Back to Journals » Drug Design, Development and Therapy » Volume 20
Intramuscular Generic Injection (QLG2072) versus Haloperidol in Chinese Patients with Acute Agitation: A Phase 3 Multicenter, Randomized, Double-Blind, Active-Controlled Trial
Authors Dong F, Wang Z, Li C, Li X, Zhu D ![]() , Li J
, Li J ![]() , Wang Z, Gong J, Zhou J, Liu H, Zhang Y, Zhang X, Chen X, Yu M, Tan X, Qian M, Luo Y, Guo WJ, Xie S, Huang J, Zhao J, Wan J, Shan Y, Li N, Wang J, Ju Y, Wang J, Bian Q, Wang G
, Wang Z, Gong J, Zhou J, Liu H, Zhang Y, Zhang X, Chen X, Yu M, Tan X, Qian M, Luo Y, Guo WJ, Xie S, Huang J, Zhao J, Wan J, Shan Y, Li N, Wang J, Ju Y, Wang J, Bian Q, Wang G
Received 19 September 2025
Accepted for publication 18 January 2026
Published 25 February 2026 Volume 2026:20 561494
DOI https://doi.org/10.2147/DDDT.S561494
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Prof. Dr. Tin Wui Wong
Fang Dong,1,2,* Zhonggang Wang,3,* Chao Li,4,* Xuan Li,5 Daomin Zhu,6 Jie Li,7 Zhoubing Wang,8 Jian Gong,9 Jianchu Zhou,10 Huanzhong Liu,11 Yunshu Zhang,12 Xuehua Zhang,13 Xiuzhe Chen,14 Mei Yu,15 Xi Tan,16 Mincai Qian,17 Yu Luo,18 Wan-Jun Guo,19 Shiping Xie,20 Jinsong Huang,21 Jingyuan Zhao,22 Jianguo Wan,23 Yihui Shan,24 Nannan Li,25 Jie Wang,25 Yunfei Ju,25 Juan Wang,25 Qingtao Bian,26 Gang Wang1,2
1Department of Psychiatry, Beijing Anding Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Advanced Innovation Center for Human Brain Protection, Capital Medical University, Beijing, People’s Republic of China; 3Department of Psychiatry, Shandong Daizhuang Hospital, Jining, People’s Republic of China; 4Department of Psychiatry, Xi’an Mental Health Center, Xi’an, People’s Republic of China; 5Department of Psychiatry, The Affiliated Brain Hospital of Guangzhou Medical University, Guangzhou, People’s Republic of China; 6Department of Psychiatry, Anhui Mental Health Center, Hefei, People’s Republic of China; 7Department of Psychiatry, Tianjin Anding Hospital, Tianjin, People’s Republic of China; 8Department of Psychiatry, Zhenjiang Mental Health Center, Zhenjiang, People’s Republic of China; 9Department of Psychiatry, The Affiliated Kangning Hospital of Ningbo University, Ningbo, People’s Republic of China; 10Department of Psychiatry, Chongqing Eleventh People’s Hospital, Chongqing, People’s Republic of China; 11Department of Psychiatry, Chaohu Hospital of Anhui Medical University, Chaohu, People’s Republic of China; 12Department of Psychiatry, Hebei Provincial Mental Health Center, Shijiazhuang, People’s Republic of China; 13Department of Adult Psychiatry, The Second People’s Hospital of Hunan Province (Hunan Brain Hospital), Changsha, People’s Republic of China; 14Department of Psychiatry, Shandong Mental Health Center, Jinan, People’s Republic of China; 15Medical Department, Urumqi Fourth People’s Hospital, Urumqi, People’s Republic of China; 16Department of Psychiatry, Chengdu Fourth People’s Hospital, Chengdu, People’s Republic of China; 17Department of Psychiatry, Huzhou Third People’s Hospital, Huzhou, People’s Republic of China; 18Department of Psychiatry, Wuxi Mental Health Center, Wuxi, People’s Republic of China; 19Department of Psychiatry, Hangzhou Seventh People’s Hospital, Hangzhou, People’s Republic of China; 20Department of Psychiatry, Nanjing Brain Hospital, Nanjing, People’s Republic of China; 21Department of Psychiatry, Dalian Seventh People’s Hospital, Dalian, People’s Republic of China; 22Department of Psychiatry, Henan Provincial Psychiatric Hospital, Xinxiang, People’s Republic of China; 23Department of Psychiatry, Jiangxi Mental Health Center, Nanchang, People’s Republic of China; 24Department of Psychiatry, The Third Hospital of Daqing, Daqing, People’s Republic of China; 25Clinical Research and Development Center, Qilu Pharmaceutical Co., Ltd, Jinan, People’s Republic of China; 26Department of Psychiatry, Beijing Huilongguan Hospital, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Gang Wang, Department of Psychiatry, Beijing Anding Hospital Capital Medical University, No. 5, Ankang Hutong, Deshengmenwai Street, Xicheng District, Beijing, 100088, People’s Republic of China, Tel +86-01058303236, Email [email protected] Qingtao Bian, Department of Psychiatry, Beijing Huilongguan Hospital, No. 7, Nandian Road, Huilongguan, Changping District, Beijing, 100096, People’s Republic of China, Tel +8613683384529, Email [email protected]
Introduction: This multicenter, randomized, double-blind, phase 3 trial aimed to assess the efficacy and safety of generic olanzapine injection (QLG2072) in managing acute agitation associated with schizophrenia/bipolar I disorder in Chinese patients.
Methods: Patients with acute agitation associated with schizophrenia/bipolar I disorder were randomly (1:1) assigned to receive 1– 3 intramuscular (IM) injections within a 24-hour treatment period, with either QLG2072 (10 mg per injection) or haloperidol (7.5 mg per injection). The primary endpoint was the change in Positive and Negative Syndrome Scale-Excited Component (PANSS-EC) score from baseline to 2 hours post-injection, assessed against a pre-specified non-inferiority margin of 2.0 for QLG2072 versus haloperidol.
