Back to Journals » Infection and Drug Resistance » Volume 15
Intrathecal or Intraventricular Tigecycline Therapy for Central Nervous System Infection Associated with Carbapenem-Resistant Klebsiella pneumoniae
Authors Du N, Mao EQ, Yang ZT ![]() , Qu HP, Qian X, Shi Y, Bian XL, He J
, Qu HP, Qian X, Shi Y, Bian XL, He J ![]() , Chen EZ
, Chen EZ
Received 30 August 2022
Accepted for publication 2 December 2022
Published 9 December 2022 Volume 2022:15 Pages 7219—7226
DOI https://doi.org/10.2147/IDR.S387346
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Ning Du,1 En-Qiang Mao,2 Zhi-Tao Yang,2 Hong-Ping Qu,3 Xian Qian,4 Ying Shi,5 Xiao-Lan Bian,6 Juan He,6,* Er-Zhen Chen2,*
1National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital & Shenzhen Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Shenzhen, People’s Republic of China; 2Emergency Intensive Care Unit, Ruijin Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 3Department of Critical Care Medicine, Ruijin Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 4Department of Pharmacy, Shanghai Eastern Hepatobiliary Surgery Hospital, Shanghai, People’s Republic of China; 5Department of Clinical Pharmacy, Shaoxing Hospital of Traditional Chinese Medicine, Zhejiang, People’s Republic of China; 6Department of Pharmacy, Ruijin Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Er-Zhen Chen, Emergency Intensive Care Unit, Ruijin Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China, Email [email protected] Juan He, Department of Pharmacy, Ruijin Hospital Affiliated to Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China, Email [email protected]
Purpose: Infection with carbapenem-resistant Klebsiella pneumoniae (CRKP) is a great challenge. Central nervous system (CNS) infection caused by CRKP is rarely reported, and effective treatment is limited. Thus, this study aimed to assess intrathecal (IT) or intraventricular (IVT) injection of tigecycline for clearing infection with CRKP in CNS.
Patients and Methods: Two patients who had intracranial infection with CRKP after craniotomy were treated in our institution and analyzed retrospectively, summarizing their therapeutic schedules.
Results: They all had a fever with the positive results of cerebrospinal fluid (CSF) test, and CSF culture showed positive for CPKP, which was sensitive only to tigecycline. In addition, the MIC of polymyxin B was not tested due to the limited laboratory conditions. After IT or IVT injection of tigecycline treatment, the temperature of the patients became normal in 3 days, with normal levels of white blood cells, protein, glucose and chlorine concentrations in the CSF. Crucially, twice CSF cultures also became negative with no clinical symptoms of intracranial infection after IT or IVT injection of tigecycline treatment. Moreover, there were no adverse drug reactions observed.
Conclusion: IT or IVT injection of tigecycline may be a bright choice to control intracranial infection with CRKP.
Keywords: central nervous system infection, CNS, carbapenem-resistant Klebsiella pneumoniae, CRKP, tigecycline, treatment
Introduction
Carbapenem-resistant Klebsiella pneumoniae (CRKP) has became a global threat in recent years, with high mortality associated with CRKP infection.1 It was reported that the mortality rates are as high as 33.24%, 46.71%, 50.06% and 44.82%, in North America, South America, Europe and Asia, respectively.2 Central nervous system (CNS) infection is one of the most severe complications of neurosurgery, and significantly aggravates the primary disease, especially healthcare-related meningitis and ventriculitis which were caused by CRKP.3 Tigecycline is one of the most important drugs for the treatment of CRKP infections.4 Previous reports mainly studied the effect of tigecycline on pulmonary infection, and skin and soft tissue infection, etc, only a few studies investigated the effect of tigecycline on CNS infection caused by Acinetobacter baumannii.5,6 Up to now, the effect of the drug on CRKP infections in CNS was rare reported.7 Herein, we reported two cases infected with CRKP in the CNS, who were cured by intrathecal (IT) or intraventricular (IVT) injection of tigecycline.
At present, rare relevant research has been reported yet on IT or IVT injection of tigecycline for treating CNS infections with CRKP.7
Case Presentation
Case 1: A female patient, 43 years old, had undergone removal of intracranial hematoma and decompressive craniectomy because of traffic accident. Ten days after the surgery (D10), she had a high fever of 39.5 °C, the blood test was performed immediately and the results showed white blood cells (WBC) were as high as 14.11×109/L with the proportion of neutrophils as high as 88%. Meanwhile, we performed lumbar puncture for her and the cerebrospinal fluid (CSF) was tested immediately. The results of CSF test revealed high WBC counts and protein concentration and low concentrations of glucose (Table 1). After 2 days, CRKP was reported form patients’ CSF cultures. Disk diffusion method was used for the susceptibility test of tigecycline because of the limited laboratory conditions. The results showed it was sensitive only to tigecycline with bacteriostatic circle of 19 mm (Table 2).8 Due to the limited laboratory conditions, the MIC of polymyxin B was not tested. But the blood culture was negative. Intracranial infection was diagnosed and meropenem (2g q8h IV) and tigecycline (50 mg q12h IV, loading dose 100mg) were administered intravenously combined with IT injection of tigecycline (2.5 mg q12h) for 14 days. On D20 and D26, results of CSF tests from repeated lumbar puncture returned to normal, and she recovered from fever and clinical symptoms of intracranial infection (Table 1). Therefore, we discontinued the antimicrobials. During the treatment period, she was effectively and safely treated without nephrotoxicity or seizures. Seven days later (D33), all of the therapies was stopped, and the patient recovered and discharged.
