Back to Journals » Substance Abuse and Rehabilitation » Volume 14
Interventions to Support Engagement in Addiction Care Postpartum: Principles and Pitfalls
Authors Mazel S, Alexander K ![]() , Cioffi C, Terplan M
, Cioffi C, Terplan M
Received 29 April 2023
Accepted for publication 27 June 2023
Published 3 July 2023 Volume 2023:14 Pages 49—59
DOI https://doi.org/10.2147/SAR.S375652
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rajendra Badgaiyan
Shayna Mazel,1,* Karen Alexander,2,* Camille Cioffi,3,* Mishka Terplan2,*
1Institute for Behavioral Health, Heller School for Social Policy and Management, Brandeis University, Waltham, MA, USA; 2Friends Research Institute, Baltimore, MD, USA; 3Center on Parenting and Opioids, Prevention Science Institute, University of Oregon, Eugene, OR, USA
*These authors contributed equally to this work
Correspondence: Mishka Terplan, Friends Research Institute, 1040 Park Ave, Suite 103, Baltimore, MD, 21201, USA, Tel +1 410 837 3977, Fax +1 410 752 4218, Email [email protected]
Abstract: There is a fundamental disconnect between the optimal management of addiction in general and care delivery in pregnancy and postpartum. Addiction is a chronic condition requiring some degree of management across the life course. Yet, in the US, reproductive care is episodic and centers more on pregnancy than at other stages of the reproductive life course. Pregnancy is prioritized in access to insurance as almost all pregnant people are Medicaid eligible but access ends at varying points postpartum. This results in a structural mismatch: the episodic management of the chronic condition of addiction only within gestational periods. Though people with substance use disorder (SUD) may access care in pregnancy, treatment attrition is common postpartum. Postpartum is a time of increased vulnerabilities where insurance churn and newborn caretaking responsibilities collide in a context of care withdrawal from the health system and health providers. In part in consequence, return to use, SUD recurrence, overdose, and overdose death are more common postpartum than in pregnancy, and drug deaths have become a leading cause of maternal deaths in the US. This review addresses interventions to support engagement in addiction care postpartum. We begin with a scoping review of model programs and evidence-informed interventions that have been shown to increase continuation of care postpartum. We then explore the realities of contemporary care through a review of clinical and ethical principles, with particular attention to harm reduction. We conclude with suggestions of strategies (clinical, research, and policy) to improve care postpartum and highlight potential pitfalls in the uptake of evidence-based and person-centered services.
Keywords: pregnancy, substance use disorder, harm reduction, medication for OUD
Introduction
There is a fundamental disconnect between the optimal management of addiction in general and care delivery in pregnancy and postpartum. Addiction is a chronic condition requiring some degree of management across the life course. Yet, in the US, reproductive care is episodic and centers more on pregnancy than at other stages of the reproductive life course. Pregnancy is prioritized in access to insurance as almost all pregnant people are Medicaid eligible but access ends at varying points postpartum. This results in a structural mismatch: the episodic management of the chronic condition of addiction only within gestational periods.
Pregnancy is often an opportunity for assessment and treatment initiation for addiction. Access to health insurance coupled with both internal and external motivation for behavior change provides the context for behavioral health care. In contrast, the postpartum period is a time of care withdrawal, newborn caretaking responsibilities, insurance churn, and greater social isolation.1,2 Postpartum is a time of increased vulnerabilities, care discontinuation, return to use, addiction recurrence, overdose, and overdose death. Overdose is one of the primary drivers of the public health crisis of maternal deaths in the United States, and almost all of these perinatal deaths occur postpartum. Interventions to support engagement in addiction care postpartum are needed to address the unique barriers to treatment access and retention postpartum.
This review addresses interventions to support engagement in addiction care postpartum. We begin with a description of model programs and evidence-informed interventions that have been shown to increase continuation of care postpartum. We then explore the realities of contemporary care through a review of clinical and ethical principles, with particular attention to the principles of harm reduction including both human rights and social justice. We conclude with suggestions of strategies (clinical, research, and policy) to improve care postpartum and highlight potential pitfalls in the uptake of evidence-based and person-centered services. Overall, we highlight principles of care for this important population and touch on pitfalls in the implementation of continuing care.
A note on language: language has power, and we are conscientiously using terminology that is both evidence-informed and person-centered. People who use drugs, especially women and other people capable of pregnancy, experience discrimination, a discrimination that is visible in language. Whether intentional or not, the words used to describe pregnant people who use drugs convey and compound prejudice. Therefore, the language of this review emphasizes treatment and recovery and, we hope, upholds the dignity of all people including those who are pregnant or parenting.
Materials and Methods
The search strategy for this narrative review consisted of the following terms: ((substance use disorder OR addiction OR opioid use disorder) AND (postpartum)) AND (adherence OR engagement). PubMed was searched with no date restrictions but limited to English language only. Inclusion criteria were articles that focused on interventions that addressed addiction care in the postpartum period. Articles outside the scope of addiction and postpartum were not included. For example, articles that measured intimate partner violence, smoking cessation, postpartum depression, contraception use, or methamphetamine use among individuals with addiction during pregnancy or postpartum were not included. Additionally, articles that only focused on experiences with treatment during pregnancy were not included. However, articles focused on interventions for individuals with addiction during pregnancy were included if they also tracked outcomes through postpartum. Articles that described treatment adherence postpartum or postpartum care attendance among individuals with OUD were both included.
Results
Literature Search
The search strategy resulted in 101 articles as of February 10, 2023. After the removal of duplicates, 41 articles met the inclusion criteria and are listed in the Supplemental Appendix. These articles were broken down into four main categories: service delivery, provider or patient experience, patient outcomes, and review articles. Service delivery (n = 18) consists of new models of care or interventions to treat postpartum individuals with addiction. Provider or patient experience (n = 12) includes studies that detail patient or provider perspectives of the treatment or other services they receive for their substance use during the postpartum period. Patient outcomes (n = 7) mostly consisted of studies that describe correlations between postpartum treatment receipt and various health-care outcomes. Review articles (n = 4) consist of articles which describe care models or clinical guidelines for treating or managing addiction during the postpartum period. The included articles represented diverse study designs. These included case studies (n = 3), chart reviews (n = 3), cohort studies (n = 3), cross sectional (n = 1), implementation studies (n = 1), prospective studies (n = 1), qualitative reviews (n = 8), qualitative studies (n = 8), randomized control or clinical trial (n = 2), and retrospective studies (n = 6). Many of the studies (approximately 30%) were qualitative, either qualitative studies such as semi-structured interviews or focus groups with postpartum individuals, or qualitative reviews of the appropriate literature.
