Back to Journals » Journal of Pain Research » Volume 13
Intrathecal Morphine Infusion Therapy via a Percutaneous Port for Refractory Cancer Pain in China: An Efficacy, Safety and Cost Utilization Analysis
Authors Qin W ![]() , Li Y
, Li Y ![]() , Liu B, Liu Y, Zhang Y, Zhang X, Li P, Fan B
, Liu B, Liu Y, Zhang Y, Zhang X, Li P, Fan B
Received 8 October 2019
Accepted for publication 14 January 2020
Published 23 January 2020 Volume 2020:13 Pages 231—237
DOI https://doi.org/10.2147/JPR.S233905
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Überall
Wangjun Qin, 1 Yifan Li, 2 Botao Liu, 2 Ying Liu, 1 Yi Zhang, 2 Xianglin Zhang, 1 Pengmei Li, 1 Bifa Fan 2
1Department of Pharmacy, China–Japan Friendship Hospital, Beijing, People’s Republic of China; 2Department of Pain Management, China–Japan Friendship Hospital, Beijing, People’s Republic of China
Correspondence: Pengmei Li; Bifa Fan 2 Yinghua Dongjie, Hepingli, Beijing 100029, People’s Republic of China
Tel/Fax +86 10 8420 5330;
+86 10 84205959
Email [email protected]; [email protected]
Purpose: Intrathecal morphine infusion therapy via a percutaneous port (IMITPP) has been used widely for its relatively low initial cost. However, there is scarce knowledge about IMITPP. In this study, we sought to evaluate efficacy, complications, and the interval required to achieve the cost equivalence of IMITPP in patients with refractory cancer pain in China.
Patients and Methods: A retrospective chart review was conducted on cancer patients who had received IMITPP at our hospital between April 2017 and April 2019. Data from the numeric pain rating scale and Karnofsky performance scores, and complications and costs related to IMITPP were collected from medical records. Daily analgesic costs before and after IMITPP were calculated based on the doses of opioids on admission and at discharge, respectively. The doses of systemic opioids before IMITPP were stratified into very high doses [VHD, oral morphine equivalent dose (OMED) > 599 mg/day], high doses (HD, 300 mg/day ≤ OMED ≤ 599 mg/day), and regular doses (RD, OMED < 300 mg/day).
Results: Intrathecal morphine infusion therapy via a percutaneous port provided significant pain relief, but impaired activities of daily living in patients with refractory cancer pain. The commonly reported complications included nausea/vomiting and urinary retention, most of which were managed with symptomatic therapies. The median interval required to achieve cost equivalence was 11.44 months. The median intervals of VHD group and HD group were significantly shorter than that of RD group.
Conclusion: Intrathecal morphine infusion therapy via a percutaneous port provided effective cancer pain management without causing serious complications. Patients with higher doses of systemic opioids would economically benefit from IMITPP in a shorter time.
Keywords: intrathecal, morphine, port catheter, cost-benefit analysis, cancer pain
Introduction
Pain is a major fear and concern of many cancer patients and often causes depression, morbid mood and reduced quality of life when poorly controlled.1,2 Intrathecal morphine infusion therapy is considered for the management of refractory cancer pain which failed to be treated with the World Health Organization (WHO) pain ladder.3–5 Intrathecal morphine infusion therapy directly delivers morphine at about 1/300 the oral dose into the cerebrospinal fluid (CSF) through an intrathecal catheter, which provides a strong analgesic effect and reduces the incidence of the adverse events caused by systemic opioids.4 The intrathecal catheter is connected to either an implanted morphine pump or a percutaneous port which is attached to an external drug infusion pump.6,7
Despite its effectiveness in pain relief, the implementation of intrathecal morphine infusion therapy is impeded by the high initial cost in cancer pain patients.7,8 Previous reports on cost effectiveness suggested different intervals for cost equivalence from 19 to 344 months between intrathecal morphine infusion therapy via an implanted morphine pump and conventional medicine therapy depending on different countries or regions.4,9–12 Intrathecal morphine infusion therapy via a percutaneous port (IMITPP) is expected to take a shorter time to reach cost equivalence than intrathecal morphine infusion therapy via an implanted morphine pump because of its relatively lower initial implantation costs, which would be a better choice for the advanced cancer patients with short life expectancy.3,4 However, there is a lack of knowledge about intervals for cost equivalence between IMITPP and conventional medical therapy.
