Back to Journals » Clinical Ophthalmology » Volume 16
Intraocular Lens Position and Anterior Chamber Parameters Evaluation After Nd:YAG Laser Posterior Capsulotomy for Posterior Capsular Opacification Using Anterior Segment Swept-Source Optical Coherence Tomography
Authors João MD ![]() , Costa JV, Monteiro T, Franqueira N, Faria Correia F, Vaz F
, Costa JV, Monteiro T, Franqueira N, Faria Correia F, Vaz F
Received 16 November 2021
Accepted for publication 17 December 2021
Published 18 January 2022 Volume 2022:16 Pages 153—159
DOI https://doi.org/10.2147/OPTH.S349649
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Marina Delgado João, Jorge Vasco Costa, Tiago Monteiro, Nuno Franqueira, Fernando Faria Correia, Fernando Vaz
Ophthalmology Department, Hospital de Braga, Braga, Portugal
Correspondence: Marina Delgado João, Tel +351 253 027 000, Fax +351 253 027 999, Email [email protected]
Purpose: To evaluate the effect of neodymium-doped yttrium aluminum garnet (Nd:YAG) laser capsulotomy on intraocular lens (IOL) position and anterior segment parameters with a new swept-source anterior segment optical coherence tomography (AS-OCT) device (Anterion®, Heidelberg Engineering GmbH).
Patients and Methods: A total of 50 eyes from 50 consecutive patients were included. All patients had visually significant posterior capsular opacification (PCO) after uneventful phacoemulsification surgery with manual capsulorhexis and single-piece C-loop acrylic IOL implantation (AcrySof® SA60AT) and were treated with Nd:YAG laser. Anterior segment images were captured with Anterion® in non-dilated conditions before and one month after the procedure. In the “Metrics App”, we collected data of the anterior chamber angle (ACA) 3 and 9 o’clock, the anterior chamber depth (ACD), the anterior chamber volume (ACV), and the central corneal thickness (CCT). We also collected demographic and clinical data [age, gender, months from surgery to Nd: YAG capsulotomy, pre- and post-capsulotomy corrected distance visual acuity (CDVA) and spherical equivalent, and axial length].
Results: We did not find a statistically significant difference in ACD after the Nd:YAG capsulotomy (3.96 ± 0.55 vs 3.97 ± 0.55 mm, p = 0.10). In 28 patients, we noted a backward movement of the IOL; in the remaining 22, the IOL moved forward or did not change at all. We did not observe significant changes in ACA at the 3 and 9 o’clock reference points, ACV, or CCT. There was an improvement in CDVA after the procedure (0.37 ± 0.21 vs 0.12 ± 0.27 logMAR, p = 0.015), without statistically significant differences in SE (–0.15 ± 0.84 vs –0.25 ± 0,93, p = 0.42). Axial length was not correlated with ACD variations after the procedure (p = 0.67).
Conclusion: Our results show that Nd:YAG laser capsulotomy does not change the axial position of a single-piece C-loop acrylic IOL inside the capsular bag, as well as other anterior chamber parameters.
Keywords: neodymium-doped yttrium aluminum garnet laser, capsulotomy, posterior capsular opacification, intraocular lens, swept-source anterior segment optical coherence tomography
Introduction
Neodymium-doped yttrium aluminum garnet (Nd:YAG) laser capsulotomy is the gold-standard technique for treating posterior capsular opacification (PCO) in pseudophakic patients, which still represents the most common long-term postoperative complication after cataract surgery.1 Nonetheless, PCO overall incidence has decreased from 50% in the 1980s to up to 10–20% today.2,3 Despite having a success rate of more than 95%, Nd:YAG capsulotomy is also associated with multiple complications, such as intraocular pressure (IOP) spikes, corneal damage, uveitis, anterior hyaloid disruption, cystoid macular edema, intraocular lens (IOL) damage, movement, or dislocation, and refractive changes.4,5
Findl et al6 reported a posterior IOL displacement after the procedure, which caused a visually significant hyperopic shift, especially in those with larger capsulotomies. Previous studies have addressed the change in IOL position and anterior chamber parameters following Nd:YAG treatment, with mixed results.7–12 However, most of these studies present relevant limitations. Some studies included a mixed group of patients submitted to phacoemulsification surgery or extracapsular cataract extraction, while others included eyes that had been implanted with different IOLs.
