Back to Journals » Drug Design, Development and Therapy » Volume 20
Intravenous Sedation-Analgesia versus Local Anesthesia for Patient Comfort and Pain Control During Interventional Procedures: A Retrospective Cohort Study
Authors Zhang K, Yang G ![]() , Li L, Sang J, Tian J
, Li L, Sang J, Tian J ![]() , Chu Q, Wang B
, Chu Q, Wang B
Received 1 January 2026
Accepted for publication 4 April 2026
Published 9 April 2026 Volume 2026:20 592463
DOI https://doi.org/10.2147/DDDT.S592463
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Georgios Panos
Kaikai Zhang,1,* Guanyu Yang,2,* Liumei Li,2 Jing Sang,2 Jiayao Tian,3 Qinjun Chu,2 Bin Wang1
1Department of Interventional Operating Room, Zhengzhou Central Hospital Affiliated to Zhengzhou University, Zhengzhou, Henan, People’s Republic of China; 2Department of Anesthesiology and Perioperative Medicine, Zhengzhou Central Hospital Affiliated to Zhengzhou University, Zhengzhou, Henan, People’s Republic of China; 3The First Clinical Medical College, Lanzhou University, Lanzhou, Gansu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qinjun Chu, Department of Anesthesiology and Perioperative Medicine, Zhengzhou Central Hospital Affiliated to Zhengzhou University, Tongbai North Road 16, Zhengzhou, Henan, 450007, People’s Republic of China, Tel +86 13643711142, Email [email protected] Bin Wang, Department of Interventional Operating Room, Zhengzhou Central Hospital Affiliated to Zhengzhou University, Tongbai North Road 16, Zhengzhou, Henan, 450007, People’s Republic of China, Tel +86 13838580733, Email [email protected]
Objective: To compare the effects of intravenous sedation‑analgesia (IVSA) versus local anesthesia (LA) on patient‑reported intraoperative comfort and pain control during elective interventional procedures.
Methods: This single‑center retrospective cohort study included 1068 adults undergoing interventional procedures between January and March 2024. Patients self‑selected LA or IVSA (midazolam, sufentanil, ketorolac). Propensity score matching (PSM) was applied to balance baseline characteristics. Primary outcomes were patient‑reported comfort and maximum pain scores (0– 10 NRS). Operative time was also compared. After PSM, generalized estimating equation (GEE) models were used to compare outcomes. Sensitivity analyses included ordinal logistic regression and inverse probability weighting.
Results: After PSM, 336 patients were included in each group. The mean comfort score was 7.2 ± 1.2 in the IVSA group and 3.5 ± 1.2 in the LA group; the mean pain score was 3.4 ± 1.3 and 7.3 ± 1.2, respectively. Median operative time was 39.5 minutes in the IVSA group and 42.5 minutes in the LA group. GEE analysis showed that IVSA was independently associated with higher comfort scores (β = 3.69, 95% CI: 3.50– 3.88; P < 0.001) and lower pain scores (β = – 3.87, 95% CI: – 4.04 to – 3.70; P < 0.001), with no significant difference in operative time (geometric mean ratio = 0.965, 95% CI: 0.912– 1.020; P = 0.211). Sensitivity analyses yielded consistent results.
Conclusion: IVSA was associated with significantly higher intraoperative patient comfort and lower pain scores compared to LA alone, without a significant difference in procedure time, though it was associated with a higher incidence of transient adverse effects.
Keywords: conscious sedation, interventional radiology, pain management, patient satisfaction
Introduction
The widespread adoption of minimally invasive interventional procedures, such as coronary angiography, percutaneous coronary intervention, radiofrequency ablation, and transcatheter arterial chemoembolization, has transformed the management of cardiovascular and oncological diseases.1,2 While offering reduced trauma and faster recovery compared to open surgery, these procedures are not devoid of discomfort. Patients frequently experience significant pain—from vascular puncture, catheter manipulation, or prolonged immobilization—and considerable anxiety while remaining conscious throughout the operation.3
General anesthesia, though effective in eliminating awareness, is often considered resource-intensive for such procedures. It necessitates endotracheal intubation, mechanical ventilation, and post-anesthesia care, leading to increased operational costs, higher risks of complications, and reduced turnover efficiency, particularly in ambulatory settings.4,5 Consequently, its routine use for shorter interventional cases is limited. Local anesthesia (LA) alone, while simple and low-risk, may be insufficient in managing procedural pain and anxiety, potentially compromising patient comfort and procedural conditions.6 Ang et al reported that among patients undergoing femoral arterial sheath removal after percutaneous coronary intervention, those receiving only local lidocaine infiltration experienced mean pain scores of 4.1 ± 3.4 on a 0–10 scale, with 11.8% requiring additional analgesics and 9.8% experiencing vasovagal reactions.7
Intravenous sedation-analgesia (IVSA) has emerged as a balanced alternative, aiming to provide “conscious sedation” through low-dose drug combinations that offer synergistic analgesia and anxiolysis while preserving spontaneous respiration and patient cooperation.8,9 This approach aligns well with the workflow of interventional suites, characterized by rapid onset and recovery.10 At our institution, a patient-centered anesthesia strategy was implemented, allowing elective interventional patients to choose between LA alone or a standardized IVSA regimen based on their perceived pain sensitivity and anxiety.
