Back to Journals » Local and Regional Anesthesia » Volume 16
Intrathecal Morphine versus Morphine-Dexmedetomidine Combination for Postoperative Pain Control After Total Knee Replacement: A Randomized Controlled Trial
Authors Omara AF ![]() , Mohsen HH, Mohammed Abo Hagar A
, Mohsen HH, Mohammed Abo Hagar A ![]() , Abdelrahman AF
, Abdelrahman AF ![]()
Received 1 May 2023
Accepted for publication 24 July 2023
Published 2 August 2023 Volume 2023:16 Pages 113—122
DOI https://doi.org/10.2147/LRA.S419465
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Stefan Wirz
Amany F Omara,1 Hadal Hassan Mohsen,2 Alaa Mohammed Abo Hagar,1 Ahmed F Abdelrahman1
1Department of Anaesthesia and Surgical Intensive Care, Faculty of Medicine, Tanta University, Tanta, Egypt; 2Department of Anaesthesia and Surgical Intensive Care, Faculty of Medicine, Ain Shams University, Ciro, Egypt
Correspondence: Amany F Omara, Department of Anaesthesia and Surgical Intensive Care, Faculty of Medicine, Tanta University, Tanta, 31527, Egypt, Tel +201008372249, Email [email protected]; [email protected]
Objective: This prospective study aimed to compare the analgesic efficacy and adverse effects of intrathecal morphine, dexmedetomidine, and a combination of both in patients undergoing total knee replacement (TKR).
Patients and Methods: This randomized prospective study was carried out in Tanta university hospital in orthopedic surgery for 6 months on 105 adult patients with American Society of Anesthesiologists Physical Status Class II and III, aged > 50 years, and scheduled for total knee replacement surgery randomly allocated into morphine group received 0.5% heavy bupivacaine plus 0.1 mg of morphine, morphine/ dexmedetomidine group, received 0.5% heavy bupivacaine plus 0.1 mg of morphine and 5 mcg of dexmedetomidine and dexmedetomidine group received 0.5% heavy bupivacaine plus 5 mcg of dexmedetomidine. The time of the first required analgesia, postoperative pain severity, the total dose of morphine, postoperative complication, and the patient’s level of sedation were recorded.
Results: About half of the patients in the dexmedetomidine group requested first rescue analgesia 6 hours after the operation, significantly shorter than the other two groups. On the other hand, the other two groups show no significant difference between them regarding the first required analgesia. At rest, the dexmedetomidine group have significantly higher VAS with a significant increase in patients who required morphine as rescue analgesia than the other two groups. While at movement, patients in the dexmedetomidine group felt pain at 4 hrs postoperatively with significantly higher VAS than the other two groups. At the same time, the sedation score was significantly lower in the dexmedetomidine group than in the other two groups. 22.2% of cases in the morphine group developed nausea and vomiting with a significant difference between the three groups.
Conclusion: Despite the absence of substantial side effects, our findings did not suggest enhanced analgesia with the combination of intrathecal morphine and dexmedetomidine.
Keywords: dexmedetomidine, intrathecal, morphine, pain, total knee replacement
Introduction
One of the most painful orthopedic surgery procedures is total knee replacement. Total knee replacement patients are typically older and have limited cardiac and pulmonary reserves. The increased susceptibility of elderly patients to medications necessitates the use of postoperative analgesic agents and procedures with few adverse effects.1
The spinal cord is a vital neuronal component in the transmission of pain. Local opioids, norepinephrine, and serotonin all reduce nociception.2 The interplay of these systems in the spinal cord may influence anti-nociception. Opioids injected intravenously or epidurally are commonly used to treat postoperative and chronic nociceptive pain caused by cancer.3
Although intravenous morphine injection to provide postoperative analgesia during the first 24 hours after surgery is a widely used technique,4 opioid therapy is limited due to side effects (hypotension, pruritus, nausea, urinary retention, respiratory depression) and intolerance.5
The pharmacologic properties of alpha-2 adrenergic agonists (clonidine and dexmedetomidine) (sedation, hypnosis, anxiolysis, sympatholytic, and analgesia) make them appropriate as adjuvants to multimodal analgesia.6
Intrathecal dexmedetomidine combined with spinal bupivacaine prolongs the sensory block by suppressing C-fiber transmitter release and hyperpolarizing post-synaptic dorsal horn neurons, whereas the binding of 2-adrenoceptor agonists to motor neurons in the dorsal horn may prolong the motor block of spinal anesthetics.7
The reason for combining analgesics with similar therapeutic effects or synergistic interactions is to increase analgesic efficacy while decreasing adverse effects by allowing each agent’s dose to be reduced.8,9 There have been limited human investigations on the antinociceptive effects of co-administered intrathecal morphine (ITM) and dexmedetomidine in postoperative pain.
We expected that adding dexmedetomidine to ITM would improve perioperative pain control while reducing the negative effects of postoperative systemic opioid use. The purpose of this study was to compare the analgesic efficacy and adverse effects of a combination of intrathecal morphine and dexmedetomidine with either medication alone in total knee replacement (TKR) patients. The primary outcome was the first-time analgesia was requested, which was defined as the onset of pain with a VAS 4 within 24 hours of intrathecal injection. The secondary outcomes included the amount of additional analgesia needed, the severity of postoperative pain within 24 hours after surgery, and postoperative complications.
Patients and Methods
This randomized prospective study was carried out in Tanta university hospital in orthopedic surgery for 6 months on 105 adult patients with American Society of Anesthesiologists (ASA) Physical Status Class I and II, aged > 50 years, and scheduled for total knee replacement surgery after approval from the institutional ethics committee at 1/6/2022 with ID; 35525/6/22. This study registered in a clinical trial. Gov. on June 30, 2022, with a unique registration number; NCT05439564. This study complies with the Declaration of Helsinki.