Results: A total of 318 participants were randomized; 159 and 158 were included in the olanzapine and haloperidol FAS groups, respectively. At 2 h post-injection, the adjusted mean reductions in PANSS-EC scores were − 9.37 (95% confidence interval [CI]: − 10.02 to − 8.72) for QLG2072 versus − 9.40 (95% CI: − 10.04 to − 8.75) for IM haloperidol with a between-group difference of 0.03 (95% CI: − 0.88 to 0.93), establishing non-inferiority of QLG2072 to IM haloperidol, as the upper limit of the 95% CI fell below the predefined margin. Consistent with the primary endpoint, comparable efficacy was observed across multiple secondary efficacy measures, including response rate and the Clinical Global Impression-Improvement scores. The overall incidence of treatment-emergent adverse events was comparable between the treatment groups. However, QLG2072 was associated with a numerically lower incidence of extrapyramidal symptoms compared to haloperidol (10.1% vs 27.2%).
Discussion: QLG2072 demonstrated non-inferiority to haloperidol in acute agitation management, with comparable efficacy and favorable neurological tolerability. These findings support its clinical application in Chinese psychiatric populations.
Trial Registration: ClinicalTrials.gov: NCT05803642.
Keywords: acute agitation, intramuscular, haloperidol, olanzapine, schizophrenia, bipolar I disorder
Introduction
Agitation is a clinically heterogeneous syndrome with multifactorial origins, characterized by excessive motor activity, emotional dysregulation, and conceptual disorganization across psychiatric, neurological, and general medical conditions.1,2 In patients with schizophrenia or bipolar I disorder, acute agitation often escalates to aggressive behaviors, posing significant risks to patient safety and clinical management. Urgent pharmacological intervention is required to achieve rapid tranquillization, reduce aggressive behaviors, and facilitate the treatment of the underlying psychiatric condition.3,4 Current clinical guidelines emphasize a multimodal management strategy, prioritizing pharmacotherapy when non-pharmacological approaches fail.2,5 Available agents include typical antipsychotics (eg, haloperidol), atypical antipsychotics (eg, olanzapine, ziprasidone), and benzodiazepines. However, their clinical utility is limited by differential safety profiles and region-specific regulatory approvals. While typical antipsychotics like haloperidol have historically prodominated the management of acute agitation,6,7 their use is often constrained by dose-dependent extrapyramidal symptoms (EPS, including dystonia, akathisia and Parkinson-like effects) and cardiovascular risks, which arise from histaminic, cholinergic and α-adrenergic antagonistic effects.8,9
In contrast, atypical antipsychotics offer favorable safety profile. Olanzapine, a prototypical atypical antipsychotic, achieves antipsychotic effects with rapid symptom control while minimizing the risk of EPS.10,11 Intramuscular (IM) olanzapine (5–10 mg) was comparable to IM haloperidol 7.5 mg in managing agitation associated with schizophrenia in clinic.7,12–15 Moreover, olanzapine’s favorable tolerability, attributed to transient binding to dopamine D2 receptor, has established it as a clinical standard for managing psychiatric agitation, as endorsed by clinical guidelines.5,16 The parenteral formulation also ensures a seamless transition to oral maintenance therapy, further enhancing its therapeutic value.17,18 Despite these pharmacological and clinical advantages, olanzapine’s adoption for acute agitation management remains uneven globally. This is largely due to regulatory hurdles and gaps in population-specific evidence.
Currently, the Chinese Expert Consensus on Psychiatric Management of Agitated Patients recommends IM haloperidol and IM ziprasidone for rapid control of acute agitation.5 However, evidence shows that IM olanzapine, which is approved for this indication globally but not yet in China, may offer important advantages associated with more rapid symptom control and a lower risk of extrapyramidal symptoms (EPS), as well as a lower risk of QTc prolongation than IM ziprasidone.19 These potential benefits highlight the need to evaluate its applicability in the Chinese clinical setting. Meanwhile, a significant unmet clinical need exists in China for rapid-acting treatments for acute agitation, a condition that often leads to emergency interventions and hospitalization. Prioritizing the development and approval of generic IM olanzapine formulations could not only serve as a cost-effective strategy to bridge this therapeutic gap, but also reduce the economic burden on China’s national healthcare system.20
To address the critical therapeutic gap in China’s management of acute agitation associated with schizophrenia or bipolar I disorder, QLG2072, a generic IM olanzapine formulation has been developed by Qilu Pharmaceutical Co., Ltd. QLG2072 has demonstrated its pharmaceutical equivalence to the reference olanzapine (Zyprexa®). Consequently, the China’s Center for Drug Evaluation (CDE) gave tacit consent to a bioequivalence study exemption for healthy volunteer population, in alignment with the Food and Drug Administration (FDA) and European Medicines Agency (EMA) regulatory guidelines for generic injectables. We conducted this study to further evaluates the therapeutic non-inferiority and safety profile of QLG2072 compared to the IM Haloperidol in Chinese patients with acute agitation associated with schizophrenia or bipolar I disorder, in accordance with the CDE’s Clinical Technical Requirements for Drugs Approved for Marketing Abroad but Not Yet in China.13
Materials and Methods
Participants and Study Design
This multicenter, double-blind, randomized, active-controlled, phase 3 non-inferiority trial (ClinicalTrials.gov NCT05803642) was conducted at 26 clinical centers in China from April 22 to December 11, 2023 (Table S1).
The study enrolled adult participants aged 18–65 years with a diagnosis of schizophrenia or bipolar I disorder, as defined by the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria. After a 3-day screening period, eligible participants experiencing acute agitation secondary to schizophrenia or bipolar I disorder were randomly allocated in a 1:1 ratio to receive IM olanzapine (10 mg) or haloperidol (7.5 mg), with randomization stratified by primary psychiatric diagnosis (schizophrenia vs bipolar I disorder). The treatment protocol allowed for up to three IM administrations (olanzapine 10mg/dose; haloperidol 7.5mg/dose) within a 24-hour period, with mandatory intervals of at least 4 hours between doses. Subsequent injections were administered at the investigator’s discretion following a clinical reassessment of agitation severity. Any post-randomization rescue medication (including benzodiazepines) was strictly prohibited throughout the 24-hour treatment and efficacy evaluation period.
Acute agitation severity was assessed using the Positive and Negative Syndrome Scale-Excited Component (PANSS-EC), with inclusion requiring a total score of ≥14 and at least one subscale score of ≥4. Participants were excluded if they were pregnancy or breast feeding, or had clinically significant comorbid medical conditions that could either increase susceptibility to adverse drug reactions or confound efficacy assessments. Full inclusion and exclusion criteria are detailed in Box S1.