With the growing emphasis on patient-centered care, patient-reported outcomes such as intraoperative comfort and pain have become increasingly important in evaluating the quality of procedural sedation.11,12 This is particularly relevant in interventional settings, where patients often remain awake during procedures and may require multiple treatment sessions. Despite its theoretical advantages, comparative real-world evidence on the impact of IVSA versus LA on patient-reported comfort, pain, and procedural efficiency during interventional procedures remains limited. Existing guidelines, such as those from the CIRSE and ASA,8,13 provide comprehensive recommendations for safe sedation practices but do not directly compare patient-centered outcomes between IVSA and LA in routine clinical settings. Furthermore, recent reviews on pain management in interventional oncology have highlighted significant heterogeneity in analgesic protocols and the lack of standardized approaches, underscoring the need for pragmatic evidence.14
Currently, available evidence consists primarily of safety guidelines and studies focusing on pharmacological interventions in specific populations.8,13,14 Several retrospective cohort studies have examined perioperative pain management in specific interventional oncology populations, such as patients undergoing radiofrequency ablation15 or transarterial chemoembolization,14 and systematic sedation protocols have been developed for abdominal interventions.16 However, direct comparisons of patient-reported outcomes between IVSA and LA across a broad range of interventional procedures remain lacking.
This retrospective cohort study aimed to compare the intraoperative comfort, pain experiences, and operative time of patients undergoing elective interventional procedures under either LA or IVSA at a single tertiary center, providing pragmatic evidence to inform anesthesia practice optimization.
Methods
Study Design and Setting
This was a single-center, retrospective cohort study conducted at Zhengzhou Central Hospital Affiliated to Zhengzhou University. The study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. The protocol was approved by the Medical Ethics Committee of Zhengzhou Central Hospital Affiliated to Zhengzhou University (ZXYY2025127) and registered in the Chinese Clinical Trial Registry (ChiCTR2500112289). This study was conducted in accordance with the principles of the Declaration of Helsinki. The requirement for informed consent was waived by the Medical Ethics Committee of Zhengzhou Central Hospital Affiliated to Zhengzhou University due to the retrospective nature of the study. All patient data were anonymized and handled with confidentiality to protect patient privacy.
Participants
We conducted a retrospective cohort study by screening the electronic medical records of adult patients aged ≥18 years with American Society of Anesthesiologists (ASA) physical status 1–3 who underwent elective interventional procedures under either LA or IVSA between January 1 and March 31, 2024. Patients undergoing procedures lasting less than 15 minutes were excluded. Additional exclusion criteria were pregnancy, chronic pain or long-term analgesic use (>3 months), multi-site procedures, documented psychiatric disorders (eg, schizophrenia, bipolar disorder, severe depression requiring hospitalization) or neurological disorders (eg, dementia, Parkinson’s disease, stroke with significant cognitive or motor impairment), and cases with missing or aberrant key data.
Rationale for the study period: The data for this analysis originated from a focused, three-month clinical practice evaluation period. During this time, the department systematically collected patient-reported intraoperative comfort and maximum pain scores (using the 0–10 Numerical Rating Scale [NRS]) for all procedures. This initiative was implemented not as a formal research protocol, but as a routine quality assessment to subjectively compare the emerging IVSA strategy against standard LA in real-world clinical practice. Consequently, this period provides a unique, internally consistent dataset where both anesthesia techniques were actively offered and their core patient-centered outcomes were uniformly documented. The concise timeframe minimizes confounding from long-term secular trends in technology, personnel, or perioperative protocols, thereby strengthening the internal validity of this retrospective comparison.
Anesthesia Protocols
Patients self-selected their anesthesia type preoperatively. During the preprocedural consultation, patients received standardized verbal and written information explaining the differences between LA and IVSA, including the anticipated level of sedation, potential benefits for pain and anxiety control, and possible risks (eg, respiratory depression, nausea). The final decision was made independently by the patient after discussion with the treating interventional radiologist, who provided guidance based on the procedural complexity and the patient’s clinical condition but did not direct the choice toward either option.
Patients in the LA group received only local infiltration anesthesia at the puncture site (eg, lidocaine) and remained awake throughout the procedure.
