Back to Journals » International Journal of General Medicine » Volume 19
Intraoperative Urine Tests and STONE Score Predict Postoperative SIRS (Systemic Inflammatory Response Syndrome) After PCNL in Patients with Negative Preoperative Urine Culture
Authors Wen J, Liu C, Lu K, Chen W, Gao R
Received 29 December 2025
Accepted for publication 11 May 2026
Published 29 June 2026 Volume 2026:19 592377
DOI https://doi.org/10.2147/IJGM.S592377
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Leonardo Reis
Jinfeng Wen,1,* Changyi Liu,2,3,* Kaixin Lu,2,3,* Wenwei Chen,2,3 Rui Gao2,3
1Department of Urology, Shengli Clinical Medical College of Fujian Medical University, Fujian Provincial Hospital, Fuzhou University Affiliated Provincial Hospital, Fuzhou, 350001, People’s Republic of China; 2Department of Urology, the First Affiliated Hospital, Fujian Medical University, Fuzhou, 350005, People’s Republic of China; 3Department of Urology, National Regional Medical Center, Binhai Campus of the First Affiliated Hospital, Fujian Medical University, Fuzhou, 350212, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Rui Gao, Email [email protected] Jinfeng Wen, Email [email protected]
Objective: This study aimed to identify predictors of postoperative systemic inflammatory response syndrome (SIRS) following percutaneous nephrolithotomy (PCNL) in patients with negative preoperative midstream urine culture (PMUC), and to assess the predictive value of intraoperative renal pelvic urine tests, urinary sediment examination, and the STONE score.
Methods: Clinical data were retrospectively collected from PMUC-negative patients with complex renal calculi who underwent first-stage single-tract PCNL at the First Affiliated Hospital of Fujian Medical University. Patients were classified into SIRS and non-SIRS groups according to the occurrence of postoperative SIRS within 72 hours. SIRS was used as an indicator of early postoperative systemic inflammatory response, as not all cases met Sepsis-3 criteria for organ dysfunction. Univariable and multivariable logistic regression analyses were performed to identify independent predictors of postoperative SIRS. A nomogram was subsequently developed and assessed for calibration and discrimination.
Results: A total of 126 patients (89 males and 37 females) were included, and 29 developed postoperative SIRS. Multivariate logistic regression identified intraoperative leukocyte esterase (LE) positivity (OR = 2.324, 95% CI 1.164– 4.641, p = 0.017), elevated intraoperative white blood cell (WBC) count (OR = 5.855, 95% CI 1.209– 28.357, p = 0.028), positive stone culture (OR = 15.929, 95% CI 1.792– 141.600, p = 0.013), and higher STONE score (OR = 1.948, 95% CI 1.125– 3.375, p < 0.017) as independent risk factors. The nomogram demonstrated good calibration (Hosmer–Lemeshow p > 0.05) and strong discriminative ability, with an AUC of 0.935.
Conclusion: Intraoperative leukocyte esterase, intraoperative white blood cell count, positive stone culture, and higher STONE score were independently associated with postoperative SIRS after first-stage PCNL in PMUC-negative patients. The nomogram may assist in early risk stratification in this population.
Keywords: percutaneous nephrolithotomy, postoperative SIS, urinary tract infection, urinary sediment, STONE score
Background
Percutaneous nephrolithotomy (PCNL) is widely recognized as the standard surgical treatment for kidney stones measuring ≥20 mm.1 Despite its established efficacy and safety, postoperative complications, including systemic inflammatory response syndrome (SIRS), remain clinically relevant. Severe postoperative systemic inflammatory responses may progress to life-threatening conditions in a subset of patients.2 Early identification of high-risk patients is therefore important for reducing morbidity and mortality.
Infected urine and stones are recognized as important sources of pathogenic bacteria contributing to postoperative infectious complications after PCNL.2 Accordingly, accurate perioperative identification of infectious status is essential for risk assessment. Preoperative midstream urine culture (PMUC) is the most commonly used test for evaluating infection risk in PCNL candidates. Although PMUC positivity is associated with increased postoperative infectious risk, patients with negative PMUC may still develop postoperative SIRS despite prophylactic antibiotics.3 This may be related to undetected upper urinary tract infection in the presence of obstruction, leading to false-negative results. In addition, bacteria embedded within calculi may be protected from antibiotics and released during lithotripsy. As a result, negative PMUC alone may underestimate perioperative infectious risk and delay early recognition.3,4
Compared with PMUC, renal pelvic urine culture (RPUC) and stone culture (SC) are considered more representative of upper urinary tract infection. However, both require at least 24 hours for culture results,5,6 limiting their role in intraoperative decision-making. In contrast, intraoperative renal pelvic urine tests, including leukocyte esterase (LE), white blood cell (WBC) count, and urinary sediment examination, provide rapid information that may support early risk assessment. Renal pelvic urine more directly reflects the upper urinary tract environment than bladder urine, as it avoids contamination from the lower urinary tract and reduces the influence of voiding conditions. Although urine-based tests provide useful diagnostic information with relatively good performance,7 preoperative results may still be affected by obstruction-related sampling bias. Therefore, intraoperative renal pelvic urine analysis may better reflect the true status of the upper urinary tract, although its predictive value for postoperative infectious complications remains to be fully defined.
