Back to Journals » Clinical Ophthalmology » Volume 17
Intraoperative Customized Reduction in Baerveldt Implant Plate Size in Elderly Patients with Glaucoma and Short Eyes
Authors Välimäki J
Received 21 April 2023
Accepted for publication 24 July 2023
Published 9 August 2023 Volume 2023:17 Pages 2287—2293
DOI https://doi.org/10.2147/OPTH.S415406
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Juha Välimäki
Department of Ophthalmology, Päijät-Häme Central Hospital, Wellbeing Services County of Päijät-Häme, Lahti, 15850, Finland
Correspondence: Juha Välimäki, Department of Ophthalmology, Wellbeing Services County of Päijät-Häme, Päijät-Sote, Keskussairaalankatu 7, Lahti, 15850, Finland, Tel +358 3 819 4801, Fax +358 3 819 4803, Email [email protected]
Purpose: Larger surface area glaucoma drainage implant plates are associated with greater IOP reduction. Older age and short axial length of the eye have been reported to be risk factors for postoperative hypotony and suprachoroidal hemorrhage after glaucoma surgery. This pilot study, the first of its type, was conducted to determine the clinical outcome of intraoperative Baerveldt implant plate size reduction in elderly patients (≥ 80 years) with short axial length (< 22 mm).
Methods: This was a retrospective study with a minimum 18-month follow-up involving 24 consecutive uncontrolled glaucoma patients who had previously undergone Baerveldt implantation with implant plate size reduction. Success was defined as intraocular pressure (IOP) < 21 mmHg with at least a 30% reduction in IOP from baseline on two consecutive follow-up visits, IOP > 5 mm Hg on two consecutive follow-up visits, and neither reoperation of glaucoma nor loss of light perception. The distance between the rectus muscles at the equator of the eyeball was measured using a surgical caliper. The Baerveldt implant plate was cut with straight dissecting scissors considering the distance between the muscles.
Results: The mean ±SD preoperative IOP before GDI was 30.2 ± 6.9 mmHg, and the mean IOP at the last follow-up visit was 13.3 ± 5.1 mmHg, the mean pressure drop being 16.9 mmHg (56%) (P< 0.001). The number of antiglaucoma medications declined from mean 3.7 ± 1.0 (range 2– 5) to 1.6 ± 1.1 (range 0– 3) at the last visit (P< 0.001). The success rate at the last follow-up visit was 79% (19 of 24 eyes). Fourteen (58%) eyes were classified as qualified success and five eyes (21%) were complete success. Complications included intraoperative suprachoroidal hemorrhage (1) and postoperative hyphema (2).
Conclusion: Baerveldt implantation with customized plate downsizing can be an effective treatment option for difficult glaucoma in elderly people with short eyes.
Keywords: short axial length, glaucoma drainage implant, hypotony, suprachoroidal hemorrhage, implant plate truncation
Introduction
Older age and short axial length of the eye have been reported to be risk factors for hypotony and suprachoroidal hemorrhage (SCH) after glaucoma surgery.1,2 Postoperative hypotony should be avoided in these high-risk eyes. A larger glaucoma drainage implant (GDI) plate size may lead to a greater degree of IOP reduction and increase the risk of postoperative hypotony in elderly patients with short eyes.3,4 Additionally, a larger GDI plate area has been reported to result in a higher frequency of postoperative diplopia than implants with a smaller plate area,5 and surgeons must be aware of this potential complication, especially in patients with short eyes.
The surface area of a GDI bleb capsule is directly proportional to the implant plate size. During the preoperative evaluation of patients, the surgeon must consider whether smaller GDI plate size is more appropriate option for lowering IOP in these high-risk eyes. The smallest available Baerveldt implant (Johnson & Johnson Vision, California, USA) plate size is 250 mm2. If the surgeon decides to implant a nonvalved GDI, such as a Baerveldt, but prefer a smaller plate area than 250 mm2, he must reduce the implant plate size. The implant plate is made from soft silicone and can be truncated by cutting with scissors. Downsizing a Baerveldt implant plate by truncation of one or both wings of the implant has been reported to be an effective and safe method for reversing persistent postoperative hypotony while maintaining IOP control.6,7 However, no previous reports exist considering GDI size customizing by cutting the plate intraoperatively to prevent complications in elderly patients with short eyes.
