Back to Journals » Drug Design, Development and Therapy » Volume 19
Intraoperative Dexmedetomidine Enhances Postoperative Microcirculation and Reduces Acute Kidney Injury in Cardiac Surgery: A Double-Blind Randomized Trial
Authors Shih PY, Wu TT, Chan KC ![]() , Hsu RB, Chang CT, Chou WH, Wu CY
, Hsu RB, Chang CT, Chou WH, Wu CY ![]()
Received 19 May 2025
Accepted for publication 10 September 2025
Published 18 September 2025 Volume 2025:19 Pages 8451—8462
DOI https://doi.org/10.2147/DDDT.S541433
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Tamer Ibrahim
Po-Yuan Shih,1 Tsung-Ta Wu,2 Kuang-Cheng Chan,1 Ron-Bin Hsu,3 Ching-Tao Chang,2 Wei-Han Chou,1 Chun-Yu Wu2
1Department of Anesthesiology, National Taiwan University Hospital, Taipei, Taiwan; 2Department of Anesthesiology, National Taiwan University Hospital Hsinchu Branch, Hsinchu, Taiwan; 3Department of Cardiovascular Surgery, National Taiwan University Hospital, Taipei, Taiwan
Correspondence: Chun-Yu Wu, Department of Anesthesiology, National Taiwan University Hospital Hsinchu Br, No. 25, Lane 442, Sec.1, Jingguo Road, Hsinchu, 300, Taiwan, Tel +886-2-23562158, Fax +886-2-23415736, Email [email protected]
Purpose: Dexmedetomidine, an alpha-2 adrenergic agonist, has shown potential benefits in various surgical settings, but its impact on microcirculation and renal function in cardiac surgery patients remains unclear.
Patients and Methods: This randomized, controlled, double-blind clinical trial was conducted at a single university hospital. Seventy patients undergoing non-emergency cardiac and aortic surgery requiring cardiopulmonary bypass were enrolled, and 68 patients were included in the final analysis. Patients were randomized to receive either dexmedetomidine (0.5 mcg/kg loading dose, followed by 0.5 mcg/kg/h) or saline. The infusion of dexmedetomidine or saline began at anesthesia induction and continued until the end of surgery. Key microcirculatory variables—total vessel density, proportion of perfused vessels, perfused vessel density, De Backer’s score, microvascular flow index, and heterogeneity index—were measured at five time points: baseline, 1 hour after cardiopulmonary bypass, 1 hour after arrival in the intensive care unit, 24 hours after surgery, and 48 hours after surgery. Data were analyzed using a mixed-effects model with Tukey’s Honestly Significant Difference correction. Intraoperative urine output, the incidence of postoperative acute kidney injury, and other postoperative complications were also compared.
Results: Patients in the dexmedetomidine group maintained higher postoperative proportion of perfused vessels and perfused vessel density compared to the saline group, with a significant interaction effect for perfused vessel density. Baseline perfused vessel density was comparable between the two study groups (17.5 [15.9– 18.6] vs 18.0 [16.1– 19.8] mm/mm², p = 0.540). At 48 hours postoperatively, patients in the dexmedetomidine group had significantly higher PVD values than those in the saline group (17.0 [15.0– 19.0] vs 15.6 [13.7– 16.9] mm/mm²; P = 0.041). The dexmedetomidine group also had significantly higher intraoperative urine output (950 vs 605 mL, p = 0.002). Additionally, the incidence of postoperative acute kidney injury was significantly lower in the dexmedetomidine group (11.8% vs 50%, p = 0.001).
Conclusion: Intraoperative dexmedetomidine infusion during cardiac surgery is associated with higher postoperative microcirculatory state and a reduced incidence of acute kidney injury.
Plain Language Summary: This study examined whether a drug called dexmedetomidine can help improve small blood flow (microcirculation) and protect kidney function during heart surgery. Heart surgeries that use a heart-lung machine can disturb blood flow to tiny vessels and may lead to complications like acute kidney injury (AKI). Dexmedetomidine is a commonly used sedative with anti-inflammatory and organ-protective effects.
In this single center study, 68 patients undergoing cardiac or aortic surgery were randomly assigned to receive either dexmedetomidine or a saline during surgery. The researchers measured blood flow in the small vessels under the tongue at several time points and tracked urine output and kidney function after surgery. Patients who received dexmedetomidine showed better blood flow in their small vessels and had more urine output during surgery. Most importantly, they had a significantly lower chance of developing AKI compared to those who received saline (11.8% vs 50%).
These results suggest that using dexmedetomidine during heart surgery may improve microcirculation and help protect the kidneys. This could lead to better recovery and fewer complications after surgery. The findings provide valuable insight for doctors seeking safer anesthesia options and ways to reduce organ damage in heart surgery patients.
Keywords: dexmedetomidine, microcirculation, acute kidney injury, cardiac surgery
Introduction
Cardiac surgery, particularly when cardiopulmonary bypass is involved, triggers systemic inflammation and induces severe hemodynamic alterations, both of which can affect microcirculation and potentially lead to organ dysfunction such as acute kidney injury (AKI).1–3 Furthermore, changes in microcirculation during cardiac surgery are correlated with prolonged stays in the postoperative intensive care unit and high mortality rates within 30 days.4 Treatments for microcirculatory disturbances during cardiac surgery include developing better hemodynamic protocols and investigating potential pharmacological treatments.4 Because real-time perioperative microcirculatory monitoring to guide hemodynamic management remains challenging,1 identifying potential pharmacological interventions is clinically relevant.
Dexmedetomidine, a highly selective alpha-2 adrenergic agonist, is widely applied as a sedative agent in critically ill patients and as an adjuvant to general anesthesia due to its effects on analgesia, anxiolysis, sympatholysis, and anti-inflammation.5 Higher doses (eg, 0.5 μg/kg/h) have been explored for potential organ-protective effects,6–8 which exceed those typically used for sedation purposes. These effects may not only promote postoperative recovery5,9 but also improve subcutaneous and intestine microcirculation, as suggested by animal studies in conditions such as sepsis10,11 and reperfusion injury-induced acute kidney injury.12 However, evidence supporting dexmedetomidine-induced microcirculatory benefits for organ protection is derived primarily from animal studies.10–12 Although one clinical study demonstrated that dexmedetomidine was associated with higher intraoperative sublingual microcirculation in patients undergoing on-pump coronary artery bypass grafting,13 microcirculatory deterioration may persist into the postoperative period following cardiac surgery.14 Consequently, it remains uncertain whether the potential microcirculatory benefits of dexmedetomidine are sustained postoperatively and whether they are associated with the occurrence of AKI after cardiac surgery. Therefore, we conducted this randomized controlled trial to investigate the influence of dexmedetomidine on perioperative sublingual microcirculation and postoperative outcomes in patients undergoing cardiac surgery.