In this study, we conducted a retrospective chart review on patients who had received IMITPP for refractory cancer pain in China. The clinical efficacy and the incidence of adverse events were assessed. Moreover, the interval required to achieve cost equivalence of IMITPP and associated factors were also studied.
Materials and Methods
Patient Population
From April 2017 to April 2019, 56 cancer pain patients were implanted with an intrathecal catheter connected to a percutaneous port (C.R. Bard, Inc., Murray Hill, NJ, USA) for IMITPP. Thirteen patients were excluded from the study for the following reasons. Two patients suffered from chronic nonmalignant pain, four patients underwent more than one operation for pain management during the same hospitalization, and seven patients did not develop opioid tolerance before IMITPP. Therefore, 43 patients were included for analysis in the study.
All procedures were performed under local anesthesia in the aseptic operating room at China–Japan Friendship Hospital. Intrathecal access was obtained in the lumbar region under the guidance of X-ray. The intrathecal catheter was implanted into the intrathecal space and the tip of catheter was placed at a spinal level correlated best with the dermatomal distribution of the pain. Then, a subcutaneous tunnel was built, and the catheter was connected to a subcutaneous port via the tunnel. Morphine diluted with 0.9% sodium chloride solution to 100 mL (Qinghai Pharmaceuticals, Xining, China) was infused to intrathecal space through the subcutaneous port by an external drug infusion pump (Hospira Inc., Chicago, IL, USA). Intrathecal morphine was initiated and titrated according to guidelines and clinical experience. Opioids given by systemic routes were then stopped or quickly weaned off before the patients were discharged from the hospital.
Data-Gathering Procedures
Medical records of enrolled patients were retrospectively reviewed. Patients’ demographic data (such as sex, age, height and weight), types of cancer, technical data (such as insertion interspace, catheter tip location), complications related to IMITPP were obtained from the medical records. Numerical pain rating scales (NRS) scores, Karnofsky performance scores (KPS), and doses of opioids before and after IMITPP were also determined. Costs before IMITPP (pre-IMITPP) were calculated based on the types and doses of systemic opioids on admission, including professional fee and costs of systemic opioids. Costs after IMITPP (post-IMITPP) were calculated based on the doses of intrathecal morphine at discharge, including professional fee, rental of the external drug infusion pump, costs of medication (morphine hydrochloride injection and 0.9% sodium chloride solution) and disposable wound care pack. The total implantation costs were determined as the total hospitalization expense, which included the costs of subcutaneous port and medication, ward fee, laboratory fee, image examination fee, anesthetic fee and operation fee.
Dose Stratification
The doses of systemic opioids before IMITPP were summarized as the oral morphine equivalent dose (OMED), and then patients were categorized according to the Edmonton classification for daily oral morphine dose.13,14 Patients with OMED > 599 mg/day were determined as very-high doses (VHD) group, 300–599 mg/day as high doses (HD) group, and <300 mg/day as regular doses (RD) group.
Assumptions
Certain assumptions were made:
- We assumed that patients would remain on their analgesic regimens without dose escalation both before and after IMITPP.
- It was assumed that patients would have a fixed visit frequency as required (once every 14 days) regardless of whether they received ITIMPP or not, so the professional fees of visits can be divided evenly.