The STONE score, proposed by Okhunov,8 is widely used to assess stone complexity and predict perioperative outcomes such as operative time and stone-free rate after PCNL.9,10 In single-tract PCNL, higher STONE scores have been associated with lower stone-free rates, as confirmed by Kumari et al, who reported an AUC of 0.680 for predicting stone-free status in 147 patients.11 More recent studies have also suggested its potential value in predicting postoperative infectious complications after PCNL.4,12 Tang et al4 analyzed 758 patients and found that the STONE score was associated with postoperative SIRS (OR = 1.902, 95% CI 1.473–2.457) and severe postoperative infectious complications requiring intensive care or organ support (OR = 1.455, 95% CI 1.064–1.988), with AUCs of 0.784 and 0.772, respectively. However, this study included both PMUC-positive and PMUC-negative patients, and subgroup performance in PMUC-negative patients was not specifically evaluated. Therefore, the predictive value of the STONE score in this clinically challenging subgroup remains uncertain.
Therefore, this study aimed to identify predictors of postoperative SIRS after PCNL in patients with negative PMUC and to assess whether combining intraoperative renal pelvic urine tests with the STONE score could improve risk stratification. A more accurate assessment strategy may support perioperative decision-making and improve early identification of patients at risk of postoperative infectious complications.
Patients and Methods
Study Population
This retrospective study included patients with complex renal calculi who were negative for preoperative midstream urine culture and underwent single-session, single-tract percutaneous nephrolithotomy (PCNL) at the Department of Urology, First Affiliated Hospital of Fujian Medical University, between September 2022 and June 2023. All procedures were performed by two experienced urologists using a standard PCNL technique with a 24–30 Fr tract. A single dose of prophylactic antibiotics was administered 30 minutes prior to the procedure.
The study was approved by the Ethics Review Board of the First Affiliated Hospital of Fujian Medical University (No. 2022–084-2). The study was conducted in accordance with the Declaration of Helsinki and institutional ethical standards. This retrospective study involved analysis of existing clinical data and did not involve any intervention beyond routine patient care. No additional procedures, interventions, or specimen collection were performed for research purposes. All clinical and laboratory data were extracted from the hospital information system. Urine sediment analysis (including white blood cell and bacterial counts), leukocyte esterase testing, and microbiological culture results were originally obtained as part of routine clinical diagnostics. Renal pelvic urine was collected intraoperatively during standard percutaneous nephrolithotomy (PCNL) following successful calyceal access, and stone specimens were obtained during routine lithotripsy procedures according to standard surgical practice. For this study, all laboratory measurements were based on residual clinical specimens and previously generated diagnostic results, without any additional testing or modification of standard clinical management. All data were de-identified prior to analysis. The requirement for informed consent was waived by the institutional ethics committee due to the retrospective design and use of anonymized data.
Intraoperative Specimen Collection
Under ultrasound and fluoroscopic guidance, a standard 18-gauge percutaneous puncture needle was used to establish renal access via the posterior calyceal system. After successful access to the renal pelvis, renal pelvic urine was aspirated into a sterile syringe and sent for bacterial culture, routine urinalysis, and urine sediment examination. Calculus specimens collected during lithotripsy were washed five times with 5 mL of physiological saline, mechanically processed, and immediately submitted for bacterial culture.
Renal pelvic urine samples were obtained immediately after successful renal access and transported to the laboratory within 30 minutes. Leukocyte esterase (LE) was assessed semi-quantitatively (negative, +, ++, +++) using an automated analyzer, and white blood cell (WBC) count was quantified using a counting chamber (cells/μL), with all findings confirmed by microscopy. Urine specimens were cultured on blood agar and MacConkey agar at 37°C for 24–48 hours, with significant bacteriuria defined as ≥104 CFU/mL.
Inclusion and Exclusion Criteria
Inclusion criteria were: age over 18 years; presence of complex renal calculi confirmed by kidney-ureter-bladder radiography or computed tomography, meeting the European Association of Urology guidelines for PCNL; and negative preoperative midstream urine culture. Exclusion criteria were: positive preoperative midstream urine culture; presence of urinary stents, nephrostomy tubes, or indwelling catheters; multi-tract PCNL; complex stone morphologies typically requiring multiple tracts or staged procedures, including complete staghorn stones, stones involving more than three calyces, and calyceal diverticular stones; renal failure; preoperative fever; history of prior urinary system surgery or procedures; concurrent bladder calculi or tumors; special conditions including pregnancy, duplex kidneys, duplex ureters, or horseshoe kidney; and incomplete perioperative clinical data.