Materials and Methods
Participant Recruitment and Group Allocation
This randomized, controlled, double-blind clinical trial adhered to the principles of the revised Declaration of Helsinki. The study design was approved by the Research Ethics Committee of National Taiwan University Hospital (Approval No. 201512224MINB; date of approval: May 23, 2016) and was registered at ClinicalTrials.gov prior to patient enrollment (Principal Investigator: Po-Yuan Shih; registration date: May 30, 2016; trial number: NCT02786212). Inclusion criteria were as follows: patients scheduled for non-emergency heart or aortic surgery requiring cardiopulmonary bypass. Exclusion criteria included: age under 20 or over 80 years, left ventricular ejection fraction <40%, angina within 48 hours before surgery, prior cardiac surgery, acute heart failure, preoperative atrioventricular block of grade 2B or higher, and known allergy to dexmedetomidine. Patient enrollment was conducted from August 2016 to April 2019. Prior to trial initiation, stratified randomization was conducted by an independent statistical expert using a block size of four. Written informed consent was obtained from each patient the day before surgery. Patients were randomly assigned in a 1:1 ratio to one of two groups using a predefined, computer-generated block randomization list generated by our institutional medical research department, with variable block sizes ranging from four to six patients: the saline group (receiving an equivalent volume of saline infusion) or the dexmedetomidine group (receiving an intraoperative dexmedetomidine infusion). To ensure blinding, the study drug was prepared and supplied by an independent pharmacy, thereby concealing group allocation from both the investigators and the clinical care team. To assess the hemodynamic impact of the 10-minute loading infusion of the experimental agent, we identified and recorded patients who developed bradycardia (heart rate <60 bpm) or hypotension (systolic blood pressure <100 mmHg).
Perioperative Care
All participants received general anesthesia induced with etomidate (0.2–0.5 mg/kg), fentanyl (0.5–1.5 μg/kg), and rocuronium (0.5–1 mg/kg). Following induction, patients in the dexmedetomidine group received a loading dose of dexmedetomidine (0.5 μg/kg) administered intravenously over 10 minutes, followed by a continuous infusion at a rate of 0.5 μg/kg/h until the end of surgery.6–8 Anesthesia was maintained with sevoflurane (0.5–3.0 vol%) and fentanyl (1–3 μg/kg/h), titrated to maintain a bispectral index between 40 and 60. Ventilation parameters were standardized with a fraction of inspired oxygen set at 50%, tidal volume at 8 mL/kg, and a respiratory rate of 10–14 breaths per minute. Intraoperative monitoring included a five-lead electrocardiogram, pulse oximetry, radial arterial catheter, pulmonary artery catheter, central venous catheter, and transesophageal echocardiography. During the off-pump phase, intravenous fluid management followed a restrictive protocol; however, a 200-mL fluid challenge could be administered if transesophageal echocardiography indicated hypovolemia accompanied by hemodynamic instability—such as a mean arterial pressure (MAP) <55 mmHg or a mixed venous oxygen saturation below 70%—without the use of colloids. During cardiopulmonary bypass (CPB), MAP was maintained between 50 and 80 mmHg, hemoglobin levels above 7 g/dL, and systemic venous oxygen saturation above 70%.15 Arterial hypertension was managed with nitroglycerin, while hypotension was treated with norepinephrine. Following weaning from cardiopulmonary bypass, MAP was maintained above 60 mmHg using fluid boluses or an epinephrine infusion as needed. In cases of persistent hypotension with preserved ventricular function confirmed by transesophageal echocardiography, intravenous norepinephrine was administered. Conversely, intravenous nitroglycerin was used when MAP remained persistently above 100 mmHg. Intravenous furosemide was given after CPB weaning for echocardiography-confirmed fluid overload to reduce preload and prevent pulmonary edema, or for diagnostic diuresis in oliguria (<0.5 mL/kg/hr) with adequate cardiac output. After surgery, all patients were transferred to the same cardiac intensive care unit (ICU), where a standardized weaning protocol was initiated to minimize the risk of prolonged mechanical ventilation. Vasoactive-inotropic scores (VIS) were calculated at ICU admission, and at 24 and 48 hours postoperatively, to assess the impact of intraoperative dexmedetomidine on the requirement for vasoactive and inotropic agents.16 AKI occurring within 48 hours after surgery, along with its severity, was defined according to the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines.17 In addition, we compared between the two study groups the proportion of patients who developed stage 2 or 3 AKI or experienced a postoperative estimated glomerular filtration rate (eGFR) decline of more than 25%, as calculated using the 2021 Chronic Kidney Disease Epidemiology Collaboration criteria.18 This composite outcome was defined as “significant acute kidney impairment”.
Sublingual Microcirculation Measurement
Microcirculatory imaging was performed sublingually using an incident dark field (IDF) illumination hand-held vital microscope (CytoCam™, Braedius Medical BV, Huizen, The Netherlands). This non-invasive technique employs a disposable protective cap placed over the probe, which is gently positioned beneath the patient’s tongue for imaging.19 The device emits polarized green light, which is absorbed by hemoglobin within red blood cells, rendering perfused microvessels as dark structures and thereby enabling visualization of the microvascular architecture and blood flow. Measurements were systematically obtained at five predefined sublingual sites, located 2–5 cm from the tip of the tongue, with 6-second video recordings captured at each site. A minimum of five recordings were acquired from various sublingual positions. All recordings underwent quality assessment according to the most recent consensus guidelines for sublingual microcirculatory imaging.19 Videos that met quality criteria were analyzed offline in a semi-manual fashion using specialized software (AVA 3.0, Microvision Medical, The Netherlands)20 by a trained operator blinded to patient clinical information. The mean values derived from these analyses were used for statistical evaluation. The study focused on microvessels with diameters less than 20 μm. Key microcirculatory parameters assessed included total vessel density (TVD), proportion of perfused vessels (PPV), perfused vessel density (PVD), De Backer’s score, microvascular flow index (MFI), and heterogeneity index (HI).19 These variables were measured at the following time points: baseline (preoperative), 1 hour after cardiopulmonary bypass, 1 hour after surgery, and at 24 and 48 hours postoperatively. The sublingual microcirculation was recorded three times at each time point for every patient. Image quality was independently scored by two research assistants using the method proposed by Massey et al,19,21 which evaluates six metrics of sublingual microcirculation image quality: illumination, duration, focus, content, stability, and pressure. Each metric was rated as good (score 1), acceptable (score 0), or unacceptable (score 10). In addition, inter-rater agreement (κ) was calculated for each image quality metric score.
Statistical Analysis
The primary outcome of this study was the perioperative difference in PVD, as PVD is considered a reliable estimate of functional capillary density.22 Previous studies have reported that reductions in PVD during cardiopulmonary bypass are primarily due to a decrease in the number of perfused microvessels.23 The sample size calculation was based on detecting a clinically relevant difference in PVD, assuming a mean score of 3 and a standard deviation of 4.23,24 A sample size of 58 patients (29 in each group) would provide a statistical power of 0.8 with a two-sided type I error of 0.05. To account for potential dropouts or protocol deviations, a total of 70 patients were enrolled.
