Back to Journals » Infection and Drug Resistance » Volume 13
Intraoperative Cefuroxime Irrigation Prophylaxis for Acute-Onset Endophthalmitis After Phacoemulsification Surgery
Received 5 March 2020
Accepted for publication 6 May 2020
Published 18 May 2020 Volume 2020:13 Pages 1455—1463
DOI https://doi.org/10.2147/IDR.S252674
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Xiubin Ma,1,2 Lixin Xie,2 Yusen Huang2
1Medical College, Qingdao University, Qingdao, People’s Republic of China; 2State Key Laboratory Cultivation Base, Shandong Provincial Key Laboratory of Ophthalmology, Shandong Eye Institute, Shandong First Medical University and Shandong Academy of Medical Sciences, Qingdao, People’s Republic of China
Correspondence: Yusen Huang; Lixin Xie
State Key Laboratory Cultivation Base, Shandong Provincial Key Laboratory of Ophthalmology, Shandong Eye Institute, Shandong First Medical University and Shandong Academy of Medical Sciences, Qingdao 266071, People’s Republic of China
Tel +86 532-85876380
Email [email protected]; [email protected]
Purpose: Acute-onset postoperative endophthalmitis usually compromises the visual function and anatomical integrity of the eye. The aim of this study was to evaluate the efficacy of intraoperative cefuroxime use in irrigating solution on prevention of acute-onset endophthalmitis after phacoemulsification.
Methods: This retrospective, comparative, interventional cohort study included patients who underwent phacoemulsification between January 1, 2012, and December 31, 2019. Under a uniform perioperative protocol, the patients who had surgery from January 1, 2012, to December 31, 2014, received irrigating infusion fluid containing balanced salt solution (BSS) only (group 1), and those from January 1, 2015, to December 31, 2019, received BSS with cefuroxime (1500 μg/mL) during surgery (group 2). All eyes were evaluated postoperatively, and the eyes suspected to have endophthalmitis were assessed and treated by a consultation team. The rates of postoperative endophthalmitis in these two groups were calculated.
Results: A total of 61,299 eyes were included over the eight years. Among these eyes, 11 in group 1 (0.07% of 15,948 eyes) and 5 in group 2 (0.01% of 45,351 eyes) developed endophthalmitis, and the difference was significant (P < 0.01). Five among 16 patients (31.25%) with endophthalmitis were positive in bacterial culture. The positive rate of bacterial culture was not significantly different between group 1 (4/11) and group 2 (1/5) (P > 0.05). No adverse events related to the irrigation of cefuroxime were found.
Conclusion: Intraoperative cefuroxime irrigation (1500 μg/mL) could decrease the rate of postoperative endophthalmitis after phacoemulsification by 7-fold. This study provides evidence that intraoperative irrigation with cefuroxime is effective as an antibiotic prophylaxis for endophthalmitis.
Keywords: cataract, postoperative endophthalmitis, intraoperative cefuroxime irrigation, phacoemulsification
Introduction
In the treatment of cataract, the leading cause of blindness worldwide, phacoemulsification has become the dominant surgical procedure of choice. However, the prevention of acute-onset endophthalmitis, which is a visually devastating complication after cataract surgery, remains a concern for many cataract surgeons. Even with prompt and appropriate treatment, postoperative endophthalmitis may significantly compromise the visual function and anatomical integrity of the eye. Despite continuing advancements in ophthalmic care, the incidence of endophthalmitis over the past decade was 0.02–0.30%.1–3
With the significant increase in the volume of cataract surgery due to the aging of the population, adopting a variety of prophylactic techniques for endophthalmitis has become a rising global imperative. At present, there is no global consensus on the optimal strategies to prevent endophthalmitis. Some approaches, such as preoperative povidone-iodine antisepsis, which is the only technique to reach category II evidence in reducing the rate of endophthalmitis, have been mandated in the guidelines for prophylaxis against endophthalmitis following cataract surgery in many countries. However, other approaches, such as use of topical and intracameral antibiotics, remain controversial.
Bacteria can enter the anterior chamber intraoperatively or early after surgery. As contamination is then present, intraoperative use of antibiotics should be reasonable. Although a certain level of intraocular antibiotics can be achieved with preoperative topical administration, the use of antibiotics during surgery can result in extremely high concentrations that last for several hours.4 Many studies conducted among different populations have reported marked reductions in the rate of postoperative endophthalmitis when intracameral antibiotics were introduced.5–8 The 2014 survey on the American Society of Cataract and Refractive Surgery members found that 36% of the respondents have used intraocular antibiotic prophylaxis compared with 14% in the 2007 survey.9
Although intracameral antibiotics are already widely accepted, the optimal choice of prophylactic routes to prevent postoperative endophthalmitis is controversial.10,11 Among the studies on intracameral antibiotics, only a few reports have been conducted on the significant effects of intracameral cefuroxime outside Europe.12,13 Moreover, only in European countries is commercial cefuroxime formulation (Aprokam) labeled and available. The off-label use of intracameral cefuroxime usually requires a two-step dilution process, and has the potential risks including dilution errors, bacterial contamination, and toxic anterior segment syndrome, leading to the reluctance of some surgeons to adopt the routine use of intracameral antibiotics.9
To address these concerns, the manner of drug preparation was modified in this study as 750 mg of cefuroxime dissolved in 500 mL of balanced salt solution (BSS) for irrigating during phacoemulsification. Although the concentration (1500 μg/mL) was about 45% of the European Society of Cataract and Refractive Surgeons (ESCRS) recommendation (3,300 μg/mL), it required only a one-step reconstitution without further dilution, which could reduce the potential risks of both preparation errors and contamination. The effect of irrigation with cefuroxime on the prevention of acute-onset endophthalmitis after phacoemulsification was investigated.
