Back to Journals » Clinical Ophthalmology » Volume 17
Intravitreal Ziv-Aflibercept versus Bevacizumab for Naïve Central Retinal Vein Occlusion with Macular Edema: An Interim Analysis of a Randomized Non-Inferiority Trial
Authors Sinawat S ![]() , Hemanak S, Chanthowong K, Sinawat S, Yospaiboon Y
, Hemanak S, Chanthowong K, Sinawat S, Yospaiboon Y ![]()
Received 4 July 2023
Accepted for publication 11 September 2023
Published 18 September 2023 Volume 2023:17 Pages 2719—2728
DOI https://doi.org/10.2147/OPTH.S428792
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Suthasinee Sinawat,1,2 Suthasinee Hemanak,1 Kwanchanok Chanthowong,1 Supat Sinawat,3 Yosanan Yospaiboon1,2
1Department of Ophthalmology, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand; 2KKU Eye Center, Khon Kaen University, Khon Kaen, Thailand; 3Department of Physiology, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand
Correspondence: Suthasinee Sinawat; Yosanan Yospaiboon, Department of Ophthalmology, Faculty of Medicine, Khon Kaen University, 123 Mitraparb Highway, Khon Kaen, 40002, Thailand, Tel +66-4336-3010, Fax +66-4334-8383, Email [email protected]; [email protected]
Purpose: To compare the efficacy of intravitreal ziv-aflibercept (IVZ) and bevacizumab (IVB) injections for the treatment of macular edema secondary to central retinal vein occlusion.
Methods: Participants were randomly assigned 1:1 to receive 3 monthly IVZ (1.25 mg/0.05 mL) or IVB (1.25 mg/0.05 mL) followed by the pro-re-nata protocol for persistent or recurrent macular edema. The primary outcomes were best-corrected visual acuity and central subfield thickness. An interim analysis was planned when half of the participants completed the follow-up.
Results: Twenty-four participants were recruited. At 6 months, mean best-corrected visual acuity in the IVB and IVZ groups improved from 1.23 ± 0.64 to 0.76 ± 0.56 logMAR (p = 0.003) and from 1.13 ± 0.59 to 0.53 ± 0.26 logMAR (p = 0.003), respectively. The percentage of visual improvement and reduction in central subfield thickness in the IVZ group were insignificantly better than those in the IVB group (44.41 ± 26.72 vs 39.64 ± 24.22%; p = 0.65) and (51.94 ± 20.35 vs 45.78 ± 24.71%; p = 0.51), respectively. Although the mean number of injections was lower in the IVZ group (4.55 ± 1.29 vs 4.82 ± 1.33), the difference was not statistically significant (p = 0.68). No ocular or systemic adverse events were observed.
Conclusion: The interim analysis demonstrated that the visual and anatomical results of IVZ were insignificantly better than those of IVB at 6 months of follow-up. The results also showed that IVZ was non-inferior to IVB for anatomical improvement but inconclusive for visual improvement.
Clinical Trial Registration: (identifier: TCTR20191205008).
Keywords: ziv-aflibercept, bevacizumab, central retinal vein occlusion, macular edema
Introduction
Macular edema (ME) is the most common complication of central retinal vein occlusion (CRVO), which can lead to visual deterioration.1 Vascular endothelial growth factor (VEGF) plays a key role in the pathogenesis of ME secondary to CRVO.2,3 Off-label anti-VEGF drug, bevacizumab, and approved anti-VEGF agents from the Food and Drug Administration, including ranibizumab and aflibercept, are used worldwide. Among anti-VEGF agents, aflibercept is considered the first choice of treatment in terms of visual improvement, which could be explained by targeting a wider range of cytokines and a stronger binding affinity.4 While previous randomized clinical trials (RCT) suggested that aflibercept and bevacizumab were comparable in their effectiveness for the treatment of ME secondary to CRVO,5,6 an exploratory post hoc analysis of a recent RCT demonstrated that bevacizumab was not inferior to aflibercept in visual improvement, but needed significantly more injections.7 Despite its effectiveness, aflibercept has a much higher cost that makes it unaffordable and unavailable to the public service.8 Therefore, bevacizumab has become the first-line treatment in real-world clinical practice owing to its acceptable efficacy and cost-effectiveness.
