Back to Journals » Advances in Medical Education and Practice » Volume 16
Intuitive Medicine: A New Vision for Medical Education
Authors Khooshab MS ![]() , Soltani H, Owlia MB
, Soltani H, Owlia MB
Received 9 July 2025
Accepted for publication 21 December 2025
Published 25 December 2025 Volume 2025:16 Pages 2431—2438
DOI https://doi.org/10.2147/AMEP.S545621
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Mohammad Sadegh Khooshab,1 Hamidreza Soltani,2 Mohammad Bagher Owlia2
1Student Research Committee, Shahid Sadoughi University of Medical Sciences, Yazd, Iran; 2Department of Rheumatology, School of Medicine, Shahid Sadoughi University of Medical Sciences, Yazd, Iran
Correspondence: Hamidreza Soltani, Department of Rheumatology, School of Medicine, Shahid Sadoughi University of Medical Sciences, Yazd, Iran, Email [email protected]
Abstract: Intuitive medicine is a skill based on experience and pattern recognition, involving a process with subconscious reasoning that plays a significant role in clinical decision-making. Its application can enhance physicians’ speed, creativity, and diagnostic accuracy while reducing treatment costs. Despite its importance, the concept, application, and learning strategies of intuition remain unclear to many young physicians and medical students. Furthermore, the dominance of guideline-based systems and the emphasis on strict adherence in medical education have limited creativity in clinical practice. This study explores the role of intuition in clinical decision-making, emphasizing its integration with evidence-based medicine and the potential of artificial intelligence (AI) as a tool to teach and strengthen intuitive skills. Integrating intuition with evidence-based medicine can foster a more creative and adaptive medical practice. The strategic use of AI in medical education offers a promising approach to formalize and enhance the teaching of intuitive clinical reasoning. Further specialized research is recommended to optimize these approaches and validate their impact on clinical performance.
Keywords: intuition, intuitive medicine, medical education, artificial intelligence
Introduction
In philosophy, the term “intuition”, derived from the Latin word “intuitus”, meaning “to look or to gaze”, has been used from Plato to Descartes to mean the direct and immediate comprehension of a concept that is understood through cognitive perception.1 However, the general concept of intuition is derived from the Latin word “intuitio”, which implies persuasion, foreboding, inspiration, sudden ideas, and perception based on foreboding.2 In addition to these meanings, clinicians often employ intuition as a form of instinctive certainty to describe their clinical reasoning processes.1
Intuition is a clinical decision-making method often used by experienced physicians.3 It refers to decisions made without conscious reasoning.4 The use of intuition in medicine is not unscientific; it is considered a creative process and a quick, skillful method that does not adhere to the logic of cause and effect.3
Intuition is an inevitable part of decision-making in medicine and is widely used in clinical practice, though it is often underestimated compared to other clinical methods.5,6 Explaining how intuition impacts clinical decisions is difficult, which is why some believe that intuition is something like a “sixth sense” that cannot be scientifically explained.7 Furthermore, intuition may involve pattern recognition, in which experts rely on their experience, and thus it may be viewed as a cognitive skill rather than subconscious reasoning.6
Specialists, due to their extensive experience and deeper understanding of clinical signs, can interpret patient symptoms more effectively than novices,8 and generally, as clinical experience increases, the use of intuition also rises.9 Typically, specialists can make probable diagnoses at the very beginning of patient encounters.10 Also, the study conducted by Vermeulen et al demonstrated that experienced physicians rely more heavily on intuitive reasoning and seamlessly integrate it into their analytical approach, whereas novice physicians switch between the two modes and give equal importance to both, highlighting the role of practice, professional experience, the therapeutic relationship, and emotional management in intuition.11
The study conducted by Ruzsa et al showed that 40% of physicians and nurses used intuition in decision-making. The probability of making decisions based on intuition was higher in physicians than in nurses, and in experienced professionals than in beginners.12
This perspective article explores the impact of factors that limit physicians’ creativity. It also discusses the value of intuitive medicine and its role in clinical decision-making.
Theoretical Background of Intuition in Medicine
Intuitive decisions are made in real time and based on the environment or situation.6 This type of decision-making does not involve an analytical thinking process, but instead relies on instinctive judgment.6 Intuition should not be assessed in the same way as evidence-based science and requires a different understanding of its use.7 Intuition in clinical decision-making applies in complex and ambiguous situations where time is limited, and also in cases where there is insufficient scientific evidence for clinical decision-making.13 Intuition may play a role in both common and rare cases and appears relevant across a broad range of clinical scenarios,14 and the assumption that intuition is exclusively applicable to complex scenarios is increasingly being challenged.
