Back to Journals » Journal of Multidisciplinary Healthcare » Volume 12
Interprofessional communication in a sociohierarchical culture: development of the TRI-O guide
Authors Claramita M ![]() , Riskiyana R, Susilo AP
, Riskiyana R, Susilo AP ![]() , Huriyati E, Wahyuningsih MSH
, Huriyati E, Wahyuningsih MSH ![]() , Norcini JJ
, Norcini JJ
Received 3 December 2018
Accepted for publication 18 January 2019
Published 14 March 2019 Volume 2019:12 Pages 191—204
DOI https://doi.org/10.2147/JMDH.S196873
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Video provided by Mora Claramita.
Views: 1059
Mora Claramita,1 Rilani Riskiyana,1 Astrid Pratidina Susilo,2 Emy Huriyati,3 Mae SH Wahyuningsih,4 John J Norcini5
1Department of Medical, Health Professions Education and Bioethics, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia; 2The Indonesian College of Health Professions Education (Iam-HPE) and The Indonesian Skills Laboratory Network and Development (ISLaND), Yogyakarta, Indonesia; 3Department of Health Nutrition, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia; 4Department of Pharmacology and Therapy, Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia; 5FAIMER Institute, Philadelphia, PA, USA
Objectives: Interprofessional education (IPE) and collaborative practice are essential for patient safety. Effective teamwork starting with partnership-based communications should be introduced early in the educational process. Many societies in the world hold socio-hierarchical culture with a wide power distance, which makes collaboration among health professionals challenging. Since an appropriate communication framework for this context is not yet available, this study filled that gap by developing a guide for interprofessional communication, which is best suited to the socio-hierarchical and socio-cultural contexts.
Materials and methods: The draft of the guide was constructed based on previous studies of communication in health care in a socio-hierarchical context, referred to international IPE literature, and refined by focus group discussions among various health professionals. Nominal group technique, also comments from national and international experts of communication skills in health care, was used to validate the guide. A pilot study with a pre–posttest design was conducted with 53 first- and 107 fourth-year undergraduate medical, nursing, and health nutrition students.
Results: We developed the “TRI-O” guide of interprofessional communication skills, emphasizing “open for collaboration, open for information, open for discussion”, and found that the application of the guide during training was feasible and positively influenced students’ perceptions.
Conclusion: The findings suggest that the TRI-O guide is beneficial to help students initiate partnership-based communication and mutual collaboration among health professionals in the socio-hierarchical and socio-cultural context.
Keywords: cross-cultural communication, interprofessional communication, interprofessional education, role-play, constructive feedback, wide power distance
Introduction
Interprofessional education (IPE) is considered important for effective health care and patient safety.1 It supports effective teamwork through development of shared values, ethics, and responsibilities with two-way communication and understanding of team dynamics.2 Interprofessional collaborative competences and frameworks have been established in several developed western countries3 and among the competencies, communication skill is perceived to be the key to effective interprofessional practice.4–6 It plays important roles in determining the effectiveness of teamwork that is associated with improved patient safety.7 In contrast, poor communication in interprofessional health care teams is associated with health care delays, which may harm the patient.8 Therefore, interprofessional communication skills training to undergraduate and postgraduate students is necessary to prepare graduates to be able to work in collaboration.
There have been several training frameworks aimed at improving team communication including Team Strategies and Tools to Enhance Performance and Patient-Safety,9 Crew Resource Management,10 and Interprofessional Team Reasoning Framework.11 These frameworks are useful to develop team building and leadership and describe generic interprofessional communication. Although proven effective in improving communication among health professionals, ie, using the SBAR (Situation, Background, Assessment, Recommendation) method,12 the best application of these frameworks in a wide power distance context or socio-hierarchical gaps is not clear. Recent study from Indonesia, exploring the attitude perceptions of health professionals, shows the lack of interprofessional communication due to limited understanding on patient-centered care, lack of face-to-face interaction, unequal decision-making, and misunderstanding about specific roles and responsibilities.13 For that particular study, the presence of the wide power distance or socio-hierarchical gaps between health professionals was clear.13
This power distance phenomena explain the relational gap in a society, ie, between those who are seen in higher positions (eg, teachers, parents, and health professionals, especially physicians) and those in the lower positions (eg, students, children, patients, and the nonphysician health professionals).14–16 These social gaps create a strong nonverbal politeness intended to avoid conflict and maintain harmony. Accordingly, people use indirect communication more than straightforward messaging. Therefore, physician–nonphysician and health professional–patient communications tend to be one way instead of effective dialog. For example, when two health professionals do not agree with each other upon a patient’s treatment plan, the one in the perceived lower social hierarchy often chooses to not speak to avoid conflict. As a result, it threatens patient safety.17
Other effect of socio-hierarchical gaps relates to a desire for group communication (eg, family or community) instead of individuals to avoid individual conflict. Interestingly, previous work in the Southeast Asian context indicates that decision-making is more heavily influenced by the family or community members than by individual preferences.18–21 In this respect, health professionals need to balance the participation of the family or community with the patients’ individual rights.
Based on the Hofstede’s global study of cultural dimensions underlying relationships between people across nations, there are many non-western countries in Asia, Africa, and the Middle East, and they hold high socio-cultural gaps due to wide “power distance” dimensions (where people accept and expect unequally distributed “power”).15 Regions with wider socio-cultural gaps contain the most highly populated countries globally and notably, and they also have very high rates of emigration. Therefore, health care providers from many countries will be expected to deal with the challenges of passive roles of patients, and the norm of one-way patient–provider communication style may threaten patient safety.16,17
Overcoming these socio-hierarchical gaps requires more partnership-based communications, underpinned by trust, equity, and two-way partnership dialogs.16,17 Unfortunately, high patient loads and restricted time for consultation often lead by necessity to one-way communication. Moreover, patients and physicians are unprepared for partnership-based communication because of gaps in educational background and lack of communication skills training for health professionals.16,17
Previous studies in the form of publications and theses from this cultural context found the application of partnership-based communication skills guides useful for health professional–patient communication.22–25 This study aimed to develop a culturally relevant partnership-based IPE communication skills guide and test its applicability with undergraduate students from three different study programs.
Materials and methods
Figure 1 depicts the steps for both the development of the guide and the subsequent applicability and feasibility study (see Tables 1 to 5).