This study was conducted in accordance with the principles of the Declaration of Helsinki and the International Council for Harmonization Good Clinical Practice (ICH-GCP). Prior to study initiation, following the approval from Ethics Committee of Beijing Anding Hospital Affiliated to Capital Medical University (No. 2022–210-202321FS-2), institutional review boards of all other participating centers granted ethical approval for trial documentation. Written informed consent was obtained for all participants or their legally authorized representatives before any procedures began. For patients with capacity, consent was provided by both the patient and their guardian (co-signed). Due to the acute nature of agitation, for patients lacking capacity at enrollment, surrogate consent was provided solely by the legally authorized representatives.
Randomization and Masking
The randomization sequence was created through a validated block randomization method using SAS software (version 9.4 or later; SAS Institute Inc., Cary, NC, USA) and was then integrated into the Randomization and Trial Supply Management (RTSM) system. A designated unblinded statistician developed the allocation sequence and medication dispensing protocol, ensuring complete separation from clinical operations. The RTSM system automatically assigned algorithm, which was triggered only after participants met all predefined stratification criteria. Blinded investigation products (IM olanzapine 10 mg/dose or haloperidol 7.5 mg/dose) were administered within a 24-hour period. Real-time enrollment tracking and drug accountability maintained through the RTSM infrastructure.
This study employed a double-blind design, which necessitated the separation of trial personnel into blinded and unblinded operational groups to maintain methodological integrity. Throughout the trial, sponsor personnel (excluding unblinded monitors and project managers), clinical investigators, outcome assessors, and execution staff were kept strictly blinded to treatment allocations, therapeutic details, and evaluation processes. In contrast, unblinded medication administrators and nursing teams were responsible for delivering the interventions.
Assessments and Endpoints
This study design, including the primary endpoint, was aligned with the pivotal trial of the reference branded IM olanzapine.7 The primary endpoint was defined as the change of Positive and Negative Syndrome Scale-Excited Component (PANSS-EC) score measured at 2 hours post-initial IM administration. The PANSS-EC evaluates agitation severity across five domains: poor impulse control, tension, hostility, uncooperativeness, and excitement. Each item was scored on a 7-point scale (1=absent; 7=extreme), yielding a total score ranging from 5 (absence of agitation) to 35 (extremely severe). The key secondary endpoint was the response rate, which was defined as the proportion of participants achieving a reduction of ≥40% at 2 hours after baseline for PANSS-EC scores. The testing of these confirmatory objectives followed a fixed-sequence procedure. Additional secondary endpoints included longitudinal PANSS-EC assessments at 30, 60, and 90 minutes post-dose; the Clinical Global Impression-Improvement (CGI-I) scores evaluated at 2 and 24 hours; the changes in both PANSS-EC and Clinical Global Impression-Severity (CGI-S) scores over the 24-hour post-treatment period; and the distribution of participants requiring one, two, or three IM injections during the 24-hour treatment period. The CGI-I was rated on a 7-point scale (1=very much improved; 7=very much worse, with 0=not assessed). Similarly, the CGI-S assessed agitation severity using a 7-point scale rating from 1 (normal) to 7 (among the most extremely ill subjects), with 0 indicating not assessed.
Safety was monitored throughout the study from the signing of the informed consent form until the final assessment on Day 7 or Day 8. Safety assessments involved surveillance of AEs and serious adverse events (SAEs), focusing on their frequency, severity, and potential relationship to the investigation drugs. Comprehensive safety monitoring included serial measurements of vital signs, standardized laboratory test, and 12-lead electrocardiograms. EPS were assessed using the Simpson-Angus Scale and Barnes-Akathisia Rating Scale. All treatment-emergent adverse events (TEAEs) were coded according to the Medical Dictionary for Regulatory Activities (MedDRA) (version 26.1).
Statistical Analyses
Based on efficacy data in prior studies7,14 and investigator estimations, it was hypothesized that there would be no difference in the change of PANSS-EC score from baseline between the treatment groups at 2 hours post-initial IM administration. This study employs a non-inferiority design based on a meta-analysis of historical haloperidol versus placebo efficacy data.7,14 Following the Guidelines for Non-Inferiority Clinical Trials (M1=2.8716, margin=0.5×M1=1.44)14 and referencing margins from olanzapine (3.0)21 and aripiprazole (2.5) trials,6 a non-inferiority margin of 2.0 was established through clinical consensus. A total of 318 patients (159 per group) were required to achieve a statistical power of 80% with a one-sided significance level (α) of 0.025, assuming no treatment difference between the investigational and control drugs, a non-inferiority margin of 2.0, and a standard deviation of 6,7 while accounting for a dropout rate of 10%. These calculations were implemented in PASS 2019 software (Version 19.0.10). This sample size also provided 90% power to assess the key secondary endpoint between groups.
All randomized participants who received ≥1 IM injection of study drug were included in the full analysis set (FAS) under the intent-to-treat (ITT) principle, for demographic, clinical, and efficacy evaluations. Participants in the FAS who adhered strictly to the protocol were included in the per-protocol analysis set (PPS). The safety analysis set (SS) included participants who received ≥1 IM dose of the investigational drug within the FAS. For the primary endpoint, between-group differences in changes at 2 hours post-injection for PANSS-EC scores were analyzed using analysis of covariance (ANCOVA). The key secondary endpoint, response rate, was summarized descriptively with two-sided 95% confidence interval (CI) by treatment group. Between-group rate differences were assessed using the Cochran-Mantel-Haenszel (CMH) test, adjusted for stratification factors (schizophrenia vs bipolar I disorder), with corresponding 95% CI reported. Secondary endpoints for continuous variables, such as changes in PANSS-EC scores at multiple timepoints, were analyzed via ANCOVA, reporting least-squares mean (LSM) differences and 95% CI. Categorical outcomes, including the distribution of injection frequencies, were compared via CMH tests stratified by the underlying etiology of agitation, reported as frequencies and percentages. The primary and key secondary efficacy analyses were conducted based on the Missing at Random (MAR) assumption. All statistical analyses were performed using SAS software (version 9.4; SAS Institute Inc., Cary, NC, USA).