Overall, our search of interventions to support engagement in addiction care postpartum yielded articles that primarily were organized into two distinct thematic domains: medications for addiction treatment, specifically medications for opioid use disorder (MOUD) and collaborative care models, including team-based care. In addition, we found a limited literature that explored the application of harm reduction principles and practices to pregnant and postpartum people.
Discussion
Medications for Opioid Use Disorder
Of the three FDA-approved medications for OUD (naltrexone, buprenorphine, and methadone), only buprenorphine and methadone have been comprehensively studied for efficacy among pregnant people with OUD and are considered the evidence-based standard of treatment for the management of OUD during pregnancy.3–5 Naltrexone is not recommended for initiation during pregnancy,6 however continuation (ie, the individual was using naltrexone prior to pregnancy) could be considered to avoid destabilization and to promote recovery.7
According to the American College of Obstetricians and Gynecologists (ACOG) and the American Society of Addiction Medicine (ASAM), quality treatment of OUD during pregnancy begins with a person-centered education regarding medication and emphasizes the individual’s choice of receiving these medications8 and empowering individuals to make decisions about what combination of services best supports their recovery.9 MOUD should be initiated regardless of gestational age10 and should be included as part of evidence-based treatment regardless of the age of the pregnant person.11,12
Medically supervised withdrawal, or detoxification, is not recommended either in pregnancy or postpartum. Compared to MOUD, medically supervised withdrawal in pregnancy is associated with care attrition, return to use, OUD recurrence, and no difference in neonatal abstinence syndrome (NAS).13 Further, NAS is a temporary condition and MOUD exposure during pregnancy has not been associated with problematic developmental outcomes for infants.14 In contrast, MOUD is associated with increased treatment retention and improved social functioning in pregnancy and postpartum.15,16 The earlier MOUD is initiated in pregnancy, the greater the likelihood of postpartum continuation.17
The normal physiological changes of pregnancy often necessitate increases in MOUD dose and frequency of dose, especially as pregnancy progresses.5,18,19 Pregnant people become “rapid metabolizers” of methadone and therefore split dosing is preferable to simply increasing the daily dose.20 The clinical use of serum methadone/metabolite ratios has been proposed to assist in decision-making around timing of split dosing.21 There is no clinical guidance to navigate MOUD decreases postpartum among people who had an increase in pregnancy. In fact, we did not identify a single article that investigated MOUD dose or frequency changes in the postpartum period. Medication dose and timing decisions should therefore be individualized. Rapid, arbitrary, or universal dose reductions are likely harmful.
Despite medical recognition that MOUD is the gold standard for managing OUD in pregnancy, it is severely underutilized.22,23 Fewer than one-quarter of pregnant individuals with OUD receive any substance use disorder treatment and even fewer receive MOUD.22,24 Postpartum, MOUD utilization decreases further.25 The short-sighted view of OUD as an acute disease during pregnancy, rather than viewing interventions in pregnancy as an opportunity for long-term recovery, has contributed to OUD being a leading cause of pregnancy-related mortality in the US.10
Overall, barriers to access and receipt of MOUD are the main reason for MOUD underutilization, barriers which only increase postpartum. One barrier is a lack of awareness among health-care providers that MOUD is safe and effective in pregnancy and during breastfeeding.26 In fact, breastfeeding while receiving MOUD can help reduce withdrawal symptoms for infants with neonatal opioid withdrawal though providers often provide conflicting information about breastfeeding safety.27 Logistical challenges, such as lack of childcare and transportation,28 coupled with a shortage of treatment programs that are family-friendly,29 an emerging federal policy priority30 further reduces MOUD access.
Stigma and discrimination toward people with addiction are common and are intensified for people who are pregnant and parenting. Stigma affects treatment receipt at the individual level (via internalized stigma), the interpersonal level (when provided suboptimal care by their provider),31,32 as well as at the structural level (when people are turned away from the clinic by the provider because they are pregnant).33 While federal policy has prioritized treatment access in pregnancy, some clinics do not act in accordance with this guidance. Further, state policies that penalize substance use during pregnancy discourage people from treatment initiation and continuation for the legitimate fear of legal consequences, such as losing child custody.34
Models of Care
Medications are important, but the environment of care delivery is critical to keep people engaged through the postpartum period. Our scoping review identified interventions that employed collaborative care and integrated care models to support engagement in addiction care postpartum. Integrated team-based care models co-locate specialized treatment to reduce access barriers.9 Collaborative care models organize care for people with multiple specialists involved in their treatment plan35 in a stepped-care manner without specialists necessarily being located in the same space.
Integrated Care Model
Integrated care models successfully improve outcomes for people with chronic diseases, such as HIV.36,37 Through co-locating interventions or specialists in one clinic, people can more easily access services and communication occurs more effectively and efficiently improving the care experience. Integrated care models which co-locate obstetrics and addiction care decrease preterm birth rates and increase prenatal care engagement.38 Integrated care models may also increase retention rates for people receiving treatment for opioid use disorder.9 In a cohort of rural pregnant women with opioid use disorder, integrated care delivery was associated with lower risks of positive maternal urine toxicology screen at birth.39
Collaborative Care Model
In a collaborative care approach, all patients are screened for conditions requiring specialized care (eg, addiction), but first-line treatments are offered within the primary or obstetric care office setting. Care coordinators facilitate initial treatment planning, brief interventions, symptom monitoring, and implementation of stepped-care recommendations. Initial brief intervention typically begins with the provision of psychoeducation and, if indicated, medication. If the patient does not respond to the initial line of treatment, care is augmented,40 and patients who need specialized treatment are stepped up to a higher level of care.41 Very often the primary care physician can implement medication changes, thereby efficiently reserving specialty care for those patients who do not respond to earlier steps in the treatment algorithm. Proposed benefits of CC include patient-centered care, receipt of behavioral and physical health care in the same familiar setting, and improved clinical outcomes.
Collaborative care is effective because it is personalized and titrates the delivery of specialized health care to the treatment intensity required for a given patient. This feature is especially useful before and after birth. Pregnant and postpartum people have unique challenges, such as the physical and mental demands of pregnancy and caring for a new infant, which can change relationships and employment status. For pregnant people, collaborative care models typically integrate behavioral health care with pre- and post-partum care42 in the obstetric practice. Connection with collaborative care support in the post-partum period is associated with breastfeeding rates twice that of groups not connected with collaborative care.43,44 The long-term prevention and engagement in post-partum depression and anxiety treatment is also improved with adherence to a collaborative care model.45
In both integrated care and collaborative care models, care coordination is an activity rather than a service. Nurses in all settings are responsible for care coordination, and especially for people who use drugs, their role is vital in ensuring access to treatment and support. Integrated care means that health-care professionals across the birthing continuum promote recovery-based services. Nurses based in outpatient obstetric or inpatient obstetric and newborn services can work collaboratively to ensure transition to primary care and other behavioral health service providers to address the holistic needs of individuals seeking care. Table 1 summarizes specific collaborative care models that demonstrated improved engagement in care postpartum. Team-Based Care.