Ethics Approval and Informed Consent
The present study was conducted in accordance with the Declaration of Helsinki and approved by the ethical committee of China–Japan Friendship Hospital (2019-BZR-16). Given that it was relatively difficult to contact all the patients and acquire written informed consents for this retrospective research, the ethical committee approved the study waiving the informed consents in view of the academic significance and the fact that the patients’ personal information was used for research only.
Data Analysis
Paired-samples t-test was used to compare NRS and KPS scores before and after IMITPP. The daily costs before and after IMITPP were compared. The total implantation costs for IMITPP were divided by the difference between the daily costs before and after IMITPP to determine the interval required to achieve cost equivalence in each patient. The intervals among different groups were tested by one-way analysis of variance (ANOVA) and post hoc Bonferroni test. Statistical analyses were conducted using SPSS version 22.0 (IBM Corp., Armonk, NY, USA). The data are expressed as median values [75% interquartile range (IQR)]. The significant level was taken as p<0.05.
Results
Complete data for 43 patients (30 male/13 female) were analyzed. Median age at beginning of IMITPP was 60 years (IQR: 53–64). Median duration of cancer pain before IMITPP was 0.75 years (IQR: 0.42–1). Thirty-five patients (81.40%) selected IMITPP due to inadequate pain relief by systemic opioids, and for others (18.60%), intolerance of systemic opioids-induced toxicity was the primary reason. The demographic characteristics of the patients are shown in Table 1.
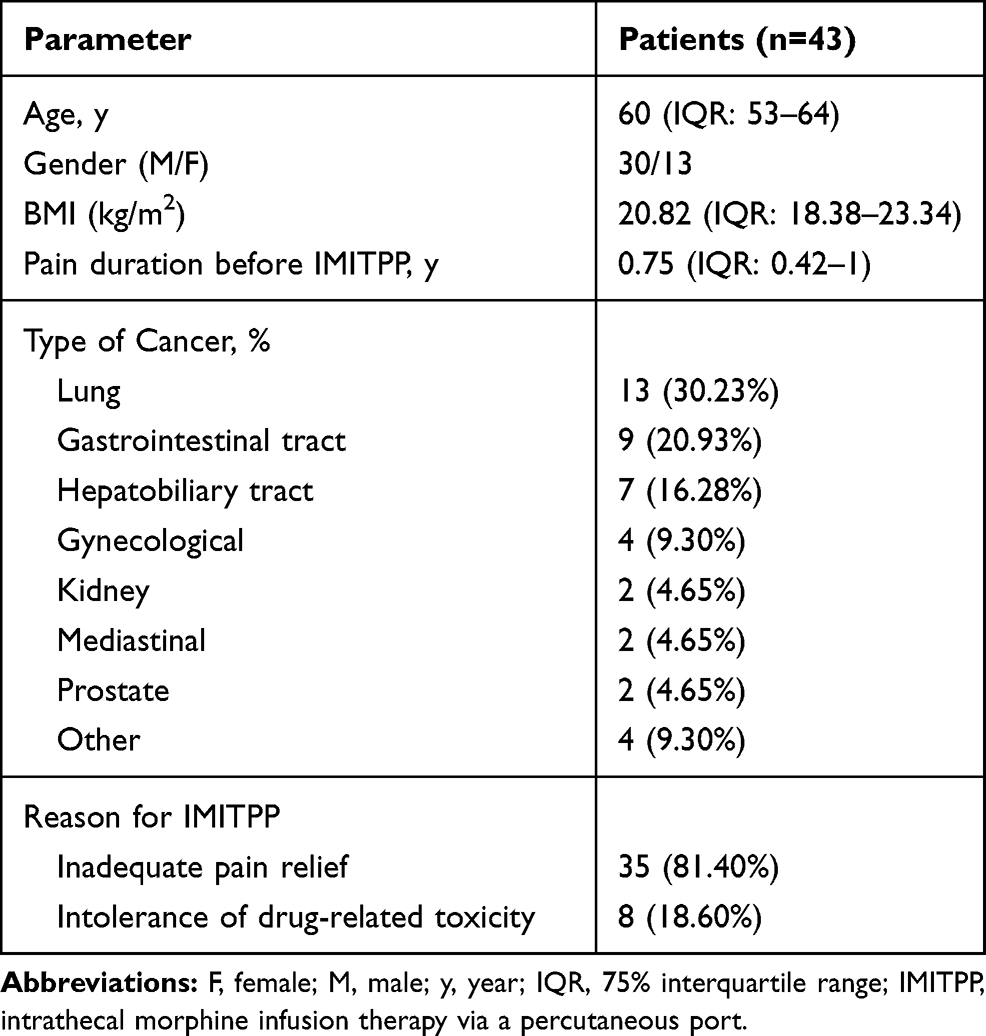 |
Table 1 Baseline Characteristics of Patients |
The intrathecal catheters were inserted at the L2-3 (n=14), L3-4 (n=25) or L4-5 (n=4) intervertebral space in all patients. The location of catheter tips was selected based on pained region and most were located at the level of the T8, T9, T10 and T11 vertebral body (16.28%, 13.95%, 18.60% and 13.95%, respectively) (Table 2).
 |
Table 2 Location of Catheter Tips |