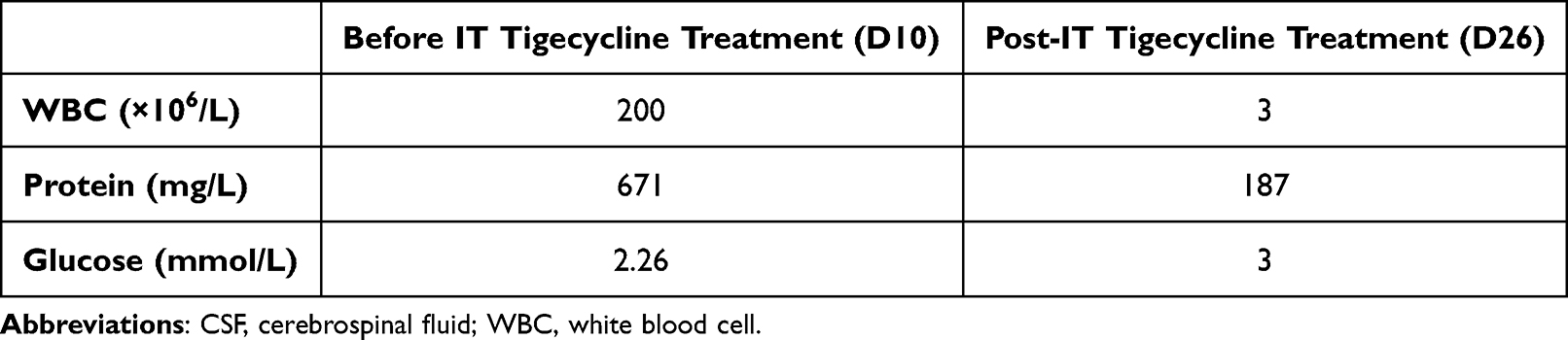 |
Table 1 CSF Test Results (Case 1) |
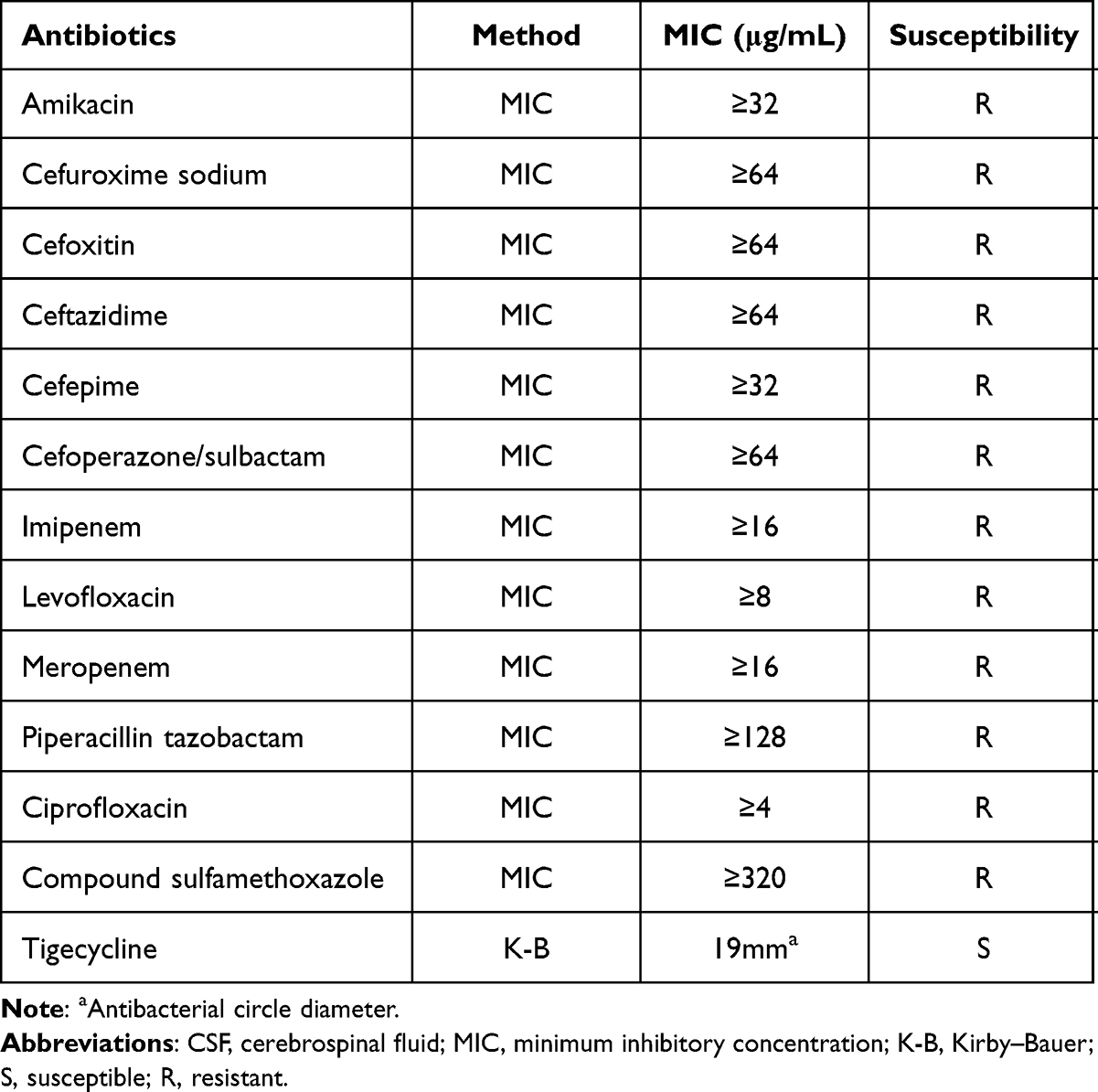 |
Table 2 Antibiotic Susceptibility Tests for Klebsiella pneumoniae in CSF of Case 1 |
Case 2: A male patient, 57 years old, was diagnosed with left frontal lobe contusion, left cerebellar contusion and subarachnoid hemorrhage because of traffic accident. Initially, we performed conservative treatment for him. On D3, computed tomography (CT) showed aggravation of left cerebral edema accompanied by diminished consciousness. Immediately, we placed a left ventricular drainage tube for him. From D15, he began to have fever with slightly turbid CSF. On D17, the temperature rose to 39°C. CSF test revealed WBC counts as high as 470×106/L, with high concentration of total protein and low glucose content of 1.7 mmol/L (Table 3). On D19, CSF culture indicated CRKP. We used disk diffusion method to test the susceptibility of tigecycline, and showed CRKP was sensitive to tigecycline with bacteriostatic circle of 19 mm (Table 4).8 MIC of polymyxin B was not tested because of the same reason mentioned above. Meanwhile, the blood microbial culture was negative. The