The aim of this pilot study, the first of its type, was to evaluate the efficacy and safety of Baerveldt implantation with customized intraoperative implant plate size reduction in elderly glaucoma patients (80 years and older) with short axial length of the eye (under 22 mm).
Materials and Methods
The cases of 24 consecutive patients who presented with Baerveldt 250 mm2 implantations performed using customized implant plate size reduction surgery were retrospectively reviewed. All patients were ≥80 years with axial length of the eye under 22 mm and operated on at the Päijät-Häme Central Hospital between February 2014 and February 2021 with a minimum 18-month follow-up by the same surgeon (JV).
Outcome measures included IOP, visual acuity, number of antiglaucoma medications, and any surgical complications. Surgical success was defined as IOP<21 mmHg with at least a 30% reduction in IOP from baseline on two consecutive follow-up visits with less than or as much antiglaucoma medication as preoperatively, IOP>5 mmHg on two consecutive follow-up visits and neither reoperation of glaucoma nor loss of light perception vision. All patients who met these criteria and were not on supplemental antiglaucoma therapy were considered complete successes. Patients who had succeeded but required supplemental antiglaucoma medication were defined as qualified successes. Cataracts were considered to have progressed if there was loss of 2 or more lines of Snellen best corrected visual acuity (BCVA) attributed to cataract at the last follow-up visit, or if cataract surgery had been carried out. None of the study patients had undergone 360-degrees scleral buckle procedure previously.
The study met the criteria set by the local ethical review board of the institution (IRB) and was performed according to the Declaration of Helsinki. Cases included from Päijät-Häme Central Hospital were approved for publication by the Päijät-Sote Institutional Committee. No informed consent was required by IRB since this is a retrospective study. Data was collected as a routine part of clinical care and stored in a patient’s electronic health record. No subjects have been recruited specifically for this retrospective analysis. No patient identifiable data necessitating consent was used in this study. The health care provider who produced the patient data can view it without the patient’s consent if it has a care relationship with the patient. No patient consent to publish was required. As such no further approval was deemed needed by the IRB for the analysis of the data. The Päijät-Häme Central Hospital verified that the study was exempt (retrospective, de-identified data) and no formal ethics approval was required in this study.
Statistical Analysis
The paired Student’s t-test for continuous data with normal distribution was conducted to compare IOP values. The Wilcoxon signed rank-sum test for continuous data without normal distribution was used to assess differences in the number of medications and visual acuity between the eyes before and after surgery. Snellen visual acuity measurements were converted to the logarithm of the minimum angle of resolution equivalents. Conventional methods and the Kaplan–Meier life-table analysis was used to determine surgical outcome. Statistical significance was implied by P value less than or equal to 0.05. Statistical analyses were performed using SSPS version 22.0 for Windows (IBM, USA).
Customization of Baerveldt Implant Plate Size
A fornix-based conjunctival flap and a subTenon/conjunctival pocket were created in the superotemporal quadrant under peribulbar anesthesia. The superior and lateral rectus muscles were isolated, and 4–0 silk traction sutures placed under the muscles. After verifying the patency of the Baerveldt implant tube by balanced salt solution (BSS) irrigation, the tube was occluded near the plate with two 6–0 polyglactin 910 (Vicryl-rapide, Ethicon, Johnson & Johnson, USA) ligation sutures placing the knots on the underside of the tube. Next, the BSS was injected into the tube to ensure the ligature was tight. The distance between the rectus muscles at the equator of the eyeball was measured using a surgical caliper. The Baerveldt implant plate was cut with straight dissecting scissors considering the distance between the muscles (Figure 1).