All the patients were receiving systemic opioids (including oral and intravenous morphine, oral oxycodone, and transdermal fentanyl) before IMITPP, at a median daily OMED of 320 mg (IQR: 170–560). The median dose of intrathecal morphine was 1.1 mg (IQR: 0.5–2.4) at discharge, and the median conversion ratio from OMED to dose of intrathecal morphine was 307.69 (IQR: 191.60–440).
The 43 patients suffered moderate to severe pain with a median NRS score of 7 (IQR: 7–7) on admission before IMITPP, even treated with systemic opioids. The median NRS score was 3 (IQR: 2–3) at discharged after IMITPP, which was significantly lower than that before IMITPP (t=21.148, p=0.000) (Figure 1).
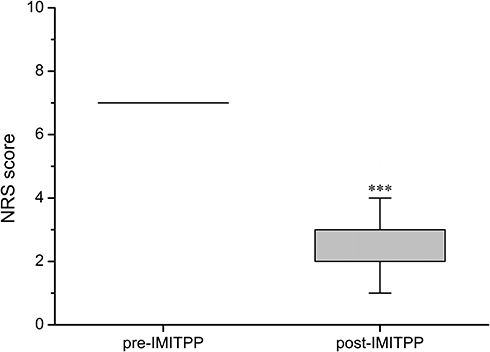 |
Figure 1 Comparison of numeric rating scale (NRS) scores before and after IMITPP (n=43). ***p <0.001 vs pre-IMITPP. Abbreviation: IMITPP, intrathecal morphine infusion therapy via a percutaneous port. |
On admission for IMITPP, the median KPS score of patients was 75 (IQR: 60–95). A significant impairment of the activity of daily living was observed when patients were discharged after IMITPP as compared by paired-samples t-test (t=2.243, p=0.030) (Figure 2).
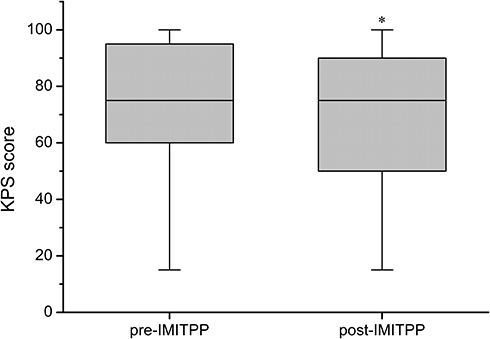 |
Figure 2 Comparison of Karnofsky performance scores (KPS) before and after IMITPP (n=43). *p <0.05 vs pre-IMITPP. Abbreviation: IMITPP, intrathecal morphine infusion therapy via a percutaneous port. |
Nausea/vomiting and urinary retention were the most frequent drug-related adverse events, which was observed in 14 patients (32.56%) and nine patients (20.93%), respectively (Figure 3). Two patients experienced severe diarrhea after conversion from systemic opioids to intrathecal morphine, which was reversed by deceleration of decreased speed of systemic opioids dosage, instead of symptomatic treatment. Other drug-related adverse advents subsided with conservative treatments within a few days. Another two patients suffered from post-dural puncture headache in consideration of cerebrospinal fluid leak, which was managed conservatively with bed rest and increased fluid intake. No other operative complications were noted.