Patients with bleeding disorders, heart, liver, or renal failure, systemic infections or infections of their injection sites, patients with a known allergy to study, those with 2nd or 3rd-degree heart block, or with low back pain or other back problems, or a history of drug or alcohol abuse, patients with BMI > 30 kg/m2, and patients with psychiatric illnesses that would interfere with perception and assessment of pain were excluded from the study.
After informed consent was obtained from all participants, all patients were assessed by history taking, physical examination, and laboratory evaluation. Noninvasive blood pressure (NIBP), electrocardiogram (ECG), end-tidal carbon dioxide (ETCO2), and pulse oximetry were all monitored when the patients arrived in the operating room, and baseline values for systolic blood pressure (SBP), diastolic blood pressure (DBP), heart rate (HR), and arterial oxygen saturation were also recorded. An intravenous (IV) line was placed, and 0.9% normal saline was administered. All patients were given 2 liters of oxygen per minute using a nasal cannula. The patients were given 0.02 mg/kg midazolam as a premedication.
The patients were placed in postures, and the skin was sterilized. Local anesthetic with 1.0 mL of 2% lidocaine was administered at the L3-L4 or L4-L5 interspaces. The 105 patients were then randomly assigned to one of three equal groups (35 patients each): Randomization was performed using the sealed opaque envelope technique; each patient randomly selected a sealed envelope containing a group number in which the patient was enrolled. Morphine group (35 patients): 0.5% heavy bupivacaine (3.5 mL) + 0.1 mg morphine was administered. Patients in the morphine-DEX group received 0.5% heavy bupivacaine (3.5 mL), 0.1 mg morphine, and 5 mcg dexmedetomidine. Patients in the DEX group received 0.5% heavy bupivacaine (3.5 mL) and 5 mcg dexmedetomidine.
Dose finding studies suggest that the optimal dose for morphine in total hip arthroplasty is 100 mcg, providing effective analgesia for up to 21 hrs.10 This dose appears to be at the upper end of the dose–response curve with lower doses lacking equivalent analgesic efficacy and higher doses increasing the incidence of side effects. Al – Ghanem et al’s study concluded that 5mcg dexmedetomidine seems to be an alternative as an adjuvant to spinal bupivacaine in surgical procedures, especially in those who need quite a long time with minimal side effects and excellent quality of analgesia.11
A nurse who was not involved in the study observation or data collection prepared the drugs and labeled them. The study medications were delivered intravenously based on group assignment. The patient assignment was concealed from the attending anesthesiologist, surgeon, and patient caregiver or data collection professionals.
Age, BMI, ASA status, duration of surgery, intraoperative systolic blood pressure (SBP), diastolic blood pressure (DBP), and heart rate (HR) were recorded for all patients at the 1st, 5th, 15th, 30th, and 60th minutes. The time of first request of analgesia was defined as the onset of pain with VAS ≥ 4 within 24 hours after intrathecal injection and Postoperative pain severity were assessed by VAS for pain at rest and movement (ranging from 0 to 10, with 0 being no pain and 10 being maximum pain) and patients with VAS 4 were given 3 mg morphine IV which can be repeated every 4 hrs (maximum 20 mg morphine/ day), and those with VAS 3 were given an intravenous infusion of Diclofenac Na (75mg) every 8 hours in all groups (as routine treatment) was recorded in all groups.
The required dose of morphine was used postoperatively, as well as any recorded postoperative complication as sedation, nausea and vomiting, and respiratory depression, and the patient’s level of sedation was assessed at the same time points using Ramsay Sedation Scale (score 3–4 mean adequate sedation) postoperatively12 was reported.
Statistical Analysis
The World Health Organization and the Centers for Disease Control and Prevention’s Epi-Info software statistical tool, version 2002, was used to compute sample size and power analyses. The criteria used for sample size calculation were a 95% confidence limit, 80% power of the study, and the estimated first time an analgesic request is made in 90% of the treatment group with the expected favorable outcome being twice that of 60% of the least favorable treatment group. The sample size was determined to be number>33 in each group based on the previously described parameters, with a 95% confidence limit, and 80% power of the study, to account for incomplete results, the researcher expanded the sample size to 35.
Data was entered into the computer and analyzed with the IBM SPSS software program version 20.0. IBM Corporation, Armonk, New York. Numbers and percentages were used to represent categorical data. The Chi-square test was used to compare three groups. When more than 20% of the cells had an expected count of less than 5, the Monte Carlo adjustment test was used. The Shapiro–Wilk test was used to determine the normality of continuous data. For regularly distributed quantitative variables, quantitative data were expressed as a range (minimum and maximum), mean, standard deviation, and median. For comparing the three examined groups, a one-way ANOVA test was employed, followed by a Post Hoc test (Tukey) for pairwise comparison. For non-regular quantitative variables, the Kruskal Wallis test was used to compare distinct groups, followed by the Post Hoc test (Dunn’s for multiple comparisons test) for pairwise comparison. The obtained results were declared significant at the 5% level.
Results
One hundred forty cases were recruited in this study, 35 of them were excluded due to (15 patients refusing to participate and 20 not meeting inclusion criteria). The remaining 105 cases were randomly assigned to three groups (35 patients in each group) as shown in Figure 1.
