Back to Journals » Journal of Pain Research » Volume 19
Intertransverse Process Block versus Erector Spinae Plane Block as Adjuncts to an Interpectoral Block for Breast Cancer Surgery: A Randomized Controlled Trial
Authors Samerchua A ![]() , Ditsatham C, Supphapipat K
, Ditsatham C, Supphapipat K ![]() , Konkarn N, Leurcharusmee P
, Konkarn N, Leurcharusmee P ![]() , Wongmaneerung P, Owaphakorn T, Prapussarakul K, Jinadech T, Wanvoharn M
, Wongmaneerung P, Owaphakorn T, Prapussarakul K, Jinadech T, Wanvoharn M
Received 5 November 2025
Accepted for publication 18 February 2026
Published 24 February 2026 Volume 2026:19 579089
DOI https://doi.org/10.2147/JPR.S579089
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jinlei Li
Artid Samerchua,1,* Chagkrit Ditsatham,2,3,* Kittitorn Supphapipat,1 Nichagoon Konkarn,1 Prangmalee Leurcharusmee,1 Phanchaporn Wongmaneerung,2,3 Thunsuda Owaphakorn,1 Kullaphun Prapussarakul,1 Thidarut Jinadech,1 Mullika Wanvoharn1
1Department of Anesthesiology, Faculty of Medicine, Chiang Mai University, Chiang Mai, 50200, Thailand; 2Division of Breast and Endocrine Surgery, Department of Surgery, Faculty of Medicine, Chiang Mai University, Chiang Mai, 50200, Thailand; 3Clinical Surgical Research, Faculty of Medicine, Chiang Mai University, Chiang Mai, 50200, Thailand
*These authors contributed equally to this work
Correspondence: Kittitorn Supphapipat, Department of Anesthesiology, Faculty of Medicine, Chiang Mai University, 110 Intavaroros Road, Muang, Chiang Mai, 50200, Thailand, Tel +66891920066, Email [email protected]
Purpose: This trial compared the efficacy of intertransverse process block (ITPB) with erector spinae plane block (ESPB), each in combination with an interpectoral block (IPB), with systemic analgesia for breast cancer surgery.
Patients and Methods: Ninety patients were randomized to ITPB/IPB, ESPB/IPB, or control under general anesthesia. The primary outcome was 24-hour morphine consumption. Secondary outcomes included intraoperative fentanyl use, numeric rating scale (NRS) pain scores, and recovery parameters. A 40% reduction in morphine consumption and a 2-point NRS decrease were prespecified as minimal clinically important differences (MCIDs). The IPB was applied equally in both intervention groups to reduce pectoral nerve-mediated pain.
Results: Median (IQR) 24-hour morphine use was 0 mg (0– 6), 3 mg (0– 4), and 6 mg (3– 6) in the ITPB/IPB, ESPB/IPB, and control groups, respectively. Morphine consumption did not differ between the ITPB/IPB and ESPB/IPB (median difference 0 mg; 95% CI 0 to 1; p = 0.275) but was lower in both groups compared with the control group (− 2.5 mg; 95% CI − 4 to 0; p = 0.014 and − 2.7 mg; 95% CI − 3 to 0; p = 0.003), exceeding the MCID despite modest absolute differences. Mean NRS pain scores were lower in both block groups than in the control group by approximately 1– 1.2 points across the postoperative period. Intraoperative fentanyl use and time to ambulation were significantly reduced in both groups compared with the control. ITPB required longer performance time (+3.4 minutes; 95% CI 1.9 to 5.0; p < 0.001).
Conclusion: Both ITPB/IPB and ESPB/IPB provided comparable and effective analgesia after breast cancer surgery. Given its shorter performance time, ESPB may be the more practical option. However, because the IPB constituted a shared analgesic component in both groups, the independent analgesic effects of ITPB and ESPB remain uncertain and warrant further investigation.
Keywords: analgesia, anesthesia, local, pain, postoperative, regional anesthesia
Introduction
Breast cancer surgery (BCS) is frequently associated with significant postoperative pain.1 Inadequate analgesia can lead to increased opioid use and a higher risk of opioid-related adverse effects. It can also delay recovery and increase the risk of developing chronic postsurgical pain (CPSP).2 In modern anesthesia practice, regional analgesia represents a key component of multimodal strategies for BCS.3,4 Various thoracic regional techniques have been shown to reduce pain, speed recovery, and potentially mitigate the risk of CPSP.5
In 2020, the Procedure-Specific Postoperative Pain Management (PROSPECT) guidelines recommended thoracic paravertebral block (PVB) as the first-line regional technique for major BCS, with PECS-II (a combination of the interpectoral block [IPB] and the pectoserratus plane block) as a second-line alternative, while the erector spinae plane block (ESPB) was not recommended due to limited evidence.3 A recent Cochrane network meta-analysis, however, reported that PVB, PECS-II, and ESPB provide broadly similar analgesic effectiveness up to 48 hours postoperatively, with only small clinically significant differences between techniques; ESPB appeared generally comparable to PVB in this context.4
Despite these findings, concerns remain regarding PVB, which carries risks of pneumothorax, neuraxial injury, technical difficulty, and block failure,6 whereas the pectoserratus plane block may cause undesired axillary spread of local anesthetic (LA).7 These limitations have prompted increasing interest in posterior truncal interfascial plane blocks, including ESPB and the intertransverse process block (ITPB), as potentially safer and more accessible alternatives.5,8
ESPB involves injection deep into the erector spinae muscle and relies on the anterior spread of LA toward the paravertebral space; however, anatomical and imaging studies suggest that this anterior diffusion may be variable and influenced by technical and anatomical factors.9,10 In contrast, ITPB targets the deeper intertransverse tissue complex adjacent to the superior costotransverse ligament, which may provide a more direct anatomical pathway for anterior spread into the paravertebral space.9 A multi-injection ITPB technique has been proposed to enhance anterior and cephalocaudal distribution and to improve the consistency of ventral rami blockade, potentially resulting in broader and more reliable anterior chest wall coverage compared with single-injection ESPB.11,12
The IPB, which anesthetizes the medial and lateral pectoral nerves, can further enhance analgesia for BCS and is increasingly incorporated into multimodal regional anesthesia strategies.3,5 When combined with posterior truncal blocks, IPB may improve analgesia related to pectoral muscle manipulation and breast tissue dissection.8 Nevertheless, clinical evidence demonstrating a consistent additive analgesic benefit of combining ESPB or ITPB with IPB remains limited.
Accordingly, this triple-arm randomized controlled trial aimed to compare the analgesic efficacy of ITPB/IPB and ESPB/IPB with systemic analgesia in patients undergoing BCS. The IPB was applied equally in both intervention groups to reduce pectoral nerve-mediated pain. The primary outcome was cumulative 24-hour morphine consumption. Secondary outcomes included intraoperative fentanyl use, postoperative pain scores, recovery parameters, and patient satisfaction.
Materials and Methods
Study Design
This single-center, randomized controlled trial was approved by the Research Ethics Committee of the Faculty of Medicine, Chiang Mai University (ANE-2565-08993) on August 31, 2022, and was registered with the Thai Clinical Trials Registry (TCTR20230103005) on December 23, 2022. The first patient was enrolled on January 10, 2023. Written informed consent was obtained from all participants before enrollment. This manuscript adheres to the Consolidated Standards of Reporting Trials (CONSORT) guidelines for randomized trials.