Ziv-aflibercept is approved for the treatment of metastatic colorectal cancer via the intravenous route.9 Ziv-aflibercept has an identical molecular structure and mechanism of action as aflibercept, which makes it potentially available for ophthalmic use at a much lower cost. Although previous studies have demonstrated that both ziv-aflibercept and bevacizumab appear safe and effective for the treatment of ME secondary to CRVO,5–7,10–14 a prospective comparison between these drugs has never been reported. Therefore, this study aimed to compare the efficacy of intravitreal ziv-aflibercept (IVZ) and intravitreal bevacizumab (IVB) treatment in patients with ME secondary to CRVO over a 6-month period.
Patients and Methods
This prospective, double-blind, randomized controlled, non-inferiority trial was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Khon Kaen University Ethics Committee for Human Research (HE621079). The study was registered in the Thai Clinical Trials Registry (identifier: TCTR20191205008) and was released on December 5, 2019. As the drug was off-label for intraocular use and may cause possible ocular and systemic complications, an interim analysis was planned to be performed when half of the participants had completed the follow-up.
Patient Eligibility
Patients with ME secondary to CRVO were recruited between December 2019 and August 2020 at KKU Eye Center, Khon Kaen University, Thailand. Written informed consent was obtained from all participants before enrollment and after an explanation of the study protocol and possible consequences. Inclusion criteria were age >45 years, diagnosis of CRVO with center-involved ME, and central subfield thickness (CST) >300 µm confirmed by spectral-domain optical coherence tomography (SD-OCT) (Spectralis, Heidelberg Engineering, Heidelberg, Germany).
The exclusion criteria were one-eyed patients, bilateral CRVO, autoimmune disorders or connective tissue diseases, ocular infections such as blepharitis and endophthalmitis, vitreoretinal diseases such as diabetic retinopathy, age-related macular degeneration, uveitis, intraocular pressure (IOP) >21 mmHg, iris neovascularization (NV), previous intravitreal corticosteroid injection, previous laser photocoagulation, previous intraocular surgery within 6 months, previous intravitreal anti-VEGF within 3 months, vitreomacular traction (VMT), or epimacular membrane (EMM) with traction on SD-OCT; media opacities that cause poor image quality; patients who could not be investigated using SD-OCT, such as nystagmus, dense posterior subcapsular cataract, and patients who could not be followed for 6 months.
Withdrawal criteria included a decrease in visual acuity >0.2 logMAR after intravitreal injections and a decrease in CST < 10% from baseline after receiving 3 monthly loading doses, defined as non-responder, severe adverse events such as endophthalmitis, retinal detachment, stroke and myocardial infarction, and patients decided to withdraw from the study.
Randomization and Masking Procedures
Participants received the intravitreal injection of either ziv-aflibercept (Zaltrap; Sanofi-Aventis, Bridgewater, NJ, USA/Regeneron, Tarrytown, NY, USA) or bevacizumab (Avastin; Genentech, South San Francisco, CA, USA). Randomization was assigned to the IVZ and IVB groups in a 1:1 ratio using a variable block randomization generator. The allocation sequence was generated using computer-generated random numbers with randomly varying block sizes. The random allocation sequence was concealed in a sealed opaque envelope, numbered sequentially, and kept by the research assistant, who was the only one who knew which code was used for the IVB or IVZ. The researchers, patients, technicians, and evaluators did not know the codes, and unblinding was performed at the end of the study.
Surgical Procedures
All patients underwent standard intravitreal injections performed by a single surgeon (SH) using a sterile technique. Three monthly intravitreal loading injections were administered and followed by the pro-re-nata (PRN) protocol. The reinjection criteria included recurrence or persistent center-involved ME and a CST >300 µm. The research assistant prepared the same volume of medication; 0.05 mL of medication, in a 1 mL syringe. The patients were disinfected with 10% povidone-iodine on the periocular skin and the eyelids. After topical anesthesia, 5% povidone-iodine was instilled and left for at least 3 min. Ziv-aflibercept 1.25 mg/0.05 mL or bevacizumab 1.25 mg/0.05 mL was injected 3–4 mm posterior to the superotemporal limbus using a 30-gauge needle. Mild pressure was applied using a cotton tip at the injection site, and a drop of antibiotics was instilled at the end.