Patients and Methods
Study Population
Patients who underwent phacoemulsification surgeries between January 1, 2012, and December 31, 2019, were enrolled in this retrospective, comparative, interventional cohort study. Group 1 included patients who received irrigation of BSS only during surgery performed from January 1, 2012 to December 31, 2014, and group 2 included patients who received BSS with cefuroxime (1500 μg/mL) during surgery performed from January 1, 2015 to December 31, 2019.
Perioperative Medical Treatment
Prior to surgery, all patients had antisepsis with topical 5% povidone-iodine eyedrops applied to the ocular surface, conjunctival sac, and upper and lower eyelashes (≥3 min prior to surgery) and 5% povidone-iodine eyedrops applied to the periorbital skin before draping. Levofloxacin 0.5% eyedrops were topically administered for one day for a total of eight times. Postoperatively, topical levofloxacin 0.5% and steroid eyedrops were prescribed four times daily for 1–2 weeks and diclofenac sodium eyedrops four times daily for four weeks. The patients were routinely examined at 1 and 7 days, 4, and 12 weeks ±1 (SD) postoperatively and given standard instructions to seek urgent medical attention if they developed symptoms of pain, redness, and loss of vision.
Drug Preparation and Surgical Procedure
The irrigating solution was prepared in hundred-level laminar flow operating rooms. The one-step reconstitution of cefuroxime irrigating solutions involved the following steps. A total of 10 mL BSS aspirated using a 10-mL syringe from 500 mL BSS (Shenyang Xingqi, Shenyang, Liaoning, China) was injected into a vial containing 750 mg cefuroxime (Esseti Farmaceutici S.r.l., Noble, Italy). After the vial was gently shaken until the solution was free from visible particles, the solution was injected into 490 mL BSS using the 10-mL syringe. The concentration (1500 μg/mL) of the mixed solution was 45% of the ESCRS standard (3,300 μg/mL). The cefuroxime irrigating solution was always reconstituted by a circulating nurse under the supervision of an instrument nurse and used within 1 hour. Each irrigation/aspiration cannula was indicated for single patient use. In the course of phacoemulsification, a 2.2- to 2.8-mm, non-sutured, clear corneal incision was made. After the emulsification of the lens, a foldable intraocular lens was inserted, and the wound was hydrated. For a proportion of pediatric cataract cases, cataract extraction combined with a standard primary posterior continuous circular capsulorhexis and anterior vitrectomy was performed through a sutured scleral tunnel incision. Patients who underwent other combined procedures, such as trabeculectomy and penetrating keratoplasty, were not included in the study. Topical anesthesia was used in the majority of patients, while local or general anesthesia was given to the remaining patients.
Diagnosis and Treatment of Presumed Endophthalmitis
Within six weeks after cataract surgery, the patient was highly suspected to have endophthalmitis if there was eye pain, anterior chamber reaction or flare, hypopyon, and/or vitritis. Acute-onset endophthalmitis was diagnosed when toxic anterior segment syndrome, non-infective uveitis, and other causes of intraocular inflammation were confirmed to be excluded. Both positive and negative bacterial cultures were included. Ultrasound biomicroscopy was performed when the fundus was invisible under an indirect ophthalmoscope. Patients with presumed endogenous endophthalmitis, traumatic endophthalmitis, and delayed onset endophthalmitis (beyond six weeks after surgery) were also excluded from the study. Once endophthalmitis was suspected, an emergency plan was immediately initiated by a consultation team, including senior experts specializing in cataract, vitreoretinal surgery, and hospital-acquired infection control.
A management protocol was conducted in accordance with the Consensus on the Treatment of Endophthalmitis Following Cataract Surgery in China,14 Endophthalmitis Vitrectomy Study guidelines,15 ESCRS guidelines,16 and our clinical experience.17 Briefly, the following measures were implemented: (1) Antibiotic irrigation (0.02 mg/mL vancomycin and 0.04 mg/mL ceftazidime) of the anterior chamber and capsular bag, in combination with topical and systemic antibiotics, was given if there were inflammatory responses clearly restricted to the anterior segment, hypopyon less than 1.0 mm, no vitreous involvement or only mild infiltration by inflammatory cells in the anterior vitreous, visualization of some retinal detail or a good red reflex, and an intact posterior capsule. An aqueous tap was then taken. (2) If the anterior chamber infection was serious with a severely inflamed or purulent vitreous body, antibiotic irrigation, intravitreal antibiotic injection or pars plana vitrectomy, and the combined use of topical and systemic antibiotics were performed. Aqueous and vitreous taps were taken.
The operated eyes were observed under a slit-lamp microscope every 4 h after the initial treatment. The subsequent treatment was modified based on the clinical response and the laboratory report. Favorable responses included an increase in visual acuity, clearing of media, a decrease in hypopyon, and the resolution of pain. In eyes that did not respond well to initial therapy within 24 h or had become worse, a further aggressive approach was considered. Repeated intravitreal antibiotic injections were administered when the fundus examination showed persistent inflammation or when there was no improvement or poor improvement in visual acuity.