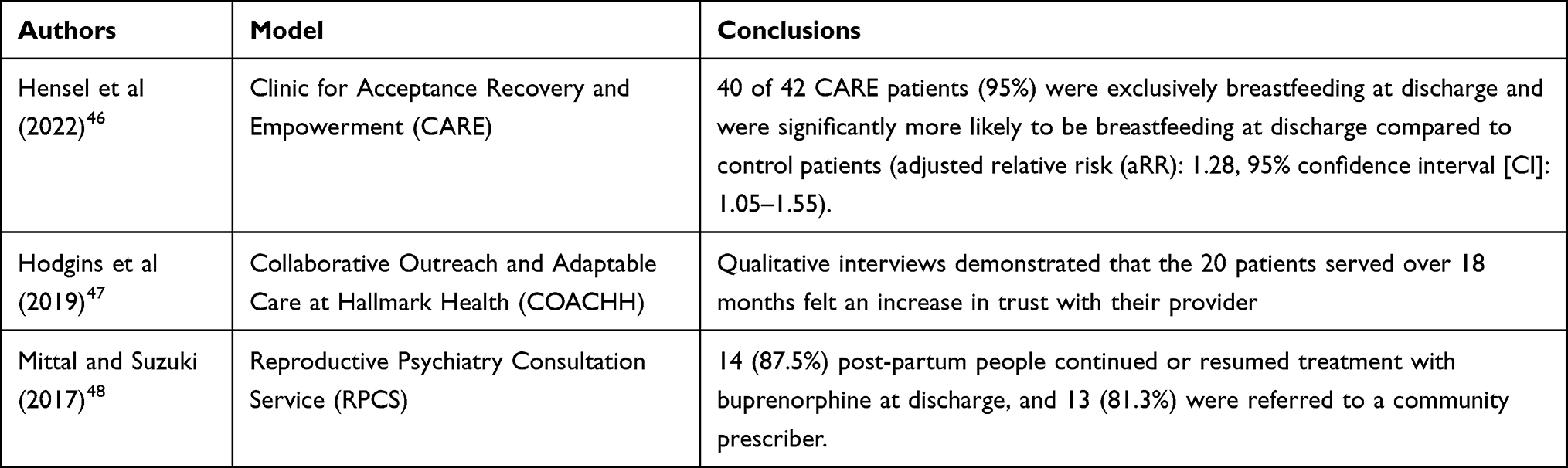 |
Table 1 Collaborative Care Interventions to Support Engagement in Addiction Care Postpartum |
Integrated and collaborative care models are only as successful as the multidisciplinary team surrounding the model. Team-based care has successfully implemented patient safety bundles through collaborative learning, quality improvement support, and rapid response data review.49,50 Team-based care can lead to health system-wide changes via shared decision-making led by clinical champions and lead coordinators.
Shared decision-making, defined as supporting the patient in choosing the best treatment,51 is particularly applicable to pregnant and postpartum people with substance use disorders. Guille et al52 developed a shared decision-making tool to assist providers and patients in addressing postpartum treatment continuation decisions. Postpartum people caring for infants have concerns about medications and breastfeeding, experience stigma, and often have unstable insurance coverage. A decision-making tool can aid in presenting the same evidence-based information to both the patient and all providers involved. Following the shared decision-making process, 95% (21 of 22) of post-partum patients reported making an informed decision to either continue (64%, 14 of 22) or taper (36%, 8 of 22) buprenorphine or methadone. Post-partum people in the study felt they were provided with adequate medical information (96%, 21 of 22) and understood their treatment choices (91%, 20 of 22).52
Harm Reduction and Postpartum
Harm reduction is an essential component of health-care practice especially postpartum. The Harm Reduction Coalition defines harm reduction as a “set of practical strategies and ideas aimed at reducing negative consequences associated with drug use” and “a movement for social justice built on a belief in, and respect for, the rights of people who use drugs”.53 For people in the postpartum period, harm reduction includes access to proven strategies that reduce the likelihood of overdose and infectious disease transmission for people who use drugs.54 However, within harm reduction efforts, systemic barriers hinder the accessibility of harm reduction services for this population. For example, access to safer injection supplies and naloxone are life preserving resources for people who use drugs55 but the demands of caring for a newborn may reduce the likelihood that a parent would have the capacity to access a syringe exchange program, or they may encounter stigma for asking for support obtaining these resources.56 In instances where a child has been removed from care, abstinence requirements sanctioned by child welfare promote concealment of use and decrease the likelihood of engagement with services.57 Moreover, the experience of termination of parental rights signifies permanent separation and intense feelings of grief and loss which neither harm reduction programs nor medical care are equipped to support.58,59 While the intention of accessibility to harm reduction services is never to promote use, the nature of the disease of addiction means that there are people who find themselves in need of harm reduction resources postpartum but experience greater barriers to participation. An intentional examination of these barriers with aligned solutions is a first step toward reducing harms associated with postpartum substance use. Table 2 provides an overview of evidence-based harm reduction strategies and potential barriers to access for people who use drugs during the postpartum period as well as potential strategies to ameliorate these barriers.