Female patients aged 20–65 years with an American Society of Anesthesiologists (ASA) physical status I–II scheduled for unilateral primary BCS were screened for eligibility. Exclusion criteria included body weight <40 kg, morbid obesity (BMI >40 kg/m2), contraindications to regional anesthesia (eg, drug allergy, local or systemic infection, or coagulopathy), pre-existing neurological deficits of the chest wall, chronic opioid use, hepatic or renal failure, and pregnancy.
Patient Grouping and Randomization
Upon arrival in the operating room an attending anesthesiologist, blinded to group allocation, supervised anesthesia induction. All patients received general anesthesia (GA) with propofol 2–3 mg/kg, fentanyl 1 µg/kg, and cisatracurium 0.12 mg/kg, followed by tracheal intubation. Anesthesia was maintained with sevoflurane to achieve a minimum alveolar concentration of 0.7–1.0. Once the condition of the patient was stable, the attending anesthesiologist exited the operating room, and the regional anesthesia team assumed care.
Participants were randomly assigned to receive ITPB + IPB (ITPB/IPB), ESPB + IPB (ESPB/IPB), or systemic analgesia alone. Group allocation was determined using a computer-generated randomization sequence (1:1:1 ratio) concealed in opaque, sealed envelopes, which were opened immediately before block performance. All blocks were performed by two regional anesthesiologists (AS and PrL), who were not blinded to group allocation. Patients, surgeons, attending anesthesiologists, and outcome assessors remained blinded to treatment allocation throughout the perioperative period.
Intervention and Comparator Groups
In the ITPB/IPB group, the ITPB was performed under sterile conditions with the patient in the lateral position, surgical side uppermost. A high-frequency linear ultrasound transducer (L11–3, SONIMAGE® HS1, Konica Minolta, Japan) was placed parasagittally at the T3–4 intertransverse level, identified by counting the ribs in the cephalad-to-caudad and lateral-to-medial directions. The probe was tilted slightly laterally and obliquely to visualize the retro–superior costotransverse ligament (SCTL) space, paravertebral space, and pleura. Using an in-plane lateral-to-medial approach, a 22-gauge, 80-mm needle (B. Braun Medical AG, Melsungen, Germany) was advanced to just superficial to the SCTL.13 Correct placement was confirmed by pleural displacement following a 1–2 mL saline test injection, after which 0.15 mL/kg of LA mixture (0.25% bupivacaine with 1% lidocaine and epinephrine 10 µg/mL) was injected. The same procedure was repeated at T4–5 and T5–6, for a total LA volume of 0.45 mL/kg.
In the ESPB/IPB group, the ESPB was performed after identifying the T4–5 level in the parasagittal plane at the base of the T4 transverse process. The needle was then advanced in a caudal-to-cephalad direction through the erector spinae muscle until its tip lay deep to the fascia. Proper placement was confirmed by injection of 1–2 mL saline to lift the erector spinae muscle off the transverse process, followed by administration of 0.45 mL/kg of the same LA mixture.
Following ITPB or ESPB, patients were turned supine with the arm abducted for the IPB. The ultrasound probe was positioned below the lateral third of the clavicle to identify the third rib and the interpectoral plane between the pectoralis major and minor muscles, along with the pectoral branch of the thoracoacromial artery. Using an in-plane cephalad-to-caudad approach, the needle was advanced into the interfascial plane, and 0.15 mL/kg of the LA mixture was injected.
In the systemic analgesia (control) group, no regional block was performed. In all groups, patients were prepped and draped to conceal the injection sites for blinding. The attending anesthesiologist then resumed intraoperative management. Standard surgical procedures for BCS were performed by the same surgical team according to the clinical indication.
Intraoperative and Postoperative Care
Intraoperatively, intravenous fentanyl (25–50 µg) was administered as needed when heart rate or systolic blood pressure increased by more than 20% from baseline. All patients received intravenous acetaminophen 1000 mg, dexamethasone 8 mg, and ondansetron 0.1 mg/kg. Intraoperative hypotension was treated with fluid resuscitation or intravenous ephedrine or phenylephrine, and bradycardia was managed with intravenous atropine as appropriate. Postoperatively, morphine 0.06 mg/kg IV was administered every 15 minutes in the post-anesthesia care unit (PACU) for numeric rating scale (NRS) pain scores > 4, and hourly as needed on the ward. Oral Codigesic® (codeine 15 mg + acetaminophen 500 mg) was given every 8 hours for three days. Intravenous metoclopramide 10 mg was administered as needed for postoperative nausea and vomiting (PONV). Nonsteroidal anti-inflammatory drugs (NSAIDs) were intentionally withheld in all study groups to standardize perioperative analgesic management.
Outcome Measurements
The primary outcome was cumulative postoperative morphine consumption over 24 hours. Secondary outcomes included: 1) Block performance time for the ITPB and ESPB (measured from probe placement to completion of LA injection), and block-related complications (bleeding, hematoma, pneumothorax, or LA toxicity), recorded by a non-blinded operator; 2) Intraoperative fentanyl consumption, documented by the attending anesthesiologist; and 3) Postoperative outcomes, including NRS pain scores at 0 (PACU), 1, 6, 12, 24, 36, and 48 hours. Pain intensity was categorized as mild (NRS 0–3), moderate (4–6), or severe (7–10). Analgesia-related adverse events, postoperative time to ambulation and time to void, incidence of PONV, and patient satisfaction (0 = none, 10 = most satisfied) at 48 hours were also recorded. All postoperative assessments were performed by a blinded assessor.
Sensory block assessment was conducted one hour after arrival in the PACU using a cold sensation test with an ice pack, evaluating dermatomes T2–T8 from the parasternal line to the anterior axillary line. The number of dermatomes with reduced cold sensation compared with the contralateral side was recorded.
Pain burden was evaluated at 2 weeks after surgery using the Pain Burden Index (PBI) described by Gärtner et al.14 The PBI was calculated by summing the product of pain severity (0–10) and frequency (0–5) across four regions: breast, axilla, chest wall, and arm, yielding a total score of 0–200, with higher scores indicating greater pain burden. A follow-up assessment was conducted via telephone by a blinded assessor.
Statistical Analyses
Statistical analyses were performed using Stata version 16.0 (StataCorp, 2019). Continuous variables are presented as mean (standard deviation, SD) or median (interquartile range, IQR), and categorical variables as counts (%). Categorical variables were compared using Fisher’s exact test. Continuous variables were analyzed using one-way ANOVA for normally distributed data and the Kruskal–Wallis test for non-normal data, with pairwise comparisons assessed by Dunn’s post hoc test. Median differences with 95% confidence intervals (CIs) were estimated using the Hodges–Lehmann method. Postoperative NRS scores were analyzed using two-way repeated-measures ANOVA. The proportions of patients with moderate-to-severe pain and PONV were compared using Fisher’s exact test; absolute risk reductions (ARRs) with 95% CIs were estimated from a logistic model using marginal predicted probabilities. Bonferroni adjustment was applied to all pairwise comparisons. All analyses followed the intention-to-treat principle, with p < 0.05 considered statistically significant.
For clinical interpretation, relative reductions in 24-hour morphine consumption and NRS scores were also assessed. The minimal clinically important difference (MCID) was prespecified as a 40% reduction in 24-hour morphine consumption and a 2-point reduction in NRS pain scores.15
Sample Size
The sample size was calculated using Stata version 16.0 (StataCorp, 2019) based on a previous trial which reported that 24-hour morphine consumption was 5.1 ± 3.3 mg lower with PVB than with ESPB (3.5 ± 3.3 mg vs 8.6 ± 3.8 mg; p < 0.001).16 Although no studies had directly compared ITPB and ESPB at that time, this variance estimate was used for planning. We hypothesized that ITPB combined with an IPB would provide superior analgesia compared with ESPB in combination with IPB and with the control group, achieving at least a 40% reduction in 24-hour morphine consumption, which was considered the MCID. Assuming equal group allocation (ITPB/IPB, ESPB/IPB, and control) and applying a Bonferroni-adjusted two-sided alpha of 0.0167 for three pairwise comparisons, 20 participants per group were required to achieve 80% power for the primary comparison (ITPB/IPB vs ESPB/IPB). To allow for secondary analyses and possible attrition, 30 patients were enrolled per group, giving a total sample size of 90.
