions have emerged as critical public health concerns that substantially compromise the physical and psychological well-being of adolescents.12 The invasiveness of surgical procedures, potential nerve damage or postoperative pain, as well as disruptions to daily routines and altered expectations in adolescent patients, frequently contribute to the development of anxiety and depression following surgery.13–15 Currently, research on postoperative anxiety and depression in adolescent populations remains limited, with underlying mechanisms poorly understood. Furthermore, evidence-based preventive and therapeutic interventions are lacking. Consequently, optimizing perioperative pharmacological management to minimize surgical trauma, alleviate postoperative pain, and prevent the development of anxiety and depressive symptoms in adolescent patients represents a critical challenge in contemporary anesthesiology practice.
(R,S)-Ketamine (commonly referred to as ketamine) is a racemic N-methyl-D-aspartate receptor (NMDAR) antagonist composed of equimolar proportions of (R)-ketamine (arketamine) and (S)-ketamine (esketamine). This compound exhibits diverse pharmacological effects, including analgesia, sedation, and notable antidepressant properties. Preclinical investigations have demonstrated that the rapid antidepressant effects of ketamine in rodent models of depression are mediated through blockade of the lateral habenula (LHb). Notably, electrophysiological studies have revealed that LHb neurons exhibit significantly enhanced burst firing patterns in animals displaying depressive-like behavioral phenotypes.16 The LHb is a type of glutamatergic neuron,17 It inhibits the brain’s reward centers, including the dopaminergic ventral tegmental area (VTA) and the serotonergic dorsal raphe nucleus (DRN). Diminished activity in the LHb has been implicated in the pathophysiology of depression. Ketamine administration has been shown to attenuate the burst firing patterns of LHb neurons, thereby mediating its rapid antidepressant effects.18,19
Esketamine, the S(+)-enantiomer of ketamine, exhibits higher binding affinity for NMDARs compared to its racemic counterpart, while demonstrating reduced adverse effects on the central nervous system.20,21 Research has demonstrated that intravenous administration of esketamine (0.5 mg/kg infused over 40 minutes) elicits rapid-onset and prolonged antidepressant responses in individuals diagnosed with treatment-resistant major depressive disorder (MDD),22,23 Subanesthetic doses of esketamine (0.2 and 0.4 mg/kg, administered via intravenous infusion) have demonstrated rapid and robust antidepressant effects in patients with treatment-resistant major depressive disorder.24 The therapeutic effectiveness of low-dose esketamine in managing treatment-resistant depression among adolescent populations has been empirically validated.25
The HPA axis activation observed in patients with anxiety and depressive disorders contributes to the manifestation of physiological stress responses. Notably, these patients exhibit significantly elevated levels of inflammatory biomarkers, including interleukin-6 (IL-6), interleukin-8 (IL-8), C-reactive protein (CRP), and tumor necrosis factor-alpha (TNF-α).26 IL-6 plays a pivotal role in initiating and modulating immune responses. As demonstrated by Sforzim et al, this pleiotropic cytokine exhibits the capacity to activate diverse immunological pathways.27 Evidence suggests that serum CRP levels are significantly elevated in patients with depression compared to non-depressed individuals, with CRP concentrations demonstrating a positive correlation with depression severity. Clinical research further indicates that neuroinflammatory processes may contribute to the pathogenesis of anxiety and depressive disorders, as evidenced by marked alterations in serum IL-6 and CRP levels during depressive and anxious states.19,28,29 Surgical trauma and postoperative pain can exacerbate the stress response in patients, subsequently elevating systemic levels of inflammatory markers, including CRP and IL-6.30 Emerging evidence indicates that esketamine exerts anti-inflammatory properties by modulating inflammatory cytokine levels, which may contribute to the mitigation of postoperative anxiety and depressive symptoms. The underlying mechanisms involve the activation of the brain-derived neurotrophic factor (BDNF)/tropomyosin receptor kinase B (TrkB) signaling pathway, coupled with the suppression of the nuclear factor-κB (NF-κB) pathway.31 Esketamine has been demonstrated to downregulate glycogen synthase kinase-3 (GSK-3) activity and suppress the kynurenine pathway, indicating a potential mechanistic link between ketamine administration and reduced pro-inflammatory cytokine levels.26
However, existing research findings are exclusively derived from adult populations, leaving a significant gap in evidence regarding adolescent cohorts. This study proposes to implement a prospective, double-blind, randomized controlled trial involving participants aged 13–18 years. The experimental intervention will involve preoperative administration of esketamine. Intraoperative monitoring will include comprehensive assessment of vital signs and measurement of serum inflammatory biomarkers, including IL-6 and CRP. Postoperative evaluation will focus on both the incidence and severity of anxiety and depressive symptoms to elucidate the potential efficacy of esketamine in mitigating these psychological sequelae in adolescent surgical patients. The study aims to establish an evidence-based clinical protocol to enhance postoperative recovery in this population. Building upon our prior findings in adult studies, we postulate the primary hypothesis that preoperative administration of sub-anesthetic dose esketamine significantly reduces postoperative anxiety symptoms as measured by HADS-A score at postoperative day 3 (POD3), with a maximal effect anticipated at POD3 and sustained improvement expected through postoperative day 14 (POD14) in adolescent patients.
Methods and Materials
Study Design and Ethics
This study employed a randomized, double-blind, controlled trial design with two parallel groups, conducted at Henan Provincial People’s Hospital. From November 2023 to December 2024, adolescents aged 13–18 years scheduled for elective surgery in the Department of Anesthesiology and Perioperative Medicine were consecutively screened, and all eligible patients were invited to participate in this study. Informed consent was obtained through a dual process: written informed consent signed by the legal guardian and written assent from the adolescent participant. This study strictly complied with the ethical principles of the Declaration of Helsinki. The study protocol was approved by the Ethics Committee of Henan Provincial People’s Hospital (Approval No. 2023–159). This study was registered at Clinical Trials.gov (identifier: NCT06073015) on October 27, 2023.
Participants
Inclusion criteria:
(1) Age 13–18 years old;
(2) Patients undergoing elective surgical procedures under general anesthesia;
(3) ASA (American Society of Anesthesiologists) physical status classification I–II.
Exclusion criteria:
- Patients anticipated to require intensive care unit (ICU) admission following surgical intervention;
- Postoperative patients necessitating continued endotracheal intubation during ward transfer;
- Patients with known hypersensitivity to the active pharmaceutical ingredients or excipients contained in Esketamine Hydrochloride Injection;
- Patients with severe disorders of consciousness, psychiatric conditions (including schizophrenia, mania, bipolar disorder, psychotic disorders, or a preoperative diagnosis of anxiety or depressive disorder), or cognitive impairment;
- Patients exhibiting congenital heart disease accompanied by significant developmental delay;
- Patients presenting with any of the following contraindications to esketamine administration were excluded: (a) individuals at elevated risk for severe hypertension or intracranial hypertension, (b) patients with elevated intraocular pressure (including glaucoma) or penetrating ocular trauma, (c) those with uncontrolled or untreated hypertension (defined as resting systolic blood pressure exceeding 180 mmHg or diastolic blood pressure exceeding 100 mmHg), and (d) patients with untreated or suboptimally managed hyperthyroidism;
- Patients with a history of ketamine abuse or dependence, chronic drug or alcohol dependence lasting more than six months, prior unsuccessful ketamine treatment trials, or documented adverse reactions to ketamine were excluded.
Randomization and Blinding
Patients fulfilling the inclusion criteria were stratified by surgical specialty (general surgery, thoracic surgery, orthopedic surgery, vascular surgery, otorhinolaryngology, and oral surgery) and subsequently randomized in a 1:1 ratio to either the esketamine group (Group S) or the control group (Group C). A computer-generated randomization sequence was maintained in sequentially numbered, opaque, sealed envelopes by personnel uninvolved in outcome assessment. Subject recruitment was conducted by investigators not participating in perioperative care. The esketamine administration was performed under blinding conditions, while outcome assessments (both primary and secondary) were carried out by researchers who were masked to treatment allocation and uninvolved in anesthetic management. Data analysis was independently conducted by two blinded assessors who had no knowledge of the randomization scheme. In instances of discordance between assessors, a third independent reviewer was consulted to achieve consensus.
Intervention and Anesthesia Management
The anesthesia protocol was implemented in accordance with established clinical guidelines. An individualized anesthetic regimen for each participant was determined by the attending anesthesiologist to optimize clinical outcomes. Patients were randomly assigned to either the esketamine group (Group S) or the control group (Group C). Group S received an intravenous bolus of 0.25 mg/kg esketamine at the time of skin incision, while Group C received an equivalent volume of normal saline. Upon arrival in the operating room, a 5 mL venous blood sample was collected for baseline measurement of serum IL-6 and CRP levels. Standard intraoperative monitoring was employed, including continuous measurement of oxygen saturation (SpO2), electrocardiography (ECG), non-invasive blood pressure, and bispectral index (BIS). Anesthesia induction was achieved using sequential administration of midazolam (0.1 mg/kg; Yichang Renfu Pharmaceutical Co., Ltd., China), sufentanil (0.8 µg/kg; Yichang Renfu Pharmaceutical Co., Ltd., China), propofol (1–2 mg/kg; Jia Bo Pharmaceutical Co., Ltd., China), and cisatracurium (0.15 mg/kg; Jiangsu Hengrui Pharmaceutical Co., Ltd., China). Endotracheal intubation or laryngeal mask insertion was performed 3–5 minutes post-induction, followed by mechanical ventilation with 50% oxygen, a tidal volume of 6–8 mL/kg, and respiratory rate adjusted for age. At the time of surgical incision, Group S received an intravenous bolus of 0.25 mg/kg esketamine (Hengrui Pharmaceutical Co., Ltd., China), while Group C received an equivalent volume of normal saline. Intraoperative end-tidal carbon dioxide (EtCO2) was maintained at 35–45 mmHg. Anesthesia was maintained with continuous intravenous infusion of propofol (4–12 mg/kg/h) and remifentanil (15–40 µg/kg/h; Jiangsu Nhwa Pharmaceutical Co., Ltd., China), supplemented by inhaled sevoflurane (0.6–1.0%; Shanghai Hengrui Hospital Co., Ltd., China). Muscle relaxation was sustained with intermittent boluses of cisatracurium. Postoperative analgesia, including patient-controlled analgesia (PCA) pump settings (eg., sufentanil 2–3 μg/kg + tropisetron 0.1 mg/kg in 100 mL saline; basal infusion 2 mL/h, bolus 2 mL/dose, lockout interval 15–30 min). For patients undergoing surgeries amenable to regional anesthesia (eg., upper limb, lower limb, or thoracic procedures), peripheral nerve blocks were performed by experienced anesthesiologists. Specifically, interscalene blocks were performed for shoulder surgeries, and femoral/sciatic nerve blocks for lower limb procedures. The blocks were standardized using 0.375% ropivacaine at a volume of 15–20 mL, depending on the anatomical site and patient weight. For thoracic surgeries, paravertebral blocks were utilized. All blocks were performed prior to induction of general anesthesia.