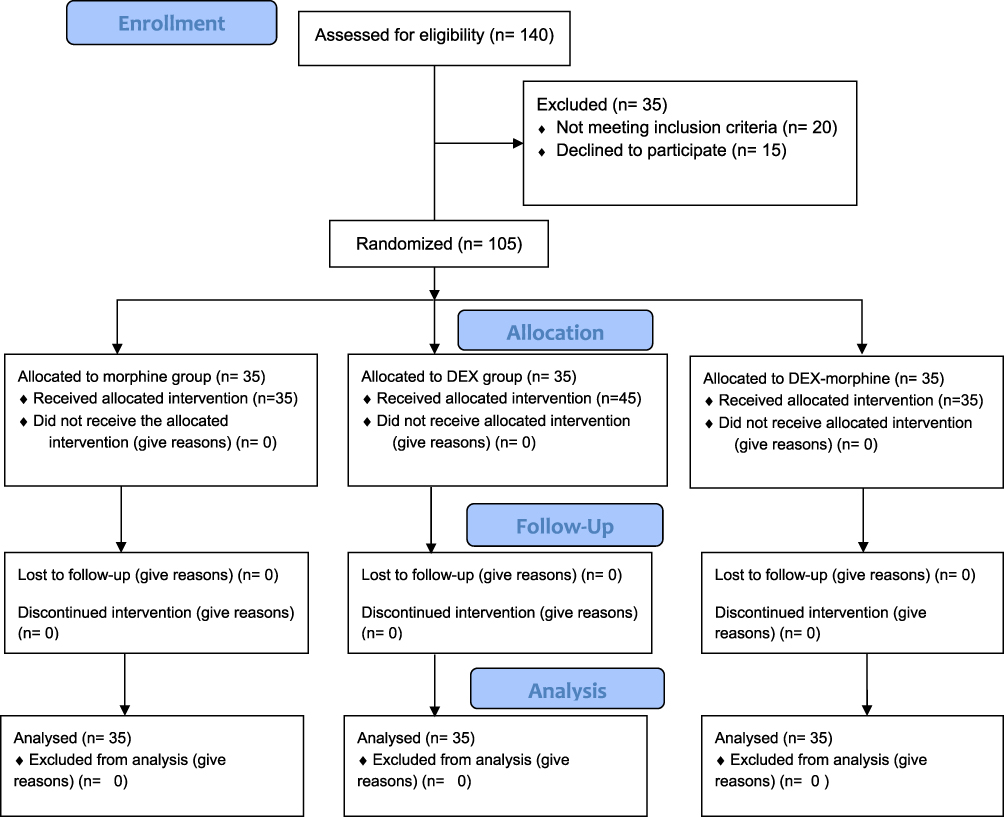 |
Figure 1 The CONSORT flow chart. |
All groups were significantly similar in age, BMI, ASA physical status, and duration of the surgery (Table 1).
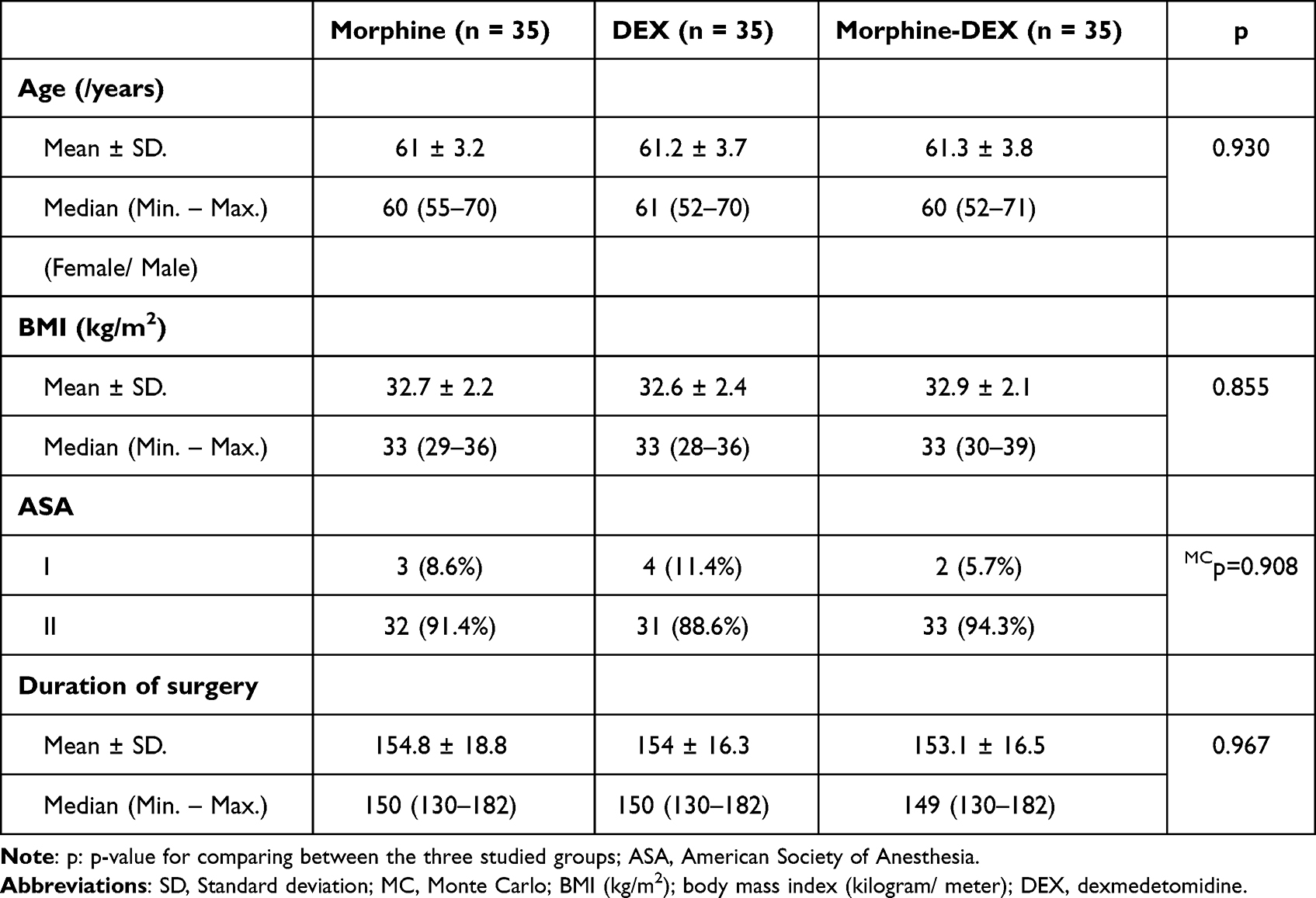 |
Table 1 Comparison Between the Three Studied Groups According to Demographic and Clinical Data |
The Dexmedetomidine group has a significantly shorter analgesic duration with an early request of rescue analgesia due to the early onset of postoperative pain than the other two groups, as about half of the patients requested first rescue analgesia after 6 hours from the operation. On the other hand, the other two groups show no significant difference between them regarding the first required analgesia (Table 2).