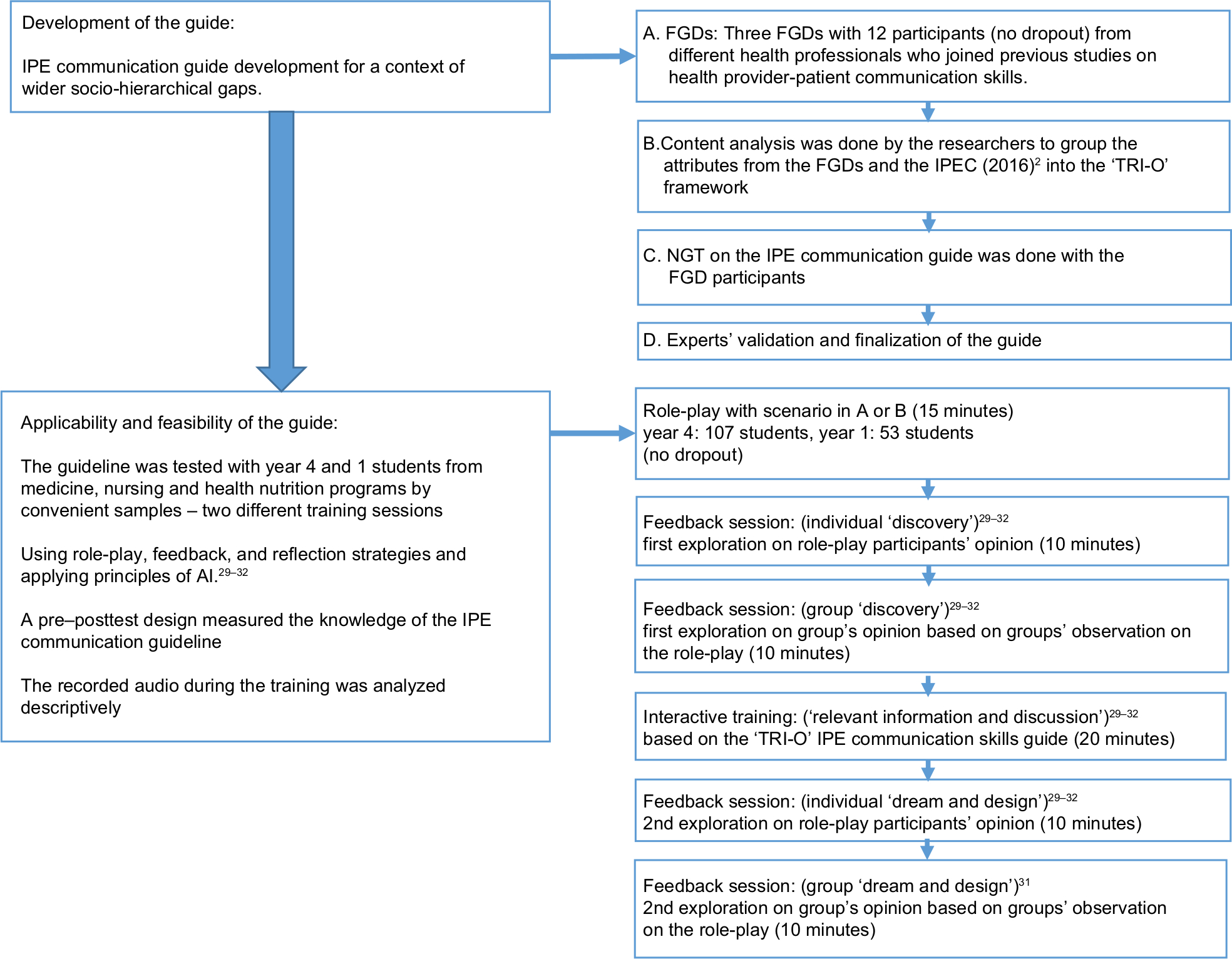 | Figure 1 Procedures of this study. Abbreviations: AI, appreciative inquiry; FGDs, focus group discussions; IPE, interprofessional education; NGT, nominal group technique; TRI-O, open for collaboration, open for information, open for discussion. |
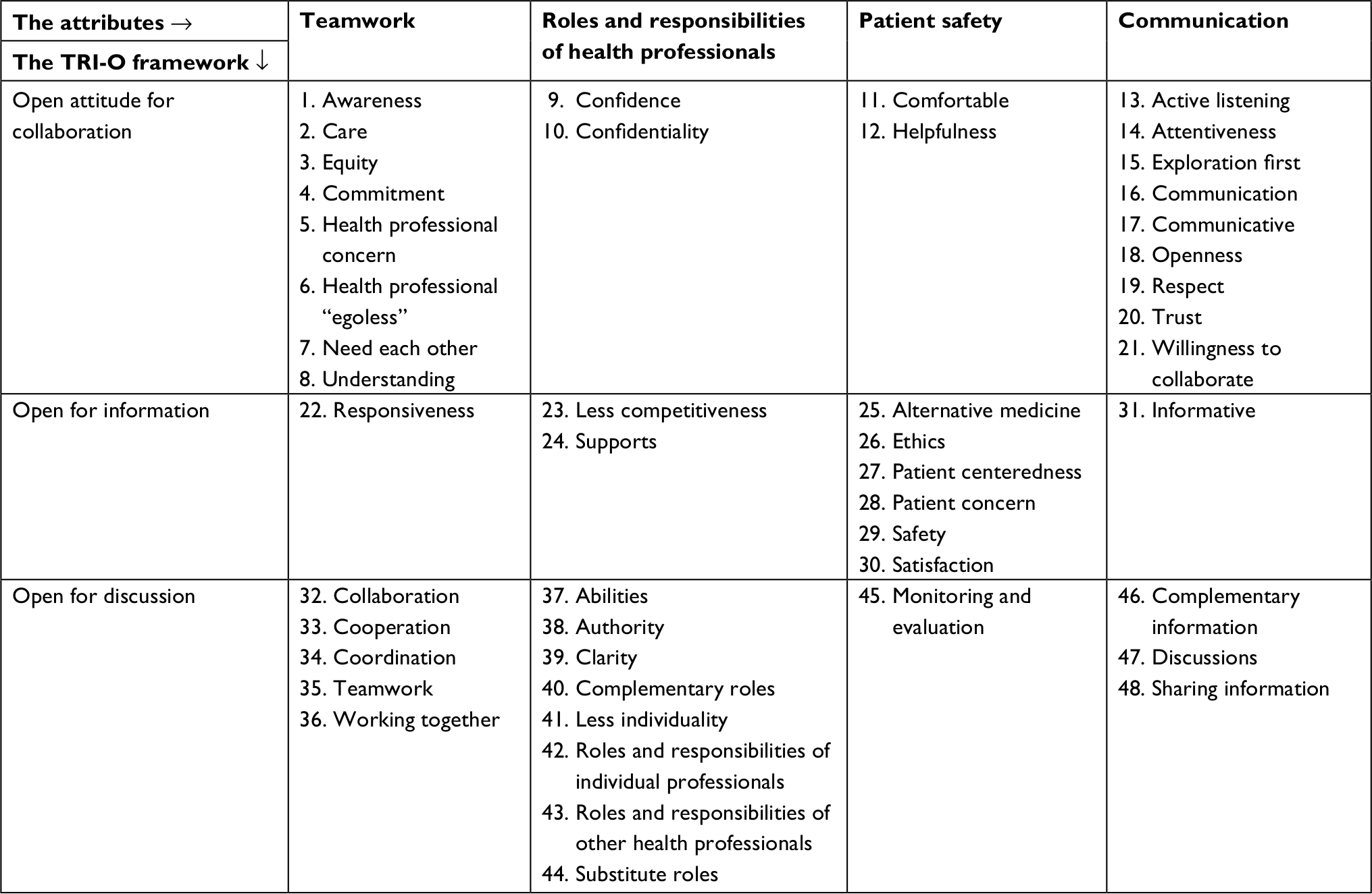 | Table 1 Attributes of IPE communication skills in the context of wider socio-cultural gaps in four initial categories and grouped into three “O” framework (TRI-O) Abbreviation: TRI-O, open for collaboration, open for information, open for discussion. |
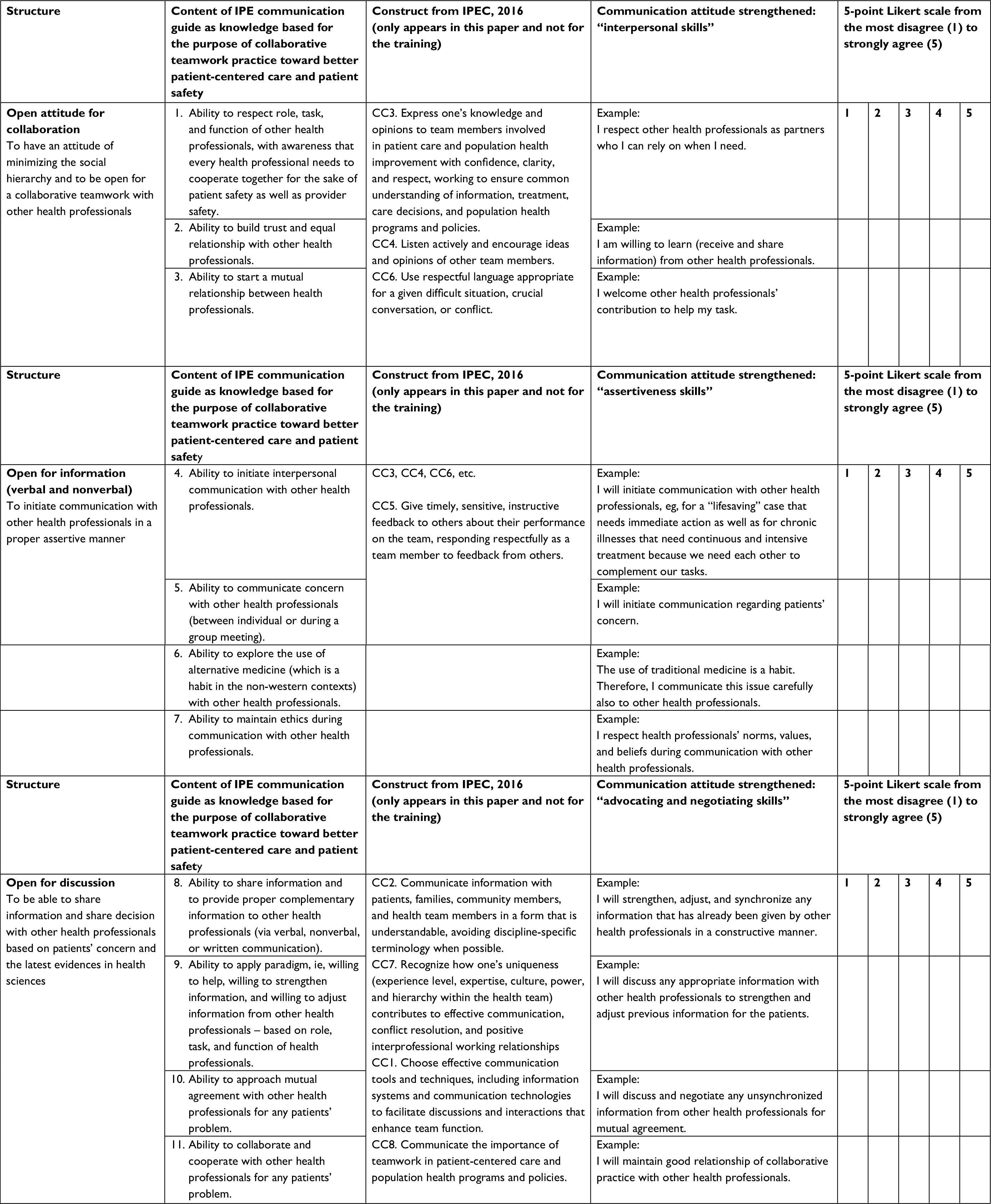 | Table 2 A guide of IPE communication developed in this study Abbreviation: IPE, interprofessional education. |