The analgesic pump was connected within 5 minutes postoperatively. All patients were promptly transferred to the Post-Anesthesia Care Unit (PACU) with continued respiratory support. The tracheal tube was extubated upon meeting the following criteria: restoration of spontaneous respiration, confirmation of adequate oxygenation, and intact airway protective reflexes. Additionally, residual neuromuscular blockade was reversed using neostigmine (0.02 mg/kg; 1 mL/0.5 mg, Henan Runhong Pharmaceutical Co., Ltd., Zhengzhou, China) and atropine (0.01 mg/kg; 1 mL/0.5 mg, Tianjin Jinyao Pharmaceutical Co., Ltd., Tianjin, China). Venous blood samples (5 mL) were collected 2 hours postoperatively for serum analysis of interleukin-6 (IL-6) and C-reactive protein (CRP) levels.
Outcome Assessments, Collect of Blood Samples and Testing
The primary outcome measures comprised anxiety and depression scores, evaluated utilizing the Hospital Anxiety and Depression Scale (HADS).32,33 Assessments were conducted preoperatively (the day prior to surgery) and postoperatively on days 1 (POD1), 3 (POD3), 7 (POD7), and 14 (POD14). The HADS instrument incorporates two distinct subscales: the Anxiety Subscale (HADS-A) and the Depression Subscale (HADS-D), each designed to quantify the respective psychological states.
Secondary outcomes comprised: the prevalence of anxiety and depression within 14 postoperative days; the area under the curve (AUC) for Numeric Rating Scale (NRS) scores at rest during the initial 48 postoperative hours (derived from NRS assessments at 2, 4, 24, and 48 hours post-surgery); time to anesthesia recovery; intraoperative adverse event rates (encompassing cough, laryngospasm, involuntary movement, tachycardia, oxygen desaturation, respiratory depression, bradycardia, hypertension, and hypotension); and postoperative adverse event incidence (including nausea, vomiting, dizziness, nightmares, pruritus, respiratory depression, convulsions, and hallucinations).
The biomarkers assessed in this study included serum levels of CRP and IL-6. Venous blood samples were obtained preoperatively and at 2 hours postoperatively. Following collection, samples were immediately centrifuged at 3000 rpm for 10 minutes at 4°C to isolate serum, which was subsequently aliquoted and stored at −80°C until analysis. Quantitative determination of serum CRP concentrations was performed using immunoturbidimetric assays (Shanghai Xinfan Biotechnology Co., Ltd)., while IL-6 levels were measured via chemiluminescence immunoassay (Shenzhen Acon Biotech Co., Ltd).
Statistical Analysis
Sample Size Calculation
The primary endpoint of this study was the HADS-A anxiety score on postoperative day 3 (POD3). Sample size calculation was performed using a two-independent-sample t-test. Based on our preliminary pilot data and previous relevant literature, the expected mean difference between the esketamine group and the control group was set at 1.5 points, which was defined as the minimal clinically important difference (MCID). The assumed standard deviation (SD) was 2.2 points. A two-sided type I error rate (α) of 0.05 and a test power (1−β) of 80% were applied. Considering an anticipated 15% dropout rate, PASS 15.0 software was used for calculation. The results indicated that 44 patients were required per group, with a total target sample size of 88 patients.
Inter-Group Comparison
For continuous variables exhibiting a normal distribution (eg., certain anxiety and depression scores), intergroup comparisons were performed using independent-samples t-tests. For non-normally distributed continuous variables (age, body mass index, operative duration), nonparametric analyses (Mann–Whitney U-tests) were applied. Categorical variables (sex, smoking status, surgical procedure type) were analyzed using chi-square tests, with Fisher’s exact test employed when sample sizes were limited or expected frequencies were low.
Analysis of Temporal Changes
To assess temporal variations in anxiety and depression scores, a repeated-measures analysis of variance(ANOVA) was employed. Given the longitudinal nature of the data with multiple time points, Generalized Estimating Equations(GEE) were additionally utilized as a sensitivity analysis to validate the ANOVA results and account for the correlated structure of repeated measurements.
Analysis of Influencing Factors
A logistic regression model was employed to evaluate the associations between various factors including sociodemographic characteristics, health risk behaviors, and surgical-related parameters—and the occurrence of postoperative anxiety or depression. Specifically, binary logistic regression was performed to identify independent risk factors, defining the outcome as a HADS‑A score ≥ 8 or HADS‑D score ≥ 8 at any time point within 14 days postoperatively.
Both the intention-to-treat (ITT) and per-protocol set (PPS) analyses were conducted for anxiety and depression outcomes (HADS scores across preoperative, POD1, POD3, POD7, and POD14 time points), whereas only PP analysis was applied to other outcomes.
Statistical significance was defined as a two-tailed P-value <0.05. All analyses were performed using IBM SPSS Statistics (version 26) and GraphPad Prism (version 9.5) software packages.
Results
Demographic and Clinical Characteristics of the Patients
A total of 102 patients were screened between November 4, 2023, and December 7, 2024. Among these, three patients were excluded based on predefined exclusion criteria, and an additional three declined participation. Consequently, 92 eligible participants were enrolled and randomized equally into two groups, with 46 patients allocated to each group. Postoperatively, 4 patients were admitted to the ICU and excluded from follow-up (2 in each group). 4 patients withdrew consent (esketamine group: 1 on POD1, 1 on POD3; control group: 2 on POD1). 4 patients were lost to follow-up (esketamine group: 1 on POD14; control group: 1 on POD7, 2 on POD14). The final distribution comprised 39 patients in the control group and 41 in the esketamine group (Figure 1). Baseline demographic and clinical characteristics, including age, body mass index (BMI), gender, residential area, sibling status, educational attainment, parental education level, social network size, academic workload, smoking status, sleep duration, and physical activity levels (Table 1), demonstrated no statistically significant differences between groups, with the exception of regional economic status.