Results
Baseline Characteristics
A total of 95 patients were assessed for eligibility, of whom 5 were excluded due to lack of consent. The remaining 90 patients were enrolled and randomly assigned to the intervention or comparator arms. One patient was subsequently excluded due to a change in the planned operation. Ultimately, 30 patients were randomized to the ITPB/IPB group, 30 to the ESPB/IPB group, and 29 to the control group (Figure 1). All participants received their allocated intervention and were included in the intention-to-treat analysis for both primary and secondary outcomes. Baseline patient characteristics and surgical procedures were similar among the three groups (Table 1).
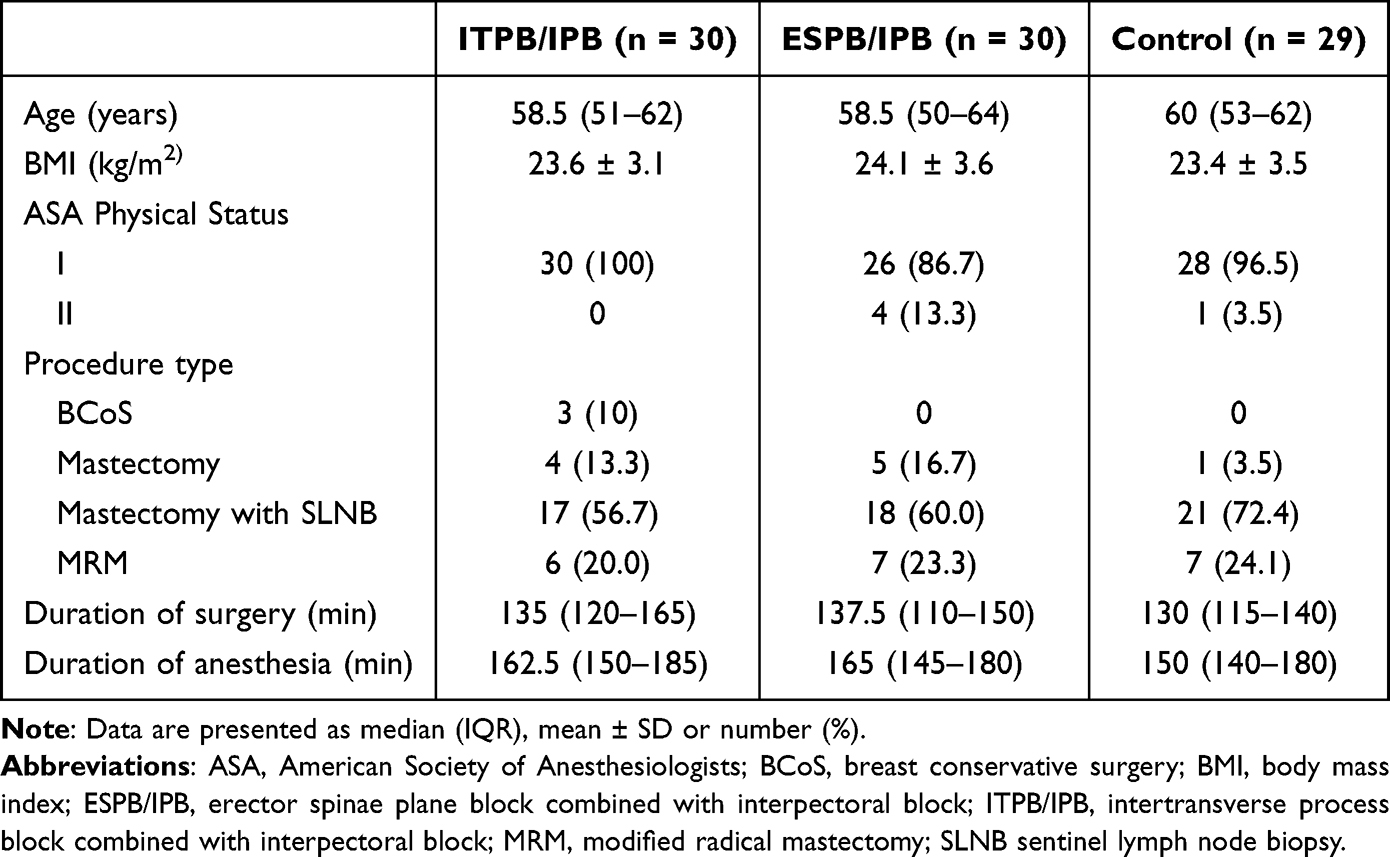 |
Table 1 Patient Characteristics |
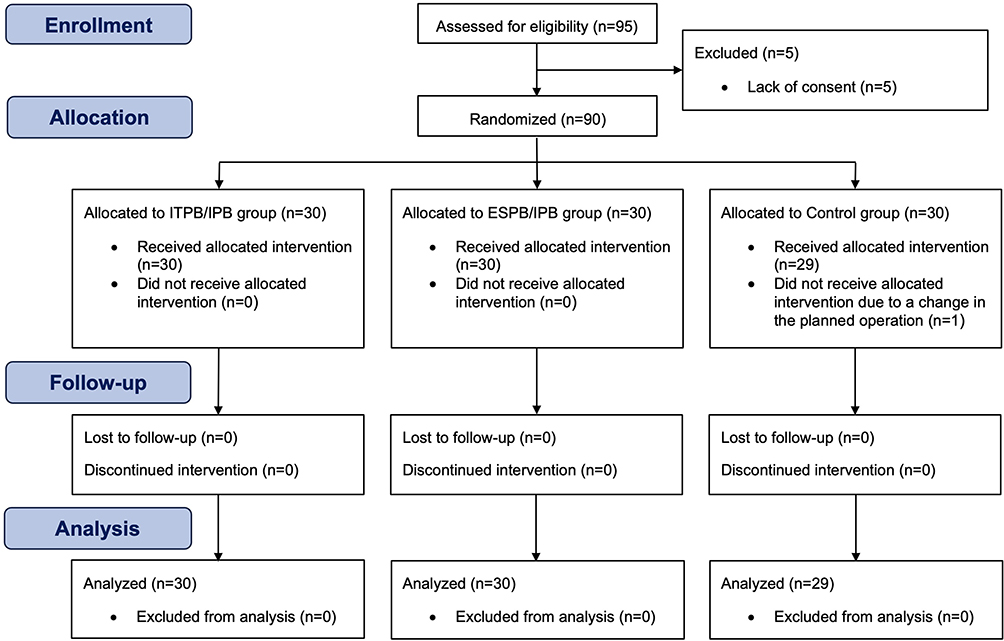 |
Figure 1 CONSORT diagram of the study. |
Primary Outcome
Median (IQR) 24-hour morphine use was 0 mg (0–6) in the ITPB/IPB group, 3 mg (0–4) in the ESPB/IPB group, and 6 mg (3–6) in the control group (Table 2). The pairwise comparison between ITPB/IPB and ESPB/IPB showed a median difference of 0 mg (95% CI, 0 to 1; p = 0.275), indicating no statistically significant difference between the two groups. In comparison with the control group, both block groups showed significantly lower 24-hour morphine use: ITPB/IPB vs control −2.5 mg (95% CI, −4 to 0; p = 0.014) and ESPB/IPB vs control −2.7 mg (95% CI, −3 to 0; p = 0.003). Based on the prespecified MCID (percentage reduction from the control median of 6 mg), these correspond to approximately 100% for ITPB/IPB and 50% for ESPB/IPB, both exceeding the 40% MCID threshold.