Patients in the IVSA group received, in addition to local anesthesia, a standardized regimen based on institutional practice and published evidence:7–9,14,15 midazolam (0.03 mg/kg), sufentanil (0.1 μg/kg), and ketorolac tromethamine (30 mg), administered intravenously to achieve conscious sedation while maintaining spontaneous respiration. Supplemental oxygen was provided via nasal cannula at 2–4 L/min.
All patients received standard monitoring (electrocardiography, non-invasive blood pressure, pulse oximetry) and had intravenous access established.
Data Collection
Data were extracted retrospectively from the hospital’s Electronic Medical Record and Anesthesia Information System. Two trained research assistants independently screened and extracted data using a standardized form. The collected covariates included demographic characteristics (sex, age, height, weight, body mass index [BMI]), ASA status, comorbidities (hypertension [HTN], diabetes mellitus [DM], coronary artery disease [CAD]), and type of interventional procedure. Procedures were categorized into five groups: 1) diagnostic angiography, 2) angioplasty/stent implantation, 3) oncologic interventional therapy, 4) electrophysiology and ablation, and 5) others.
Outcomes
The primary outcomes were: 1) patient-reported intraoperative comfort score, 2) patient-reported maximum intraoperative pain score, and 3) total operative time (from procedure start to end). Comfort and pain intensity were both assessed immediately post-procedure using a 0–10 NRS (0 = “Extremely uncomfortable”/“No pain”, 10 = “Extremely comfortable”/“Worst imaginable pain”). Nurses provided standardized pre-procedure instructions on scale use to ensure patients understood how to rate their comfort and pain accurately. Secondary outcomes included the incidence of intraoperative hypoxemia (SpO2 < 94%) and the incidence of nausea/vomiting.
Statistical Analysis
As a retrospective study encompassing all eligible cases within the specified period, no a priori sample size calculation was performed.
Continuous variables were assessed for normality using the Shapiro–Wilk test. Normally distributed data are presented as mean ± standard deviation and compared using independent t-tests; non-normally distributed data are presented as median (interquartile range) and compared using the Mann–Whitney U-test. Categorical variables are presented as counts (percentages) and compared using the chi-square or Fisher’s exact test.
To control for potential confounding, propensity score matching (PSM) was performed. Propensity scores were estimated using logistic regression with anesthesia type as the dependent variable and covariates (sex, age, height, weight, BMI, ASA status, comorbidities, and type of interventional procedure) as independent variables. A 1:1 nearest neighbor matching without replacement was applied with a caliper width of 0.2 standard deviations of the logit propensity score. Prior to matching, the distribution of propensity scores was plotted for both groups to assess overlap, and patients with propensity scores outside the common support region (ie, IVSA patients with scores below the minimum LA score, or LA patients with scores above the maximum IVSA score) were excluded from matching. The analysis estimated the average treatment effect on the treated, representing the effect of IVSA among patients who received it. Covariate balance before and after matching was assessed using standardized mean differences (SMD), with an SMD < 0.1 considered indicative of adequate balance.
After PSM, generalized estimating equation (GEE) analyses were performed with an exchangeable correlation structure, specifying matched pair as the clustering variable. For normally distributed continuous outcomes, linear GEE models with identity link were used. For skewed continuous outcomes, a gamma GEE model with log link was used. All models included anesthesia type as the primary independent variable and adjusted for age, BMI, sex, ASA status, comorbidities, and procedure type (Due to multicollinearity with BMI, height and weight were not included separately). Robust sandwich variance estimators were used to calculate standard errors. For binary outcomes (hypoxemia and nausea/vomiting), unadjusted ORs with 95% CIs were calculated.
Ordinal logistic regression was performed as a sensitivity analysis for the pain and comfort scores. These models treated the scores as ordered categorical variables and included the same covariates as the primary GEE models. Results are presented as regression coefficients (β) with 95% CIs and P values.
Inverse probability weighting (IPTW) was additionally performed as a sensitivity analysis using stabilized weights in the original cohort. Weighted GEE models with an exchangeable correlation structure were fitted for the primary outcomes, adjusting for the same covariates.
A complete-case analysis was performed, excluding patients with missing data for any of the variables included in the propensity score model or outcome assessments.
All analyses were performed using R software (version 4.3.0). A two-tailed P < 0.05 was considered statistically significant.