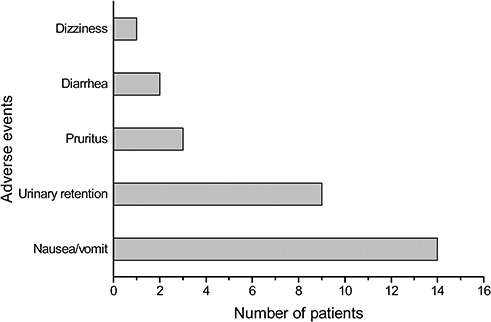 |
Figure 3 Adverse events related to intrathecal morphine experienced by IMITPP patients. |
The costs of IMITPP include the initial implantation costs and daily maintenance costs. The median daily analgesic costs before and after IMITPP were 130.67 RMB (IQR: 67.17–321.37) and 4.62 RMB (IQR: 4.36–5.38), respectively. The median hospitalization expense for IMITPP was 47058.70 RMB (IQR: 40812.56–54741.41), and the median interval required to achieve cost equivalence was 11.44 months (IQR: 5.88–28.40). The estimated interval to cost equivalence varied significantly when patients were categorized according to different OMED before IMITPP (F=42.01, p<0.001) (Figure 4). Very-high doses group (2.89 months, IQR: 2.15–4.07) had a significant shorter interval than both HD group (9.71 months, IQR: 7.43–11.30) (p<0.001) and RD group (28.83 months, IQR: 20.90–36.18) (p<0.001), and HD group also had a shorter interval compared with RD group (p<0.001).
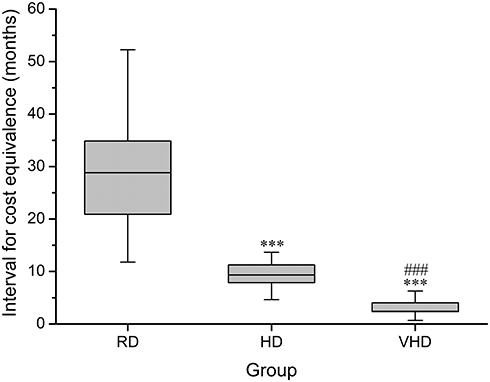 |
Figure 4 Interval required to achieve cost equivalence among different pre-IMITPP oral morphine equivalent dose (OMED) groups. N=19 for RD group, n=14 for HD group, and n=10 for VHD group. ***p <0.001 vs RD group, ###p <0.001 vs HD group. Abbreviations: RD, regular doses; HD, high doses; VHD, very high doses. |
Discussion
Intrathecal morphine infusion therapy is an effective treatment option for refractory cancer pain, which delivers smaller doses of morphine into the intrathecal space to produce powerful analgesic effect with minimal systemic adverse effects.3–5 The implanted intrathecal morphine pump is usually used for intrathecal morphine infusion therapy and is suitable for long-term use. However, the high initial cost is a major obstacle.15 Recently, intrathecal morphine infusion therapy via a percutaneous port (IMITPP) has become a widely used approach in some countries for its relatively lower cost.3,16–18 The efficacy and safety of IMITPP were assessed in this study. A significant decrease of NRS and KPS scores was observed after IMITPP, without serious drug-related adverse events and operative complications. The present study was the first to examine the cost utilization of IMITPP in patients with refractory cancer pain in China. Our results showed a median interval required to achieve cost equivalence at 11.44 months, but at 9.71 months and 2.89 months for HD group and VHD group, respectively. Our results suggested IMITPP as an effective approach and more cost-saving selection for cancer pain patients with limited life expectancy.
