Back to Journals » Orthopedic Research and Reviews » Volume 11
Interprosthetic femoral fractures: management challenges
Authors Rozell JC, Delagrammaticas DE, Schwarzkopf R
Received 22 March 2019
Accepted for publication 14 August 2019
Published 16 September 2019 Volume 2019:11 Pages 119—128
DOI https://doi.org/10.2147/ORR.S209647
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Joshua C Rozell,1 Dimitri E Delagrammaticas,2 Ran Schwarzkopf1
1Department of Orthopaedic Surgery, NYU Langone Orthopaedic Hospital, New York, NY, USA; 2Central Coast Orthopedics, San Luis Obispo, CA, USA
Correspondence: Ran Schwarzkopf
NYU Langone Orthopaedic Hospital, 301 East 17th St, Suite 1402, New York, NY 10003, USA
Tel +1 212 598 2783
Email [email protected]
Abstract: Interprosthetic femur fractures are a rare but serious complication following total hip and knee arthroplasty. Classification systems have focused not only on diagnosis but also on treatment algorithm. Critical to the evaluation of patients with these fractures are an assessment of fracture location, bone quality, and the presence of stemmed implants. The gold standard for fracture fixation is locked plating with bicortical and unicortical screws, supplemented with wires or cables as needed. For patients with compromised bone stock or insufficient bony area for fixation, allograft augmentation with struts or interprosthetic sleeves may be used. For fractures with severe bone loss, conversion to a megaprosthesis or total femur replacement may be warranted.
Keywords: interprosthetic, total knee arthroplasty, total hip arthroplasty, revision, periprosthetic fracture
Introduction
Hip and knee arthroplasty continue to be among the most common surgical procedures performed in the United States with an expected increase in utilization as indications expand and an aging population lives longer with an increased demand for more active, pain-free lifestyles.1 As a result, the likelihood of patients having ipsilateral hip and knee prostheses increases, as does the risk of periprosthetic complications, specifically, interprosthetic femur fractures (IFF), defined by a fracture of the femur between an ipsilateral hip and knee prostheses. Early reports on the treatment of these fractures were presented with significant reservation. The earliest report by Dave et al described successful treatment of a single patient who sustained an interprosthetic femur shaft fracture around a stemmed total knee and total hip implant with the use of a Mennan plate, iliac crest bone grafting, and a 3-month period of restricted weight-bearing.2 However, subsequent reports by Kenny et al demonstrated poor outcomes in treating similar fractures, with all four patients in that series failing initial treatment, two of whom required either above knee amputation or hip disarticulation.3 Since these early reports advancement in treatment strategies, namely implant choice and understanding and classifying the fracture pattern have improved the outcomes for these complex injuries. Management and avoidance of treatment complications are dependent on understanding the patient, fracture pattern, intraoperative techniques, and the arthroplasty reconstructive options.4,5
Epidemiology and patient characteristics
The rising number of patients who are living longer and undergoing joint replacement, combined with technology advances and anesthetic protocols for rapid recovery have led to a dramatic increase in the number of patients living with joint replacement.6–8 An estimated 620,000 of these patients have undergone both THA and TKA. Furthermore, about 19,200 Americans are living with ipsilateral hip and knee arthroplasties.9 Patients are remaining active as their quality of life improves and thus more demands are placed on their implants. As a result, the rates of periprosthetic fractures have also risen. While still uncommon, THA periprosthetic fracture rates are reported at 0.1–5% while TKA periprosthetic fractures occur at a rate of 0.3–5.5%.6,10–12
A subset of these fractures known as IFFs was first described by Dave et al in 1995.2 Early estimates regarding the rate of IFFs were made by Kenny et al, reporting a rate of 1.25% in their series of over 300 patients.3 The actual number of IFFs is difficult to estimate, but more recent reports estimate the risk to be about 5–7% of all periprosthetic fractures.13 In some smaller series, Sah et al reported on 22 fractures over a 4-year period, while Platzer et al reported 23 patients in 16 years.14,15 Valle Cruz’s group reported on 6 fractures over a period of 6 years in a cohort of 112 patients.16 While uncommon, these fractures can have significant implications for patient outcomes. Recognition and effective management of these injuries are paramount to maintaining preinjury quality of life for the patient.