Results
Patient Cohort
From January to March 2024, a total of 2117 patients underwent interventional procedures at our center. After applying the predefined inclusion and exclusion criteria, 1068 patients were included in the final analysis. The detailed screening process is illustrated in Figure 1. Among the 2117 screened patients, 39 (1.8%) were excluded due to missing data. Missing values occurred in the outcome measures in 35 cases (comfort and pain scores) and in baseline covariates (height and/or weight) in 4 cases. The final unmatched cohort consisted of 337 patients in the LA group and 731 patients in the IVSA group. Baseline characteristics of the two groups are presented in Table 1. Before PSM, patients in the IVSA group had higher body weight (SMD = 0.220) and BMI (SMD = 0.274), a lower prevalence of HTN (SMD = 0.203) and CAD (SMD = 0.302), and a higher proportion of oncologic interventional therapy (SMD = 0.183). After PSM, these variables were well balanced, with all SMDs below 0.1, as shown in Table 1.
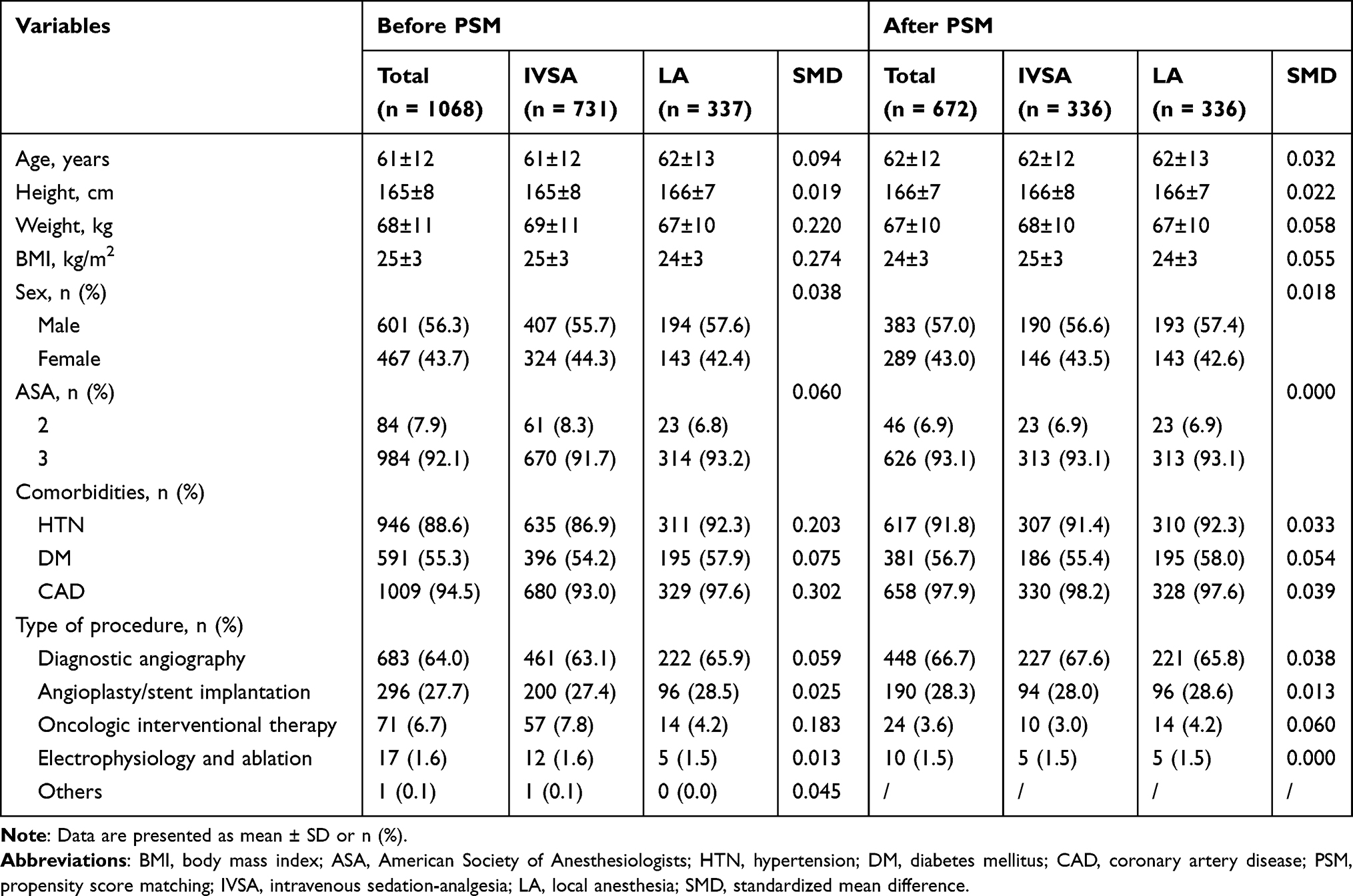 |
Table 1 Patient Characteristics Before and After PSM |
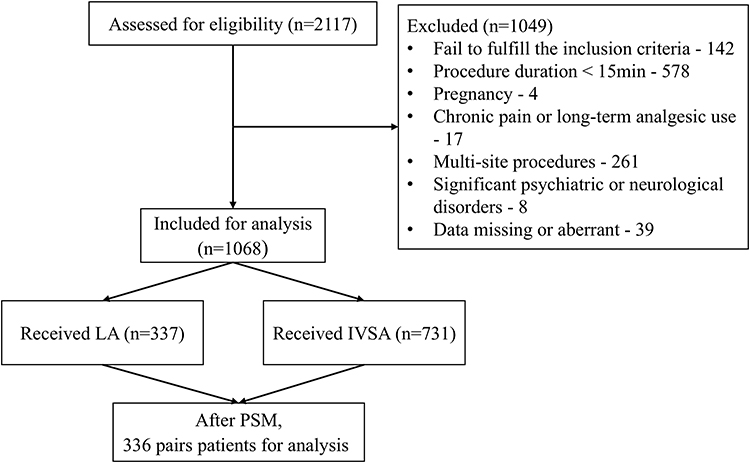 |
Figure 1 Flowchart of patient selection. |
Primary Outcomes
Descriptive summaries of the primary outcomes in the matched cohort are presented in Table 2. The mean comfort score was 7.2 ± 1.2 in the IVSA group and 3.5 ± 1.2 in the LA group; the mean pain score was 3.4 ± 1.3 and 7.3 ± 1.2, respectively. Median operative time was 39.5 minutes (IQR: 24–74) in the IVSA group and 42.5 minutes (IQR: 24–79) in the LA group. After adjusting for potential confounders using GEE models to account for matched-pair clustering, IVSA remained associated with significantly higher intraoperative comfort scores (β = 3.69, 95% CI: 3.50–3.88, P < 0.001) and significantly lower maximum pain scores (β = –3.87, 95% CI: –4.04 to –3.70, P < 0.001), whereas no significant difference in operative time was observed (geometric mean ratio = 0.965, 95% CI: 0.912–1.020, P = 0.211) (Table 3).