patient was administered immediately with meropenem (2 g q8h IV) and tigecycline (50 mg q12h IV). However, his body temperature was still as high as 39°C for 3 days. Repeated analysis of CSF showed significantly abnormal results (Table 3). D24, repeated CSF test showed WBC count of 416×106/L, with high rate total protein of 1641 mg/L and glucose of 1.5 mmol/L (Table 3). On D25, CSF culture showed CRKP with the same drug sensitivity as before. Then, we stopped intravenous drip of tigecycline and used IVT injection of tigecycline (2.5 mg q12h) instead. Regimen of meropenem (2 g q8h IV) remained unchanged. The therapeutic schedule of IVT tigecycline was instituted with permission from members of the patient’s family. Seven days after the treatment (D32), the patient’s results of CSF test improved and the left ventricular drainage fluid became clear gradually (Table 3). On D39, the temperature, clinical symptoms and laboratory tests of CSF returned to normal (Table 3). More importantly, CSF culture got negative for three consecutive times. Therefore, we discontinued the antimicrobial therapy and the left ventricular drainage tube was removed. The patient recovered and discharged 1 week later. There were no adverse drug reactions observed during IVT injection of tigecycline.
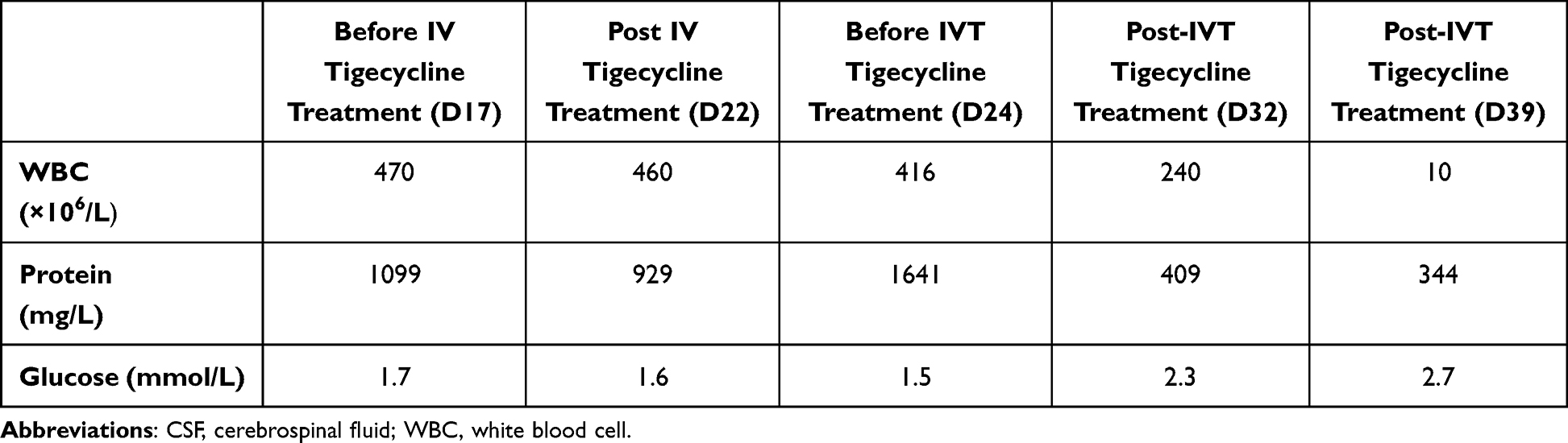 |
Table 3 CSF Test Results (Case 2) |
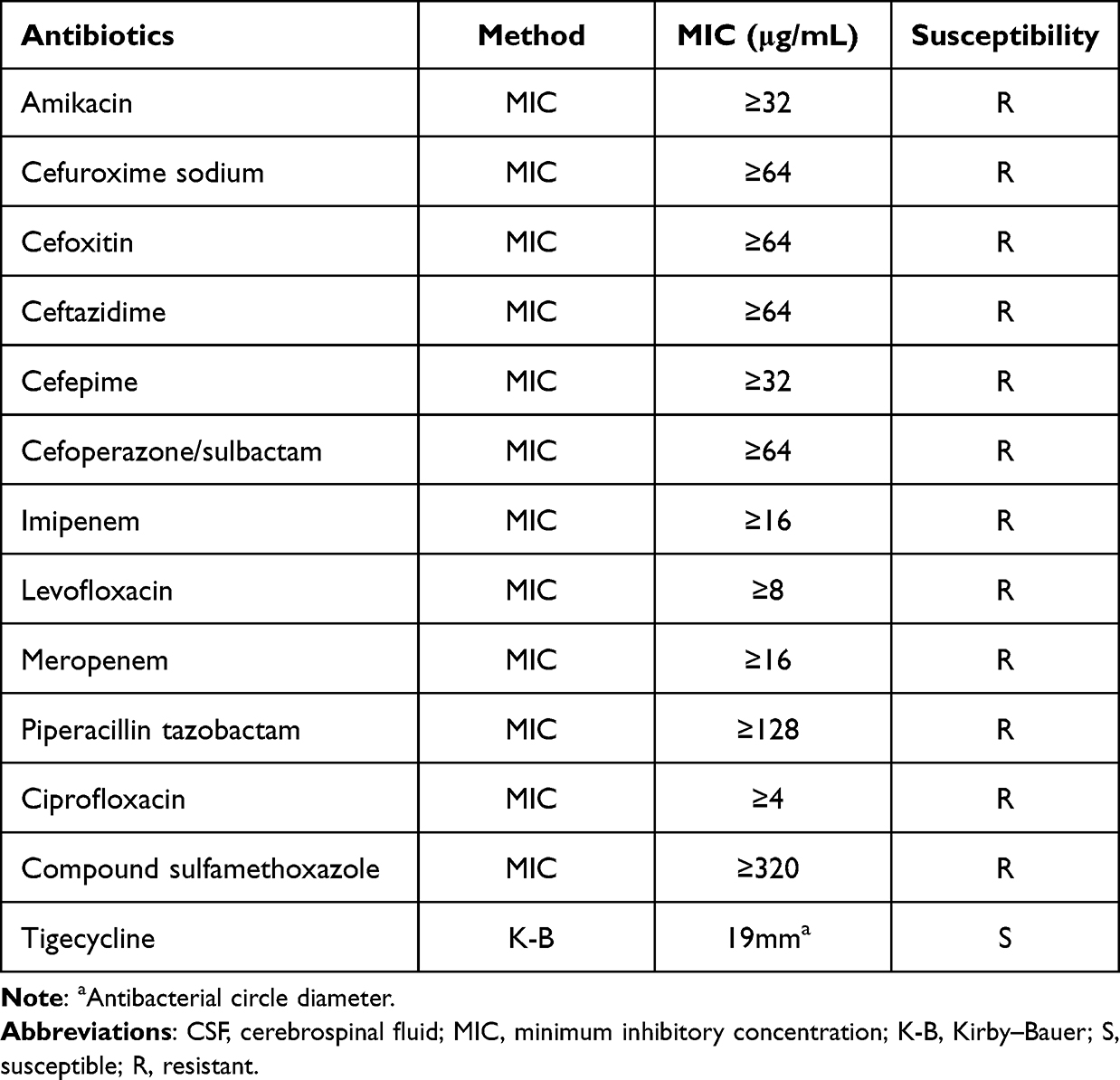 |
Table 4 Antibiotic Susceptibility Tests for Klebsiella pneumoniae in CSF of Case 2 |
Discussion
The spread of CRKP infection has become a worldwide challenge. It was reported that the mortality rate of CRKP infection is as high as 40% to 50%.9 In addition, rapid growth of bacterial resistance to imipenem and meropenem was found in recent years according to the CHINET data, because of the widespread use of carbapenems. The antibiotics for CNS infections with CRKP are very limited. Intracranial infections caused by Gram-negative bacilli have shown a significant upward trend in recent years.10 Based on the CHINET data published in 2020, Klebsiella pneumonia is one of the top five bacteria responsible for CSF infection.10 Intracranial infection of CRKP using IT or IVT tigecycline therapy was rarely reported so far. Here, we report the curative effect of intracranial tigecycline on the CNS infections caused by CRKP, through two cases.