The logarithm of the minimal angle of resolution (logMAR) corrected distance visual acuity (CDVA) was evaluated. Finger counting and hand movement were considered to denote a CDVA of 2.00 and 3.00, respectively. Light perception was recorded as a CDVA of 4.00, whereas no light perception and loss of globe were recorded as 5.00.
Statistical Analysis
The total number of cataract surgeries performed in each group was digitally registered at our institution. The clinical notes of each endophthalmitis case were recorded. Statistical analysis was performed using SPSS version 20.0 and Stata version 11.1 (Stata Corp. LP, College Station, TX). The categorical variables were expressed as frequency (percentage). Fisher’s exact test was used to compare endophthalmitis, culture-positive endophthalmitis, sex and systemic diseases, and nonparametric Mann–Whitney U-test was used to compare mean age, duration from surgery to presentation, CDVA at presentation, and final CDVA between groups. A P value of less than 0.05 was considered statistically significant.
Results
Over the eight-year study period, 61,299 consecutive phacoemulsification surgeries in 46,068 patients were performed. Sixteen eyes (16 patients) developed postoperative endophthalmitis. The median time from cataract extraction to onset was 7.56 days (range, 1–30). Five out of 16 eyes (31.25%) subjected to culture were found to be positive. No adverse drug reactions, such as toxic anterior segment syndrome or corneal decompensation, which were related to the administration of intracameral antibiotics, were reported during the entire study period. Tables 1 and 2 show the demographic and clinical features, treatment, and outcomes of the 16 patients. Capsular tear occurred in 819 eyes receiving combined anterior vitrectomy or not, including posterior capsule rupture without vitreous loss in 46 eyes, posterior capsule rupture with vitreous loss in 429 eyes, and primary posterior continuous circular capsulorhexis and anterior vitrectomy in 344 eyes with pediatric cataract, and none developed endophthalmitis. All the 16 eyes with endophthalmitis only underwent phacoemulsification with IOL implantation, with no capsular tear or anterior vitrectomy. No incision leakage was found in these eyes when endophthalmitis was initially identified.
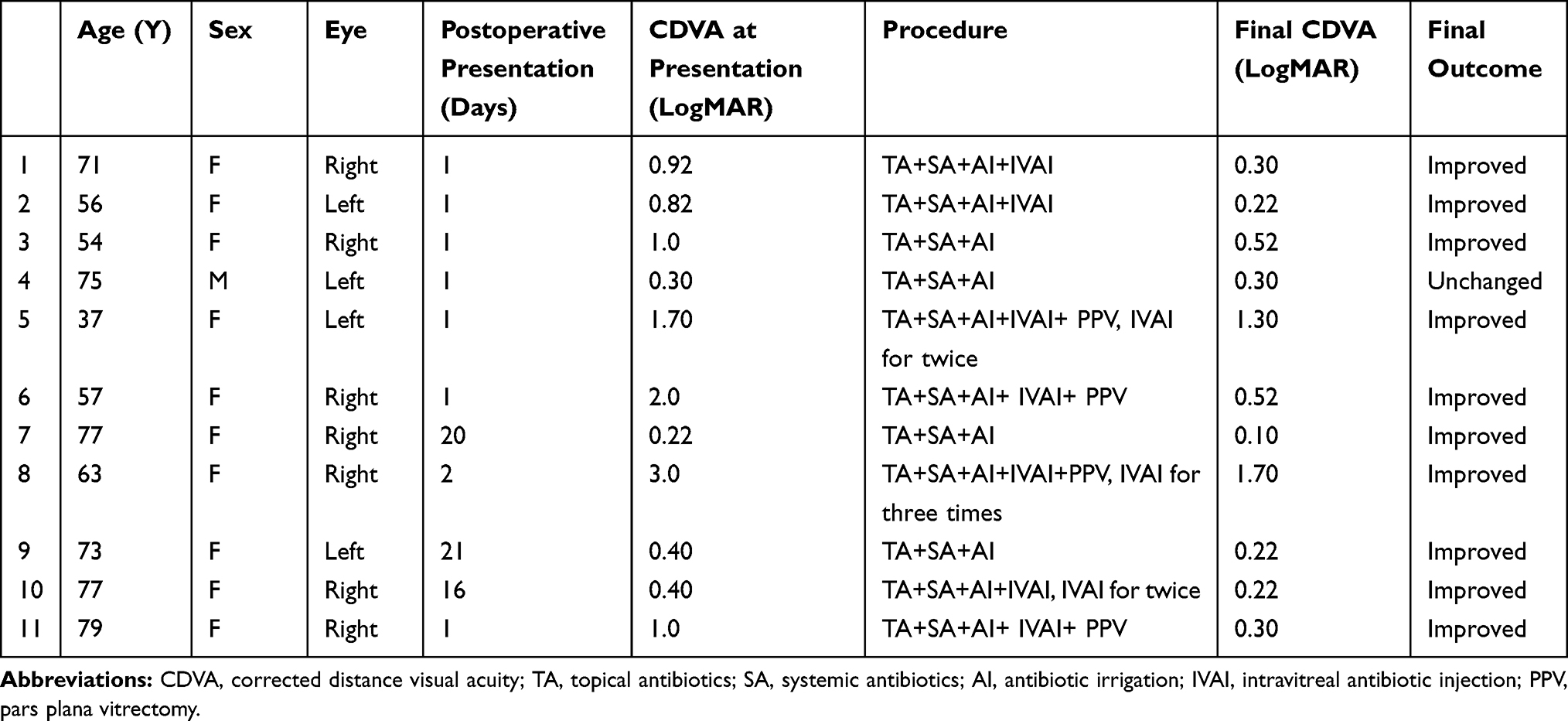 |
Table 1 Characteristics of the 11 Eyes Suffering Endophthalmitis in Group 1 |
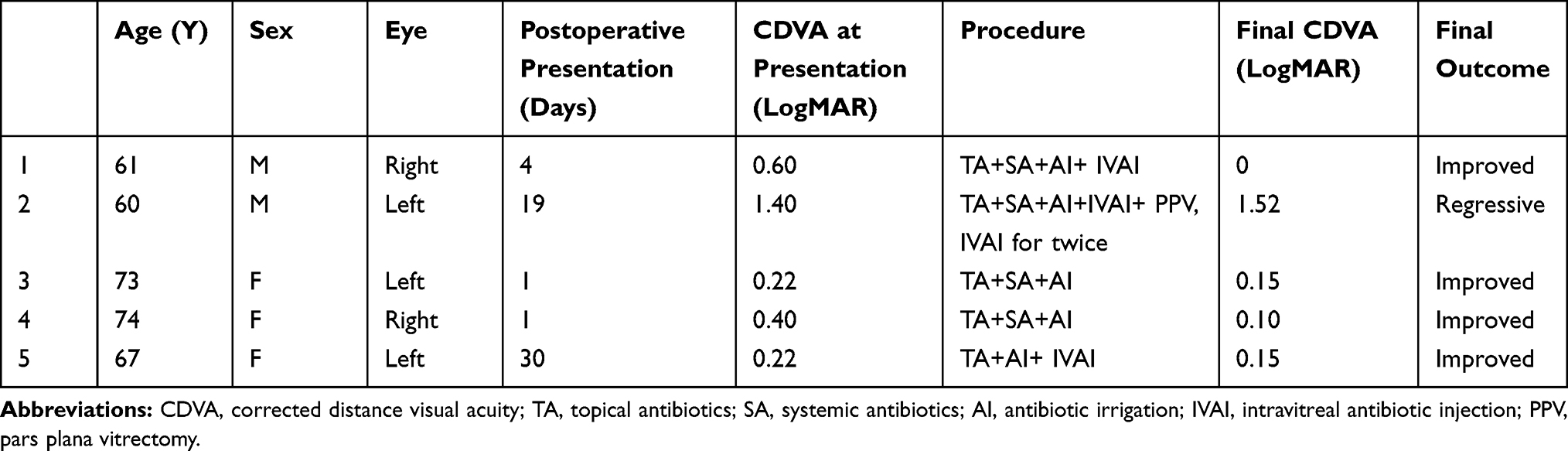 |
Table 2 Characteristics of the 5 Eyes Suffering Endophthalmitis in Group 2 |
Among the 16 patients with endophthalmitis, six were treated with topical and systemic antibiotics and antibiotic irrigation; four received topical and systemic antibiotics, antibiotic irrigation, and intravitreal antibiotic injection; one was administered with topical antibiotic irrigation and intravitreal antibiotic injection; five were treated with topical and systemic antibiotics, antibiotic irrigation, intravitreal antibiotic injection, and pars plana vitrectomy.