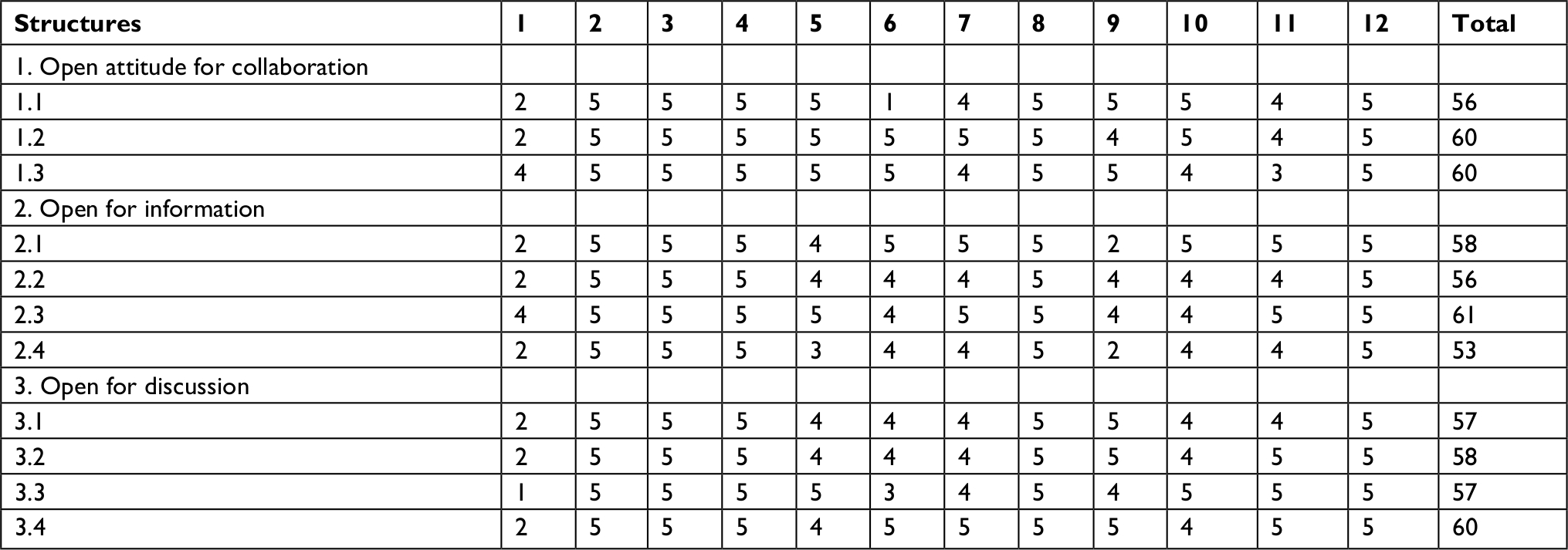 | Table 3 Results of the NGT Abbreviation: NGT, nominal group technique. |
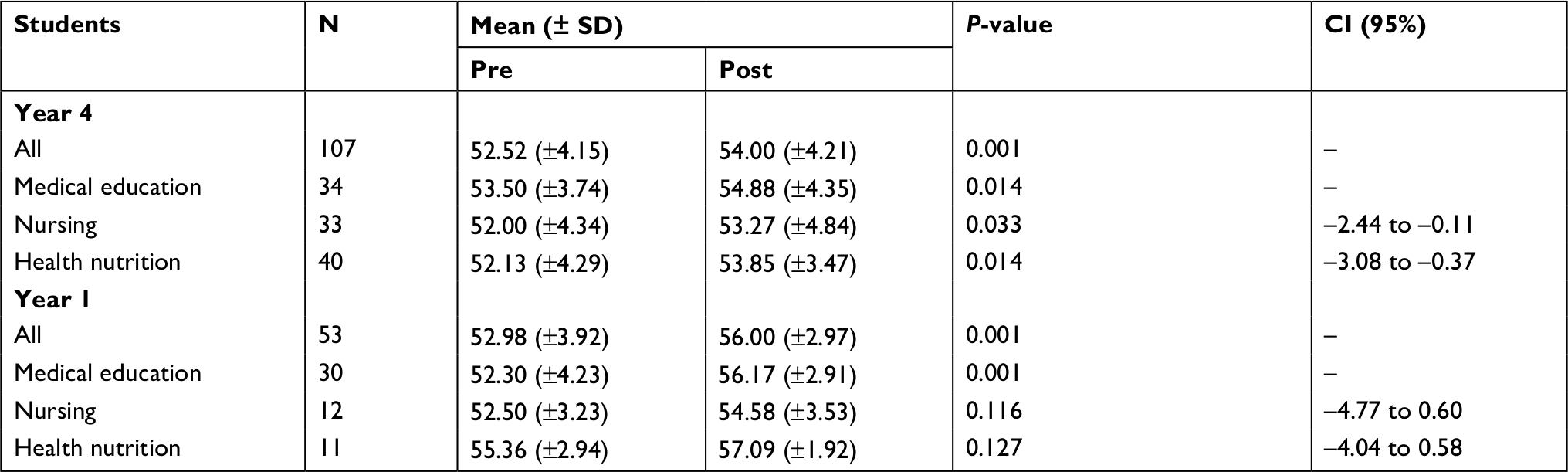 | Table 4 Pre–posttest results on year 4 and 1 students’ perceptions before and after training using the TRI-O IPE communication guide Note: Paired sample t-test, significant if P<0.05. Abbreviation: TRI-O, open for collaboration, open for information, open for discussion. |
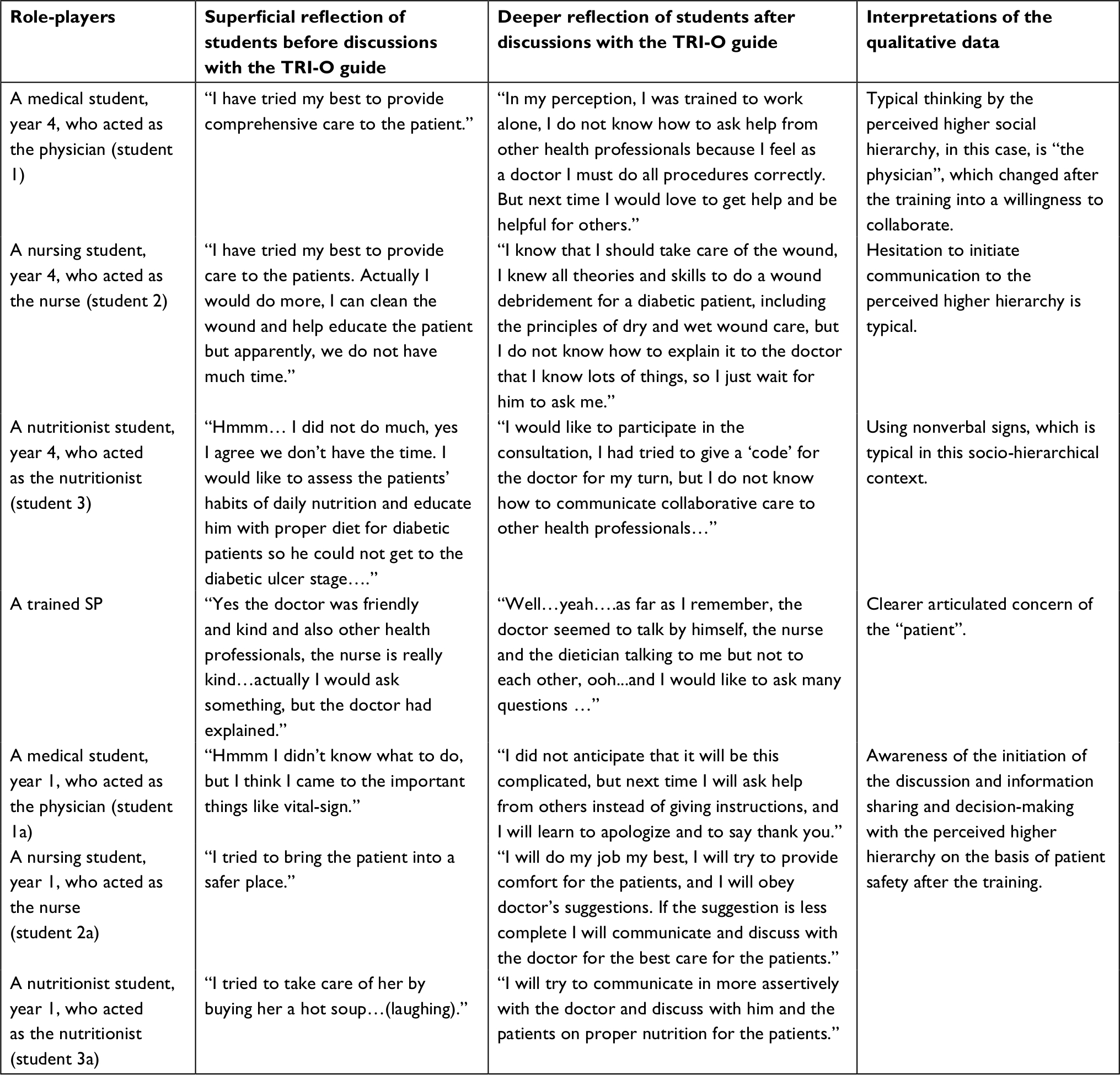 | Table 5 Perceptions of students, years 4 and 1, before and after training using the TRI-O guide Abbreviations: SP, simulated patient; TRI-O, open for collaboration, open for information, open for discussion. |
Development of the guide
The development of a draft IPE communication guide for health professionals in socio-cultural and socio-hierarchical contexts was done based on participatory approaches with different health professionals on three focus group discussions (FGDs). Each FGD was composed of physicians, nurses, nutritionists, and pharmacists, who were mid-career academicians/clinicians and involved in previous studies of communication skills.22–25 Three participants from each profession (n=12) with a male/female ratio of 5:7 between the ages of 40–60 years attended the FGDs. All participants had doctorate degrees with one professor from medicine and one from pharmacy. They were lecturers from five of the oldest and most established faculties of medicine in Indonesia. All the FGDs were conducted in a lecture room at a Faculty of Medicine.