Results
Patient Disposition and Baseline Characteristics
Between April 22, 2023, and December 05 2023, a total of 356 potential participants were screened for the study. Among them, 318 participants were randomly assigned in a 1:1 ratio to receive either IM olanzapine (N=159) or IM haloperidol (N=159). A total of 317 participants (159 in the olanzapine group and 158 in the haloperidol group) received at least one dose of the study medication (Figure 1). The median age of the participants was 33.0 years (range: 18–64), with 52.1% (165/317) being male. Most (94.0%, 298/317) of the participants were of Han Chinese ethnicity. Demographic and clinical characteristics were comparable between the two groups (Table 1). Diagnostic stratification showed nearly equivalent distributions: schizophrenia was diagnosed in 51.6% (82/159) of the olanzapine group and 51.9% (82/158) of the haloperidol group, while bipolar I disorder in 48.4% (77/159) and 48.1% (76/158). At baseline, the mean PANSS-EC score was 19.2 ± 3.3, and the CGI-S score was 4.9 ± 0.8, indicating baseline moderate-to-severe agitation levels.
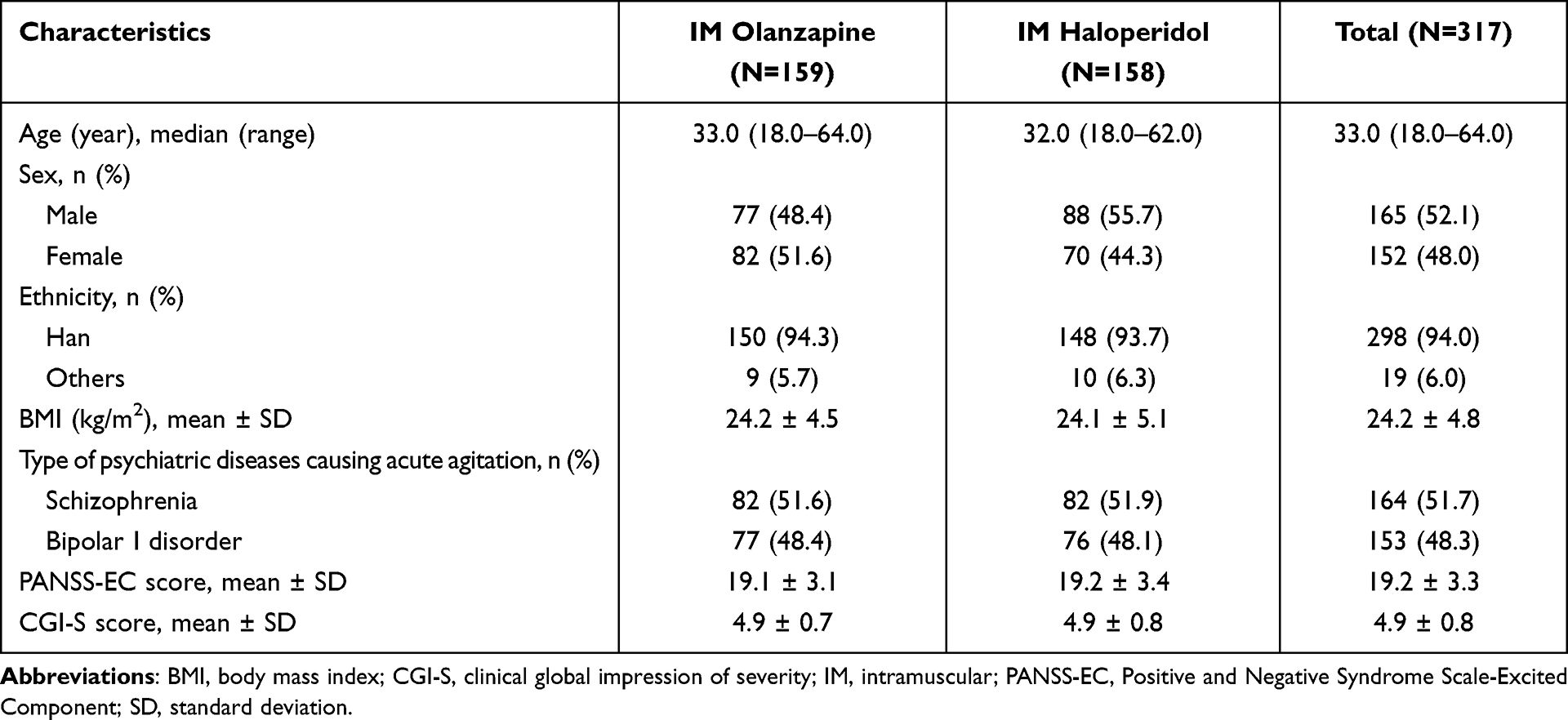 |
Table 1 Baseline Demographic (Full Analysis Set) |
 |
Figure 1 Patient disposition. Abbreviations: FAS, full analysis set; PPS, per-protocol analysis set; SS, safety analysis set. |
Efficacy
For the primary endpoint, both treatment groups demonstrated substantial reductions at the 2-hour post-injection timepoint for PANSS-EC scores in the FAS population. Specifically, the adjusted mean change was −9.37 (95% CI: −10.02 to −8.72) for IM olanzapine compared with −9.40 (95% CI: −10.04 to −8.75) for IM haloperidol. This resulted in a between-group difference (IM olanzapine minus IM haloperidol) of 0.03 (95% CI: −0.88 to 0.93). Notably, the upper 95% CI confidence limit of 0.93 was well below the predefined non-inferiority margin of 2.0, thereby statistically supporting the non-inferiority of IM olanzapine (Figure 2). These outcomes were consistent across sensitivity analyses conducted in the PPS population and FAS population excluding 35 subjects who were asleep at 2 h post the first IM injection (Table S2).
 |
Figure 2 Mean changes in the Positive and Negative Syndrome Scale-Excited Component (PANSS-EC) scores from baseline to each time point within 2 hours after the first intramuscular (IM) injection. * Indicates the differences of adjusted change between groups (IM olanzapine vs IM haloperidol), mean (95% CI) from 30 min to 120 min. Squares in boxes indicate the adjusted mean; the top box lines, upper quartile; the bottom box line, lower quartile; bars in boxes, median; whiskers, data falling within 1.5 times the interquartile range; dots, values outside the range indicated by the whiskers. The adjusted mean are the least squares estimated values after the pooled analysis of the covariance analysis model using the Rubin method. The covariance analysis model takes the change value of the PANSS-EC score at 2 h from baseline as the dependent variable, the treatment groups and stratification factors (schizophrenia vs bipolar I disorder) as fixed effects, and the baseline PANSS-EC score as the covariate. Missing PANSS-EC scores were imputed using the Markov Chain Monte Carlo (MCMC) multiple imputation method, under the assumption that missing data adhered to the missing-at-random mechanism. Abbreviations: CI, confidence interval; PANSS-EC, Positive and Negative Syndrome Scale-Excited Component. |
Analysis of the key secondary endpoint revealed comparable response rates, with a proportion of 64.3% (95% CI: 56.5 to 72.1) and 62.5% (95% CI: 54.6 to 70.4) of patients achieving ≥40% PANSS-EC reduction at 2 hours in the IM olanzapine and IM haloperidol groups, respectively (Table 2). The statistical analysis supported the comparability of IM olanzapine to IM haloperidol (Z = 3.190, with a critical Z >1.96), and the results in the PPS population mirrored the results in the FAS population, reinforcing the robustness of this secondary efficacy endpoint.