The effectiveness of intrathecal morphine infusion therapy via an implanted morphine pump has been validated for both cancer pain and non-cancer pain worldwide.19–22 Our present study shows that IMITPP is also effective for cancer pain refractory to the World Health Organization’s (WHO) “analgesic ladder” of pain management, which coincides with Zheng’s as well as Kim’s reports.16,18 Positions of catheter tips were supposed to be important for the effectiveness of IMITPP, which varied between C7 and L5 in the 43 patients in the present study. As the existence of concentration gradients for many compounds in the CSF after intrathecal infusion was supported by recent magnetic resonance imaging evidences, it seems to be helpful for improving effectiveness to place the catheter tip close to the target receptors of the spinal segment responsible for the pain generator.5,23–25 Despite its effectiveness in pain relief, IMITPP was demonstrated to be harmful to the patients’ activities of daily living, which contrasts with a previous study showing an improvement in the quality of life and the ability to participate more fully in daily activities in patients treated with intrathecal morphine infusion therapy via an implanted morphine pump.26 There are several explanations for the decrease of KPS scores after IMITPP in this study. First, the patient treated with IMITPP had to wear an external drug infusion pump, which hinders patient’s movement.3 Second, meticulous exit site care with appropriate measures is necessary to avoid infection and catheter dislodgement or removal.6
Concerns regarding complications impede the further dissemination of IMITPP.22,27 Although intrathecal morphine infusion therapy reduces the incidence of the adverse advents caused by systemic opioids due to high morphine concentrations at the site of action, several operative and drug-related complications may arise after implantation.3,4 As compared to intrathecal morphine infusion therapy via an implanted morphine pump, disadvantages of IMITPP in operative complications are infection and the possibility of inadvertent catheter dislodgement or removal, which could be avoided by careful maintenance and was not observed in this study.6 Drug-related adverse events were the most common complications in intrathecal morphine infusion therapy.4 In the present study, most of the drug-related adverse events were controlled by symptomatic treatments and generally subsided within a few days, which is in accordance with other studies.11,22 It is notable that severe diarrhea was reported in two patients after conversion from systemic opioids to intrathecal morphine, which was reversed by deceleration of decreased speed of systemic opioids dosage, but not by symptomatic treatment. We considered diarrhea as a gastrointestinal withdrawal symptom associated with systemic opioids withdrawal in the two patients.27 Additional studies examining factors associated with risks of gastrointestinal withdrawal symptom are required.
The cost savings attributable to intrathecal morphine infusion therapy deserve further mention because of its high initial costs. The advantage of intrathecal morphine infusion therapy in expenditure is the lower maintenance cost.4 So, it takes time for patients to cost benefit from intrathecal morphine infusion therapy. An interval of 334 months was required to reach cost equivalence in cancer patients with intrathecal morphine infusion therapy via an implanted morphine pump in the USA, while the interval was 24.2 months in Korea and 28 months for chronic low back pain in Canada.10–12 Based on our results, IMITPP may become cost-beneficial at a shorter interval (11.44 months) than intrathecal morphine infusion therapy via an implanted morphine pump, profiting from the relatively low initial costs of IMITPP. Notably, patients in the VHD group achieved cost equivalence in less than 3 months in this study, suggesting that IMITPP is suitable for patients with extremely limited life expectancy. As we assumed that patients would remain on their analgesic regimen without dose escalation, the cost of systemic opioids was expected to be significantly underestimated, which leads to a longer calculated interval than it should be.10
Inevitably, there are still some limitations in this study. First, it is a retrospective study without clinical follow-ups, which makes it difficult to assess the long-term complications of IMITPP. Second, the present study only included patients who underwent IMITPP in China–Japan Friendship Hospital and did not consider the differences in medical costs between hospitals. Finally, a contrastive analysis of IMITPP and intrathecal morphine infusion therapy via an implanted morphine pump should be conducted in further study, which could reveal the advantages of IMITPP in cost utilization better.