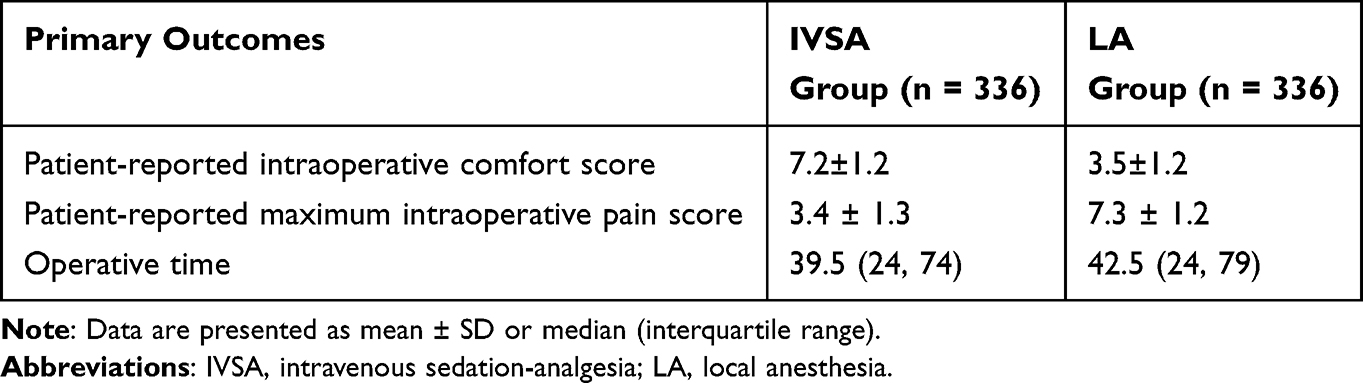 |
Table 2 Primary Outcomes in the Matched Cohort |
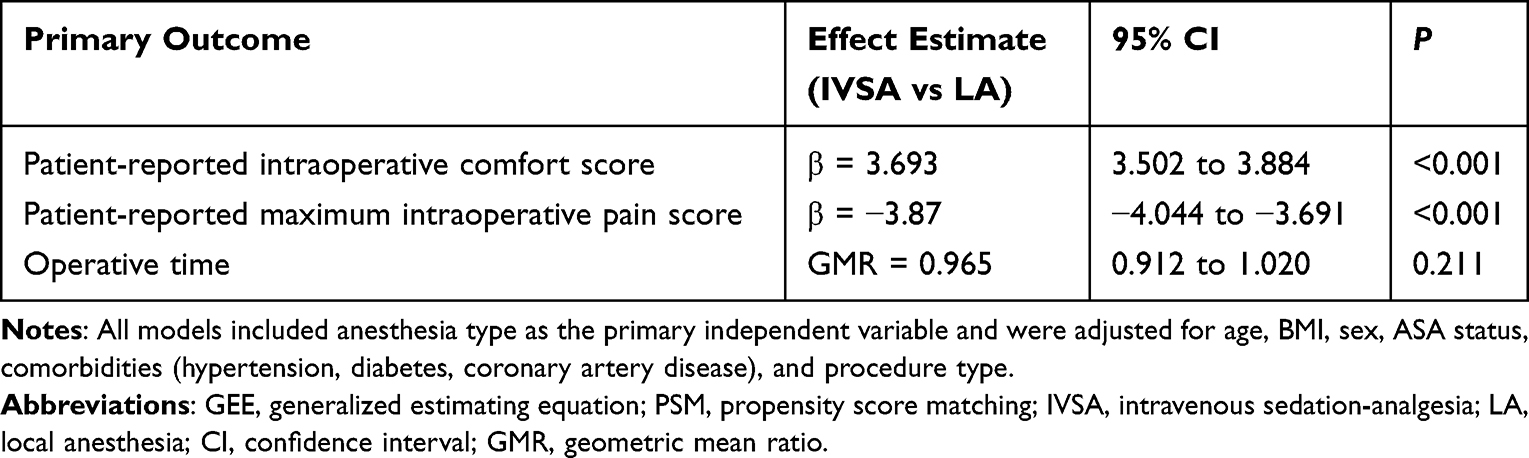 |
Table 3 Adjusted GEE Analysis of Primary Outcomes After PSM |
Secondary Outcomes
In the matched cohort, the incidence of intraoperative hypoxemia was significantly higher in the IVSA group than in the LA group (27 [8.0%] vs 3 [0.9%]; unadjusted OR = 9.70, 95% CI: 2.91–32.29, P < 0.001). The incidence of nausea/vomiting was also greater in the IVSA group (32 [9.5%] vs 8 [2.4%]; unadjusted OR = 4.32, 95% CI: 1.96–9.51, P < 0.001). Given the small number of events (27 for hypoxemia and 32 for nausea/vomiting), these unadjusted ORs should be interpreted with caution.
Sensitivity Analyses
Ordinal logistic regression analyses yielded results consistent with the primary GEE models. IVSA was associated with significantly lower pain scores (β = –6.686, 95% CI: –7.466 to –5.906, P < 0.001) and significantly higher comfort scores (β = 6.316, 95% CI: 5.592 to 7.041, P < 0.001) compared to LA. IPTW analysis also produced results consistent with the primary findings (Supplementary Table S1).
Discussion
In this retrospective cohort study comparing IVSA with LA in patients undergoing elective interventional procedures, we found that IVSA was associated with significantly higher patient‑reported intraoperative comfort scores and lower maximum pain scores, while no significant difference in operative time was observed. These results suggest that IVSA, as an intermediate strategy between LA and general anesthesia, can effectively enhance the patient experience without compromising procedural efficiency in a real‑world clinical setting.