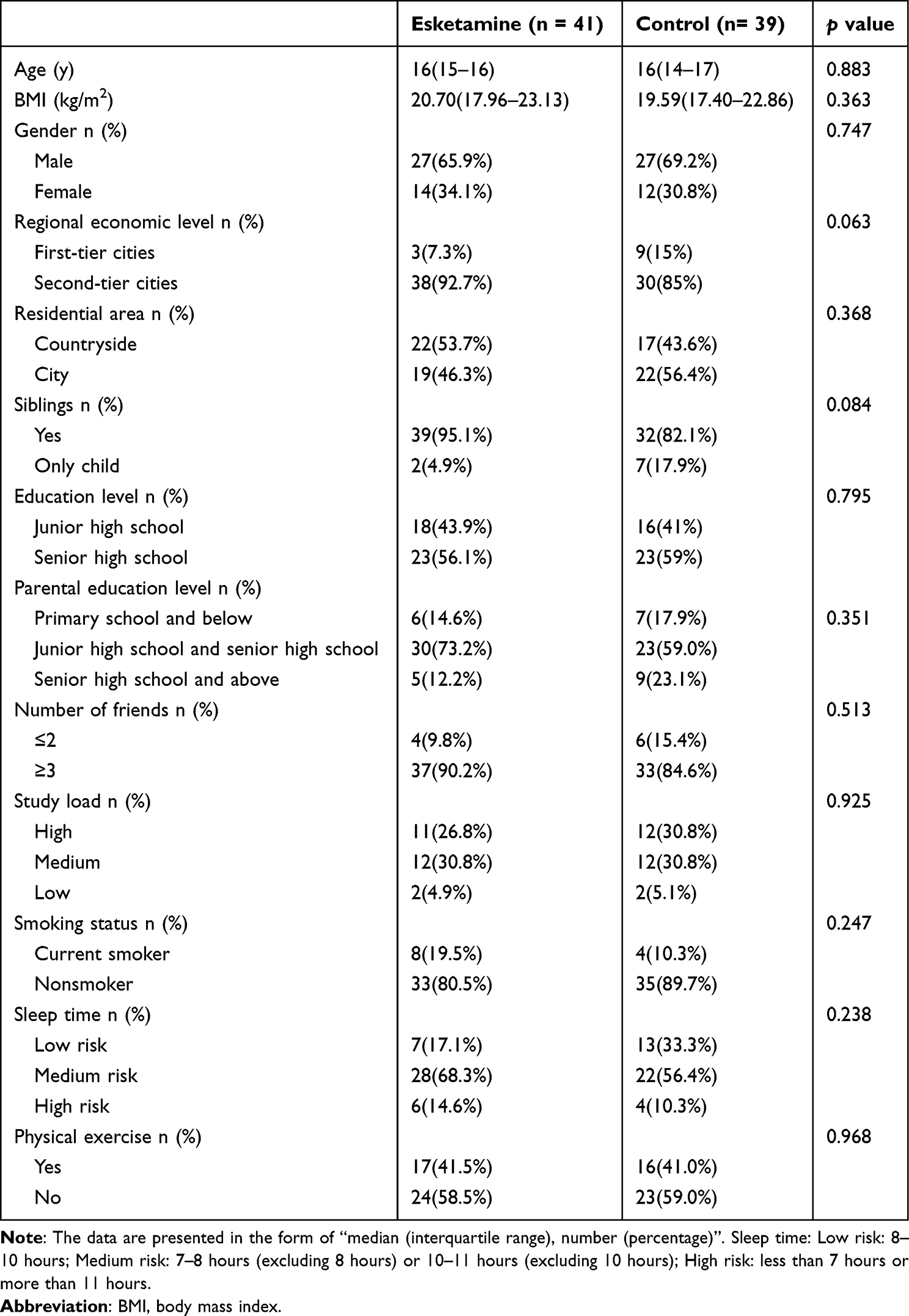 |
Table 1 Patient Characteristics Between the Esketamine Group and Control Group |
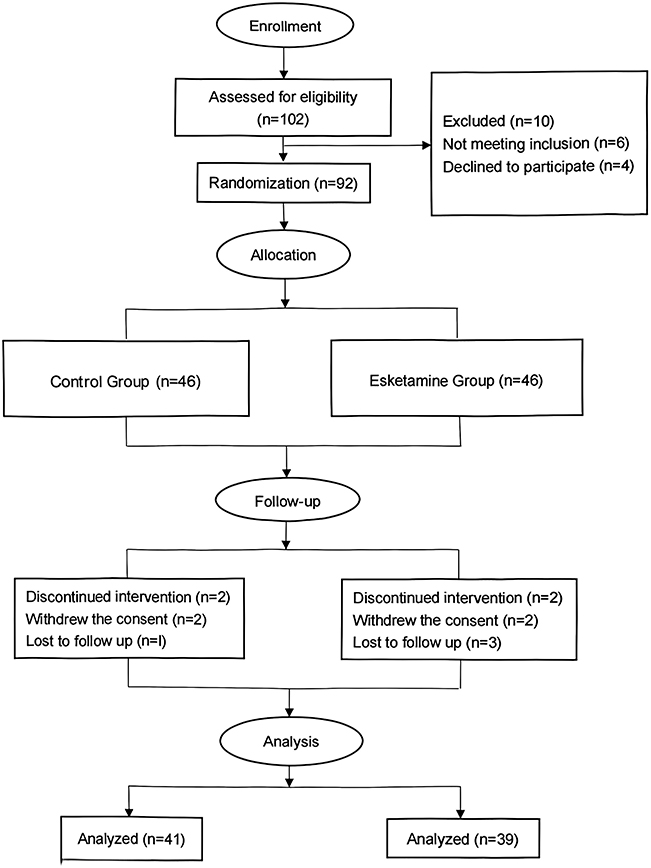 |
Figure 1 Study flow chart. |
Clinical Characteristics
A comprehensive comparison was conducted between the two patient cohorts regarding preoperative, intraoperative, and postoperative parameters, including surgical history, preoperative hematological indices (white blood cell and lymphocyte counts), operative characteristics (surgical type, duration, and blood loss), anesthetic management (extubation time, sufentanil dosage, patient-controlled analgesia utilization, and nerve block status). Statistical analysis revealed no significant intergroup differences in any of these variables (Table 2).
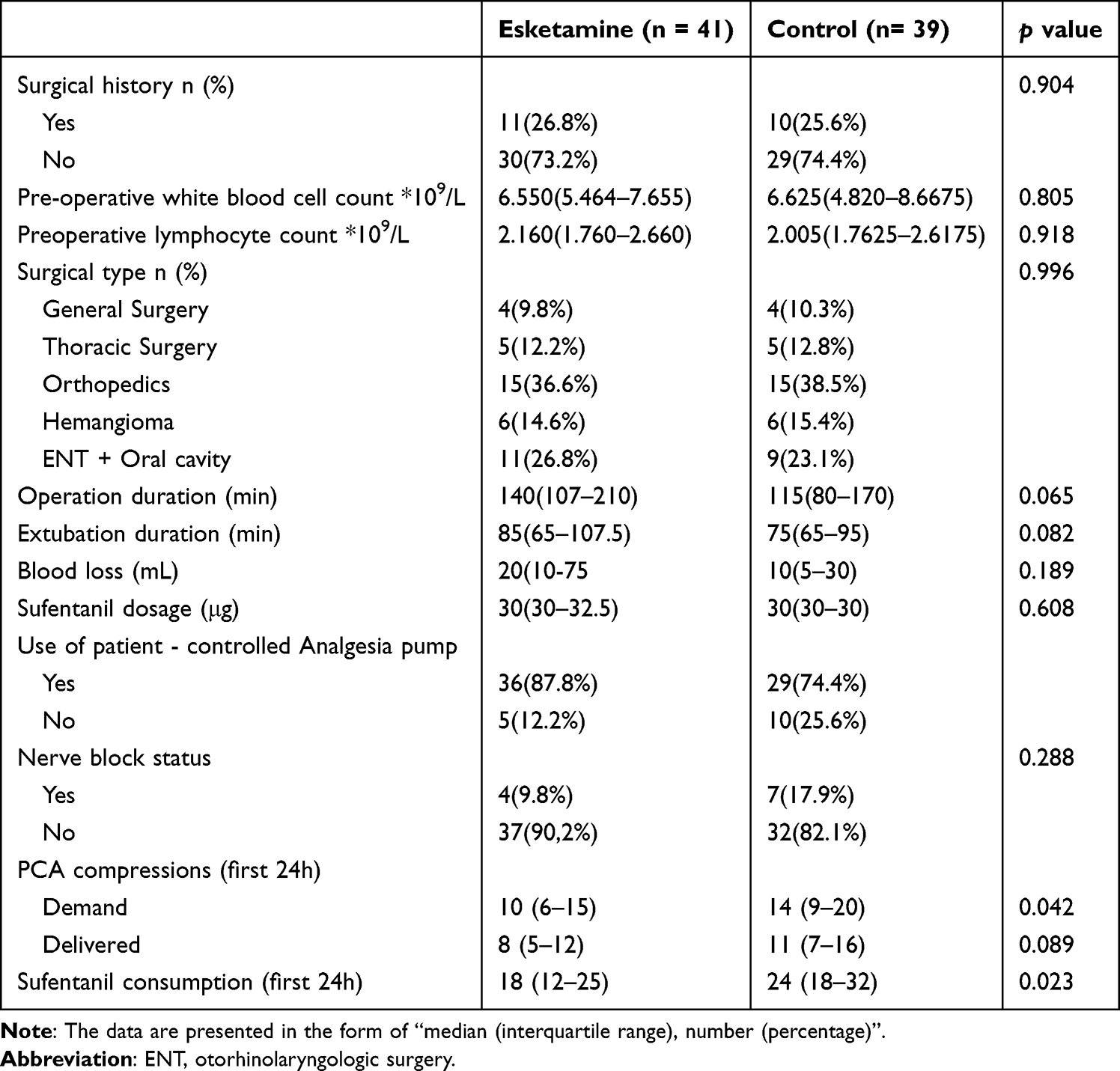 |
Table 2 Clinical Characteristics and Outcomes of the Patients Between the Two Groups |
Emotional Performance
For PPS analysis (N=80), the HADS-A and HADS-D scores of the two groups are presented in Figure 2 and Supplementary Table 1. Statistically significant differences in HADS-A scores were observed between the esketamine group and the control group at multiple postoperative time points: POD1 (median [IQR]: 4.5 [3.0–6.0] vs. 6.0 [4.0–8.0], P=0.023), POD3 (3.75 [2.5–5.0] vs. 5.5 [4.0–7.0], P=0.002), POD7 (3.5 [2.0–5.0] vs. 6.0 [4.0–8.0], P=0.008), and POD14 (4.25 [2.0–6.5] vs. 5.5 [4.0–7.0], P=0.013). A significant between-group difference in HADS-D scores was detected only at POD14 (mean ± SD: 4.34 ± 2.17 vs. 5.38 ± 2.41, P=0.043). The results of the ITT analysis (see Supplementary Table 2) showed a consistent trend with those of the PPS, and the conclusions were stableThese findings demonstrate that preoperative esketamine administration significantly reduces postoperative anxiety symptoms.