In group 1, 11 of 15,948 eyes suffered acute-onset postoperative endophthalmitis at a rate of 0.07%. The 11 patients comprised one male and 10 females, aged 37–79 years (mean, 65.36 years). Two of them had diabetes mellitus, which might increase the incidence of endophthalmitis. The duration from surgery to presentation was 1–21 days (mean, 6.0 days). Aqueous and/or vitreous aspirates from the 11 infected eyes were sent for microbial workup. Four eyes had positive culture results, with Staphylococcus hominissubsp., Neisseria mucosa, Corynebacterium xerosis, and Enterococcus faecalis being identified (Table 3). The mean CDVA increased from 1.07 logMAR (range, 0.22–3.00 logMAR) at presentation to 0.52 logMAR (range, 0.10–1.70 logMAR) at the final follow-up visit. Vision in one eye was not improved. In group 2, totally 45,351 eyes received cefuroxime irrigation at the time of cataract surgery. The incidence rate of clinical endophthalmitis was 0.01% (5 eyes), which was significantly lower than that in group 1 (P < 0.01). The two male patients and three female patients were aged 60–74 years (mean, 67.0 years). Two patients were in an immunocompromised state secondary to either multiple sclerosis or psoriasis. Both of these systemic diseases were risk factors of endophthalmitis. The duration from surgery to presentation was 1–30 days (mean, 11.0 days). Streptococcus gordonii was isolated from one eye (Table 3). The positive rate of bacterial culture was not significantly different between group 1 and group 2 (P > 0.05). The CDVA was 0.22–1.40 logMAR (mean, 0.57 logMAR) at presentation and 0.00–1.52 logMAR (mean, 0.38 logMAR) at the final visit. One eye did not achieve improved vision. The two groups were comparable in sex, systemic diseases, mean age, duration from surgery to presentation, CDVA at presentation, and final CDVA (P = 0.21, 0.55, Fisher’s exact test; P = 0.91, 0.34, 0.16, and 0.69, nonparametric Mann–Whitney U-test).
 |
Table 3 Causative Microorganisms and Their Antibiotic Susceptibility Patterns in the Five Cases with Endophthalmitis |
Discussion
The optimum antibiotics selected to prevent endophthalmitis after phacoemulsification should possess the properties of broad spectrum, intraocular safety, minimized resistance, and easy preparation. In the present study, intraoperative cefuroxime irrigation was confirmed to effectively reduce the incidence of postoperative endophthalmitis with no adverse events. To our knowledge, this is the first large population-based study to determine the role of intraoperative cefuroxime irrigation prophylaxis for acute-onset endophthalmitis after phacoemulsification surgery.