Below, we will briefly review several existing theories regarding intuition:
Hubert Dreyfus’s Theory
Dreyfus believes that intuition is a holistic process in which the brain perceives situations as a whole without analyzing individual elements. In advanced stages of expertise, intuition replaces analytical and rule-based thinking, and this process is strengthened through experience and practice.15
Herbert Simon’s Theory
Simon considers intuition to be the result of pattern recognition and mechanical learning. In other words, intuition develops through recognizing familiar patterns and associating them with previous actions. He argues that experienced experts store a large number of patterns (chunks) in their long-term memory and reach solutions quickly by recognizing these patterns.15
Template Theory
This theory explains intuition as a combination of pattern recognition, gradual learning, and the association of emotions with cognitive processes. It emphasizes that intuition is not merely a holistic process or simple pattern recognition.15
Dual Process Theory
This theory states that the human mind has two types of thinking processes: System 1, which is fast and intuitive, and System 2, which is slow and analytical. According to this theory, intuition or System 1 processes are based on embodied predictive processing — meaning that intuition results from the brain’s rapid, involuntary predictions that estimate the likelihood of events based on past experiences and sensory information.16
Clinical Application and Case Studies
To clarify how intuition is applied in clinical decision-making, we present two real case examples where physicians used intuition to make correct diagnoses and important decisions:
Case 1, Taken and Adapted from Adam and Dempsey (2020)
Bella, a newborn girl, was born at 26 weeks of gestation, weighing 780 grams. Due to severe respiratory distress, she was immediately placed on bag-mask ventilation. However, despite initial intervention, the expected improvement in oxygen saturation and respiratory effort was not observed. In this situation, neonatologists, based on their clinical experience and intuitive understanding of the newborn’s condition, realized that the observed improvement was insufficient. Consequently, they decided to proceed with intubation and administer surfactant to enhance lung function. This decision, made in the absence of definitive criteria, played a crucial role in stabilizing the newborn. By the third day, her respiratory parameters had improved, blood tests indicated recovery, and a cranial ultrasound showed normal findings.17
Case 2, Taken and Adapted from Mitchell and Bellis (2007)
A 62-year-old patient with NSTEMI, hypercholesterolemia, diabetes, and hypertension presented to the emergency department with chest pain. Although the initial symptoms suggested pulmonary embolism, rapid changes in his clinical condition, including blood pressure instability and severe fluctuations, prompted physicians to conduct further investigations. At this stage, the physicians’ clinical intuition, based on the patient’s sudden hemodynamic changes—especially the extreme blood pressure fluctuations—raised the suspicion of pheochromocytoma. To confirm the diagnosis, an informal abdominal ultrasound was performed by a specialist, revealing a mass in the right adrenal gland. These findings ultimately led to the final diagnosis of pheochromocytoma.18
In case number 1, despite the absence of criteria for intubation and surfactant administration, their use based on clinical intuition led to an improvement in the patient’s condition. In case number 2, despite the lower likelihood of pheochromocytoma, the physicians reached the diagnosis earlier through clinical intuition. As you can see, the use of intuition in some situations can perform better than other types of clinical decision-making and lead to faster diagnosis and treatment.