Certain implant construct characteristics increase the preponderance or pose management challenges for IFFs. Regarding interprosthetic distance, there is no clear consensus on how far apart hip and knee stems should be to mitigate fracture risk. Theoretically, a reduced distance may lead to higher stress concentration in the femoral shaft and thus an increased risk for fracture at this location. A biomechanical study by Soenen et al observed that gaps <110 mm between stems increased risk of fracture; however, this study did not take into account cortical thickness.17 An alternative argument in the risk for IFF is cortical and medullary diameters. In a series of 23 patients, Lipof et al found that the IFF group was more likely to have significantly narrower femoral cortices at the isthmus compared with intact femurs, but larger medullary canals, suggestive of the typical biomechanical changes seen in patients of older age and those with osteoporosis.6 Similarly, Valle Cruz et al found a higher rate of IFF in areas distal to the hip stem tip which correlated to widening of the femoral canal and narrowing of the femoral cortices.16 Despite diaphyseal stress risers being considered more high risk for fracture compared with metaphyseal ones, Mamczaks’ data corroborated this notion, showing a higher incidence of IFF in the supracondylar area.8
These changes in femoral architecture predisposing patients to periprosthetic and interprosthetic fractures more generally relate to overall bone health; thus, patient risk factors for IFF are similar to those for periprosthetic fractures. These include female gender, advanced age, revision surgery, osteoporosis, and inflammatory diseases such as rheumatoid arthritis.18 Implant-related factors include press-fit stems as a risk for early fracture and the development of osteolytic lesions with the use of conventional polyethylene as a late risk for fracture.19,20 Osteolysis surrounding total hip implants is far less prevalent today as a result of the use of highly cross-linked polyethylene (HXLPE) introduced in the late 1990s. However, patients who underwent hip arthroplasty prior to the use of HXLPE are at higher risk for the development of wear and osteolytic lesions leading to decreased femoral structural stability. Osteoporosis is additionally considered an independent risk factor for fracture. Modular mismatch between the bone–implant interface contributes to stress shielding in already weakened bone which may predispose the patient to fracture in low energy mechanisms of injury. Further, careful consideration should be given to prolonged bisphosphonate use in these patients, as there may be a risk of increased, atypical fractures as a result of the combination of suppressed bone turnover and repetitive stress.21 Platzer et al reported on the presence of severe osteoporosis or rheumatoid arthritis in 73% of the patients treated for distal femoral periprosthetic fracture.22
Interprosthetic fracture classification
Classification of intertrochanteric femur fractures has evolved from initial modifications of the Vancouver and Société Française de Chirurgie Orthopédique et Traumatologique classifications, traditionally used to describe periprosthetic femur and knee fractures, respectively, to an interprosthetic fracture specific classification system described by Pires et al (Figure 1).23–25 In this classification system, interprosthetic fractures are divided into three main types: Type I which describes fractures around a femoral prosthesis, Type II which describes fractures around a knee prosthesis without a stem, and Type III which describes fractures around a knee prosthesis that contain a stem extension. Type I and II fractures are further subdivided into groups A (stable femoral and knee prosthesis), B (unstable femoral but stable knee prosthesis), C (stable femoral but unstable knee prosthesis), and D (unstable femoral and knee prostheses). For Type III fractures, the subgroup differs from Types I and II in that group Type IIIA represents stable prostheses with viable bone between the prostheses, Type IIIB describes stable femoral and knee prostheses with a nonviable fragment or lack of bone between prostheses ends, Type IIIC describes unstable prostheses (hip, knee, or both) with viable bone between the prostheses, and Type IIID represents unstable prostheses (hip, knee, or both) with a nonviable interval fragment due to lack of viable bone between prostheses’ ends. By providing a description of the fracture location, identification of the type of arthroplasty prosthesis that is present, and delineating stability of the prosthesis, this classification system provides both descriptive utility and also aims to direct treatment strategies. For Type I and II fractures, treatment includes plate fixation in the case of a stable prosthesis (subtype A) or revision of an unstable prosthesis to a longer and/or stemmed prosthesis with or without the addition of supplemental plate fixation as needed for fracture fixation (subtypes B-C). For Type III fractures, stable implants without sufficient bone stock or unstable implants with insufficient bone stock can be treated with revision arthroplasty and/or plate fixation with or without bone grafting. Depending on the quality of bone and usability of the original arthroplasty prostheses, consideration of a total femoral replacement or augmentation of the femur with a strut allograft is available tools in the armamentarium of this treatment algorithm (Type ID, IID, or III B-D).25,26
