Back to Journals » Drug Design, Development and Therapy » Volume 19
Investigating Effective Application Times for Topical Anesthetics in Non-Coring Needle Insertion Over Totally Implantable Venous Access Devices
Authors Jiang G, Yang X, Yang L, Liu J, Yuan H ![]() , Jiang X
, Jiang X ![]()
Received 6 September 2025
Accepted for publication 21 December 2025
Published 26 December 2025 Volume 2025:19 Pages 11779—11788
DOI https://doi.org/10.2147/DDDT.S565220
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Tamer Ibrahim
Guowei Jiang,* Xiaolei Yang,* Liye Yang,* Jiajing Liu, Hongbin Yuan, Xin Jiang
Department of Anesthesiology, Shanghai Changzheng Hospital, Second Affiliated Hospital of Naval Medical University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hongbin Yuan, Department of Anesthesiology, Shanghai Changzheng Hospital, Second Affiliated Hospital of Naval Medical University, Shanghai, 200003, People’s Republic of China, Tel +86 21 81885822, Email [email protected] Xin Jiang, Department of Anesthesiology, Shanghai Changzheng Hospital, Second Affiliated Hospital of Naval Medical University, Shanghai, 200003, People’s Republic of China, Tel +86 21 81885826, Email [email protected]
Purpose: This study aims to ascertain the median effective time (ET50) and the 95% effective time (ET95) of EMLA cream and tetracaine hydrochloride gel for analgesia during non-coring needle insertion into totally implantable venous access devices (TIVADs).
Patients and Methods: Participants were randomly assigned to either Group E, receiving 2g of EMLA cream, or Group T, receiving 1g of tetracaine hydrochloride gel. Prior to needle insertion, the topical anesthetic was uniformly applied to a 1 cm radius around the puncture site. The initial target application time was set at 60 minutes for Group E and 30 minutes for Group T. For each subsequent participant, the target time was adjusted using a 1:1.1-time gradient, based on the Numeric Rating Scale (NRS) score of the preceding participant. Baseline characteristics, NRS scores, and adverse reactions were documented by a researcher who was not involved in the needle insertion process. The probit analysis method was employed to determine the ET50 and ET95 values.
Results: The ET50 and ET95 of patients to achieve painless non-coring needle insertion with EMLA cream were 55.882 minutes (95% Confidence Interval [CI]: 51.369– 59.935 minutes) and 63.587 minutes (95% CI: 59.684– 92.592 minutes), respectively. In comparison, the ET50 and ET95 for tetracaine hydrochloride gel were 39.092 minutes (95% CI: 36.646– 41.678 minutes) and 43.388 minutes (95% CI: 41.111– 56.859 minutes), respectively. There was no statistically significant difference between the two groups regarding the incidence of mild and serious adverse reactions.
Conclusion: Application of EMLA cream for 64 minutes or tetracaine gel for 44 minutes at the site of TIVADs resulted in a safely conducted, painless non-coring needle puncture for 95% of patients.
Plain Language Summary: While totally implantable venous access ports (TIVADs) have significantly improved the comfort and safety of infusion therapy for cancer patients, patients still commonly experience pain from non-coring needle insertion prior to treatment. Topical anesthesia with local anesthetics can effectively reduce this puncture-related pain, yet the optimal application time remains undetermined. In this study, the researchers applied EMLA cream and tetracaine gel were applied to alleviate such pain. Using the up-and-down method and probit analysis, they estimated the median effective time (ET50) and the 95% effective time (ET95) for both anesthetics. The results show that 95% of patients had a safe, painless port needle puncture using either EMLA cream for 64 minutes or tetracaine gel for 44 minutes.
Keywords: lidocaine and prilocaine cream, tetracaine hydrochloride gel, topical anesthesia, effective time, PORT
Introduction
In recent years, the extensive adoption of totally implantable venous access devices (TIVADs), commonly referred to as PORTs, has conferred substantial benefits to patients necessitating long-term, recurrent intravenous drug therapy.1,2 Compared with peripherally inserted central catheters (PICCs) and central venous catheters, TIVADs demonstrate reduced overall complication rates, diminished incidences of removal due to complications, and decreased rates of thrombosis. TIVADs not only ensure a high degree of safety but also eliminate externally exposed components, thereby enhancing aesthetic appeal, bolstering patient confidence, and improving convenience in daily life. Despite these advantages, the maintenance and utilization of TIVADs necessitate repeated non-coring needle insertions, which frequently result in patient discomfort and provoke anxiety and fear.3 Consequently, it is imperative to address and mitigate the pain associated with non-coring needle insertions.