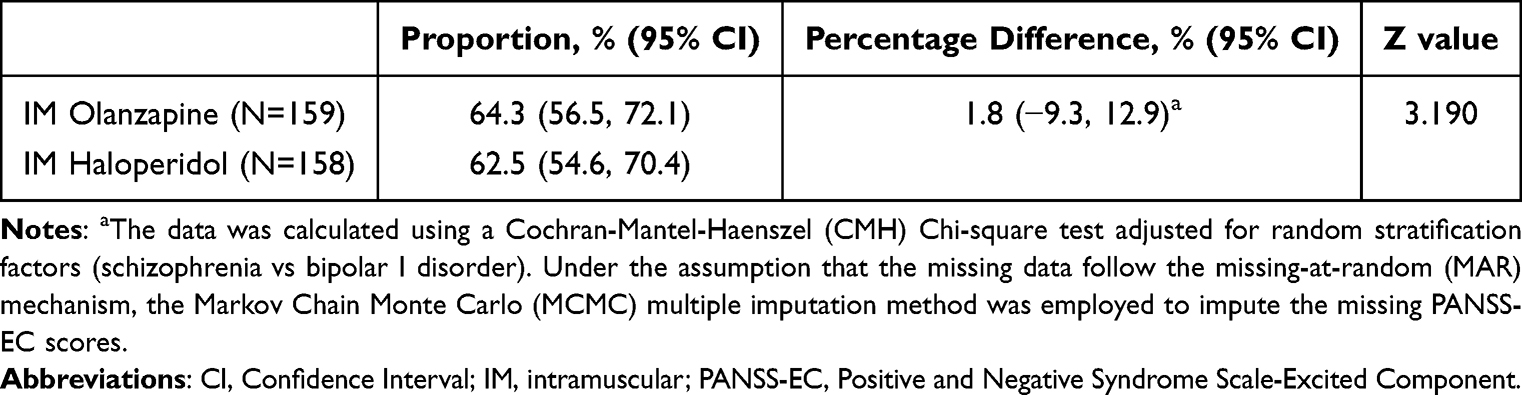 |
Table 2 Proportion of Patients with a Reduction of ≥ 40% in the PANSS-EC at 2 hours Post the First Injection (Full Analysis Set) |
Following the initial injection, no significant differences (IM olanzapine vs IM haloperidol) were observed in PANSS-EC reductions at interim timepoints of 30, 60, 90 minutes or during the 24-hour follow-up period (Figure 2). Similarly, CGI-I scores showed parallel improvement pattern between groups at both 2-hour and 24-hour assessments, without statistical significance (Table S3). CGI-S at 24 hours also exhibited comparable patterns between groups (Table S3). Most participants required only single-dose administration. In the olanzapine group, 91.2% (145/159) of patients received a single dose, similar to the proportion of 94.9% (150/158) in the haloperidol group. Repeat injection rates showed non-significant variation, with 8.8% (14/159) receiving a second dose in the olanzapine group and 5.1% (8/158) in the haloperidol group. Notably, no participants in either group required a third injection. Overall, there were no significant differences (IM olanzapine vs IM haloperidol) in dosing profiles between the two groups throughout the 24-hour period (Table S4).
Subgroup Analyses
According to subgroup analyses for the primary endpoint, IM olanzapine exhibited favorable effect in reduction of PANSS-EC scores when compared to IM haloperidol in patients with bipolar I disorder (mean change [IM olanzapine vs IM haloperidol]: −9.88 vs −9.43; difference [IM olanzapine minus IM haloperidol]: −0.46, 95% CI [-1.76, 0.85]), male participants (mean change: −9.30 vs −8.83; difference: −0.47, 95% CI: −1.59 to 0.65), and individuals with baseline PANSS-EC scores of <20 (mean change: −8.08 vs −7.35; difference: −0.73, 95% CI: −1.81 to 0.35) (Figure 3). Subgroup analyses for the key secondary endpoint showed that, IM olanzapine was associated with a numerically higher proportion of patients achieving a ≥40% PANSS-EC score reduction at 2 hours in patients with bipolar I disorder (mean [IM olanzapine vs IM haloperidol]: 67.7% vs 56.9%; difference [IM olanzapine minus IM haloperidol]: 10.8%, 95% CI: −5.2% to 26.9%), male participants (mean: 64.9% vs 54.9%; difference: −10.0%, 95% CI: −5.9% to 26.0%), and individuals with baseline PANSS-EC scores of <20 (mean: 63.6% vs 51.3%; difference: 12.6%, 95% CI: −1.7% to 26.9%) (Figure S1).
 |
Figure 3 Forest plots of the change of PANSS-EC at 2 hours post the first intramuscular injection from baseline in the full analysis set. * The adjusted mean are the least squares estimated values after the pooled analysis of the covariance analysis model using the Rubin method. Abbreviations: CI, confidence interval; PANSS-EC, Positive and Negative Syndrome Scale-Excited Component. |
Safety
The study demonstrated high treatment adherence in both groups, although one patient in the haloperidol group did not receive treatment. The safety population included 317 participants, with 159 in the IM olanzapine group and 158 in the IM haloperidol group. A total of 437 TEAEs were documented across both groups. The incidence of TEAE was 62.9% (100/159) in the olanzapine group and 67.7% (107/158) in the haloperidol group. TRAEs occurred in 40.9% (65/159) of participants receiving olanzapine and 44.3% (70/158) of those treated with haloperidol. Most of TEAEs were graded mild-to-moderate in severity. The most common TEAEs with incidence ≥5% were constipation (11.3% vs 7.6%), EPS (10.1% vs 27.2%), somnolence (8.2% vs 4.4%), drowsiness (8.2% vs 3.2%), and hypokalemia (6.9% vs 5.7%) (Table 3). Additionally, no TEAEs leading to study discontinuation or SAEs, and no deaths were reported during the study period.