The participants were previously involved in the development of communication guides for their individual health professions. Specifically, guides were developed for doctor–patient,22 nurse–client,25,26 nutritionist–client,23 and pharmacist–client communications.24 Notably, the guide for physicians referred to “patients” while the other professions referred to “clients”. All of the guides were structured around the communication skill set tasks of the “greet–invite–discuss” model of communications. The only exception was the nurses’ guide, who added the step of “ready” prior to “greet” based on the well-known communication skills sequences in that profession.25,26
The guiding questions for the FGDs were as follows: “What basic communication skills do you think are important for an IPE communication guide and explain why?” Each of the FGDs was lasted until no new ideas were generated by the participants/saturation (generally 40–50 minutes).22–25 The results were recorded by two assistants and then transcribed within 48 hours. Given these data, the authors conducted a manual content analysis.27 These were turned into a draft guide within the context of previous work and organized around the partnership-based communication model22–25 that is suitable for the cultural context explained in this study, also based on an international IPE guide2 (Tables 1 and 2).
This draft was submitted to the same groups applying nominal group techniques (NGTs)28 (Table 3). They were instructed to study the guide independently and then the group discussed the elements one by one. Afterward, each participant rated every item in the draft on a 5-point scale, where “1” was “disagree strongly” and “5” was “agree strongly”. Participants were told that items would be deleted if they received a mean rating <3.33 (the center value of the 5-point scale).
Upon calibration, the authors communicated with participants and ensured clarity of content. In particular, items with average ratings of <3 were highlighted so that participants could reconfirm their initial judgments. Finally, this draft was sent to communication experts from different professions from Indonesia and the Netherlands. Experts’ recommendations are incorporated in the final guide (Table 2).
Applicability and feasibility study
To test the applicability and feasibility of the guide in practice, we conducted a training by an open recruitment of medical, nursing, and nutrition students from years 1 (novice) and 4 (advanced) of their education. Students were from a Faculty of Medicine, Public Health and Nursing in Indonesia, which has the three study programs, and were from all 33 Indonesian provinces. Considering Indonesia is the fourth most populated country in the world, participants could be regarded as optimally varied. Before joining the training, students were given information about the study and written voluntarily consents were obtained.
The year 4 cohort (N=107) was composed of 35 medical students, 33 nursing students, and 40 health nutrition students. The main instruments were a perception scale (5-point Likert scale) based on the IPE communication guide and case scenarios for role-plays (Table 2; scenario A). A simulated patient underwent a briefing with the researchers before the session started. Figure 1 shows the lesson plan.
Scenario A and instruction for role-play of year 4 students
A patient (trained simulated patient) with type 2 diabetes mellitus made a routine physician visit to a primary care clinic. Past history revealed chronic hypertension and severe uric acid symptoms. The patient worried about a potential foot ulcer. A nurse who understood the treatment of diabetic ulcers was there with a dietician working in the same clinic.
The instruction was as follows: students 1, 2, 3 may have a role as a physician, nurse, and health nutritionist according to their future professions. Once the role-play begins, all students should comment on the role-play between students, using the TRI-O guide: What went well and what needs improvement in the communication between the three health professions? Students 1, 2, 3, 4 may reflect on the recommendations they have gained from the role-play. Finally, they all may reflect on the training based on the TRI-O guide.
A research assistant distributed the questionnaires and audiotaped the training process. We analyzed students’ perceptions concerning the IPE guide before and after the training using paired-sample t-tests.
The year 1 cohort (N=53) was composed of 30 medical students, 12 nursing students, and 11 health nutrition students. We used the same perception instrument, lesson plan, procedures, and analyses. The only difference was the scenario B, which was based on the limited prior knowledge of the year 1 students, who were only in their first week of school. A simulated patient (a student) was briefed by the researchers before the session. The role-play and feedback strategies were often used to train students in skills involving communication with patients.29–32
Scenario B and instruction for role-play of year 1 students
Ten students from different health professional programs should volunteer in the role-play. During an orientation day, in a very hot summer day, ten students (as one learning group) should queue on a line to start an activity. Suddenly, one of students falls down (as if she is in a syncope stage).
The instruction is as follows: students may have a role as a medical student, a nursing student, and a health nutritionist student, according to their study program. What will you do as a medical student/nursing student/health nutrition student, if one of your friends falls down? Use your own perceptions as a new student. All students should comment on the role-play: What went well and what needs improvement? Finally, they all may reflect on the training based on the TRI-O guide.
Ethics statement
This study was approved by the Committee of Ethics, Faculty of Medicine, UGM (no. EC: KE/FK/232/EC/2011–2015).
Results
Development of the guide
Although the focus groups were consistently directed to concentrate on communication, the discussions that took place ranged broadly, discussing general aspects of IPE. This is not surprising, given the central role communication plays in all facets of interprofessional practice. For example, “patient safety” is an important outcome of effective interprofessional communication. Likewise, teamwork and roles and responsibilities are two important attributes that IPE depends on, and the result of, good communication among professionals. Table 1 summarizes the attributes of good interprofessional practice, as distilled from the focus groups and categorized under the headings of patient safety, teamwork, roles and responsibilities, and communication.