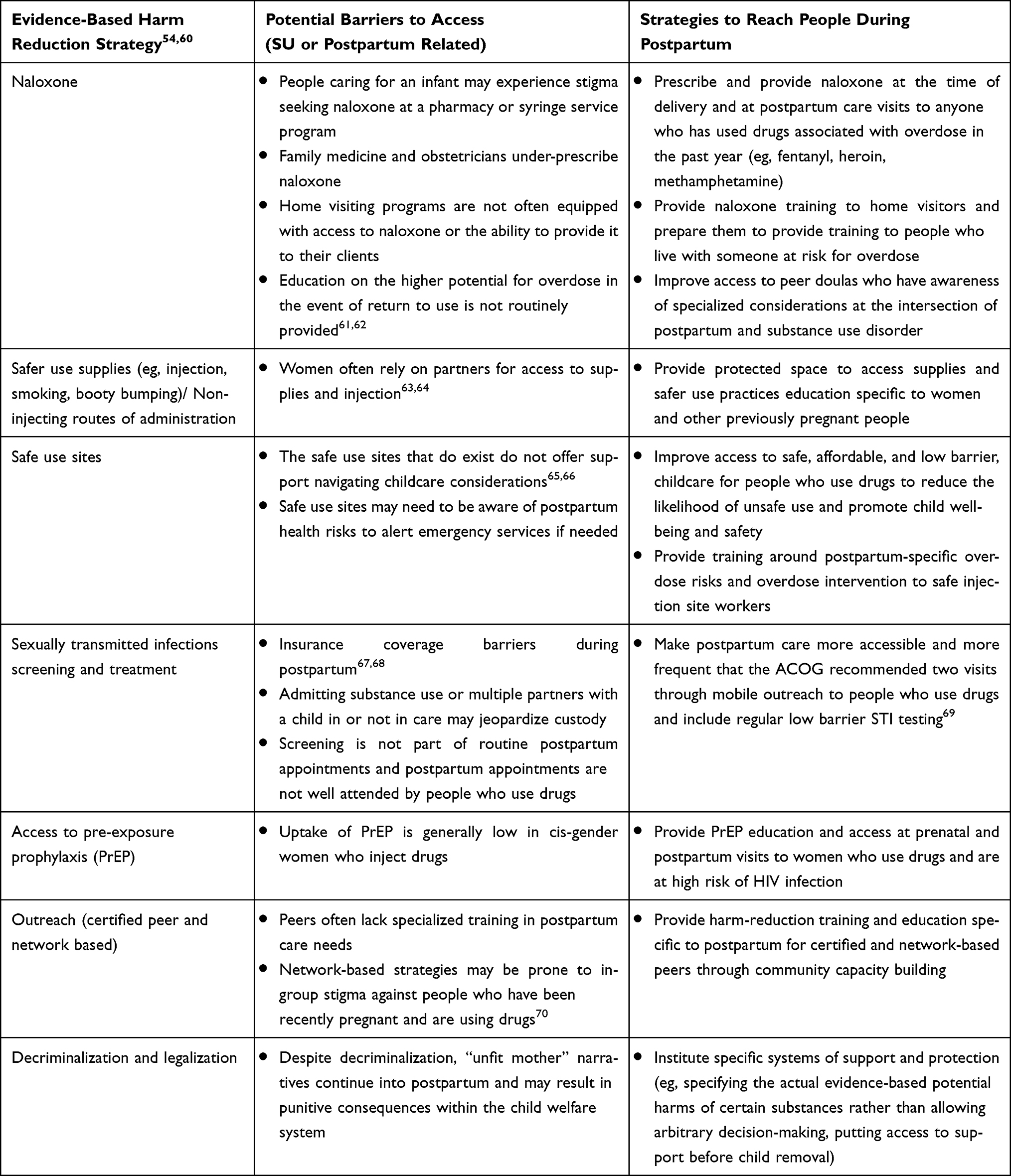 |
Table 2 Barriers and Strategies of Evidence-Based Harm Reduction Strategies to Support Engagement in Addiction Care Postpartum |
From a solutions perspective, for parents at risk of return to use who are caring for an infant or other children, there is a need to promote awareness of risk reducing behaviors such as never using alone.60 Promoting and providing access to phone or web-based services that call emergency services if an individual does not respond could be one strategy to prevent death among people who may otherwise choose to use while caring for a child. Additionally, offering voluntary respite promotes family unity and community which may ultimately maximize child safety as well as parental well-being.71
Harm reduction strategies generally focus on the individual, however there are structural inequities which impinge upon people’s ability to engage in care and recovery. For example, the lack of universal paid family leave means that people who are economically under resourced must work even within days after giving birth in order to survive.72,73 Similarly, the termination of Medicaid within 6 weeks of birth in some states is often structurally incompatible with the life course management of chronic conditions. Among adults, the connection of substance use and economic disadvantage is well documented, and policies that provide systematic support to give individuals the time, financial resources, and social support to care for a newborn are necessary to sustain reduced use patterns.74,75
Harm reduction goes beyond the provision of supplies and education of health promotion strategies. Hawk et al76 outline a set of harm reduction principles for health-care settings that include humanism, pragmatism, individualism, autonomy, incrementalism, and accountability without termination. These principles are revised and applied to addiction care during the postpartum period in Table 3. Addiction services during postpartum often lack a harm reduction perspective, emphasizing abstinence as the only pathway to successful parenting.77,78 While retaining or regaining child custody is a significant motivator for many,79 the emphasis on abstinence is problematic. Specifically, using the evidence-based definition of addiction as a chronic and recurring disorder, we know that return to use occurs frequently, albeit not always. This means that our systems must be designed to provide support through episodes of return to use and recognize that punishment deters individuals from engagement with care.80–82
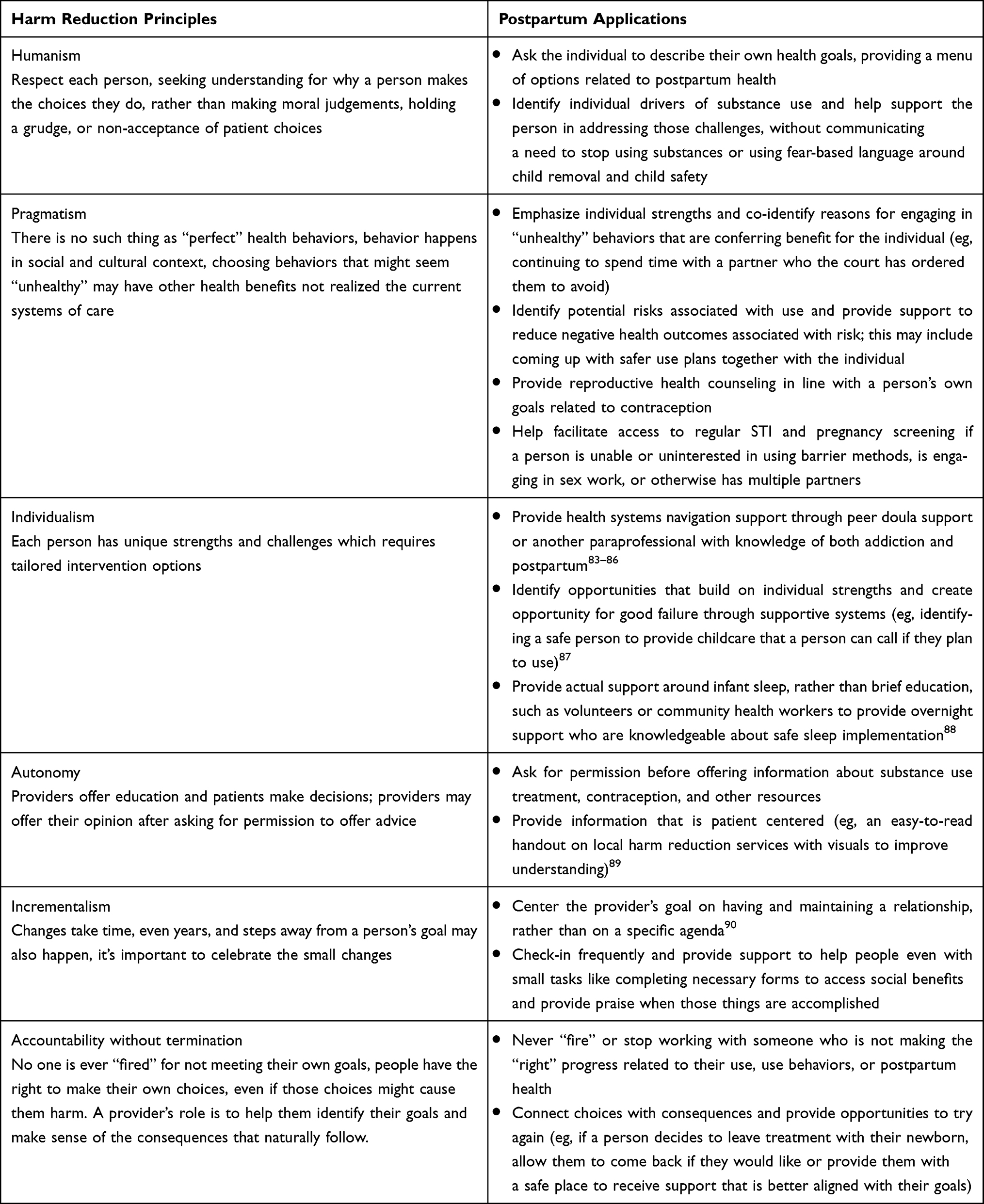 |
Table 3 Harm Reduction Principles and Postpartum Applications |
Conclusion
This review highlights the vulnerabilities that emerge postpartum for people with OUD. The episodic nature of care delivery for pregnancy, which is reflected in the episodic access to health insurance, complicates chronic disease management. The structure of health care at the intersection of reproductive and behavioral health abandons people postpartum, an abandonment that can be fatal for people with OUD. Although MOUD is the standard-of-care and methadone and buprenorphine are the safest and most effective medications for OUD in pregnancy, access in inequitable and MOUD continuation lags postpartum. Interventions to support engagement in addiction care postpartum exist but are under-utilized. Specifically, the expansion of collaborative care models from pregnancy through early parenting is needed. Future research should focus on the integration of team-based care services into addiction treatment for pregnant and postpartum people and explore sustainability from a chronic disease management perspective. From a harm reduction perspective, harm reduction includes both practical strategies and principles to ultimately improve care engagement and health outcomes. These strategies and principles are sparsely implemented and have the potential to transform care during this period, though more evidence is needed to clarify appropriate applications. Policy priorities include expansion and continuation of health insurance coverage through the postpartum period and the rolling back of punitive policies which force people away from care.
Acknowledgement