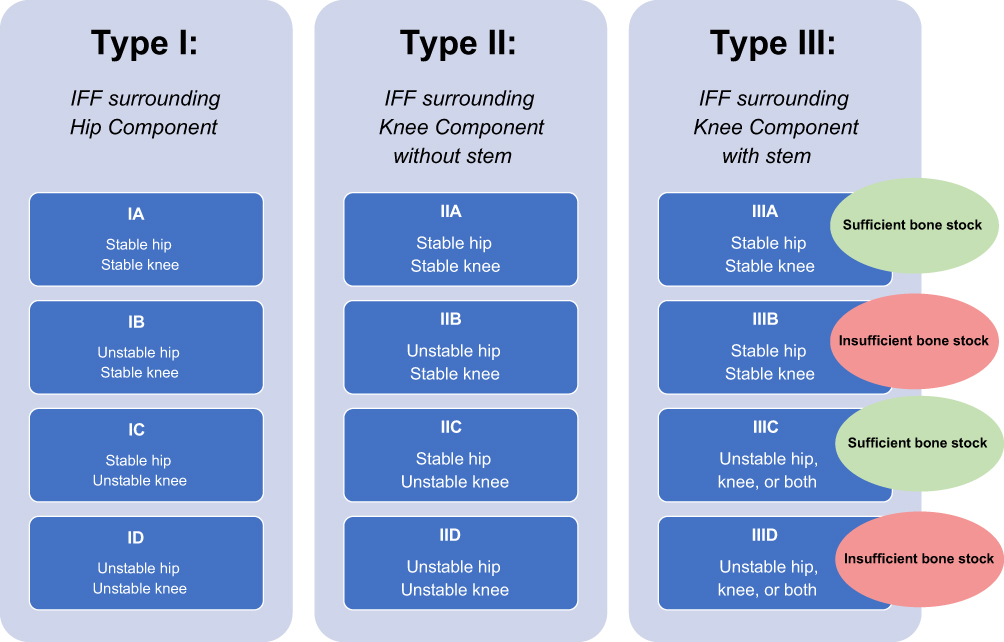 |
Figure 1 Interprosthetic femur fracture classification as described by Pires et al.Note: Data from Pires et al.25,26 |
Intraoperative considerations
Operative management of IFFs poses significant surgical challenges. Navigating these difficult fractures should rely on preoperative patient optimization of medical conditions and an algorithmic, practical surgical approach with a focus on adherence to Arbeitsgemeinschaft für Osteosynthesefragen (AO) principles. Development of a preoperative surgical plan complete with any necessary implants, trays, and adjunct grafts is paramount to success in the operating room. When positioning patients for surgery, our preferred method is in the semi-lateral position on a beanbag over a fully radiolucent table. If a beanbag is not available, one may use an inflatable rapid infuser sleeve attached to a blood pressure cuff machine. The sleeve is placed under the patient’s ipsilateral buttock and during various portions of the procedure the bag may be inflated or deflated to accommodate radiographic views or surgical visualization. Surgical approach may incorporate prior incisions but typically follows an extensile lateral exposure to the femur to facilitate exposure, fracture reduction, and fixation. Careful attention should be paid during dissection to limit periosteal stripping and soft tissue destruction as this may lead to a higher incidence of nonunion. In the case of a short lateral and large medial fracture fragment, a lazy “S” incision that starts laterally and then the lateral femur and tracking medially to expose the knee distally. The patient’s prior medial parapatellar arthrotomy may be re-incised to limit any patellar devascularization with a parallel lateral parapatellar arthrotomy. This will provide an extensile exposure to both the medial and lateral aspects of the distal femur and more easily allow for supplemental neutralizing fixation on the medial side of the femur following lateral plate fixation if varus stress testing produces lateral opening.
As noted earlier, the fracture classification has aided in elucidating fixation options for interprosthetic fractures, depending on the fracture pattern and location, stability of the prostheses, and the patient’s bone quality. For patients with adequate bone stock, constructs may include locking plates, cables, intramedullary nails, or some combination of these. Currently, locking plates are the implant of choice in the treatment of IFFs (Figure 2A–D).14,27–29 These implants provide stable fixation even in osteoporotic bone, help to resist varus collapse when placed on the tensile side of the femur, and are often applied overlying periosteal tissues to preserve the blood supply to the bone.5 The major treatment goals are adequate fixation with restoration of length, alignment, and rotation, early mobilization, and fracture union. Locking plates should be applied along the length of the femur, spanning the prior implant stem(s) by at least two cortical diameters. This serves to maximally disperse forces across the bone, protect the bone from further fracture, and decrease the overall stress concentration at implant–bone interfaces. Many modern locking plates are titanium with a similar modulus of elasticity as bone to limit modulus mismatch. In addition, strategically placed screw holes within the plate function to allow screws to be inserted around hip or knee stems and also prevent a postage stamping effect within the bone, thereby decreasing the risk of further fracture. Finally, to limit the stiffness of the construct and the potential for nonunion, screw density within the plate should be approximately 40–50% (Figure 3A–D). In areas where fixation may not be amenable to bicortical screws due to the presence of prior arthroplasty implants, the use of cerclage cables or unicortical locking screws may supplement fixation (Figure 4). Additionally, in the presence of a cruciate retaining TKA or one with an open box configuration, a retrograde nail may be used. This is typically used in the setting of a revision or interprosthetic nonunion where a supplemental plate is also used, as the nail is unable to overlap the hip stem and causes an area of stress concentration just distal to the hip prosthesis (Figure 5). A recent case series performed by Hussain et al review 9 IFFs treated with a combination of a retrograde nail and laterally locked plate. Fixation proximal to the fracture included an average of 3 bicortical screws and one unicortical screw, and a minimum of four cortices of fixation. They observed a 100% union rate with immediate weight-bearing.30 Utilization of the intramedullary nail functions biologically and biomechanically. Reaming the canal for the nail allows for cancellous bone to be impacted into the fracture site after preliminary reduction with the plate. Biomechanically, an intramedullary nail imparts longitudinal and rotational stability and enhances fixation stability.