Data Collection
Demographic and clinical information, including age, sex, body mass index, and history of diabetes, was collected. Stone characteristics were assessed using the STONE score based on preoperative non-contrast computed tomography (CT).
Laboratory data included preoperative blood routine, urine routine, urine sediment examination, intraoperative renal pelvic urine analysis, stone culture, and postoperative blood routine and C-reactive protein (CRP) levels. Urine sediment examination was performed using standardized microscopy after centrifugation at 1500 rpm for 5 minutes. White blood cell (WBC) counts and bacterial counts in urine samples were quantified under high-power fields and reported as cells/μL using a standardized microscopic counting method. Leukocyte esterase (LE) was measured using a semi-quantitative urine dipstick test and recorded as negative, +, ++, or +++.
Renal pelvic urine and stone specimens were additionally submitted for microbiological culture according to institutional protocols. Significant bacteriuria in renal pelvic urine culture (RPUC) was defined as ≥104 CFU/mL, while any bacterial growth in stone culture (SC) was considered positive.
Operative time was defined as the total duration of the procedure, from the initial insertion of the ureteroscope for retrograde ureteral catheter placement to the completion of nephrostomy tube placement following percutaneous nephrolithotomy (PCNL). Postoperative vital signs were recorded.
Postoperative systemic inflammatory response syndrome (SIRS), defined as the presence of ≥2 criteria within 72 hours after surgery, was used as the primary outcome measure, since not all patients met the Sepsis-3 definition requiring organ dysfunction.13 SIRS was used as an early and sensitive indicator of postoperative systemic inflammatory response. Patients were classified into the SIRS group if they met ≥2 of the following criteria:1 temperature >38°C or <36°C;2 heart rate >90 beats/min;3 respiratory rate >20 breaths/min or PaCO2 <32 mmHg;4 WBC >12,000/μL or <4,000/μL, or >10% immature neutrophils. Patients who developed SIRS beyond 72 hours postoperatively were excluded. Patients meeting these criteria were assigned to the SIRS group, while the remaining patients were classified as the non-SIRS group.
Statistical Analysis
Statistical analyses were performed using SPSS version 25.0 and R software. The Kolmogorov–Smirnov test was used to assess the normality of continuous variables. Normally distributed variables were compared using independent t-tests, and non-normally distributed variables using Mann–Whitney U-tests. Categorical variables were analyzed using chi-square or Fisher’s exact tests. Variables with statistically significant differences in univariate analysis were included in multivariate logistic regression with backward stepwise selection. A nomogram was constructed to predict postoperative SIRS based on the multivariate results. Model performance was evaluated using receiver operating characteristic curves, calibration curves, and the Hosmer-Lemeshow goodness-of-fit test. A p-value less than 0.05 was considered statistically significant.
Results
Clinical Evolution of the Entire Cohort
All 126 patients successfully underwent single-tract PCNL. Within 72 hours after surgery, 29 patients (23.0%) developed postoperative SIRS and were assigned to the SIRS group, while the remaining 97 patients (77.0%) did not meet SIRS criteria.
The median hospital stay was 5 days (IQR 4–6) in the non-SIRS group. In patients who developed SIRS, the median time to onset was 14.5 hours (IQR 8.0–22.5), and fever was the most frequent initial symptom (89.7%). Two patients (1.6% of the entire cohort) progressed to septic shock and required ICU care. No in-hospital deaths occurred. Hospitalization was significantly longer in the SIRS group compared with the non-SIRS group (9 vs. 5 days, p < 0.001).
Univariate analysis of clinical factors associated with postoperative SIRS after PCNL in PMUC-negative patients
A total of 182 patients with complex renal stones underwent single-tract PCNL during the study period, and 126 were finally included after applying the selection criteria. Postoperative SIRS occurred in 29 patients (23.0%). Among them, 2 patients (6.9% of the SIRS group; 1.6% overall) developed septic shock and required ICU management. All patients recovered following appropriate treatment, including antibiotic escalation and supportive care, and no in-hospital mortality was observed.
Univariate regression analysis identified several factors associated with the development of postoperative SIRS in PMUC-negative patients undergoing PCNL. Female gender (p = 0.011), positive preoperative leukocyte esterase (LE) (p = 0.004), elevated preoperative bacterial count (p < 0.001), intraoperative LE (p < 0.001), intraoperative white blood cell (WBC) count (p < 0.001), increased intraoperative urinary bacteria (p < 0.001), positive renal pelvis urine culture (RPUC) (p < 0.001), positive stone culture (SC) (p < 0.001), longer operative time (p < 0.001), higher STONE score (p < 0.001), and elevated postoperative C-reactive protein (CRP) (p < 0.001) were all significantly associated with postoperative SIRS. In contrast, age (p = 0.409), body mass index (p = 0.907), history of diabetes (p = 0.777), preoperative nitrite (p = 0.906), preoperative WBC (p = 0.058), and intraoperative nitrite in renal pelvic urine (p = 0.230) were not significantly different between groups (Table 1). Both preoperative and intraoperative urinary parameters, together with surgical and stone-related factors, were associated with postoperative SIRS.