To develop the first draft of the communication guide, the authors classified the items in Table 1 according to the previous communication skills model from the same context, but in this study, we relabeled the guide from the verbal communication tasks (the greet–invite–discuss) into a more attitudinal guide. The IPE communication skills guide in this study is called TRI-O, consisting of three “O”: 1) to have an “open attitude”, implies attitude of minimizing the social hierarchy in the study context and being open to working together with other health professionals, 2) to be “open for information” implies willingness to initiate communication with other health professionals in an assertive manner using active listening skills and open-ended questions, and by being aware of unspoken concern expressed through nonverbal cues, and 3) to be “open for discussions” implies sharing information and decisions with other health professionals based on patients’ concerns and on the latest evidences in health sciences via two-way dialogs.
For example, the attributes as summarized in Table 1 of awareness, care, commitment, equity, health professional concerns, health professional egoless, need each other, understanding, confidence, confidentiality, comfortable, helpfulness, active listening, attentiveness, exploration first, communication, communicative, openness, respect, trust, and willingness to collaborate were put in the Open attitude for collaboration” section in the TRI-O guide. These became three statements as summarized in Table 2:
- Ability to respect roles, tasks, and functions of other health professionals with awareness that all health professionals need to cooperate for the sake of patient safety and provider safety.
- Ability to build trust and equal relationships with other health professionals.
- Ability to start a mutual relationship between health professionals.
The other steps of the TRI-O development follow this example.
The three steps of TRI-O should be used in each encounter, with the emphasis on “open attitude for collaboration” at the beginning of the encounter, “open for information” in the middle, and “open for discussion” near the end. The communication items in IPEC (2016)2 were reorganized according to these steps and included in the final guide. For example, “communicating information to the patients and families…” was an early consideration in IPEC (CC2), but we consider it as part of the “open for discussion” step in the guide. The “share information and share decisions” was regarded as part of the final step in the guide. In contrast, the “respect” item of the IPEC (CC6) was moved forward into the “open attitude for collaboration” step of the guide. Figure 2 illustrates the gradual increasing complexity of the three steps of the TRI-O guide as introduced in an educational program.
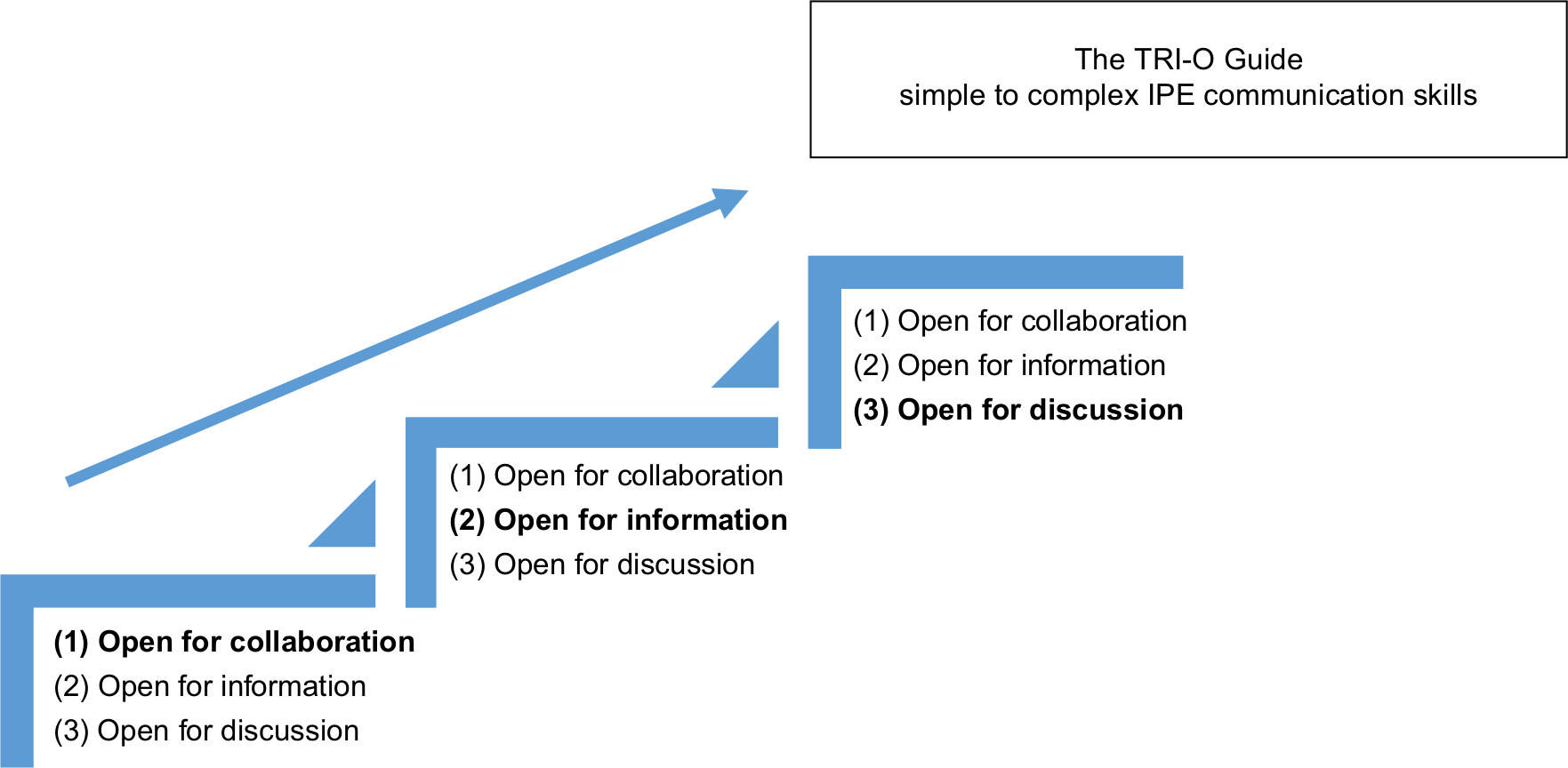 | Figure 2 Illustration of the use of the IPE TRI-O communication guide in the study. Abbreviations: IPE, interprofessional education; TRI-O, open for collaboration, open for information, open for discussion. |
The draft guide was submitted to the same FGD’s participants for rating, and the results are summarized in Table 3. An overall mean score of 57.81 (out of total value of 60) and an individual mean score of 4.81 per individual (out of 5) showed high agreement among the participants. As summarized in Table 3, the first participant (rater 1) gave lower ratings than the other participants and rater 6 gave the lowest score for the “partnership between health professionals” item. Both of the participants were found to be the physicians, and the authors confirmed that these results were an accurate appraisal of their perceptions.
There is no way of having a partnership relation with other health professionals because we have different tasks (Respondent No. 6).
The experts commented on the scenarios A and B:
Both scenarios represent the daily working context of health professionals with simple degree of cases. To consider ‘simple to complex’ learning, a role-play could start with only two health professionals from different professions. Then the next role-play could involve more than 2 health professionals.