Benefits and Challenges
In general, the benefits of intuitive medicine can be categorized into three main areas:
- Increased decision-making speed: In emergency situations, the ability to quickly recognize clinical patterns by specialists can reduce the time to provide vital treatments.17,19
- Enhanced creativity and flexibility: Intuitive medicine allows doctors to present different and creative solutions when facing complex conditions.7,19
- Reduced costs and unnecessary interventions: By relying on scientific experience, doctors can avoid unnecessary tests and interventions, thereby reducing treatment costs.20
Despite the benefits mentioned above, intuition in medical decision-making has challenges and limitations, including the need for the development of tools for assessment, variability based on the individual and environment, the risk of errors, and the need for complementing it with scientific evidence (Table 1).6,7
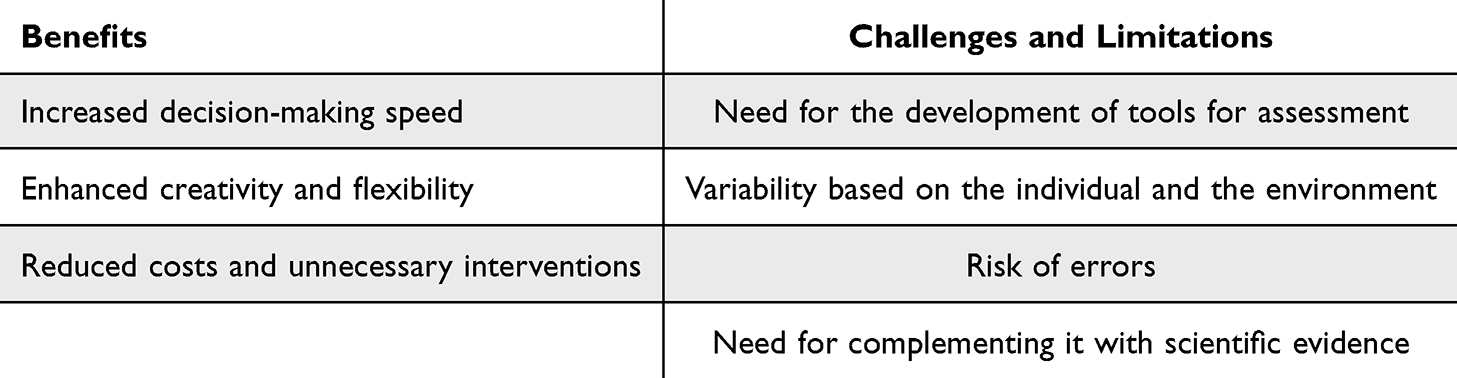 |
Table 1 Intuitive Medicine Benefits and Challenges |
In order to overcome the limitations and challenges mentioned, strategies such as fostering a culture of feedback and continuous learning can be proposed to facilitate the improvement of physicians’ skills and reduce the risk of errors. Additionally, implementing group decision-making models, where the intuitions of multiple doctors are compared, could help reduce individual errors and the influence of environmental factors on medical decisions, leading to more accurate and comprehensive decisions.
Evidence-Based Medicine: Principles, Position, and Interaction with Intuitive Medicine
Evidence-based medicine (EBM) refers to the conscious use of existing evidence to make clinical decisions.21 In practice, this concept means integrating the skills and clinical judgment of the physician, acquired through experience, with scientific evidence obtained from systematic research.21
EBM is based on three epistemological principles: First, not all evidence is of the same quality and scientific value, and therefore, medical actions should be based on the most reliable and best available evidence; Second, in the decision-making process, all relevant evidence should be comprehensively evaluated, and selective use of evidence to support a particular claim is considered an incorrect approach; Finally, clinical decision-making can only be properly done when it is based not only on scientific evidence but also on the values, preferences, and individual conditions of the patients.22
In the evidence pyramid of evidence-based medicine (EBM), randomized controlled trials (RCTs) and systematic reviews are at the highest level, while observational studies and expert opinions are placed at lower levels due to their greater susceptibility to bias and confounding factors.23 GRADE (Grades of Recommendation Assessment, Development, and Evaluation) is one of the tools used in EBM to evaluate the quality of the evidence and guide clinical decision-making.24
The following explores the differences and interactions between the two approaches: evidence-based medicine and intuitive medicine (Table 2):
- Use of Scientific Evidence vs Personal Experience: EBM emphasizes the use of scientific data and clinical research, while intuitive medicine relies on the physician’s emotional perception and experience, which is particularly useful in dealing with diseases where scientific evidence is insufficient.3,25
- Limitations of Each Approach: EBM can scientifically and precisely evaluate treatments, but in some cases, it may not be able to account for all aspects of the patient’s condition, and in contrast, intuitive medicine, especially in complex and unknown situations, can address aspects of treatment that go beyond scientific evidence.3,26
- Attention to Patient Individuality: Intuitive medicine pays more attention to the personal characteristics and specific conditions of each patient, enabling more personalized treatment, while EBM may sometimes adopt a more generalist approach, potentially paying less attention to the individual needs of the patient.27,28
- Complementarity in Dual-Process Reasoning: Contemporary cognitive research supports that effective clinical reasoning arises from the interaction between intuitive (System 1) and analytical (System 2) processes, rather than from either alone.29 Expert clinicians fluidly shift between these modes, using intuition for rapid pattern recognition and EBM for verification, resulting in faster yet reliable diagnoses.
 |
Table 2 Differences Between Evidence-Based Medicine (EBM) and Intuitive Medicine |
In the end, an integrated strategy that combines intuitive medicine with evidence-based medicine can result in more comprehensive, accurate, and patient-centered decision-making. This combination allows doctors to take advantage of their clinical expertise and consider the personal characteristics of their patients while also benefiting from scientific evidence.
