Back to Journals » Open Access Emergency Medicine » Volume 14
Interprofessional On-floor Education on Oxygen Therapy in COVID-19 Patients, Cardiac Arrest, and Procedural Sedation: Perception of Health-care Workers in Emergency Setting
Authors Farooq M, Ahmad S ![]() , Hanjra FK, Zafar O, Bashir K
, Hanjra FK, Zafar O, Bashir K ![]()
Received 27 December 2021
Accepted for publication 13 September 2022
Published 30 September 2022 Volume 2022:14 Pages 535—543
DOI https://doi.org/10.2147/OAEM.S349656
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Munawar Farooq, Shabbir Ahmad, Faisal K Hanjra, Obaidullah Zafar, Khalid Bashir
Emergency Department, Hamad General Hospital, Doha, Qatar
Correspondence: Khalid Bashir, Tel +974 33766596, Email [email protected]
Objective: There is paucity of evidence for interprofessional education (IPE) conducted within the working environment of emergency departments (EDs). This study demonstrates favorable perception of on-floor IPE sessions conducted in a busy emergency department.
Materials and Methods: Between January and December 2020, IPE was conducted in EDs using low fidelity manikins and involved nurses, doctors, respiratory therapists, and medical students already present on floor. The three key areas were, taught cardiac arrest, escalating oxygen therapy for COVID-19 patients, and procedural sedation. Each session lasted 30 min, and feedback was obtained immediately after the session in both transcribed and written forms through scannable survey monkey links.
Results: Forty-seven sessions were conducted covering the three topics for 141 participants. The majority of the participants benefited from on-floor IPE and preferred this approach in the future. Both participant and faculty recommended to have some protected time to maximize the learnings.
Conclusion: IPE in the clinical environment is feasible, with careful planning it can enhance collaborative learning in the ED.
Keywords: interprofessional education, cardiac arrest, procedural sedation, COVID-19, clinical environment, emergency department
Introduction
Interprofessional education (IPE) is an important educational approach that helps to prepare health professionals from different backgrounds to work together in a collaborative team environment to improve patient management.1 Health professionals working in interprofessional teams not only improves patient care, but also reduces the length of stay and reduces medical errors.2 Several credible organizations such as the World Health Organization (WHO) and the American Public Health Association have highly recommended the training of different professionals together.2
The emergency department is a busy environment where IPE is important for optimal patient care. It is a high-intensity, high-acuity workplace, with an increased communication load on clinicians.3 Poor collaboration and lack of interprofessional effective communication can lead to medical errors, poor patient care, and lower job satisfaction. Better collaboration among different healthcare professionals depends upon effective IPE.3 The World Health Organization (WHO) has advised implementing interprofessional training in the medical syllabus so that medical students can learn about the important theoretical and practical aspects before entering the workplace including the emergency department.2,4
The emergency department poses unique clinical challenges, the combination of undifferentiated patients, high level of acuity, increased volume of patients and shift work pose a considerable clinical risk, particularly if there is dearth of collaborative training. It has been established that several adverse events experienced by patients can be attributed to a breakdown in communication amongst members of the multidisciplinary team. Therefore, effective and efficient teamwork amongst a multidisciplinary clinical team is an essential component of providing safe clinical care.5 Interprofessional simulation provides a useful framework to improve collaboration and communication within the multidisciplinary team.6 Furthermore, conducting simulated exercises in real-time in the clinical environment “shop-floor” provides an added sense of realism allowing effective standard operating procedures to be developed and any operational shortcomings to be addressed. By undertaking simulation regularly, a protocolized culture is established allowing for staff to work effectively in different teams and in ever-changing circumstances, but operating within a defined clinical framework.7
In January 2020, we established a program of education for the multidisciplinary team working in the emergency department. Referred to as a ”Skills and Drills” (S&D) program, it aimed to promote familiarization, adherence, and standardized implementation of existing emergency department guidelines, policies, and checklists with a particular emphasis on close collaboration between medical and nursing staff. Three specific areas were chosen:
- Management of cardiac arrests in non-acute areas of the emergency department
- Safe procedural sedation in the emergency department
- Oxygen escalation therapy in the emergency department for patients with COVID-19
The above three areas were chosen as a quality improvement initiative based on feedback from morbidity and mortality meetings, a reflection of the ongoing clinical pressures by the COVID-19 pandemic, and the opportunity to enhance greater communication and teamwork amongst the multidisciplinary team. Each session lasted for 30 min, involved a clinical scenario and defined learning outcomes which included clinical knowledge, awareness of local guidelines and an emphasis on human factors and team dynamics.