Polymyxin B and tigecycline are now regarded as the last-line antibiotics especially for XDR gram-negative bacillus infections. However, it is difficult to penetrate into the brain for polymyxin B, unless intrathecally injected. However, intrathecally injection of polymyxin B could lead to high incidence of nephrological and neurological side effects. As reported previously, approximately 6–54% of the patients develop drug-related nephrotoxicity.11,12 Besides, polymyxins are associated with side effects including peripheral paresthesia, vertigo, visual disturbances, confusion, ataxia, and even neuromuscular blockade, which could lead to respiratory failure, even apnea. Other neurologic adverse reactions include psychosis, coma, convulsion, ptosis, diplopia, areflexia, dysphagia, and dysphonia, etc.13,14 These neurotoxicities are easily confused with the clinical symptoms found in patients with brain trauma, which increased difficulties in clinical differential diagnosis. Polymyxin B could even induce skin hyperpigmentation as reported by our previous study.15 Studies show that colistin might affect mitochondrial functions of nerve tissues, which induce mitochondrial dysfunction of nervous cells in mice.16 Further study demonstrated that polymyxin-induced neurotoxicity in neuroblastoma-2a (N2a) cells is related to inflammatory response partly regulated by IL-1β/p-IκB-α/NF-κB pathways.17 Due to the serious nephrological and neurological side effects of polymyxins and the drug was not available in the hospital, we are more preferred to use tigecycline for the treatment of XDR-bacterial infections for these two cases.
Tigecycline is a broad-spectrum antibiotic that inhibits gram-positive, gram-negative, and anaerobic bacteria that were common strains in CNS infections.18 In Europe and the United States, it had been approved for the treatment of complicated skin and skin structure infections as well as complicated intra-abdominal infection (cIAI).19 It has a favorable nervous system toxicity compared with polymyxin B.20 However, tigecycline hardly reaches the MIC in brain due to low penetration into blood–brain barrier (BBB).21 Compared with the plasma levels of tigecycline, the concentration is only 11% in the brain.20,22 Another study showed that the peak level of tigecycline in the CSF could reach 41% of plasma levels in patients with meningitis. Even then, at a dose of 50 mg q12h, the concentration is still too low for efficient treatment of meningitis.23 Additionally, tigecycline is a bacteriostatic agent. Considering the severity of CRKP intracranial infection and its poor prognosis above mentioned, we decided to use IT or IVT tigecycline for treatment of CRKP in CNS. We deemed that IT or IVT tigecycline was the main reason for the successful cure of the two patients. Hence, IT or IVT may be a potential method to cure CRKP intracranial infection.
The dose and the length of IT or IVT tigecycline is another key we have to consider. It has been reported that intrathecal or intraventricular tigecycline is effective on intracranial infection with multidrug-resistant Acinetobacter baumannii, Klebsiella pneumonia, and vancomycin-resistant Enterococci. These papers showed several treatment options for reference6,24–37 (Table 5). In these literatures, IT, IVT or continuous ventricular irrigation (CVI) of tigecycline was used for treating intracranial infection in adults and infants. Lauretti et al firstly reported IVT tigecycline for treatment of meningitis by XDR-Acinetobacter baumannii in 2017. Till now, there were only three papers on successful treatment of IVT tigecycline for treating XDR-Klebsiella pneumonia CNS infection, two for adults and one for infant. In our present study, besides IVT tigecycline, we also reported a successful experience of IT tigecycline for the treatment of CNS CRKP infection, for the first time. The dosage of intravenous injection commonly ranged from 50 mg to 100 mg twice daily in the label and literatures. The IT, IVT, or CVI dose of 2–20 mg/day was successfully used in adult and pediatric cases without any toxicity. The length of therapy was between 12 days and 78 days (Table 3). In our cases, the patients had undergone surgery operation and resulted in CNS infection with CRKP. In addition, the sensitive of the CRKP is poor, only sensitive to tigecycline. Finally, IT or IVT injection of 2.5 mg of tigecycline was administered twice a day for 14 days, based on the literature reports and the characteristics of pharmacokinetics and pharmacodynamics of tigecycline. Consequently, the temperature, routine tests and biochemistry indicators of the CSF were normal. Repeated CSF cultures were all negative after IT or IVT tigecycline treatment, and there were no side effects observed.