Limitations of Guideline- and Protocol-Based Systems and Their Impact on Physicians’ Creativity
Modern medicine has been designed with precise standards and guidelines in order to prevent mistakes and make physicians accountable to patients.30 As a result, doctors are often forced to follow fixed and repetitive steps, even when complex and unusual situations arise. In cases where a doctor, based on their previous experiences, believes that following a specific treatment step might lead to favorable outcomes, the obligation to follow a long chain of treatment steps may cause delays in providing essential care.
This approach is also evident in today’s educational systems. An excessive focus on protocols and scientific evidence drives medical students to focus more on learning pre-established instructions than on enhancing critical thinking and intuitive skills. As a result, this generation of doctors, despite having high theoretical knowledge, may lack the ability to apply their experiences and intuition when confronted with unconventional and emergency situations.
It is essential to accept medicine as a combination of science, art, and individual experience in order to change this approach in medicine. In this regard, medical education should eliminate exams that solely assess memorizing guidelines and instead design exams to assess critical and creative thinking. It is also important to introduce clinical exercises in educational environments where students can use their intuition and logic to make decisions. Physician performance evaluation systems should also be revised to assess treatment efficacy and quality of care provided, rather than just adherence to guidelines.
Applications of Artificial Intelligence in Intuitive Medicine
Artificial intelligence systems are playing an increasing role in decision-making processes, particularly in healthcare.31 Moreover, this technology acts as a powerful tool to enhance decision-making and revolutionize medical education.32 AI plays an effective role in areas such as telemedicine, skill training, and medical diagnostics.33 By utilizing AI tools, including advanced chatbots, smart educational systems, virtual patients, gamification, and adaptive learning systems, medical education can be widely enhanced and delivered in an innovative way.32
Below, we will discuss some applications of AI systems that can be effective in teaching intuition to medical students and in intuition-based clinical decision-making.
Case-Based Medical Education
AI systems such as advanced chatbots are capable of presenting various clinical cases to students and analyzing their intuitive responses. This process can help improve students’ understanding and diagnostic abilities.
Human-AI Collaboration in Diagnosis
The combination of AI’s processing power with the intuitive abilities of physicians results in greater diagnostic accuracy and a reduction in diagnostic errors. AI can further bridge intuition and evidence by dynamically retrieving and summarizing the most relevant research evidence during the diagnostic process. Emerging models described in Nilsen et al34 work conceptualize this as “EBM 2.0”, where AI continuously updates clinical guidance and aligns it with intuitive, context-based reasoning.
Learning Clinical Patterns
Machine learning systems can recognize the diagnostic patterns of experienced physicians. This knowledge can be shared with new physicians to improve their diagnostic abilities.
Adaptive Feedback and Reflective Learning
AI systems can analyze the alignment between a learner’s intuitive responses and evidence-based recommendations, providing individualized reflective prompts. This AI-mediated reflection adopts metacognition, helping students discern when to trust intuition versus when to verify analytically.35
Building upon this perspective, the present article proposes a structured conceptual framework (Figure 1) that illustrates the dynamic relationship between intuitive medicine, EBM, and AI. This model depicts how clinical experience and pattern recognition lead to intuitive knowledge, which is integrated with analytical reasoning and reinforced through AI-mediated feedback to enhance decision-making speed, creativity, and patient-centered care.
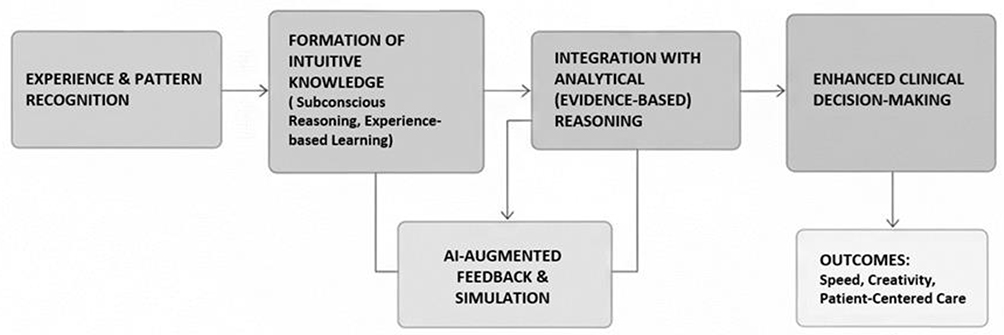 |
Figure 1 Structured conceptual framework illustrating the relationship between intuitive medicine, evidence-based medicine, and artificial intelligence. |
The discussed aspects represent a preliminary overview of AI applications in intuitive medicine, necessitating additional research to enhance the integration of these technologies in the discipline.