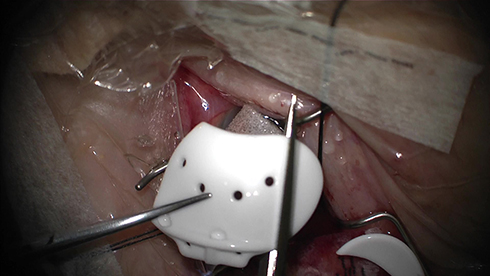 |
Figure 1 Customizing a Baerveldt 250 mm2 implant plate size considering the distance between the rectus muscles by cutting with straight dissecting scissors. |
The custom-made Baerveldt implant was secured to the sclera usually 8 mm posterior to the limbus with 8-0 nylon (Ethilon, Ethicon, Johnson & Johnson, USA) sutures and the knots were placed inside the implant plate holes. A lamellar scleral tunnel was created with a crescent knife from near the anterior edge of the plate to 2 mm from the limbus. The tunnel was completed with a 23 G needle, which was used to penetrate into the anterior chamber at an angle parallel to the iris plane. The end of the implant tube was shortened and beveled up in order for the tube to extend a maximum of 2 mm inside the anterior chamber. The implant tube was inserted into the anterior chamber via the intrascleral tunnel. The conjunctiva was closed using running 9–0 polyglactin (Vicryl, Ethicon, Johnson & Johnson, USA) sutures. Postoperatively, topical dexamethasone drops combined with chloramphenicol (Oftan Dexa-Chlora, Santen, Tampere, Finland) were applied for five weeks.
Results
Patients’ characteristics and preoperative data are summarized in Table 1. The mean ±SD baseline IOP before the GDI procedure was 30.2 ± 6.9 mmHg (range 20–54), and the mean IOP at the last follow-up visit was 13.3 ± 5.1 mmHg (range 3–22), with a mean pressure drop of 16.9 mmHg (56%) (P<0.001). There was a statistically significant drop in IOP at 3 months, 6 months, and at 1 year (46%, 51%, 52%, respectively; P<0.001) (Figure 2). The number of antiglaucoma medications declined from mean 3.7 ± 1.0 (range 2–5) to 1.6 ± 1.1 (range 0–3) at the last visit (P<0.001) (Figure 3). The conventional success rate at the last follow-up visit was 79% (19 of 24 eyes). Fourteen (58%) of the 24 eyes were classified as qualified successes and five eyes (21%) complete successes. The Kaplan–Meier life-table analysis showed a 90% success rate after 24 months of follow-up (Figure 4).
 |
Table 1 Patient Demographics |
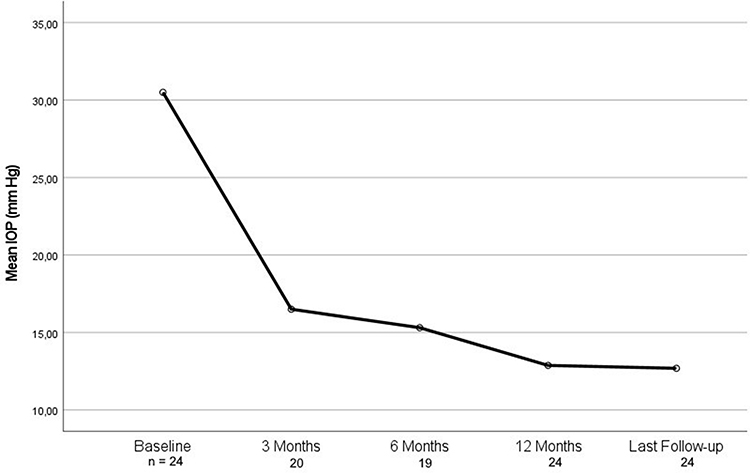 |
Figure 2 Mean intraocular pressure (IOP) of 24 eyes (24 patients) at baseline, over the 12 months’ time, and at the last follow-up visit. |
 |
Figure 3 Mean number of antiglaucoma medications of 24 eyes (24 patients) at baseline, over the 12 months’ time, and at the last follow-up visit. |
 |
Figure 4 Kaplan–Meier survival curve after 24 eyes of 24 glaucoma patients who presented with Baerveldt 250 mm2 implant plate customized size reduction surgery. Surgical success was defined as IOP <21 mmHg with at least a 30% reduction in IOP from baseline on two consecutive follow-up visits, IOP >5 mmHg on two consecutive follow-up visits, and neither reoperation of glaucoma nor loss of light perception vision. |
Complications included intraoperative SCH in one patient, postoperative hyphema in two patients and cataract in two patients. No significant ocular motility disturbance causing diplopia was detected. Visual acuity (± SD) decreased from 0.32 logMAR (± 0.22) to 0.43 logMAR (± 0.38) (P=0.018). Vision decreased in 7 of the 24 eyes (29%) due to diabetic maculopathy (2), cataract (2), central retinal vein occlusion (1), glaucoma progression (1), and intraoperative suprachoroidal hemorrhage (SCH) (1). None of the study patients required additional surgery due to complications, with the exception of two patients with cataract progression who underwent phacoemulsification with intraocular lens during the follow-up. All ligation sutures around the tube of the Baerveldt implant dissolved spontaneously between the third and fifth postoperative weeks.