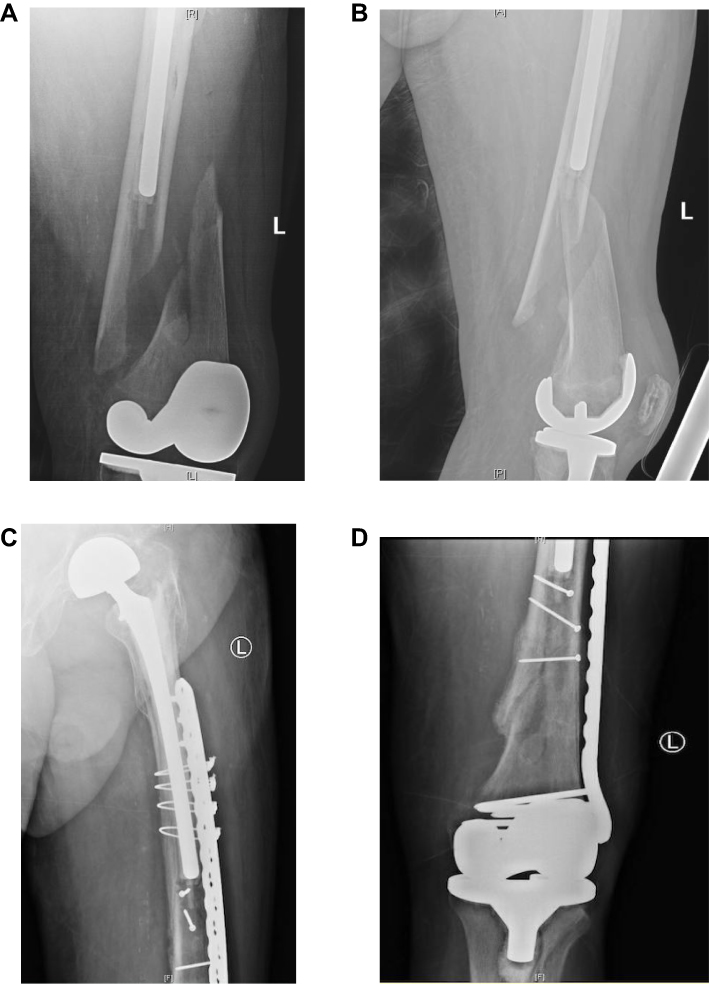 |
Figure 2 Preoperative radiographs (A, B) demonstrating a long spiral oblique interprosthetic fracture with apex posterior angulation. A laterally based femoral locking plate was used for internal fixation of this fracture (C, D) with the addition of interfragmentary lag and position screws. |
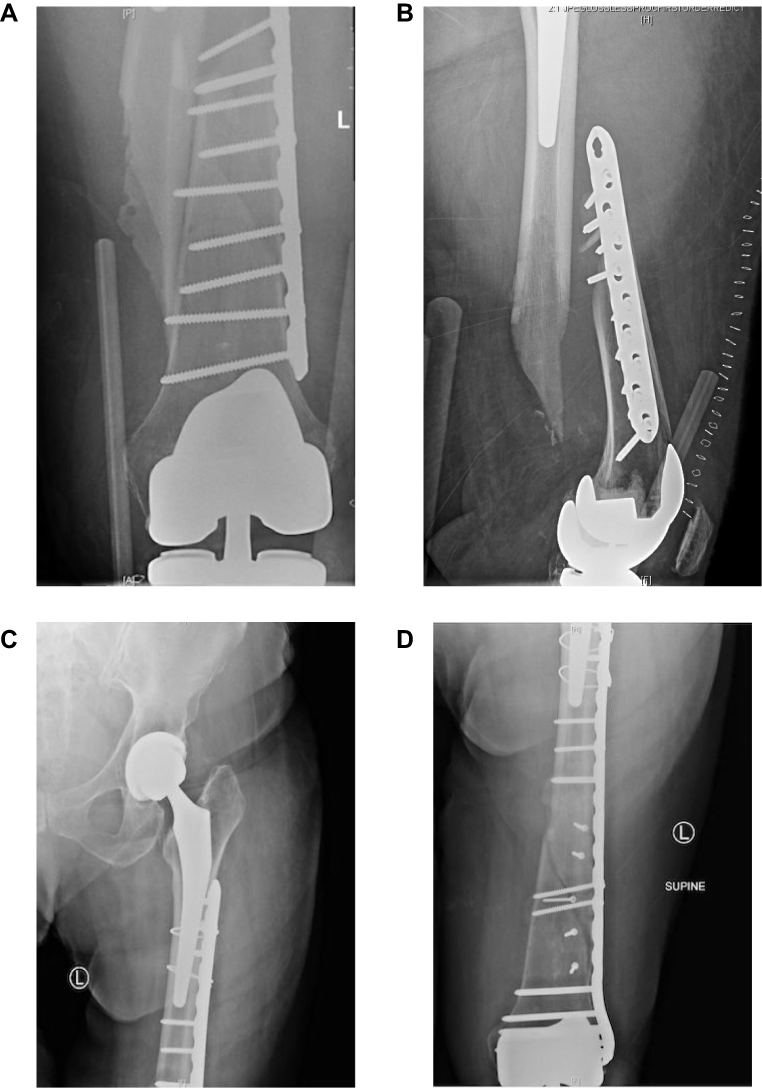 |
Figure 3 Preoperative anteroposterior (A) and lateral (B) radiographs showing plate osteosynthesis with a lateral locking plate and high screw density and thus stiff construct, resulting in a failure of fixation. Anteroposterior (C, D) radiographs of the revision construct demonstrating interfragmentary screws, decreased screw density and construct stiffness, and appropriate prosthesis overlap. |
 |
Figure 4 Anteroposterior radiograph of the proximal femur demonstrating periprosthetic fracture fixation around a long, cemented hip stem. Unicortical screws (outlined by red box) and supplemental cables are useful in this situation with limited bone stock around the stem and a stiff cement mantle. |
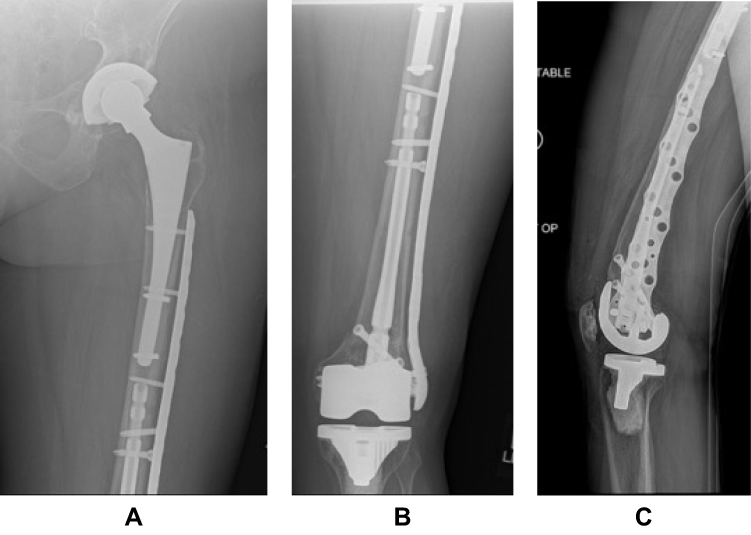 |
Figure 5 Anteroposterior (A, B) and lateral (C) radiographs of a distal periprosthetic femur fracture fixed with a short retrograde nail and supplemented with a long lateral locking plate in a patient with osteoporotic bone. The lateral radiograph demonstrates the staggered screw holes to maximize coverage around the nail and hip stem. (Image Courtesy: Derek J. Donegan, MD). |
