Back to Journals » Clinical Ophthalmology » Volume 20
Intraocular Lens Power Calculation for Combined Cataract and Pterygium Surgeries
Authors Li Z ![]() , Tan B, Chen Y, Liu R, Wang H, Kuang J, Luo F, Zeng M
, Tan B, Chen Y, Liu R, Wang H, Kuang J, Luo F, Zeng M ![]()
Received 26 October 2025
Accepted for publication 5 February 2026
Published 17 February 2026 Volume 2026:20 575469
DOI https://doi.org/10.2147/OPTH.S575469
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Bharat Gurnani
Zebin Li,1,2,* Beiling Tan,1,2,* Yanting Chen,2 Rubing Liu,1,2 Han Wang,1,2 Jifa Kuang,2 Furong Luo,2 Mingbing Zeng1,2,*
1State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat-Sen University, Guangzhou, Guangdong, People’s Republic of China; 2Hainan Eye Hospital and Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat-sen University, Haikou, Hainan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Mingbing Zeng, State Key Laboratory of Ophthalmology, Zhongshan Ophthalmic Center, Sun Yat-sen University, Guangzhou, Guangdong, People’s Republic of China, Tel +86898-68628583, Fax +86898-68628587, Email [email protected]
Background: For patients with both cataract and pterygium, combined surgery reduces the burden and cost associated with two separate procedures. However, the accuracy of intraocular lens (IOL) power calculation is compromised in eyes with pterygium, as the lesion disturbs the corneal surface and tear film, leading to erroneous keratometry measurements. This often results in unpredictable postoperative refraction and a tendency toward myopic shift. Therefore, developing a reliable method to determine true corneal power for IOL calculation in such eyes is essential to improve refractive outcomes after combined surgery.
Purpose: This study aimed to develop and validate a topography-guided selective keratometry input method to improve the accuracy of intraocular lens power calculation in eyes undergoing combined cataract and pterygium surgery.
Methods: In this comparative study, patients were randomly allocated to two groups. In the control group (Uncorrected Corneal Power Group), the IOL power was calculated using the standard keratometry (K1, K2) values obtained directly from the IOLMaster’s integrated Barrett Universal II formula. In the study group (Corrected Corneal Power Group), a novel topography-guided method was employed: the flat keratometry (K1) was derived from the average of simulated keratometry (SimK) readings along the vertical meridian within the central 3mm zone on the Pentacam axial map, while the steep keratometry (K2) was taken from the contralateral (temporal) quadrant. These customized K-values were manually entered into the Barrett Universal II calculator. All patients underwent combined phacoemulsification and pterygium excision. Postoperative outcomes, including visual acuity, refraction, and the Mean Absolute Error (MAE) of the predicted versus actual spherical equivalent, were compared between groups.
Results: Postoperative corneal power increased significantly only in the ipsilateral quadrant on the pterygium side, while remained largely unchanged in the vertical and contralateral quadrants. The study group (corrected method) achieved significantly better uncorrected distance visual acuity (UDVA) and a mean spherical equivalent closer to target, compared to the control group. Most importantly, the Mean Absolute Error (MAE) was significantly lower in the study group (0.22 ± 0.18 D) than in the control group (1.18 ± 0.95 D) (P < 0.001), demonstrating superior predictive accuracy of the novel calculation method.
Conclusion: The novel topography-guided selective keratometry method, which utilizes the contralateral quadrant and vertical meridians for IOL calculation, significantly improves the predictive accuracy (as evidenced by a markedly lower Mean Absolute Error) and enhances the refractive and visual outcomes in patients undergoing simultaneous cataract extraction and pterygium excision.
Keywords: cataract, pterygium, corneal power, surgery, intraocular lens power calculation
Introduction
Pterygium is a common ocular surface lesion originating from the limbal conjunctiva within the palpebral fissure with progressive involvement of the cornea, with an increased incidence in latitudes nearer the equator and in individuals with a history of increased UV exposure.1,2 Approximately 90% of patients with pterygium present with grade 1 or 2 lesions, where the affected area does not extend into the central 3 mm optical zone.3,4 A cataract is a clouding of the lens in the eye, leading to a decrease in vision, which is most commonly due to aging.5 Pterygium induces corneal curvature changes, astigmatism, and keratometry errors. Therefore, for patients with both conditions, the optimal sequence has traditionally been to perform pterygium excision first, followed by cataract surgery. The combined operative procedure is recommended because neither pterygium excision nor cataract extraction can restore full visual recovery in such cases.6,7 A combined procedure is time-saving, cost-effective, and spares patients the burden of two separate surgeries. However, for combined surgeries, the postoperative refractive status is difficult to predict and a myopic shift often occurs. Although the mean absolute error in refractive prediction following cataract surgery in patients with pterygium is comparable to that of normal subjects, its distribution exhibits significantly greater dispersion. Moreover, the magnitude of prediction error shows a positive correlation with pterygium size.8 Kamiya et al investigated the predictability of IOL calculation after combined surgery and proposed a regression formula. However, such a formula lacks individualization and is difficult to apply accurately across different cases.9 Kim et al found that pterygium exceeding a length of 2.0 mm induced a significant corneal power change after surgery and recommended the mean K predicted from the regression analysis for pterygium surgery.10
The modern corneal topography instruments can measure and show corneal power point-to-point in situ, which enables ophthalmologists to analyze the surgery-induced refractive change by comparing the preoperative and postoperative corneal power point to point.11 Previous studies showed that the corneal power increased after pterygium excision and and suggested that pterygium leads to corneal flattening.12 However, we found that only the ipsilateral quadrant corneal power increased and the contralateral quadrant and the other vertical quadrants changed little after pterygium excision, indicating that the tear film between the corneal apex and pterygium head caused the corneal power measuring difference. Therefore, we hypothesized that selectively using corneal power from unaffected regions could improve IOL calculation accuracy in combined surgery. The postoperative refractive errors in simultaneous cataract and pterygium removal surgery can be reduced by neglecting the ipsilateral quadrant corneal power and using the contralateral quadrant and its other vertical quadrants corneal power to calculate IOL power.