This study was supported by NIDA award - P50DA048756 (C Cioffi).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Admon LK, Zivin K, Kozhimannil KB. Perinatal insurance coverage and behavioural health-related maternal mortality. Int Rev Psychiatry. 2021;33(6):553–556. doi:10.1080/09540261.2021.1903843
2. Interrante JD, Admon LK, Carroll C, Henning-Smith C, Chastain P, Kozhimannil KB. Association of health insurance, geography, and race and ethnicity with disparities in receipt of recommended postpartum care in the US. JAMA Health Forum. 2022;3(10):e223292. doi:10.1001/jamahealthforum.2022.3292
3. CDC. Opioid use disorder and pregnancy. Centers for Disease Control and Prevention; 2022. Available from: https://www.cdc.gov/pregnancy/opioids/treatment.html.
4. Substance Abuse and Mental Health Services Administration. A collaborative approach to the treatment of pregnant women with opioid use disorders. Substance Abuse and Mental Health Services Administration; 2016. Available from: https://store.samhsa.gov/product/A-Collaborative-Approach-to-the-Treatment-of-Pregnant-Women-with-Opioid-Use-Disorders/SMA16-4978.
5. American Society of Addiction Medicine, The American College of Obstetricians and Gynecologists’ Committee on obstetric practice. ACOG Committee Opinion: Opioid Use and Opioid Use Disorder in Pregnancy; 2017. Available from: https://www.acog.org/Clinical-Guidance-and-Publications/Committee-Opinions/Committee-on-Obstetric-Practice/Opioid-Use-and-Opioid-Use-Disorder-in-Pregnancy.
6. Harter K. Opioid use disorder in pregnancy. Ment Health Clin. 2019;9(6):359–372. doi:10.9740/mhc.2019.11.359
7. Wachman EM, Saia K, Miller M, et al. Naltrexone treatment for pregnant women with opioid use disorder compared with matched buprenorphine control subjects. Clin Ther. 2019;41(9):1681–1689. doi:10.1016/j.clinthera.2019.07.003
8. Ecker J, Abuhamad A, Hill W, et al. Substance use disorders in pregnancy: clinical, ethical, and research imperatives of the opioid epidemic: a report of a joint workshop of the Society for Maternal-Fetal Medicine, American College of Obstetricians and Gynecologists, and American Society of Addiction Medicine. Am J Obstet Gynecol. 2019;221(1):B5–B28. doi:10.1016/j.ajog.2019.03.022
9. Ellis LP, Parlier-Ahmad AB, Scheikl M, Martin CE. An integrated care model for pregnant and postpartum individuals receiving medication for opioid use disorder. J Addict Med. 2023;17(2):131–139. doi:10.1097/ADM.0000000000001052
10. Saia KA, Schiff D, Wachman EM, et al. Caring for pregnant women with opioid use disorder in the USA: expanding and improving treatment. Curr Obstet Gynecol Rep. 2016;5(3):257–263. doi:10.1007/s13669-016-0168-9
11. The Society for Adolescent Health and Medicine. Medication for adolescents and young adults with opioid use disorder (position paper). J Adolesc Health. 2021;68(3):632–636. doi:10.1016/j.jadohealth.2020.12.129
12. Cunningham C, Edlund MJ, Fishman M, et al. The ASAM national practice guideline for the treatment of opioid use disorder: 2020 focused update. J Addict Med. 2020;14(2S):1. doi:10.1097/ADM.0000000000000633
13. Terplan M, Laird HJ, Hand DJ, et al. Opioid detoxification during pregnancy: a systematic review. Obstet Gynecol. 2018;131(5):803–814. doi:10.1097/AOG.0000000000002562
14. Jones HE, Jansson LM, O’Grady KE, Kaltenbach K. The relationship between maternal methadone dose at delivery and neonatal outcome: methodological and design considerations. Neurotoxicol Teratol. 2013;39:110–115. doi:10.1016/j.ntt.2013.05.003
15. Jones HE, Kaltenbach K, Heil SH, et al. Neonatal abstinence syndrome after methadone or buprenorphine exposure. N Engl J Med. 2010;363(24):2320–2331. doi:10.1056/NEJMoa1005359
16. Mattick RP, Breen C, Kimber J, Davoli M. Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence. Cochrane Database Syst Rev. 2014;(2):CD002207. doi:10.1002/14651858.CD002207.pub4
17. Krans EE, Kim JY, Chen Q, et al. [coding hypertensive/other things] Outcomes associated with the use of medications for opioid use disorder during pregnancy. Addict Abingdon Engl. 2021;116(12):3504–3514. doi:10.1111/add.15582
18. Rizk AH, Simonsen SE, Roberts L, Taylor-Swanson L, Lemoine JB, Smid M. Maternity care for pregnant women with opioid use disorder: a review. J Midwifery Womens Health. 2019;64(5):532–544. doi:10.1111/jmwh.13019
19. Pond SM, Kreek MJ, Tong TG, Raghunath J, Benowitz NL. Altered methadone pharmacokinetics in methadone-maintained pregnant women. J Pharmacol Exp Ther. 1985;233(1):1–6.