Due to the relatively low incidence of IFFs, the clinical literature is primarily in the form of case reports and case series. Recently, however, Bonnevialle et al conducted a retrospective, multicenter study of 51 patients with a mean age of 82.5 years who suffered an IFF between 2009 and 2015. At a mean follow-up of 27 months, there were 6 mechanical complications, 2 surgical site infections, and 2 cases of loosening, illustrating the morbid nature of this injury. The overall mortality at final review was 31% (9 deaths in the first 6 months) with a median survival of 3.45 years.13
In a smaller series, Hoffman et al conducted a retrospective review of 27 IFFs, the majority of whom were females, over a 7-year period. They reported an 89% union rate with long, lateral, titanium plates. They advocated a submuscular plating technique to avoid soft-tissue stripping and adequate proximal fixation around the hip stem.9 One patient did develop hardware failure that required further treatment with dual plating. This serves as an additional option for fixation in cases of limited bone stock anterior or posterior to the stem. A smaller plate may be placed on the anterior surface of the femur to improve biomechanical stability with screws angled medially or laterally to the stem if possible. Sah et al evaluated 22 patients with IFFs treated with locked, condylar plating via a minimally invasive technique. All fractures healed within 14 weeks.14 Similarly, Platzer et al retrospectively evaluated 23 IFFs treated with locked plating and supplementary cerclage cables. By 6 months, 82% were radiographically healed. The four failures were attributed to poor reduction and fixation techniques.15 Moreover, while a treatment algorithm has not been universally adopted, adherence to fixation and surgical principles described earlier can maximize the chance of union and a satisfactory outcome in these difficult fracture patterns.