Normality of data distribution was assessed using the Shapiro–Wilk test. Continuous variables with a normal distribution are presented as mean ± standard deviation, while non-normally distributed variables are expressed as median (range). Between-group comparisons for continuous variables were performed using Student’s t-test for normally distributed data and the Mann–Whitney U-test for non-normal data. Categorical variables are presented as frequencies (percentages) and were compared using the chi-square test or Fisher’s exact test, as appropriate. A P value <0.05 was considered statistically significant. To evaluate changes in microcirculatory variables over time between the two groups, mixed effect model was conducted, including time and group as factors. When applicable, Tukey’s Honest Significant Difference (HSD) test correction was used for post hoc comparisons. A P value <0.10 was considered indicative of a group-by-time interaction trend approaching statistical significance.25,26
In addition to the primary analysis using a mixed-effects model for repeated measures, we conducted two complementary sensitivity analyses for the perioperative PVD data. First, we performed an analysis of covariance (ANCOVA) at interested postoperative time points (24 h and 48 h) with treatment group as the fixed factor and baseline PVD as the covariate, to adjust for any baseline imbalance and improve precision. Second, we calculated the area under the curve for PVD from baseline to 48 h using the trapezoidal rule, and expressed this as a 0–48 h time-weighted average (TWA) PVD. Between-group differences in TWA were assessed using both Welch’s t-test and ANCOVA adjusting for baseline PVD. In addition, given the relatively small sample size and the potential imbalance in perioperative variables, multiple logistic regression was used to assess the effect of dexmedetomidine on the occurrence of postoperative AKI. All statistical analyses and graphics were performed using R version 4.5.1 (R Foundation for Statistical Computing, Vienna, Austria).
Results
A total of 103 patients scheduled for cardiac surgery were screened for eligibility. Of these, 28 were excluded, 3 withdrew consent, and 2 were excluded due to a lack of research personnel (Figure 1). Ultimately, 70 patients were enrolled in the study, with 2 subsequently unable to complete microcirculatory assessments due to limited research staffing during the SARS-CoV-2 pandemic. Table 1 summarizes the clinical and demographic characteristics of the study participants. Baseline variables, including age, sex, comorbidities, and EuroSCORE II, were comparable between the two groups. However, there were procedural differences: a greater proportion of patients in the saline group underwent single valve replacement surgery (67.6% vs 50.0%), while more patients in the dexmedetomidine group underwent aortic surgery (17.6% vs 0%). This difference approached but did not reach statistical significance (p = 0.074; Table 1).
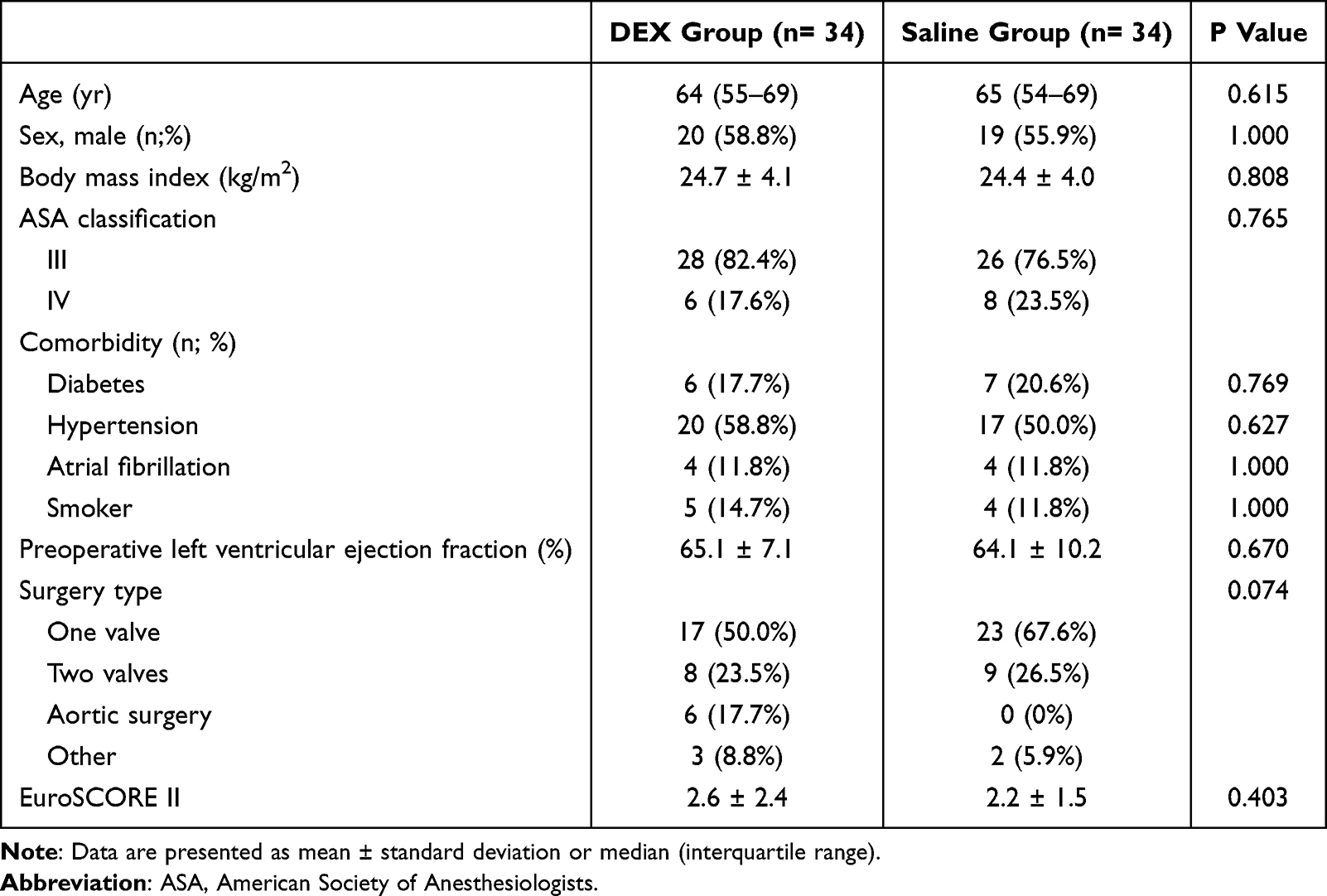 |
Table 1 Patient Characteristics |
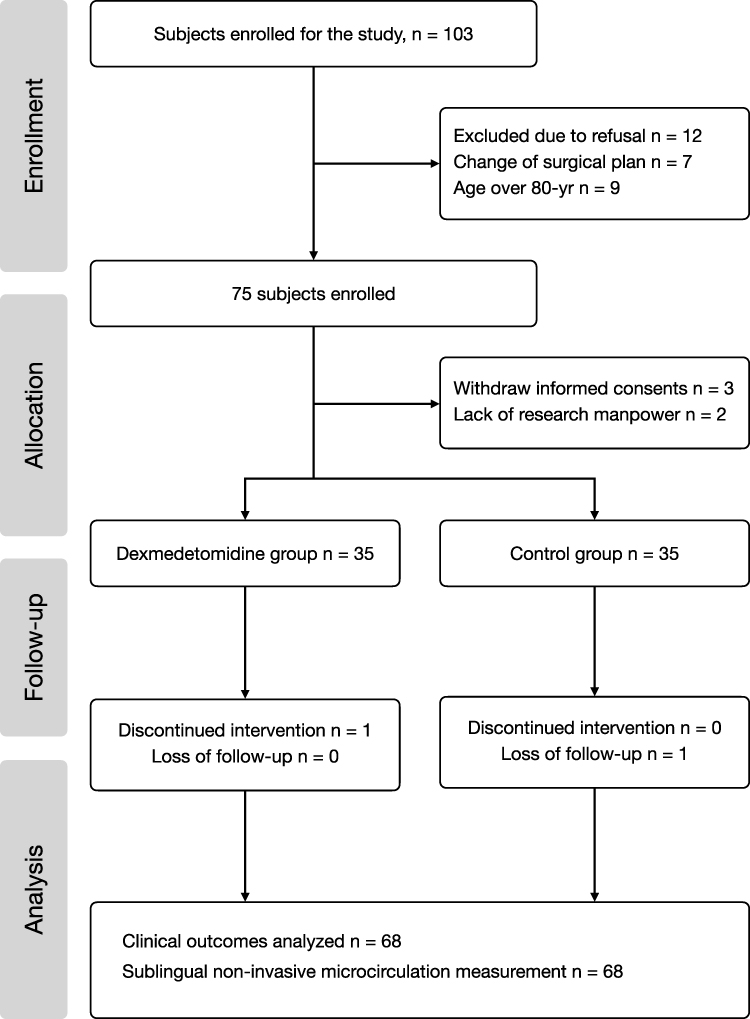 |
Figure 1 Consort diagram. |
Perioperative PVD and PPV