20. McCarthy JJ, Jones HE, Terplan M, Rudolf VP, von Klimo MC. Changing outdated methadone regulations that harm pregnant patients. J Addict Med. 2021;15(2):93–95. doi:10.1097/ADM.0000000000000720
21. McCarthy JJ, Vasti EJ, Leamon MH, Graas J, Ward C, Fassbender C. The use of serum methadone/metabolite ratios to monitor changing perinatal pharmacokinetics. J Addict Med. 2018;12(3):241–246. doi:10.1097/ADM.0000000000000398
22. Clemans-Cope L, Lynch V, Howell E, et al. Pregnant women with opioid use disorder and their infants in three state Medicaid programs in 2013–2016. Drug Alcohol Depend. 2019;195:156–163. doi:10.1016/j.drugalcdep.2018.12.005
23. Krans EE, Kim JY, James AE, Kelley D, Jarlenski MP. Medication-assisted treatment use among pregnant women with opioid use disorder. Obstet Gynecol. 2019;133(5):943–951. doi:10.1097/AOG.0000000000003231
24. Guille C, Simpson AN, Douglas E, et al. Treatment of opioid use disorder in pregnant women via telemedicine: a nonrandomized controlled trial. JAMA Netw Open. 2020;3(1):e1920177. doi:10.1001/jamanetworkopen.2019.20177
25. Schiff DM, Nielsen TC, Hoeppner BB, et al. Methadone and buprenorphine discontinuation among postpartum women with opioid use disorder. Am J Obstet Gynecol. 2021;225(4):424.e1–424.e12. doi:10.1016/j.ajog.2021.04.210
26. Short VL, Cambareri K, Gannon M, Alexander K, Abatemarco DJ. A pilot study to assess breastfeeding knowledge, attitudes, and perceptions of individuals who work in perinatal opioid use disorder treatment settings. Breastfeed Med. 2019;14(5):307–312. doi:10.1089/bfm.2018.0257
27. Collins M. Breastfeeding recommendations for people who use substances: AWHONN practice brief number 16. J Obstet Gynecol Neonatal Nurs. 2023;52(1):e1–e4. doi:10.1016/j.jogn.2022.08.003
28. Godersky ME, Saxon AJ, Merrill JO, Samet JH, Simoni JM, Tsui JI. Provider and patient perspectives on barriers to buprenorphine adherence and the acceptability of video directly observed therapy to enhance adherence. Addict Sci Clin Pract. 2019;14(1):11. doi:10.1186/s13722-019-0139-3
29. Feder KA, Mojtabai R, Musci RJ, Letourneau EJ. U.S. adults with opioid use disorder living with children: treatment use and barriers to care. J Subst Abuse Treat. 2018;93:31–37. doi:10.1016/j.jsat.2018.07.011
30. U.S. Department of Health and Human Services Assistant Secretary for Planning and Evaluation Office of Disability. State policy levers for expanding family-centered medication-assisted treatment. Aging and Long-Term Care Policy; 2019:1–55. Available from: https://aspe.hhs.gov/sites/default/files/migrated_legacy_files//187076/ExpandFCMAT.pdf.
31. Syvertsen JL, Toneff H, Howard H, Spadola C, Madden D, Clapp J. Conceptualizing stigma in contexts of pregnancy and opioid misuse: a qualitative study with women and healthcare providers in Ohio. Drug Alcohol Depend. 2021;222:108677. doi:10.1016/j.drugalcdep.2021.108677
32. Skaggs P, Bell SB, Scutchfield FD, Robinson LE. Providers’ stigmas and the effects on patients with opioid use disorder: a scoping review. J Appalachian Health. 2022. doi:10.13023/JAH.0403.06
33. Patrick SW, Richards MR, Dupont WD, et al. Association of pregnancy and insurance status with treatment access for opioid use disorder. JAMA Netw Open. 2020;3(8):e2013456–e2013456. doi:10.1001/jamanetworkopen.2020.13456
34. Patrick SW, Schiff DM, Ryan SA, Quigley J, Gonzalez PK, Walker LR. A public health response to opioid use in pregnancy. Pediatrics. 2017;139(3):e20164070. doi:10.1542/peds.2016-4070
35. Goodrich DE, Kilbourne AM, Nord KM, Bauer MS. Mental health collaborative care and its role in primary care settings. Curr Psychiatry Rep. 2013;15(8):383. doi:10.1007/s11920-013-0383-2
36. Weaver MR, Conover CJ, Proescholdbell RJ, et al. Cost-effectiveness analysis of integrated care for people with HIV, chronic mental illness and substance abuse disorders. J Ment Health Policy Econ. 2009;12(1):33–46.