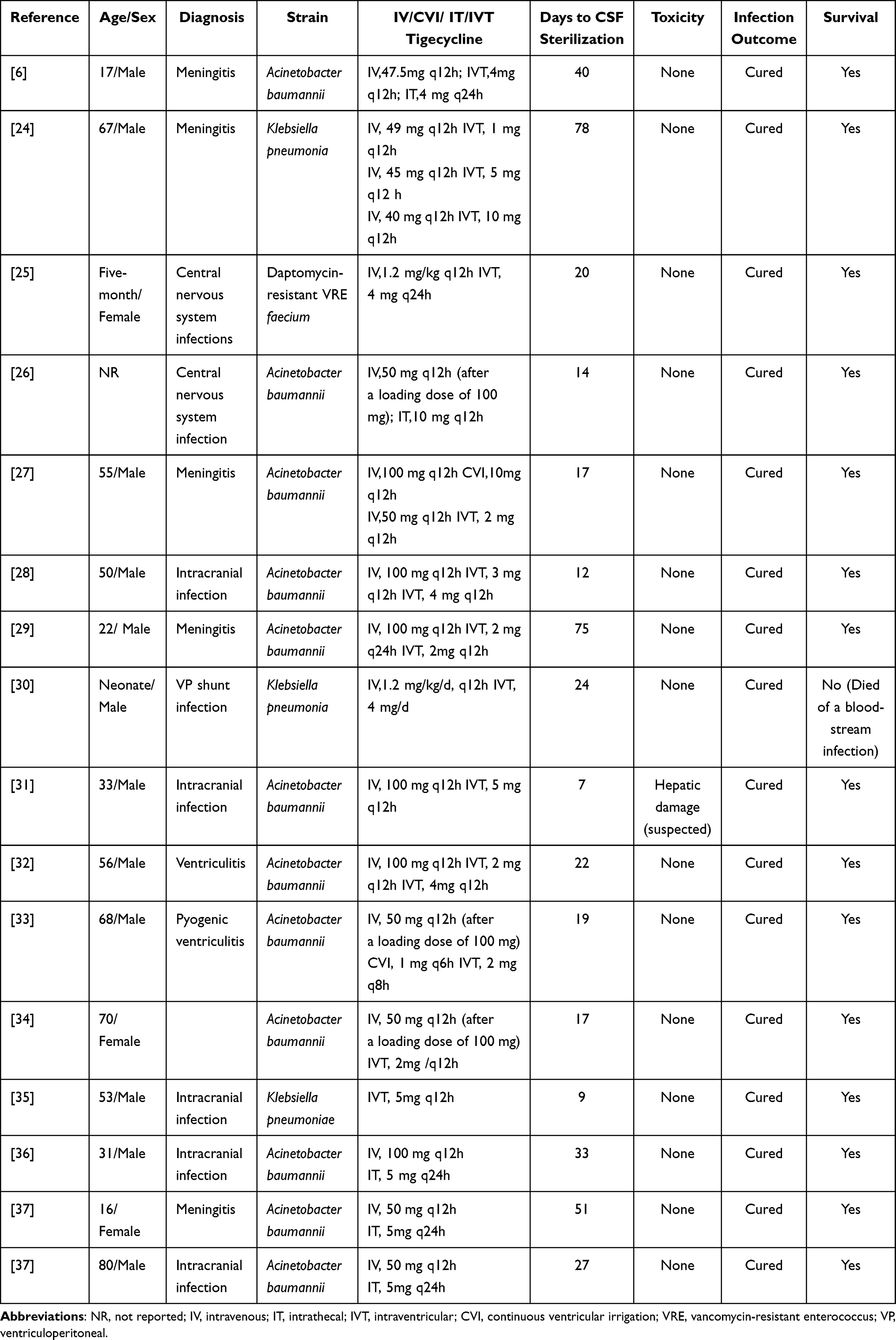 |
Table 5 Administration of Tigecycline in the Literatures |
The limitations of this study should be mentioned. Firstly, IT or IVT injection of tigecycline is off-label usage. Secondly, only two cases were assessed which were too limited to precisely estimate the effect of tigecycline in the CNS infection. Further prospective and well-designed clinical trials are required, especially with large samples, to further evaluate the therapeutic effects of tigecycline in patients with CRKP infection in the CNS.
Conclusion
It is a huge challenge to cure healthcare-related meningitis and ventriculitis which were caused by CRKP. Timely and effective surgical drainage and anti-infectious treatment are important measures to improve the efficacy and reduce the mortality of these patients. Due to poor prognosis and high mortality in CRKP intracranial infection, as well as too low penetration of commonly used antibiotics into BBB, IT or IVT tigecycline therapy may be an effective choice for the treatment of intracranial infection with CRKP, especially in the nowadays, the resistance rate of superbacteria to antimicrobials remains high.
Ethics Approval and Informed Consent
This study was approved by Ruijin Hospital Institutional Review Board and has been performed in accordance with the ethical standards laid down in “Declaration of Helsinki 1964” and its later amendments or comparable ethical standards. Two patients were enrolled in the study and informed consent forms were signed by the patients.
Acknowledgments
The authors thank the staff of the EICU Department of Ruijin Hospital affiliated to Medical School of Shanghai Jiao Tong University for their facilities and collaboration.