A total of 1020 sublingual microcirculation images were recorded for assessment, with none rated as unacceptable in quality (Table 2). The inter-rater agreement for microcirculation image quality at different time points is presented in Table 2, demonstrating satisfactory reliability, with κ values ranging from 0.77 to 0.85. There were no significant differences in image quality ratings between the two raters. The trajectory of perioperative changes in TVD, PPV, PVD, De Backer’s score, MFI, and HI is illustrated in Figure 2. The mean difference, effect size, and 95% confidence interval for each microcirculatory variable between the two study groups at different time points was also summarized in Supplementary Table 1. Baseline values of all microcirculatory parameters were comparable between the two groups (Figure 2). Throughout the perioperative period, PPV and PVD tended to remain higher in the dexmedetomidine group compared to the saline group, with group-by-time interaction effects approaching statistical significance (PVD: P = 0.042, Figure 2A; PPV: P = 0.065, Figure 2B). At 48 hours postoperatively, patients in the dexmedetomidine group had significantly higher PVD values than those in the saline group (17.0 [15.0–19.0] vs 15.6 [13.7–16.9] mm/mm²; P = 0.041).
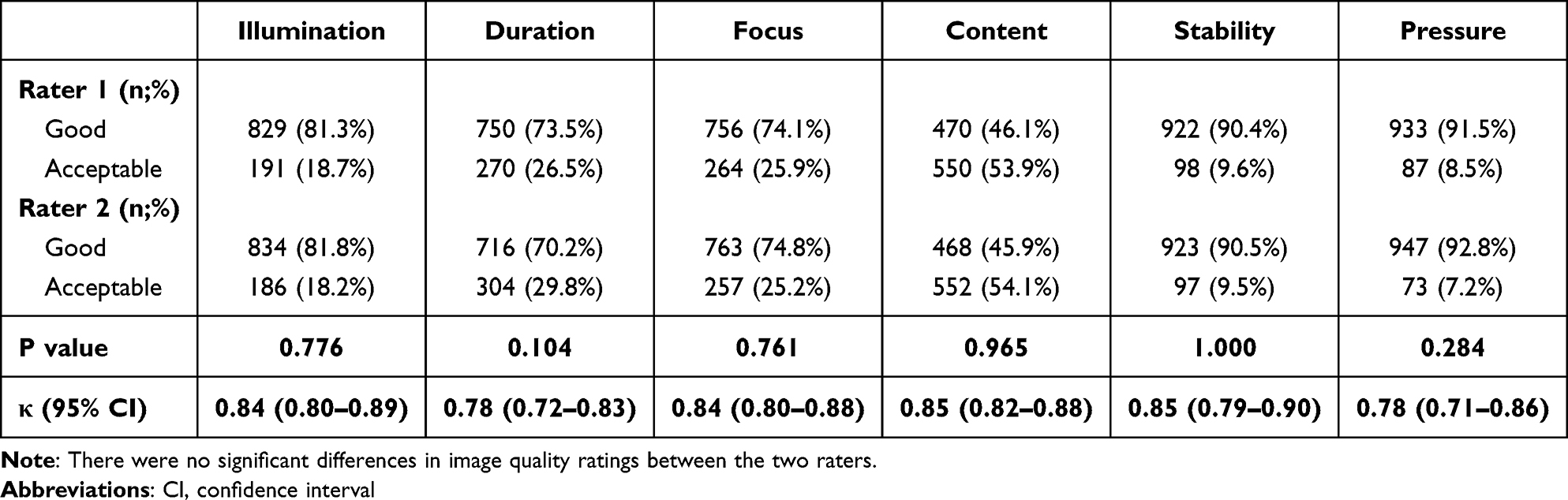 |
Table 2 Quality of 1020 Sublingual Microcirculation Images and Inter-Rater Agreement Between Two Independent Raters |
 |
Figure 2 Perioperative changes in microcirculation. (A) Perioperative changes in the perfused vessel density. (B) Perioperative changes in the proportion of perfused vessel. (C) Perioperative changes in total vessel density. (D) Perioperative changes in microvascular flow index. (E). Perioperative changes in De Backer’s score. (F) Perioperative changes in heterogeneity index. The light red stripes represent the saline control group, and the light green stripes represent the dexmedetomidine group. |
Sensitivity Analyses of the Primary Outcome – PVD
Baseline-adjusted ANCOVA demonstrated that DEX patients had higher PVD at both 24 h (adjusted mean difference [DEX–Saline], 1.129 mm/mm²; 95% CI, 0.026 to 2.232 mm/mm²; P = 0.045) and 48 h (1.340 mm/mm²; 95% CI, 0.001 to 2.680 mm/mm²; P = 0.050) compared with saline. Over the 0–48 h period, DEX patients had a higher time-weighted average PVD (mean ± SD, 17.16 ± 2.23 mm/mm²) than Saline patients (15.84 ± 2.53 mm/mm²; Welch’s t-test P = 0.027). This difference remained significant after baseline adjustment (adjusted mean difference, 1.154 mm/mm²; 95% CI, 0.145 to 2.163 mm/mm²; P = 0.025). These results are consistent with the direction and magnitude of the treatment effect observed in the primary mixed-effects model, supporting the robustness of the findings.
The Other Perioperative Microcirculatory Parameters
Other postoperative microcirculatory variables, including TVD, MFI, and De Backer’s score, were consistently higher in the dexmedetomidine group, though the differences did not reach statistical significance (Figure 2C–E). Similarly, HI tended to be lower in the dexmedetomidine group (Figure 2F). Notably, MFI values at 24 and 48 hours postoperatively were higher in the dexmedetomidine group (24 h: 2.10 ± 0.25 vs 1.96 ± 0.33, P = 0.072; 48 h: 2.17 ± 0.30 vs 2.00 ± 0.42, P = 0.059), although these differences also did not achieve statistical significance.