Conclusion
Clinical intuition is one of the key elements in medical decision-making, playing a significant role in accelerating diagnosis, fostering creativity in treatment, and reducing unnecessary interventions. As demonstrated by the case studies in this article, the use of intuition—rooted in experience, pattern recognition, and tacit knowledge—can yield favorable outcomes in both complex and routine clinical situations. Despite its importance, modern educational and healthcare systems, with their excessive emphasis on guidelines and scientific evidence, sometimes hinder the development of this vital capability in physicians.
Integrating intuition with evidence-based medicine creates a more comprehensive and effective approach to clinical care. Moreover, modern technologies such as artificial intelligence can serve as effective tools in teaching and enhancing clinical intuition. The use of pattern-learning systems, case-based learning, and human-machine collaboration in diagnosis opens new avenues for cultivating this skill.
In addition, practical recommendations for medical education and training should include targeted curriculum changes to integrate intuition-focused learning, development of assessment tools specifically designed to evaluate intuitive skills, and implementation of practical AI applications to support experiential learning and clinical decision-making. Such initiatives can bridge the gap between theoretical knowledge and real-world practice, ultimately preparing physicians to make faster, more accurate, and creative clinical decisions.
Ultimately, considering the current findings and challenges, it is recommended that future studies focus on the following areas:
- Designing standardized tools to assess clinical intuition in physicians with varying levels of experience.
- Conducting further research on the application of artificial intelligence in teaching intuition, with the aim of improving clinical decision-making through simulation, adaptive learning, and real-time diagnostic support.
Clinical Trial Number
Not applicable. This article is based on a literature review and does not include a clinical trial or primary data.
Data Sharing Statement
This article is based on a literature review and does not involve primary data. All referenced materials are publicly available.
Ethics Statement
This perspective article does not involve human participants and thus requires no ethical approval.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There was no financial support.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Braude HD. Intuition in Medicine: A Philosophical Defense of Clinical Reasoning. University of Chicago Press; 2019.
2. Kirliauskienė R, Abramauskienė J. Intuition in music education. Glob J Arts Educ. 2020;10(2):157–166. doi:10.18844/gjae.v10i2.4734
3. Greenhalgh T. Intuition and evidence--uneasy bedfellows? Br J Gen Pract. 2002;52(478):395–400.
4. Woolley A, Kostopoulou O. Clinical intuition in family medicine: more than first impressions. Ann Fam Med. 2013;11(1):60–66. doi:10.1370/afm.1433
5. Hall KH. Reviewing intuitive decision-making and uncertainty: the implications for medical education. Med Educ. 2002;36(3):216–224. doi:10.1046/j.1365-2923.2002.01140.x
6. Pearson H. Science and intuition: do both have a place in clinical decision making? Br J Nurs. 2013;22(4):212–215. doi:10.12968/bjon.2013.22.4.212
7. Nyatanga B, Vocht H. Intuition in clinical decision-making: a psychological penumbra. Int J Palliat Nurs. 2008;14(10):492–496. doi:10.12968/ijpn.2008.14.10.31493
8. Benner P. From novice to expert. Menlo Park. 1984;84(1480):10–1097.
9. Polge J. Critical thinking: the use of intuition in making clinical nursing judgments. J N Y State Nurses Assoc. 1995;26(2):4–9.