In this study, we evaluated the effective lens position and anterior chamber parameters before and after Nd:YAG capsulotomy in patients with PCO after uneventful phacoemulsification cataract surgery and single-piece C-loop IOL implantation. All parameters were obtained with a novel high-resolution swept-source anterior segment optical coherence tomography (AS-OCT) device (Anterion®, Heidelberg Engineering GmbH, Heidelberg, Germany).
Materials and Methods
This prospective study conformed to the tenets of the Declaration of Helsinki. Full ethical approval from the Ethical Commission of Hospital de Braga was obtained. All patients signed an informed consent after a careful explanation of the procedure and before the interventions were performed. 50 eyes from 50 consecutive patients were included. All patients had visually significant PCO after uneventful phacoemulsification surgery with manual capsulorhexis and single-piece acrylic IOL implantation (AcrySof® SA60AT, Alcon, Texas, United States of America). We excluded patients with intraoperative (eg, posterior capsule rupture, zonolysis) or postoperative (eg, posterior synechia, bag-IOL subluxation) complications, previous ocular surgery (besides phacoemulsification surgery), history of corneal pathology, glaucoma, pseudoexfoliation syndrome, uveitis, posterior segment pathology, history of ocular trauma, and a dilated pupil diameter <5.0 mm.
All patients were treated with Nd:YAG (Ultra Q®, Ellex, Minneapolis, United States of America) capsulotomy. The laser was posterior offset by 200 µm to prevent IOL optic damage. A 4.0–4.5 mm diameter circle was cleared using a standard contact lens. We used energy levels starting from 0.8 to 2.4 mJ, which was necessary to disrupt the capsule. All patients received a standard medical procedure before (2 mg/mL brimonidine eye drops, 30 minutes before the Nd:YAG capsulotomy) and after (0.3 mg/mL Bromfenac eye drops, twice daily for 15 days) the procedure.
Anterior segment images were captured with a swept-source AS-OCT imaging device (Anterion®, Heidelberg Engineering GmbH, Heidelberg, Germany) in non-dilated conditions before and one month after the procedure. In addition to anterior segment imaging, this device also allows for axial length measurement, ocular biometry, and IOL calculation. This AS-OCT uses a 1300 nm wavelength light source and a scan speed of 50,000 A-scans per second, which offers an axial resolution of less than 10 µm, a transverse resolution inferior to 30 µm, a scan depth of 14 ± 0.5 mm, and a maximum scan width of 16.5 mm. This technology delivers detailed high-resolution images of the anterior segment along with accurate and reliable measurements of the anterior segment. In the “Metrics App”, the device printout details the anterior chamber angle (ACA), the scleral spur angle, the angle opening distance, the trabecular-iris space area, the lens thickness, the lens vault, the anterior chamber depth (ACD), the anterior chamber volume (ACV), the angle-to-angle distance, the spur-to-spur distance, the central corneal thickness (CCT), the white-to-white, the pupil diameter, and the kappa angle. Figure 1 demonstrates a pre-procedure printout with all the evaluated AS-OCT parameters. We also collected demographic and clinical data, namely age, gender, months from surgery to Nd:YAG capsulotomy, pre- and post-capsulotomy corrected distance visual acuity (CDVA) and spherical equivalent, and axial length. The primary study outcome was to compare the ACD before and after the procedure. The secondary outcomes were to access other AS-OCT parameters (ACA at 3 and 9 o’clock, ACV, and CCT) before and after the Nd:YAG capsulotomy. We also analyzed clinical data (CDVA and SE) and investigated if the axial length was correlated with changes in IOL positioning after the procedure. All AS-OCT measurements were obtained by the same experienced technician. We performed three consecutive measurements to eliminate potential acquisition errors. No complications were noted one month after the Nd:YAG capsulotomy.