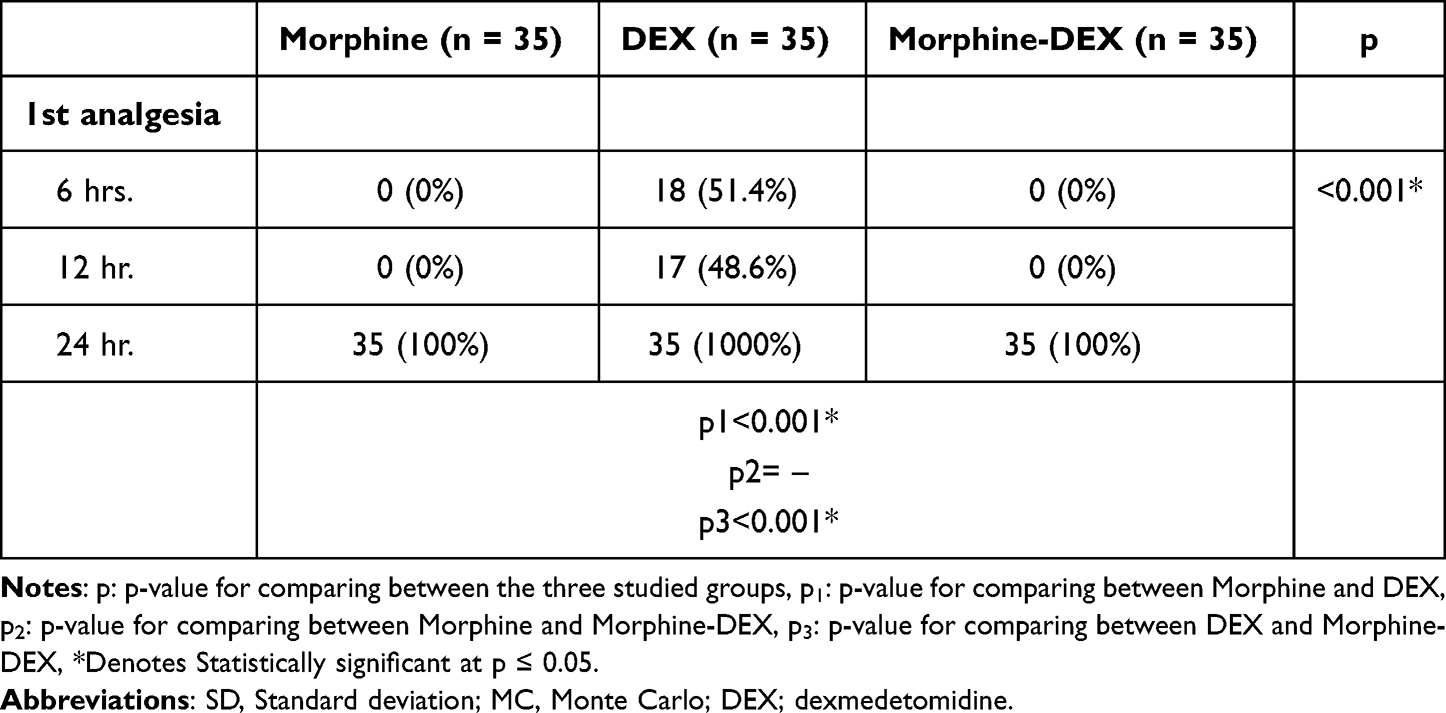 |
Table 2 Comparison Between the Three Studied Groups According to the Time of the 1st Analgesia Request |
At rest, all groups were pain-free in the first 4 hours postoperatively. But at 6 hours and 12 hours postoperative, patients in the DEX group have significantly higher VAS with a significant increase in patients who required morphine as rescue analgesia than the other two groups. After 24hrs after the operation, all groups have high VAS without significant differences between the groups. All patients required morphine analgesia after 24hrs from surgery. While at movement, patients in the DEX group felt pain at 4 hrs postoperatively with significantly higher VAS than the other two groups. (Table 3 and Figure 2).