Patient Evaluation and Outcome Measures
Demographic data, including sex, age, underlying systemic diseases, previous ocular surgeries, duration of symptoms (from the onset of symptoms reported by the patients to the date of intravitreal injection), and lens status were recorded. Complete ophthalmic examinations were performed at baseline and monthly follow-up visits, including slit-lamp biomicroscopy and best-corrected visual acuity (BCVA). IOP measurement using Goldmann applanation tonometry, indirect ophthalmoscopy, and fundus photography. The CST, intraretinal fluid (IRF), subretinal fluid (SRF), and vitreomacular interface were evaluated using SD-OCT. Systemic and ocular adverse events were also recorded.
The primary outcomes were BCVA and CST. Visual improvement was defined as the mean change in BCVA at six months compared with baseline, and the percentage of visual improvement was calculated as the visual improvement multiplied by 100 and divided by the baseline BCVA. CST reduction was defined as the mean change in CST at six months compared to baseline, and the percentage of CST reduction was calculated in the same manner. The secondary outcomes were the number of intravitreal injections and related adverse events.
Statistical Analysis
We estimated that both groups would have a final BCVA improvement in six months. At a 95% confidence level and a power of 80%, mean difference in visual improvement of 0.07 logMAR,6 standard deviation of 0.15 logMAR,6 and the acceptable margin of non-inferiority in the final visual improvement of 15% for a one-tailed test, the estimated sample size required was 17 eyes per group. With an expected 20% protocol non-compliance rate, the final estimate of enrollment consisted of 21 patients per group. For a one-tailed test, equivalence was declared if the lower one-sided confidence limit exceeded a defined level. We chose to use a one-sided test in this study to confirm that IVZ is not inferior to IVB. Equivalence and superiority were considered as positive outcomes. Analyses were performed with both intention-to-treat and per-protocol principles using Stata version 16.1 (StataCorp LP College Station, Texas, USA). Fisher’s exact test and chi-square test were used to analyze categorical variables. The Wilcoxon rank-sum test and t-test were used to analyze continuous variables. A multilevel regression model was used to analyze the variables with repeated measurements. Statistical significance was set at p <0.05.
Results
Baseline Characteristics and Patient Disposition
A total of 32 consecutive patients with unilateral CRVO and ME were evaluated; however, seven patients did not meet the inclusion criteria and one declined to participate. The causes of exclusion were recent intravitreal anti-VEGF injection (four eyes), EMM with traction (two eyes), and high IOP (one eye). Therefore, there were 24 patients enrolled in this study (Figure 1).
 |
Figure 1 Study flow chart. |
The majority of patients (58.33%) were female. The mean age of the patients was 57.15 ± 7.65 years. The mean duration of the symptoms was 1.86 ± 1.77 months. The mean initial BCVA was 1.18 ± 0.60 logMAR. Twenty-two out of 24 eyes were phakic, ranging from clear lens to mild nuclear sclerosis. Two pseudophakic eyes were in IVB group. The mean baseline CST was 746.17 ± 264.95 µm. Cystoid macular edema was found in all the studied eyes, while subfoveal serous macular detachment was present in half of cases. The demographic data and clinical characteristics of the patients are presented in Table 1. No significant differences were observed between the two groups for any of the baseline variables.
 |
Table 1 Demographic Data of Patients in the Study |
Visual Outcome
At six months, there was a statistically significant visual improvement in both the IVZ and IVB groups. The mean BCVA in the IVB group improved from 1.23 ± 0.64 logMAR at baseline to 0.76 ± 0.56 logMAR at 6 months (p = 0.003; Table 2). In the same manner, mean BCVA in the IVZ group improved from 1.13 ± 0.59 logMAR at baseline to 0.53 ± 0.26 logMAR at 6 months (p = 0.003; Table 2). Significant visual improvement in both groups occurred as early as the first month after injection and was maintained for 6 months. When comparing the groups, visual improvement of both the IVB and IVZ groups was not significantly different (p = 0.39) by multi-level regression analysis of every month BCVA from baseline to month 6 (Figure 2).
 |
Table 2 Visual Improvement at Each Visit of the Patients in Both Groups, Presented as Mean ± Standard Deviation (95% Confidence Interval) |
 |
Figure 2 Mean visual acuity at each visit of patients in the IVZ and IVB groups. Visual improvement of both groups was not significantly different (p = 0.39) by multi-level regression analysis. |
Although patients in the IVZ group had higher percentage of visual improvement than those in the IVB group (44.41 ± 26.72% vs 39.64 ± 24.22%), it was not statistically significant (mean difference 4.78%, 95% confidence interval (CI) −16.81, 26.37, p = 0.65; Table 3).