 |
Figure 1 Pre-procedure Anterion® printout showing cornea, anterior chamber, lens, and pupil parameters. |
Statistical analysis was performed using IBM SPSS Statistics 27® (SPSS Inc, IBM). Data normality was calculated with Kolmogorov–Smirnov test; parametric and non-parametric tests were used accordingly. P-values <0.05 were considered to be statistically significant.
Results
50 eyes from 50 consecutive patients (32 females and 18 males) were included. The mean age was 71.41 ± 15.02 years (range 23–93). All patients were previously submitted to uneventful phacoemulsification surgery and single-piece C-loop AcrySof® SA60AT IOL implantation. The surgery was performed 33.42 ± 22.82 months before the Nd:YAG capsulotomy.
Table 1 summarizes the AS-OCT evaluated parameters results obtained before capsulotomy and one month after the procedure. We did not find a statistically significant difference between the IOL position before and after the Nd:YAG capsulotomy (3.96 ± 0.55 vs 3.97 ± 0.55 mm, p = 0.10). In 28 patients, we noted a backward movement of the IOL; in the remaining 22, the IOL moved forward or did not change at all. In addition, no significant change was observed in ACA at the 3 and 9 o’clock reference points, ACV, or CCT. Figure 2 demonstrates the parameter values’ distribution.
 |
Table 1 Anterior Segment Optical Coherence Tomography Parameters Comparison Before and One Month After Nd:YAG Laser Posterior Capsulotomy |
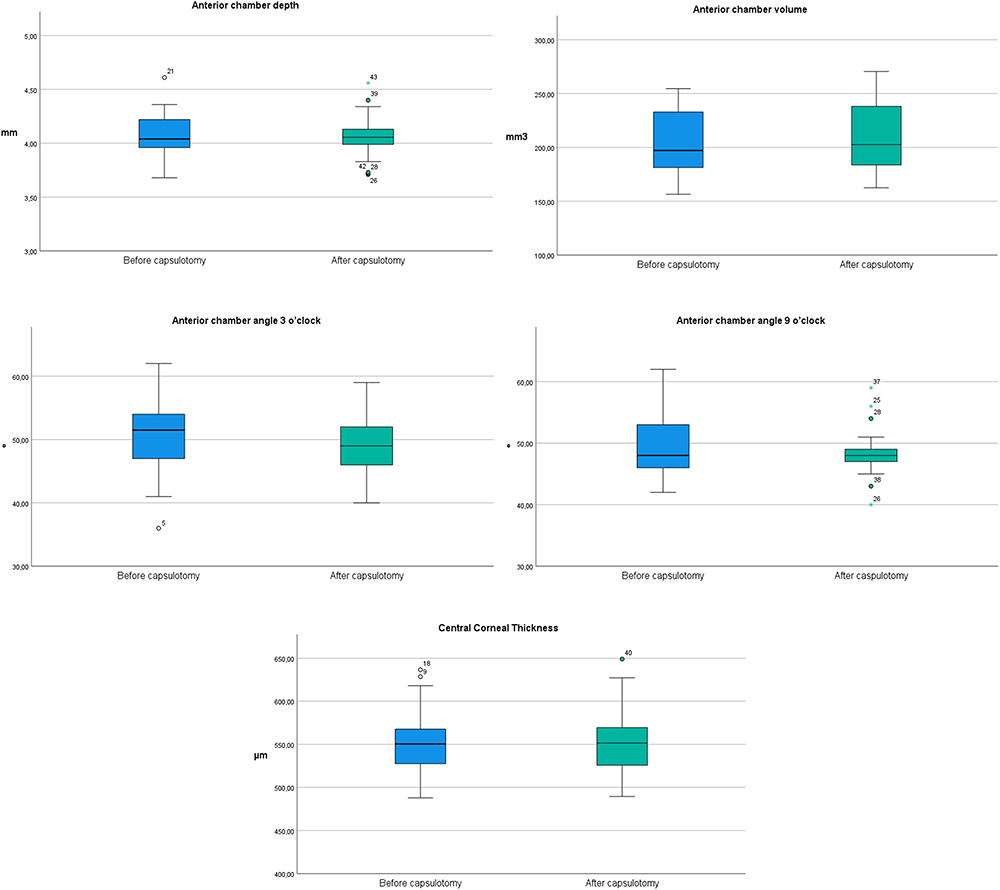 |
Figure 2 Box plots of anterior segment optical coherence tomography parameters before and after Nd:YAG posterior capsulotomy. |