Despite the use of preoperative antisepsis regimens, the ocular surface cannot be rendered completely aseptic. In patients who have blepharitis and meibomian gland dysfunction, meibomian secretion can go into the surgical field under the extrusion of the eye speculum and the irritation of the operation. Regardless of the administration of antibiotics and povidone-iodine before surgery and following the careful sterilization and aseptic protocols, bacterial contamination of the anterior chamber at the end of cataract surgery occurs in 20–40% of cases.18–22 Moreover, evidence shows that postoperative bacterial endophthalmitis is commonly caused by exposure to bacteria from the external eye during or after cataract surgery. The etiologies of the aqueous fluid contamination during cataract surgery are as follows: the entry of multiple instruments may carry external ocular surface flora into the anterior chamber; incision leakage caused by poor or delayed wound healing may allow the retrograde influx of external surface fluid during and after surgery; contaminated surgical instruments or implants may induce infection. Therefore, cefuroxime irrigation was intended to reduce the bacterial flora on the ocular surface and kill bacterial microbes that could be introduced into the aqueous humor.
Cefuroxime is a broad-spectrum antibiotic that covers most gram-positive and gram-negative organisms commonly associated with postoperative infectious endophthalmitis. The bactericidal activity of cefuroxime is both concentration and time dependent and occurs at concentrations that are 4–5 times higher than the minimal inhibitory concentration (MIC). No data are available on the duration of effectiveness of intracameral cefuroxime concentrations after being used. In the physiological state, aqueous is constantly replenished at a rate of 1% per minute.23 Aprokam, which has an intracameral cefuroxime concentration of about 3,300 μg/mL (assuming a 0.3 mL anterior chamber volume), cites mean aqueous humor levels of 2,614 +/− 209 μg/mL at 30 s after drug administration. Montan et al23 reported that the intracameral cefuroxime concentration declined to 1,027 ± 43 μg/mL at 1 h (28% of the value at 30 s), which was attributed to the removal of cefuroxime through the trabecular meshwork and partial diffusing into the vitreous. In this study, the initial cefuroxime concentration in the anterior chamber was 1500 μg/mL. Theoretically, the concentration is superior to the MIC (2–4 μg/mL) after 2 h for most bacteria responsible for postoperative endophthalmitis.24 The efficiency of off-label intracameral cefuroxime in the prophylaxis of endophthalmitis in patients undergoing cataract surgery has been demonstrated. In a landmark, randomized, and multinational ESCRS trial, the incidence of endophthalmitis was significantly lower in patients receiving intracameral cefuroxime with 0.5% levofloxacin ophthalmic solution than in those receiving 0.5% levofloxacin solution only (0.05% vs 0.25%).5 In other two large, prospective studies, the incidence of endophthalmitis was also significantly lower in patients who were treated with intracameral cefuroxime compared with those who were not (0.05% vs 0.35% and 0.05% vs 0.22%).2,25 Subsequent retrospective studies further disclosed the efficacy of intracameral cefuroxime.2,12,13,26-29 Recently, the intracameral injection of Aprokam after cataract surgery was reported to show an 8.5-fold reduction in endophthalmitis (0.02% vs 0.17%).30
The rate of postoperative endophthalmitis was 0.07% (11/15, 948) in group 1 of the current study, lower than 0.32% (13/3, 990), 0.59% (39/6, 595), and 1.24% (35/2, 826) in patients without intracameral cefuroxime in the ESCRS,5 Spanish,27 and French26 studies, respectively. Although the cefuroxime concentration in group 2 of our study was about 45% of the ESCRS recommendation, intraoperative cefuroxime irrigation (750 mg/500 mL) reduced endophthalmitis by 7.0-fold (0.07% vs 0.01%). The rate (0.01%) was slightly higher than those reported in large-scale retrospective studies performed in Iran (0%, cefuroxime)31 but lower than those reported by researchers from France (0.02%, Aprokam; 0.04%, cefuroxime),26,30 India (0.02%, moxifloxacin),32 Sweden (0.03%, multiple),33 Spain (0.04%, cefuroxime),34 the United States (0.04%, cefazolin),35 and Australia (0.05%, vancomycin).2 A recent meta-analysis assessed the endophthalmitis incidence among over 900,000 eyes reported in 17 studies, finding that the average postoperative endophthalmitis incidence with intracameral cefuroxime, moxifloxacin, and vancomycin was 0.03%, 0.02%, and 0.01%, respectively, in the recent two decades.36
Although there is growing evidence to support the efficacy of using cefuroxime as prophylaxis against endophthalmitis, the most important deterrent appears to be the lack of a commercially approved preparation in countries outside Europe. The preparation of intracameral cefuroxime involves a two-step dilution to achieve the desired concentration of 1 mg in 0.1 mL. Mixing antibiotics in the operating room increases the theoretical risk of dosing errors and the potential for introducing intraocular contaminants when several doses of cefuroxime are decanted from one vial.37,38 Moreover, the inaccurate preparation of intracameral cefuroxime was reported to result in ocular toxicity.39–42 Aprokam, a prediluted preparation of 1 mg/0.1 mL cefuroxime, was approved by the European Medicines Agency in 2012 for intracameral injection for the prophylaxis of postoperative endophthalmitis after cataract surgery. It requires only a one-step reconstitution without further dilution, which has the potential to reduce the risk of preparation errors. The modified method introduced in this study is also composed of only one step conducted by the operating room staff before surgery without further dilution, minimizing both preparation errors and contamination.