 |
Table 3 The Percentage of Visual Improvement and CST Reduction of Patients in Both Groups, Presented as Mean ± Standard Deviation (95% Confidence Interval) |
Anatomical Outcome
DME could be resolved during the study in the majority of patients; however, there was one patient with refractory DME in each group. At 6 months, the mean CST in the IVB group was reduced from 783.7 ± 292.3 µm at baseline to 381.2 ± 184.5 µm (p < 0.001). The mean CST in the IVZ group was also reduced from 708.7 ± 241.3 µm at baseline to 303.3 ± 67.9 µm (p < 0.001; Table 4). It is also noted from Table 4 that significant CST reduction in both groups occurred as early as the first month after injection. Multi-level regression analysis of CST every month until month 6 showed that CST reduction in both groups was not significantly different (p = 0.79; Figure 3). Although the percentage of CST reduction was higher in the IVZ group than those in the IVB group (51.94 ± 20.35% vs 45.78 ± 24.71%), it was not statistically significant (mean difference 6.16%, 95% CI −13.0, 25.33, p = 0.51; Table 3).
 |
Table 4 Central Subfield Thickness of the Patients in Both Groups, Presented as Mean ± Standard Deviation (95% Confidence Interval) |
 |
Figure 3 Mean central subfield thickness at each visit of patients in the IVZ and IVB groups. CST reduction of both groups was not significantly different (p = 0.79) by multi-level regression analysis. |
Figure 4 shows that the percentage of visual improvement in the IVZ group was better than IVB group, but the 95% confidence interval extended to the left of Δ and included zero line. This indicated that non-inferiority was inconclusive (upper bar). For CST reduction, the percentage of reduction in the IVZ group was also better than IVB group, but the 95% confidence interval extended to the right of Δ and included zero line. This indicated that the IVZ was non-inferior to the IVB (lower bar).15
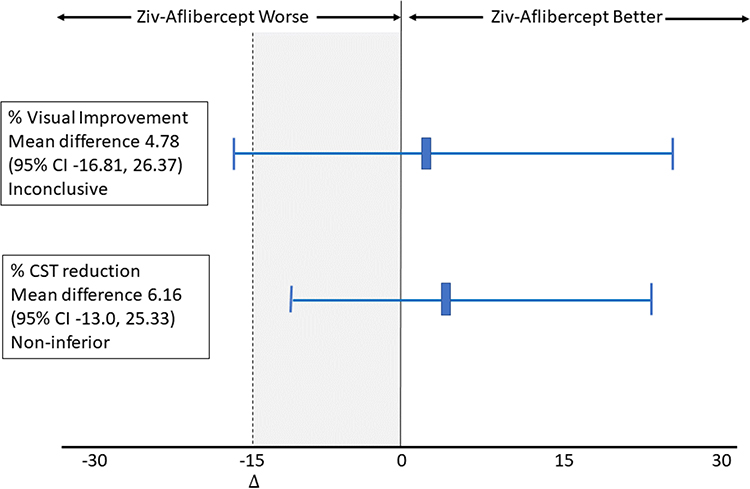 |
Figure 4 Non-inferiority analysis of the treatment difference (IVZ minus VB). The vertical dotted line represents the margin of clinical equivalence; the vertical solid line, the null effect. The shaded area indicates zone of inferiority. Error bars indicate 2-sided 95% confidence intervals. |
Number of Injections
The mean number of injections was 4.55 ± 1.29 and 4.82 ± 1.33 in the IVZ group and the IVB group, respectively. Although the mean number of injections was lower in the IVZ group, the difference was not statistically significant (p = 0.68).
Complications
The most common complication was tiny subconjunctival hemorrhage (30.77%) that resolved spontaneously within a few days. An increase in IOP was observed in one patient (4.17%) after the sixth IVB injection; however, IOP could be controlled with 0.5% timolol eye drops twice a day and resolved completely after a few days. Although no cataract and EMM progression were observed, one patient developed an EMM without traction after six IVB injections. No serious systemic adverse events or ocular complications were noted.
Discussion
Bevacizumab is commonly used as an initial anti-VEGF drug for the treatment of ME secondary to CRVO because it produces the best cost utility among anti-VEGF agents, and the real-world results also indicate good outcomes.16–19 However, bevacizumab requires significantly more injections than aflibercept in the treatment.7 Multiple visits can also be an economic and time burden, especially in remote areas. Ziv-aflibercept has the same molecular structure and mechanism of action as aflibercept; therefore, it is potentially available for ophthalmic use at a much lower cost.