We could also use simulated professionals (simulated physicians, simulated nurses, and simulated physiotherapist). It is important to divide roles among students. We must consider students’ prior knowledge. Thus, it is important to distinguish different scenarios for different level of students. The advantage in this study is that you involve many health professions in the role-play. Students could act as themselves whom study a profession.
Applicability and feasibility study
Table 4 summarizes the mean, SD, and the results of the t-tests of the year 1 and 4 students. As a group, the students showed statistically significant improvements in their perceptions following interprofessional communication skills training. The same was true for each of the different disciplines. For year 1 students, although the positive improvement was the same for the nursing and nutritionist students, it did not reach a level of statistical significance, probably due to the relatively smaller group sizes.
To stimulate reflection and follow-up plans based on role-plays, year 4 students were asked to reflect on their experiences of the ideal IPE communication. Overall reflection is presented in Table 5. Next, in the training, was all students were asked to share what they observed during the role-play as listed below:
- When a simulated patient came, a nursing student greeted the patient in a nice manner and then asked the main complaint while taking basic vital signs.
- The nursing student then referred the patient to the medical student.
- The medical student carefully examined the patient starting from history taking and complete physical examinations.
- When all the data were gathered from the simulated patient, the medical student started the patient education and counseling process.
- However, there was not much to do for the nursing student and the nutrition student during that process.
- We can observe the way nursing and nutrition students’ body languages that leaning toward the medical student, waiting for a turn to participate in the consultation.
- The nonverbal of waiting for a turn to participate in a consultation was also shown by the simulated patient.
- The simulated physician seemed to have a physician-centered consultation.
- Did he notice how other health professionals were waiting for their turn?
- The patient also seemed to wish to express something. Who do we know who does what and when?
The list then discussed based on the TRI-O guide is summarized in Table 2. After hearing the overall discussion and reflections, students moved from superficial awareness into deeper awareness of the appropriate IPE communication as summarized in Table 5.
During the summary phase, discussions with the fourth-year students reflected the action plan:
We know that we could not work alone. By working with other health professionals, we will get somebody to remind us the importance of patient-safety.
It may be better to always be exploring the needs first rather than direct the education.
We understand now that we should communicate our thinking to each other and that all tasks should have a spirit of a ‘complementary’ of each other’s roles.
We replicated this process with the first-year students, initially asking them to do the role-play as the professionals of their study program (physician/nurse/nutritionist), and as a student who simulated fainting. Their initial reflections revealed their limited awareness of the ideal interprofessional communication (Table 5). The process was followed by asking other participants about what they observed during the role-play as listed below:
- When a student fell down, two nursing students immediately took their friend to the nearest chair or shady spot and were trying to provide an open air for better breathing.
- A medical student said (shouting): “Measure the pulse!”
- Another medical student said (shouting): “Who knows this lady? Did she have a specific illness?”
- Another medical student said (shouting): “Give her a sugary liquid.”
- A nutritionist student tried to provide a sugary liquid and a hot soup (simulated).
- When the syncope student felt better, she said: “I did not have any breakfast.”
- Another medical student said: “You should have breakfast so you don’t get any problem!”
Afterward, we discussed the list using the IPE TRI-O guide as the ideal reference. Year 1 students also shifted from unawareness into awareness stage of openness to interprofessional collaboration and were able to develop action plans as presented below:
We did not understand our role very clearly, we felt lack of coordination, but the nursing students were quite responsive to take care of their syncope friend immediately to a proper place. The medical students also think the proper way, as well as the health-nutrition students. However, when somebody has a syncope condition, others should provide adequate open air environment and not to get closer to the patient without doing nothing. Who should take the lead? We hear only instructions from the medical students which could be transformed better into a thank you message, asking for help intonation with “please”, or direct the care plan in a more suggestive and motivating intonation.
Discussion
The TRI-O guide emphasizes the attitudinal framework underlying the verbal skill set of communication, which is applicable to overcome the wide socio-cultural and socio-hierarchical gap of interprofessional collaboration being addressed in this study. The content and skills emphasized in our work are similar to the international recommendations for interprofessional communication skills.2–6 The strength of the TRI-O communication framework used in this study relies on a set of simple to complex communication skills. Gradual complexity is important in training communication skills,29 which is not addressed in the IPEC guide (2016).2 The nature of health professional–patient communication is somewhat different from the interprofessional communication, therefore, rather than using the same verbal communication skill set from the previous communication skills guide, the “greet–invite–discuss”,22–25 the TRI-O emphasizes the openness attitude and awareness of all health professionals to work together.
The open attitudes emphasized throughout the guide will shift the previous norm of paternalistic culture into a more partnership-based communication. For example, in the “open for collaboration” step, the guide emphasized patient safety orientation, equity, and initiation of the mutual relationship. These are the fundamental bases of communication problems in the socio-hierarchical culture found in previous studies.13–18 Therefore, “open for collaboration” attitude is essential to move toward the partnership-based communication. The highlighted items are somewhat different in countries with a narrower gap of power, which already have equity of participation and the less problematic initiation of a closer relationship between people, ie, the western countries.3–12 The TRI-O with the “open for collaboration” will guide the health professionals in the study context to overcome cultural barriers: the anxiousness to speak up due to the wide gap of social distance, the hesitation to disturb others, and shame on their perceived potential mistakes,13–18 thus help initiate a partnership-based communication.
The “open for information” step in the TRI-O guide emphasized some of the unique characteristics of the socio-hierarchical culture that the health professionals should be aware of the presence of nonverbal subtleness, the belief of alternative medicine, and spiritual concern.16 These characteristics are less recognized in western culture, where articulation of concerns is a common norm and modern health care is highly systematic and trusted.3–12
In the “open for discussion” step, the guide emphasized the two-way information exchange, dialog, and complementary actions rather than blaming each other so that mutual agreement becomes shared decision-making. Again, we highlighted these items in the guide to move from the existing paternalistic culture to the partnership-based communication.19–21 In addition, the TRI-O approach could be seen as a motivational spirit to work together, ie, in a trio group.
During the guide’s development, we recognized the dominant position of the physicians. There were several contradictory statements expressed by the physicians during FGDs and their scores during the review process. In the initial phase of the guide development, physicians, who are at the top of the hierarchy in this context, may have trouble adopting the new partnership paradigm among health professionals. This phenomenon is also related to the original nature of the physicians’ communication style toward more biomedical issues than other health professionals who are more inclined toward patients’ psychological concerns.5,24
Interestingly, the perception of dominancy can be found in both year 1 and 4 medical students, indicating that this perception is strongly rooted in the culture. Domination of physicians may also be found in other parts of the world,5 but is more prominent in existing socio-hierarchical cultures.13–17 It was challenging for the medical students to actually experience and reflect on the IPE role-plays. Nevertheless, the results indicated a significant change toward working collaboratively with other health professionals after the IPE TRI-O communication skills training. Likewise, it was challenging for nonmedical students to be more assertive and prioritizing patient safety over maintaining harmonious relationship and avoiding conflicts with physicians. After the training, the nonmedical students also learned to participate more appropriately in patient care. This insight is highly important, because team awareness of shared mutual goals influences how individuals interact and communicate.1–6 Regardless of the professions, the students acquired a better understanding of the importance of safety as the ultimate goal of patient care, despite the socio-hierarchical gaps.