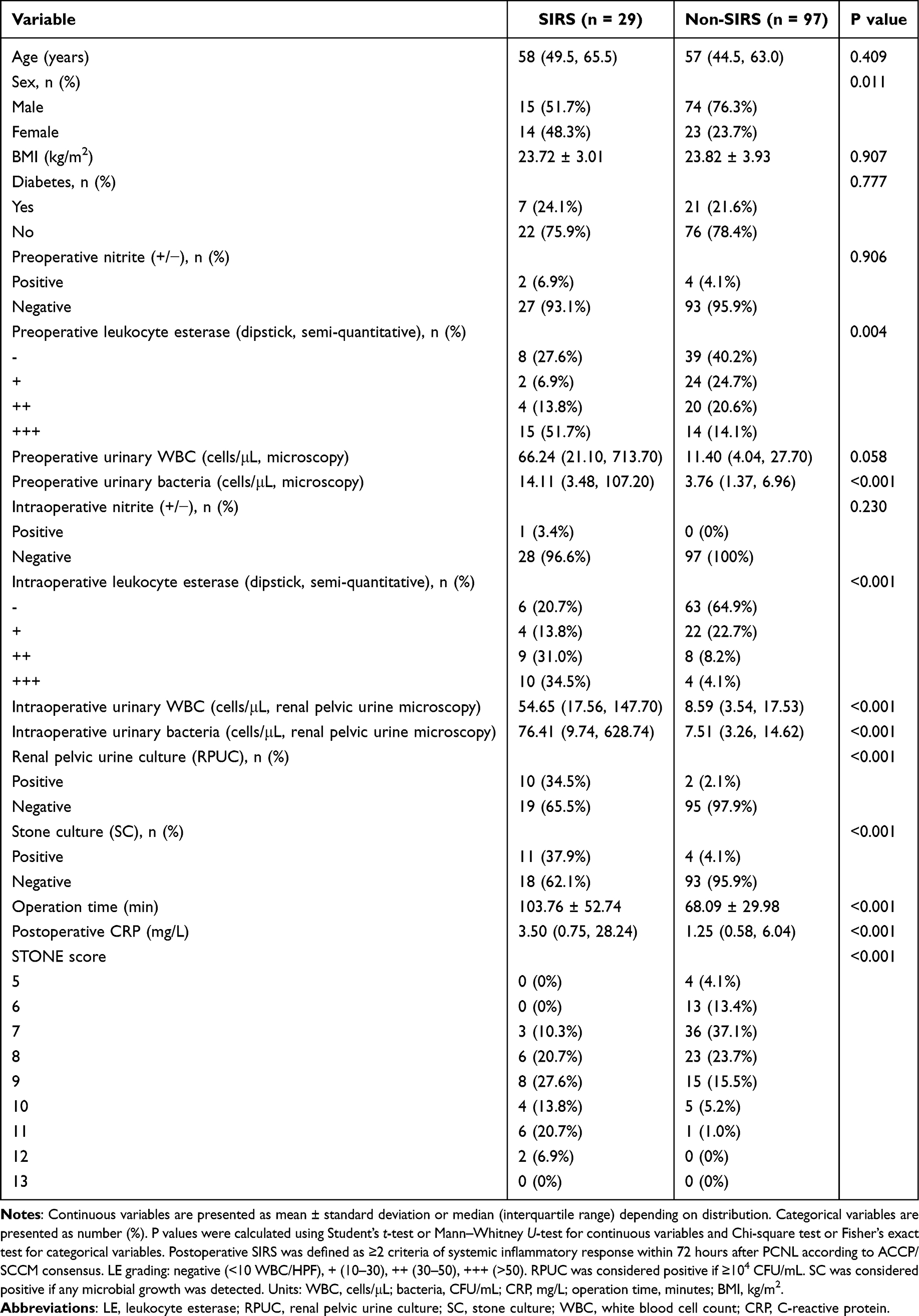 |
Table 1 Univariate Analysis of Clinical Factors Associated with Postoperative SIRS After PCNL in PMUC-Negative Patients |
Optimal Cutoffs for Clinical Factors via ROC Curve
Variables identified as significant in univariate analysis were further evaluated using receiver operating characteristic (ROC) curve analysis. Optimal cutoff values were determined for preoperative bacterial count, intraoperative WBC, intraoperative bacterial count, operative time, and postoperative CRP, which were 8.27, 12.76, 18.42, 95.50, and 27.02, respectively. Based on these thresholds, patients were categorized as positive or negative for each variable (Table 2), with values above the cutoff defined as positive and those below defined as negative. These dichotomized variables were then entered into multivariate analysis (Figure 1).