The application of topical anesthetics serves as an effective method for pain relief, characterized by minimal discomfort.4 The EMLA cream, an emulsion in which the oil phase is a eutectic mixture of 2.5% lidocaine and 2.5% prilocaine, represents the earliest and most extensively utilized formulation, albeit requiring 60–120 minutes to achieve satisfactory analgesia.5 Research suggests that tetracaine hydrochloride gel, another frequently employed agent, demonstrates a slightly more rapid onset.6,7 To date, no studies have explored the time to 50% efficacy (ET50) and time to 95% efficacy (ET95) of topical anesthetics for pain relief in non-coring needle insertion. Thus, in order to assess the efficacy and safety of EMLA cream and tetracaine gel used in non-coring needle insertion over TIVAD, this study aims to determine the median and 95% effective time of topical anesthetics and observe related adverse reactions.
Materials and Methods
Ethics Statement
This study was approved by the Ethics Committee of the Second Affiliated Hospital of Naval Medical University (Approval No. 2024SL160) and was registered with the China Clinical Trial Registry (Registration No. ChiCTR2500099576). Data collection for this trial took place at the ambulatory ward of the Second Affiliated Hospital of Naval Medical University from March to May 2025.
Participants and Inclusion Criteria
The inclusion criteria comprised patients undergoing non-coring needle insertion over TIVADs at our center during the study period, who were aged 18 years or older at the time of providing informed consent. The exclusion criteria included individuals with allergies to local anesthetics, contraindications to local anesthetics, long-term use of analgesic drugs, neurological or psychiatric disorders (such as aphasia or epilepsy), and those using medications that may affect the metabolism of local anesthetics. Withdrawal criteria encompassed the occurrence of serious adverse reactions, the investigator’s decision to terminate the study for safety reasons, and voluntary withdrawal by the participants.
Fundamental Theory
This study utilized the modified sequential method of Dixon-Mood, a technique frequently employed in medical research to investigate the 50% effective doses, concentrations, or volumes for intravenous or perineural drug administration.8,9 We hypothesize that the transdermal absorption rate of both investigational drugs increases linearly with the duration of use, a relationship that has been previously established in vitro and in animal studies in some topical anesthetics.10–12 Since the transdermal absorption of both topical anesthetics cannot be precisely quantified, we explored the relationship between duration of use—rather than dose—and analgesic efficacy.
Study Protocol
Patients were randomly assigned to either Group E (EMLA cream 2g) or Group T (tetracaine hydrochloride gel 1g) and were sequentially numbered from ‘1” to “n” within each group. Operational process diagram was shown in Figure 1. All port sites were located on the chest wall. Prior to the puncture, topical anesthetics were uniformly applied to a 1 cm radius of the skin around the puncture site. After the designated application period, the drug was removed, and a sterile puncture was immediately performed by the same experienced nurse using a 22G non-coring needle.(Figure 1) Pain levels were evaluated using an 11-point verbal numeric rating scale (NRS) within 5 minutes post-puncture, where 0 represented “No pain” and 10 represented “Worst imaginable pain”.13 Subjects were continuously monitored for changes in local skin conditions (such as pallor, erythema, edema, or rash) and local sensory abnormalities (such as alterations in temperature sensation or pruritus) following the administration of the anesthetics. In case of serious adverse reactions, such as systemic allergic reactions or toxic responses, routine symptomatic management or emergency resuscitation was administered. In such cases, the patient met the exit criteria, and their designated application time was transferred to the next enrolled patient.