Patients and Methods
A comparative study was conducted at the Hainan Eye Hospital, Zhongshan Ophthalmic Center, from January 2018 to August 2019. The study protocol for the research project conformed to the provisions of the Declaration of Helsinki. Approval was obtained from the Institutional Review Board (IRB)/ Ethics Committee. This study was registered in the Chinese Clinical Trial Registry. Ethical approval was obtained from the Ethics Review Committee of Hainan Eye Hospital (Reference Number: ChiCTR2200057893; Ethics number: 2016–001). All the patients provided written consent to being randomized and to participating in the study and anonymity was preserved. All the data were approved for acquisition and analysis.
Patients who were older than 55 years old with a diagnosis of age-related cataract and pterygium, for which phacoemulsification cataract extraction with IOL plantation and pterygium excision with conjunctival autograft were planned to be conducted, were recruited to participate. Other inclusion criteria were a dilated pupil of 7.0 mm or larger and a corneal endothelial cell count greater than 1200 cells/mm2. Patients were excluded if they had other eye or general disorders affecting vision, such as diabetic retinopathy, glaucoma, age-related macular degeneration, uveitis, or previous intraocular surgery. Patients with unilateral pterygium were included in this study. Patients were excluded if they had bilateral pterygia or if the pterygium reached the 3 mm central cornea.
After the patients were enrolled and provided informed consent, standard preoperative examinations were performed, which included lens nucleus density grading according to the Lens Opacities Classification System II (LOCS II). All patients were analyzed using an anterior eye segment analysis system (Pentacam; Münchholzhäuser, Germany). The pre- and postoperative corneal powers of the four quadrants in the central 3 mm were compared and statistically analyzed point-to-point separately.
IOL power calculations were performed using the Barrett Universal II Formula V1.05 based on the axial length measured by the IOL Master 500™ (Carl Zeiss Meditec, Jena, Germany). Patients were randomly allocated to one of two groups. The randomization was performed using a permuted block design and was conducted by an independent party not involved in the study. The IOL calculation strategy differed between the two groups as follows:
Control Group (Uncorrected Corneal Power Group, UCG): The IOL power was the direct output from the IOLMaster’s integrated Barrett Universal II calculation. The device automatically used its own measured K1 (flat keratometry) and K2 (steep keratometry) values.
Study Group (Corrected Corneal Power Group, CCG): A manual input strategy was employed using Pentacam HR (Oculus, Wetzlar, Germany) topography to derive customized keratometry values. Specifically, the Axial (Sagittal) Curvature Map was used. The flat keratometry (K1) was defined as the average of the SimK readings along the vertical meridian (approximately 70–110 degrees) within the central 3mm zone on this map. The steep keratometry (K2) was the SimK value from the topographic hemisphere contralateral (temporal) to the pterygium, as reported by the device. These two specifically selected K1 and K2 values were then manually entered into the online Barrett Universal II calculator (https://calc.apacrs.org/barrett_universal2105/) to derive the final IOL power.