37. Beichler H, Grabovac I, Dorner TE. Integrated care as a model for interprofessional disease management and the benefits for people living with HIV/AIDS. Int J Environ Res Public Health. 2023;20(4):3374. doi:10.3390/ijerph20043374
38. Milligan K, Niccols A, Sword W, Thabane L, Henderson J, Smith A. Birth outcomes for infants born to women participating in integrated substance abuse treatment programs: a meta-analytic review. Addict Res Theory. 2011;19(6):542–555. doi:10.3109/16066359.2010.545153
39. Goodman DJ, Saunders EC, Frew JR, et al. Integrated vs nonintegrated treatment for perinatal opioid use disorder: retrospective cohort study. Am J Obstet Gynecol MFM. 2022;4(1):100489. doi:10.1016/j.ajogmf.2021.100489
40. Katon WJ. The Institute of Medicine “Chasm” report: implications for depression collaborative care models. Gen Hosp Psychiatry. 2003;25(4):222–229. doi:10.1016/s0163-8343(03)00064-1
41. Huffman JC, Niazi SK, Rundell JR, Sharpe M, Katon WJ. Essential articles on collaborative care models for the treatment of psychiatric disorders in medical settings: a publication by the Academy of Psychosomatic Medicine Research and Evidence-based Practice Committee. Psychosomatics. 2014;55(2):109–122. doi:10.1016/j.psym.2013.09.002
42. Huang H, Tabb KM, Cerimele JM, Ahmed N, Bhat A, Kester R. Collaborative care for women with depression: a systematic review. Psychosomatics. 2017;58(1):11–18. doi:10.1016/j.psym.2016.09.002
43. Freytsis M, Phillippi JC, Cox KJ, Romano A, Cragin L. The American College of Nurse-midwives clarity in collaboration project: describing midwifery care in interprofessional collaborative care models. J Midwifery Womens Health. 2017;62(1):101–108. doi:10.1111/jmwh.12521
44. Allen EC, Sakowicz A, Parzyszek CL, McDonald A, Miller ES. The association between engagement in a perinatal collaborative care program and breastfeeding among people with identified mental health conditions. Am J Obstet Gynecol MFM. 2022;4(3):100591. doi:10.1016/j.ajogmf.2022.100591
45. Miller ES, Grobman WA, Ciolino JD, et al. Increased depression screening and treatment recommendations after implementation of a perinatal collaborative care program. Psychiatr Serv Wash DC. 2021;72(11):1268–1275. doi:10.1176/appi.ps.202000563
46. Hensel D, Helou NE, Zhang F, et al. The impact of a multidisciplinary opioid use disorder prenatal clinic on breastfeeding rates and postpartum care. Am J Perinatol. 2022. doi:10.1055/s-0042-1748526
47. Hodgins FE, Lang JM, Malseptic GG, Melby LH, Connolly KA. Coordinating outpatient care for pregnant and postpartum women with opioid use disorder: implications from the COACHH program. Matern Child Health J. 2019;23(5):585–591. doi:10.1007/s10995-018-2683-y
48. Mittal L, Suzuki J. Feasibility of collaborative care treatment of opioid use disorders with buprenorphine during pregnancy. Subst Abuse. 2017;38(3):261–264. doi:10.1080/08897077.2015.1129525
49. Iddins BW, Frank JS, Kannar P, et al. Evaluation of team-based care in an urban free clinic setting. Nurs Adm Q. 2015;39(3):254–262. doi:10.1097/NAQ.0000000000000103
50. Keshmiri F, Rezai M, Tavakoli N. The effect of interprofessional education on healthcare providers’ intentions to engage in interprofessional shared decision-making: perspectives from the theory of planned behaviour. J Eval Clin Pract. 2020;26(4):1153–1161. doi:10.1111/jep.13379
51. Hargraves IG, Fournier AK, Montori VM, Bierman AS. Generalized shared decision making approaches and patient problems. Adapting AHRQ’s SHARE approach for purposeful SDM. Patient Educ Couns. 2020;103(10):2192–2199. doi:10.1016/j.pec.2020.06.022
52. Guille C, Jones HE, Abuhamad A, Brady KT. Shared decision-making tool for treatment of perinatal opioid use disorder. Psychiatr Res Clin Pract. 2019;1(1):27–31. doi:10.1176/appi.prcp.20180004
53. Principles of Harm Reduction. National harm reduction coalition. Available from: https://harmreduction.org/about-us/principles-of-harm-reduction/.
54. Hawk KF, Vaca FE, D’Onofrio G. Reducing fatal opioid overdose: prevention, treatment and harm reduction strategies. Yale J Biol Med. 2015;88(3):235–245.
55. Castillo T. Harm reduction strategies for the opiod crisis. N C Med J. 2018;79(3):192–194. doi:10.18043/ncm.79.3.192
56. Escañuela Sánchez T, Matvienko-Sikar K, Linehan L, O’Donoghue K, Byrne M, Meaney S. Facilitators and barriers to substance-free pregnancies in high-income countries: a meta-synthesis of qualitative research. Women Birth J Aust Coll Midwives. 2022;35(2):e99–e110. doi:10.1016/j.wombi.2021.04.010
57. Wolfson L, Schmidt RA, Stinson J, Poole N. Examining barriers to harm reduction and child welfare services for pregnant women and mothers who use substances using a stigma action framework. Health Soc Care Community. 2021;29(3):589–601. doi:10.1111/hsc.13335
58. Blanton TL, Deschner J. Biological mothers’ grief: the postadoptive experience in open versus confidential adoption. Child Welfare. 1990;69(6):525–535.
59. Kenny KS, Barrington C, Green SL. “I felt for a long time like everything beautiful in me had been taken out”: women’s suffering, remembering, and survival following the loss of child custody. Int J Drug Policy. 2015;26(11):1158–1166. doi:10.1016/j.drugpo.2015.05.024
60. Ritter A, Cameron J. A review of the efficacy and effectiveness of harm reduction strategies for alcohol, tobacco and illicit drugs. Drug Alcohol Rev. 2006;25(6):611–624. doi:10.1080/09595230600944529
61. Brown HL. Opioid management in pregnancy and postpartum. Obstet Gynecol Clin North Am. 2020;47(3):421–427. doi:10.1016/j.ogc.2020.04.005
62. Rankin L, Mendoza NS, Grisham L. Unpacking perinatal experiences with opioid use disorder: relapse risk implications. Clin Soc Work J. 2023;51(1):34–45. doi:10.1007/s10615-022-00847-x
63. El-Bassel N, Shaw SA, Dasgupta A, Strathdee SA. People who inject drugs in intimate relationships: it takes two to combat HIV. Curr HIV/AIDS Rep. 2014;11(1):45–51. doi:10.1007/s11904-013-0192-6
64. Morris MD, Andrew E, Tan JY, et al. Injecting-related trust, cooperation, intimacy, and power as key factors influencing risk perception among drug injecting partnerships. PLoS One. 2019;14(5):e0217811. doi:10.1371/journal.pone.0217811
65. Kashak D. An overview of issues, impacts and services for women who are using substances and are pregnant or parenting within the City of Thunder Bay. Thunder Bay Thunder Bay Drug Strategy. 2015.