Intraoperative and Postoperative Clinical Profiles
Perioperative profiles are summarized in Table 3. During the 10-minute loading infusion of the experimental agent, a non-significantly higher proportion of patients in the dexmedetomidine group experienced bradycardia (73.5% vs 52.9%; p = 0.131) and hypotension (61.8% vs 50.0%; p = 0.464). The high incidence of hemodynamic instability in both groups may be attributable to the overlap of this 10-minute interval with anesthesia induction. Two patients in the saline group received an intravenous furosemide bolus (one received 5 mg and one received 10 mg), whereas no patients in the dexmedetomidine group received diuretics (5.9% vs 0%; p = 0.493). There were no statistically significant differences in surgical profiles between the two groups, including amount of iv. fluid administration during off-pump phase, average intraoperative BIS values, operation time, cardiopulmonary bypass duration, and aortic cross-clamp time (Table 3). Similarly, no significant differences were observed in the proportion of patients requiring perioperative blood transfusion, and the vasoactive-inotropic scores at the end of surgery, as well as at 24 and 48 hours postoperatively, were comparable between the dexmedetomidine and saline groups (Table 3). However, patients in the dexmedetomidine group had significantly higher urine output during cardiopulmonary bypass [600 (400–850) vs 350 (183–515) mL; p < 0.001] and at the completion of surgery [950 (563–1245) vs 605 (401–875) mL; p = 0.002] (Table 3).
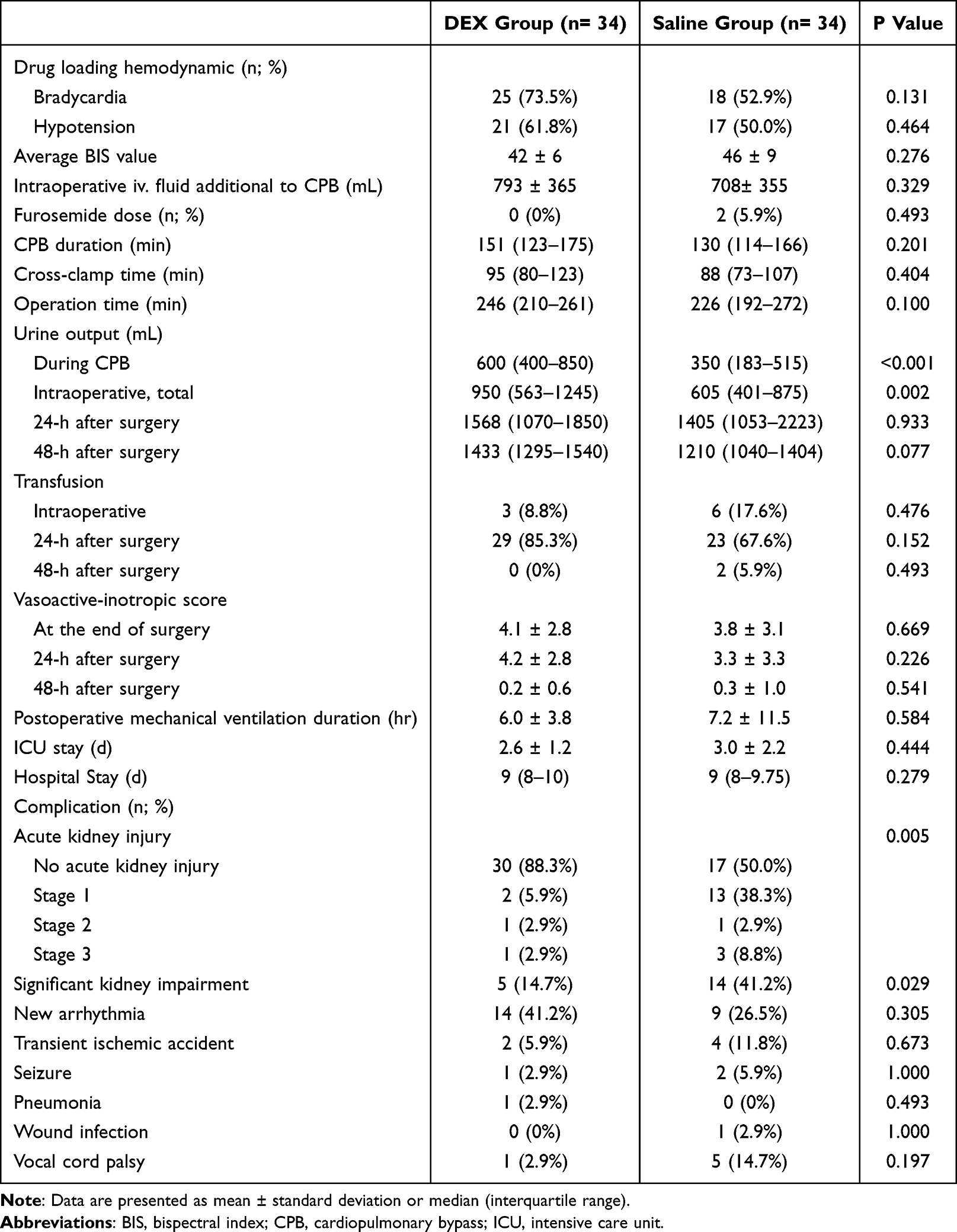 |
Table 3 Perioperative Profiles |
With regard to postoperative outcomes, there were no significant differences in the duration of mechanical ventilation, length of ICU stay, or total hospital stay between the two groups. Postoperative complication rates—including new-onset arrhythmia, transient ischemic attack, seizure, wound infection, and pneumonia—were also similar between groups. However, a significantly higher incidence of postoperative acute kidney injury (AKI) was observed in the control group compared to the dexmedetomidine group (50.0% vs 11.8%; p = 0.001). The majority of AKI cases were classified as KDIGO stage 1 (71.4%) (Table 3). Multiple regression showed that CPB duration (OR = 1.03; 95% CI: 1.01–1.04; p < 0.001) and the saline control group (OR = 25.2; 95% CI: 4.28–148.73; p < 0.001) were risk factor. In addition, a higher proportion of patients in the saline group developed significant acute kidney impairment compared with those in the dexmedetomidine group (41.2% vs 14.7%; p = 0.029; Table 3). The perioperative trajectories of serum creatinine alongside changes in eGFR in Supplementary Figures 1 and 2, which showed a trend toward higher eGFR in the dexmedetomidine group compared with the saline group, approaching statistical significance (group-by-time interaction p = 0.09).
Discussion
This study yielded several important findings. First, intraoperative dexmedetomidine infusion during cardiac surgery was associated with higher postoperative PPV and PVD values at 24 and 48 hours after surgery. Second, patients who received dexmedetomidine demonstrated significantly higher intraoperative urine output and a lower incidence of acute kidney injury within 48 hours postoperatively.