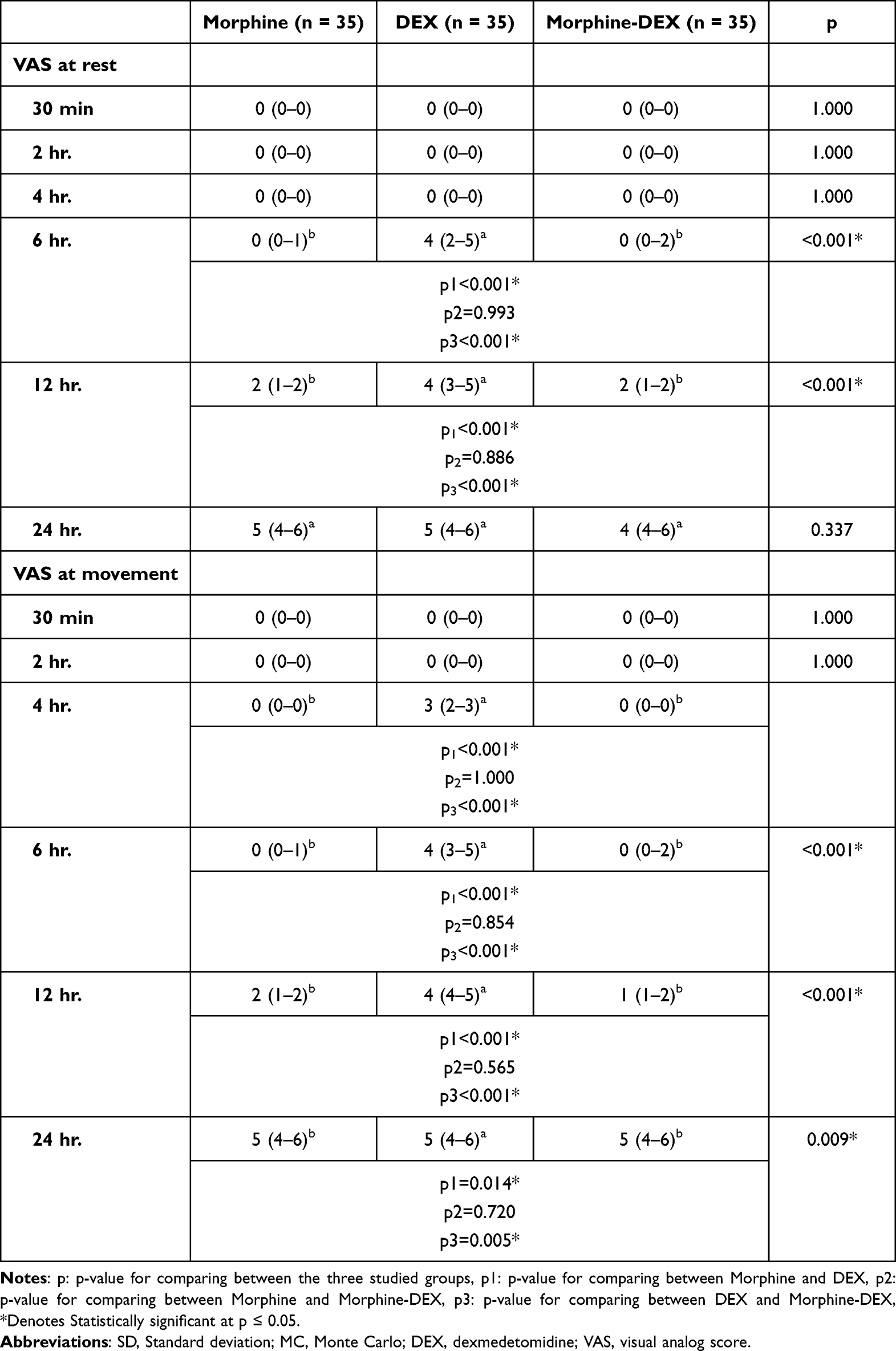 |
Table 3 Comparison Between the Three Studied Groups According to VAS |
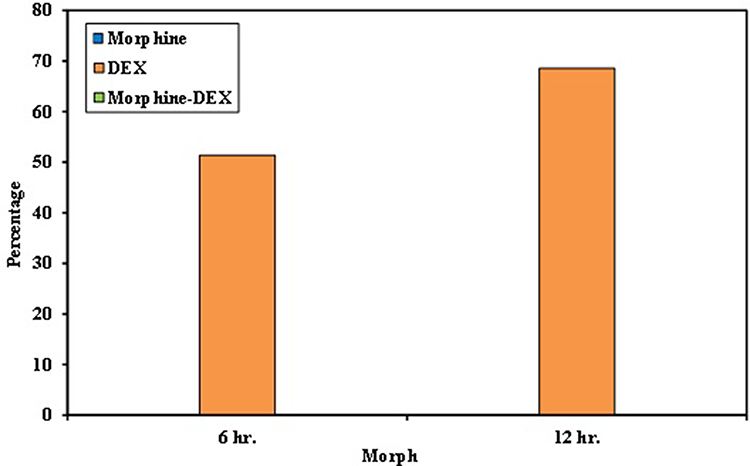 |
Figure 2 Comparison between the three studied groups according to morphine consumption postoperatively. Abbreviation: DEX; dexmedetomidine. |
At the same time, the DEX group significantly lower sedation score than the other two groups. No case in the three groups developed postoperative respiratory depression. But 22.2% of cases in the morphine group developed PONV with a significant difference between the three groups (Table 4).
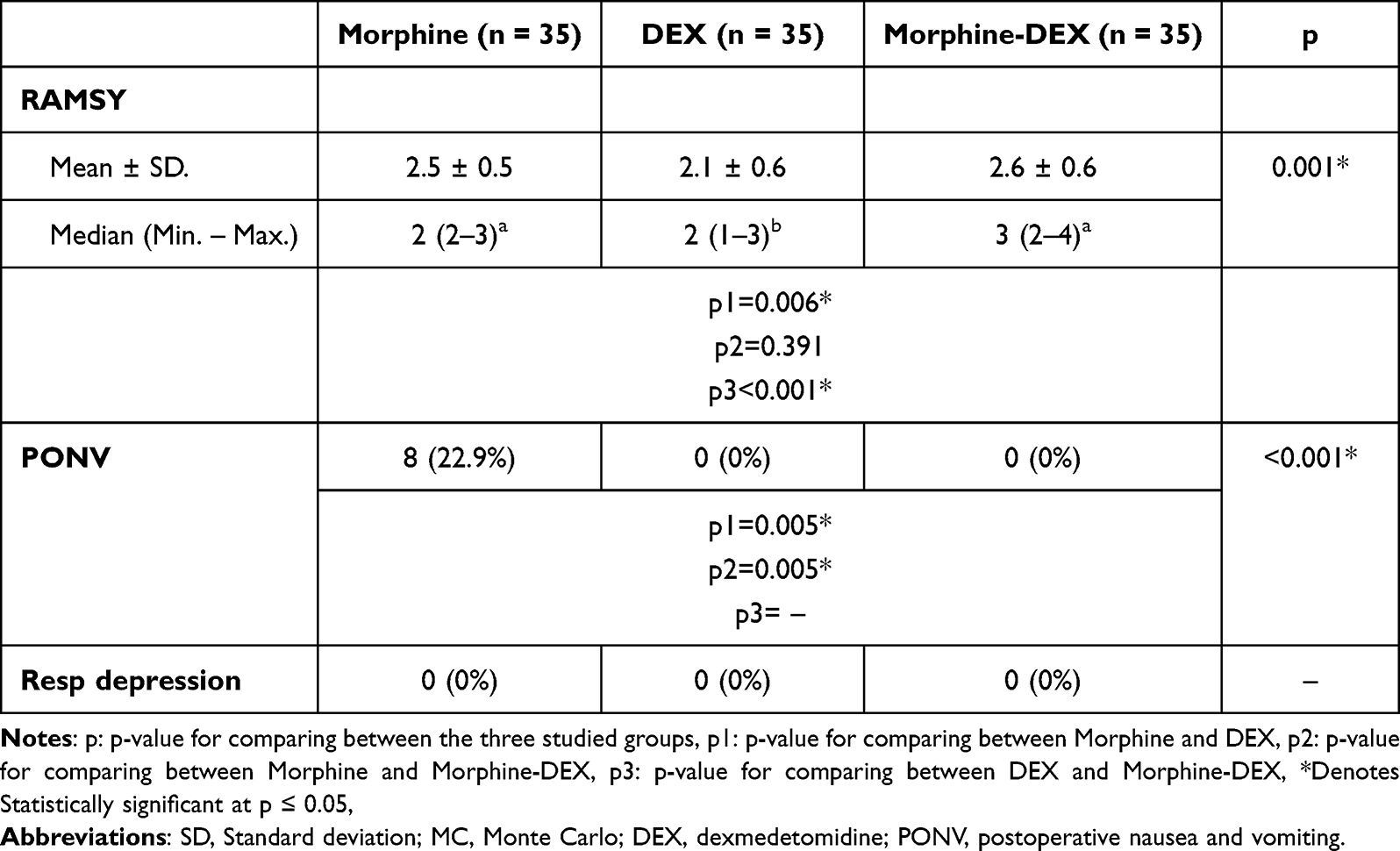 |
Table 4 Comparison Between the Three Studied Groups According to Clinical Data |
Discussion
The results of the present study showed that the analgesic effect of mixed intrathecal dexmedetomidine- morphine prolonged up to 24 hrs postoperatively at rest and up to 12 hrs during movement which like intrathecal administration of morphine only, but co-administration of dexmedetomidine decreased incidence of PONV side effect of intrathecal morphine alone from 22.9% to 0% without increasing the incidence of postoperative respiratory depression or sedation. The long duration of action of 0.1 mg ITM, which may mask the analgesic effect of dexmedetomidine, could explain our findings. The addition of dexmedetomidine to lower dosages of ITM or other short-acting intrathecal opioids such as fentanyl could be clinically important.
This study was the first study to compare the analgesic efficacy of combined intrathecal morphine and dexmedetomidine with either drug alone in patients undergoing TKR. To date, no consensus has been made regarding the optimal dose of intrathecal morphine but appears to be 100–250 mcg. In this study, 100 mcg of morphine was used.13
Subarachnoid block with hyperbaric bupivacaine is an established technique for surgeries on the lower body. However, its short duration of postoperative analgesia is a limitation.14
While hip and knee arthroplasty are increasingly being performed ambulatorily or with a short hospital stay, anesthetists are hesitant to administer intrathecal morphine, despite its expected analgesic effect, due to concerns about potential side effects, particularly postoperative nausea, and vomiting (PONV) and respiratory depression. These issues may need hospitalization or a longer length of stay, increase surgical morbidity, and degrade patients’ experiences, weakening the analgesic efficacy and patient advantages of this analgesic modality, particularly in the context of accelerated recovery.15