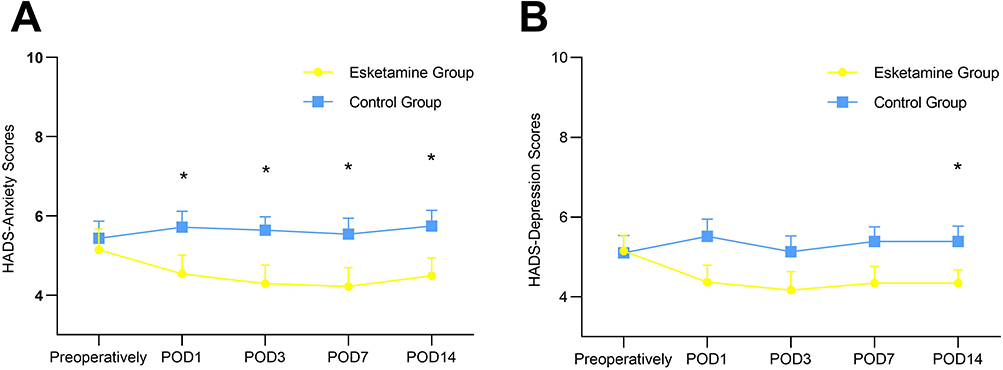 |
Figure 2 HAD-A, HAD-D between the two groups. (A) HADS-Anxiety (HADS-A) scores at each time point in the two groups. (B) HADS-Depression (HADS-D) scores at each time point in the two groups. Abbreviations: POD1, postoperative day 1; POD3, postoperative day 3; POD7, postoperative day 7; POD14, postoperative day 14; HADS-A, Hospital Anxiety and Depression Scale Anxiety subscale; HADS-D, Hospital Anxiety and Depression Scale Depression subscale. Note: Data are presented as mean ± SD or median with interquartile range (IQR). *P<0.05. |
A comparative analysis of postoperative anxiety and depressive symptoms between the two groups was conducted (Table 3). Anxiety and depressive symptoms were operationally defined as HADS-A and Depression HADS-D subscale scores ≥8, respectively. The esketamine group demonstrated a significantly lower incidence of anxiety compared to the control group (p<0.05). However, no statistically significant intergroup difference was observed in the incidence of depressive symptoms (p>0.05).
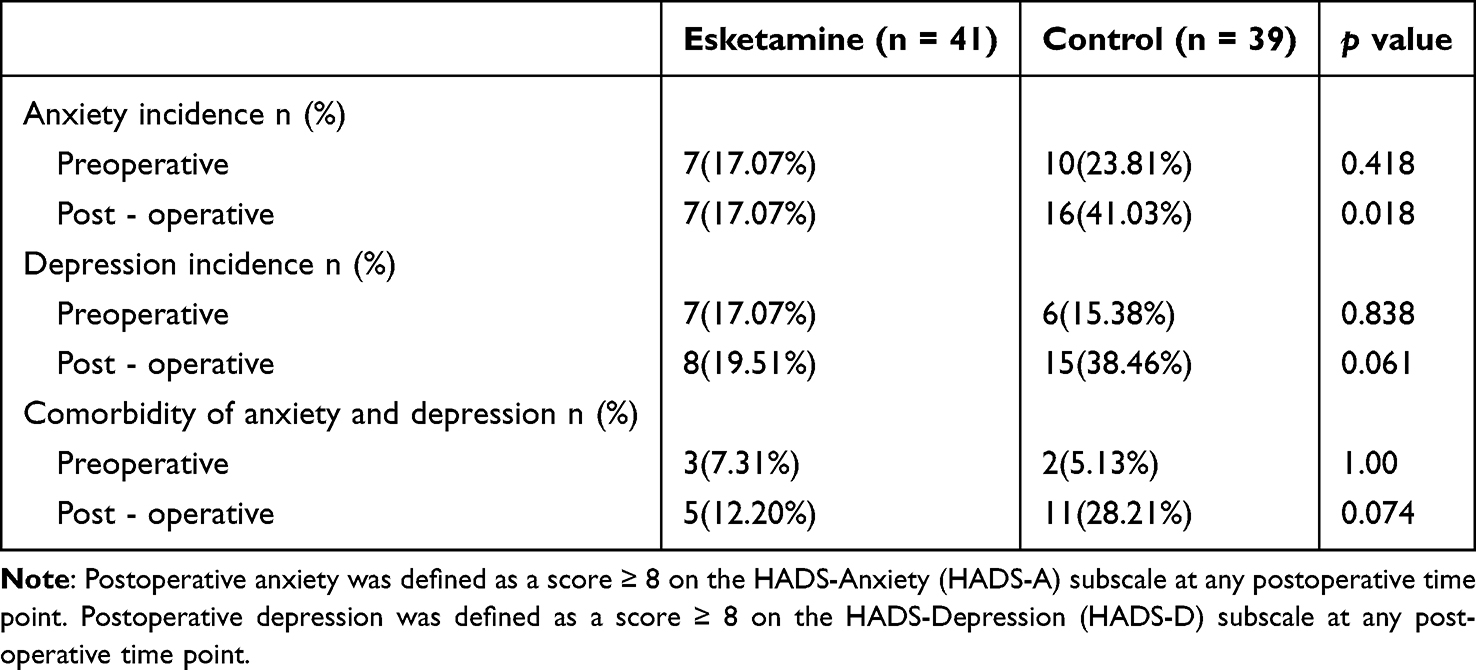 |
Table 3 Incidence of Anxiety and Depression Between the Two Groups |
To examine temporal variations in anxiety and depression scores, repeated-measures analysis of variance was performed independently (Table 4). Regarding anxiety scores, both groups exhibited minimal fluctuations across time points. However, multivariate analysis demonstrated a statistically significant time-by-group interaction effect (P = 0.011), indicating differential patterns of anxiety score changes between groups over time. Notably, the main effect of time alone did not reach statistical significance (P = 0.081). Similarly, depression scores showed limited temporal variation in both groups. Multivariate testing revealed a significant time-by-group interaction (P = 0.021), suggesting distinct temporal trajectories of depression scores between groups. The isolated effect of time on depression scores was non-significant (P = 0.274). Consistent with these findings, GEE analysis confirmed a significant interaction effect (HADS-A: Wald χ2 = 14.497, P = 0.006; HADS-D: Wald χ2 = 12.443, P = 0.014), reinforcing the robustness of the observed temporal changes.
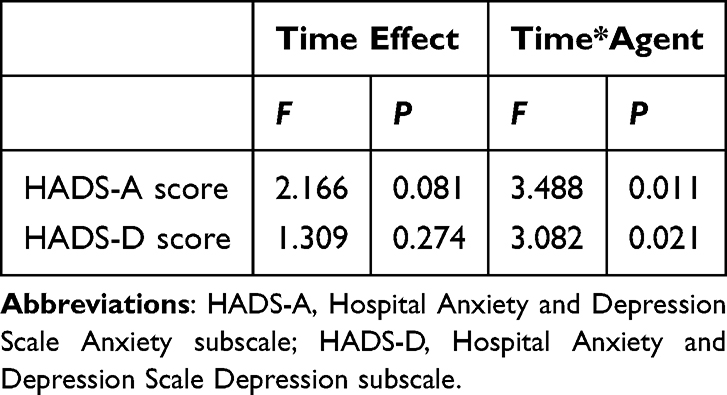 |
Table 4 The Impact of Time and Esketamine Intervention on Anxiety and Depression Scores |
Blood Biomarkers
The biomarker assessment results are presented in Table 5. No statistically significant differences were detected in serum IL-6 levels (preoperative: IQR 1.56–4.74 vs. 2.08–5.66, P=0.214; 2-hour postoperative: IQR 2.02–12.06 vs. 3.45–16.50, P=0.106) or CRP concentrations (preoperative: IQR 3.20–5.88 vs. 1.91–7.80, P=0.214; 2-hour postoperative: IQR 3.11–5.25 vs. 3.90–11.30, P=0.057) between the study groups at either time point.
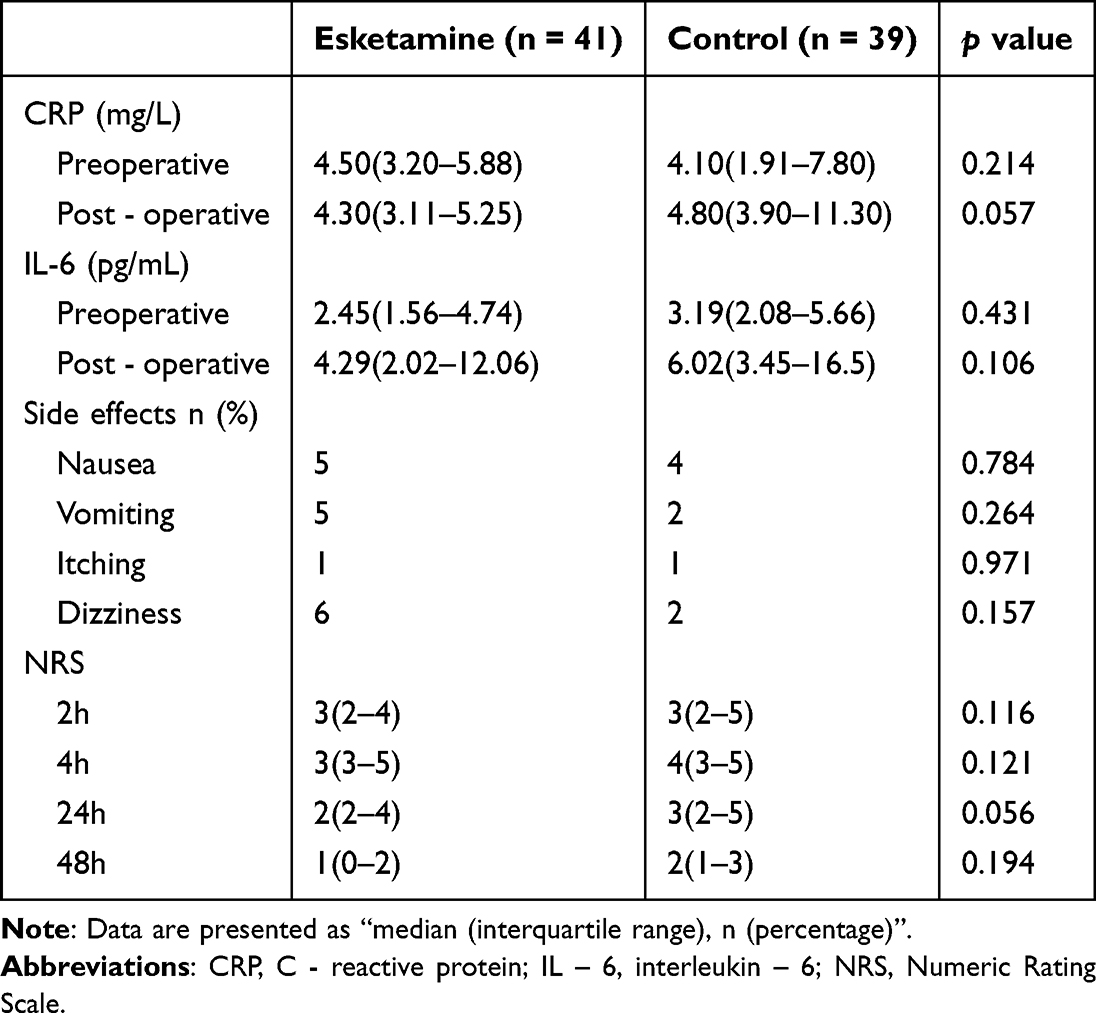 |
Table 5 The Outcomes of the Patients Between the Esketamine Group and Control Group |
Side Effects
The analysis revealed no statistically significant differences between the two groups in the incidence of postoperative nausea (12.2% vs. 10.3%, P=0.784), vomiting (12.2% vs. 5.1%, P=0.784), pruritus (2.4% vs. 2.5%, P=0.971), or dizziness (14.6% vs. 5.1%, P=0.157) (Table 5). Furthermore, no cases of nightmares, respiratory depression, seizures, or hallucinations were reported in either group. Hemodynamic monitoring demonstrated no significant elevations in blood pressure or heart rate among patients receiving esketamine.