66. Mitra S, Rachlis B, Krysowaty B, et al. Potential use of supervised injection services among people who inject drugs in a remote and mid-size Canadian setting. BMC Public Health. 2019;19(1):284. doi:10.1186/s12889-019-6606-7
67. Daw JR, Winkelman TNA, Dalton VK, Kozhimannil KB, Admon LK. Medicaid expansion improved perinatal insurance continuity for low-income women. Health Aff Proj Hope. 2020;39(9):1531–1539. doi:10.1377/hlthaff.2019.01835
68. Daw JR, Kolenic GE, Dalton VK, et al. Racial and ethnic disparities in perinatal insurance coverage. Obstet Gynecol. 2020;135(4):917–924. doi:10.1097/AOG.0000000000003728
69. McKinney J, Keyser L, Clinton S, Pagliano C. ACOG Committee Opinion No. 736: optimizing postpartum care. Obstet Gynecol. 2018;132(3):784–785. doi:10.1097/AOG.0000000000002849
70. Williams LD, Mackesy-Amiti ME, Latkin C, Boodram B. Drug use-related stigma, safer injection norms, and hepatitis C infection among a network-based sample of young people who inject drugs. Drug Alcohol Depend. 2021;221:108626. doi:10.1016/j.drugalcdep.2021.108626
71. Safe Families for Children (SFFC). Safe families for children evidence-based evaluation; 2021:2. Available from: http://safe-families.org/wp-content/uploads/2021/06/Evidence-based-Summary.pdf.
72. Fass S. Paid leave in the states: a critical support for low-wage workers and their families. National Center for Children in Poverty (NCCP); 2009. Available from: https://www.nccp.org/publication/paid-leave-in-the-states/.
73. Reno R, Barnhart S, Gabbe PT. A critical inquiry of breastfeeding attitudes, barriers, and experiences of African American women living in poverty. J Poverty. 2018;22(6):518–536. doi:10.1080/10875549.2018.1496374
74. Karriker-Jaffe KJ. Areas of disadvantage: a systematic review of effects of area-level socioeconomic status on substance use outcomes. Drug Alcohol Rev. 2011;30(1):84–95. doi:10.1111/j.1465-3362.2010.00191.x
75. Linton SL, Haley DF, Hunter-Jones J, Ross Z, Cooper HLF. Social causation and neighborhood selection underlie associations of neighborhood factors with illicit drug-using social networks and illicit drug use among adults relocated from public housing. Soc Sci Med. 2017;185:81–90. doi:10.1016/j.socscimed.2017.04.055
76. Hawk M, Coulter RWS, Egan JE, et al. Harm reduction principles for healthcare settings. Harm Reduct J. 2017;14(1):70. doi:10.1186/s12954-017-0196-4
77. Hyshka E, Morris H, Anderson-Baron J, Nixon L, Dong K, Salvalaggio G. Patient perspectives on a harm reduction-oriented addiction medicine consultation team implemented in a large acute care hospital. Drug Alcohol Depend. 2019;204:107523. doi:10.1016/j.drugalcdep.2019.06.025
78. Brown C, Stewart SH. Harm reduction for women in treatment for alcohol use problems: exploring the impact of dominant addiction discourse. Qual Health Res. 2021;31(1):54–69. doi:10.1177/1049732320954396
79. Cioffi CC, Seeley JR. Voluntary pregnancy screening at syringe exchanges: a feasibility study. J Prev Health Promot. 2021;2(1):57–80. doi:10.1177/2632077020973362
80. White SA, McCourt A, Bandara S, Goodman DJ, Patel E, McGinty EE. Implementation of state laws giving pregnant people priority access to drug treatment programs in the context of coexisting punitive laws. Womens Health Issues. 2023;33(2):117–125. doi:10.1016/j.whi.2022.09.001
81. Faherty LJ, Kranz AM, Russell-Fritch J, Patrick SW, Cantor J, Stein BD. Association of punitive and reporting state policies related to substance use in pregnancy with rates of neonatal abstinence syndrome. JAMA Netw Open. 2019;2(11):e1914078. doi:10.1001/jamanetworkopen.2019.14078
82. Poland ML, Dombrowski MP, Ager JW, Sokol RJ. Punishing pregnant drug users: enhancing the flight from care. Drug Alcohol Depend. 1993;31(3):199–203. doi:10.1016/0376-8716(93)90001-7
83. Mosley EA, Lanning RK. Evidence and guidelines for trauma-informed doula care. Midwifery. 2020;83:102643. doi:10.1016/j.midw.2020.102643
84. Gannon M, Short V, Becker M, et al. Doula engagement and maternal opioid use disorder (OUD): experiences of women in OUD recovery during the perinatal period. Midwifery. 2022;106:103243. doi:10.1016/j.midw.2021.103243
85. Allen L, Wodtke L, Hayward A, Read C, Cyr M, Cidro J. Pregnant and early parenting Indigenous women who use substances in Canada: a scoping review of health and social issues, supports, and strategies. J Ethn Subst Abuse. 2022;1–31. doi:10.1080/15332640.2022.2043799
86. Becker M, Gannon M. The impact of doula-supported care on stress levels of women receiving opioid addiction treatment. Phase 1 Pap 10; 2021. Available from: https://jdc.jefferson.edu/si_hs_2023_phase1/10.
87. Stubbs JL. Harm reduction throughout the opioid crisis: a community responds. Br Columbia Med J. 2019;2019:
88. Bosk EA, Paris R, Hanson KE, Ruisard D, Suchman NE. Innovations in child welfare interventions for caregivers with substance use disorders and their children. Child Youth Serv Rev. 2019;101:99–112. doi:10.1016/j.childyouth.2019.03.040
89. Marchand K, Beaumont S, Westfall J, et al. Conceptualizing patient-centered care for substance use disorder treatment: findings from a systematic scoping review. Subst Abuse Treat Prev Policy. 2019;14(1):37. doi:10.1186/s13011-019-0227-0
90. Pantridge CE, Charles VA, DeHart DD, et al. A qualitative study of the role of peer support specialists in substance use disorder treatment: examining the types of support provided. Alcohol Treat Q. 2016;34(3):337–353. doi:10.1080/07347324.2016.1182815
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.