Conclusion
Intrathecal morphine infusion therapy via a percutaneous port could provide effective pain relief without causing serious complications in patients with refractory cancer pain. Cancer pain patients with limited life expectancy were expected to cost benefit from IMITPP for its merits of easy operation and cost savings. Intrathecal morphine infusion therapy via a percutaneous port may be a more cost-beneficial treatment option for patients receiving systemic opioids in large doses.
Acknowledgment
The present work was supported by the Beijing Natural Science Foundation (7154236).
Author Contributions
Wangjun Qin, Yifan Li, Botao Liu, Ying Liu, Yi Zhang and Xianglin Zhang were responsible for data acquisition, analysis and interpretation and drafting the article. Pengmei Li and Bifa Fan contributed toward conception and design and provided critical revision of the manuscript. All authors critically reviewed the content and approved the final version for publication and agree to be accountable for the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mastenbroek TC, Kramp-Hendriks BJ, Kallewaard JW, Vonk JM. Multimodal intrathecal analgesia in refractory cancer pain. Scand J Pain. 2017;14:39–43. doi:10.1016/j.sjpain.2016.10.002
2. van den Beuken-van EM, de Rijke JM, Kessels AG, et al. Prevalence of pain in patients with cancer: a systematic review of the past 40 years. Ann Oncol. 2007;18(9):1437–1449. doi:10.1093/annonc/mdm056
3. De Andres J, Rubio-Haro R, De Andres-serrano C, Asensio-Samper JM, Fabregat-Cid G. Intrathecal drug delivery. Methods Mol Biol. 2020;2059:75–108. doi: 10.1007/978-1-4939-9798-5_3
4. Bhatia G, Lau ME, Koury KM, Gulur P. Intrathecal Drug Delivery (ITDD) systems for cancer pain. F1000Res. 2013;2:96. doi:10.12688/f1000research.2-96.v1
5. Deer TR, Hayek SM, Pope JE, et al. The Polyanalgesic Consensus Conference (PACC): recommendations for trialing of intrathecal drug delivery infusion therapy. Neuromodulation. 2017;20(2):133–154. doi:10.1111/ner.12543
6. Brogan SE. Intrathecal therapy for the management of cancer pain. Curr Pain Headache Rep. 2006;10(4):254–259. doi:10.1007/s11916-006-0029-8
7. Bruel BM, Burton AW. Intrathecal therapy for cancer-related pain. Pain Med. 2016;17(12):2404–2421. doi:10.1093/pm/pnw060
8. Upadhyay SP, Mallick PN. Intrathecal drug delivery system (IDDS) for cancer pain management: a review and updates. Am J Hosp Palliat Care. 2012;29(5):388–398. doi:10.1177/1049909111426134
9. Kim EK, Shin JY, Castaneda AM, et al. Retrospective analysis of the financial break-even point for intrathecal morphine pump use in Korea. Korean J Pain. 2017;30(4):272–280. doi:10.3344/kjp.2017.30.4.272
10. Brogan SE, Winter NB, Abiodun A, Safarpour R. A cost utilization analysis of intrathecal therapy for refractory cancer pain: identifying factors associated with cost benefit. Pain Med. 2013;14(4):478–486. doi:10.1111/pme.12060
11. Kim EJ, Moon JY, Kim YC, Park KS, Yoo YJ. Intrathecal morphine infusion therapy in management of chronic pain: present and future implementation in Korea. Yonsei Med J. 2016;57(2):475–481. doi:10.3349/ymj.2016.57.2.475
12. Kumar K, Hunter G, Demeria DD. Treatment of chronic pain by using intrathecal drug therapy compared with conventional pain therapies: a cost-effectiveness analysis. J Neurosurg. 2002;97(4):803–810. doi:10.3171/jns.2002.97.4.0803
13. Bruera E, Schoeller T, Wenk R, et al. A prospective multicenter assessment of the Edmonton staging system for cancer pain. J Pain Symptom Manage. 1995;10(5):348–355. doi:10.1016/0885-3924(95)00052-Z
14. Mercadante S, Caraceni A. Conversion ratios for opioid switching in the treatment of cancer pain: a systematic review. Palliat Med. 2011;25(5):504–515. doi:10.1177/0269216311406577
15. Hayek SM, Deer TR, Pope JE, Panchal SJ, Patel VB. Intrathecal therapy for cancer and non-cancer pain. Pain Physician. 2011;14(3):219–248.