Postoperative Pain Score
The postoperative NRS scores are presented in Tables 3–5. Comparative analysis revealed no statistically significant differences in pain scores between the esketamine (S group) and control (C group) cohorts at the 2-hour (median [IQR]: S group 2 [2–4] vs. C group 2 [2–5], P=0.116), 4-hour (median [IQR]: S group 3 [3–5] vs. C group 3 [3–5], P=0.121), 24-hour (median [IQR]: S group 2 [2–4] vs. C group 2 [2–5], P=0.056), or 48-hour (median [IQR]: S group 0 [0–2] vs. C group 1 [1–3], P=0.023) postoperative intervals. Furthermore, the AUC analysis of pain scores demonstrated no significant intergroup disparity (P=0.194) (Figure 3).
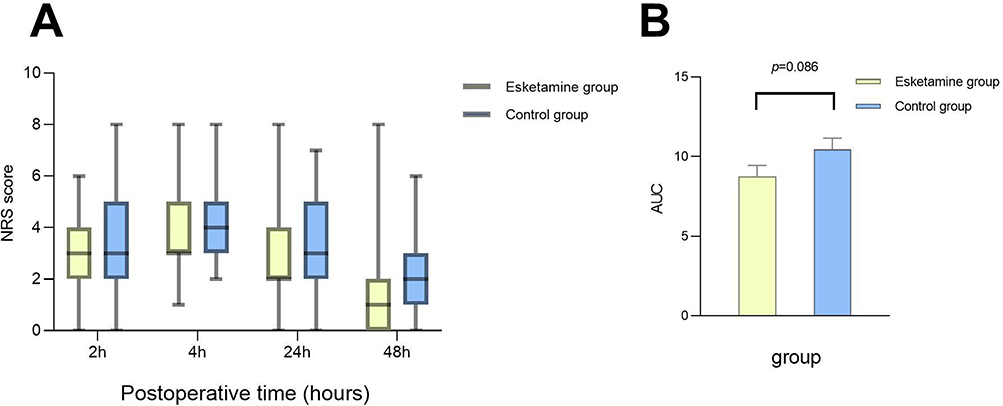 |
Figure 3 Postoperative NRS Pain Scores of the Two Groups of Patients. (A) Box plot of NRS pain scores at 2 h, 4 h, 24 h, and 48 h postoperatively. (B) Bar graph of AUC values for NRS pain scores at 48 h postoperatively between the two groups. |
Influencing Factor Logistic Analysis
A binary logistic regression analysis was performed (Tables 6 and 7). Initially, univariate logistic regression was conducted to assess sociodemographic characteristics, health risk behaviors, and surgical-related factors, including age, gender, sibling status, regional economic level, residential area, educational attainment, parental education level, social network size, academic workload, smoking status, physical activity level, surgical type, anesthesia duration, postoperative analgesia methods, preoperative anxiety (HADS-A ≥ 8), preoperative depression (HADS-D ≥ 8) and nerve block conditions. Variables demonstrating statistical significance in the univariate analysis (parental education level, surgical type, preoperative anxiety, preoperative depression and esketamine administration) were subsequently incorporated into the multivariate logistic regression model. The multivariate analysis revealed that esketamine use, preoperative anxiety, and preoperative depression were independently and significantly associated with the incidence of postoperative anxiety and depression. In contrast, parental education level and surgical type only showed marginal trends and did not reach statistical significance.
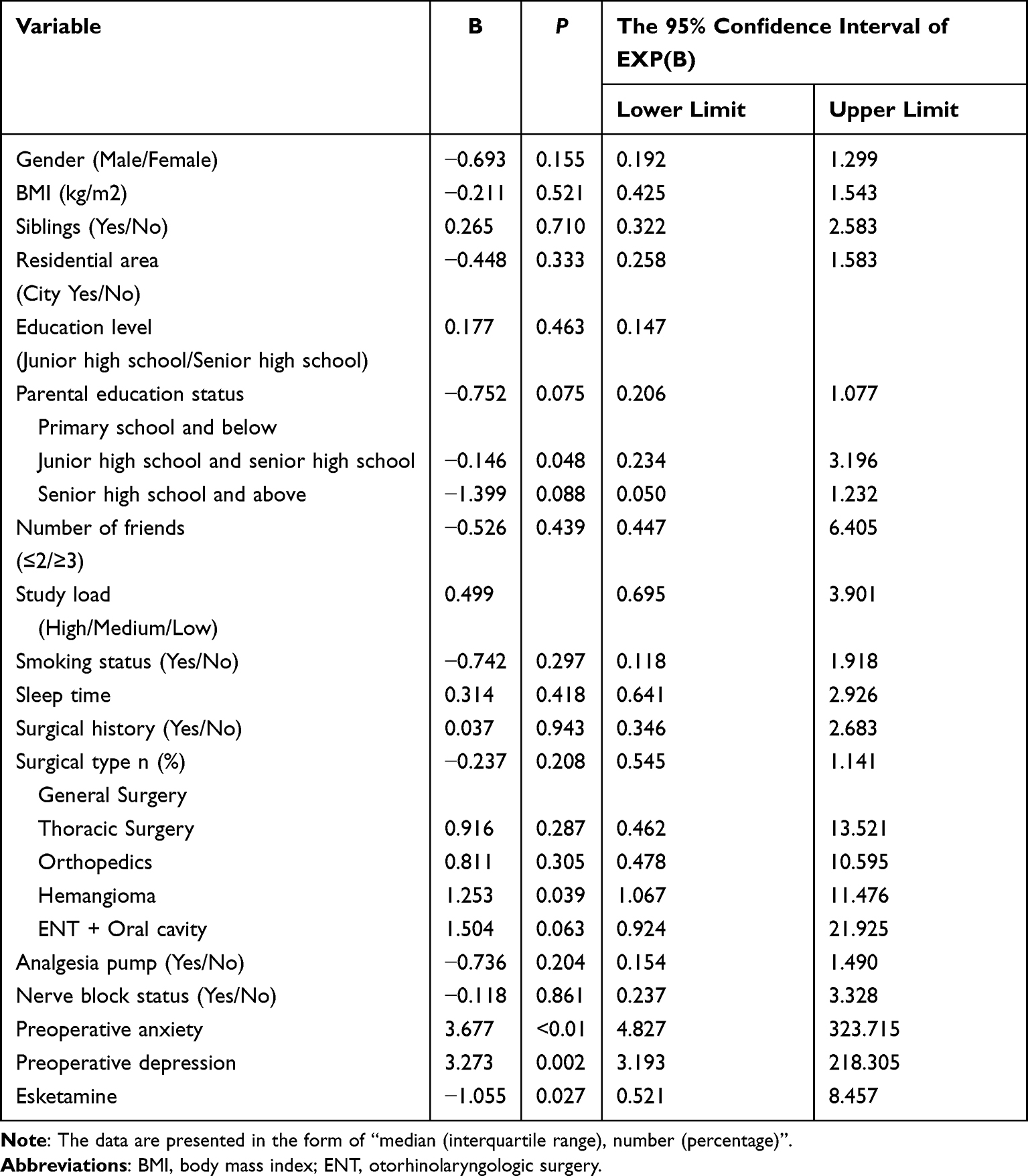 |
Table 6 Univariate Analysis of Logistic Regression |
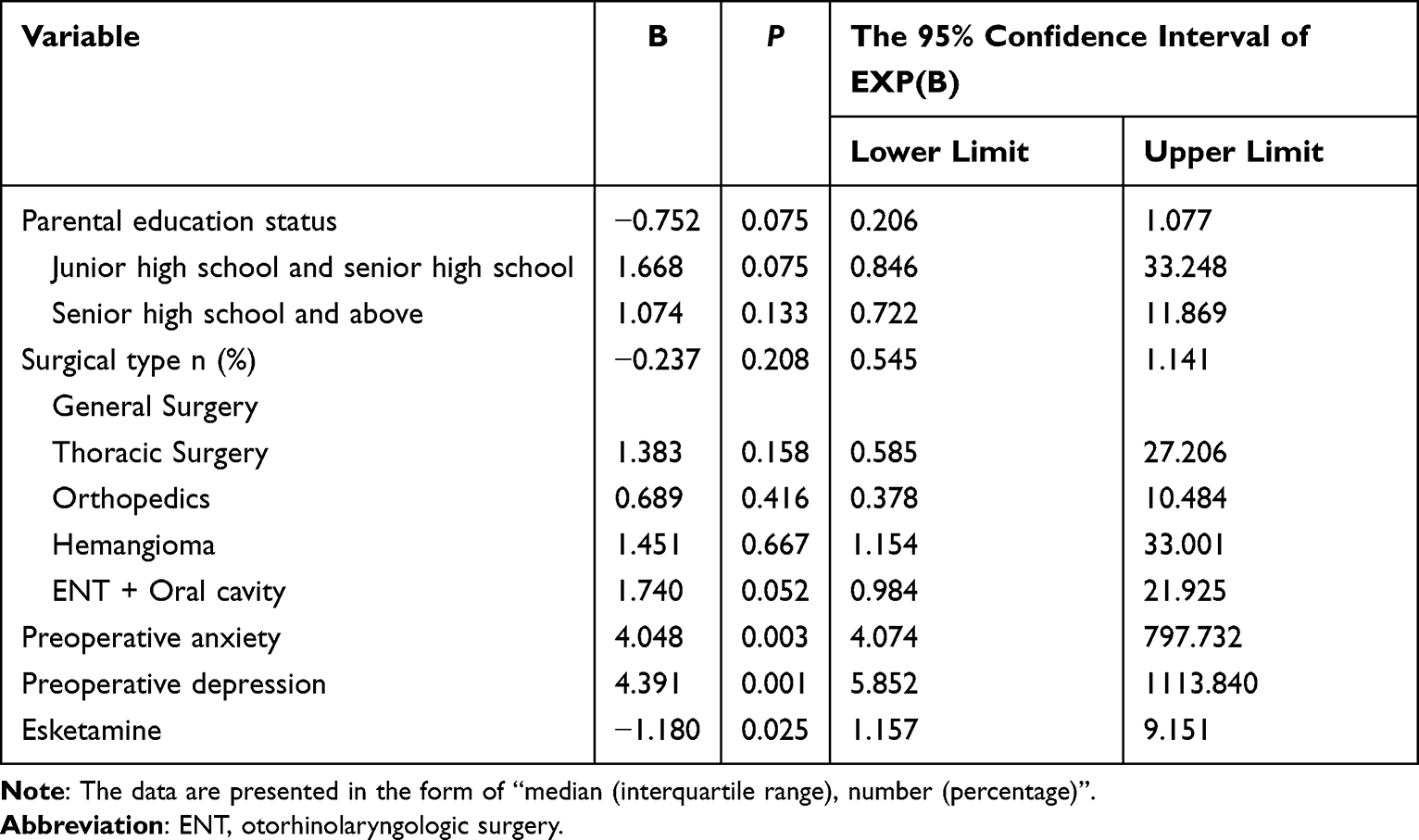 |
Table 7 Multivariate Analysis of Logistic Regression |
Discussion
This study enrolled adolescent patients aged 13–18 years who met the predefined inclusion criteria. The results demonstrated significant between-group differences in emotional manifestations, with the esketamine group exhibiting lower HADS-A scores at multiple postoperative time points and reduced HADS-D scores on postoperative day 14 compared to the control group. Importantly, the observed reduction in HADS-A scores in the esketamine group crossed the predefined MCID threshold at multiple early postoperative time points (POD1, POD3, and POD7), underscoring the potential of subanesthetic esketamine to produce tangible clinical benefits in adolescent patients.34 Furthermore, the incidence of postoperative anxiety was significantly lower in the esketamine group, whereas no statistically significant difference was observed in depression incidence between the two groups. Longitudinal analysis of anxiety and depression scores revealed a significant interaction effect between time points and group allocation, though the main effect of time alone was not statistically significant. Regarding inflammatory biomarkers, no significant differences were detected in serum IL-6 or CRP levels between the two groups at either the preoperative (1 hour before surgery) or postoperative (2 hours after surgery) time points. Adverse event profiles were comparable between groups, with no significant differences in the incidence of postoperative nausea, vomiting, pruritus, or dizziness. No serious adverse events occurred in the esketamine group, and hemodynamic parameters (blood pressure and heart rate) remained stable throughout the surgical procedure. Postoperative pain scores at all assessed time points, as well as the AUC for pain scores, did not differ significantly between groups. The logistic regression analysis yielded two critical findings. First, baseline psychological status exerted a dominant influence on postoperative outcomes. Both preoperative anxiety and depression were identified as extremely strong independent risk factors. Second, even after adjusting for these powerful baseline confounders, esketamine administration retained its statistical significance as a protective factor. This demonstrates that the beneficial effect of esketamine is not merely a byproduct of differences in baseline symptoms, but rather an independent therapeutic contribution.