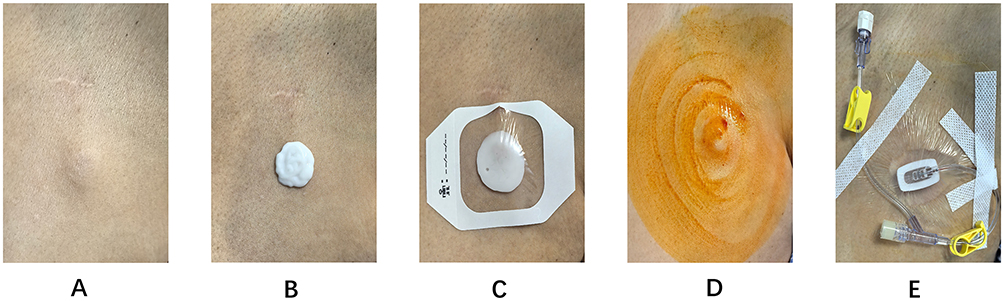 |
Figure 1 Operation Flow Diagram. (A) Skin condition prior to procedure. (B) Apply the prescribed dosage of medication above the puncture site. (C) Spread evenly into a circle approximately 1 cm in diameter and cover with a protective dressing. (D) Remove medication and disinfect skin. (E) Conduct the puncture using a non-traumatic needle. |
Setting of Target Time and Termination
The target time for the nth patient is defined as tn, and the target time gradient ratio is set to 1.1, meaning it satisfies either tn/tn+1=1.1 or tn+1/tn=1.1. The initial time, t1, was set according to Taddio’s study,6 60 minutes for group E and 30 minutes for group T.
The target time for each subsequent patient increased or decreased based on the previous patient’s NRS score. If the nth patient experiences no pain (NRS = 0), the target time for the n + 1st patient is t(n+1) = tn / 1.1; Conversely, if the nth patient experiences pain (NRS > 0), the target time for the n + 1st patient is t(n+1) = tn × 1.1. Sequential graphs were plotted based on pain response and target time for each patient. Statistical analyses were performed when seven folds were reached in each group, at which point the study concluded.8
Data Collection
The study data were independently recorded by a researcher distinct from the puncture nurse. Baseline characteristics encompassed patients’ diagnosis, sex, age, height, and weight. The primary outcomes assessed were ET50, ET95, and their confidence intervals (CIs) for the efficacy of EMLA cream or tetracaine hydrochloride gel in rendering non-coring needle insertion painless. Secondary outcomes included patients’ NRS scores; mild adverse reactions, such as pallor, erythema, edema, rash, alterations in temperature sensation, and pruritus of the skin; and serious adverse reactions, including systemic allergic and toxic reactions.
Statistical Analysis
Statistical analyses were conducted using SPSS (version 26.0) and R software (version 4.4.2). The Shapiro–Wilk test was employed to assess the normality of the data distribution. Data following a normal distribution were reported as mean ± standard deviation, with t-tests used for intergroup comparisons. Data not following a normal distribution were presented as median (interquartile range), with Mann–Whitney U-tests employed for intergroup comparisons. Categorical data were expressed as numerical values (percentages), and chi-square tests or Fisher’s exact probability method were utilized for intergroup comparisons. Statistical significance was determined at a threshold of P < 0.05. The Probit analysis method was employed to estimate the median effective time and the 95% effective time for topical anesthetics to achieve painless non-coring needle insertion over TIVADs. The effective time (ET) of EMLA/ tetracaine is established through the Dixon up-and-down method, with time–response data analyzed via probit regression. Regression coefficients are calculated using regression analysis to estimate the effective time value on the linear probit regression plot, thereby creating a time–response curve for EMLA/ tetracaine. The sequential formula and probit regression model were used to calculate ET50, and ET95 was determined using the probit regression model.
Results
Study Characteristics
Group E enrolled a total of 26 patients, whereas Group T enrolled 25 patients. Baseline characteristics are detailed in Table 1. There were no statistically significant differences between the two groups regarding baseline characteristics (p>0.05), including gender, age, height, weight, BMI, and diagnosis. The average age of the patients was 65.8 ± 9.14 years, and the mean BMI was 22.8 ± 2.45 kg/m2. All participants were diagnosed with either myeloma or lymphoma, with no significant differences in the distribution of these diagnoses between the groups.
 |
Table 1 Baseline Characteristics |
ET50 and ET95 for EMLA Cream or Tetracaine Hydrochloride Gel
Sequential plots illustrating the time-pain response to topical anesthetics following non-coring needle insertion were generated, considering both the duration of anesthetic application and the corresponding pain response in each patient (Figures 2 and 3). A probit regression linear model was employed to fit the time-effect curves for the topical anesthetics (Figures 4 and 5). The estimated times for 50% and 95% effectiveness (ET50 and ET95) of EMLA cream in rendering non-coring needle insertion painless were 55.882 minutes (95% CI: 51.369–59.935 minutes) and 63.587 minutes (95% CI: 59.684–92.592 minutes), respectively. In comparison, the ET50 and ET95 for tetracaine hydrochloride gel were 39.092 minutes (95% CI: 36.646–41.678 minutes) and 43.388 minutes (95% CI: 41.111–56.859 minutes), respectively.