All surgeries were performed by the same surgeon who had undergone phacoemulsification cataract extraction with IOL insertion and pterygium excision with a conjunctival autograft (see Video S1 for surgical details). Standard phacoemulsification cataract extraction and IOL insertion techniques were used with the Infiniti Vision System with Torsional continual mode (Alcon, CA, USA), as introduced by Yizhi Liu.13 The surgical technique consisted of capsulorhexis, nucleus and cortex extraction, and a monofocal IOL (ZCB00, AMO, IL, USA) implantation through a temporal 2.8 mm clear corneal incision. We selected emmetropia or the least myopia as the target refraction. After subconjunctival injection of lidocaine epinephrine (1:100,000) into the tissue, the pterygium head was bluntly lifted from the cornea, and the pterygium head and body were excised 3–4 mm from the limbus. Abnormal subconjunctival fibrous tissue was trimmed away, and abnormal scarring of the cornea was polished. A conjunctival autograft was taken from the superior bulbar conjunctiva in order to cover the defect area with 8–0 absorbable polyglycolic sutures without using mitomycin C. Postoperatively, tobramycin/dexamethasone ophthalmic suspension 0.3% / 0.05% (ToraDex, Alcon, TX, USA) and antibiotics (0.3% levofloxacin, Santen, Osaka, Japan) were topically administered 4 times daily for 2 weeks, with the dose being reduced gradually thereafter postoperative corneal power, corneal astigmatism, refractive errors, and spherical equivalent were obtained using autorefraction (RM-8000A, Topcon, Tokyo, Japan).
The postoperative outcomes were assessed by an examiner who did not participate in the surgery and was not aware of the treatment assignment. Patients were followed-up for 1 d, 7 days, 30 days, and 3 months postoperatively. The postoperative logMAR UDVA, logMAR CDVA, corneal power, corneal astigmatism, and SE were documented and statistically analyzed 1 and 3 months later.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics for Windows (version 18.0; IBM, USA). In addition to the comparisons of visual acuity and refractive outcomes, the predictive accuracy of the IOL calculation was assessed by calculating the Mean Absolute Error (MAE) and Median Absolute Error (MedAE) of the predicted versus the actual postoperative spherical equivalent refraction for each group. The standard deviation (SD) of the prediction error and the percentages of eyes within ±0.25 D, ±0.50 D, ±0.75 D, and ±1.00 D of the predicted refraction were also reported. Changes in corneal power after surgery were evaluated by Analysis of Variance. The differences in UCVA, CCVA, corneal power (CP), corneal astigmatism (CA), and SE between groups were evaluated using the independent sample t-test. Statistical significance was set at p < 0.05.
Results
A total of 56 eyes (56 patients) in the CCG group and 56 eyes (56 patients) in the UCG group were enrolled in the study. The mean patient age was 69.5±19.3 (SD) years, and no statistically significant differences between the groups were found by Independent Samples T-Test (P>0.05). The nuclear density grade comparison was not statistically significant by X2 (Chi-square) test (P>0.05).
One posterior capsule rupture occurred in the CCG and two in the UCG. Because the effused vitreous had to be cleared by anterior vitrectomy and could potentially affect the outcome, these two cases were excluded from the final analysis. The intraoperative differences in Ultrasound Time (UST) and mean cumulative dissipated energy (CDE) between the two groups were not statistically significant. No postoperative complications such as fibrin formation, synechias, macrophages on the IOL optic, or endophthalmitis were observed in any patient during the short-term observation. No postoperative complications associated with pterygium excision, such as recurrence, corneal scarring, corneal perforation, strabismus, non-healing epithelial defects, or scleral melt, were observed during the follow-up.
In the CCG group, 92.8% (52/56) of eyes achieved a refractive outcome within ±0.5 D. In stark contrast, none of the eyes in the UCG group (0/56) fell within this range. Additionally, 10.7% (6/56) of patients achieved outcomes ranging from ±0.5 D to ±1.0 D, and the majority, 89.3% (50/56), had refractive results between ±1.0 D and ±2.0 D.
One month or three months after surgery, the difference in corneal power in the upper, lower, and contralateral quadrants compared with those before surgery was not statistically significant through variance analysis (P>0.05). Slit-lamp photography (Figure 1A) and corresponding preoperative topography (Figure 1B) showed a lower corneal curvature of the pterygium surface and its ipsilateral tear lakes between the pterygium and corneal apex than the other three equivalents. However, after surgery, the pterygium ipsilateral corneal curvature showed little difference compared with the other three equivalents (Figure 1C and D). The average ipsilateral quadrant corneal power before pterygium excision was 40.14±4.51 (n=55), while it was 43.51±1.8 (n=55) and 43.79±1.7 (n=55) after 1 and 3 months of operations. The difference between the preoperative corneal power and 1 month (P<0.001) or 3 months (P<0.001) postoperative corneal power was statistically significant through variance analysis followed by the Least Significant Difference (LSD) test. The difference in ipsilateral quadrant corneal power between 1 and 3 months after surgery was statistically significant (P<0.001) (Table 1).