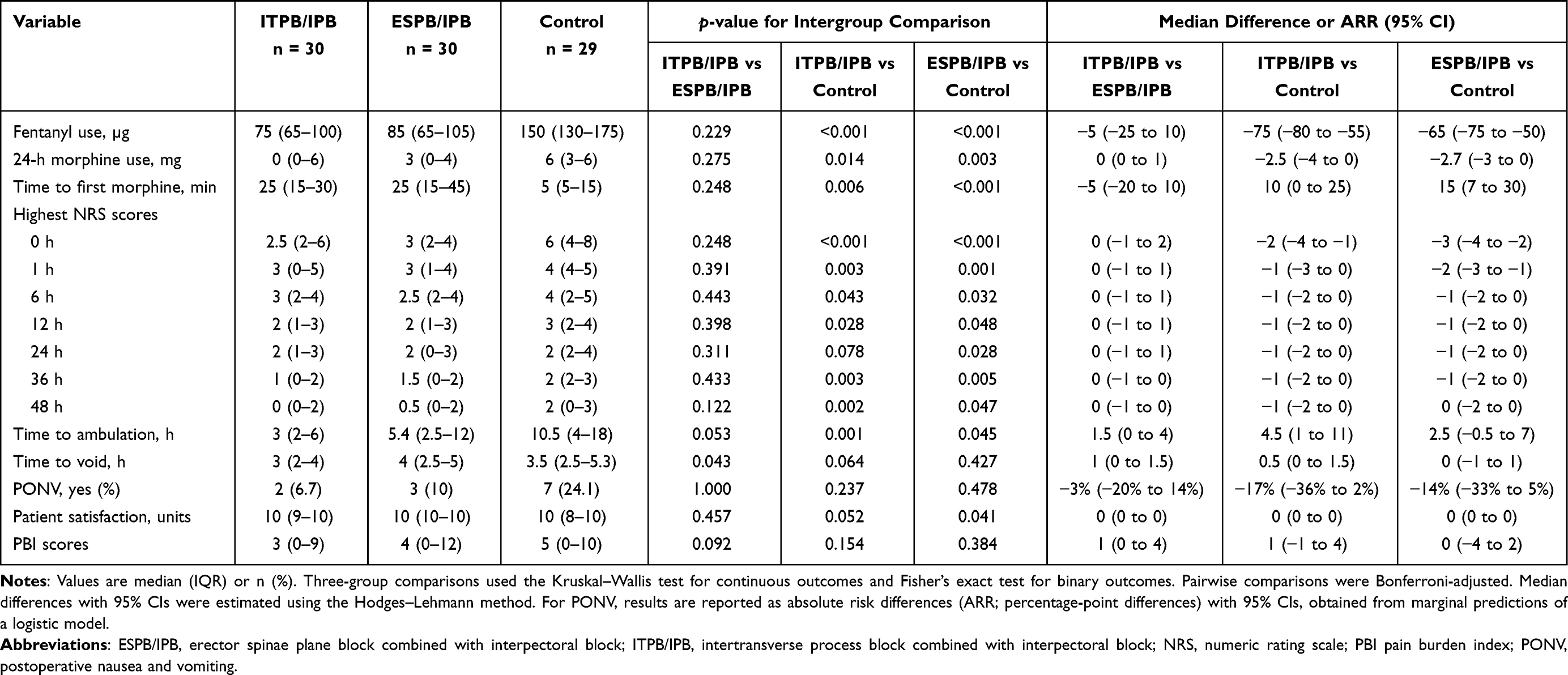 |
Table 2 Outcomes |
Secondary Outcomes
As shown in Table 2, significantly reduced intraoperative fentanyl use was reported in both the ITPB/IPB and ESPB/IPB groups in comparison to controls, with median differences of −75 µg (95% CI, −80 to −55; p < 0.001) and −65 µg (95% CI, −75 to −50; p < 0.001), respectively. No significant difference was observed between ITPB/IPB and ESPB/IPB. Although the time to first postoperative morphine requirement did not differ between the two block groups, both significantly prolonged this interval compared with the control group by 10 minutes for ITPB/IPB and 15 minutes for ESPB/IPB. No patients in any group required intravenous morphine beyond 24 hours postoperatively.
Significantly reduced NRS pain scores were recorded in both ITPB/IPB and ESPB/IPB groups in comparison with the control group at most time points up to 36 hours, although clinically meaningful reductions (≥ 2 points) were only observed during the first postoperative hour (Table 2). Repeated-measures ANOVA showed no significant group × time interaction (p = 0.067) (Figure 2), indicating that pain scores followed a similar temporal trend across groups. Post hoc analysis confirmed lower mean pain scores for ITPB/IPB (−1.23; 95% CI, −1.66 to −0.80; p < 0.001) and ESPB/IPB (−1.15; 95% CI, −1.58 to −0.72; p < 0.001) compared with control, with no difference recorded between ITPB/IPB and ESPB/IPB groups (0.08; 95% CI, −0.35 to 0.50; p = 1.000).
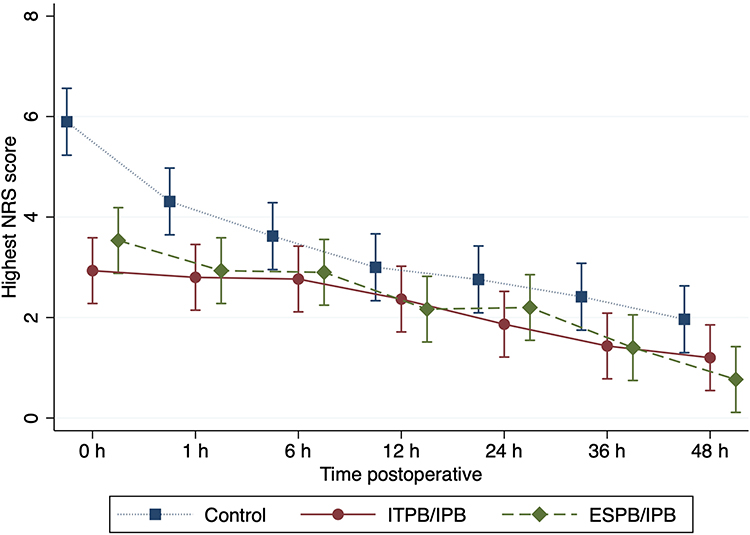 |
Figure 2 Postoperative pain intensity over time. |
Consistent with these findings, moderate-to-severe pain was less frequent in the block groups, affecting approximately one-third of patients early postoperatively compared with nearly three-quarters in the control group (Figure 3 and Table 3). Over 0–48 hours, the ARR for moderate-to-severe pain was 24.1% for ITPB/IPB (95% CI, 8.3%–39.8%; p = 0.001) and 25.7% for ESPB/IPB (95% CI, 10.2%–41.3%; p < 0.001) compared with control. No significant difference was found between ITPB/IPB and ESPB/IPB (ARR −1.7%, 95% CI, −15.4% to 12.1%; p = 1.000).