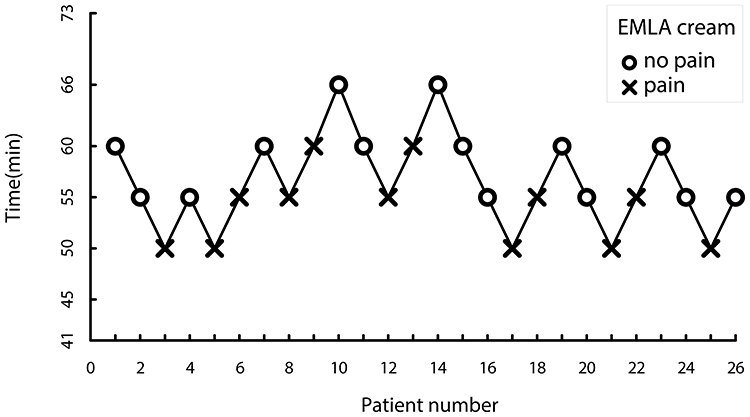 |
Figure 2 Sequential graph of EMLA cream. |
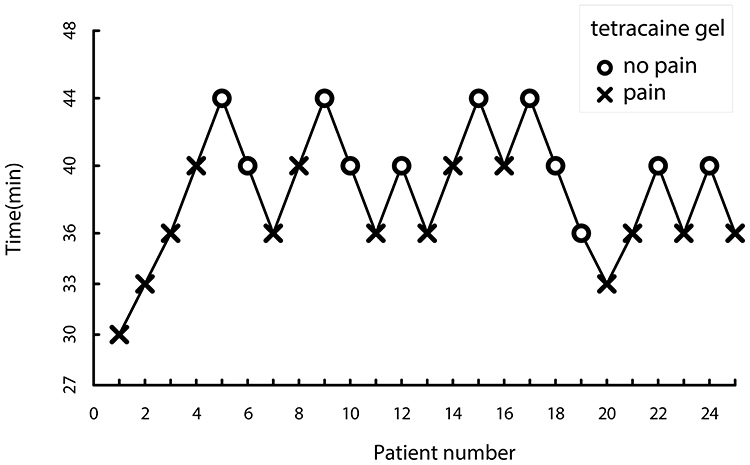 |
Figure 3 Sequential graph of tetracaine hydrochloride gel. |
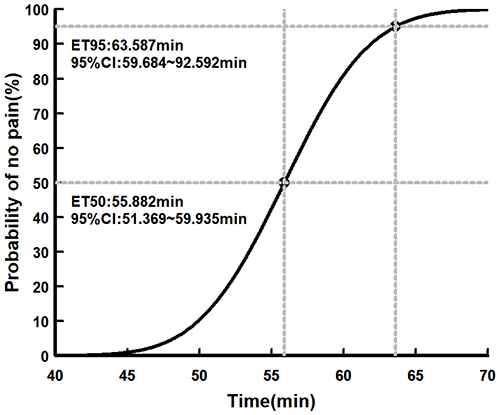 |
Figure 4 Fitted time-effect curve for EMLA cream. |
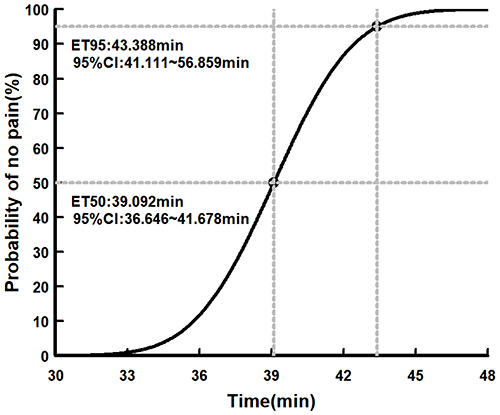 |
Figure 5 Fitted time-effect curve for tetracaine hydrochloride gel. |
NRS Scores
Detailed NRS scores for both groups are shown in Tables 2 and 3. All patients experienced no pain or mild pain.