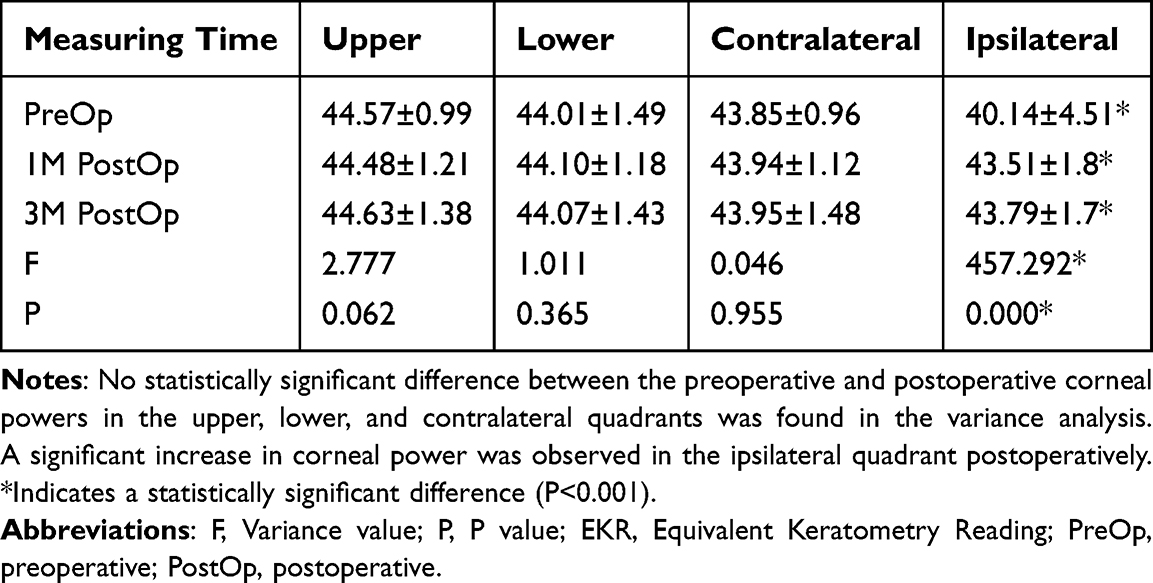 |
Table 1 The Preoperative and Postoperative EKR ( |

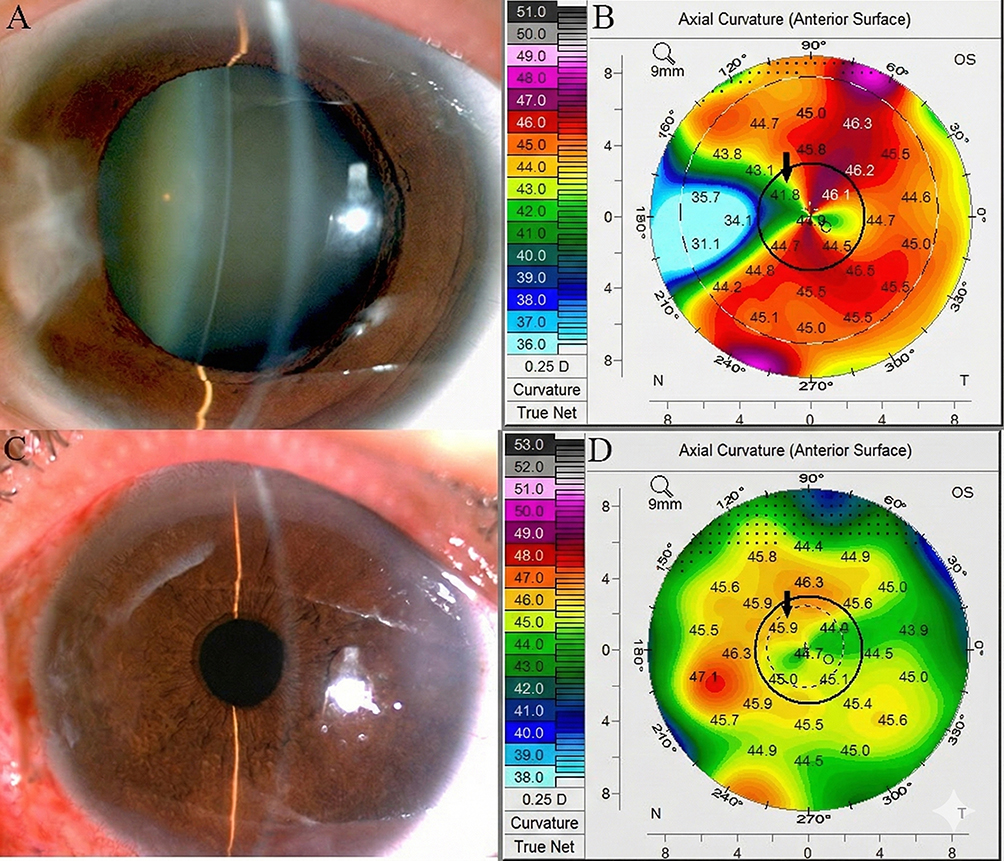 |
Figure 1 Representative photographs and corneal topography maps before and after pterygium excision. (A) Preoperative slit-lamp photograph showing the nasal pterygium. (B) Preoperative axial curvature map from Pentacam. The solid inner circle demarcates the central 3mm zone for keratometry analysis. The larger outer dashed circle indicates the 6mm analysis zone. The black arrow points to the inferonasal quadrant between the pterygium head and the corneal apex, where the corneal power was measured at 41.8 D, notably lower than other quadrants. (C) Postoperative slit-lamp photograph following pterygium removal. (D) Postoperative axial curvature map. The solid inner circle indicates the central 3mm zone. The smaller inner dashed circle approximates the pupillary area. The black arrow points to the same quadrant as in (B), showing an increase in corneal power to 45.9 D postoperatively, while curvatures in the contralateral, superior, and inferior quadrants remained relatively unchanged. |
At 1 or 3 months after surgery, the difference in UDVA between CCG and UCG was statistically significant (P<0.001) by Independent Samples T-Test, while the CDVA was not significant (P>0.05). All the patients in the UCG developed myopia, and the average SE was −1.49±1.25 and −1.43±1.05 (n=55) 1 month and 3 months after surgery, respectively, while the SE in the CCG developed close to the target diopter −0.10±0.50 and 0.02±0.55, respectively, 1 month and 3 months after surgery. The difference in the SE was statistically significant (P<0.001). The differences in CDVA, corneal power, and corneal astigmatism between the two groups were not significant (P>0.05) (Table 2).