The design of this study has a potential weakness. Intraoperative cefuroxime irrigation for the prevention of acute-onset postoperative endophthalmitis seems to be simple, safe, and efficacious, but it was used on an off-label basis with all the potential legal consequences. The use of a compounding pharmacy was not without risks. As ocular toxicity in patients who took an intracameral injection of 1 mg cefuroxime during cataract surgery was not reported in previous studies,23,42 we did not specifically discuss the adverse events, such as changes in intraocular pressure, induced laser flare, endothelial cell count, and macular thickness, in this study.
Endophthalmitis is associated with a variety of factors, including the species and quantity of bacteria entering the anterior chamber, operative technique, sanitary condition, perioperative aseptic measures, and postoperative patient education.43 Studies have reported intracameral antibiotics present no benefits when topical antibiotics are used,3 or vice versa.44 Lack of consensus makes it unlikely to conclusively define the optimal endophthalmitis prophylaxis techniques via additional clinical trials. It may differ in determining whether to use intraoperative antibiotic prophylaxis, which antibiotic and which route to choose, based on the clinical settings in different countries or regions. Concerns about toxicity, contamination, and institutional regulations remain with the use of antibiotics. Individual centers and surgeons should evaluate the benefits and risks associated with various intracameral antibiotics and the resources available to ensure appropriate dilution and antiseptic sterility.
In developing countries, patients who have cataract surgery in small- and medium-scale departments of ophthalmology may be at a higher risk for infectious endophthalmitis because of outdated equipment or surgery rooms, inadequate patient hygiene, delayed postoperative follow-up, and poor compliance with doctor’s advice.45 Once infection occurs, deferred diagnosis and delayed treatment are common because few experienced vitreoretinal surgeons are available. Intraoperative cefuroxime irrigation with the one-step preparation seems to be feasible and helpful in such settings.
In conclusion, with a modified, one-step reconstitution of cefuroxime irrigation during cataract surgery, the potential risk of drug dilution errors and contamination can be minimized, and the bacterial microbes in the aqueous humor and conjunctival sac can be reduced, achieving a decline in the risk of endophthalmitis. Outside Europe, the use of intraoperative cefuroxime irrigation may be a good option to prevent acute-onset endophthalmitis after phacoemulsification before a commercial intracameral antibiotic is available.
Data Sharing Statement
All data relevant to the study are included in the article. The datasets used and analyzed during the current study are available from the corresponding authors at any time upon reasonable request.
Ethics and Consent Statement
The study was approved by the ethics committee of the Shandong Eye Institute, registered on the Chinese Clinical Trial (ChiCTR1900021335), and performed in accordance with the ethical standards presented in the 1964 Declaration of Helsinki and its later amendments. Written informed consent was obtained from all patients before the procedure.
Acknowledgment
We would like to thank Ping Lin for her linguistic and editorial assistance.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
All authors report no conflicts of interest related to this article.