Our most notable finding is the substantial difference in both comfort and pain scores observed between the IVSA and LA groups. The mean comfort score in the IVSA group (7.2) was more than double that in the LA group (3.5), and the pain score was less than half (3.4 vs. 7.3). This aligns with the growing body of evidence suggesting that procedural sedation may help alleviate anxiety and pain during minimally invasive interventions.17–19 Previous guidelines, such as the CIRSE standards,8 recommend sedation‑analgesia for procedures expected to cause significant discomfort or anxiety, a recommendation corroborated by our findings. The fact that operative time did not differ significantly between groups further strengthens the practical feasibility of IVSA, as a common concern with sedative techniques is potential prolongation of procedure duration.
Our findings align with these guidelines supporting sedation-analgesia,8,14 but also highlight that even with such regimens, a subset of patients may still experience significant discomfort. Lee et al reported that among patients undergoing radiofrequency ablation under intravenous pethidine with local lidocaine, 25% experienced severe pain (scores ≥8) and 22.8% required supplemental analgesics, with tumor location adjacent to the parietal peritoneum identified as an independent predictor.15 These findings highlight that individual patient and procedural factors influence analgesic requirements, underscoring the need for optimized multi-modal strategies such as the IVSA regimen evaluated in this study. However, direct comparisons between different IVSA regimens in interventional radiology remain limited, warranting further investigation.