The present study demonstrated that esketamine significantly reduced the severity of postoperative anxiety symptoms and produced a mild improvement in depressive symptoms in adolescent patients. These findings are consistent with previous studies showing that esketamine may alleviate perioperative anxiety and depressive symptoms in adolescents,35 This phenomenon can be explained by several key pharmacological properties of esketamine. First, esketamine demonstrates rapid-onset anxiolytic and antidepressant effects, typically manifesting within minutes following administration. Furthermore, these therapeutic effects exhibit remarkable persistence, maintaining efficacy for periods ranging from several hours to multiple days after a single dose.36 Esketamine, functioning as an NMDA receptor antagonist, exerts rapid therapeutic effects through the competitive inhibition of glutamate-mediated neurotransmission. This pharmacological mechanism results in the attenuation of anxiety and depressive symptomatology by modulating excitatory synaptic transmission in key neural circuits.37 Esketamine demonstrates the capacity to rapidly modulate neurotransmitter levels while concurrently facilitating synaptic plasticity and strengthening neural connectivity, thereby inducing more sustained therapeutic outcomes.38 For patients exhibiting inadequate response to conventional antidepressant therapies, esketamine demonstrates therapeutic efficacy through distinct pharmacological mechanisms. These include NMDA receptor antagonism and the facilitation of brain-derived neurotrophic factor BDNF release, which collectively contribute to its effectiveness in treatment-resistant depression cases.39 At low doses, esketamine exhibits pronounced anxiolytic and antidepressant properties while circumventing adverse effects, including hallucinations, which are typically associated with higher dosages.35 In addition to its well-documented anxiolytic and antidepressant effects, esketamine demonstrates significant analgesic properties. Through its antagonistic action on NMDA receptors, esketamine effectively modulates postoperative pain by inhibiting central pain signal transduction pathways. This pharmacological mechanism not only provides direct analgesic effects but may also contribute to the secondary amelioration of anxiety and depressive symptoms in postoperative patients,40 Its analgesic effect can reduce the dosage of opioid drugs after surgery, thus reducing the risks of addiction and respiratory depression.41 Esketamine demonstrates therapeutic efficacy in ameliorating anxiety, depressive symptoms, and pain perception, which collectively contribute to enhanced postoperative recovery outcomes in adolescent patients.42
Previous research on esketamine has predominantly examined its effects in adult populations. The current study addresses a critical knowledge gap by investigating its therapeutic potential in adolescent cohorts. Our findings demonstrate that esketamine exhibits comparable efficacy in alleviating symptoms of anxiety and depression among adolescents, consistent with observations in adult populations.22,43 However, notable variations may exist in both the magnitude of effects and associated influencing factors. In adult clinical studies, heterogeneity in patients’ comorbidities and physiological conditions introduces limitations when extrapolating findings on dose-response relationships and drug-drug interactions to adolescent populations. As demonstrated by Dwyer et al, substantial differences in pharmacokinetic profiles and neurobiological responses between adolescent and adult patients necessitate careful consideration when determining appropriate esketamine dosing regimens and predicting therapeutic outcomes.44–46 The administration of esketamine in postoperative adult patients demonstrates a significant reduction in anxiety and depression scores, with sustained therapeutic effects persisting for at least 72 hours following surgical intervention,47 however, in the present study, adolescent patients exhibited a more rapid improvement in postoperative anxiety scores, albeit with a shorter duration of effect (approximately 24–48 hours). This transient efficacy may be attributed to the accelerated metabolic rate and enhanced neuroplasticity characteristic of the developing adolescent nervous system.48 The current investigation demonstrated significant temporal variations and differential magnitudes of improvement in postoperative anxiety scores between adolescent and adult patient populations, accompanied by notable disparities in corresponding biomarker profiles,49 This implies that the mechanism of action and therapeutic efficacy of esketamine may exhibit distinct features in adolescent populations, warranting comprehensive investigation through rigorous clinical studies.
The findings of this study demonstrated no statistically significant differences in serum CRP and IL-6 concentrations between the Esketamine Group and the Control Group at both preoperative and 2-hour postoperative time points. This observation appears inconsistent with previously reported anti-inflammatory properties of esketamine in adult populations, potentially attributable to several factors: Adolescents represent a distinct developmental stage characterized by unique immune regulatory mechanisms. Existing evidence suggests that the postoperative inflammatory response in adolescent populations typically exhibits rapid activation followed by spontaneous resolution, rather than sustained elevation observed in adult cohorts.50 The present study involved relatively minor surgical trauma, which may have been insufficient to elicit a robust inflammatory cascade, potentially explaining the comparable baseline levels of inflammatory markers observed between the two groups. Furthermore, the assessment of inflammatory markers was limited to preoperative and 2-hour postoperative time points, which may not have captured the peak inflammatory response. Future investigations should consider extending the sampling window (eg, to 24 hours postoperatively) to enable a more comprehensive evaluation of esketamine’s effects on inflammatory dynamics.