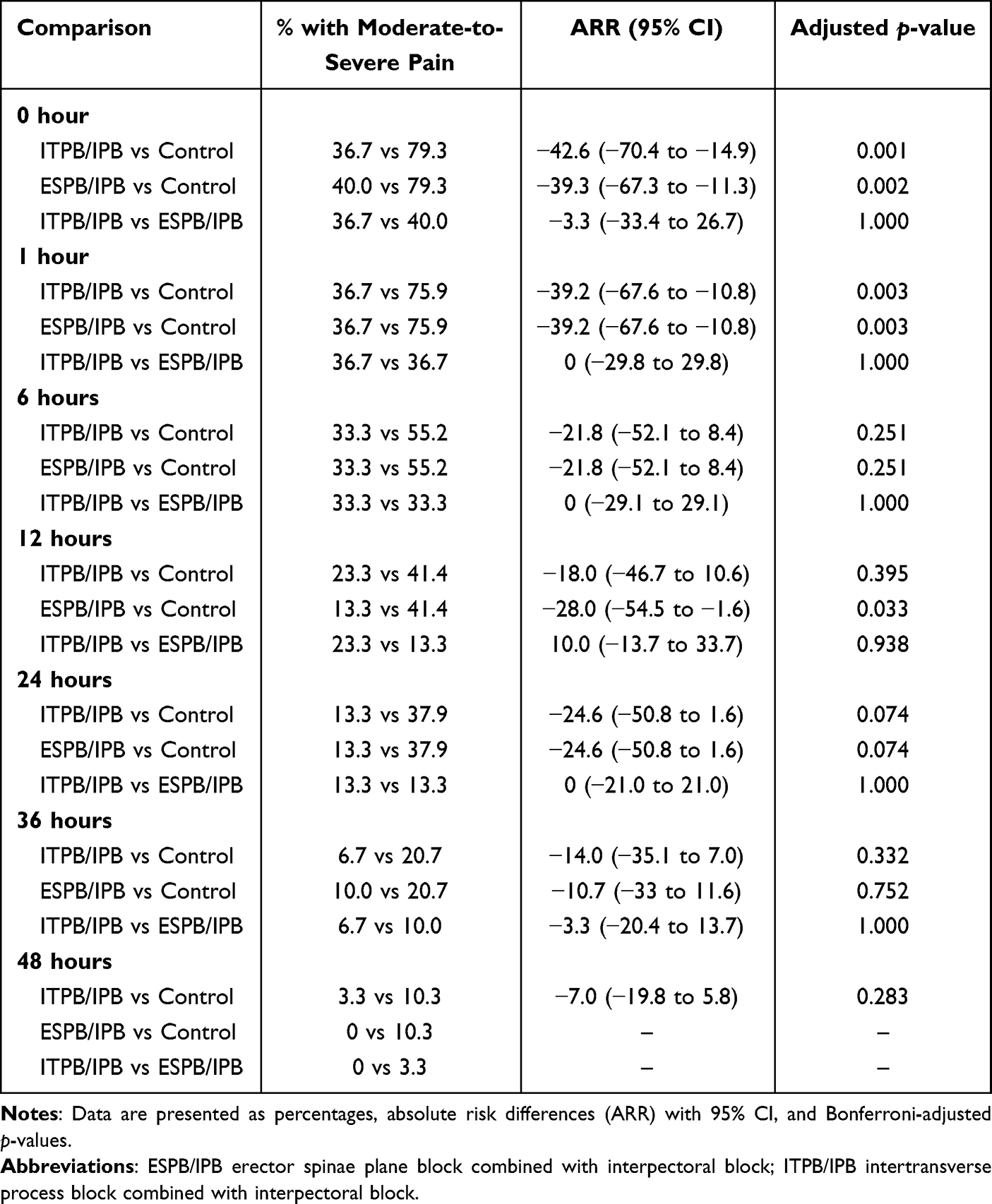 |
Table 3 Proportion of Patients with Moderate-to-Severe Pain Over 0–48 hours |
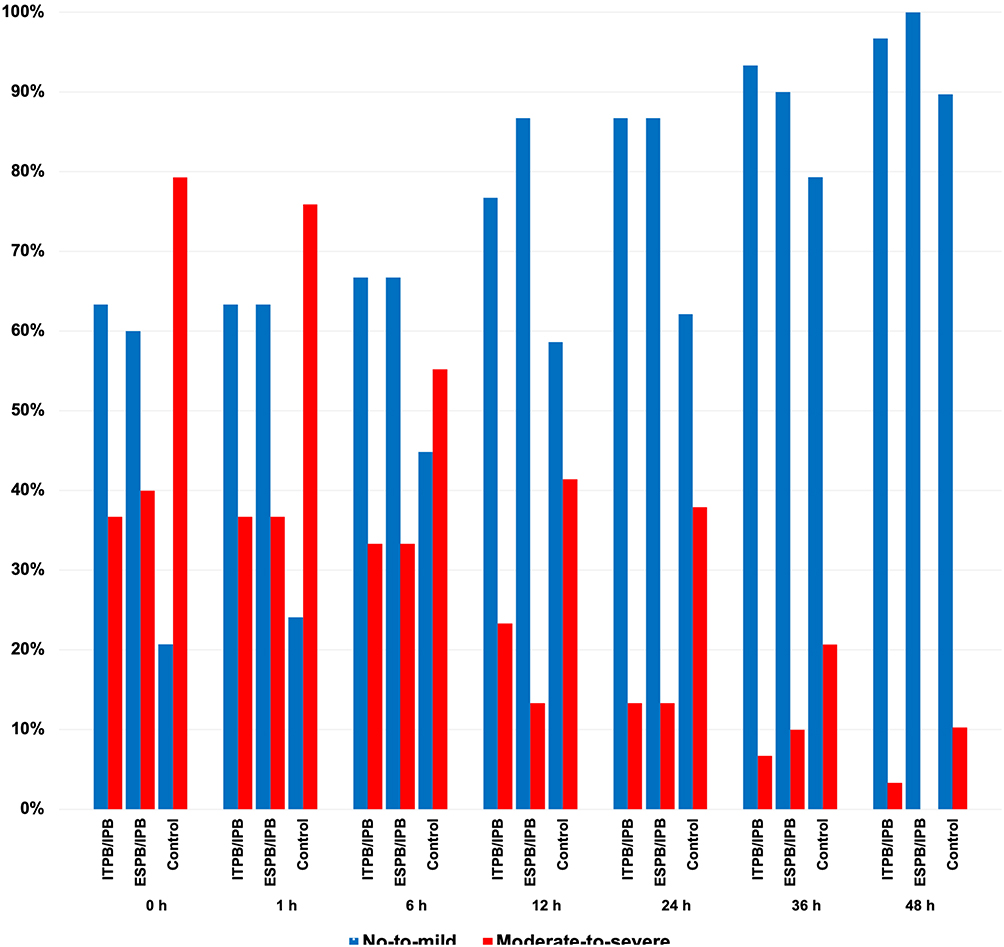 |
Figure 3 Proportion of patients reporting no-to-mild and moderate-to-severe pain at each postoperative time point across study groups. |
Time to ambulation was 4.5 hours shorter with ITPB/IPB than with control and 2.5 hours shorter with ESPB/IPB than with control, with both differences reaching statistical significance. The incidence of PONV did not differ between groups. Patient satisfaction was high, and PBI scores were low and comparable across all groups (Table 2).
The ITPB had a longer median (IQR) block performance time than the ESPB [9.0 (7.5–11.0) min vs 5.3 (3.4–8.1) min; median difference, 3.4 min; 95% CI, 1.9–5.0 min; p < 0.001]. No block-related complications were observed in either group. The ITPB/IPB group had a median (IQR) of 5 (4–6) blocked dermatomes across the anterior hemithorax (T2–T7), compared with 4 (4–5) in the ESPB/IPB group, with a median difference of 0 (95% CI, –1 to 0; p = 0.302). The distribution of blocked dermatomes is presented in Table 4. Sensory loss did not extend beyond T8, and no bilateral blockade occurred in either block group. No sensory loss was detected in the control group.