Cardiac arrest is a time-critical condition and is usually managed by a team of nurses, physicians, and respiratory therapists. Despite recent improvement in patient survival from cardiac arrest due to enhanced training and availability of equipment, it is still one of the leading causes of death in the emergency department.
Procedural sedation is frequently carried out in the ED for various types of medical and surgical conditions. Teamworking during procedural sedation can help individuals from various specialties to learn from each other and improve the overall safety of the procedure.7,8
Escalating oxygen therapy has become a commonly used intervention in the emergency department due to the high incidence and prevalence of COVID-19 infections. Oxygen escalation therapy involves stepwise approaches that are used to improve symptoms of patients with COVID-19 infection. Common types of oxygen escalation therapy include a nasal cannula, simple and non-rebreathing masks, venturi mask, high flow nasal cannula, continuous positive pressure ventilation and intubation. COVID-19 patients requiring oxygen therapy need careful management and interventions that are not possible without a collaborative health care workforce.9
The feedback was collected to explore the usefulness of S&D sessions which could be interpreted as abbreviated and low fidelity in situ simulation. We hypothesized that our S&D sessions are low burden, practical, engaging, and impactful. Our S&D training is not replacement for simulation training in training centres and full in situ simulation, rather it has supplementary, reinforcing, encouraging, and monitoring role for previous formal training. In this project, we have studied the feasibility and self-reported benefit of IPE in emergency conditions such as cardiac arrest, procedural sedation, and escalating oxygen therapy in COVID-19 patients. The IPE education was evaluated through Level 1 of the Kirkpatrick training evaluation model.10
Materials and Methods
The ED at Hamad General Hospital (HGH) is one of the largest and busiest departments in the world seeing up to 1500 patients per day. Our ED has approximately 230 physicians, more than 1000 nurse and allied health-care professionals. The medical staffing includes medical interns, residents, fellows, specialists, and consultant grade doctors. It has an Accreditation Council of Graduate Medical Education-International (ACGME-I) accredited emergency medicine residency program. The department runs two years advanced leadership EM fellowship training and one year consolidation training for specialists. The department is affiliated with two medical schools and provides EM training block for year 4 and year 5 medical students. Respiratory therapists, clinical pharmacists, porters, and security staff work in the ED as allied health-care professionals in clinical areas. There are dedicated training activities for training grade doctors and continuous medical education (CME) activities for each health-care workers provided through their respective programs. IPE on the shop floor using the actual equipment involving all relevant staff is practically a higher level of learning. We conducted IPE within the clinical areas of ED using low fidelity manikins for CPR and simulated patients played by faculty. Low fidelity manikins are full size without clinical signs. The cardiac arrest trolleys, equipment in clinical area and training equipment were used for training sessions to be as realistic as possible, however minimizing unnecessary waste. The teaching faculty used clinical scenarios and a structured template to facilitate the delivery of sessions. The three main topics taught were cardiac arrest, procedural sedation, and oxygen escalation therapy for COVID-19 patients (Table 1). These three topics were recommended by the quality assurance team due to suboptimal management of some patients in these areas. Each session lasted for 30 min. Immediately after the session, verbal feedback was transcribed. Written feedback was also collected from both faculty and learners using a structured survey using SurveyMonkey. The QR code directed SurveyMonkey online feedback was used for this purpose too. (Tables 2 and 3). The survey recorded reactions and perception of the participants about the session and its effectiveness. A register of participants recorded the details of the participants including their discipline and grade. Anonymized data was entered into a master Excel sheet for further analysis.