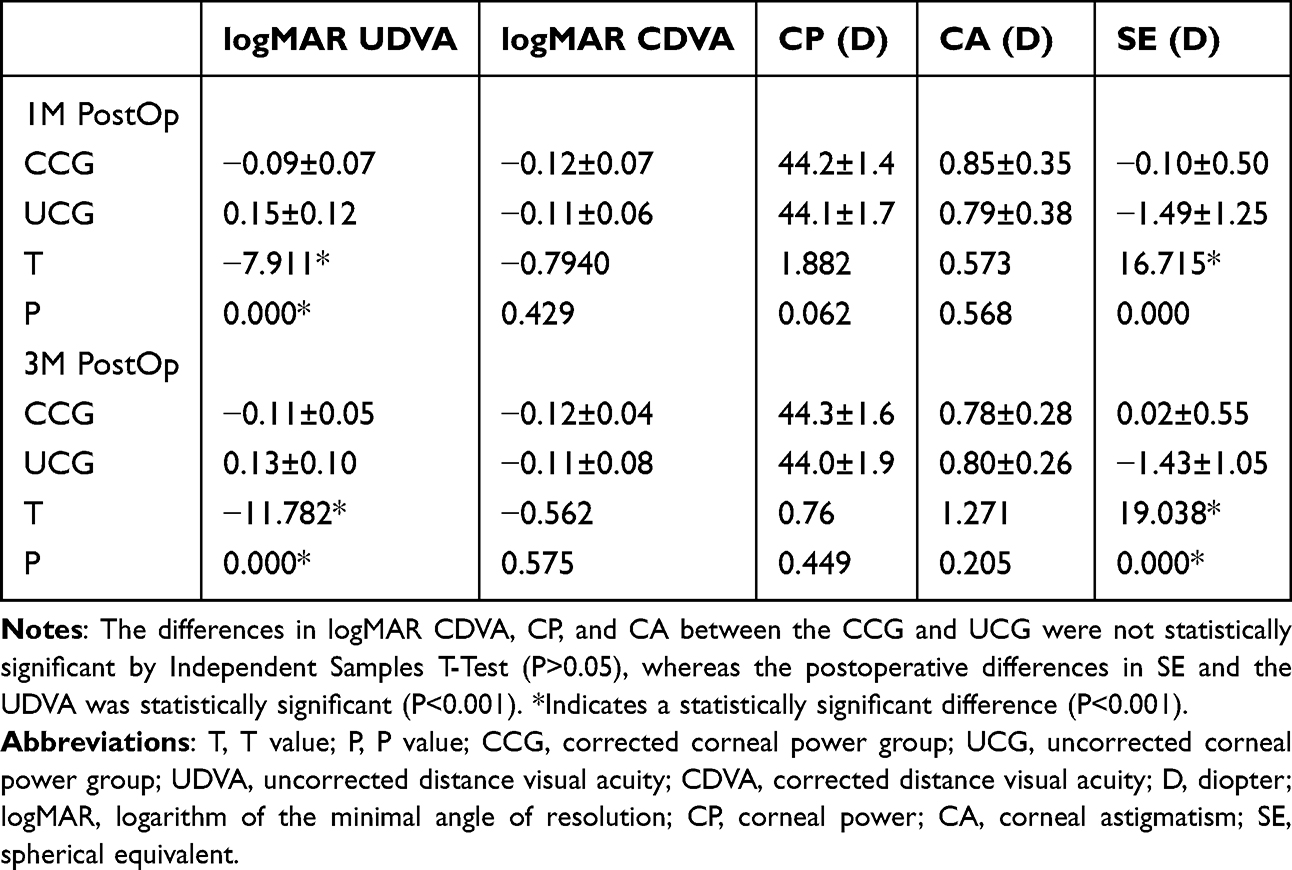 |
Table 2 The LogMAR UDVA, LogMAR CDVA, Corneal Power, Corneal Astigmatism and Spherical Equivalent ( |

The analysis of refractive prediction accuracy revealed a marked superiority of the novel method. The Mean Absolute Error (MAE) was significantly lower in the CCG group (0.22 ± 0.18 D) compared to the UCG group (1.18 ± 0.95 D) (P < 0.001). Similarly, the Median Absolute Error (MedAE) was 0.19 D in the CCG versus 0.98 D in the UCG. The standard deviation of the prediction error, indicating the variability of outcomes, was also substantially smaller in the CCG (0.18 D) than in the UCG (0.95 D). In terms of clinical relevance, 92.9% (52/56) of eyes in the CCG achieved a prediction error within ±0.50 D, and 100% were within ±1.00 D. In stark contrast, only 10.7% (6/56) of eyes in the UCG were within ±1.00 D, with the majority (89.3%, 50/56) exhibiting errors between ±1.00 D and ±2.00 D, and no eyes achieving an error within ±0.50 D. These results demonstrate the superior predictive accuracy of the corrected calculation method.