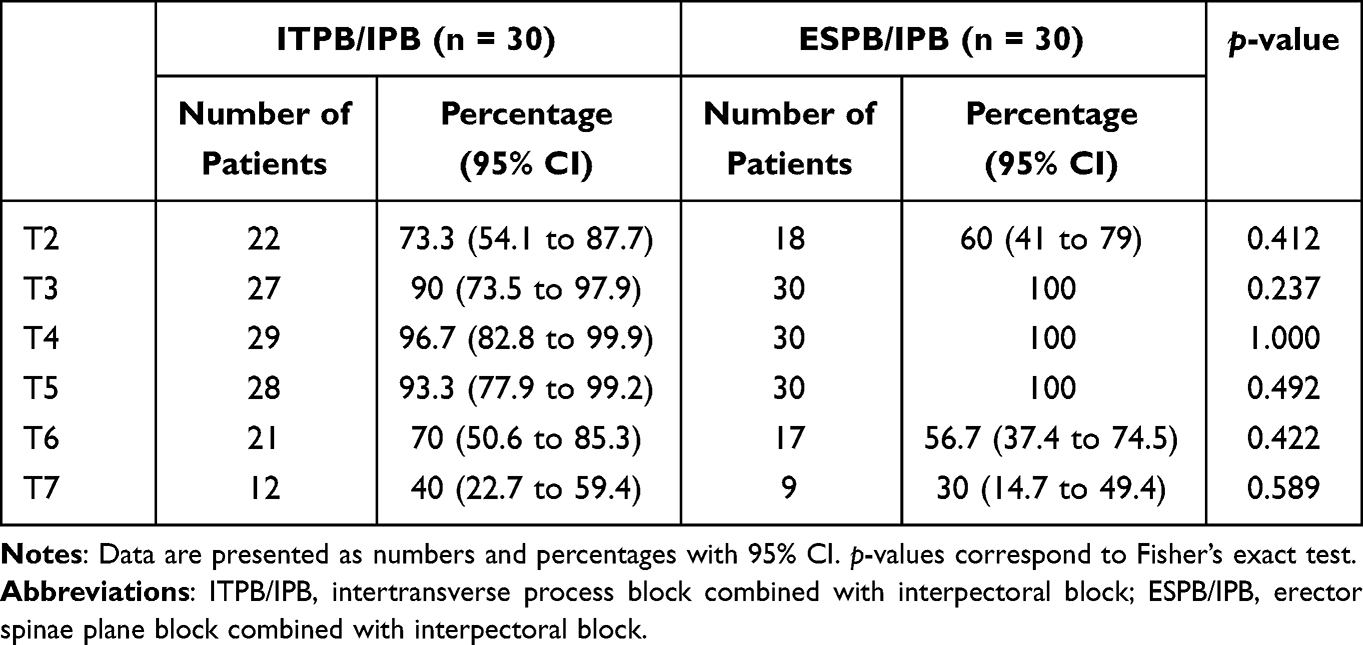 |
Table 4 Sensory Block Distribution of the Anterior Chest Wall |
Discussion
The trial was powered to detect a 40% reduction in 24-hour morphine consumption for ITPB/IPB and ESPB/IPB relative to control; however, no statistically or clinically significant difference was observed between the two techniques, suggesting comparable opioid-sparing efficacy. Nevertheless, significantly reduced morphine consumption was recorded in both experimental groups compared with systemic analgesia, exceeding the predefined 40% MCID threshold for clinical relevance. These findings suggest that ITPB and ESPB offer comparable analgesic efficacy when combined with an IPB and represent effective components of multimodal analgesia for BCS.
The ITPB and ESPB techniques primarily target the ventral rami or thoracic intercostal nerves, which provide the main sensory innervation to the breast.5,8,9 In our study, the IPB was incorporated into both intervention groups, as we speculated that it could enhance perioperative analgesia following BCS. The IPB blocks the medial and lateral pectoral nerves, which are particularly useful in mastectomy and submuscular breast augmentation.5,17 Blocking of these nerves could augment the surgical anesthesia achieved with a PVB in primary BCS.18 Furthermore, anatomical studies have demonstrated that the IPB can also involve the intercostal nerves (T3–T6), thereby enhancing the efficacy of both ITPB and ESPB.17 In addition, spread to the long thoracic and thoracodorsal nerves has been reported, which may provide additional benefit in patients undergoing axillary lymph node dissection.5,17
The ITPB is a novel thoracic nerve block technique in which LA is injected into the retro-SCTL space between two adjacent transverse processes.8 The injected LA may spread anteriorly through the intertransverse tissue complex into the paravertebral space, medially into the epidural space and intervertebral foramen, laterally into the intercostal space, posteriorly into the erector spinae plane, and cephalocaudally through the costotransverse space.10 Several technical variations of ITPB have been described, differing in the number (single or multiple) and location of injections, with reported sites including the midpoint between the transverse process and pleura, the junction of the SCTL and transverse process, the costotransverse foramen, or immediately posterior to the SCTL.8 Although no standardized technique has been established, we adopted a triple-injection approach immediately posterior to the SCTL, which has been shown to reliably anesthetize the ipsilateral thoracic dermatomes and has been anatomically validated to provide consistent spread into the paravertebral space.11,19–21
To date, evidence regarding the analgesic efficacy of the ITPB in BCS remains limited and inconsistent. Reported findings include the superiority of ITPB over systemic analgesia,22 equivalence with systemic analgesia,13 and comparable efficacy to PVB.21,23 In a randomized trial, Sethi et al24 found comparable early analgesia between ITPB and ESPB, each performed with a single 15-mL injection of LA followed by an infusion at 5 mL/h. However, ITPB was associated with higher pain scores over the subsequent 24 hours after BCS, possibly due to inconsistent cephalocaudal spread of LA.24,25 Conversely, Qian et al12 demonstrated that a multi-injection ITPB technique produced broader anterior thoracic coverage and better early analgesia than single-injection ESPB, likely due to more reliable anterior spread achieved with multiple injections in ITPB.
In contrast, the result of our study demonstrated comparable anterior thoracic sensory blockade and postoperative analgesia between ITPB/IPB and ESPB/IPB. We speculate that the effective analgesia observed with ESPB in our study may be attributable to technical differences in injection site. Unlike Qian et al12 who injected at the tip of the transverse process, we performed ESPB at the base of the transverse process (paralaminar plane), which is closer to the medial slip of the SCTL and the costotransverse foramen, and may have facilitated the anterior spread of LA into the paravertebral space.26,27
The analgesic efficacy of ESPB for BCS remains controversial. A meta-analysis found comparable postoperative pain scores and opioid consumption between ESPB and PVB,28 whereas a large randomized trial reported higher morphine use with ESPB despite similar pain scores.29 In comparison with systemic analgesia, ESPB may also provide limited clinical benefit, as its effects did not exceed the absolute MCID thresholds of 10 mg IV morphine or 1.1 cm on the NRS.30 To better capture potential benefits of ESPB, Sorenson et al15 recently advocated for relative thresholds, such as a 40% reduction in opioid consumption or a two-point decrease in pain score, as more appropriate indicators of clinical relevance.