 |
Table 1 Skills and Drills Sessions Conducted |
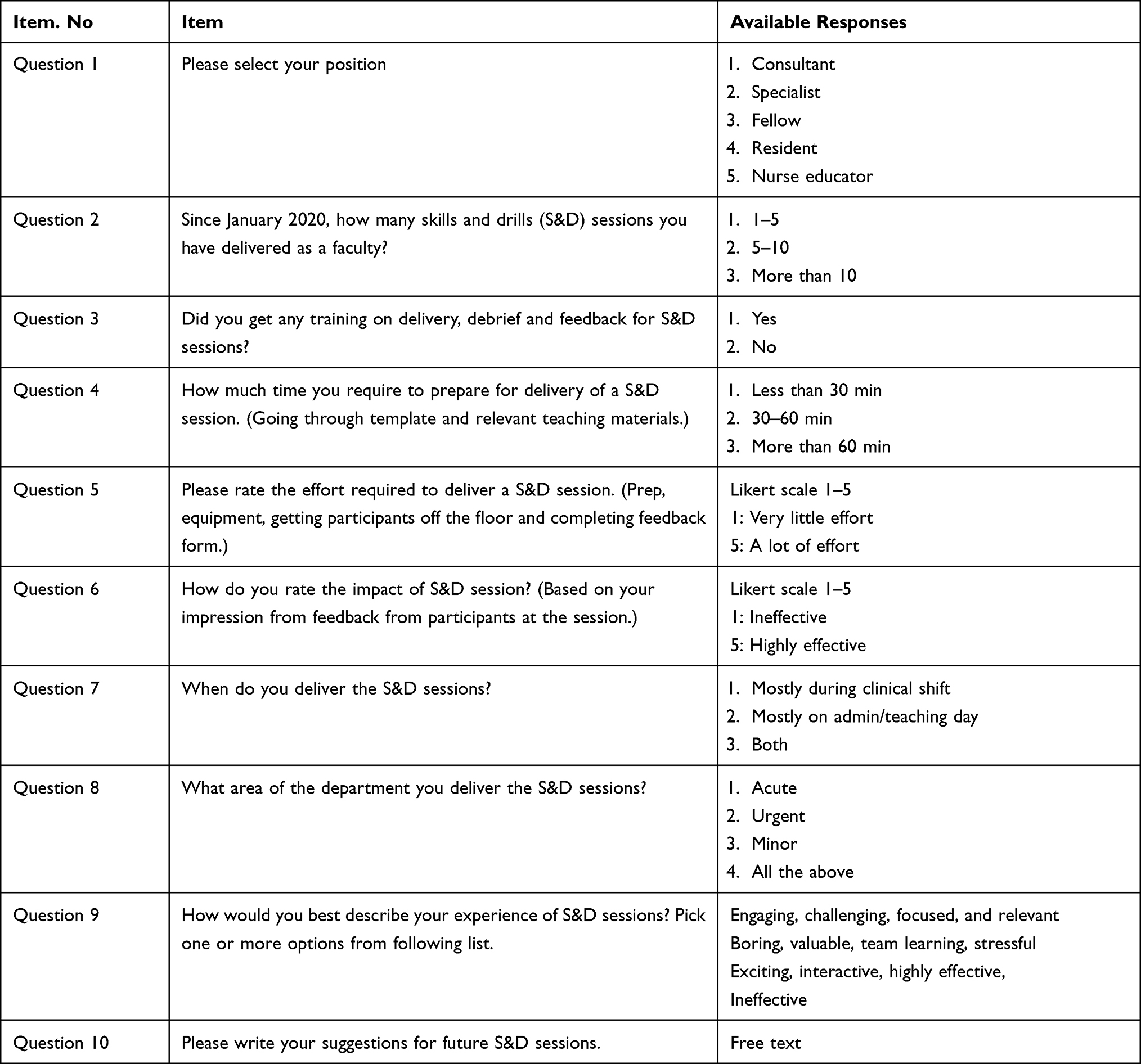 |
Table 2 S&D Faculty Survey Questionnaire |
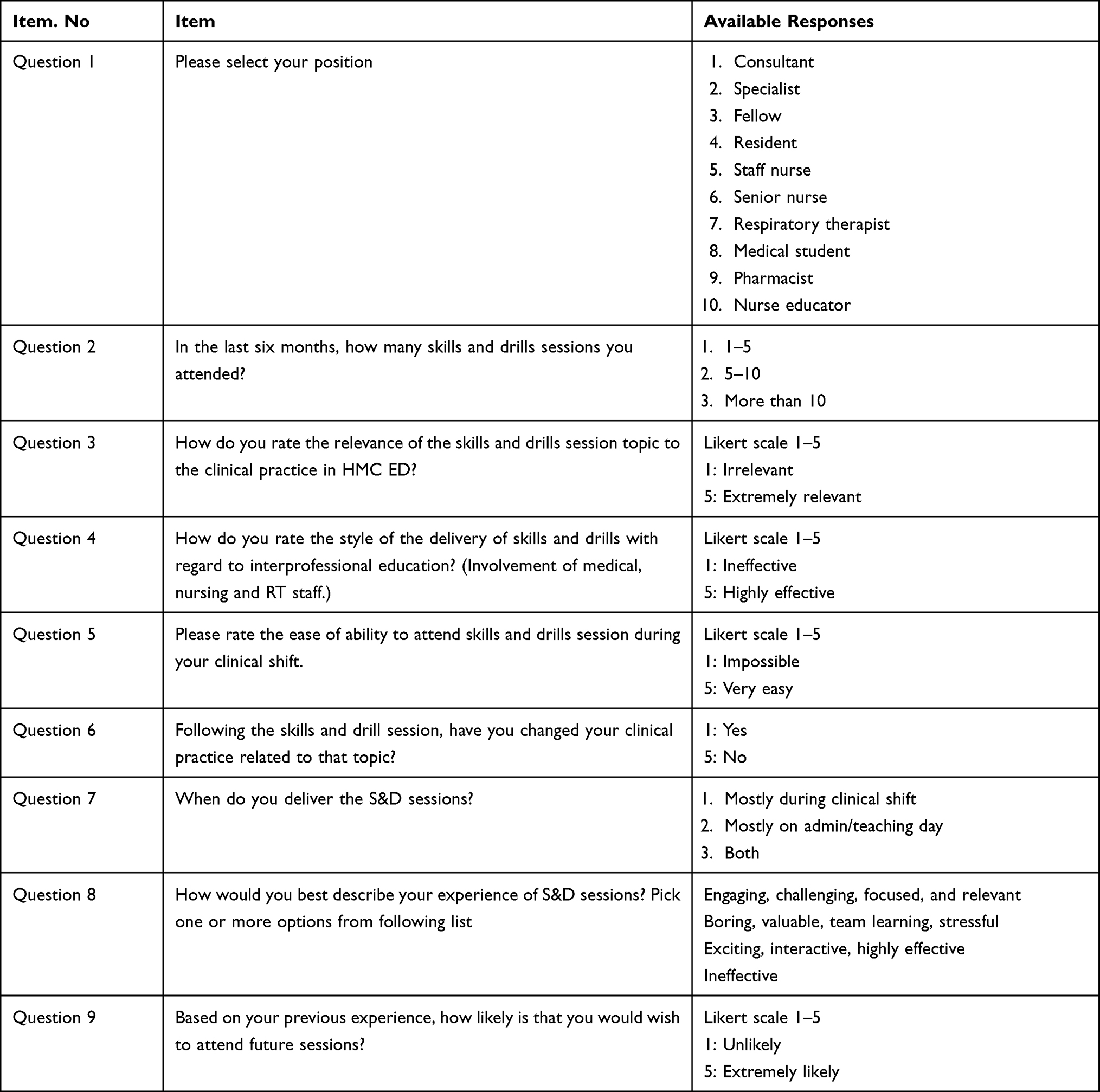 |
Table 3 S&D Learners’ Survey Questionnaire |
The Ethics Committee of Hamad Medical Corporation Qatar approved the study as a QIP and waived the need to obtain consent for data collection, analysis, and publication. The study was conducted in accordance with the Declaration of Helsinki as revised in 2013.