Postoperative deterioration of sublingual microcirculation has been widely documented in both cardiac and non-cardiac surgeries.14 Decreased postoperative sublingual microcirculatory parameters—particularly PVD and PPV—have been associated with elevated serum lactate levels27–29 and increased risk of postoperative organ injury.28,30 In the context of cardiac surgery, cardiopulmonary bypass is recognized as a major contributor to impaired sublingual microcirculatory perfusion, as evidenced by reduced PVD and PPV.23 Mohamed et al previously reported that intraoperative dexmedetomidine infusion improved sublingual microcirculation in patients undergoing on-pump coronary artery bypass grafting.13 However, microcirculatory dysfunction may persist for up to three days after cardiac surgery,31 and is believed to play a central role in the pathogenesis of postoperative organ dysfunction.32 A previous study reported that dexmedetomidine used for post–cardiac surgery sedation is associated with more favorable microcirculation compared with propofol sedation.33 Since dexmedetomidine is also frequently administered during cardiac surgery9 an important question is whether intraoperative use confers microcirculatory protection that persists into the postoperative period. This issue remains to be fully clarified. In the present study, we observed potential microcirculatory protective effects of dexmedetomidine, as reflected by significantly higher postoperative PVD and PPV at 48 hours after surgery in the dexmedetomidine group. This time frame is consistent with prior reports of prolonged postoperative microcirculatory impairment and underscores the clinical relevance of our findings. Several mechanisms may explain these observations. First, Dekker et al demonstrated that CPB-induced endothelial hyperpermeability in renal and pulmonary tissues—marked by elevated angiopoietin-2 and soluble Tie2 levels—was associated with impaired sublingual microcirculatory perfusion.34 Notably, dexmedetomidine has been shown to reduce angiopoietin-2 levels in both septic and ischemic animal models,35,36 suggesting that the higher postoperative PVD and PPV observed in our study may be partly mediated by suppression of the angiopoietin-2 pathway during CPB. Second, cardiopulmonary bypass-associated factors such as hypothermia, hemodilution, and mechanical stress are known to impair red blood cell deformability, thereby compromising microcirculatory flow.37 Dexmedetomidine has been reported to improve RBC deformability during surgery,38 which may also contribute to the observed microvascular benefits. Third, dexmedetomidine may be associated with higher postoperative PVD through its sympatholytic effects, which significantly reduce plasma norepinephrine and dopamine levels.39
Recent technological advancements have facilitated perioperative microcirculatory monitoring through the development of hand-held video microscopes. In this study, we employed the Cytocam incident dark field (IDF) illumination imaging system to assess sublingual microcirculatory changes. Compared to older technologies such as sidestream dark field (SDF) imaging, Cytocam-IDF offers improved image contrast, sharpness, and resolution, enhancing visualization of both venules and capillaries.19,40,41 Moreover, its semi-automated analysis platform reduces operator-dependent variability and subjectivity, allowing for more consistent and reproducible results.40
In addition to the more favorable microcirculatory profiles, we also observed a lower incidence of postoperative acute kidney injury in the dexmedetomidine group, a finding that aligns with the results of a recent meta-analysis.42 In contrast, Wang et al recently reported that dexmedetomidine infusion did not reduce the incidence of AKI in patients undergoing valvular surgery, based on a secondary analysis of a randomized controlled trial.43 This discrepancy may be attributed to differences in surgical complexity: in their study, a greater proportion of patients in the dexmedetomidine group underwent multiple valve surgeries, while those in the control group more often underwent single-valve procedures.43 Furthermore, AKI is more commonly observed following aortic surgery compared to other types of cardiac surgery.44 Interestingly, dexmedetomidine has been reported to reduce the incidence of acute kidney injury in patients undergoing aortic surgery.45 In the present study, despite a higher proportion of aortic surgeries in the dexmedetomidine group, the incidence of postoperative acute kidney injury was significantly lower compared to the control group. This finding further supports the potential renoprotective effects of dexmedetomidine in the context of complex cardiac surgery.
The potential mechanisms by which dexmedetomidine may prevent acute kidney injury after cardiac surgery are multifactorial. One major pathway involves its sympatholytic effects, which can enhance renal blood flow and promote diuresis.45–47 Notably, low urine output during cardiopulmonary bypass has been identified as a risk factor for the development of acute kidney injury.48,49 In the present study, patients who received intraoperative dexmedetomidine exhibited significantly higher urine output during cardiopulmonary bypass and a lower incidence of postoperative acute kidney injury, supporting this mechanistic hypothesis. Additionally, dexmedetomidine has been shown to attenuate the perioperative stress and inflammatory responses in various clinical and experimental settings,5 which may contribute to improved renal microcirculation. Evidence from preclinical studies has demonstrated that dexmedetomidine enhances renal microvascular perfusion in rat models,12 and improves sublingual microcirculation and early postoperative renal function in kidney transplant recipients.50 These findings suggest that dexmedetomidine may exert both systemic and renal-specific protective effects during and after cardiac surgery.
Several limitations should be acknowledged in the present study. First, patient enrollment was significantly affected by the COVID-19 pandemic, which contributed to a smaller sample size and may have limited the statistical power to detect differences in certain microcirculatory parameters, such as TVD, MFI, and HI. Second, there was an imbalance in surgical complexity between the two groups: more patients in the saline group underwent less complex single-valve replacement procedures and had shorter operative times. Despite this, patients in the dexmedetomidine group demonstrated more favorable outcomes, underscoring the potential benefits of dexmedetomidine in cardiac surgery. In addition, we have applied the multiple logistic regression instead of matching. This is because that matching would exclude a substantial number of patients but the regression approach allowed adjustment for all clinically relevant covariates and is a validated alternative when baseline characteristics are adequately balanced and sample size needs to be preserved.51 The regression further indicates the dexmedetomidine as a protective factor to AKI further supporting the robustness of our results. Third, most cases of acute kidney injury in our cohort were classified as KDIGO stage 1, raising uncertainty about the generalizability of dexmedetomidine’s protective effects against more severe forms of acute kidney injury. However, even KDIGO stage 1 AKI is associated with adverse postoperative outcomes, including increased risk of infection, prolonged ICU stay, extended hospital stay52 a and the development or progression of chronic kidney disease.53 Given that a higher proportion of patients in the dexmedetomidine group underwent more complex aortic surgery, our findings may underestimate the renal protective effects of dexmedetomidine in patients undergoing cardiac surgery.