Table 2 shows our visual and refractive results. There was an improvement in CDVA (0.37 ± 0.21 vs 0.12 ± 0.27 logMAR, p = 0.015), without statistically significant differences in SE (−0.15 ± 0.84 vs −0.25 ± 0.93, p = 0.42). Axial length was not correlated with ACD variations after the procedure (p = 0.67). Figure 3 evidences this result.
 |
Table 2 Visual and Refractive Results Before and One Month After Nd:YAG Laser Posterior Capsulotomy |
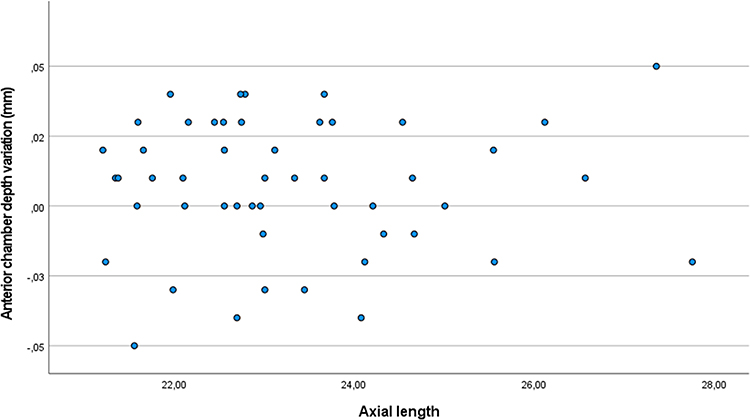 |
Figure 3 Scatter plot showing the anterior chamber depth variation after the Nd:YAG posterior capsulotomy according to axial length. |
Discussion
In our current practice, accurate and stable IOL positioning after cataract surgery is becoming more important than ever before. Every year, new multifocal and extended depths of focus IOLs are released, widening our variety of options and ability to offer the best solution to our increasingly demanding patients. However, these IOLs are extremely sensitive to movement and decentration,13 which results in increased higher-order aberrations, coma, photic phenomena, and visual quality degradation,14,15 especially in near activities.16 Even though IOL positioning seems to greatly influence multifocal IOL performance, monofocal IOLs decentration has also been studied and shown to decrease vision quality.17 Therefore, movement of the IOL after Nd:YAG capsulotomy in the treatment of PCO could potentially cause refractive changes and visual quality degradation.