Previous small case series of 1.25 mg/0.05 mL IVZ showed significant visual improvement and CST reduction in the treatment of ME secondary to CRVO.11–14 Eldeeb et al documented 12-month outcomes of IVZ in 6 patients with naïve ME secondary to non-ischemic CRVO and reported that Ziv-aflibercept achieved favorable functional and structural outcomes in ME due to CRVO.11 Mansour et al evaluated the efficacy of ziv-aflibercept in various macular diseases including 11 eyes of ME secondary to CRVO and showed that ziv-aflibercept were efficacious in the treatment of macular diseases.12 Braimah et al investigated retrospectively the efficacy of ziv-aflibercept in patients with ME from retinal vein occlusion (RVO) and demonstrated a significant improvement in both anatomical and functional outcomes at 12 months of follow-up.13 However, in a small prospective study of nine eyes with persistent or recurrent ME due to RVOs (five CRVOs and four BRVOs), Paulose et al reported that IVZ significantly improved the mean central macular thickness, but the mean BCVA did not improve from baseline.14
Although previous studies have demonstrated the efficacy of both IVZ and IVB in the treatment of ME secondary to CRVO,5–7,10–14 a prospective comparative study of IVZ and IVB has not been reported. In a retrospective study, Braimah et al compared the effectiveness of IVZ and IVB in patients with ME post-BRVO and showed that both drugs had similar visual improvement and central macular thickness reduction; however, IVZ had a smaller number of injections and visits than IVB. In our prospective RCT specifically studied in naïve CRVO, both IVZ and IVB showed significant visual improvement and CST reduction as early as in the first month and were maintained until month 6, when compared to the baseline. These results are in good agreement with those of previous studies.5–7,10–14 However, when comparing between groups, the IVZ appeared to have a better mean percentage of visual improvement and CST reduction than the IVB, but the difference was not statistically significant.
Regarding safety, the disinclination toward IVZ injection has been due to concerns about its highly concentrated buffered solution. The high osmolarity of ziv-aflibercept could lead to cellular toxicity.19 However, large and long-term studies of intravitreal 1.25 mg/0.5 mL ziv-aflibercept injections showed an acceptable safety profile.19,20 Moreover, the safety of IVZ (1.25, 2 and 2.5 mg) has been established through electroretinography studies, and no retinal toxicity was observed up to 52 weeks.21–23 In our study, off-label ziv-aflibercept requires compounding, raising concerns about sterility, shelf-life stability, and variability of drug concentration. Therefore, an interim analysis was planned for the early termination of the study if unacceptable adverse effects were apparent. The interim results demonstrated that ziv-aflibercept and bevacizumab were both effective and safe in the treatment of ME due to CRVO. The IVZ seemed to have a better mean percentage of visual improvement than bevacizumab. However, the wide confidence interval extends to the left of the non-inferiority zone and includes zero values. The result indicates that the difference is not significant, and the result regarding non-inferiority is inconclusive.15 This may be due to the small sample size or high variability of the data. However, the confidence interval of mean percentage of CST reduction stayed in the zone of non-inferiority.15 The results demonstrated that ziv-aflibercept was not inferior to bevacizumab in terms of anatomical outcomes, but the analysis of visual outcome was inconclusive.
Ocular and systemic side effects associated with IVZ injections are rare. Ocular adverse events previously reported included conjunctival thinning, scleral nodule, iridocyclitis, transient increase in IOP, cataract progression, epimacular membrane, retinal pigment epithelium tear, and endophthalmitis.19 Systemic adverse events included myocardial infarction and stroke.19 In our study, increased IOP was observed in one eye after the sixth intravitreal injection of bevacizumab. This condition was completely resolved with topical anti-glaucomatous medication for a few days.
To the best of our knowledge, this study is the first comparative RCT to evaluate the efficacy and safety of bevacizumab and ziv-aflibercept in naïve CRVO with ME. The main strength of this study was the design with double-masked RCT. The surgeon, patients, technicians, and assessors remained blinded until code breaking for the interim analysis. Furthermore, no patient was lost to follow-up or withdrawn during the 6-month follow-up period. However, this study had some limitations. The short follow-up time might not indicate a difference in the number of injections between the two drugs, especially when these drugs are used monthly in the first 3-month of loading injection. The small sample size might be another limitation to statistical insignificance. An increased sample size might result in small variability, and the confidence interval might move to the inferiority or even superiority zone. This finding indicates that an additional study should be conducted.