Funding
This study was supported by the National Natural Science Foundation of China (Grant No. 81772107 and 81571931). This study was also funded by the Important and weak discipline construction plan for health and family planning system of Shanghai (No.2016ZB0206), and Project of three-year plan to promote clinical skills and innovation ability of Municipal Hospitals (No.SHDC2020CR1028B).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Ripabelli G, Sammarco ML, Salzo A, Scutella M, Felice V, Tamburro M. New Delhi metallo-beta-lactamase (NDM-1)-producing Klebsiella pneumoniae of sequence type ST11: first identification in a hospital of central Italy. Lett Appl Microbiol. 2020;71(6):652–659. doi:10.1111/lam.13384
2. Xu L, Sun X, Ma X. Systematic review and meta-analysis of mortality of patients infected with carbapenem-resistant Klebsiella pneumoniae. Ann Clin Microbiol Antimicrob. 2017;16(1):18. doi:10.1186/s12941-017-0191-3
3. McGill F, Heyderman RS, Panagiotou S, Tunkel AR, Solomon T. Acute bacterial meningitis in adults. Lancet. 2016;388(10063):3036–3047. doi:10.1016/S0140-6736(16)30654-7
4. Chiu SK, Chan MC, Huang LY, et al. Tigecycline resistance among carbapenem-resistant Klebsiella pneumoniae: clinical characteristics and expression levels of efflux pump genes. PLoS One. 2017;12(4):e0175140. doi:10.1371/journal.pone.0175140
5. Tasina E, Haidich AB, Kokkali S, Arvanitidou M. Efficacy and safety of tigecycline for the treatment of infectious diseases: a meta-analysis. Lancet Infect Dis. 2011;11(11):834–844. doi:10.1016/S1473-3099(11)70177-3
6. Deng ZW, Wang J, Qiu CF, Yang Y, Shi ZH, Zhou JL. A case report of intraventricular and intrathecal tigecycline infusions for an extensively drug-resistant intracranial Acinetobacter baumannii infection. Medicine. 2019;98(15):e15139. doi:10.1097/MD.0000000000015139
7. Li J, Liu Y, Wu G, Wang H, Xu X. Intravenous plus intraventricular tigecycline-amikacin therapy for the treatment of carbapenem-resistant Klebsiella pneumoniae ventriculitis: a case report. Medicine. 2022;101(30):e29635. doi:10.1097/MD.0000000000029635
8. Humphries R, Bobenchik AM, Hindler JA, Schuetz AN. Overview of changes to the clinical and laboratory standards institute performance standards for antimicrobial susceptibility testing, M100, 31st edition. J Clin Microbiol. 2021;59(12):e0021321. doi:10.1128/JCM.00213-21
9. Band VI, Satola SW, Burd EM, Farley MM, Jacob JT, Weiss DS. Carbapenem-resistant Klebsiella pneumoniae exhibiting clinically undetected colistin heteroresistance leads to treatment failure in a murine model of infection. mBio. 2018;9(2):e02448.
10. Hu F, Wang M, Zhu D, Wang F . CHINET efforts to control antimicrobial resistance in China. J Glob Antimicrob Resist. 2020;21:76–77. doi:10.1016/j.jgar.2020.03.007
11. Lim LM, Ly N, Anderson D, et al. Resurgence of colistin: a review of resistance, toxicity, pharmacodynamics, and dosing. Pharmacotherapy. 2010;30(12):1279–1291. doi:10.1592/phco.30.12.1279
12. Mendes CA, Cordeiro JA, Burdmann EA. Prevalence and risk factors for acute kidney injury associated with parenteral polymyxin B use. Ann Pharmacother. 2009;43(12):1948–1955. doi:10.1345/aph.1M277
13. Lindesmith LA, Baines RD
14. Wolinsky E, Hines JD. Neurotoxic and nephrotoxic effects of colistin in patients with renal disease. N Engl J Med. 1962;266(15):759–762. doi:10.1056/NEJM196204122661505
15. Zheng G, Cao L, Che Z, Mao E, Chen E, He J. Polymyxin B-induced skin hyperpigmentation: a rare case report and literature review. BMC Pharmacol Toxicol. 2018;19(1):41. doi:10.1186/s40360-018-0226-1
16. Dai C, Li J, Li J. New insight in colistin induced neurotoxicity with the mitochondrial dysfunction in mice central nervous tissues. Exp Toxicol Pathol. 2013;65(6):941–948. doi:10.1016/j.etp.2013.01.008
17. Dai C, Ciccotosto GD, Cappai R, et al. Curcumin attenuates colistin-induced neurotoxicity in N2a cells via anti-inflammatory activity, suppression of oxidative stress, and apoptosis. Mol Neurobiol. 2018;55(1):421–434. doi:10.1007/s12035-016-0276-6
18. Kaewpoowat Q, Ostrosky-Zeichner L. Tigecycline: a critical safety review. Expert Opin Drug Saf. 2015;14(2):335–342. doi:10.1517/14740338.2015.997206
19. Rodriguez-Bano J, Gutierrez-Gutierrez B, Machuca I, Pascual A. Treatment of infections caused by extended-spectrum-beta-lactamase-, AmpC-, and carbapenemase-producing Enterobacteriaceae. Clin Microbiol Rev. 2018;31(2). doi:10.1128/CMR.00079-17