Results
During the study period, 47 sessions were conducted on the three topics selected for this study including cardiac arrest, oxygen escalation in COVID-19, and procedural sedation.
Sixteen S&D sessions were delivered for teaching cardiac arrest and 141 staff attended these sessions during 2020. HGH ED is divided into multiple areas based on acuity of patients namely, High acuity, urgent and minor injury, and illness areas. Cardiac arrest S&D were carried out in different areas to train staff in the drills, equipment familiarity, effective resuscitation, and patient flow. Sixty-nine doctors, 59 nurses, and 13 respiratory therapists attended cardiac arrest S&D training sessions. The recommended minimal team in HGH ED internal cardiac arrest (code blue) response include two doctors, four nurses and an RT. In some complex cases more staff are called including porters and security staff. The attendance of 141 for 16 sessions is realistic compared to a real life scenario (Figure 1).
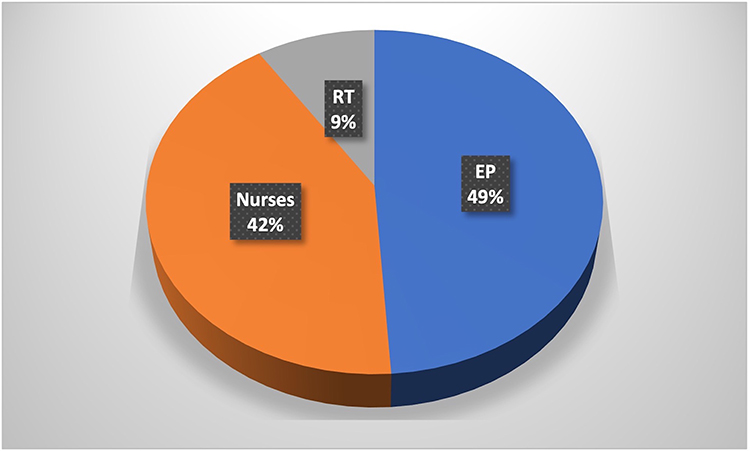 |
Figure 1 Participants of cardiac arrest session. |
Twenty-three sessions were delivered about procedural sedation and 121 learners attended these sessions. The breakdown of the attendees included 80 doctors, 35 nurses, three RTs and five medical students. The S&D session for procedural sedation was aimed at promoting the preparation checklist, timeout checklist and structured documentation. HGH ED standard operating procedure for procedural sedation mandates minimum two doctors, two nurse or one nurse and one RT for procedural sedation. The attendance for this S&D training sessions roughly mirrored the real-world scenario (Figure 2). Eight sessions were delivered during training of escalated oxygen therapy and 80 learners participated. During the COVID-19 pandemic in 2020, patients who required oxygen were treated in dedicated areas of the ED. These areas were staffed by medical and nursing staff and RTs were mainly in high acuity areas looking after patients who required NIV and intubation. There were emerging and conflicting protocols about oxygen therapy in terms of flow and devices. HMC ED formulated oxygen escalation protocol for COVID-19 patients. S&D training sessions were conducted to train staff regarding the oxygen therapy. Participants for this S&D activity comprised of 34 doctors and 46 nurses (Figure 3).