In our trial, both block groups resulted in clinically meaningful pain reductions during the first postoperative hour, surpassing the 1- and 2-point MCID thresholds, although the benefit decreased to about 1 NRS point after 6 hours. Throughout the postoperative period, mean pain scores were approximately 1.2 points lower in the block groups than in the control group, exceeding the 1-point MCID and approaching the 2-point threshold, which highlights the overall analgesic benefit of the regional block techniques used in our study.15
In addition, both block groups demonstrated reduced 24-hour morphine consumption compared with the control group. Although the absolute opioid-sparing effect (2–3 mg IV morphine) did not meet the 10-mg benchmark30 it exceeded our predefined 40% threshold, supporting its clinical relevance. This modest absolute reduction is consistent with existing evidence, which suggests reductions of approximately 6 mg and 5 mg of IV morphine equivalents with ESPB and pectoral nerve blocks, respectively, compared with control.30,31 In this context, the approximately 3 mg reduction observed in our study falls within the expected range of opioid-sparing effects, particularly in a setting where baseline opioid requirements are low. The higher intraoperative fentanyl use and earlier administration of morphine in the PACU observed in the control group likely contributed to the modest between-group differences in 24-hour opioid consumption.
Moderate-to-severe pain is common after BCS, affecting nearly half of patients within the first postoperative day.32 Truncal regional blocks reduced this burden, with only 28% of patients reporting moderate-to-severe pain at 2 hours compared with 49% without a block.1 Consistent with prior studies, both ITPB and ESPB in combination with IPB provided strong early analgesia, with ~40% fewer patients experiencing moderate-to-severe pain at 0–1 h versus controls. Over 48 hours, both blocks achieved an ARR of 24–25% (Number needed to treat ~4), demonstrating clinically meaningful analgesic benefits.33 However, the relatively high incidence of moderate-to-severe pain observed in our study may be partly attributed to withholding NSAIDs in all cases to maintain treatment uniformity and to minimize the risk of adverse effects such as renal impairment, gastrointestinal irritation, or allergic reactions. This approach may have increased overall pain intensity and influenced the magnitude of the observed analgesic effects. At 2 weeks, low PBI values indicated a mild overall pain burden and may reflect a lower risk of CPSP.2 The uniformly low PBI scores across groups suggest favorable pain resolution and highlight the importance of effective early multimodal analgesia in minimizing CPSP risk.2,34
Both ITPB/IPB and ESPB/IPB resulted in a significantly reduced intraoperative fentanyl requirement in comparison with the control group, confirming effective intraoperative analgesia and opioid-sparing properties. In addition, faster postoperative recovery was recorded in both block groups, as demonstrated by significantly shorter ambulation times. These results are consistent with previous studies which reported that ITPB and ESPB facilitate recovery after BCS.35,36 Given its shorter performance time and requirement for only a single, more superficial needle puncture, ESPB may be the more practical option for clinical use.
Our study has several limitations. First, because both intervention groups intentionally received an IPB to minimize confounding related to pectoral nerve-mediated pain, the isolated comparative analgesic effects of ITPB and ESPB could not be determined. Second, all types of BCS were included, so the effectiveness of each block regimen for specific procedures could not be fully assessed. Third, postoperative recovery metrics such as the Quality of Recovery-15 were not evaluated; hence, overall recovery quality could not be comprehensively assessed. Fourth, our study assessed only acute and subacute outcomes, and the potential effects of these blocks on the development of CPSP were not investigated. Further studies with longer follow-up and procedure-specific designs are warranted. Finally, the study was powered for the primary comparison between ITPB/IPB and ESPB/IPB, whereas comparisons with the control group were secondary and may be underpowered. These findings should therefore be interpreted cautiously and confirmed in larger trials.
Conclusion
When combined with an IPB, both ITPB and ESPB provided comparable and effective analgesia after breast cancer surgery. Because the IPB was used in both intervention groups, this study cannot determine the individual analgesic contribution of the ITPB and ESPB or the additional benefit provided by the IPB itself. Instead, the findings reflect the relative performance of the two posterior truncal block techniques within a multimodal regional anesthesia approach and highlight the need for further studies to clarify their independent effects. Although analgesic efficacy was similar, ESPB required a shorter performance time and may offer practical advantages related to technical simplicity, ease of workflow integration, and broader applicability across institutions with varying levels of regional anesthesia expertise.
Data Sharing Statement
The datasets from this study are available from the corresponding authors upon reasonable request.
Ethics Statement
This study was approved by the Research Ethics Committee of the Faculty of Medicine, Chiang Mai University (Approved number: ANE-2565-08993) on August 31, 2022, and was conducted in accordance with the Helsinki Declaration and its later amendments.
Acknowledgment
The authors wish to acknowledge the assistance of the Research Administration Section, Faculty of Medicine, Chiang Mai University. ChatGPT-4.0 (OpenAI, San Francisco, CA, USA) was used for language editing during manuscript preparation. After using this service, the authors reviewed and revised the content as necessary and take full responsibility for the content of the published article. This study received no funding.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Zinboonyahgoon N, Vlassakov K, Lirk P, et al. Benefit of regional anaesthesia on postoperative pain following mastectomy: the influence of catastrophising. Br J Anaesth. 2019;123(2):e293–13. doi:10.1016/j.bja.2019.01.041
2. Andersen KG, Duriaud HM, Jensen HE, Kroman N, Kehlet H. Predictive factors for the development of persistent pain after breast cancer surgery. Pain. 2015;156(12):2413–2422. doi:10.1097/j.pain.0000000000000298
3. Jacobs A, Lemoine A, Joshi GP, Van de Velde M, Bonnet F. PROSPECT guideline for oncological breast surgery: a systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2020;75(5):664–673. doi:10.1111/anae.14964
4. Clephas PR, Orbach-Zinger S, Gosteli-Peter MA, et al. Regional analgesia techniques for postoperative pain after breast cancer surgery: a network meta-analysis. Cochrane Database Syst Rev. 2025;6(6):Cd014818. doi:10.1002/14651858.CD014818.pub2
5. Woodworth GE, Ivie RMJ, Nelson SM, Walker CM, Maniker RB. Perioperative breast analgesia: a qualitative review of anatomy and regional techniques. Reg Anesth Pain Med. 2017;42(5):609–631. doi:10.1097/aap.0000000000000641
6. Nair S, Gallagher H, Conlon N. Paravertebral blocks and novel alternatives. Bja Educ. 2020;20(5):158–165. doi:10.1016/j.bjae.2020.01.006
7. Kim DH, Kim S, Kim CS, et al. Efficacy of pectoral nerve block type II for breast-conserving surgery and sentinel lymph node biopsy: a prospective randomized controlled study. Pain Res Manag. 2018;2018:4315931. doi:10.1155/2018/4315931