In conclusion, this randomized, controlled, double-blind study demonstrated that intraoperative dexmedetomidine infusion was associated with attenuated postoperative sublingual microcirculatory perfusion deficits—reflected by higher postoperative PPV and PVD—greater intraoperative urine output, and a reduced incidence of postoperative acute kidney injury in patients undergoing cardiac surgery, including valve replacement and aortic procedures.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgment
We thank the staff of Department of Medical Research, National Taiwan University Hospital Hsin-Chu Branch for their assistance in statistical analysis. This work was supported by the institutional grant from National Taiwan University Hospital (NTUH 106-02).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Flick M, Hilty MP, Duranteau J, Saugel B. The microcirculation in perioperative medicine: a narrative review. Br J Anaesth. 2024;132(1):25–34. doi:10.1016/j.bja.2023.10.033
2. Flick M, Duranteau J, Scheeren TWL, Saugel B. Monitoring of the sublingual microcirculation during cardiac surgery: current knowledge and future directions. J Cardiothorac Vasc Anesth. 2020;34(10):2754–2765. doi:10.1053/j.jvca.2019.10.038
3. Le Dorze M, Legrand M, Payen D, Ince C. The role of the microcirculation in acute kidney injury. Curr Opin Crit Care. 2009;15(6):503–508. doi:10.1097/MCC.0b013e328332f6cf
4. De Cuyper H, Poelaert J. Microcirculatory alterations in cardiac surgery: a comprehensive guide. J Cardiothorac Vasc Anesth. 2024;38(3):829–838. doi:10.1053/j.jvca.2023.11.042
5. Wang K, Wu M, Xu J, et al. Effects of dexmedetomidine on perioperative stress, inflammation, and immune function: systematic review and meta-analysis. Br J Anaesth. 2019;123(6):777–794. doi:10.1016/j.bja.2019.07.027
6. Chen PH, Tsuang FY, Lee CT, et al. Neuroprotective effects of intraoperative dexmedetomidine versus saline infusion combined with goal-directed haemodynamic therapy for patients undergoing cranial surgery: a randomised controlled trial. Eur J Anaesthesiol. 2021;38(12):1262–1271. doi:10.1097/EJA.0000000000001532
7. Bao N, Tang B. Organ-protective effects and the underlying mechanism of dexmedetomidine. Mediators Inflamm. 2020;2020:6136105. doi:10.1155/2020/6136105
8. Wu CY, Lu YF, Wang ML, et al. Effects of dexmedetomidine infusion on inflammatory responses and injury of lung tidal volume changes during one-lung ventilation in thoracoscopic surgery: a randomized controlled trial. Mediators Inflamm. 2018;2018:2575910. doi:10.1155/2018/2575910
9. Poon WH, Ling RR, Yang IX, et al. Dexmedetomidine for adult cardiac surgery: a systematic review, meta-analysis and trial sequential analysis. Anaesthesia. 2023;78(3):371–380. doi:10.1111/anae.15947
10. Yeh YC, Wu CY, Cheng YJ, et al. Effects of dexmedetomidine on intestinal microcirculation and intestinal epithelial barrier in endotoxemic rats. Anesthesiology. 2016;125(2):355–367. doi:10.1097/ALN.0000000000001135
11. Miranda ML, Balarini MM, Bouskela E. Dexmedetomidine attenuates the microcirculatory derangements evoked by experimental sepsis. Anesthesiology. 2015;122(3):619–630. doi:10.1097/ALN.0000000000000491
12. Yang SJ, Fan CN, Wang MJ, et al. Effects of dexmedetomidine on renal microcirculation in ischemia/reperfusion-induced acute kidney injury in rats. Sci Rep. 2021;11(1):2026. doi:10.1038/s41598-021-81288-3
13. Mohamed H, Hosny H, Tawadros Md P, Elayashy Md Desa Fcai M, El-Ashmawi Md H. Effect of dexmedetomidine infusion on sublingual microcirculation in patients undergoing on-pump coronary artery bypass graft surgery: a prospective randomized trial. J Cardiothorac Vasc Anesth. 2019;33(2):334–340. doi:10.1053/j.jvca.2018.06.016
14. Chalkias A, Papagiannakis N, Mavrovounis G, et al. Sublingual microcirculatory alterations during the immediate and early postoperative period: a systematic review and meta-analysis. Clin Hemorheol Microcirc. 2022;80(3):253–265. doi:10.3233/CH-211214
15. Kunst G, Milojevic M, Milojevic M, et al; Authors/Task Force M. 2019 EACTS/EACTA/EBCP guidelines on cardiopulmonary bypass in adult cardiac surgery. Br J Anaesth. 2019;123(6):713–757. doi:10.1016/j.bja.2019.09.012
16. Koponen T, Karttunen J, Musialowicz T, Pietilainen L, Uusaro A, Lahtinen P. Vasoactive-inotropic score and the prediction of morbidity and mortality after cardiac surgery. Br J Anaesth. 2019;122(4):428–436. doi:10.1016/j.bja.2018.12.019
17. Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract. 2012;120(4):c179–84. doi:10.1159/000339789
18. Inker LA, Eneanya ND, Coresh J, et al. New creatinine- and cystatin C-based equations to estimate GFR without race. N Engl J Med. 2021;385(19):1737–1749. doi:10.1056/NEJMoa2102953
19. Ince C, Boerma EC, Cecconi M, et al. Second consensus on the assessment of sublingual microcirculation in critically ill patients: results from a task force of the European Society of Intensive Care Medicine. Intensive Care Med. 2018;44(3):281–299. doi:10.1007/s00134-018-5070-7
20. Dobbe JG, Streekstra GJ, Atasever B, van Zijderveld R, Ince C. Measurement of functional microcirculatory geometry and velocity distributions using automated image analysis. Med Biol Eng Comput. 2008;46(7):659–670. doi:10.1007/s11517-008-0349-4
21. Massey MJ, Larochelle E, Najarro G, et al. The microcirculation image quality score: development and preliminary evaluation of a proposed approach to grading quality of image acquisition for bedside videomicroscopy. J Crit Care. 2013;28(6):913–917. doi:10.1016/j.jcrc.2013.06.015
22. De Backer D, Hollenberg S, Boerma C, et al. How to evaluate the microcirculation: report of a round table conference. Crit Care. 2007;11(5):R101. doi:10.1186/cc6118
23. den Os MM, van den Brom CE, van Leeuwen ALI, Dekker NAM. Microcirculatory perfusion disturbances following cardiopulmonary bypass: a systematic review. Crit Care. 2020;24(1):218. doi:10.1186/s13054-020-02948-w
24. Koning NJ, Vonk AB, van Barneveld LJ, et al. Pulsatile flow during cardiopulmonary bypass preserves postoperative microcirculatory perfusion irrespective of systemic hemodynamics. J Appl Physiol. 2012;112(10):1727–1734. doi:10.1152/japplphysiol.01191.2011
25. Lee CT, Lin CP, Chan KC, Wu YL, Teng HC, Wu CY. Effects of goal-directed hemodynamic therapy using a noninvasive finger-cuff monitoring device on intraoperative cerebral oxygenation and early delayed neurocognitive recovery in patients undergoing beach chair position shoulder surgery: a randomized controlled trial. Anesth Analg. 2023;136(2):355–364. doi:10.1213/ANE.0000000000006200
26. Thiese MS, Ronna B, Ott U. P value interpretations and considerations. J Thorac Dis. 2016;8(9):E928–E931. doi:10.21037/jtd.2016.08.16
27. Yeh YC, Wang MJ, Chao A, et al. Correlation between early sublingual small vessel density and late blood lactate level in critically ill surgical patients. J Surg Res. 2013;180(2):317–321. doi:10.1016/j.jss.2012.05.006