20. Pankey GA. Tigecycline. J Antimicrob Chemother. 2005;56(3):470–480. doi:10.1093/jac/dki248
21. Tattevin P, Solomon T, Brouwer MC. Understanding central nervous system efficacy of antimicrobials. Intensive Care Med. 2019;45(1):93–96. doi:10.1007/s00134-018-5270-1
22. Rodvold KA, Gotfried MH, Cwik M, Korth-Bradley JM, Dukart G, Ellis-Grosse EJ. Serum, tissue and body fluid concentrations of tigecycline after a single 100 mg dose. J Antimicrob Chemother. 2006;58(6):1221–1229. doi:10.1093/jac/dkl403
23. Lengerke C, Haap M, Mayer F, et al. Low tigecycline concentrations in the cerebrospinal fluid of a neutropenic patient with inflamed meninges. Antimicrob Agents Chemother. 2011;55(1):449–450. doi:10.1128/AAC.00635-10
24. Wu Y, Chen K, Zhao J, Wang Q, Zhou J. Intraventricular administration of tigecycline for the treatment of multidrug-resistant bacterial meningitis after craniotomy: a case report. J Chemother. 2018;30(1):49–52. doi:10.1080/1120009X.2017.1338846
25. Sahin A, Dalgic N. Intraventricular plus intravenous tigecycline for the treatment of daptomycin nonsusceptible vancomycin-resistant enterococci in an infant with ventriculoperitoneal shunt infection. World Neurosurg. 2019;130:470–473. doi:10.1016/j.wneu.2019.07.045
26. Wang L, Zhang J, Yu X, et al. Intrathecal injection of tigecycline in treatment of multidrug-resistant Acinetobacter baumannii meningitis: a case report. Eur J Hosp Pharm. 2017;24(3):182–184. doi:10.1136/ejhpharm-2016-000972
27. Long W, Yuan J, Liu J, et al. Multidrug resistant brain abscess due to Acinetobacter baumannii ventriculitis cleared by intraventricular and intravenous tigecycline therapy: a case report and review of literature. Front Neurol. 2018;9:518. doi:10.3389/fneur.2018.00518
28. Fang YQ, Zhan RC, Jia W, Zhang BQ, Wang JJ. A case report of intraventricular tigecycline therapy for intracranial infection with extremely drug resistant Acinetobacter baumannii. Medicine. 2017;96(31):e7703. doi:10.1097/MD.0000000000007703
29. Lauretti L, D’Alessandris QG, Fantoni M, et al. First reported case of intraventricular tigecycline for meningitis from extremely drug-resistant Acinetobacter baumannii. J Neurosurg. 2017;127(2):370–373. doi:10.3171/2016.6.JNS16352
30. Curebal B, Dalgic N, Bayraktar B. Intraventricular tigecycline for the treatment of shunt infection: a case in pediatrics. J Neurosurg Pediatr. 2018;23(2):247–250. doi:10.3171/2018.9.PEDS18470
31. Zhong L, Shi XZ, Su L, Liu ZF. Sequential intraventricular injection of tigecycline and polymyxin B in the treatment of intracranial Acinetobacter baumannii infection after trauma: a case report and review of the literature. Mil Med Res. 2020;7(1):23. doi:10.1186/s40779-020-00253-9
32. Abdallah M, Alsaleh H, Baradwan A, et al. Intraventricular tigecycline as a last resort therapy in a patient with difficult-to-treat healthcare-associated Acinetobacter baumannii ventriculitis: a case report. SN Compr Clin Med. 2020;2(9):1683–1687. doi:10.1007/s42399-020-00433-7
33. Li W, Li DD, Yin B, Lin DD, Sheng HS, Zhang N. Successful treatment of pyogenic ventriculitis caused by extensively drug-resistant Acinetobacter baumannii with multi-route tigecycline: a case report. World J Clin Cases. 2021;9(3):651–658. doi:10.12998/wjcc.v9.i3.651
34. Liu Y, Pu Z, Zhao M. Case report of successful treatment of extensively drug-resistant Acinetobacter baumannii ventriculitis with intravenous plus intraventricular tigecycline. Antimicrob Agents Chemother. 2018;62(11). doi:10.1128/AAC.01625-18
35. Wang H, Zhou Q, Huang K, Yang X, Wen L. Intraventricular plus systemic antibiotic therapy for treating polymyxin-resistant Klebsiella pneumoniae ventriculitis: a case report. Open Forum Infect Dis. 2022;9(4):ofac084. doi:10.1093/ofid/ofac084
36. Li Z, An Y, Li L, Yi H. Intrathecal injection of tigecycline and polymyxin B in the treatment of extensively drug-resistant intracranial Acinetobacter baumannii infection: a case report and review of the literature. Infect Drug Resist. 2022;15:1411–1423. doi:10.2147/IDR.S354460
37. Huang G, Lai W, Wu D, Huang Q, Zhong Q, Ye X. Two cases report of intrathecal tigecycline therapy for intracranial infection with Acinetobacter baumannii and review of literatures. Infect Drug Resist. 2022;15:2211–2217. doi:10.2147/IDR.S357087
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.