10. Brush JE, Sherbino J, Norman GR. How expert clinicians intuitively recognize a medical diagnosis. Am J Med. 2017;130(6):629–634. doi:10.1016/j.amjmed.2017.01.045
11. Vermeulen P, Dyer JO, Rochette A, Collins T. The place of intuition in the clinical reasoning of occupational therapists: a multiple‐case study. Health Soc Care Community. 2024;2024(1). doi:10.1155/2024/8385716
12. Ruzsa G, Szeverenyi C, Varga K. Person- and job-specific factors of intuitive decision-making in clinical practice: results of a sample survey among Hungarian physicians and nurses. Health Psychol Behav Med. 2020;8(1):152–184. doi:10.1080/21642850.2020.1741372
13. Nalliah RP. Clinical decision making - choosing between intuition, experience and scientific evidence. Br Dent J. 2016;221(12):752–754. doi:10.1038/sj.bdj.2016.942
14. Vanstone M, Monteiro S, Colvin E, et al. Experienced physician descriptions of intuition in clinical reasoning: a typology. Diagnosis. 2019;6(3):259–268. doi:10.1515/dx-2018-0069
15. Gobet F, Chassy P. Expertise and intuition: a tale of three theories. Minds Mach. 2009;19(2):151–180. doi:10.1007/s11023-008-9131-5
16. Bellini-Leite SC. Dual process theory: embodied and predictive; symbolic and classical. Front Psychol. 2022;13:805386. doi:10.3389/fpsyg.2022.805386
17. Adam F, Dempsey E. Intuition in decision making - risk and opportunity. J Decis Syst. 2020;29(sup1):98–116. doi:10.1080/12460125.2020.1848375
18. Mitchell L, Bellis F. Phaeochromocytoma—“the great mimic”: an unusual presentation. Emerg Med J. 2007;24(9):672–673. doi:10.1136/emj.2007.049569
19. Banning M. A review of clinical decision making: models and current research. J Clin Nurs. 2008;17(2):187–195. doi:10.1111/j.1365-2702.2006.01791.x
20. Hoops KEM, Fackler JC, King A, Colantuoni E, Milstone AM, Woods-Hill C. How good is our diagnostic intuition? Clinician prediction of bacteremia in critically ill children. BMC Med Inform Decis Mak. 2020;20(1):144. doi:10.1186/s12911-020-01165-3
21. Sackett DL, editor. Evidence-Based Medicine: Seminars in Perinatology. Elsevier; 1997.
22. Djulbegovic B, Guyatt GH. Progress in evidence-based medicine: a quarter century on. Lancet. 2017;390(10092):415–423. doi:10.1016/S0140-6736(16)31592-6
23. Koretz RL. Assessing the evidence in evidence-based medicine. Nutr Clin Pract. 2019;34(1):60–72. doi:10.1002/ncp.10227
24. Twells LK. Evidence-based decision-making 1: critical appraisal. In: Clinical Epidemiology: Practice and Methods. Springer; 2021:389–404.
25. Fisher CG, Wood KB. Introduction to and techniques of evidence-based medicine. Spine. 2007;32(19):S66–S72. doi:10.1097/BRS.0b013e318145308d
26. Sheridan DJ, Julian DG. Achievements and limitations of evidence-based medicine. J Am Coll Cardiol. 2016;68(2):204–213. doi:10.1016/j.jacc.2016.03.600
27. Horwitz RI, Singer BH. Why evidence-based medicine failed in patient care and medicine-based evidence will succeed. J Clin Epidemiol. 2017;84:14–17. doi:10.1016/j.jclinepi.2017.02.003
28. Sacristan JA, Knottnerus JA. Individual point-of-care trials: a new approach to incorporate patient’s preferences into personalized pragmatic clinical trials. J Clin Epidemiol. 2021;130:152–155. doi:10.1016/j.jclinepi.2020.09.038
29. Norman G, Pelaccia T, Wyer P, Sherbino J. Dual process models of clinical reasoning: the central role of knowledge in diagnostic expertise. J Eval Clin Pract. 2024;30(5):788–796. doi:10.1111/jep.13998
30. Mignini L. Review of clinical practice guidelines. In: Systematic Reviews to Support Evidence-Based Medicine. CRC Press; 2022:165–170.
31. Chen V, Liao QV, Wortman Vaughan J, Bansal G. Understanding the role of human intuition on reliance in human-AI decision-making with explanations. Proc ACM Hum Comput Interact. 2023;7(CSCW2):1–32.
32. Suresh N, Rajprasath R, Elantamilan D, Arghya D. Artificial intelligence revolutionizing the field of medical education. Cureus. 2023;15(11):e49604. doi:10.7759/cureus.49604
33. Acharya V, Padhan P, Bahinipati J, et al. Artificial intelligence in medical education. J Integr Med Res. 2023;1(3):87–91. doi:10.4103/jimr.jimr_17_23
34. Nilsen P, Sundemo D, Heintz F, et al. Towards evidence-based practice 2.0: leveraging artificial intelligence in healthcare. Front Health Serv. 2024;4:1368030. doi:10.3389/frhs.2024.1368030
35. Cohen B, DuBois S, Lynch PA, Swami N, Noftle K, Arensberg MB. Use of an artificial intelligence-driven digital platform for reflective learning to support continuing medical and professional education and opportunities for interprofessional education and equitable access. Educ Sci. 2023;13(8):760. doi:10.3390/educsci13080760
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.