Discussion
An accurate intraocular lens power calculation is based on measurements of corneal power, ocular axial length, anterior chamber depth, and appropriate formulas. Improved instrumentation for measuring the eye’s axial length (AL), anterior depth, and the use of more precise mathematical formulas have significantly improved the accuracy of IOL power and reduced postoperative refractive errors.13 Though a new generation of keratometry can provide more accurate corneal power measurement, healthy corneal epithelial and smooth tear film are essential for accurate corneal power measurement.14 Any localized or diffuse disturbances on this surface will result in a decreasing accuracy of corneal power measurements. Small focal disturbances in the corneal periphery typically have little effect on vision. In contrast, any anomaly producing surface irregularities over the visual axis, although small, will have profound effects. The presence of a pterygium can significantly influence corneal refraction, including spherical power and astigmatism.15
Almost all keratometries provide the average corneal power of a corneal meridian, which cannot ensure accurate corneal power values if asymmetric corneal disturbances exist.16 To our knowledge, this is the first study to assess pterygium removal surgery-induced corneal power change by analyzing the contralateral and ipsilateral quadrants in the central cornea separately. Although the measurements of corneal curvature/power can be performed with a variety of instruments, most commonly a keratometer, IOL Master, or corneal topography device with different measuring principles, only the central cornea is usually measured for IOL calculations.17,18 We attempted to evaluate the influence of pterygium on corneal power by choosing a unilateral pterygium that is not large enough to reach a 3 mm central corneal optical area. By comparing preoperative and postoperative corneal power, we found that pterygium excision caused the ipsilateral quadrant corneal power to increase, but had little influence on the contralateral quadrant or vertical quadrants. The ipsilateral quadrant corneal power difference between 1 and 3 months postoperatively was not statistically significant. Because the pterygium did not reach the 3 mm central cornea, the cornea was not influenced by surgery-induced opacification, scarring, or traction. The tear film between the corneal apex and pterygium head leads to a disparity in corneal power measurement, which is consistent with the measurement principles of keratometry, reflecting the air-tear film surface instead of the tear film-corneal epithelial surface. Through point-to-point preoperative and postoperative corneal power comparisons, our study verifies Yasar’s opinion that the pooling of tears at the pterygium apex plays an important role, but fibrovascular traction has no effect on the corneal topographical changes induced by pterygium.19,20 In addition to the size of the pterygium, pterygium thickness and distance from the corneal apex have a close correlation with the corneal power change, which is related to the thickness of the tear film.
Corneal power and astigmatism can change with age, showing with-the-rule or against-the-rule astigmatism. Whether with-the-rule or against-the-rule regular astigmatism, the corneal power of a meridian appears symmetrical, and the side-to-side difference of the same meridian is smaller than the total difference of its vertical meridian. Because the contralateral quadrant corneal power of the pterygium changed little, we used it as the meridian power to calculate IOL power instead of the corneal power provided by keratometry. The absolute value of postoperative refractive errors in the corrected group (0.10±0.50 (n=55) was smaller than that in the uncorrected groups 1.49±1.25 (n=55).
A key finding of this study is that pterygium can induce artifactual corneal flattening within the central optical zone even when its head is outside the standard measurement area. We propose the following pathophysiological mechanism to explain this phenomenon and the resultant inaccuracy in standard biometry: (1) The elevated body of the pterygium creates a physical ridge, forming an abnormal tear film meniscus or pool between itself and the corneal apex. (2) This interposed fluid layer, through surface tension and mechanical coupling, transmits a flattening force anteriorly to the central corneal surface. (3) Keratometric devices (eg, IOLMaster), which measure the reflection from the air-tear-film interface, consequently record an artifactually flatter corneal curvature than the true stromal curvature. (4) Following pterygium excision, this abnormal fluid bridge is eliminated, allowing the cornea to assume its true, steeper anatomical curvature. (5) If uncorrected, the use of the preoperatively measured flat K-values leads to an over-powered IOL and a predictable postoperative myopic shift. Our novel calculation method, which selectively uses topography-derived K-values from less-affected regions (vertical meridian average and contralateral quadrant), is designed specifically to circumvent this tear-film-mediated artifact and approximate the eye’s latent corneal power.