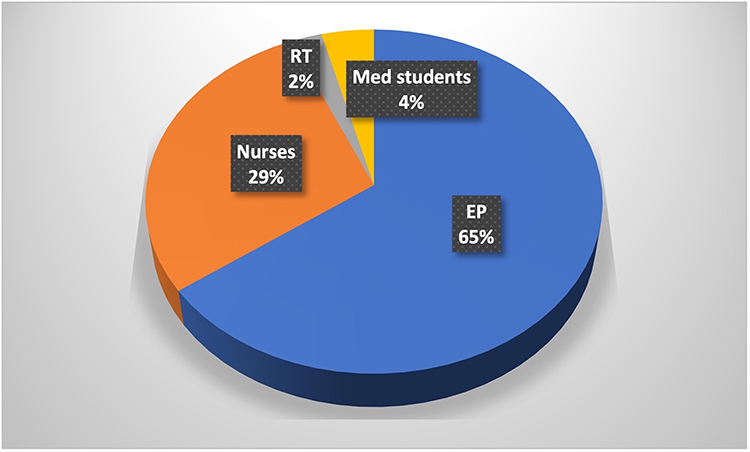 |
Figure 2 Participants of procedural sedation S&D. |
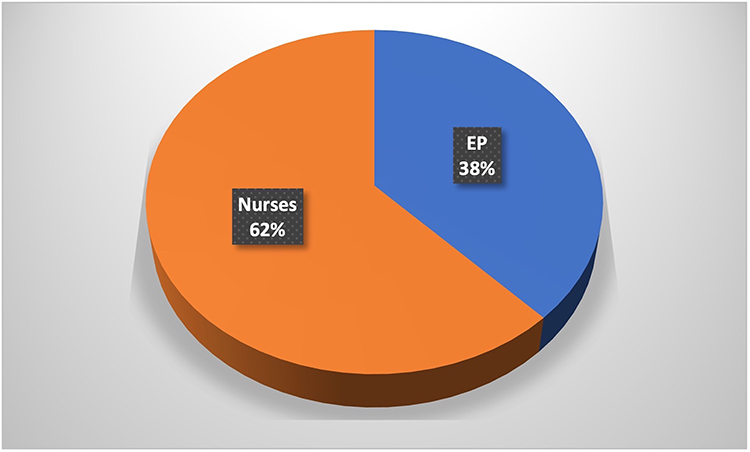 |
Figure 3 Participants of oxygen therapy S&D. |
Forty learners completed online feedback survey which represented all discipline and grades of participants. A Likert scale was used for recording reaction and perception of the respondents. Feedback survey results from learners showed that over 95% of respondents considered S&D relevant to their clinical practice and the style of delivery to be very effective. Most learners indicated that it was easy to attend the session and they were interested in future sessions. All respondents except one, indicated that they would change their practice after attending the session. Participants overwhelmingly chose positive descriptors from the list to express their experience as a learner (Figure 4).
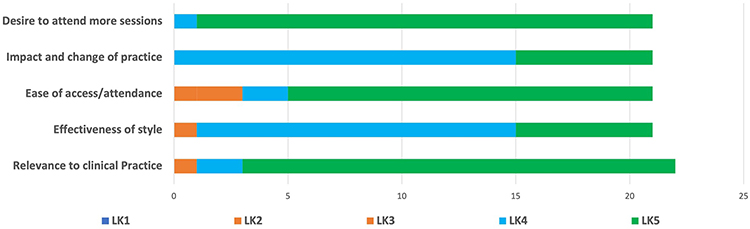 |
Figure 4 S&D learners’ feedback results. |
For the faculty feedback,14 consultants and two fellows completed the online survey. S&D trainers were asked about their experience, perception of its impact and burden of delivery. Qualitative and quantitative variables were used in the questionnaire. Some faculty have previously delivered more than 10 sessions at the time of participation in the survey. Almost half of the faculty indicated that they had some type of training in delivering S&D sessions. Most faculty required 30–60 min of preparation time and they described it as a moderate effort to get learners for the session during clinical shift. More than 90% of faculty believed that their session was impactful for the learners. The faculty picked positive descriptors from the list to describe their experience of teaching S&D (Figure 5).