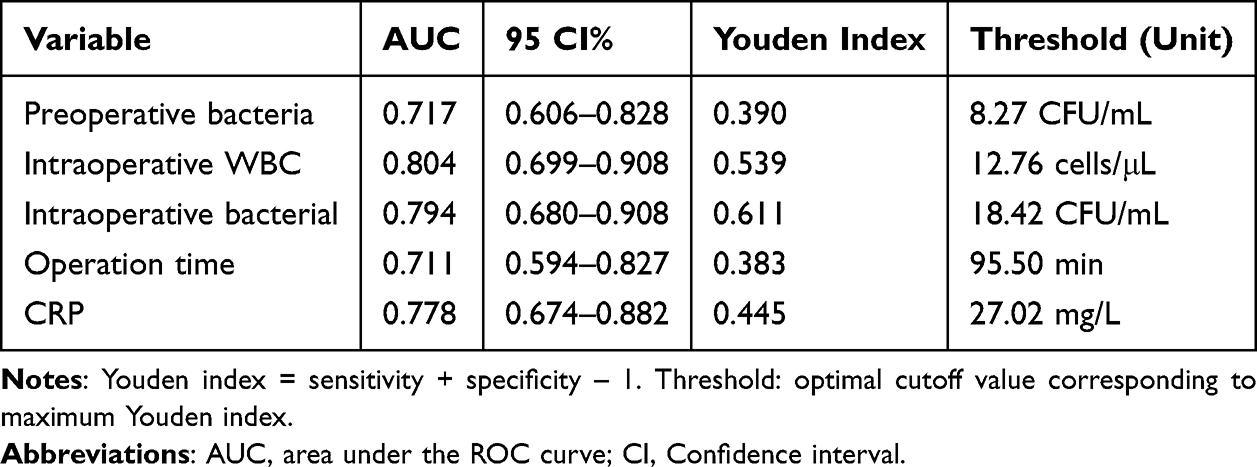 |
Table 2 AUC and Optimal Cutoff Value of Perioperative Indicators |
 |
Figure 1 Receiver operating characteristic (ROC) curves of clinical factors significantly associated with postoperative SIRS in univariate analysis. The area under the curve (AUC) indicates the predictive performance of each factor in PMUC-negative patients undergoing PCNL. |
Multivariate Analysis of Independent Risk Factors for Postoperative SIRS After PCNL in PMUC-Negative Patients
Multivariate logistic regression identified positive intraoperative leukocyte esterase (LE) (defined as above the ROC-derived cutoff; p = 0.017, OR = 2.324, 95% CI 1.164–4.641), positive intraoperative white blood cell (WBC) count (p = 0.028, OR = 5.855, 95% CI 1.209–28.357), positive stone culture (SC) (p = 0.013, OR = 15.929, 95% CI 1.792–141.600), and higher STONE score (per point increase; p < 0.017, OR = 1.948, 95% CI 1.125–3.375) as independent risk factors for postoperative SIRS after PCNL (Table 3).
 |
Table 3 Multivariate Logistic Regression Analysis of Independent Predictors of Postoperative SIRS After PCNL in PMUC-Negative Patients |
Establishment and Evaluation of the Nomogram Model for Postoperative SIRS After PCNL
Based on multivariate logistic regression results, a nomogram was constructed to predict the probability of postoperative SIRS after PCNL. In the model, positive intraoperative white blood cell (WBC) count in renal pelvic urine (above the ROC-derived cutoff) contributed 24.42 points. Each increment in qualitative intraoperative leukocyte esterase (LE) added 11.11 points. Positive stone culture (SC) contributed 38.17 points, and each one-point increase in STONE score contributed 14.29 points (Figure 2). The model showed good calibration, with a Hosmer–Lemeshow test result of χ2 = 9.416 (p = 0.224) (Figure 3). Discrimination was high, with an AUC of 0.935 (95% CI 0.890–0.980, p < 0.001) (Figure 4).