Dexmedetomidine is a strong and highly selective a2-adrenoceptor agonist. The stimulation of a2-adrenoceptors in the central nervous system is thought to be responsible for their anti-nociceptive function. Its intrathecal infusion has anti-nociceptive benefits, but it also has several undesirable side effects (for example, hypotension, bradycardia, and drowsiness).16,17
Our results explained by animal studies demonstrated a synergistic interaction between opioid and alpha-2 adrenergic anti-nociception in the rat spinal cord. The intrathecal administration of morphine and dexmedetomidine in combination was discovered to create a synergistic effect-state magnitude, and such synergism is mediated by the mu opioid receptor subtype rather than the delta opioid receptor subtype.18,19 The reason for combining analgesics with similar therapeutic effects or synergistic interactions is to increase analgesic efficacy while decreasing adverse effects by allowing each agent’s dose to be reduced.8,9
Human research on the antinociceptive effects of intrathecal morphine (ITM) and dexmedetomidine in postoperative pain is currently lacking.
Morphine and dexmedetomidine may interact synergistically in a variety of ways. Because opioids, glutamate, and 2-adrenoceptors are numerous in the spinal cord,20 co-activation and antagonism of these receptors may favor pain sensation inhibition at low doses with little adverse effects. The mechanisms of action of morphine and dexmedetomidine are not the same. One of these is the inhibition of transmitter release from the C-fiber primary afferent terminal, however, they also inhibit interneurons and projecting neurons.21 The increased activity may also be due to a decrease in drug clearance from the intrathecal region, as animal tests have indicated that the combination’s duration of effect was greater than that of morphine or dexmedetomidine alone.19
Although the biochemical reason is still unknown, this helpful antiemetic action may be explained by the direct antiemetic characteristics of α2 agonists. Furthermore, since excessive catecholamine concentrations can cause nausea and vomiting, a decline in sympathetic tone may account for dexmedetomidine’s antiemetic effects. Finally, the consumption of intraoperative opioids, which increases the risk of PONV,22 may be reduced through the use of dexmedetomidine.23
All three; Intrathecal morphine, intrathecal dexmedetomidine, and titrated doses of PO morphine with multimodal analgesia do not cause significant sedation. Ramsay scale the in majority of the patients in the three groups is 2 with sporadic cases as 3. In patients who underwent TKR, this is regarded as the normal state. The statistical significance of this issue does not have a clinical impact.