Our study also objectively quantified the trade-offs associated with IVSA. As expected, the incidences of intraoperative hypoxemia (SpO2 < 94%) and nausea/vomiting were significantly higher in the IVSA group. These findings are largely attributable to the pharmacological properties of the agents used, particularly the respiratory depressant effect of the benzodiazepine-opioid combination and the emetogenic potential of sufentanil, although procedural factors may also contribute.20,21 Alternative regimens, including dexamethasone, parecoxib, or remifentanil as adjuncts or substitutes, have been explored to reduce side effects.14 Importantly, these adverse events were managed effectively under standard monitoring protocols; all hypoxemic episodes were transient and resolved with minimal intervention (eg, verbal stimulation or increased oxygen flow), and no serious sequelae were reported. When balanced against the substantial improvement in patient-reported comfort and pain, this risk profile appears clinically acceptable for the majority of patients undergoing elective interventions, provided that appropriate personnel, equipment, and protocols for sedation management are available.
Several limitations of our study must be acknowledged. First, its retrospective and single‑center design limits generalizability. Second, despite the use of PSM and regression adjustment, residual confounding due to unmeasured factors (eg, baseline anxiety levels, operator experience, or subtle differences in procedural complexity) cannot be ruled out. Patient self-selection of anesthesia may introduce selection bias, as those with higher anxiety or lower pain tolerance may have preferentially chosen IVSA; thus, the observed differences in comfort and pain scores may partly reflect patient preference rather than the analgesic modality itself. Third, the term “interventional procedures” in this study encompasses a broad range of interventions with varying levels of invasiveness and pain, which may limit the generalizability of our findings to specific procedural categories. Fourth, the patient‑reported outcomes were collected immediately post‑procedure and may be influenced by recall bias, and the amnestic effects of midazolam in the IVSA group may have led patients to underreport unpleasant intraoperative experiences, potentially overestimating the true benefit of IVSA compared to LA. Finally, the study period was relatively short, and we did not assess longer‑term outcomes such as patient satisfaction after full recovery or the incidence of delayed complications. Future studies with larger sample sizes should consider stratifying analyses by procedure type (eg, diagnostic angiography, angioplasty, oncologic interventions) to better understand how the benefits of IVSA may differ across clinical contexts, and incorporate more objective or standardized approaches for assessing comfort and pain, such as combined use of self-reported scales with behavioral observations or physiological parameters, to minimize potential bias.
Our study leaves several questions unanswered. For instance, while we assessed immediate intraoperative comfort and pain, the impact of IVSA on post‑procedure recovery metrics (eg, time to discharge, resumption of daily activities) and cost‑effectiveness remains unclear. Additionally, the optimal dosing regimen within the IVSA approach (eg, drug selection, titration protocols) for different types of interventions warrants further investigation. These gaps could be addressed in future prospective studies designed to collect a broader range of perioperative outcomes and incorporate economic evaluations.
The findings from this study carry important clinical implications. They provide real‑world evidence suggesting that IVSA may be a viable option for improving patient comfort during interventional procedures, supporting its broader integration into routine practice where resources allow. Based on our results, we hypothesize that standardized IVSA protocols could particularly benefit patients undergoing longer or more stimulating interventions (eg, oncologic interventional therapy, angioplasty), as well as those with high baseline anxiety or lower pain tolerance. Conversely, patients at increased risk for respiratory complications or those undergoing brief, low‑stimulation procedures might be adequately managed with LA alone. These considerations may help guide individualized anesthesia selection in clinical practice, though prospective validation is needed. We recommend that future research focus on multicenter, randomized controlled trials to confirm these findings and to refine patient selection criteria. Further studies could also explore the role of non‑pharmacological adjuncts (eg, virtual reality distraction) in combination with IVSA to further optimize the patient experience while minimizing pharmacological load.
Conclusion
In summary, this study found that IVSA was associated with significantly higher patient‑reported intraoperative comfort and lower pain scores compared to LA alone, with no significant difference in operative time. These findings suggest that IVSA may represent a valuable patient‑centered option, potentially offering greater benefits for patients undergoing more stimulating procedures or those with higher baseline anxiety. Further prospective studies are needed to confirm these associations and refine implementation protocols.
Trial Registration
Registered at the Chinese Clinical Trial Registry on November 12, 2025. Trial Registration Number: ChiCTR2500112289.