 |
Figure 2 Nomogram for predicting postoperative SIRS in PMUC-negative patients undergoing PCNL. Points are assigned to independent risk factors identified by multivariate logistic regression (intraoperative leukocyte esterase, intraoperative WBC, positive stone culture, and STONE score). The total score corresponds to the predicted probability of postoperative SIRS. |
 |
Figure 3 ROC curve of the nomogram prediction model (combined multivariate model). The AUC (0.935, 95% CI 0.890–0.980, p<0.001) demonstrates the model’s discriminatory ability to identify patients at risk of postoperative SIRS. |
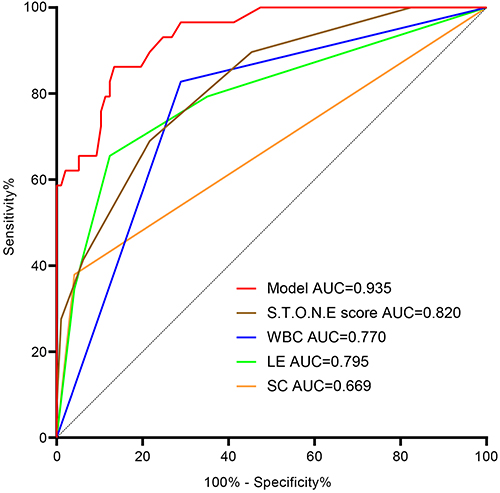 |
Figure 4 Calibration curve of the nomogram prediction model. Predicted probabilities are compared with observed incidences of postoperative SIRS (defined as ≥2 criteria within 72 hours). The model shows good agreement, supported by the Hosmer–Lemeshow test (χ2=9.416, p=0.224). |
Discussion
The current gold standard for kidney stones larger than 20 mm is percutaneous nephrolithotomy (PCNL).1 However, postoperative infectious complications, including fever, SIRS, and infection-related systemic inflammatory responses, remain clinically relevant challenges. In this cohort, 23.0% of patients developed postoperative SIRS (defined as ≥2 SIRS criteria within 72 hours), which is consistent with previous reports from other centers.3,14 Although female gender has been suggested as a potential risk factor due to anatomical and hormonal characteristics,15–17 this association was not observed in our multivariate analysis, possibly related to the exclusion of PMUC-positive patients. The contribution of upper versus lower urinary tract infection in excluded populations remains uncertain and requires further investigation.
Escherichia coli was the most frequently identified pathogen in culture-positive upper urinary tract specimens, including both renal pelvis urine culture (RPUC) and stone culture (SC), consistent with prior studies.18,19 PMUC, RPUC, and SC have been reported as predictors of postoperative SIRS and infection-related systemic complications.20 However, PMUC positivity does not necessarily correspond to postoperative SIRS (≥2 criteria within 72 hours), which may be influenced by preoperative antibiotic exposure or limited reflection of upper tract microbiota in midstream urine. In the present cohort, despite all patients being PMUC-negative, 11.9% were SC-positive, 9.5% were RPUC-positive, and 7.1% were positive for both, while 23% developed SIRS. These findings further support the limited predictive value of PMUC alone. Consistent with previous studies,4,21–23 SC remained an independent predictor of postoperative SIRS, underscoring the importance of stone microbiology in risk stratification.
Preoperative antibiotic administration may reduce detectable RPUC positivity, particularly in obstructed systems, but is unlikely to eliminate bacteria embedded within stones, which may subsequently contribute to systemic inflammatory responses. In addition, some patients with negative SC and RPUC still developed postoperative SIRS, which may be related to false-negative cultures24 or endotoxin release from infected stones.25 These observations suggest that intraoperative microbiological assessment may complement preoperative testing. Preoperative urinary markers such as WBC, leukocyte esterase (LE), and nitrite have been associated with postoperative infectious complications; however, their reliability may be reduced in the presence of obstruction or altered urinary drainage. In this study, intraoperative renal pelvic urine WBC elevation (above ROC-derived cutoff) and positive LE (above ROC threshold) were independent predictors, suggesting that intraoperative sampling may better reflect upper urinary tract inflammatory status.
The STONE score was also identified as an independent predictor of postoperative SIRS. This CT-based scoring system has been validated for predicting stone-free rates and postoperative complications.26 As previously reported by Tang et al4 and Yang et al,11 the STONE score is associated with both SIRS and infection-related complications after PCNL. Our findings extend these observations to a strictly PMUC-negative population, supporting its value in preoperative risk stratification.
The incidence of postoperative SIRS in this cohort was 23.0%, which is higher than the reported 0.3%–4.7% in the general PCNL population.2 This discrepancy is likely related to the inclusion of patients with complex stones and higher STONE scores, which are associated with longer operative time, more extensive intrarenal manipulation, and increased bacterial burden. In this study, 11.9% of patients had positive stone cultures and 9.5% had positive renal pelvis urine cultures, despite all being preoperative PMUC-negative. This further indicates that a negative midstream urine culture does not exclude upper urinary tract colonization. Bacteria may persist within the stone matrix or behind obstructed systems and escape preoperative antibiotic eradication, with potential release during lithotripsy triggering systemic inflammatory responses.21 In addition, a negative PMUC may reduce clinical suspicion and delay early recognition of postoperative infection.
Regarding outcome definition, postoperative SIRS (≥2 criteria within 72 hours) was used as the primary endpoint rather than Sepsis-3–defined sepsis. This more sensitive definition may include patients with mild systemic inflammatory responses. Consistently, only 2 of 29 SIRS-positive patients (6.9%) progressed to septic shock requiring ICU admission, indicating that most cases represented early or mild systemic inflammation rather than organ dysfunction–associated sepsis. All patients recovered following appropriate management, and no mortality occurred.