We accessed IOL movement through a comparison of ACD (distance from the anterior surface of the IOL to the corneal endothelium) before and one month after the capsulotomy, using a novel swept-source AS-OCT. Using this device, we were able to correctly and accurately determine the ACD. In some cases, we observed interfering signals on the anterior IOL surface; therefore, each image was carefully observed and manually corrected, if necessary. By using this high-resolution technology, we were able to demonstrate that the axial position of this single-piece C-loop IOL did not change significantly after a 4–4.5 mm Nd:YAG capsulotomy when controlling for used energy (even though more energy was used in patients with thicker PCO). This result is also supported by the fact that there was no difference in SE after the procedure. This finding contradicts the results from a previous study of our group.7 This might be because that, in that study, our group did not measure the capsulotomy size. It has been reported that a backward movement of the IOL and, therefore, a hyperopic shift may be caused by a larger capsulotomy size.6,12
Findl et al6 reported a posterior axial shift in IOL positioning after Nd:YAG capsulotomy. Three different IOLs were included [single-piece poly(methyl methacrylate) IOL, a three-piece foldable IOL, and a plate-haptic IOL] and dual-beam partial coherence interferometry was used. However, in Findl’s study, the IOL position was evaluated immediately after the Nd:YAG capsulotomy was performed; also, all patients were evaluated after pupil dilation, which could potentially alter the IOL position. Khambhiphant et al11 reported no significant difference in ACD three months after the procedure with a slightly larger capsulotomy size of 5 mm in a cohort of 47 pseudophakic patients. Other studies also found similar conclusions.8,18 However, Oztas et al10 observed a decrease in ACD after Nd:YAG capsulotomy, as well as a temporary increase in ACA, despite an unaltered ACV. Only patients with an angulated hydrophobic acrylic three-piece intraocular lens (Sensar®, Advanced Medical Optics, California, United States of America) were evaluated. Vitreous pressure can explain the anterior displacement of this specific IOL. The ACA variations found in this study can be explained by the temporary obstruction of the trabecular meshwork following Nd:YAG capsulotomy; as stated by the authors, the ACA returned to the baseline values one month after the procedure. Parajuli et al19 reported an increase in ACD one hour after the procedure, which continued to increase at the one-month follow-up evaluation. However, the authors included patients who had undergone manual small incision cataract surgery and phacoemulsification and omit which IOLs were included in the study; also, they did not offer any explanation for the ACD increase. Our study included a homogeneous sample, which allows for simple and straightforward conclusions.
Our study presents some limitations. All measurements were obtained under non-dilated conditions. Pseudoaccomodation could be a confounding factor. In addition, we did not take into consideration PCO severity, which can alter IOL position. We only included pseudophakic patients with a single-piece C-loop acrylic IOL (AcrySof® SA60AT); our conclusions do not apply to other IOL designs and further studies are necessary to determine the effect of Nd:YAG capsulotomy on the position of these IOLs. We did not measure IOL tilt and decentration, which can induce astigmatism and higher-order aberrations. Studies evaluating the three-dimensional position of the IOL, supported by a wavefront aberrometer and a quality of vision questionnaire might provide further insight on the subject.
Conclusion
In conclusion, our data demonstrate that Nd:YAG laser posterior capsulotomy does not alter the axial position of a single-piece C-loop acrylic IOL inside the capsular bag, as well as other anterior chamber parameters. All parameters were obtained using a novel swept-source AS-OCT imaging device, which provides accurate and reliable measurements of the anterior segment.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Raj SM, Vasavada AR, Johar SRK, et al. Post-operative capsular opacification: a review. Int J Biomed Sci Master Publ Group. 2007;3:237–250.
2. Ursell PG, Dhariwal M, Majirska K, et al. Three-year incidence of Nd: yAGcapsulotomy and posterior capsule opacification and its relationship to monofocal acrylic IOL biomaterial: a UK Real World Evidence study. Eye (Lond). 2018;32(10):1579–1589. doi:10.1038/s41433-018-0131-2
3. Lindholm JM, Laine I, Tuuminen R. Five-year cumulative incidence and risk factors of Nd: yAGCapsulotomy in 10 044 hydrophobic acrylic 1-piece and 3-piece intraocular lenses. Am J Ophthalmol. 2019;200:218–223. doi:10.1016/j.ajo.2019.01.010
4. Billotte C, Berdeaux G. Adverse clinical consequences of neodymium: yAGlaser treatment of posterior capsule opacification. J Cataract Refract Surg. 2004;30(10):2064–2071. doi:10.1016/j.jcrs.2004.05.003
5. Karahan E, Er D, Kaynak S. An overview of Nd: yAG Laser capsulotomy. Med Hypothesis Discov Innov Ophthalmol. 2014;3(2):45–50.