Conclusions
In this study, both IVZ and IVB showed significant visual improvement and CST reduction as early as the first month, and were maintained until month 6. When comparing the groups, ziv-aflibercept had insignificantly better visual and anatomical outcomes than bevacizumab in the treatment of ME secondary to CRVO. The mean number of injections was lower in the ziv-aflibercept group; however, the difference was not statistically significant. These results demonstrate the potential of ziv-aflibercept for the treatment of ME due to CRVO.
Data Sharing Statement
The study protocol and the clinical data collected during the trial, after deidentification, could be shared on personal request.
Acknowledgments
The authors would like to thank Dr. Kaewjai Thepsuthammarat, Clinical Epidemiology Unit, Faculty of Medicine, Khon Kaen University, for statistical analyses. We acknowledge Dr. Dylan Southard for the English language editing of this manuscript via the KKU Publication Clinic (Thailand). This study was supported by the Invitation Research Fund of the Faculty of Medicine, Khon Kaen University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hayreh SS, Zimmerman MB, Podhajsky P. Incidence of various types of retinal vein occlusion and their recurrence and demographic characteristics. Am J Ophthalmol. 1994;117(4):429–441. doi:10.1016/S0002-9394(14)70001-7
2. Noma H, Funatsu H, Mimura T, Harino S, Hori S. Vitreous levels of interleukin-6 and vascular endothelial growth factor in macular edema with central retinal vein occlusion. Ophthalmology. 2009;116(1):87–93. doi:10.1016/j.ophtha.2008.09.034
3. Koss MJ, Pfister M, Rothweiler F, et al. Comparison of cytokine levels from undiluted vitreous of untreated patients with retinal vein occlusion. Acta Ophthalmol. 2012;90(2):e98–e103. doi:10.1111/j.1755-3768.2011.02292.x
4. Qian T, Zhao M, Wan Y, Li M, Xu X. Comparison of the efficacy and safety of drug therapies for macular edema secondary to central retinal vein occlusion. BMJ Open. 2018;8(12):e022700. doi:10.1136/bmjopen-2018-022700
5. Scott IU, VanVeldhuisen PC, Ip MS, et al.; SCORE2 Investigator Group. Effect of bevacizumab vs aflibercept on visual acuity among patients with macular edema due to central retinal vein occlusion: the SCORE2 randomized clinical trial. JAMA. 2017;317(20):2072–2087. doi:10.1001/jama.2017.4568
6. Lotfy A, Solaiman KAM, Abdelrahman A, Samir A. Efficacy and frequency of intravitreal aflibercept versus bevacizumab for macular edema secondary to central retinal vein occlusion. Retina. 2018;38(9):1795–1800. doi:10.1097/IAE.0000000000001782
7. Hykin P, Prevost AT, Vasconcelos JC, et al.; LEAVO Study Group. Clinical effectiveness of intravitreal therapy with ranibizumab vs aflibercept vs bevacizumab for macular edema secondary to central retinal vein occlusion: a randomized clinical trial. JAMA Ophthalmol. 2019;137(11):1256–1264. doi:10.1001/jamaophthalmol.2019.3305
8. Rhoades W, Dickson D, Nguyen QD, Do DV. Management of macular edema due to central retinal vein occlusion - The role of aflibercept. Taiwan J Ophthalmol. 2017;7(2):70–76. doi:10.4103/tjo.tjo_9_17
9. Chung C, Pherwani N. Ziv-aflibercept: a novel angiogenesis inhibitor for the treatment of metastatic colorectal cancer. Am J Health Syst Pharm. 2013;70(21):1887–1896. doi:10.2146/ajhp130143
10. Wu L, Acon D, Berrocal MH, et al. Five-year outcomes after intravitreal bevacizumab of treatment-naïve eyes with macular edema secondary to CRVO in routine clinical practice: results of the Pan-American Collaborative Retina Study (PACORES) group. Int Ophthalmol. 2022;42(3):951–958. doi:10.1007/s10792-021-02077-5