As a single-center retrospective study, selection bias cannot be excluded, and external validation is required. The relatively high incidence observed in this study highlights the risk profile of PMUC-negative patients with complex stones. Conventional preoperative evaluation alone appears insufficient for accurate risk stratification in this subgroup. This gap supports the use of a combined model incorporating intraoperative urinary markers and the STONE score for early identification of high-risk patients.
Several limitations should be acknowledged. This study is retrospective and single-center with a limited sample size. Patients with extremely high stone complexity (STONE score of 13) were not included, which may introduce selection bias. In addition, postoperative SIRS was used as a surrogate endpoint rather than Sepsis-3–defined sepsis with organ dysfunction. Although this approach improves sensitivity for early detection, it may overestimate clinically significant infectious events. Future prospective multicenter studies using standardized Sepsis-3 criteria are needed to validate these findings and further clarify the role of stone microbiology in infection pathogenesis. Intraoperative culture-guided strategies may also be explored to determine whether they can reduce the incidence and severity of postoperative infectious complications.
Conclusion
In this study, four independent risk factors for postoperative SIRS after PCNL in patients with negative preoperative urine cultures were identified, including positive intraoperative leukocyte esterase (above the ROC-derived threshold), elevated white blood cell count in renal pelvic urine (above the ROC cutoff), higher STONE score, and positive stone culture (detectable bacteria within stones). Based on these variables, a nomogram was developed to estimate individual risk of postoperative SIRS. The combination of intraoperative renal pelvic urine parameters and the STONE score provided more comprehensive information on infection risk than preoperative urine testing alone. These findings suggest that intraoperative urinary assessment, together with stone complexity scoring, may improve early risk stratification in PMUC-negative patients undergoing PCNL. Further multicenter studies are needed to validate these findings and to clarify the role of stone microbiology in the development of postoperative infectious complications.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author via Email request.
Ethics Approval
The study was approved by the Ethics Review Board of the First Affiliated Hospital of Fujian Medical University (No. 2022-084-2). The study was conducted in accordance with the Declaration of Helsinki and institutional ethical standards. No additional procedures or sample collection were performed for research purposes beyond routine clinical care.
Consent to Participate Declaration
Due to the retrospective design and the use of de-identified clinical data, the requirement for written informed consent was waived by the ethics committee.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
1. Joint Funds for the Innovation of Science and Technology, Fujian Province (No.2023Y9040); 2. Natural Science Foundation of Fujian Province (No.2023J01593); 3.Youth Scientific Research Project of Fujian Provincial Health Commission (No.2023QNA028).
Disclosure
Jinfeng Wen, Changyi Liu, and Kaixin Lu are co-first authors for this study. The authors declare that they have no conflicts of interest in this work.
References
1. Kim K, Alam SM, Kuo F, et al. Molecular heterogeneity and immune infiltration drive clinical outcomes in upper tract urothelial carcinoma. Europ Urol. 2025;87(3):342–11. doi:10.1016/j.eururo.2024.10.024
2. Wang C, Xu R, Zhang Y, et al. Nomograms for predicting the risk of sirs and urosepsis after uroscopic minimally invasive lithotripsy. Biomed Res Int. 2022;2022:6808239. doi:10.1155/2022/6808239
3. Liu M, Chen J, Gao M, et al. Preoperative midstream urine cultures vs renal pelvic urine culture or stone culture in predicting systemic inflammatory response syndrome and urosepsis after percutaneous nephrolithotomy: a systematic review and meta-analysis. J Endourol. 2021;35(10):1467–1478. doi:10.1089/end.2020.1140
4. Tang Y, Zhang C, Mo C, Gui C, Luo J, Wu R. Predictive model for systemic infection after percutaneous nephrolithotomy and related factors analysis. Front Surg. 2021;8:696463. doi:10.3389/fsurg.2021.696463
5. Grossmann NC, Schuettfort VM, Betschart J, et al. Risk factors for concomitant positive midstream urine culture in patients presenting with symptomatic ureterolithiasis. Urolithiasis. 2022;50(3):293–302. doi:10.1007/s00240-022-01323-4
6. Tzou DT, Stern KL, Duty BD, et al. Heterogeneity in stone culture protocols and endourologist practice patterns: a multi-institutional survey. Urolithiasis. 2022;51(1):15. doi:10.1007/s00240-022-01373-8