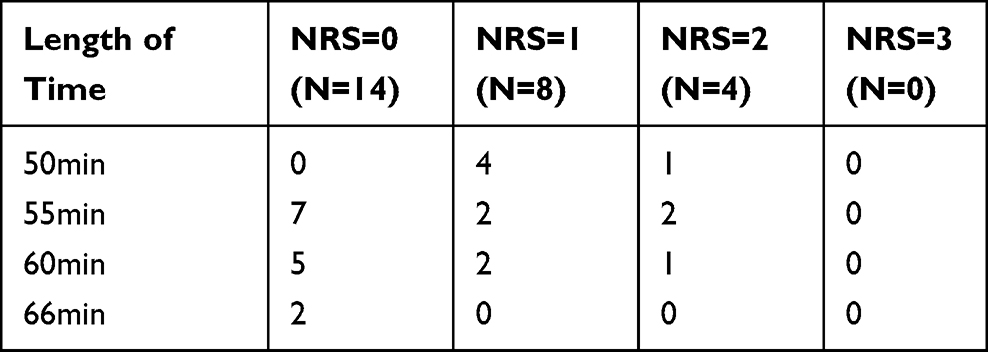 |
Table 2 NRS in Group E |
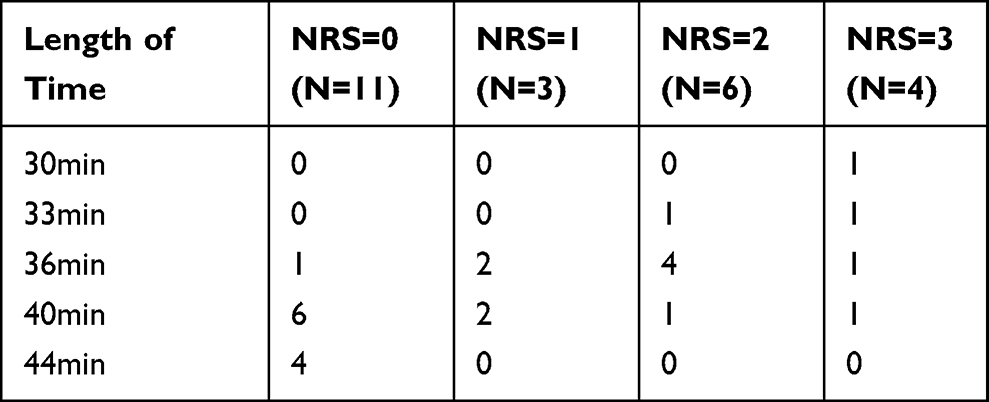 |
Table 3 NRS in Group T |
Adverse Reactions
There was no significant between-group difference in the incidence of mild adverse reactions (pallor, erythema, edema, rash, alteration in temperature sensation, and pruritus of the skin) between the two groups (Table 4). No systemic allergic or toxic reactions were reported in either group (0/26 vs 0/25).
 |
Table 4 Mild Adverse Reactions |
Discussion
TIVADs has many benefits over PICC lines, so it is becoming the preferred choice for patients requiring long-term or repeated intravenous therapy, such as chemotherapy, total parenteral nutrition (TPN), blood product administration, or frequent blood sampling, particularly those with malignancies undergoing prolonged treatment. The use of TIVADs offers convenience to patients, while still accompanied by a certain degree of puncture pain. Research indicates that the incidence of mild and moderate to severe pain associated with non-coring needle insertion is 67.5% and 37.9%, respectively, with a mean Visual Analog Scale (VAS) score up to 3.91±1.35.14 Both EMLA cream and tetracaine hydrochloride gel have been demonstrated to effectively alleviate this pain;15 however, the relationship between application duration and the analgesic efficacy of these agents remains unclear. This study is the first to investigate the time-effect relationship of topical anesthetics using a sequential approach, which minimizes patient exposure to suboptimal interventions and requires a smaller sample size.16
No significant differences were observed in the baseline characteristics between the two groups. Furthermore, the degree of puncture pain may be influenced by factors such as needle size, insertion site, and tip penetration force. To minimize potential bias, all patients in our study were punctured by the same experienced nurse using a 22-gauge non-coring needle, with the infusion ports positioned in the anterior thorax of the patients. The assessment of procedural pain from needle-based interventions relies inherently on subjective patient-reported outcomes. Although mild pain (NRS scores 1–3) is often deemed acceptable, the discrimination between a score of 3 (mild) and 4 (moderate) is frequently inconsistent in practice. This ambiguity compromises the reliability of such intermediate values as robust study endpoints.17 To enhance objectivity, we defined the primary endpoint as a complete absence of pain (NRS=0). This criterion provides an unambiguous, dichotomous measure, thereby improving reliability. Consequently, the analgesic target time identified in our study maybe substantially longer than the time required to achieve merely an “acceptable” level of pain (NRS ≤3).