References
1. Weston K, Nicholson R, Bunce C, Yang YF. An 8-year retrospective study of cataract surgery and postoperative endophthalmitis: injectable intraocular lenses may reduce the incidence of postoperative endophthalmitis. Br J Ophthalmol. 2015;99(10):1377–1380. doi:10.1136/bjophthalmol-2014-306372
2. Au CP, White AJ, Healey PR. Efficacy and cost-effectiveness of intracameral vancomycin in reducing postoperative endophthalmitis incidence in Australia. Clin Exp Ophthalmol. 2016;44(9):803–811. doi:10.1111/ceo.12789
3. Kessel L, Flesner P, Andresen J, Erngaard D, Tendal B, Hjortdal J. Antibiotic prevention of postcataract endophthalmitis: a systematic review and meta-analysis. Acta Ophthalmol. 2015;93(4):303–317. doi:10.1111/aos.12684
4. Murphy CC, Nicholson S, Quah SA, et al. Pharmacokinetics of vancomycin following intracameral bolus injection in patients undergoing phacoemulsification cataract surgery. Br J Ophthalmol. 2007;91(10):1350–1353. doi:10.1136/bjo.2006.112060
5. Endophthalmitis Study Group, and European Society of Cataract & Refractive Surgeons. Prophylaxis of postoperative endophthalmitis following cataract surgery: results of the ESCRS multicenter study and identification of risk factors. J Cataract Refract Surg. 2007;33(6):978–988. doi:10.1016/j.jcrs.2007.02.032
6. Tan CS, Wong HK, Yang FP. Epidemiology of postoperative endophthalmitis in an Asian population: 11-year incidence and effect of intracameral antibiotic agents. J Cataract Refract Surg. 2012;38(3):425–430. doi:10.1016/j.jcrs.2011.09.040
7. Lipsky L, Barrett G. Intracameral antibiotics for prophylaxis of postoperative endophthalmitis in Australia: a review. Clin Exp Ophthalmol. 2019;47(4):537–541. doi:10.1111/ceo.13419
8. Ng AL, Tang WW, Li PS, Li KK. Intracameral cefuroxime in the prevention of postoperative endophthalmitis: an experience from Hong Kong. Graefes Arch Clin Exp Ophthalmol. 2016;254(10):1987–1992. doi:10.1007/s00417-016-3473-0
9. Chang DF, Braga-Mele R, Henderson BA, et al. Antibiotic prophylaxis of postoperative endophthalmitis after cataract surgery: results of the 2014 ASCRS member survey. J Cataract Refract Surg. 2015;41(6):1300–1305. doi:10.1016/j.jcrs.2015.01.014
10. Ng JQ, Morlet N, Bulsara MK, Semmens JB. Reducing the risk for endophthalmitis after cataract surgery: population-based nested case-control study: endophthalmitis population study of Western Australia sixth report. J Cataract Refract Surg. 2007;33(2):269–280. doi:10.1016/j.jcrs.2006.10.067
11. Rudnisky CJ, Wan D, Weis E. Antibiotic choice for the prophylaxis of post-cataract extraction endophthalmitis. Ophthalmology. 2014;121(4):835–841. doi:10.1016/j.ophtha.2013.08.046
12. Shorstein NH, Winthrop KL, Herrinton LJ. Decreased postoperative endophthalmitis rate after institution of intracameral antibiotics in a Northern California eye department. J Cataract Refract Surg. 2013;39(1):8–14. doi:10.1016/j.jcrs.2012.07.031
13. Van der Merwe J, Mustak H, Cook C. Endophthalmitis prophylaxis with intracameral cefuroxime in South Africa. J Cataract Refract Surg. 2012;38(11):2054. doi:10.1016/j.jcrs.2012.09.004
14. Chinese Cataract Society. Consensus on treatment of post-cataract endophthalmitis in China. Zhonghua Yan Ke Za Zhi. 2010;46:764–766. (In Chinese.).
15. Results of the Endophthalmitis Vitrectomy Study. A randomized trial of immediate vitrectomy and of intravenous antibiotics for the treatment of postoperative bacterial endophthalmitis. Arch Ophthalmol. 1995;113(12):1479–1496. doi:10.1001/archopht.1995.01100120009001
16. Barry P, Cordovés L, Gardner S. ESCRS Guidelines for Prevention and Treatment of Endophthalmitis Following Cataract Surgery: Data,Dilemmas and Conclusions. Dublin, Ireland: The European Society for Cataract & Refractive Surgeons; 2013.
17. Huang Y, Zhan Y, Xie L. Clinical observations of acute-onset endophthalmitis after clear corneal phacoemulsification. [Zhonghua Yan Ke Za Zhi] Chin J Ophthalmol. 2015;51(12):918–923.
18. Sobaci G, Tuncer K, Tas A, et al. The effect of intraoperative antibiotics in irrigating solutions on aqueous humor contamination and endophthalmitis after phacoemulsification surgery. Eur J Ophthalmol. 2003;13(9–10):773–778. doi:10.1177/1120672103013009-1007
19. Balestrazzi A, Malandrini A, Montagnani F, et al. Phacoemulsificator and sterile drapes contamination during cataract surgery: a microbiological study. Eur J Ophthalmol. 2012;22(2):188–194. doi:10.5301/EJO.2011.8434
20. Durand ML. Endophthalmitis. Clin Microbiol Infect. 2013;19(3):227–234. doi:10.1111/1469-0691.12118
21. Bausz M, Fodor E, Resch MD, et al. Bacterial contamination in the anterior chamber after povidone-iodine application and the effect of the lens implantation device. J Cataract Refract Surg. 2006;32(10):1691–1695. doi:10.1016/j.jcrs.2006.05.019
22. Leong JK, Shah R, McCluskey PJ, Benn RA, Taylor RF. Bacterial contamination of the anterior chamber during phacoemulsification cataract surgery. J Cataract Refract Surg. 2002;28(5):826–833. doi:10.1016/S0886-3350(01)01160-9