Postoperative numerical rating scale (NRS) scores at multiple time points demonstrated no statistically significant differences in pain levels between the two groups. The majority of patients in both cohorts utilized patient-controlled analgesia (PCA) pumps postoperatively (Esketamine Group: 74.4% vs. Control Group: 87.8%), potentially obscuring esketamine’s putative analgesic effects. Furthermore, supplemental administration of non-steroidal anti-inflammatory drugs (NSAIDs) and opioid analgesics to some patients in both groups upon ward return may have further attenuated the potential differential efficacy of esketamine. The observed findings suggest that sub-anesthetic doses of esketamine may primarily modulate central sensitization mechanisms rather than exert direct analgesic effects. Dose escalation or extended infusion duration could potentially yield more pronounced reductions in pain scores.
No significant difference in the incidence of adverse reactions was observed between the Esketamine Group and the Control Group, with no occurrence of serious complications, indicating that sub-anesthetic doses of esketamine exhibit a favorable safety profile in adolescent populations. In contrast, studies involving adult participants have reported that higher doses of esketamine (>0.5 mg/kg) may elicit dissociative symptoms or cardiovascular responses,51 This study employed a single intravenous bolus administration of 0.25 mg/kg esketamine, which effectively minimized cumulative toxicity while mitigating potential risks through rapid metabolic clearance. The observed incidence of nausea and vomiting was comparatively low (approximately 12%), likely attributable to both the enhanced metabolic rate characteristic of adolescent populations and the synergistic effects of intraoperative 5-HT3 receptor antagonist co-administration, coupled with optimized postoperative antiemetic protocols.
Logistic regression analysis demonstrated that esketamine significantly influenced the occurrence of anxiety and depression (p < 0.05), consistent with both the primary hypothesis of this study and clinical observations, thereby reinforcing its therapeutic efficacy in mitigating postoperative anxiety and depression in adolescent patients. While parental education level and surgical type exhibited marginal associations, these factors did not achieve statistical significance (p > 0.05), potentially attributable to the restricted sample size, which may have limited the detection of subtle effects. Prior research has established that familial environment and educational background may exert substantial influences on adolescent psychological development,52,53 However, this finding was not fully substantiated in the present study. The lack of significant association with surgical type may be attributed to the relatively homogeneous distribution of cases across different surgical procedures or potential limitations in the study design that precluded adequate detection of differential psychological effects among surgical categories. Future investigations should incorporate larger sample sizes and implement more granular classifications of surgical variables to enable a more precise evaluation of their relationship with esketamine’s therapeutic outcomes.
This study has several limitations that warrant consideration. First, the relatively small sample size, despite power calculations and preliminary experiments, may compromise the statistical power and reliability of the findings, particularly in detecting subtle yet clinically relevant associations when analyzing influencing factors. Second, the single-center design with a homogeneous patient population may introduce regional and institutional biases, thereby limiting the external validity and generalizability of the results. Third, the study primarily assessed short-term perioperative anxiety and depression, lacking longitudinal follow-up to evaluate patients’ psychological states over time, which precludes conclusions regarding the long-term effects of esketamine. Fourth, the lack of adjustment for multiple comparisons across the various endpoints and time points increases the risk of Type I error (false positives). While our primary hypothesis regarding POD3 HADS-A scores was pre-specified, the analyses of secondary outcomes, particularly the biomarker data and pain scores, were largely exploratory. Future studies with larger sample sizes and prespecified correction methods are needed to validate these findings. Fifth, although stratified randomization by surgical specialty was performed, the inclusion of a mixed surgical population (eg, general, thoracic, orthopedic, and ENT/oral surgeries) introduces clinical heterogeneity that should be carefully considered when interpreting the results. Sixth, postoperative analgesia was not standardized across participants; instead, patient-controlled analgesia (PCA) and nerve blocks were tailored by anesthesiologists based on individual needs, which may have introduced variability in postoperative pain management and subsequent psychological responses. Seventh, structured psychiatric diagnostic interviews were not employed, although patients with pre-existing diagnosed psychiatric disorders were excluded, the potential influence of subclinical or undiagnosed conditions cannot be entirely ruled out. Eighth, the assessment of inflammatory markers was limited to preoperative and 2-hour postoperative time points, which may not have captured the peak inflammatory response. Specifically, IL-6, as an early inflammatory marker, may still be in the initial stages of elevation at 2 hours, whereas CRP, a marker of mid-to-late stage inflammation, typically requires 24–48 hours to reach its peak concentration and was unlikely to show significant elevation at this early time point. Consequently, the lack of significant differences in biomarkers between the two groups should be interpreted with caution, as the sampling window may have been too narrow to detect dynamic changes in the inflammatory cascade. Furthermore, although multiple covariates were analyzed, residual confounding factors may persist, potentially influencing the interpretation of the results.
Future research should focus on several key directions to advance understanding in this field. First, multicenter studies with expanded sample sizes should be implemented to incorporate adolescent patients from diverse geographical regions and clinical settings, thereby enhancing the external validity and robustness of the findings. Second, longitudinal investigations with extended follow-up periods are warranted to assess the sustained psychological impact of esketamine administration in adolescent populations, particularly regarding the temporal patterns of anxiety and depressive symptom development postoperatively. Third, methodological refinements should be pursued to systematically evaluate potential confounding variables, including psychosocial determinants and familial influences, while employing sophisticated statistical modeling techniques. Fourth, dose-response studies are needed to establish the optimal therapeutic window for esketamine in adolescents, carefully evaluating the risk-benefit ratio across different dosage regimens. Finally, combination therapy trials should be conducted to examine potential synergistic effects between esketamine and other pharmacological or non-pharmacological interventions for postoperative psychological distress in this vulnerable population.
Conclusion
The present study demonstrates that preoperative administration of 0.25 mg/kg esketamine significantly reduces the incidence of postoperative anxiety in adolescent patients while exhibiting modest yet clinically relevant improvements in depressive symptoms by postoperative day 14. Notably, these symptom improvements were observed without an increase in adverse events. However, given that postoperative anxiety and depression are mostly transient, the long-term clinical significance of the present findings still needs to be further verified. Conclusions should be interpreted cautiously and only serve as preliminary evidence supporting short-term mood improvement, and should not be regarded as a basis for preventing clinical anxiety or depressive disorders.
Data Sharing Statement
The individual deidentified participant data, the study protocol, and the statistical analysis plan can be accessed from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Choi KW, Kim YK, Jeon HJ. Comorbid anxiety and depression: clinical and conceptual consideration and transdiagnostic treatment. Adv Exp Med Biol. 2020;1191:219–18. doi:10.1007/978-981-32-9705-0_14
2. Tiller JW. Depression and anxiety. Med J Aust. 2013;199(S6):S28–31. doi:10.5694/mja12.10628
3. Chen J. Clinical efficacy of laparoscopic cholecystectomy in the treatment of acute calculous cholecystitis and its impact on psychological status. Psychological Monthly. 2020;24:216–217.
4. Clark DA, Beck AT. Cognitive theory and therapy of anxiety and depression: convergence with neurobiological findings. Trends Cognit Sci. 2010;14(9):418–424. doi:10.1016/j.tics.2010.06.007
5. Yamazaki M, Yasuda H, Koda K. Single-incision laparoscopic cholecystectomy: a systematic review of methodology and outcomes. Surg Today. 2015;45(5):537–548. doi:10.1007/s00595-014-0908-2
6. Calabro FJ, Murty VP, Jalbrzikowski M, Tervo-Clemmens B, Luna B. Development of hippocampal-prefrontal cortex interactions through adolescence. Cereb Cortex. 2020;30(3):1548–1558. doi:10.1093/cercor/bhz186
7. Li DC, Hinton EA, Guo J. Social experience in adolescence shapes prefrontal cortex structure and function in adulthood. Mol Psychiatry. 2024;29(9):2787–2798. doi:10.1038/s41380-024-02540-6
8. Silvers JA, Insel C, Powers A, et al. vlPFC-vmPFC-amygdala interactions underlie age-related differences in cognitive regulation of emotion. Cereb Cortex. 2017;27(7):3502–3514. doi:10.1093/cercor/bhw073
9. Windle M, Gray JC, Lei KM, et al. Age sensitive associations of adolescent substance use with amygdalar, ventral striatum, and frontal volumes in young adulthood. Drug Alcohol Depend. 2018;186:94–101. doi:10.1016/j.drugalcdep.2018.02.007
10. Shelkar GP, Liu J, Dravid SM. Astrocytic NMDA receptors in the basolateral amygdala contribute to facilitation of fear extinction. Int J Neuropsychopharmacol. 2021;24(11):907–919. doi:10.1093/ijnp/pyab055
11. Shelkar GP, Pavuluri R, Gandhi PJ, et al. Differential effect of NMDA receptor GluN2C and GluN2D subunit ablation on behavior and channel blocker-induced schizophrenia phenotypes. Sci Rep. 2019;9(1):7572. doi:10.1038/s41598-019-43957-2
12. Wang M, B TF, Wu XY. Research progress on comorbidity of anxiety and depression in children and adolescents. Chin J Prevent Med. 2022;56:1011–6.