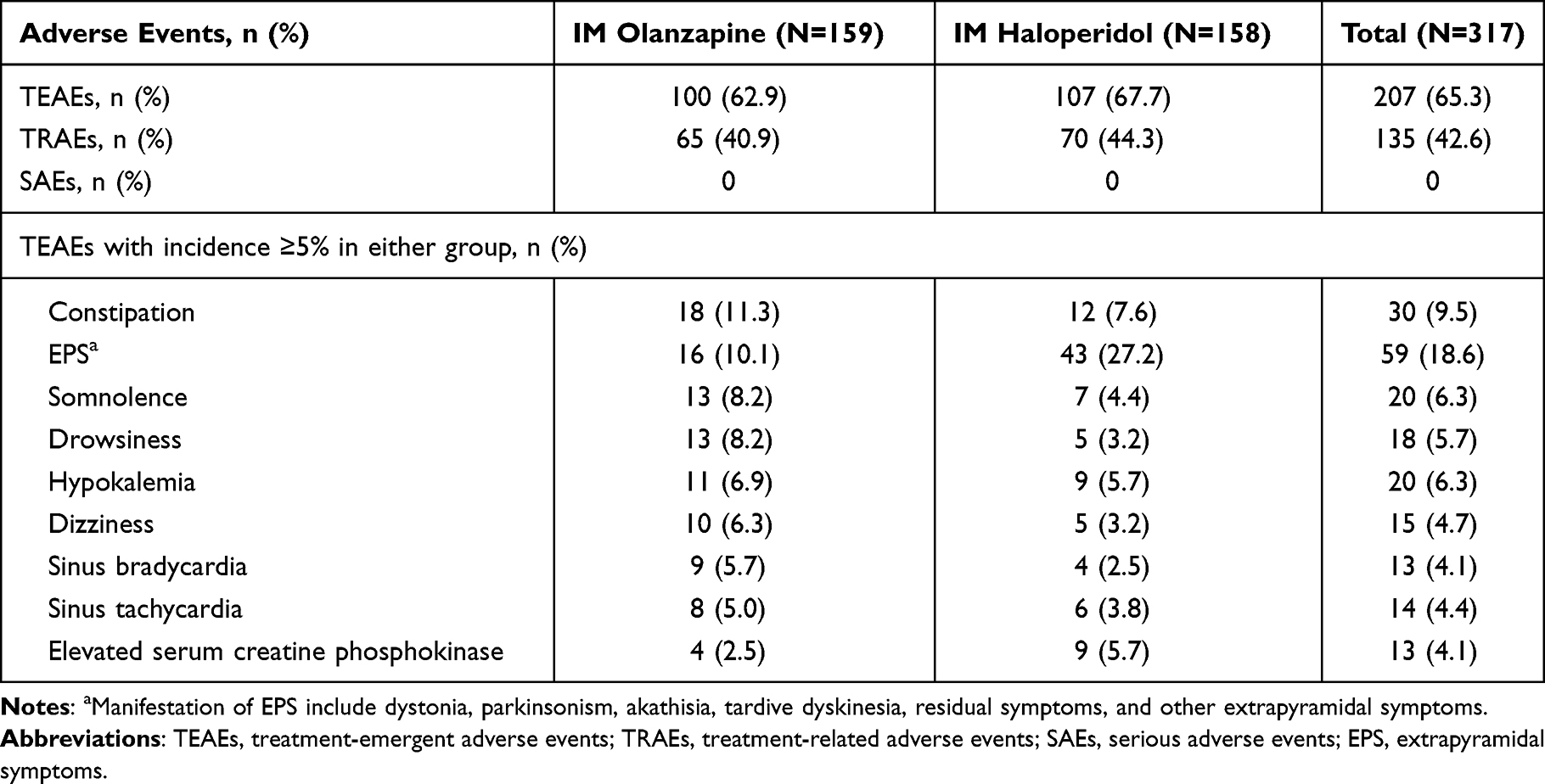 |
Table 3 Incidence of Adverse Events During the Treatment Period (Safety Set) |
Discussion
This phase 3 trial supported the non-inferiority of QLG2072 (10 mg), a generic IM olanzapine, compared to IM haloperidol (7.5 mg) in management of acute agitation associated with schizophrenia or bipolar I disorder in Chinese patients. While IM olanzapine exhibited an overall similar safety profile to IM haloperidol, it demonstrated a lower incidence of EPS compared to IM haloperidol (10.1% vs 27.2%). The comparable efficacy combined with its favorable EPS tolerability profile established QLG2072 as a viable option for acute agitation associated with schizophrenia or bipolar I disorder.
This randomized, positive-controlled trial employed a prespecified non-inferiority margin of 2.0 on the PANSS-EC scale. Statistical non-inferiority was demonstrated, because the upper limit of the 95% CI of the between-group difference in mean reduction of PNASS-EC at 2 hours after the first dose was substantially below the predefined margin. Historical data indicate that the reference IM olanzapine 10 mg achieved mean PANSS-EC score reductions of 7.7–9.4 points in schizophrenia-related acute agitation and 9.6 points in bipolar mania at 2 hours after the first IM injection, compared to 7.5–7.7 point reductions with IM haloperidol 7.5 mg in schizophrenia patients.7,14,21 While cross-trial comparisons require cautious interpretation, the generic IM olanzapine formulation exhibited comparable efficacy to the reference IM olanzapine, demonstrating similar magnitude of PANSS-EC score reduction at the 2-hour timepoint.7,14,21 Notably, the observed between-group difference in adjusted mean PANSS-EC score change from baseline at 2 hours post-injection (generic olanzapine versus haloperidol) closely matched the 0.1-point non-inferiority reported in the original olanzapine pivotal trial.7 This therapeutic concordance supports the clinical non-inferiority of the generic formulation.