7. Ruan S, Chen Z, Zhu Z, Zeng H, Chen J, Chen H. Value of preoperative urine white blood cell and nitrite in predicting postoperative infection following percutaneous nephrolithotomy: a meta-analysis. Transl Androlo Urol. 2021;10(1):195–203. doi:10.21037/tau-20-930
8. Okhunov Z, Friedlander JI, George AK, et al. S.T.O.N.E. nephrolithometry: novel surgical classification system for kidney calculi. Urology. 2013;81(6):1154–1159. doi:10.1016/j.urology.2012.10.083
9. Sigdel B, Shrestha S, Maskey P. Predicting the outcome of mini percutaneous nephrolithotomy using STONE nephrolithometry score-a single-center experience. Urolithiasis. 2022;51(1):14. doi:10.1007/s00240-022-01379-2
10. Biswas K, Gupta SK, Tak GR, Ganpule AP, Sabnis RB, Desai MR. Comparison of STONE score, Guy’s stone score and Clinical Research Office of the Endourological Society (CROES) score as predictive tools for percutaneous nephrolithotomy outcome: a prospective study. BJU Int. 2020;126(4):494–501. doi:10.1111/bju.15130
11. Illahi Bux K, Rizwan Ahmed R, Farooq F, et al. Clinical utility of S.T.O.N.E, Guy’s scoring system, and renal stone complexity scoring in predicting outcome of single-tract percutaneous nephrolithotomy. Cureus. 2023;15(12):e50983. doi:10.7759/cureus.50983
12. He Z, Tang F, Lei H, Chen Y, Zeng G. Risk factors for systemic inflammatory response syndrome after percutaneous nephrolithotomy. Progres en urologie. 2018;28(12):582–587. doi:10.1016/j.purol.2018.06.006
13. Singer M, Deutschman CS, Seymour CW, et al. The Third International consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
14. Zhu Z, Cui Y, Zeng H, et al. The evaluation of early predictive factors for urosepsis in patients with negative preoperative urine culture following mini-percutaneous nephrolithotomy. World J Urol. 2020;38(10):2629–2636. doi:10.1007/s00345-019-03050-9
15. Ye Z, Zeng G, Yang H, et al. The status and characteristics of urinary stone composition in China. BJU Int. 2020;125(6):801–809. doi:10.1111/bju.14765
16. Xun Y, Yang Y, Yu X, Li C, Lu J, Wang S. A preoperative nomogram for sepsis in percutaneous nephrolithotomy treating solitary, unilateral and proximal ureteral stones. PeerJ. 2020;8:e9435. doi:10.7717/peerj.9435
17. Liu J, Yang Q, Lan J, Hong Y, Huang X, Yang B. Risk factors and prediction model of urosepsis in patients with diabetes after percutaneous nephrolithotomy. BMC Urol. 2021;21(1):74. doi:10.1186/s12894-021-00799-3
18. Yang Z, Lin D, Hong Y, et al. The effect of preoperative urine culture and bacterial species on infection after percutaneous nephrolithotomy for patients with upper urinary tract stones. Sci Rep. 2022;12(1):4833. doi:10.1038/s41598-022-08913-7
19. Singh I, Shah S, Gupta S, Singh NP. Efficacy of intraoperative renal stone culture in predicting postpercutaneous nephrolithotomy urosepsis/systemic inflammatory response syndrome: a prospective analytical study with review of literature. J Endourol. 2019;33(2):84–92. doi:10.1089/end.2018.0842
20. Zhou G, Zhou Y, Chen R, et al. The influencing factors of infectious complications after percutaneous nephrolithotomy: a systematic review and meta-analysis. Urolithiasis. 2022;51(1):17. doi:10.1007/s00240-022-01376-5
21. Wollin DA, Joyce AD, Gupta M, et al. Antibiotic use and the prevention and management of infectious complications in stone disease. World J Urol. 2017;35(9):1369–1379. doi:10.1007/s00345-017-2005-9
22. Rivera M, Viers B, Cockerill P, Agarwal D, Mehta R, Krambeck A. Pre- and postoperative predictors of infection-related complications in patients undergoing percutaneous nephrolithotomy. J Endourol. 2016;30(9):982–986. doi:10.1089/end.2016.0191
23. Mishra A, Mittal J, Tripathi S, Paul S. Factors predicting infective complications following percutaneous nephrolithotomy and retrograde intrarenal surgery according to systemic inflammatory response syndrome and quick sequential organ failure assessment: a prospective study. Urol Annals. 2023;15(3):295–303. doi:10.4103/ua.ua_150_22
24. Liu J, Zhou C, Gao W, Huang H, Jiang X, Zhang D. Does preoperative urine culture still play a role in predicting post-PCNL SIRS? A retrospective cohort study. Urolithiasis. 2020;48(3):251–256. doi:10.1007/s00240-019-01148-8
25. Paterson RF, Kuo RL, Lingeman JE. Staghorn calculus endotoxin expression in sepsis. Urology. 2003;62(1):197;authorreply–8. doi:10.1016/S0090-4295(02)02132-5
26. Srivastava A, Yadav P, Madhavan K, et al. Inter-observer variability amongst surgeons and radiologists in assessment of Guy’s Stone Score and S.T.O.N.E. nephrolithometry score: a prospective evaluation. Arab J Urol. 2019;18(2):118–123. doi:10.1080/2090598X.2019.1703278
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.