16. Kim JH, Jung JY, Cho MS. Continuous intrathecal morphine administration for cancer pain management using an intrathecal catheter connected to a subcutaneous injection port: a retrospective analysis of 22 terminal cancer patients in korean population. Korean J Pain. 2013;26(1):32–38. doi:10.3344/kjp.2013.26.1.32
17. Hattori S, Sano H, Tanaka K, Yokota M. Intrathecal morphine treatment in advanced cancer pain patients. Masui. 2009;58(11):1384–1392.
18. Zheng S, He L, Yang X, Li X, Yang Z. Evaluation of intrathecal drug delivery system for intractable pain in advanced malignancies: a prospective cohort study. Medicine (Baltimore). 2017;96(11):e6354. doi:10.1097/MD.0000000000006354
19. Kleinmann B, Wolter T. Managing chronic non-malignant pain in the elderly: intrathecal therapy. Drugs Aging. 2019;36(9):789–797. doi:10.1007/s40266-019-00692-7
20. Deer TR, Pope JE, Hanes MC, McDowell GC. Intrathecal therapy for chronic pain: a review of morphine and ziconotide as firstline options. Pain Med. 2019;20(4):784–798. doi:10.1093/pm/pny132
21. Dupoiron D. Intrathecal therapy for pain in cancer patients. Curr Opin Support Palliat Care. 2019;13(2):75–80. doi:10.1097/SPC.0000000000000427
22. Kleinmann B, Wolter T. Intrathecal opioid therapy for non-malignant chronic pain: a long-term perspective. Neuromodulation. 2017;20(7):719–726. doi: 10.1111/ner.12617
23. Reina MA, Lopez-Garcia A, Dittmann M, de Andres JA. Structural analysis of the thickness of human dura mater with scanning electron microscopy. Rev Esp Anestesiol Reanim. 1996;43(4):135–137.
24. Wallace M, Yaksh TL. Characteristics of distribution of morphine and metabolites in cerebrospinal fluid and plasma with chronic intrathecal morphine infusion in humans. Anesth Analg. 2012;115(4):797–804. doi:10.1213/ANE.0b013e3182645dfd
25. Tangen KM, Leval R, Mehta AI, Linninger AA. Computational and in vitro experimental investigation of intrathecal drug distribution: parametric study of the effect of injection volume, cerebrospinal fluid pulsatility, and drug uptake. Anesth Analg. 2017;124(5):1686–1696. doi:10.1213/ANE.0000000000002011
26. Smith TJ, Staats PS, Deer T, et al. Randomized clinical trial of an implantable drug delivery system compared with comprehensive medical management for refractory cancer pain: impact on pain, drug-related toxicity, and survival. J Clin Oncol. 2002;20(19):4040–4049. doi:10.1200/JCO.2002.02.118
27. Adler JA, Lotz NM. Intrathecal pain management: a team-based approach. J Pain Res. 2017;10:2565–2575. doi:10.2147/JPR.S142147
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.