28. Greenwood JC, Jang DH, Hallisey SD, et al. Severe impairment of microcirculatory perfused vessel density is associated with postoperative lactate and acute organ injury after cardiac surgery. J Cardiothorac Vasc Anesth. 2021;35(1):106–115. doi:10.1053/j.jvca.2020.04.045
29. Greenwood JC, Jang DH, Spelde AE, et al. Low microcirculatory perfused vessel density and high heterogeneity are associated with increased intensity and duration of lactic acidosis after cardiac surgery with cardiopulmonary bypass. Shock. 2021;56(2):245–254. doi:10.1097/SHK.0000000000001713
30. Jhanji S, Lee C, Watson D, Hinds C, Pearse RM. Microvascular flow and tissue oxygenation after major abdominal surgery: association with post-operative complications. Intensive Care Med. 2009;35(4):671–677. doi:10.1007/s00134-008-1325-z
31. Dekker NAM, Veerhoek D, Koning NJ, et al. Postoperative microcirculatory perfusion and endothelial glycocalyx shedding following cardiac surgery with cardiopulmonary bypass. Anaesthesia. 2019;74(5):609–618. doi:10.1111/anae.14577
32. Kant S, Banerjee D, Sabe SA, Sellke F, Feng J. Microvascular dysfunction following cardiopulmonary bypass plays a central role in postoperative organ dysfunction. Front Med. 2023;10:1110532. doi:10.3389/fmed.2023.1110532
33. Liu X, Zhang K, Wang W, et al. Dexmedetomidine versus propofol sedation improves sublingual microcirculation after cardiac surgery: a randomized controlled trial. J Cardiothorac Vasc Anesth. 2016;30(6):1509–1515. doi:10.1053/j.jvca.2016.05.038
34. Dekker NAM, Van leeuwen ALI, van Strien WWJ, et al. Microcirculatory perfusion disturbances following cardiac surgery with cardiopulmonary bypass are associated with in vitro endothelial hyperpermeability and increased angiopoietin-2 levels. Crit Care. 2019;23(1):117. doi:10.1186/s13054-019-2418-5
35. Zhang P, Peng J, Ren YQ, Zheng H, Yan H. Dexmedetomidine protects against endothelial injury in septic rats induced by cecal ligation and puncture by decreasing angiopoietin 2 and increasing vascular endothelial cadherin levels. Exp Ther Med. 2021;21(2):111. doi:10.3892/etm.2020.9543
36. Fang B, Li XQ, Bi B, et al. Dexmedetomidine attenuates blood-spinal cord barrier disruption induced by spinal cord ischemia reperfusion injury in rats. Cell Physiol Biochem. 2015;36(1):373–383. doi:10.1159/000430107
37. Kameneva MV, Undar A, Antaki JF, Watach MJ, Calhoon JH, Borovetz HS. Decrease in red blood cell deformability caused by hypothermia, hemodilution, and mechanical stress: factors related to cardiopulmonary bypass. ASAIO J. 1999;45(4):307–310. doi:10.1097/00002480-199907000-00010
38. Yang XM, Liu J, Ji J, Xie J. Effects of dexmedetomidine on the deformability of erythrocytes in vitro and in anesthesia. Exp Ther Med. 2014;7(6):1631–1634. doi:10.3892/etm.2014.1633
39. Xu J, Wang Y, Shu C, Chang W, Guo F. Dexmedetomidine improves microcirculatory alterations in patients with initial resuscitated septic shock. J Intensive Care Med. 2025;40(2):137–144. doi:10.1177/08850666241267860
40. Aykut G, Veenstra G, Scorcella C, Ince C, Boerma C. Cytocam-IDF (incident dark field illumination) imaging for bedside monitoring of the microcirculation. Intensive Care Med Exp. 2015;3(1):40. doi:10.1186/s40635-015-0040-7
41. Gilbert-Kawai E, Coppel J, Bountziouka V, et al. A comparison of the quality of image acquisition between the incident dark field and sidestream dark field video-microscopes. BMC Med Imaging. 2016;16:10. doi:10.1186/s12880-015-0078-8
42. Peng K, Li D, Applegate RL 2nd, Lubarsky DA, Ji FH, Liu H. Effect of dexmedetomidine on cardiac surgery-associated acute kidney injury: a meta-analysis with trial sequential analysis of randomized controlled trials. J Cardiothorac Vasc Anesth. 2020;34(3):603–613. doi:10.1053/j.jvca.2019.09.011
43. Wang HB, Jia Y, Zhang CB, et al. A randomised controlled trial of dexmedetomidine for delirium in adults undergoing heart valve surgery. Anaesthesia. 2023;78(5):571–576. doi:10.1111/anae.15983
44. Cheruku SR, Raphael J, Neyra JA, Fox AA. Acute kidney injury after cardiac surgery: prediction, prevention, and management. Anesthesiology. 2023;139(6):880–898. doi:10.1097/ALN.0000000000004734
45. Soh S, Shim JK, Song JW, Bae JC, Kwak YL. Effect of dexmedetomidine on acute kidney injury after aortic surgery: a single-centre, placebo-controlled, randomised controlled trial. Br J Anaesth. 2020;124:386–394. doi:10.1016/j.bja.2019.12.036
46. Gao X, Wu YJB, Communications BR. Perioperative acute kidney injury: the renoprotective effect and mechanism of dexmedetomidine. Biochem Biophys Res Commun. 2023;695:149402. doi:10.1016/j.bbrc.2023.149402
47. Liu Y, Sheng B, Wang S, Lu F, Zhen J, Chen W. Dexmedetomidine prevents acute kidney injury after adult cardiac surgery: a meta-analysis of randomized controlled trials. BMC Anesthesiol. 2018;18(1):7. doi:10.1186/s12871-018-0472-1
48. Song Y, Kim DW, Kwak YL, et al. Urine output during cardiopulmonary bypass predicts acute kidney injury after cardiac surgery: a single-center retrospective analysis. Medicine. 2016;95(22):e3757. doi:10.1097/MD.0000000000003757
49. Hori D, Katz NM, Fine DM, et al. Defining oliguria during cardiopulmonary bypass and its relationship with cardiac surgery-associated acute kidney injury. Br J Anaesth. 2016;117(6):733–740. doi:10.1093/bja/aew340
50. Wang YC, Wang MJ, Lee CY, et al. Effects of perioperative dexmedetomidine infusion on renal function and microcirculation in kidney transplant recipients: a randomised controlled trial. Ann Med. 2022;54(1):1233–1243. doi:10.1080/07853890.2022.2067351
51. Cepeda MS, Boston R, Farrar JT, Strom BL. Comparison of logistic regression versus propensity score when the number of events is low and there are multiple confounders. Am J Epidemiol. 2003;158(3):280–287. doi:10.1093/aje/kwg115
52. Griffin BR, Teixeira JP, Ambruso S, et al. Stage 1 acute kidney injury is independently associated with infection following cardiac surgery. J Thorac Cardiovasc Surg. 2021;161(4):1346–1355e3. doi:10.1016/j.jtcvs.2019.11.004
53. Long TE, Helgason D, Helgadottir S, et al. Mild stage 1 post-operative acute kidney injury: association with chronic kidney disease and long-term survival. Clin Kidney J. 2021;14(1):237–244. doi:10.1093/ckj/sfz197
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Dexmedetomidine May Reduce the Incidence of Acute Kidney Injury in Elderly Patients Undergoing Orthopedic Surgery: A Randomized, Double-Blind Clinical Trial
Zheng XY, Su Z, Zhang Y, Yan J, Li XY, Peng K, Liu H, Shan XS, Ji FH
Drug Design, Development and Therapy 2026, 20:571990
Published Date: 20 February 2026
Association of Dexmedetomidine Exposure with Long-Term Mortality in Patients with Dialysis-Requiring Acute Kidney Injury: A Propensity Score–Matched Retrospective Cohort Study
Hung KC, Chang LC, Chang YJ, Lai YC, Lin CM, Chen IW
Drug Design, Development and Therapy 2026, 20:598443
Published Date: 27 April 2026
The Effect of Dexmedetomidine on Postoperative Acute Kidney Injury in High-Risk Partial Nephrectomy Patients: A Retrospective Cohort Study
Zhang HD, Gao Y, Zhang ZY, Zhang YX, Kong H
Drug Design, Development and Therapy 2026, 20:607823
Published Date: 29 May 2026