8. Yu X, Liu C. Intertransverse process block: a narrative review. J Clin Anesth. 2025;104:111857. doi:10.1016/j.jclinane.2025.111857
9. Varela V, Ruíz C, Montecinos S, Prats-Galino A, Sala-Blanch X. Spread of local anesthetic injected in the paravertebral space, intertransverse processes space, and erector spinae plane: a cadaveric model. Reg Anesth Pain Med. 2024;49(3):228–232. doi:10.1136/rapm-2023-104342
10. Sivakumar RK, Karmakar MK. Variable anterior spread of local anesthetic after erector spinae plane block (ESPB): time to turn the spotlight on the ‘retro-SCTL space’. Reg Anesth Pain Med. 2023;48(9):483–484. doi:10.1136/rapm-2023-104362
11. Nielsen MV, Moriggl B, Hoermann R, Nielsen TD, Bendtsen TF, Børglum J. Are single-injection erector spinae plane block and multiple-injection costotransverse block equivalent to thoracic paravertebral block? Acta Anaesthesiol Scand. 2019;63(9):1231–1238. doi:10.1111/aas.13424
12. Qian L, Zhang H, Miao Y, et al. Comparison between ultrasound-guided intertransverse process and erector spinae plane blocks for breast cancer surgery: a randomised controlled trial. Eur J Anaesthesiol. 2025;42(3):224–232. doi:10.1097/eja.0000000000002091
13. Nielsen MV, Tanggaard K, Hansen LB, Hansen CK, Vazin M, Børglum J. Insignificant influence of the intertransverse process block for major breast cancer surgery: a randomized, blinded, placebo-controlled, clinical trial. Reg Anesth Pain Med. 2024;49(1):10–16. doi:10.1136/rapm-2023-104479
14. Gärtner R, Jensen MB, Nielsen J, Ewertz M, Kroman N, Kehlet H. Prevalence of and factors associated with persistent pain following breast cancer surgery. JAMA. 2009;302(18):1985–1992. doi:10.1001/jama.2009.1568
15. Sorenson S, Flyger SSB, Pingel L, et al. Primary outcomes and anticipated effect sizes in randomised clinical trials assessing peripheral and truncal nerve blocks: a systematic scoping review. Br J Anaesth. 2025;134(2):535–544. doi:10.1016/j.bja.2024.09.029
16. Wittayapairoj A, Sinthuchao N, Somintara O, Thincheelong V, Somdee W. A randomized double-blind controlled study comparing erector spinae plane block and thoracic paravertebral block for postoperative analgesia after breast surgery. Anesth Pain Med. 2022;17(4):445–453. doi:10.17085/apm.22157
17. Goswami S, Kundra P, Bhattacharyya J. Pectoral nerve block1 versus modified pectoral nerve block2 for postoperative pain relief in patients undergoing modified radical mastectomy: a randomized clinical trial. Br J Anaesth. 2017;119(4):830–835. doi:10.1093/bja/aex201
18. Karmakar MK, Pakpirom J, Songthamwat B, Sivakumar RK, Samy W. Subpectoral plexus block to enhance surgical anesthesia produced by a multilevel thoracic paravertebral block for primary breast cancer surgery: a prospective randomized double-blind study. Reg Anesth Pain Med. 2025;rapm–2024–106126. doi:10.1136/rapm-2024-106126
19. Nielsen MV, Tanggaard K, Bojesen S, et al. Efficacy of the intertransverse process block: single or multiple injection? A randomized, non-inferiority, blinded, cross-over trial in healthy volunteers. Reg Anesth Pain Med. 2024;49(10):708–715. doi:10.1136/rapm-2023-104972
20. Supphapipat K, Samerchua A, Leurcharusmee P, et al. Single- versus multiple-injection intertransverse process block for VATS: a randomized trial on dermatomal sensory blockade. J Pain Res. 2025;18:4791–4800. doi:10.2147/jpr.S545731
21. Zhang H, Qu Z, Miao Y, et al. Comparison between ultrasound-guided multi-injection intertransverse process and thoracic paravertebral blocks for major breast cancer surgery: a randomized non-inferiority trial. Reg Anesth Pain Med. 2023;48(4):161–166. doi:10.1136/rapm-2022-104003
22. Aygun H, Kiziloglu I, Ozturk NK, et al. Use of ultrasound guided single shot costotransverse block (intertransverse process) in breast cancer surgery: a prospective, randomized, assessor blinded, controlled clinical trial. BMC Anesthesiol. 2022;22(1):110. doi:10.1186/s12871-022-01651-3
23. Kahramanlar AA, Aksoy M, Ince I, Dostbıl A, Karadenız E. The comparison of postoperative analgesic efficacy of ultrasound-guided paravertebral block and mid-point transverse process pleura block in mastectomy surgeries: a randomized study. J Invest Surg. 2022;35(9):1694–1699. doi:10.1080/08941939.2022.2098544
24. Sethi P, Kaur M, Bhatia PK, et al. Comparison of midpoint transverse process to pleura (MTP) block and erector spinae plane block (ESP) for postoperative analgesia in modified radical mastectomy patients: a double-blinded, randomized control trial. J Anaesthesiol Clin Pharmacol. 2024;40(2):344–350. doi:10.4103/joacp.joacp_429_22
25. Elkoundi A. Why erector spinae plane block is more efficient than midtransverse process to pleura block in lumbar spinal surgery: possible underlying mechanisms. Der Anaesthesist. 2021;70(Suppl 1):74–75. doi:10.1007/s00101-021-01029-z
26. Shibata Y, Kampitak W, Tansatit T. The novel costotransverse foramen block technique: distribution characteristics of injectate compared with erector spinae plane block. Pain Physician. 2020;23(3):E305–E314.
27. Cho TH, Kim SH, J O, Kwon HJ, Kim KW, Yang HM. Anatomy of the thoracic paravertebral space: 3D micro-CT findings and their clinical implications for nerve blockade. Reg Anesth Pain Med. 2021;46(8):699–703. doi:10.1136/rapm-2021-102588
28. Xiong C, Han C, Zhao D, Peng W, Xu D, Lan Z. Postoperative analgesic effects of paravertebral block versus erector spinae plane block for thoracic and breast surgery: a meta-analysis. PLoS One. 2021;16(8):e0256611. doi:10.1371/journal.pone.0256611
29. Raft J, Dureau S, Fuzier R, et al. Erector spinae plane block versus paravertebral block for major oncological breast surgery: a multicentre randomised controlled trial. Br J Anaesth. 2025;135(3):772–778. doi:10.1016/j.bja.2025.05.051
30. Hussain N, Brull R, Noble J, et al. Statistically significant but clinically unimportant: a systematic review and meta-analysis of the analgesic benefits of erector spinae plane block following breast cancer surgery. Reg Anesth Pain Med. 2021;46(1):3–12. doi:10.1136/rapm-2020-101917
31. Lovett-Carter D, Kendall MC, McCormick ZL, Suh EI, Cohen AD, De Oliveira GS. Pectoral nerve blocks and postoperative pain outcomes after mastectomy: a meta-analysis of randomized controlled trials. Reg Anesth Pain Med. 2019;44(10):923–928. doi:10.1136/rapm-2019-100658
32. Okamoto A, Yamasaki M, Yokota I, et al. Classification of acute pain trajectory after breast cancer surgery identifies patients at risk for persistent pain: a prospective observational study. J Pain Res. 2018;11:2197–2206. doi:10.2147/jpr.S171680
33. Katz N, Paillard FC, Van Inwegen R. A review of the use of the number needed to treat to evaluate the efficacy of analgesics. J Pain. 2015;16(2):116–123. doi:10.1016/j.jpain.2014.08.005
34. Xin L, Hou N, Zhang Z, Feng Y. The effect of preoperative ultrasound-guided erector spinae plane block on chronic postsurgical pain after breast cancer surgery: a propensity score-matched cohort study. Pain Ther. 2022;11(1):93–106. doi:10.1007/s40122-021-00339-9
35. Yao Y, Li H, He Q, Chen T, Wang Y, Zheng X. Efficacy of ultrasound-guided erector spinae plane block on postoperative quality of recovery and analgesia after modified radical mastectomy: randomized controlled trial. Reg Anesth Pain Med. 2019. doi:10.1136/rapm-2019-100983
36. Gupta G, Jindal S, Gupta D, Palta S, Kaushik R. Quality of recovery after breast surgery: a randomized clinical trial comparing dexamethasone with dexmedetomidine as adjuvant to ropivacaine in ultrasound guided single shot mid- point transverse process to pleura block. Perioper Care Oper Room Manag. 2025;38:100456. doi:10.1016/j.pcorm.2024.100456
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.