When acute agitation associated with bipolar I disorder/schizophrenia were treated with IM olanzapine, sedation was an important consideration influencing the PNASS-EC change. In a randomized, double-blind, placebo-controlled study in Japanese patients with schizophrenia and acute agitation,22 the IM olanzapine (10 mg) was found to slightly increase the Agitation-Calmness Evaluation Scale (ACES) change from baseline compared with the placebo group. At 2 hours post-first injection, the mean (standard deviation) ACES scores were 3.5 (1.7) and 2.2 (1.3), with changes from baseline of 1.9 (1.5) and 0.6 (1.1), respectively. Furthermore, in a double-blind, placebo-controlled study,14 IM olanzapine (7.5 mg) showed similar mild sedation to IM haloperidol (7.5 mg) as the ACES change from baseline was similar in patients with acute agitation in schizophrenia treated with IM olanzapine or IM haloperidol. Since the ACES was not used in this study, a sensitivity analysis for PANSS-EC was performed by excluding sedated participants. The analysis indicated that the anti-agitation effect of IM olanzapine is non-inferior to that of haloperidol, independent of its sedative effects. Moreover, the efficacy of generic IM olanzapine in Chinese patients showed remarkable consistency with outcomes of the reference drug in Taiwanese population,23 though it should be cautious to interpret the results across trials.
Subgroup analyses revealed a non-significant trend toward greater therapeutic benefits of generic IM olanzapine in three specific patient populations: those with bipolar I disorder diagnosis, male patients, and individuals with baseline PANSS-EC scores of <20. To contextualize the subgroup trends, we note that the IM olanzapine has demonstrated efficacy in broadly similar acute agitation populations in separate studies, with response rates of 80.6% in patients with acutely agitated bipolar mania21 and 73.3% in patients with acute agitation and schizophrenia.7 Collectively, these data indicated the efficacy of IM olanzapine in acute agitation. However, the choice between generic IM olanzapine and haloperidol may be nuanced, with patient characteristics possibly influencing the relative therapeutic benefit.
As a second-generation antipsychotics, olanzapine injection has the characteristics of rapid onset (15–30 minutes) and remarkable therapeutic effect.7 In this study, the IM olanzapine was associated with low repeat dosing requirements, with only 8.8% of participants requiring a second IM olanzapine injection and no cases requiring a third injection within 24 hours, indicated the sustained efficacy of IM olanzapine in acute agitation management. Therefore, IM olanzapine is of particular value for the rapid management of acute agitation.24
The safety profile was overall similar between the two groups. However, generic IM olanzapine demonstrated favorable neurological tolerability, as evidenced by a lower incidence of EPS when compared with IM haloperidol. These findings were consistent with the well-documented safety characteristics of the originator product observed in clinical trials.7,14,25 The favorable safety of IM olanzapine was also supported by no occurrence of severe adverse events, treatment discontinuations, or unexpected safety signals during the study period. The observed EPS sparing effect, a characteristic pharmacological advantage of atypical antipsychotics, stems from their transient D2 receptor occupancy kinetics.26,27 Collectively, the demonstrated 24-hour therapeutic coverage, reduced requirement for rescue medication, and favorable EPS profile position generic olanzapine as a pharmacologically optimized treatment alternative supported by robust clinical evidence.
Several limitations should be considered when interpreting the results. Firstly, the potential sedation of IM olanzapine and IM haloperidol was not quantified in this study, which could directly cause informative missing and might have influenced the efficacy evaluations. Secondly, the absence of disease-specific mood scales (eg, the Young Mania Rating Scale) restricted the assessment of core mood symptoms for bipolar I patients. However, this study specifically evaluated the control of acute motor agitation. A comprehensive assessment of the broader manic symptom spectrum was beyond the scope of this trial and warrants further investigation. Thirdly, the lack of participants receiving three-dose generic IM olanzapine prevents comprehensive safety evaluation of multiple injections. Cautious clinical implementation of such dosing strategies warrants heightened pharmacovigilance. Fourthly, the non-inferiority of generic IM olanzapine was suggested in a strictly defined Chinese population, and thus, post-marketing surveillance or studies in broader acute agitation population would be valuable to confirm the safety and generalizability.
In conclusion, this phase 3 trial indicated the non-inferiority of generic IM olanzapine (QLG2072, 10 mg) to IM haloperidol in managing acute agitation associated with schizophrenia or bipolar I disorder in Chinese population. The non-inferior efficacy combined with favorable EPS profile supports the conclusion that QLG2072 offers a clinically valuable new treatment option for managing acute agitation in China.
Data Sharing Statement
The datasets generated and/or analyzed during this study are not publicly available due to privacy restrictions but are available from the corresponding author (Prof. Gang Wang, E-mail: [email protected]) upon reasonable request.
Ethics Approval
The study protocol was approved by Ethic Committee of each sites. The study was conduct adhered strictly to the Declaration of Helsinki, International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use Good Clinical Practice (ICH-GCP) guidelines.
Consent to Participate
All enrolled participants provided written informed consent.
Consent for Publication
The work is original and has not been published previously. The manuscript is not under consideration elsewhere. All authors have approved the final version and agree to its submission to Drug Design, Development and Therapy. All authors take public responsibility for the content. Appropriate permissions have been obtained for any reproduced material.
All authors meet the ICMJE criteria for authorship.
Acknowledgments
The authors thank all the patients and their families, investigators, and institutions involved in this study. We sincerely acknowledge all collaborators, for details, see Supplementary Materials Table S1.
Author Contributions
Fang Dong, Zhonggang Wang, and Chao Li share first authorship. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Gang Wang and Qingtao Bian equally contributed to this paper and thus shared the co-corresponding authorship.
Funding
This study was sponsored by Qilu Pharmaceutical Co., Ltd.
Disclosure
Nannan Li, Jie Wang, Yunfei Ju, and Juan Wang are full-time employees of Qilu Pharmaceutical Co. Ltd. The remaining authors declare no competing interests.
References
1. Roberts J, Gracia Canales A, Blanthorn-Hazell S, Craciun Boldeanu A, Judge D. Characterizing the experience of agitation in patients with bipolar disorder and schizophrenia. BMC Psychiatry. 2018;18(1):104. doi:10.1186/s12888-018-1673-3
2. Garriga M, Pacchiarotti I, Kasper S, et al. Assessment and management of agitation in psychiatry: expert consensus. World J Biol Psychiatry. 2016;17(2):86–12. doi:10.3109/15622975.2015.1132007
3. Zimbroff DL. Pharmacological control of acute agitation: focus on intramuscular preparations. CNS Drugs. 2008;22(3):199–212. doi:10.2165/00023210-200822030-00002
4. Amodeo G, Fagiolini A, Sachs G, Erfurth A. Older and newer strategies for the pharmacological management of agitation in patients with bipolar disorder or schizophrenia. CNS Neurol Disord Drug Targets. 2017;16(8):885–890.