Discussion
The axial length of an emmetropic human adult eye is approximately 22.0–24.8 mm with no significant difference between sexes and age groups.8 Short eyes have a shorter axial length, typically < 22 mm, and a shallower anterior chamber. Patients with short eyes tend to have a smaller orbital volume and GDI surgery in short eyes presents specific, unique situations.
New-onset persistent diplopia is a common complication after GDI placement.5,9 Decreases in orbital axial and coronal volumes as well as increased orbital rim distances have been detected in diplopic GDI patients.10 Patients with larger GDIs or higher profile plate GDIs were more likely to experience diplopia.10 In the present study, no patients developed new-onset persistent diplopia during the follow-up. However, this observation was only based on a verbal interview by a glaucoma specialist and not on a strabismus specialist examination.
The study by Heuer et al suggested that the double plate Molteno (270 mm2) provided better IOP control than the single plate (135 mm2) at 1 to 2 years postoperatively.3 However, there might be an upper limit beyond which a further increase in plate surface area does not benefit the decrease in IOP.11 The Baerveldt implant with a surface area of 350 mm2 has been found to have a significantly higher risk of hypotony (IOP ≤ 5 mmHg) compared to the Ahmed implant (New World Medical, Inc., California, USA) with a surface area of 184 mm2.12 Delayed hypotony after Baerveldt implantation can develop in 5% of patients.13 This hypotony places patients at risk of vision loss due to SCH.
SCHs may be categorized as either intraoperative or postoperative with relationship to the surgery. The reported incidence rates of postoperative SCH occurring within 3 months of GDI surgery varied from 1.2% to 2.7% among patients with a mean age of 66 years.14 None had postoperative SCH during the follow-up period, but one study patient had intraoperative SCH. She had several characteristics, including high preoperative IOP up to 54 mmHg, a history of leukemia and antiplatelet medications, which increase the risk of perioperative SCH. Postoperatively this patient developed persistent hypotony and loss of light perception vision and was classified as a surgical failure. Even if potential complication such as postoperative SCH did not exist, it is not possible to estimate if customized downsizing of the implant plate reduces the risk of this rare complication due to the small size of this special group of patients.
GDI models made from silicone have been shown to offer improved IOP reduction, as well as a lower incidence of excessive encapsulation when compared to polypropylene models.15 During the present study period the Baerveldt implant was used at our clinic as the primary GDI. The smallest original implant plate size is 250 mm2 among all GDI implants made from silicone. The originally smaller plate size is available only with hard plate GDIs made from polypropylene, which are resistant to cutting with scissors intraoperatively. Of the commercially available GDIs, only the Baerveldt implant, the PAUL Glaucoma Implant (Advanced Ophthalmic Innovations, Singapore, Republic of Singapore), the Aadi Glaucoma Shunt (Aurolab, India), and the Ahmed ClearPath (New World Medical, Inc., California, USA) plates are made from soft silicone and can be downsized by cutting with scissors.
Conclusions
In elderly patients with short eyes, the surgeon should, whenever possible, try to prevent hypotony after GDI surgery. Among these patients one may consider using intraoperative truncation of the GDI plate instead of an original GDI plate size to avoid hypotony and other complications in the postoperative period. According to the present pilot study, the Baerveldt implant with customized intraoperative implant plate size reduction seems to be an effective and safe treatment option for uncontrolled glaucoma in elderly patients with short eyes.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The study was presented in part at the 15th European Glaucoma Society Congress on June 7th, 2022, Athens, Greece.
Funding
This work was supported by the Päijät-Häme Joint Authority for Health and Wellbeing (Finland) research grant.