13. Chan P, Skaggs DL, Sanders AE. Pain is the greatest preoperative concern for patients and parents before posterior spinal fusion for adolescent idiopathic scoliosis. Spine. 2017;42(21):E1245–E1250. doi:10.1097/BRS.0000000000002147
14. Sieberg CB, Manganella J, Manalo G, Simons LE, Hresko MT. Predicting postsurgical satisfaction in adolescents with idiopathic scoliosis: the role of presurgical functioning and expectations. J Pediatr Orthop. 2017;37(8):e548–e551. doi:10.1097/BPO.0000000000000778
15. Duramaz A, Yılmaz S, Ziroğlu N, Bursal Duramaz B, Kara T. The effect of deformity correction on psychiatric condition of the adolescent with adolescent idiopathic scoliosis. Eur Spine J. 2018;27(9):2233–2240. doi:10.1007/s00586-018-5639-4
16. Yang Y, Cui Y, Sang K, et al. Ketamine blocks bursting in the lateral habenula to rapidly relieve depression. Nature. 2018;554(7692):317–322. doi:10.1038/nature25509
17. Aizawa H, Okamoto H. Molecular characterization of the subnuclei in rat habenula. J Comp Neurol. 2012;520:4501–66.
18. Tye KM, Mirzabekov JJ, Warden MR, et al. Dopamine neurons modulate neural encoding and expression of depression-related behaviour. Nature. 2013;493(7433):537–541. doi:10.1038/nature11740
19. Hao A, Huang J, Xu X. Anxiety and depression in glioma patients: prevalence, risk factors, and their correlation with survival. Irish J Med Sci. 2021;190(3):1155–1164. doi:10.1007/s11845-020-02374-5
20. Hashimoto K. Molecular mechanisms of the rapid-acting and long-lasting antidepressant actions of (R)-ketamine. Biochem Pharmacol. 2020;177:113935.. doi:10.1016/j.bcp.2020.113935
21. Wei Y, Chang L, Hashimoto K. Molecular mechanisms underlying the antidepressant actions of arketamine: beyond the NMDA receptor. Mol Psychiatry. 2022;27(1):559–573. doi:10.1038/s41380-021-01121-1
22. Zarate CA Jr, Singh JB, Carlson PJ. A randomized trial of an N-methyl-D-aspartate antagonist in treatment-resistant major depression. Arch Gen Psychiatry. 2006;63(8):856. doi:10.1001/archpsyc.63.8.856
23. Murrough JW, Iosifescu DV, Chang LC. Antidepressant efficacy of ketamine in treatment-resistant major depression: a two-site randomized controlled trial. Am J Psychiatry. 2013;170(10):1134–1142. doi:10.1176/appi.ajp.2013.13030392
24. Singh JB, Fedgchin M, Daly E, et al. Intravenous esketamine in adult treatment-resistant depression: a double-blind, double-randomization, placebo-controlled study. Biol Psychiatry. 2016;80(6):424–431. doi:10.1016/j.biopsych.2015.10.018
25. Lan X, Wang C, Zhang F, et al. Short-term cognitive effects of repeated-dose esketamine in adolescents with major depressive disorder and suicidal ideation: a randomized controlled trial. Child Adolesc Psychiatry Ment Health. 2023;17(1). doi:10.1186/s13034-023-00647-2
26. Liu RJ, Fuchikami M, Dwyer JM, Lepack AE, Duman RS, Aghajanian GK. GSK-3 inhibition potentiates the synaptogenic and antidepressant-like effects of subthreshold doses of ketamine. Neuropsychopharmacology. 2013;38(11):2268–2277. doi:10.1038/npp.2013.128
27. Sforzini L, Pariante CM, Palacios JE, et al. Inflammation associated with coronary heart disease predicts onset of depression in a three-year prospective follow-up: a preliminary study. Brain Behav Immun. 2019;81:659–664. doi:10.1016/j.bbi.2019.07.023
28. Maes M, Berk M. Targeting classical IL-6 signalling or IL-6 trans-signalling in depression? Expert Opin Ther Targets. 2014;18:495–512.
29. Yahui L, Qiushuang Q, Gang M. Analysis of acute phase reactant levels in elderly patients with depression. Int J Psychiat. 2019;3:413–416.
30. Hu X, Liu C, Zeng Y, Mao Y, Bai L. Effect of ultrasound-guided transversus abdominis plane block on postoperative analgesia in patients undergoing hepatic surgery. Hainan Med J. 2019;8:999–1003.
31. Autry AE, Adachi M, Nosyreva E. NMDA receptor blockade at rest triggers rapid behavioural antidepressant responses. Nature. 2011;475(7354):91–95. doi:10.1038/nature10130
32. White D, Leach C, Sims R, Atkinson M, Cottrell D. Validation of the hospital anxiety and depression scale for use with adolescents. Br J Psychiatry. 1999;175:452–454. doi:10.1192/bjp.175.5.452
33. Jörngården A, Wettergen L, von Essen L. Measuring health-related quality of life in adolescents and young adults: swedish normative data for the SF-36 and the HADS, and the influence of age, gender, and method of administration. Health Qual Life Outcomes. 2006;4:91. doi:10.1186/1477-7525-4-91
34. Ng QX, Lim YL, Ong C, New S, Fam J, Liew TM. Hype or hope? Ketamine for the treatment of depression: results from the application of deep learning to Twitter posts from 2010 to 2023. Front Psychiatry. 2024;15:1369727. doi:10.3389/fpsyt.2024.1369727
35. Zhou Y, Lan X, Wang C, et al. Effect of repeated intravenous esketamine on adolescents with major depressive disorder and suicidal ideation: a randomized active-placebo-controlled trial. J Am Acad Child Adolesc Psychiatry. 2024;63(5):507–518. doi:10.1016/j.jaac.2023.05.031
36. Li S, Li H, Zhang R, Zhang F, Yin J, He L. Effect of modified opioid sparing anaesthesia on postoperative quality of recovery in patients undergoing laparoscopic bariatric surgery: protocol for a monocentre, double-blind randomised controlled trial - the MOSA study. BMJ Open. 2024;14(7):e086523. doi:10.1136/bmjopen-2024-086523
37. Mihaljević S, Pavlović M, Reiner K, Ćaćić M. Therapeutic Mechanisms of Ketamine. Psychiatry Danub. 2020;32(3–4):325–333. doi:10.24869/psyd.2020.325
38. Wen Y, Xu J, Shen J, et al. Esketamine prevents postoperative emotional and cognitive dysfunction by suppressing microglial m1 polarization and regulating the BDNF-TrkB pathway in ageing rats with preoperative sleep disturbance. Mol Neurobiol. 2024;61(8):5680–5698. doi:10.1007/s12035-023-03860-4
39. Hess EM, Riggs LM, Michaelides M, Gould TD. Mechanisms of ketamine and its metabolites as antidepressants. Biochem Pharmacol. 2022;197:114892. doi:10.1016/j.bcp.2021.114892
40. Yan H, Chen W, Chen Y, et al. Opioid-free versus opioid-based anesthesia on postoperative pain after thoracoscopic surgery: the use of intravenous and epidural esketamine. Anesth Analg. 2023;137(2):399–408. doi:10.1213/ane.0000000000006547
41. Carron M, Tamburini E, Linassi F, Pettenuzzo T, Boscolo A, Navalesi P. Efficacy of nonopioid analgesics and adjuvants in multimodal analgesia for reducing postoperative opioid consumption and complications in obesity: a systematic review and network meta-analysis. Br J Anaesth. 2024;133(6):1234–1249. doi:10.1016/j.bja.2024.08.009
42. Duan WY, Peng K, Qin HM, et al. Esketamine accelerates emergence from isoflurane general anaesthesia by activating the paraventricular thalamus glutamatergic neurones in mice. Br J Anaesth. 2024;132(2):334–342. doi:10.1016/j.bja.2023.10.038
43. Singh JB, Fedgchin M, Daly EJ, et al. A double-blind, randomized, placebo-controlled, dose-frequency study of intravenous ketamine in patients with treatment-resistant depression. Am J Psychiatry. 2016;173(8):816–826. doi:10.1176/appi.ajp.2016.16010037
44. Jonkman K, Duma A, Olofsen E, et al. Pharmacokinetics and bioavailability of inhaled esketamine in healthy volunteers. Anesthesiology. 2017;127(4):675–683. doi:10.1097/aln.0000000000001798
45. Kamp J, Jonkman K, van Velzen M, et al. Pharmacokinetics of ketamine and its major metabolites norketamine, hydroxynorketamine, and dehydronorketamine: a model-based analysis. Br J Anaesth. 2020;125(5):750–761. doi:10.1016/j.bja.2020.06.067
46. Matłoka M, Janowska S, Gajos-Draus A, et al. Esketamine inhaled as dry powder: pharmacokinetic, pharmacodynamic and safety assessment in a preclinical study. Pulm Pharmacol Ther. 2022;73-74:102127. doi:10.1016/j.pupt.2022.102127
47. Qu S, Zhang WJ, Zhou HJ, Deng F, Liu RJ, Yan WJ. The efficacy and safety of patient-controlled intravenous analgesia with esketamine after total hip arthroplasty: a randomized controlled trial. BMC Anesthesiol. 2025;25(1):31. doi:10.1186/s12871-025-02894-6
48. Ashtary-Larky D, Bagheri R, Abbasnezhad A, Tinsley GM, Alipour M, Wong A. Effects of gradual weight loss v. rapid weight loss on body composition and RMR: a systematic review and meta-analysis. Br J Nutr. 2020;124(11):1121–1132. doi:10.1017/s000711452000224x
49. Medeiros GC, Gould TD, Prueitt WL, et al. Blood-based biomarkers of antidepressant response to ketamine and esketamine: a systematic review and meta-analysis. Mol Psychiatry. 2022;27(9):3658–3669. doi:10.1038/s41380-022-01652-1
50. Serhan CN, Brain SD, Buckley CD, et al. Resolution of inflammation: state of the art, definitions and terms. FASEB J. 2007;21(2):325–332. doi:10.1096/fj.06-7227rev
51. Feeney A, Papakostas GI. Pharmacotherapy: ketamine and Esketamine. Psychiatr Clin North Am. 2023;46(2):277–290. doi:10.1016/j.psc.2023.02.003
52. Klein CC, Bruns KM, McLaughlin LE, Blom TJ, Patino Duran LR, DelBello MP. Family environment of youth with first episode Mania. Clin Child Psychol Psychiatry. 2023;28(4):1279–1290. doi:10.1177/13591045221141773
53. Garaigordobil M. Educational psychology: the key to prevention and child-adolescent mental Health. Psicothema. 2023;35(4):327–339. doi:10.7334/psicothema2023.1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.