Our findings demonstrate that tetracaine gel achieves effective analgesia in significantly less time than EMLA cream for both 50% and 95% of patients (ET50: 56 minutes for EMLA vs 39 minutes for tetracaine; ET95: 64 minutes vs 43 minutes). The time-effect curve for EMLA in alleviating non-coring needle penetration pain (Figure 4) exhibited a profile analogous to that reported in studies of EMLA for venipuncture analgesia, indicating a minimum application time of 45 minutes in adults, with a 94% rate of successful analgesia attained between 60 and 180 minutes.18 In contrast, a previous investigation assessing non-coring needle penetration pain reported complete pain relief in only 1.5%, 35.3%, and 54% of patients receiving no EMLA, EMLA applied for 30 minutes, and EMLA applied for 60 minutes, respectively.19 Notably, the ET35 derived from our data was 54 minutes—substantially longer than the 30-minute application time associated with 35.3% pain relief in the earlier study. This discrepancy may be attributable to differences in study population characteristics: the prior study exclusively enrolled patients with previous needle puncture experience, whereas our cohort included both naive and experienced patients. It is plausible that prior exposure to the procedure shapes preprocedural anticipation of pain, potentially modulating pain perception and reported outcomes. The clinical evidence base for tetracaine gel as analgesia during non-coring needle port access is currently confined to pediatric populations. Although a prior study in children demonstrated comparable efficacy between tetracaine gel applied for 30 minutes and EMLA cream applied for 60 minutes (mean faces pain scale scores: 2.0 vs 1.5, p=0.09),15 data in adult patients remain absent. This lack of adult data may reflect the gel’s cost and a prevailing assumption of high pain tolerance in adults,7 reducing the perceived need for intervention. Our study addresses this gap by providing evidence for its application in adults.
In our study, mild adverse reactions to EMLA included pallor and erythema, whereas tetracaine gel was associated with erythema, pruritus, and edema. No serious adverse reactions to EMLA were identified, likely due to its low incidence, minimal dosage, and short duration of administration. Even with continuous application of 15 g of EMLA for four hours, no systemic allergic or toxic reactions were observed in healthy Chinese subjects.20 Similarly, our study did not identify any serious adverse reactions to tetracaine gel. Although the overall frequency of cutaneous adverse events is similar between the two treatments, study evidence suggests divergent skin reactions: EMLA cream primarily causes skin blanching, while tetracaine gel more commonly induces erythema.21,22
Furthermore, the mean age of the study population exceeded 60 years, indicating that our findings may not be applicable to pediatric populations. Nonetheless, the necessity for topical anesthetics is notably higher in children. A study demonstrated that the mean VAS pain score for children decreased from 3.5 to 1.7 after 60 minutes of EMLA application compared to 40 minutes.23 According to current clinical guidance, tetracaine-based creams are the suggested first-line option in scenarios requiring rapid-onset analgesia for cannulation or puncture within a 30–45 minute window. Conversely, for all other elective, non-emergent needle procedures in children, EMLA cream is recommended, with the stipulation that it be applied for over 60 minutes as prescribed.7
This study has several limitations. Firstly, an intraindividual, comparative trial, akin to the methodology employed by Junputipong et al24 might have been more advantageous; however, this approach was not adopted due to uncertainties regarding patient attendance. Secondly, the study’s sample size was limited, which may not adequately capture the incidence of rare adverse reactions. Thirdly, the experimental design adopted in this study essentially limits the feasibility of intergroup comparisons. Consequently, a study with a larger sample size is warranted to comprehensively assess the safety profile of both drugs.
Additionally, the duration required for topical anesthetics to achieve effective analgesia remains prolonged. There are numerous strategies worth investigating to reduce this duration. Accelerating transdermal anesthetic rates through methods such as heating,25 ultrasound-driven,26 or microneedle technology.27 Alternatively, synergistic analgesic techniques, including the Valsalva maneuver,4 cold therapy,14,28 distraction29 and aromatherapy,30 could be employed in combination.