6. Findl O, Drexler W, Menapace R, et al. Changes in intraocular lens position after neodymium: yAG capsulotomy. J Cataract Refract Surg. 1999;25(5):659–662. doi:10.1016/S0886-3350(99)00010-3
7. Monteiro T, Soares A, Leite RD, et al. Comparative study of induced changes in effective lens position and refraction after Nd: yAG laser capsulotomy according to intraocular lens design. Clin Ophthalmol. 2018;12:533–537. doi:10.2147/OPTH.S156703
8. Thornval P, Naeser K. Refraction and anterior chamber depth before and after neodymium-YAG laser treatment for posterior capsule opacification in pseudophakic eyes: a prospective study. J Cataract Refract Surg. 1995;21(4):457–460. doi:10.1016/S0886-3350(13)80540-8
9. Uzel MM, Ozates S, Koc M, et al. Decentration and tilt of intraocular lens after posterior capsulotomy. Semin Ophthalmol. 2018;33(6):766–771. doi:10.1080/08820538.2018.1443146
10. Oztas Z, Palamar M, Afrashi F, Yagci A. The effects of Nd: yAGlaser capsulotomy on anterior segment parameters in patients with posterior capsular opacification. Clin Exp Optom. 2015;98(2):168–171. doi:10.1111/cxo.12205
11. Khambhiphant B, Liumsirijarern C, Saehout P. The effect of Nd: yAGlaser treatment of posterior capsule opacification on anterior chamber depth and refraction in pseudophakic eyes. Clin Ophthalmol. 2015;9:557–561. doi:10.2147/OPTH.S80220
12. Yilmaz S, Ozdil MA, Bozkir N, Maden A. The effect of Nd: yAGlaser capsulotomy size on refraction and visual acuity. J Refract Surg. 2006;22(7):719–721. doi:10.3928/1081-597X-20060901-16
13. Alio JL, Plaza-Puche AB, Férnandez-Buenaga R, et al. Multifocal intraocular lenses: an overview. Surv Ophthalmol. 2017;62(5):611–634. doi:10.1016/j.survophthal.2017.03.005
14. Xu J, Zheng T, Lu Y. Effect of decentration on the optical quality of monofocal, extended depth of focus, and bifocal intraocular lenses. J Refract Surg. 2019;35(8):484–492. doi:10.3928/1081597X-20190708-02
15. He W, Qiu X, Zhang S, et al. Comparison of long-term decentration and tilt in two types of multifocal intraocular lenses with OPD-Scan III aberrometer. Eye (Lond). 2018;32(7):1237–1243. doi:10.1038/s41433-018-0068-5
16. Liu X, Xie L, Huang Y. Effects of decentration and tilt at different orientations on the optical performance of a rotationally asymmetric multifocal intraocular lens. J Cataract Refract Surg. 2019;45(4):507–514. doi:10.1016/j.jcrs.2018.10.045
17. Eppig T, Scholz K, Löffler A, et al. Effect of decentration and tilt on the image quality of aspheric intraocular lens designs in a model eye. J Cataract Refract Surg. 2009;35(6):1091–1100. doi:10.1016/j.jcrs.2009.01.034
18. Ozkurt YB, Sengor T, Evciman T, Haboglu M. Refraction, intraocular pressure and anterior chamber depth changes after Nd: yAGlaser treatment for posterior capsular opacification in pseudophakic eyes. Clin Exp Optom. 2009;92(5):412–415. doi:10.1111/j.1444-0938.2009.00401.x
19. Parajuli A, Joshi P, Subedi P, Pradhan C. Effect of Nd: yAG laser posterior capsulotomy on intraocular pressure, refraction, anterior chamber depth, and macular thickness. Clin Ophthalmol. 2019;13:945–952. doi:10.2147/OPTH.S203677
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.