5. Schizophrenia Collaboration Group, Chinese Society of Psychiatry. Expert consensus on psychiatric management of agitated patients. Chin J Psychiatry. 2017;50(6):401–409.
6. Andrezina R, Josiassen RC, Marcus RN, et al. Intramuscular aripiprazole for the treatment of acute agitation in patients with schizophrenia or schizoaffective disorder: a double-blind, placebo-controlled comparison with intramuscular haloperidol. Psychopharmacology. 2006;188(3):281–292. doi:10.1007/s00213-006-0541-x
7. Wright P, Birkett M, David SR, et al. Double-blind, placebo-controlled comparison of intramuscular olanzapine and intramuscular haloperidol in the treatment of acute agitation in schizophrenia. Am J Psychiatry. 2001;158(7):1149–1151. doi:10.1176/appi.ajp.158.7.1149
8. Powney MJ, Adams CE, Jones H. Haloperidol for psychosis-induced aggression or agitation (rapid tranquillisation). Cochrane Database Syst Rev. 2012;11:Cd009377. doi:10.1002/14651858.CD009377.pub2
9. Miceli JJ, Tensfeldt TG, Shiovitz T, Anziano RJ, O’Gorman C, Harrigan RH. Effects of high-dose ziprasidone and haloperidol on the QTc interval after intramuscular administration: a randomized, single-blind, parallel-group study in patients with schizophrenia or schizoaffective disorder. Clin. Ther. 2010;32(3):472–491. doi:10.1016/j.clinthera.2010.03.003
10. Stahl SM. “Hit-and-run” actions at dopamine receptors, part 1: mechanism of action of atypical antipsychotics. J Clini Psych. 2001;62(9):670–671. doi:10.4088/JCP.v62n0901
11. Wagstaff AJ, Easton J, Scott LJ. Intramuscular olanzapine: a review of its use in the management of acute agitation. CNS Drugs. 2005;19(2):147–164. doi:10.2165/00023210-200519020-00005
12. Perrin E, Anand E, Dyachkova Y, Wagner T, Frediani S, Ballerini A. A prospective, observational study of the safety and effectiveness of intramuscular psychotropic treatment in acutely agitated patients with schizophrenia and bipolar mania. European Psychiatry. 2012;27(4):234–239. doi:10.1016/j.eurpsy.2010.04.005
13. Centorrino F, Meyers AL, Ahl J, et al. An observational study of the effectiveness and safety of intramuscular olanzapine in the treatment of acute agitation in patients with bipolar mania or schizophrenia/schizoaffective disorder. Hum. Psychopharmacol. 2007;22(7):455–462. doi:10.1002/hup.870
14. Breier A, Meehan K, Birkett M, et al. A double-blind, placebo-controlled dose-response comparison of intramuscular olanzapine and haloperidol in the treatment of acute agitation in schizophrenia. Arch. Gen. Psychiatry. 2002;59(5):441–448. doi:10.1001/archpsyc.59.5.441
15. Citrome L. Comparison of intramuscular ziprasidone, olanzapine, or aripiprazole for agitation: a quantitative review of efficacy and safety. J Clini Psych. 2007;68(12):1876–1885. doi:10.4088/JCP.v68n1207
16. Wilson MP, Pepper D, Currier GW, Holloman GH Jr, Feifel D. The psychopharmacology of agitation: consensus statement of the American association for emergency psychiatry project Beta psychopharmacology workgroup. West J Emerg Med. 2012;13(1):26–34. doi:10.5811/westjem.2011.9.6866
17. Newcomer JW, Weiden PJ, Buchanan RW. Switching antipsychotic medications to reduce adverse event burden in schizophrenia: establishing evidence-based practice. J Clini Psych. 2013;74(11):1108–1120. doi:10.4088/JCP.12028ah1
18. Davis JM, Leucht S. Commentary on strategies for switching antipsychotics. BMC Med. 2008;6:18. doi:10.1186/1741-7015-6-18
19. Leucht S, Cipriani A, Spineli L, et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis. Lancet. 2013;382(9896):951–962. doi:10.1016/S0140-6736(13)60733-3
20. Kesselheim AS, Avorn J, Sarpatwari A. The High Cost of Prescription Drugs in the United States: origins and Prospects for Reform. JAMA. 2016;316(8):858–871. doi:10.1001/jama.2016.11237
21. Meehan K, Zhang F, David S, et al. A double-blind, randomized comparison of the efficacy and safety of intramuscular injections of olanzapine, lorazepam, or placebo in treating acutely agitated patients diagnosed with bipolar mania. J Clin Psychopharmacol. 2001;21(4):389–397. doi:10.1097/00004714-200108000-00006
22. Katagiri H, Fujikoshi S, Suzuki T, et al. A randomized, double-blind, placebo-controlled study of rapid-acting intramuscular olanzapine in Japanese patients for schizophrenia with acute agitation. BMC Psychiatry. 2013;13:20. doi:10.1186/1471-244X-13-20
23. Chan HY, Ree SC, Su LW, et al. A double-blind, randomized comparison study of efficacy and safety of intramuscular olanzapine and intramuscular haloperidol in patients with schizophrenia and acute agitated behavior. J Clin Psychopharmacol. 2014;34(3):355–358. doi:10.1097/JCP.0000000000000120
24. Ward K, Citrome L. The treatment of acute agitation associated with schizophrenia or bipolar disorder: investigational drugs in early stages of their clinical development, and their clinical context and potential place in therapy. Expert Opin Invest Drugs. 2020;29(3):245–257. doi:10.1080/13543784.2020.1727884
25. Lund BC, Perry PJ. Olanzapine: an atypical antipsychotic for schizophrenia. Expert Opin Pharmacother. 2000;1(2):305–323. doi:10.1517/14656566.1.2.305
26. Kapur S, Seeman P. Does fast dissociation from the dopamine d(2) receptor explain the action of atypical antipsychotics?: a new hypothesis. Am J Psychiatry. 2001;158(3):360–369. doi:10.1176/appi.ajp.158.3.360
27. Langlois X, Megens A, Lavreysen H, et al. Pharmacology of JNJ-37822681, a specific and fast-dissociating D2 antagonist for the treatment of schizophrenia. J Pharmacol Exp Ther. 2012;342(1):91–105. doi:10.1124/jpet.111.190702
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.