23. Montan PG, Wejde G, Koranyi G, Rylander M. Prophylactic intracameral cefuroxime. Efficacy in preventing endophthalmitis after cataract surgery. J Cataract Refract Surg. 2002;28(6):977–981. doi:10.1016/S0886-3350(01)01269-X
24. Mendivil SA, Mendivil MP. The effect of topical povidone-iodine, intraocular vancomycin, or both on aqueous humor cultures at the time of cataract surgery. Am J Ophthalmol. 2001;131(3):293–300. doi:10.1016/S0002-9394(00)00651-6
25. Wejde G, Montan P, Lundstrom M, Stenevi U, Thorburn W. Endophthalmitis following cataract surgery in Sweden: national prospective survey 1999–2001. Acta Ophthalmol Scand. 2005;83(1):7–10. doi:10.1111/j.1600-0420.2005.00377.x
26. Barreau G, Mounier M, Marin B, Adenis JP, Robert PY. Intracameral cefuroxime injection at the end of cataract surgery to reduce the incidence of endophthalmitis: French study. J Cataract Refract Surg. 2012;38(8):1370–1375. doi:10.1016/j.jcrs.2012.03.024
27. Garcia-Saenz MC, Arias-Puente A, Rodriguez-Caravaca G, Banuelos JB. Effectiveness of intracameral cefuroxime in preventing endophthalmitis after cataract surgery Ten-year comparative study. J Cataract Refract Surg. 2010;36(2):203–207. doi:10.1016/j.jcrs.2009.08.023
28. Fontanet JM, March F, Moron A, Gorgas MQ. Effectiveness of the use of intracameral cefuroxime as prophylaxis in cataract surgery. Farm Hosp. 2012;36(3):170–172. doi:10.1016/j.farma.2011.07.003
29. Gualino V, San S, Guillot E, et al. Intracameral cefuroxime injections in prophylaxis of postoperative endophthalmitis after cataract surgery: implementation and results. J Fr Ophtalmol. 2010;33(8):551–555. doi:10.1016/j.jfo.2010.07.011
30. Mesnard C, Beral L, Hage R, et al. Endophthalmitis after cataract surgery despite intracameral antibiotic prophylaxis with licensed cefuroxime. J Cataract Refract Surg. 2016;42(9):1318–1323. doi:10.1016/j.jcrs.2016.06.030
31. Jabbarvand M, Hashemian H, Khodaparast M, et al. Endophthalmitis occurring after cataract surgery: outcomes of more than 480 000 cataract surgeries, epidemiologic features, and risk factors. Ophthalmology. 2016;123(2):295–301. doi:10.1016/j.ophtha.2015.08.023
32. Haripriya A, Chang DF, Ravindran RD. Endophthalmitis reduction with intracameral moxifloxacin prophylaxis: analysis of 600 000 surgeries. Ophthalmology. 2017;124(6):768–775. doi:10.1016/j.ophtha.2017.01.026
33. Friling E, Lundstrom M, Stenevi U, Montan P. Six-year incidence of endophthalmitis after cataract surgery: swedish national study. J Cataract Refract Surg. 2013;39(1):15–21. doi:10.1016/j.jcrs.2012.10.037
34. Rodriguez-Caravaca G, Garcia-Saenz MC, Villar-Del-Campo MC, Andres-Alba Y, Arias-Puente A. Incidence of endophthalmitis and impact of prophylaxis with cefuroxime on cataract surgery. J Cataract Refract Surg. 2013;39(9):1399–1403. doi:10.1016/j.jcrs.2013.03.031
35. Herrinton LJ, Shorstein NH, Paschal JF, et al. Comparative effectiveness of antibiotic prophylaxis in cataract surgery. Ophthalmology. 2016;123(2):287–294. doi:10.1016/j.ophtha.2015.08.039
36. Bowen RC, Zhou AX, Bondalapati S, et al. Comparative analysis of the safety and efficacy of intracameral cefuroxime, moxifloxacin and vancomycin at the end of cataract surgery: a meta-analysis. Br J Ophthalmol. 2018;102(9):1268–1276. doi:10.1136/bjophthalmol-2017-311051
37. Lockington D, Flowers H, Young D, Yorston D. Assessing the accuracy of intracameral antibiotic preparation for use in cataract surgery. J Cataract Refract Surg. 2010;36(2):286–289. doi:10.1016/j.jcrs.2009.08.034
38. Delyfer MN, Rougier MB, Leoni S, et al. Ocular toxicity after intracameral injection of very high doses of cefuroxime during cataract surgery. J Cataract Refract Surg. 2011;37(2):271–278. doi:10.1016/j.jcrs.2010.08.047
39. Olavi P. Ocular toxicity in cataract surgery because of inaccurate preparation and erroneous use of 50mg/mL intracameral cefuroxime. Acta Ophthalmol (Copenh). 2012;90(2):e153–4. doi:10.1111/j.1755-3768.2010.02103.x
40. Qureshi F, Clark D. Macular infarction after inadvertent intracameral cefuroxime. J Cataract Refract Surg. 2011;37(6):1168–1169. doi:10.1016/j.jcrs.2011.03.032
41. Sakarya Y, Sakarya R. Cefuroxime dilution error. Eur J Ophthalmol. 2010;20(2):460–461. doi:10.1177/112067211002000232
42. Gupta MS, McKee HD, Saldana M, Stewart OG. Macular thickness after cataract surgery with intracameral cefuroxime. J Cataract Refract Surg. 2005;31(6):1163–1166. doi:10.1016/j.jcrs.2004.10.074
43. Garg P, Roy A, Sharma S. Endophthalmitis after cataract surgery: epidemiology, risk factors, and evidence on protection. Curr Opin Ophthalmol. 2017;28(1):67–72. doi:10.1097/ICU.0000000000000326
44. Vazirani J, Basu S. Role of topical, subconjunctival, intracameral, and irrigative antibiotics in cataract surgery. Curr Opin Ophthalmol. 2013;24(1):60–65. doi:10.1097/ICU.0b013e32835a93be
45. Zhu Y, Chen X, Chen P, et al. The occurrence rate of acute-onset postoperative endophthalmitis after cataract surgery in Chinese small- and medium-scale departments of ophthalmology. Sci Rep. 2017;7(1):40776. doi:10.1038/srep40776
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.