Toric IOL has been widely used to reduce postoperative refractive astigmatism and spectacle dependence following cataract surgery.21 Due to the presence of pterygium, such patients often present with a considerable degree of astigmatism postoperative corneal astigmatism after pterygium excision and its axis were difficult to predict, and the monofocal lens was used for refractive correction after cataract extraction in this study. Toric IOL is not recommended for correcting preexisting astigmatism in patients with cataracts and pterygium until reliable methods to predict postoperative astigmatism and its axis are found.
Limitations
This study has several limitations. First, it included only patients with unilateral pterygium not involving the central 3 mm cornea, so the findings may not be generalizable to larger or bilateral pterygia. Second, the sample size, though sufficient to show statistical significance, was moderate. Future studies with larger cohorts and more diverse pterygium morphology are warranted to validate and refine this method.
Although neglecting the direct measurement of the ipsilateral quadrant corneal power of the pterygium is beneficial for reducing the average postoperative refractive errors, the limitation of the study is that it may not precisely reflect the meridian’s corneal power for individual patients. Our method is an easy and effective way to solve the problems of corneal power measurement in patients with preexisting pterygium and cataracts. If the pterygium is large enough to reach the central optical area or if nasal and temporal pterygium are simultaneously present, in which the contralateral corneal power is possibly influenced by the thickened tear film, it is best to calculate the IOL power by avoiding the horizontal corneal power. Only the corneal power of the vertical meridians can be used to calculate the IOL power. It is found from the keratometer or IOL master that a smaller corneal curvature is from the meridian of the pterygium. If it is calculated simply by the higher meridian, according to the SRK II IOL calculation formula, the contribution of a single meridian to the power of IOL is 1/2; therefore, the myopia drift caused by it is 1/2 of the power of astigmatism. Therefore, half of the astigmatism degree was subtracted from the calculated IOL power to achieve emmetropia.
This study has been strengthened by the incorporation of the Mean Absolute Error (MAE), the gold standard metric for evaluating IOL calculation accuracy. Our reported MAE of 0.22 D for the corrected method not only validates its precision but also allows for direct comparison with future studies. The strong correlation between the excellent MAE and the superior UDVA outcomes in the CCG group underscores that improved computational accuracy directly translates into better unaided visual function for patients.
Data Sharing Statement
The deidentified individual participant data that underlies the results reported in this article, as well as the study protocol and statistical analysis plan, will be made available upon reasonable request to the corresponding author, beginning 9 months and ending 36 months following article publication. Data sharing will be contingent on the proposal’s approval by an independent review committee and the completion of a data use agreement, in compliance with the ethical obligations of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the [National Natural Science Foundation of China] under Grant [No:82060176]; [Natural Science Foundation of Hainan Province] under Grant [822MS190]; and [Hainan Province Eye Clinical Medical Center].
Disclosure
We have no interests to declare.
References
1. Coroneo MT. Pterygium as an early indicator of ultraviolet insolation: a hypothesis. Br J Ophthalmol. 1993;77(11):734–8. doi:10.1136/bjo.77.11.734
2. Droutsas K, Sekundo W. Epidemiology of pterygium. A review. Ophthalmologe. 2010;107(6):511–512,514–516. doi:10.1007/s00347-009-2101-3
3. Gazzard G, Saw SM, Farook M, et al. Pterygium in Indonesia: prevalence, severity and risk factors. Br J Ophthalmol. 2002;86(12):1341–1346. doi:10.1136/bjo.86.12.1341
4. Durkin SR, Abhary S, Newland HS, Selva D, Aung T, Casson RJ. The prevalence, severity and risk factors for pterygium in central Myanmar: the Meiktila Eye Study. Br J Ophthalmol. 2008;92(1):25–29. doi:10.1136/bjo.2007.119842
5. Allen D, Vasavada A. Cataract and surgery for cataract. BMJ. 2006;333(7559):128–132. doi:10.1136/bmj.333.7559.128
6. Ibechukwu BI. Simultaneous pterygium and intraocular surgery. Br J Ophthalmol. 1990;74(5):265–266. doi:10.1136/bjo.74.5.265