One point worth debating is the alleged risk of postoperative hypoventilation. Even though the intrathecal morphine group had more patients, there was no difference in the rates of hypoxemia or respiratory depression. This is significant since many clinicians believe that continuous monitoring is required, as recommended by the American Society of Anesthesiologists. While respiratory depression may have been a clinical problem with intrathecal morphine doses of 2.5 mg, as reported in the late 1980s,24 recent evidence shows that respiratory depression is not present with doses less than 150 ug,25 even in elderly patients undergoing hip arthroplasty.26 Thus, a 100-mcg intrathecal morphine dose for lower limb arthroplasty appears to warrant no more than standard postoperative care. Notably, the effect of intrathecal morphine is estimated to last up to 16 hours.27
The current study found good evidence that intrathecal morphine provides effective analgesia after lower limb arthroplasty, without an increased risk of respiratory depression, by systematically searching the literature for trials comparing intrathecal morphine with a control group in patients undergoing hip or knee arthroplasty under spinal anesthesia. The 100 ug dose is a “ceiling” dose for analgesia as well as a threshold dose for increased postoperative nausea and vomiting.28
Furthermore, in a rat model of neuropathic pain, Kabalak et al compared the synergistic anti-allodynic interaction and side effects of intrathecal morphine and dexmedetomidine. They discovered that intrathecal administration of morphine and dexmedetomidine, both alone and in combination, generated a dose-dependent anti-allodynic effect with a synergistic effect-state magnitude. Furthermore, when morphine or dexmedetomidine was administered in high doses alone, the incidence of side effects was higher, but extremely low when these two drugs were used in combination, and Kabalak et al provide a rationale for combining such drugs in the future to improve human postoperative or neuropathic pain treatment.19
Similarly, Abdel-Ghaffar et al studied 90 patients who were randomly assigned to receive intrathecal bupivacaine, bupivacaine, and 0.5 mg morphine (Morphine Group), or bupivacaine, 0.5 mg morphine, and 5 mcg dexmedetomidine (morphine-Dex Group). Morphine and morphine-Dex groups showed lower pain scores (P < 0.001), with longer time to first use of morphine in morphine (22.13 ± 5.21h) and morphine-Dex (23.46 ± 4.69h) groups compared with bupivacaine group (0.50 ± 0.09h) as dexmedetomidine addition increased the duration of intrathecal morphine (ITM) analgesia by 1.33 h (P = 0.485). Morphine (10.83 2.96 mg) and morphine-Dex (11.00 3.32 mg) groups consumed less morphine than the bupivacaine group (27.5 4.30 mg), with a non-significant difference between morphine and morphine-Dex groups (P = 0.375). Their findings did not support the addition of dexmedetomidine to ITM, as there were no significant differences in the time to first request postoperative analgesia, morphine consumption, or pain scores between the morphine and morphine-Dex groups, which can be attributed to the nature of the patients (Cancer patients).29
In addition, In Liu, Gao et al double-blind cross-over study administered ITM and dexmedetomidine to patients with refractory cancer pain either intrathecal morphine alone or intrathecal morphine plus dexmedetomidine. They found that pain intensity and frequency were significantly decreased in both groups compared with baseline. Daily morphine consumption and bolus dose injection times in combined morphine plus dexmedetomidine were significantly decreased compared with morphine alone.30
This study has limitations as we did not assess motor or sensory level blocks. Also, the sample size is small. Additional research with bigger samples is required to assess the value of such combinations.
Conclusion
In conclusion, adding dexmedetomidine to ITM did not improve postoperative analgesia in adult patients following total knee replacement surgery under spinal anesthesia, although it did reduce opioid-related side effects. Future research with a larger sample size is required to confirm or declare our findings.
Data Sharing Statement
All the individual participant data collected are available from a data repository immediately after publication without an end date. The study protocol, statistical analysis plan, clinical study report, and analytic code are also available. Anyone can access the data, and the data can be used for any purpose.
Disclosure
The authors declare no competing interests.
References
1. Priebe H-J. The aged cardiovascular risk patient. Br J Anaesth. 2000;85(5):763–778. doi:10.1093/bja/85.5.763
2. Yaksh T. CNS mechanisms of pain and analgesia. Cancer Surv. 1988;7(1):5–28.
3. Moher D, Liberati A, Tetzlaff J, Altman DG; Group* P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–269. doi:10.7326/0003-4819-151-4-200908180-00135
4. Giovannelli M, Bedforth N, Aitkenhead A. Survey of intrathecal opioid usage in the UK. Eur J Anaesthesiol. 2008;25(2):118–122. doi:10.1017/S0265021507001305
5. Payne R. Neuropathic pain syndromes, with special reference to causalgia and reflex sympathetic dystrophy. Clin J Pain. 1986;2(1):59–73. doi:10.1097/00002508-198602010-00010
6. Mantz J, Josserand J, Hamada S. Dexmedetomidine: new insights. Eur J Anaesthesiol. 2011;28(1):3–6. doi:10.1097/EJA.0b013e32833e266d
7. Harada Y, Nishioka K, Kitahata L, Kishikawa K, Collins J. Visceral antinociceptive effects of spinal clonidine combined with morphine,[D-Pen sup 2, D-Pen sup 5] enkephalin, or U50, 488H. J Am Soc Anesthesiol. 1995;83(2):344–352.