Considerations in patients with poor bone stock
Special consideration should be given to circumstances where poor bone stock limits standard fixation or arthroplasty reconstruction methods. The initial management as mentioned previously requires assessment of the stability of the implants, which will dictate the ability to retain or need to revise the existing prostheses. For stable implants, fixation methods may include a plate with or without adjunct bone grafting or cortical strut augmentation; a long, lateral locking plate remains the implant of choice for osteoporotic or compromised bone stock.9,14,15,28,29,31–33 When permitted by a knee prosthesis that allows for the introduction of an intramedullary device, dual fixation methods to include both intramedullary nail and plate fixation as previously described may be an option in the initial treatment.30 In the situation of an unstable knee prosthesis without a stemmed component, revision to a stemmed component with or without supplemental metaphyseal fixation may be required (Figure 6). For unstable hip prostheses, treatment first includes revision to a longer distally engaging prosthesis. Definitive fracture fixation with plate and supplemental bone augmentation as needed should follow arthroplasty component revision. Interprosthetic sleeves can be useful to help bypass insufficient diaphyseal bone between stemmed prosthesis.34 Cortical strut augmentation in the setting of interprosthetic fractures has not been explicitly described; however, experience in the setting of single joint periprosthetic fracture can be extrapolated and applied to treatment of interprosthetic fractures with deficient bone stock or nonunion. In these situations, the cortical struts can serve to restore bone stock for noncircumferential loss of cortical bone, bypass stress risers, and further provide biological stabilization at the allograft-host bone interface.31–33 Adjunct autograft or allograft bone graft can further provide osteoinductive and osteoconductive support to fracture healing.35 In certain circumstances where revision reconstructive options are limited due to substantial bone loss around a loose femoral or knee prosthesis, or where both prostheses are loose and reconstruction of both is not a viable option, revision to a total femur prosthesis may be required.3,5,14,25 Similarly, in the situation of multiple failed fracture fixation or persistent fracture non-union, revision to a megaprosthesis may provide a route to definitive treatment.3,5
 |
Figure 6 Anteroposterior (A) and lateral (B) radiographs of a stemmed revision total knee arthroplasty following periprosthetic fracture around a loose total knee prosthesis. Fixation is supplemented with a long lateral locking plate and several adaption plates to maximize screw purchase around the stems. Abundant callus is noted around the stem junction indicating a robust healing response. |
Authors’ preferred management strategy
Our preferred algorithm combines a treatment approach based on the classification by Pires et al with adherence to strict surgical principles to maximize bony healing and restoration of limb alignment (Figure 7). For IFFs with stable hip and knee implants, fixation includes a long, lateral femoral locking plate that spans both implants by at least two cortical diameters. If the total knee prosthesis does not have a stem, the flare of the locking plate extends into the condylar region with multiple locking screws clustered around the implant wherever possible. In cases of cemented implants, diamond tip drill bits may be used to pierce the cement mantle to allow more screw fixation. The plate should be applied with minimal damage to periosteal soft tissues and extended proximally beyond the hip stem and secured with both unicortical and bicortical locking screws as appropriate. Cerclage cables may be applied through reliefs in the plate to supplement fixation. In cases of a loose femoral hip or knee component and a fracture distant from the implant, the arthroplasty is revised to a diaphyseal engaging femoral implant or stemmed knee prosthesis, respectively, and supplemented with plate osteosynthesis. If the fracture closely surrounds one implant that is determined to be loose, such that the fracture is distant from the other implant and without diaphyseal extension of the fracture, that singular component is revised with the fracture bypassed with revision component. In general, however, one should be liberal in the use of supplemental plate fixation to disperse contact forces across the entire femur and limit stress risers, especially in areas of bone with high modulus mismatch. If both implants are loose, further evaluation of the bone quality will dictate more extensive treatment options. If the bone quality is adequate, both components may be revised and an interprosthetic sleeve placed as an internal strut. Cortical strut grafting may be supplemented for additional biologic and structural fixation and secured in place with cerclage cables. If bone stock is inadequate, the patient may obtain the most benefit and a more expedient surgery with conversion to a total femur replacement.
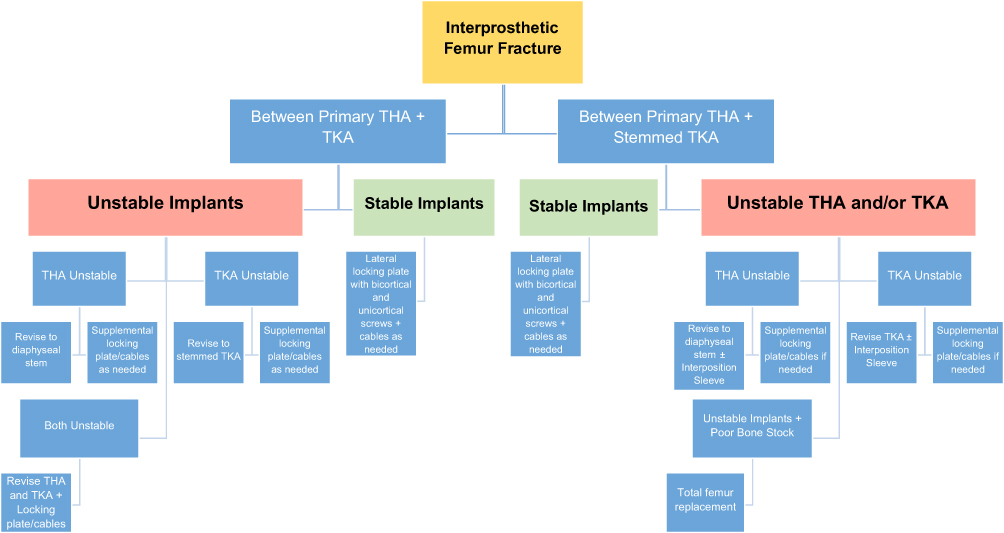 |
Figure 7 Authors’ preferred management strategy for fixation of interprosthetic femur fractures based upon fracture location, implant stability, and bone stock. |
Postoperative rehabilitation
Following fixation of interprosthetic fractures, allowing bony union and maintaining a stable construct is of paramount importance. Therefore, patients are typically kept toe-touch weight-bearing (10%) with a walker for the first 6 weeks after surgery. Multimodal pain management strategies with acetaminophen, minimal and judicious opioid use, and various gabapentanoids are used. Use of nonsteroidal anti-inflammatory medications remains controversial regarding their effects on fracture healing, but often three doses of intramuscular or intravenous ketorolac may be given in the immediate postoperative period. Physical therapy begins on the day of surgery or first postoperative day and focuses on range of motion, strengthening, and gait training. At the 6-week visit, follow-up radiographs are obtained to assess the degree of healing. At that time patients may be progressed to partial weight-bearing and transitioned to full weight-bearing as tolerated over the next 2–4 months.