11. Eldeeb M, Chan EW, Dedhia CJ, Mansour A, Chhablani J. One-year outcomes of ziv-aflibercept for macular edema in central retinal vein occlusion. Am J Ophthalmol Case Rep. 2017;8:58–61. doi:10.1016/j.ajoc.2017.10.011
12. Mansour AM, Ashraf M, Charbaji A, et al.; Ziv-aflibercept study group investigators. Two-year outcomes of intravitreal ziv-aflibercept. Br J Ophthalmol. 2018;102(10):1387–1390. doi:10.1136/bjophthalmol-2017-311591
13. Braimah IZ, Agyabeng K, Amoaku WM. Efficacy of intravitreal ziv-aflibercept in patients with macular edema following retinal vein occlusion in Korle-Bu Teaching Hospital, Ghana: a retrospective case series. Int Ophthalmol. 2021;41(7):2445–2453. doi:10.1007/s10792-021-01799-w
14. Paulose R, Chhablani J, Dedhia CJ, Stewart MW, Mansour AM. Intravitreal ziv-aflibercept for macular edema following retinal vein occlusion. Clin Ophthalmol. 2016;10:1853–1858. doi:10.2147/OPTH.S116343
15. Piaggio G, Elbourne DR, Pocock SJ, Evans SJW, Altman DG; CONSORT Group. Reporting of non-inferiority and equivalence randomized trials: extension of the CONSORT 2010 statement. JAMA. 2012;308(24):2594–2604. doi:10.1001/jama.2012.87802
16. Lin J, Gibbons A, Smiddy WE. Cost-utility of anti-vascular endothelial growth factor treatment for macular edema secondary to central retinal vein occlusion. Ophthalmol Retina. 2021;5(7):656–663. doi:10.1016/j.oret.2020.09.017
17. Wecker T, Ehlken C, Bühler A, et al. Five-year visual acuity outcomes and injection patterns in patients with pro-re-nata treatments for AMD, DME, RVO and myopic CNV. Br J Ophthalmol. 2017;101(3):353–359. doi:10.1136/bjophthalmol-2016-308668
18. Jumper JM, Dugel PU, Chen S, Blinder KJ, Walt JG. Anti-VEGF treatment of macular edema associated with retinal vein occlusion: patterns of use and effectiveness in clinical practice (ECHO study report 2). Clin Ophthalmol. 2018;12:621–629. doi:10.2147/OPTH.S163859
19. Singh SR, Stewart MW, Chattannavar G, et al. Safety of 5914 intravitreal ziv-aflibercept injections. Br J Ophthalmol. 2019;103(6):805–810. doi:10.1136/bjophthalmol-2018-312453
20. Chhablani J, Dedhia CJ, Peguda HK, Stewart M. Short-term safety of 2 MG intravitreal ziv-aflibercept. Retina. 2017;37(10):1859–1865. doi:10.1097/IAE.0000000000001440
21. de Oliveira Dias JR, de Andrade GC, Kniggendorf VF, et al. Clinical and electrophysiological evaluation after intravitreal ziv-aflibercept for exudative age-related macular degeneration. Retina. 2017;37(8):1499–1507. doi:10.1097/IAE.0000000000001385
22. de Andrade GC, de Oliveira Dias JR, Maia A, Farah ME, Meyer CH, Rodrigues EB. Intravitreal Ziv-Aflibercept for Diabetic Macular Edema: 48-Week Outcomes. Ophthalmic Surg Lasers Imaging Retina. 2018;49(4):245–250. doi:10.3928/23258160-20180329-06
23. de Oliveira Dias JR, Costa de Andrade G, Kniggendorf VF. Intravitreal ziv-aflibercept for neovascular age-related macular degeneration: 52-Week Results. Retina. 2019;39(4):648–655. doi:10.1097/IAE.0000000000002001
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effectiveness of the Use of Three-Dose Intravitreal Ziv-Aflibercept in the Management of Diabetic Macular Edema in a Real-Life Setting
Munayco-Guillén F, Vazquez-Membrillo MA, Garcia-Roa MR, De La Cruz-Vargas JA, García-Perdomo HA, Pichardo-Rodriguez R
Clinical Ophthalmology 2023, 17:1129-1135
Published Date: 12 April 2023
Influence of Retinal Venous Pressure on Visual and Structural Outcomes in Eyes with Central Retinal Vein Occlusion Undergoing Anti-VEGF Treatment
Hidasa I, Yang KB, Zhang ML, Wang BY, Zhang GQ, Gao ZY, Liu ZY, Qi P, Xie J, Wang H, Liu L, Zhang H
Clinical Ophthalmology 2025, 19:2551-2563
Published Date: 1 August 2025