Conclusion
Using either EMLA cream for 64 minutes or tetracaine gel for 44 minutes at the TIVADs site for a non-coring needle puncture resulted in a safely conducted, painless procedure for 95% of patients.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the Xin Jiang and Hongbin Yuan upon reasonable request.
Ethics Approval and Consent to Participate
This study was performed in line with the principles of the Declaration of Helsinki and approved by the Medical Ethics Committee of the Second Affiliated Hospital of Naval Medical University (Approval No. 2024SL160). The study was registered at the China Clinical Trials Registry (Registration No. ChiCTR2500099576). Written informed consent was obtained from all participants, or, when applicable, from their legal representatives.
Acknowledgments
We thank Lian Zhu for linguistic assistance.
Funding
This work was supported by Military clinical key specialty (JDLCZDZK to Y.H.B).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Xu Y, Fei XY, Xue YH, et al. Chinese expert consensus on the nursing management of the totally implantable venous access device. J Cancer Res Ther. 2022;18(5):1231–1240. doi:10.4103/jcrt.jcrt_387_22
2. Yeow M, Soh S, Yap R, et al. A systematic review and network meta-analysis of randomized controlled trials on choice of central venous access device for delivery of chemotherapy. J Vasc Surg Venous Lymphat Disord. 2022;10(5):1184–1191e1188. doi:10.1016/j.jvsv.2022.03.007
3. Savas EH, Semerci R, Bayram C. The effect of a biofeedback-based virtual reality game on pain, fear and anxiety levels during port catheter needle insertion in pediatric oncology patients: a randomized controlled study. Eur J Oncol Nurs. 2024;70:102621. doi:10.1016/j.ejon.2024.102621
4. Shi S, Zhu R, Huang X, et al. Comparison of the effects of Valsalva maneuver, EMLA cream, and the combination of both in relieving pain of needle insertion on totally implantable access port: a randomized controlled study. J Vasc Access. 2024;25(5):1576–1583. doi:10.1177/11297298231169155
5. Drugs@FDA Database [homepage on the Internet]. EMLA cream: Package insert. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/019941s021lbl.pdf.
6. Taddio A, Gurguis MG, Koren G. Lidocaine-prilocaine cream versus tetracaine gel for procedural pain in children. Ann Pharmacother. 2002;36(4):687–692. doi:10.1345/aph.1A138
7. Stavleu DC, Mulder RL, Kruimer DM, et al. Topical analgesia during needle-related procedures in children: a clinical practice guideline. Arch Dis Child. 2025;110(8):657–661. doi:10.1136/archdischild-2024-326917
8. Gorges M, Zhou G, Brant R, Ansermino JM. Sequential allocation trial design in anesthesia: an introduction to methods, modeling, and clinical applications. Paediatr Anaesth. 2017;27(3):240–247. doi:10.1111/pan.13088
9. Zhu Q, Cui L, Li X, Li Q, Wang Y. Young, healthy, underweight women require higher effective doses of propofol for successful gastroscope insertion: a dose-finding study using Dixon’s up-and-down method. Drug Des Devel Ther. 2025;19:3017–3028. doi:10.2147/DDDT.S512554
10. Du W, Qian J, Yue M, Wang T, Liu J. Preparation and pharmacodynamics study of compound ropivacaine cream. Pharm Care Res. 2017;17(6):432–436.
11. Tao M, Peng L, Wang Q, et al. Preparation and evaluation of tetracaine hydrochloride gel. Drug Eval Res. 2019;42(08):1551–1556.