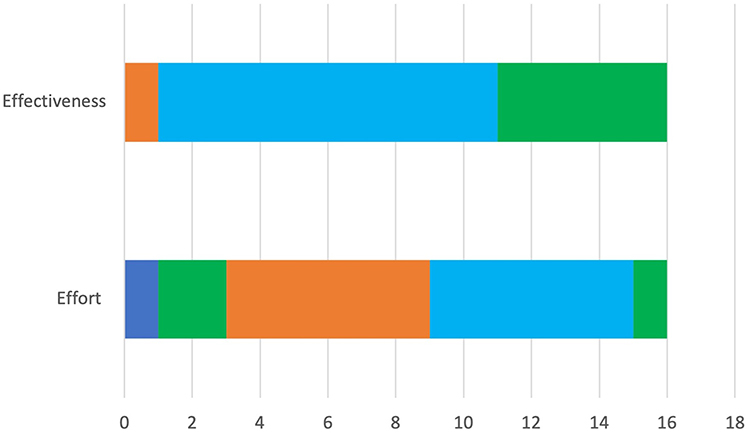 |
Figure 5 Faculty survey results. |
This feedback obtained immediately after the session consisted of feasibility, barriers of IPE, and suggestions for improvement of attendance and pertinent topics for future education. The comments included “easy to attend”, “engage more faculty members from nurses and RTs, “should include more topics which need more refinement, those topics, or skills that we practice in our daily routine on the shop floor” Continue great work, “continue to be responsive to hospital needs, “engage more faculty members from nurses and RTs”.
Discussion
Our first experience of IPE in ED has been encouraging given the positive feedback by both participants and teaching faculty. Participants felt this method was a feasible and engaging learning experience. Overcoming interprofessional barriers can increase satisfaction and collaboration amongst a diverse health-care team. Knowledge about IPE should be included in the curricula of medical and nursing students. On ”shopfloor” IPE can prove to be an effective teaching tool for medical professionals.
Health-care professionals found it easy to attend the sessions that were conducted on-site. Conducting the learning sessions about IPE in the lecture hall or classroom is more time-consuming and requires more preparation time and work adjustments. If IPE is offered on site, it may increase the attendance by participants as it will require less interruption in the schedule. To enhance knowledge through IPE, on-site learning and training can provide a realistic environment for health-care professionals to learn from a collaborative experience. As a result of education at workplace, this approach is more acceptable to medical students, nurses, teaching faculty, and other participants that are a part of the emergency department workforce.11
In our study, the lack of dedicated time was highlighted both by participants and faculty as one of the barriers to the successful implementation of IPE. Dedicated time allows faculty the appropriate preparatory time for the delivery of the educational session while for the learner dedicated time allows an unhurried learning environment. With the recent pandemic face-to-face learning has been largely replaced by online teaching through electronic and social media platforms. The convenient and easy use of such platforms has resulted in increased popularity and demand. IPE allows for face-to-face learning in an environment that is convenient for both teacher and student and results in better teamwork in the ED.12
We utilized the cases to simulate real clinical scenarios, which appeared to be an effective strategy. Interprofessional education can be taught in various formats that include interprofessional simulations, reading clubs, and case discussions.12
Many barriers exist in literature in the clinical practice of simulation-based interprofessional education, which ranges from simple planning to administrative barriers at various institutions. Here are some of the major challenges and limitations regarding interprofessional education in hospital settings:
- Lack of collaboration and coordination among certification and competency requirements
- Lack of research and clinical trials in interprofessional education
- The decreased interest of administrative staff and faculty in providing resources and a favorable environment for interprofessional education
- Administrative resistance and faculty barriers
These barriers and limitations should be overcome for all types of education and communication-based programs including interprofessional education programs. IPE will improve decision-making regarding patients’ health and disease and enhance teamwork and workforce in different departments of hospitals including the emergency department.13
Some limitation needs to be considered regarding the above study. First, low fidelity manikins were used in the simulated teaching sessions where the clinical signs were not present in the manikins. This was the only pragmatic approach available to us to practice IPE as it would been unethical to study on real sick patients. Second, the training was only completed in one emergency department of a local teaching hospital. The sample may not be representative of other emergency departments, hence results from the study may not be generalizable. Third, the majority of the participants were millennial learners who prefer to learn by doing, the results may be different with different age groups.14 Fourth, we did not use a blended learning approach, which may have been better due to shift work and availability of free time.15
Conclusions
We have found that on-site IPE in the emergency department between different health-care professionals is an effective and efficient means of delivering training. The results of initial experience of teaching escalation oxygen therapy in COVID-19 patients, cardiac arrest and conscious sedation is achievable and has been valued by the participants and teaching faculty.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Brashers VL, Curry CE, Harper DC, et al. Interprofessional health care education: recommendations of the National Academies of Practice expert panel on health care in the 21st century. Issues Interdiscip Care. 2001;3:21–31.