8. Horvath G, Joo G, Dobos I, Klimscha W, Toth G, Benedek G. The synergistic antinociceptive interactions of endomorphin-1 with dexmedetomidine and/or S (+)-ketamine in rats. Anesth Analg. 2001;93(4):1018–1024. doi:10.1097/00000539-200110000-00044
9. Meert TF, De Kock M. Potentiation of the analgesic properties of fentanyl-like opioids with alpha 2-adrenoceptor agonists in rats. Anesthesiology. 1994;81(3):677–688. doi:10.1097/00000542-199409000-00022
10. Murphy P, Stack D, Kinirons B, Laffey J. Optimizing the dose of intrathecal morphine in older patients undergoing Hip arthroplasty. Anesth Analg. 2003;97(6):1709–1715. doi:10.1213/01.ANE.0000089965.75585.0D
11. Al-Ghanem SM, Massad IM, Al-Mustafa MM, et al. Effect of adding dexmedetomidine versus fentanyl to intrathecal bupivacaine on spinal block characteristics in gynecological procedures: a double blind controlled study. Am J Appl Sci. 2009;6(5):882. doi:10.3844/ajassp.2009.882.887
12. Ramsay M, Savege T, Simpson B, Goodwin R. Controlled sedation with alphaxalone-alphadolone. BMJ. 1974;2(5920):656–659. doi:10.1136/bmj.2.5920.656
13. Khandelwal M, Rao H, Kumar P, Bafna U, Beniwal S. Comparative study of morphine or dexmedetomidine as intrathecal adjuvants to 0.5% hyperbaric bupivacaine in infraumbilical surgeries. Indian J Pain. 2019;33(3):156. doi:10.4103/ijpn.ijpn_31_19
14. Shaikh SI, Dattatri R. Dexmedetomidine as an adjuvant to hyperbaric spinal bupivacaine for infra-umbilical procedures: a dose related study. Anaesth Pain Intensive Care. 2019;2019:180–185.
15. Kehlet H. Enhanced postoperative recovery: good from afar, but far from good? Anaesthesia. 2020;75:e54–e61. doi:10.1111/anae.14860
16. Maze M, Scarfini C, Cavaliere F. New agents for sedation in the intensive care unit. Crit Care Clin. 2001;17(4):881–898. doi:10.1016/S0749-0704(05)70185-8
17. Blaudszun G, Lysakowski C, Elia N, Tramer MR. Effect of perioperative systemic α2 agonists on postoperative morphine consumption and pain intensity: systematic review and meta-analysis of randomized controlled trials. J Am Soc Anesthesiol. 2012;116(6):1312–1322.
18. Sullivan A, Kalso E, McQuay H, Dickenson A. The antinociceptive actions of dexmedetomidine on dorsal horn neuronal responses in the anaesthetized rat. Eur J Pharmacol. 1992;215(1):127–133. doi:10.1016/0014-2999(92)90617-D
19. Kabalak A, Ekmekçioğlu E, Ceylan A, Kahveci K. The synergistic antinociceptive interactions of morphine and dexmedetomidine in rats with nerve-ligation injury. Hippokratia. 2013;17(4):326.
20. Coggeshall RE, Carlton SM. Receptor localization in the mammalian dorsal horn and primary afferent neurons. Brain Res Rev. 1997;24(1):28–66. doi:10.1016/s0165-0173(97)00010-6
21. Ueda M, Oyama T, Kuraishi Y, Akaike A, Satoh M. Alpha2-adrenoceptor-mediated inhibition of capsaicin-evoked release of glutamate from rat spinal dorsal horn slices. Neurosci Lett. 1995;188(2):137–139. doi:10.1016/0304-3940(95)11397-F
22. Smith I, Walley G, Bridgman S. Omitting fentanyl reduces nausea and vomiting, without increasing pain, after sevoflurane for day surgery. Eur J Anaesthesiol. 2008;25(10):790–799. doi:10.1017/S026502150800464X
23. Liang X, Zhou M, Feng JJ, et al. Efficacy of dexmedetomidine on postoperative nausea and vomiting: a meta-analysis of randomized controlled trials. Int J Clin Exp Med. 2015;8(6):8450–8471.
24. Jacobson L, Chabal C, Brody MC. A dose-response study of intrathecal morphine: efficacy, duration, optimal dose, and side effects. Anesth Analg. 1988;67(11):1082–1088. doi:10.1213/00000539-198867110-00011
25. Crowgey TR, Dominguez JE, Peterson-Layne C, Allen TK, Muir HA, Habib AS. A retrospective assessment of the incidence of respiratory depression after neuraxial morphine administration for postcesarean delivery analgesia. Anesth Analg. 2013;117(6):1368–1370. doi:10.1213/ANE.0b013e3182a9b042
26. Albrecht E, Bayon V, Hirotsu C, Al Ja’Bari A, Heinzer R. Intrathecal morphine and sleep apnoea severity in patients undergoing Hip arthroplasty: a randomised, controlled, triple-blinded trial. Br J Anaesth. 2020;125(5):811–817. doi:10.1016/j.bja.2020.07.052
27. Cousins MJ, Cousins M, Mather L. Intrathecal and epidural administration of opioids. Anesthesiology. 1984;61:276–310. doi:10.1097/00000542-198409000-00008
28. Gonvers E, El‐Boghdadly K, Grape S, Albrecht E. Efficacy and safety of intrathecal morphine for analgesia after lower joint arthroplasty: a systematic review and meta‐analysis with meta‐regression and trial sequential analysis. Anaesthesia. 2021;76(12):1648–1658. doi:10.1111/anae.15569
29. Abdel-Ghaffar HS, Mohamed SA, Fares KM. Combined intrathecal morphine and dexmedetomidine for postoperative analgesia in patients undergoing major abdominal cancer surgery. Pain Med. 2016;17(11):2109–2118. doi:10.1093/pm/pnw031
30. Liu H-J, Gao X-Z, Liu X-M, Xia M, Li W-Y, Jin Y. Effect of intrathecal dexmedetomidine on spinal morphine analgesia in patients with refractory cancer pain. J Palliat Med. 2014;17(7):837–840. doi:10.1089/jpm.2013.0544
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Antioxidant Therapy Reverses Sound Stress-Induced Opioid Resistance in a Mouse Model of Mechanical Allodynia
Kasai S, Furuta A, Kuroda J, Takagi M, Sawai T, Yamada D, Saitoh A, Yoshizawa K
Journal of Pain Research 2026, 19:550094
Published Date: 25 June 2026