Disclosure
The author declares that there is no conflict of interest regarding the publication of this article.
References
1. Jeganathan VS, Ghosh S, Ruddle JB, et al. Risk factors for delayed suprachoroidal haemorrhage following glaucoma surgery. Br J Ophthalmol. 2008;92(10):1393–1396. doi:10.1136/bjo.2008.141689
2. Wijesinghe HK, Puthuran GV, Gedde SJ, et al. Incidence and outcomes of suprachoroidal hemorrhage following aurolab aqueous drainage 4. Implant in adult and pediatric glaucoma. J Glaucoma. 2021;30(6):497–550. doi:10.1097/IJG.0000000000001761
3. Heuer DK, Lloyd MA, Abrams DA, et al. Which is better? One or two? A randomized clinical trial of single-plate versus double-plate molteno implantation for glaucomas in aphakia and pseudophakia. Ophthalmology. 1992;99(10):1512–1519. doi:10.1016/S0161-6420(92)31772-5
4. Gedde SJ, Parrish RK, Budenz DL, Heuer DK. Update on aqueous shunts. Exp Eye Res. 2011;93(3):284–290. doi:10.1016/j.exer.2011.03.013
5. Sun PY, Leske DA, Holmes JM, Khanna CL. Diplopia in medically and surgically treated patients with glaucoma. Ophthalmology. 2017;124(2):257–262. doi:10.1016/j.ophtha.2016.10.006
6. Chen PP. Truncation of in situ baerveldt glaucoma drainage device for treatment of late persistent postoperative hypotony. J Glaucoma. 2017;26(2):e113–e114. doi:10.1097/IJG.0000000000000601
7. Mavrommatis MA, Dangda S, Sidoti PA, Panarelli JF. Downsizing a baerveldt glaucoma implant for the management of persistent postoperative hypotony: a case series. J Glaucoma. 2019;28(11):1019–1022. doi:10.1097/IJG.0000000000001365
8. Bekerman I, Gottlieb P, Vaiman M. Variations in eyeball diameters of the healthy adults. J Ophthalmol. 2014;2014:503645. doi:10.1155/2014/503645
9. Gedde JS, Herndon LW, Brandt JD, Budenz DL, Feuer WJ, Schiffman JC; Tube versus trabeculectomy study group. Postoperative complications in tube versus trabeculectomy (TVT) study during five years of follow-up. Am J Ophthalmol. 2012;153(5):804–814. doi:10.1016/j.ajo.2011.10.024
10. Kilgore KP, Wang F, Stern NC, et al. Rates of diplopia in Ahmed FP7, Baerveldt 250, and 350 glaucoma patients compared with medical controls. J Glaucoma. 2021;30(7):579–584. doi:10.1097/IJG.0000000000001886
11. Lloyd MA, Baerveldt G, Fellenbaum PS, et al. Intermediate-term results of a randomized clinical trial of the 350- versus the 500-mm2 Baerveldt implant. Ophthalmology. 1994;101(8):1456–1463. doi:10.1016/S0161-6420(94)31152-3
12. Christakis PG, Kalenak JW, Tsai JC, et al. The Ahmed Versus Baerveldt Study: five-year treatment outcomes. Ophthalmology. 2016;123(10):2093–2102. doi:10.1016/j.ophtha.2016.06.035
13. Christakis PG, Zhang D, Budenz DL, et al. Five-year pooled data analysis of the Ahmed Baerveldt Comparison Study and the Ahmed Versus Baerveldt Study. Am J Ophthalmol. 2017;176:118–126. doi:10.1016/j.ajo.2017.01.003
14. Vaziri K, Schwartz SG, Kishor KS, et al. Incidence of postoperative suprachoroidal hemorrhage after glaucoma filtration surgeries in the United States. Clin Ophthalmol. 2015;9:579–584. doi:10.2147/OPTH.S78359
15. Ishida K, Netland PA, Costa VP, Shiroma L, Khan B, Ahmed IIK. Comparison of polypropylene and silicone Ahmed glaucoma valves. Ophthalmology. 2006;113(2):1320–1326. doi:10.1016/j.ophtha.2006.04.020
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.