Conclusion
Interprosthetic femur fractures represent a difficult clinical problem with a growing incidence in the face of more patients living with ipsilateral total hip and knee arthroplasties. When treating a patient with an IFF, careful consideration of the patient’s preoperative medical status, implant type and stability, and surrounding bone stock will help guide treatment options. Standard fixation options include locking plates and screws, supplemental cerclage cables, with possible bone grafting. In cases of unstable or loose implants, techniques including intramedullary nails, interprosthetic sleeves, revision arthroplasty components, and graft material. Finally, total femur replacements or a megaprosthesis are typically reserved for patients with limited bone stock and loose implants.
Disclosure
Dr Ran Schwarzkopf provided consultancy service to Smith & Nephew, holds stock options from Intelijoint, and involved in the Gauss Surgical Research for Smith & Nephew. The authors report no other conflicts of interest in this work.
References
1. Fingar KR, Stocks C, Weiss AJ, Steiner CA. Most Frequent Operating Room Procedures Performed in U.S. Hospitals, 2003–2012: Statistical Brief #186. 2014 Dec. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2006. Available from: https://www.ncbi.nlm.nih.gov/books/NBK274246/. Accessed September 06, 2019.
2. Dave D, Koka S, James S. Mennen plate fixation for fracture of the femoral shaft with ipsilateral total hip and knee arthroplasties. J Arthroplasty. 1995;10(1):113–115.
3. Kenny P, Rice J, Quinlan W. Interprosthetic fracture of the femoral shaft. J Arthroplasty. 1998;13(3):361–364.
4. Jennison T, Yarlagadda R. Outcome of surgical treatment of inter prosthetic fractures: a case series. Orthop Traumatol Surg Res. 2019;105(4):587–589.
5. Scolaro JA, Schwarzkopf R. Management of interprosthetic femur fractures. J Am Acad Orthop Surg. 2017;25(4):e63–e69. doi:10.5435/JAAOS-D-15-00664
6. Lipof JS, Amitai AD, Judd KT, Gorczyca JT. Radiographic risk factors for interprosthetic femur fractures. Iowa Orthop J. 2017;37:35–39.
7. Kremers HM, Larson DR, Crowson CS, et al. Prevalence of total hip and knee replacement in the United States. J Bone Jt Surg Am Vol. 2014;97(17):1386–1397. doi:10.2106/JBJS.N.01141
8. Mamczak C, Gardner M, Bolhofner B, Borrelli J, Streubel P, Ricci W. Interprosthetic femoral fractures. J Orthop Trauma. 2010;24(12):740–744. doi:10.1097/BOT.0b013e3181d73508
9. Hoffmann MF, Lotzien S, Schildhauer TA. Clinical outcome of interprosthetic femoral fractures treated with polyaxial locking plates. Injury. 2016;47(4):934–938. doi:10.1016/j.injury.2015.12.026
10. Berry D. Epidemiology: hip and knee. Orthop Clin North Am. 1999;30(2):183–190.
11. Kim K-I, Egol KA, Hozack WJ, Parvizi J. Periprosthetic fractures after total knee arthroplasties. Clin Orthop Relat Res. 2006;446:167–175. doi:10.1097/01.blo.0000214417.29335.19
12. Rorabeck C, Taylor J. Periprosthetic fractures of the femur complicating total knee arthroplasty. Orthop Clin North Am. 1999;30(2):265–277.
13. Bonnevialle P, Marcheix PS, Nicolau X, et al. Interprosthetic femoral fractures: morbidity and mortality in a retrospective, multicenter study. Orthop Traumatol Surg Res. 2019;105(4):579–585.