Data Sharing Statement
Datasets can be obtained from the corresponding author (Bin Wang) upon reasonable request, subject to ethical and legal restrictions.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Truffa MA, Alves GM, Bernardi F, et al. Does Ad Hoc coronary intervention reduce radiation exposure? - Analysis of 568 patients. Arq Bras Cardiol. 2015;105(5):487–9. doi:10.5935/abc.20150110
2. Li W, Yu Y, He H, et al. Urinary kidney injury molecule-1 as an early indicator to predict contrast-induced acute kidney injury in patients with diabetes mellitus undergoing percutaneous coronary intervention. Biomed Rep. 2015;3(4):509–512. doi:10.3892/br.2015.449
3. Li Z, Wang C, Li J, et al. MR-guided microwave ablation of hepatocellular carcinoma (HCC): is general anesthesia more effective than local anesthesia? BMC Cancer. 2021;21(1):562. doi:10.1186/s12885-021-08298-2
4. Sithole PA, Motshabi-Chakane P, Muteba MK. The characteristics and perioperative outcomes of children with orofacial clefts managed at an academic hospital in Johannesburg, South Africa. BMC Pediatr. 2022;22(1):214. doi:10.1186/s12887-022-03267-5
5. Green SM, Krauss B. Procedural sedation terminology: moving beyond “conscious sedation”. Ann Emerg Med. 2002;39(4):433–435. doi:10.1067/mem.2002.122770
6. Li X, Trerotola SO. Local anesthesia in interventional radiology. Semin Intervent Radiol. 2022;39(4):381–386. doi:10.1055/s-0042-1757342
7. Kiat Ang C, Leung DY, Lo S, French JK, Juergens CP. Effect of local anesthesia and intravenous sedation on pain perception and vasovagal reactions during femoral arterial sheath removal after percutaneous coronary intervention. Int J Cardiol. 2007;116(3):321–326. doi:10.1016/j.ijcard.2006.04.045
8. Romagnoli S, Fanelli F, Barbani F, et al. CIRSE standards of practice on analgesia and sedation for interventional radiology in adults. Cardiovasc Intervent Radiol. 2020;43(9):1251–1260. doi:10.1007/s00270-020-02536-z
9. Lee MJ, Fanelli F, Haage P, et al. Patient safety in interventional radiology: a CIRSE IR checklist. Cardiovasc Intervent Radiol. 2012;35(2):244–246. doi:10.1007/s00270-011-0289-5
10. Feldman A. Anesthesia and analgesia for interventional radiology. Tech Vasc Interv Radiol. 2025;28(2):101037. doi:10.1016/j.tvir.2025.101037
11. Zhou H, Yao M, Gu X, et al. Application of patient-reported outcome measurements in clinical trials in China. JAMA Network Open. 2022;5(5):e2211644. doi:10.1001/jamanetworkopen.2022.11644
12. Roper L, Belton J, Weinmann C, et al. Associations of baseline characteristics, patient-reported outcomes, and satisfaction with pain therapy with the patient’s global impression of change: a prospective cohort study. Br J Anaesth. 2026;136(4):1341–1348. doi:10.1016/j.bja.2026.01.010
13. Ractice P. Practice guidelines for moderate procedural sedation and analgesia 2018: a report by the American society of anesthesiologists task force on moderate procedural sedation and analgesia, the American association of oral and maxillofacial surgeons, American college of radiology, American dental association, American society of dentist anesthesiologists, and society of interventional radiology. Anesthesiology. 2018;128(3):437–479. doi:10.1097/ALN.0000000000002043
14. Zhang WZ, Chin KY, Zakaria R, Hassan NH. Strategies for pain management in hepatocellular carcinoma patients undergoing transarterial chemoembolisation: a scoping review of current evidence. Healthcare. 2025;13(9):994. doi:10.3390/healthcare13090994
15. Lee S, Rhim H, Kim YS, et al. Percutaneous radiofrequency ablation of hepatocellular carcinomas: factors related to intraprocedural and postprocedural pain. AJR Am J Roentgenol. 2009;192(4):1064–1070. doi:10.2214/AJR.08.1350
16. Skehan SJ, Malone DE, Buckley N, et al. Sedation and analgesia in adult patients: evaluation of a staged-dose system based on body weight for use in abdominal interventional radiology. Radiology. 2000;216(3):653–659. doi:10.1148/radiology.216.3.r00se09653
17. Bello C, Paisansathan C, Riva T, Luedi MM, Andereggen L. Anesthesia care in the interventional neuroradiology suite: an update. Curr Opin Anaesthesiol. 2022;35(4):457–464. doi:10.1097/ACO.0000000000001151
18. Bravo E, Tempesta D, Viault N. Improving Pre- and Post-IR procedure experience: what the anesthesiologists can offer. Cardiovasc Intervent Radiol. 2025;48(7):970–975. doi:10.1007/s00270-025-03960-9
19. Landrigan-Ossar M. Common procedures and strategies for anaesthesia in interventional radiology. Curr Opin Anaesthesiol. 2015;28(4):458–463. doi:10.1097/ACO.0000000000000208
20. Varshneya NB, Hassanien SH, Holt MC, et al. Respiratory depressant effects of fentanyl analogs are opioid receptor-mediated. Biochem Pharmacol. 2022;195:114805. doi:10.1016/j.bcp.2021.114805
21. Fakhri A, Ritvo A, Casarella J, Tang YL. Opioid use disorder and concurrent benzodiazepine use: clinical risks and management strategies. J Addict Dis. 2025;1–8. doi:10.1080/10550887.2025.2593244
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.