7. Gulani A, Dastur YK. Simultaneous pterygium and cataract surgery. J Postgrad Med. 1995;41(1):8–11.
8. Jain P, Nema N. Incidence of refractive Surprise after phacoemulsification in patients of cataract with primary pterygium. Saudi J Ophthalmol. 2023;37(2):79–82. doi:10.4103/sjopt.sjopt_211_21
9. Kamiya K, Shimizu K, Iijima K, Shoji N, Kobashi H. Predictability of intraocular lens power calculation after simultaneous pterygium excision and cataract surgery. Medicine. 2015;94(52):e2232. doi:10.1097/MD.0000000000002232
10. Kim SW, Park S, Im CY, Seo KY, Kim EK. Prediction of mean corneal power change after pterygium excision. Cornea. 2014;33(2):148–153. doi:10.1097/ICO.0000000000000036
11. Mi H, Tan N, Ang M, Htoon HM, Mehta JS. Comparison of anterior and posterior topographic analysis between 3 imaging systems. J Cataract Refract Surg. 2015;41(11):2533–2545. doi:10.1016/j.jcrs.2015.05.039
12. Kheirkhah A, Safi H, Molaei S, Nazari R, Behrouz MJ, Raju VK. Effects of pterygium surgery on front and back corneal astigmatism. Can J Ophthalmol. 2012;47(5):423–428. doi:10.1016/j.jcjo.2012.07.002
13. Liu Y, Zeng M, Liu X, et al. Torsional mode versus conventional ultrasound mode phacoemulsification: randomized comparative clinical study. J Cataract Refract Surg. 2007;33(2):287–292. doi:10.1016/j.jcrs.2006.10.044
14. Lee AC, Qazi MA, Pepose JS. Biometry and intraocular lens power calculation. Curr Opin Ophthalmol. 2008;19(1):13–17. doi:10.1097/ICU.0b013e3282f1c5ad
15. Hong J, Sun X, Wei A, et al. Assessment of tear film stability in dry eye with a newly developed keratograph. Cornea. 2013;32(5):716–721. doi:10.1097/ICO.0b013e3182714425
16. Tomidokoro A, Miyata K, Sakaguchi Y, Samejima T, Tokunaga T, Oshika T. Effects of pterygium on corneal spherical power and astigmatism. Ophthalmology. 2000;107(8):1568–1571. doi:10.1016/S0161-6420(00)00219-0
17. Nichols JJ, Steger-May K, Edrington TB, Zadnik K. CLEK study group. The relation between disease asymmetry and severity in keratoconus. Br J Ophthalmol. 2004;88(6):788–791. doi:10.1136/bjo.2003.034520
18. Shirayama M, Wang L, Koch DD, Weikert MP. Comparison of accuracy of intraocular lens calculations using automated keratometry, a Placido-based corneal topographer, and a combined Placido-based and dual Scheimpflug corneal topographer. Cornea. 2010;29(10):1136–1138. doi:10.1097/ICO.0b013e3181d3d689
19. Chen YA, Hirnschall N, Findl O. Evaluation of 2 new optical biometry devices and comparison with the current gold standard biometer. J Cataract Refract Surg. 2011;37(3):513–517. doi:10.1016/j.jcrs.2010.10.041
20. Yasar T, Ozdemir M, Cinal A, Demirok A, Ilhan B, Durmus AC. Effects of fibrovascular traction and pooling of tears on corneal topographic changes induced by pterygium. Eye. 2003;17(4):492–496. doi:10.1038/sj.eye.6700377
21. Emesz M, Dexl AK, Krall EM, et al. Randomized controlled clinical trial to evaluate different intraocular lenses for the surgical compensation of low to moderate-to-high regular corneal astigmatism during cataract surgery. J Cataract Refract Surg. 2015;41(12):2683–2694. doi:10.1016/j.jcrs.2015.07.036
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Visual Improvement and Lowered Intraocular Pressure After Surgical Management of In-The-Bag Intraocular Lens Dislocation and Aphakia Correction; Retrospective Analysis of Scleral Suturing versus Retropupillary Fixated Iris-Claw Intraocular Lens During a 5-Year Period
Johansson Iranipour B, Rosander JH, Zetterberg M
Clinical Ophthalmology 2024, 18:315-324
Published Date: 2 February 2024
A New Methodology for Evaluating the Potential Impact of Residual Refractive Astigmatism in Pseudophakic Patients
Hida WT, Vilar C, Moscovici BK, Motta AFP, Carricondo PC
Clinical Ophthalmology 2024, 18:1909-1914
Published Date: 1 July 2024
The Effects of Distraction on Cataract Surgery Performance in Consultants and Trainees Using a Simulator
El Salloukh A, Khan M, Watts P, Newton PM, Williams GS
Clinical Ophthalmology 2024, 18:3297-3312
Published Date: 18 November 2024
Comparison of Ultrasound Energy Delivered to the Anterior Segment Across Different Phacoemulsification Surgical Platforms
Nelson TK, Ricks RG, Cardenas IA, Whitaker T, Jensen JL, Olson RJ, Pettey JH
Medical Devices: Evidence and Research 2025, 18:29-35
Published Date: 14 January 2025