14. Sah AP, Marshall A, Virkus WV, Estok DM, Della Valle CJ. Interprosthetic fractures of the Femur. Treatment with a single-locked plate. J Arthroplasty. 2010;25(2):280–286. doi:10.1016/j.arth.2008.10.008
15. Platzer P, Schuster R, Luxl M, et al. Management and outcome of interprosthetic femoral fractures. Injury. 2011;42(11):1219–1225. doi:10.1016/j.injury.2010.08.020
16. Valle Cruz JA, Urda AL, Serrano L, et al. Incidence of and risk factors for femoral fractures in the gap between hip and knee implants. Int Orthop. 2016;40(8):1697–1702. doi:10.1007/s00264-015-2978-1
17. Soenen M, Baracchi M, De Corte R, Labey L, Innocenti B. Stemmed TKA in a Femur with a total hip arthroplasty: is there a safe distance between the stem tips? J Arthroplasty. 2013;28(8):1437–1445. doi:10.1016/j.arth.2013.01.010
18. Solarino G, Vicenti G, Moretti L, Abate A, Spinarelli A, Moretti B. Interprosthetic femoral fractures - A challenge of treatment. A systematic review of the literature. Injury. 2014;45(2):362–368. doi:10.1016/j.injury.2013.09.028
19. Marsland D, Mears SC. A review of periprosthetic femoral fractures associated with total hip arthroplasty. Geriatr Orthop Surg Rehabil. 2012;3(3):107–120. doi:10.1177/2151458512462870
20. Zhu Y, Chen W, Sun T, Zhang X, Liu S, Zhang Y. Risk factors for the periprosthetic fracture after total hip arthroplasty: a systematic review and meta-analysis. Scand J Surg. 2014;104(3):139–145. doi:10.1177/1457496914543979
21. Chen F, Bhattacharyya T. Periprosthetic fracture of the femur after long-term bisphosphonate use. JBJS Case Connect. 2012;2(2):e21. doi:10.2106/JBJS.CC.K.00085
22. Platzer P, Schuster R, Aldrian S, et al. Management and outcome of periprosthetic fractures after total knee arthroplasty. J Trauma Inj Infect Crit Care. 2010;68(6):1464–1470. doi:10.1097/TA.0b013e3181d53f81
23. Fink B, Fuerst M, Singer J. Periprosthetic fractures of the femur associated with hip arthroplasty. Arch Orthop Trauma Surg. 2005;125(7):433–442. doi:10.1007/s00402-005-0828-0
24. Soenen M, Migaud H, Bonnomet F, Girard J, Mathevon H, Ehlinger M. Interprosthetic femoral fractures: analysis of 14 cases. Proposal for an additional grade in the Vancouver and SoFCOT classifications. Orthop Traumatol Surg Res. 2011;97(7):693–698. doi:10.1016/j.otsr.2011.07.009
25. Pires RES, De Toledo Lourenço PRB, Labronici PJ, et al. Interprosthetic femoral fractures: proposed new classification system and treatment algorithm. Injury. 2014;45(S5):S2–S6. doi:10.1016/S0020-1383(14)70012-9
26. Pires RES, Silveira MPS, Da Silva Resende AR, et al. Validation of a new classification system for interprosthetic femoral fractures. Injury. 2017;48(7):1388–1392. doi:10.1016/j.injury.2017.04.008
27. Ehlinger M, Czekaj J, Adam P, Brinkert D, Ducrot G, Bonnomet F. Minimally invasive fixation of type B and C interprosthetic femoral fractures. Orthop Traumatol Surg Res. 2013;99(5):563–569. doi:10.1016/j.otsr.2013.01.011
28. Ebraheim N, Carroll T, Moral MZ, Lea J, Hirschfeld A, Liu J. Interprosthetic femoral fractures treated with locking plate. Int Orthop. 2014;38(10):2183–2189. doi:10.1007/s00264-014-2414-y
29. Hou Z, Moore B, Bowen TR, et al. Treatment of interprosthetic fractures of the femur. J Trauma Inj Infect Crit Care. 2011;71(6):1715–1719. doi:10.1097/TA.0b013e31821dd9f1
30. Hussain MS, Dailey SK, Avilucea FR. Stable fixation and immediate weight-bearing after combined retrograde intramedullary nailing and open reduction internal fixation of noncomminuted distal interprosthetic femur fractures. J Orthop Trauma. 2018;32(6):e237–e240. doi:10.1097/BOT.0000000000001154
31. Judas F, Saavedra MJ, Mendes AF, Dias R. Cortical strut allografting in reconstructive orthopaedic surgery. Acta Reumatol Port. 2011;36(1):24–28.
32. Gross AE, Wong PKC, Hutchison CR, King AE. Onlay cortical strut grafting in revision arthroplasty of the hip. J Arthroplasty. 2003;18(3SUPPL. 1):104–106. doi:10.1054/arth.2003.50077
33. Haddad F, Duncan C, Berry D, Lewallen D, Gross A, Chandler H. Periprosthetic femoral fractures around well-fixed implants: use of cortical onlay allografts with or without a plate. J Bone Jt Surg. 2002;84A:945. doi:10.2106/00004623-200206000-00008
34. Abdelaziz H, Saleri S, Mau H, et al. Interprosthetic femoral sleeves in revision arthroplasty: a 20-year experience. J Arthroplasty. 2019. doi:10.1016/j.arth.2019.02.055
35. Tsiridis E, Spence G, Gamie Z, El Masry MA, Giannoudis PV. Grafting for periprosthetic femoral fractures: strut, impaction or femoral replacement. Injury. 2007;38(6):688–697. doi:10.1016/j.injury.2007.02.046
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.