2. Institute of Medicine Committee on the Health Professions Education Summit: Institute of Medicine (US) Committee on the Health Professions Education Summit. Health Professions Education: A Bridge to Quality. In: Greiner AC, Knebel E, eds. Washington (DC): National Academies Press (US); 2003.
3. World Health Organization. Learning together to work together for health. Report of a WHO Study Group on Multiprofessional Education of Health Personnel: the Team Approach. World Health Organ Tech Rep Ser. 1988;769:1–72. PMID: 3140499.
4. Bekkink MO, Farrell SE, Takayesu JK. Interprofessional communication in the emergency department: residents’ perceptions and implications for medical education. Int J Med Edu. 2018;9:262–270. doi:10.5116/ijme.5bb5.c111
5. Eisenmann D, Stroben F, Gerken J, et al. Interprofessional emergency training leads to changes in the workplace. West J Emerg Med. 2018;19:185–192. doi:10.5811/westjem.2017.11.35275
6. Wilbur L, Chisholm CC. Interprofessional education and collaboration: a call to action for emergency medicine. Acad Emerg Med. 2014;21(7):833–834. doi:10.1111/acem.12404
7. Carne B, Kennedy M, Gray T. Review article: crisis resource management in emergency medicine. Emerg Med Australas. 2012;24:7–13. doi:10.1111/j.1742-6723.2011.01495.x
8. Homma Y, Norii T, Kanazawa T, et al. A mini‐review of procedural sedation and analgesia in the emergency department. Acute Med Surg. 2020;7:e574. doi:10.1002/ams2.574
9. Sauter TC, Hautz WE, Hostettler S, et al. Interprofessional and interdisciplinary simulation-based training leads to safe sedation procedures in the emergency department. Scand J Trauma Resusc Emerg Med. 2016;24(1):97. doi:10.1186/s13049-016-0291-7
10. McManus NM, Offman R, Oetman JD. Emergency department management of COVID- 19: an evidence-based approach. West J Emerg Med. 2020;21:32–44. doi:10.5811/westjem.2020.8.48288
11. Smidt A, Balandin S, Sigafoos J, et al. The Kirkpatrick model: a useful tool for evaluating training outcomes. J Intellect Dev Disabil. 2009;34:266–274. PMID: 19681007. doi:10.1080/13668250903093125
12. Partecke M, Balzer C, Finkenzeller I, et al. Interprofessional learning - development and implementation of joint medical emergency team trainings for medical and nursing students at Universitätsmedizin Greifswald. GMS J Med Edu. 2016;33:32. doi:10.3205/zma001031
13. Yang L-Y, Yang YY, Huang CC, et al. Simulation-based inter-professional education to improve attitudes towards collaborative practice: a prospective comparative pilot study in a Chinese medical centre. BMJ Open. 2017;7:e015105.
14. Bashir K, Farook KS, Thomas SH. The learning preferences of millennial emergency medicine residents in Qatar. Int J Med Edu. 2019;10:136–137. doi:10.5116/ijme.5d1b.ae92
15. Bashir K, Thomas S. Educational approach of blended learning in teaching benign paroxysmal positional vertigo in an emergency department. J Coll Physicians Surg Pak. 2020;30(3):299–303. doi:10.29271/jcpsp.2020.03.299
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.