12. Wei H, Chen Y, Xu L, Zheng J. Percutaneous penetration kinetics of lidocaine and prilocaine in two local anesthetic formulations assessed by in vivo microdialysis in pigs. Biol Pharm Bull. 2007;30(4):830–834. doi:10.1248/bpb.30.830
13. Bielewicz J, Daniluk B, Kamieniak P. VAS and NRS, same or different? Are visual analog scale values and numerical rating scale equally viable tools for assessing patients after microdiscectomy? Pain Res Manag. 2022;2022:5337483. doi:10.1155/2022/5337483
14. Shin J, Kim GS, Sim H. Comparing the effectiveness of three pain relief methods for inserting a needle into the implanted venous access chemoport: a randomized controlled trial. Int J Nurs Pract. 2022;28(4):e12974. doi:10.1111/ijn.12974
15. Bishai R, Taddio A, Bar-Oz B, Freedman MH, Koren G. Relative efficacy of amethocaine gel and lidocaine-prilocaine cream for Port-a-Cath puncture in children. Pediatrics. 1999;104(3):e31. doi:10.1542/peds.104.3.e31
16. Pace NL, Stylianou MP. Advances in and limitations of up-and-down methodology: a precis of clinical use, study design, and dose estimation in anesthesia research. Anesthesiology. 2007;107(1):144–152. doi:10.1097/01.anes.0000267514.42592.2a
17. Wan L, Zhao Q, Chen J, et al. Expert consensus on the application of pain evaluation questionnaires in China (2020). Chin J Painol. 2020;16(3):177–187.
18. Biccard BM. EMLA--1 h is not enough for venous cannulation. Anaesthesia. 2001;56(10):1027–1028. doi:10.1046/j.1365-2044.2001.02279-42.x
19. Yin L, Jiang S. Evaluation of EMLA cream for relieving pain during needle insertion on totally implantable venous access device. J Vasc Access. 2018;19(6):634–638. doi:10.1177/1129729818768182
20. Li L, Cai B, Li H, Wei J, Tao L, Ma P. Dermal effects and pharmacokinetic evaluation of the lidocaine/prilocaine cream in healthy Chinese volunteers. BMC Pharmacol Toxicol. 2023;24(1):51. doi:10.1186/s40360-023-00690-x
21. Ravishankar N, Elliot SC, Beardow Z, Mallick A. A comparison of Rapydan(R) patch and Ametop(R) gel for venous cannulation. Anaesthesia. 2012;67(4):367–370. doi:10.1111/j.1365-2044.2011.07000.x
22. Choy L, Collier J, Watson AR. Comparison of lignocaine-prilocaine cream and amethocaine gel for local analgesia before venepuncture in children. Acta Paediatr Int J Paediatr. 1999;88(9):961–964. doi:10.1111/j.1651-2227.1999.tb00190.x
23. Lullmann B, Leonhardt J, Metzelder M, et al. Pain reduction in children during port-a-cath catheter puncture using local anaesthesia with EMLA. Eur J Pediatr. 2010;169(12):1465–1469. doi:10.1007/s00431-010-1244-1
24. Junputipong N, Rojhirunsakool S, Deewongkij P, Kamanamool N, Udompataikul M. Comparison of the onset, depth, and duration of cutaneous anesthesia between topical 10% lidocaine and EMLA creams: a randomized, intraindividual, comparative trial. J DermatolTreat. 2022;33(7):3047–3052. doi:10.1080/09546634.2022.2109566
25. Sawyer J, Febbraro S, Masud S, Ashburn MA, Campbell JC. Heated lidocaine/tetracaine patch (Synera, Rapydan) compared with lidocaine/prilocaine cream (EMLA) for topical anaesthesia before vascular access. Br J Anaesth. 2009;102(2):210–215. doi:10.1093/bja/aen364
26. Katz NP, Shapiro DE, Herrmann TE, Kost J, Custer LM. Rapid onset of cutaneous anesthesia with EMLA cream after pretreatment with a new ultrasound-emitting device. Anesth Analg. 2004;98(2):371–376. doi:10.1213/01.ANE.0000099716.02783.C4
27. Davies LB, Gateley C, Holland P, Coulman SA, Birchall JC. Accelerating topical anaesthesia using microneedles. Skin Pharmacol Physiol. 2017;30(6):277–283. doi:10.1159/000479530
28. Li J, Sun W. Effects of cold spray on pain after non-coring needle insertion into totally implantable access port. Chin J Clin Nutr. 2022;30(1):
29. Yu Z, Zhou Y, Xu X, Lin L, Le Q, Gu Y. Pharmacological and non-pharmacological interventions in management of peripheral venipuncture-related pain: a randomized clinical trial. BMC Pediatr. 2023;23(1):58. doi:10.1186/s12887-023-03855-z
30. Yayla EM, Ozdemir L. Effect of inhalation aromatherapy on procedural pain and anxiety after needle insertion into an implantable central venous port catheter: a quasi-randomized controlled pilot study. Cancer Nurs. 2019;42(1):35–41. doi:10.1097/NCC.0000000000000551
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.