In the context of wider socio-hierarchical culture, such a small group discussions like the FGDs may be an effective way to train health professionals of an IPE communication skills based on reassuring exchange information that occurs. “Participatory learning” through involvement in the development of the learning guide seemed to be a powerful and subtle training strategy well suited to academicians and practicing health professionals.22 For the students, involvement in the role-play, feedback, and reflections are forms of participatory learning that proven beneficially in this study.
The IPE communication skills training in this study was quite effective in moving the students toward the new paradigm of collaboration among health professionals based on two important strengths. First, there was a “cycle of feedback” (a two-way information and reaction) based on role-playing.29–32 By actually observing their own simulated performances, students could better understand the reactions of both the simulated patients and the health professionals. Second, self-assessment following the experience, along with feedback from peers, provided important insights. Debriefing of “what happened” and “what should have happened” provided reflection opportunities using prior knowledge and moral sensibilities.29 After discussions among students, facilitators may do reinforcement and feedback based on the TRI-O guide. This process provided appreciative principles toward shared experiences to create positive and safe learning environment.30 The TRI-O model was introduced at an appropriate moment when the students felt knowledge gap.31,32
Limitations
Limitations of this study include how the pre–posttest design was conducted in a single institution and used a cross-sectional design rather than quasi-experimental research with a control group. However, we involved students from three different health professions and two levels of students and found that this guide was applicable for both levels. These findings certainly need to be replicated in other settings with similar cultural backgrounds. Such studies could incorporate different health professionals, more students, and even patients. However, in regard to the process of participative learning in this study with role-playing, feedback, and series of reflections, a similar transition from the “unconscious incompetence” to the “conscious incompetence” students will likely be demonstrated in a replication study.29–32 It may also be more useful to apply the training model we describe in clinical education or a longitudinal curriculum of IPE.33 Looking further, refining the way health care providers are educated could change the system and culture of the health care practice into a partnership-based fashion.
Conclusion
The TRI-O guide can be beneficial to improve interprofessional communication skills for undergraduate students in the socio-hierarchical cultures. Participatory learning through involvement in developing the communication guide seemed to be a powerful and subtle training strategy that well suited the practicing health professionals in this context. Students’ involvement in the role-play, feedback, and reflection is an applicable participatory learning within the context of the study.
Acknowledgments
Mora Claramita received the funding of a senior research grant from the Faculty of Medicine, Universitas Gadjah Mada (DAMAS/FK-UGM/2011–2015) and from the Ministry of Research, Technology, and Higher Education, Republic of Indonesia - the WCP Project 2018. The authors are grateful and respectful to our colleagues: Ardi Findyartini, MD, PhD (Universitas Indonesia), Professor Budi Ana Keliat, Ns.M.App.Sc., PhD (Universitas Indonesia), Professor Achir Yani S Hamid, MN, DNSc (Universitas Indonesia), Retno Pangastuti, DCN, M.Kes (Sardjito Hospital, Yogyakarta), Kusindrati Soedibyo, MCN, MARS (Cipto Mangunkusumo Hospital, Jakarta), Bondan Ardiningtyas, Apth., MSc, PhD (Universitas Gadjah Mada), and Jan Van Dalen, PhD (Maastricht University) who helped validate the guide in this study and related communication skills guides.
Disclosure
The authors report no conflicts of interest in this work.
References
World Health Organization. Framework for Action on Interprofessional Education and Collaborative Practice. Geneva: World Health Organization; 2010. Available from: http://apps.who.int/iris/bitstream/handle/10665/70185/WHO_HRH_HPN_10.3_eng.pdf;jsessionid=93D77481DA5DD0CF2860EEA901179039?sequence=1. Accessed July 8, 2015. | ||
Interprofessional Education Collaborative Expert Panel. Core Competencies for Interprofessional Collaborative Practice: Report of An Expert Panel (Update); 2016. Available from: https://aamc-meded.global.ssl.fastly.net/production/media/filer_public/70/9f/709fedd7-3c53-492c-b9f0-b13715d11cb6/core_competencies_for_collaborative_practice.pdf. Accessed July 8, 2015. | ||
Thistlethwaite JE, Forman D, Matthews LR, Rogers G, Steketee C, Yassine T. Competencies and frameworks in interprofessional education: a comparative analysis. Acad Med. 2014;89(6):p869–875. | ||
Suter E, Arndt J, Arthur N, Parboosingh J, Taylor E, Deutschlander S. Role understanding and effective communication as core competencies for collaborative practice. J Interprof Care. 2009;23(1):41–51. | ||
Weller JM, Barrow M, Gasquoine S. Interprofessional collaboration among junior doctors and nurses in the hospital setting. Med Educ. 2011;45(5):478–487. | ||
Kilminster S, Hale C, Lascelles M, et al. Learning for real life: patient-focused interprofessional workshops offer added value. Med Educ. 2004;38(7):717–726. | ||
Abu-Rish E, Kim S, Choe L, et al. Current trends in interprofessional education of health sciences students: a literature review. J Interprof Care. 2012;26(6):444–451. | ||
Peebles E, Subbe CP, Hughes P, Gemmell L. Timing and teamwork – an observational pilot study of patients referred to a Rapid Response Team with the aim of identifying factors amenable to re-design of a Rapid Response System. Resuscitation. 2012;83(6):782–787. | ||
Ferguson SL. TeamSTEPPS: integrating teamwork principles into adult health/medical-surgical practice. Med Surg Nursing. 2008;17(2):122. | ||
Robertson B, Kaplan B, Atallah H, Higgins M, Lewitt MJ, Ander DS. The use of simulation and a modified TeamSTEPPS curriculum for medical and nursing student team training. Simul Health 2010;5(6):332–337. | ||
Packard K, Chelal H, Maio A, et al. Interprofessional team Reasoning framework as a tool for case study analysis with health professions students: a randomized study. J Res Interprof Pract and Educ. 2012; 2(3)29. | ||
Gausvik C, Lautar A, Miller L, Pallerla H, Schlaudecker J. Structured nursing communication on interdisciplinary acute care teams improves perceptions of safety, efficiency, understanding of care plan and teamwork as well as job satisfaction. J Multidiscip Healthc. 2015;8:33–37. | ||
Lestari E, Stalmeijer RE, Widyandana D, Scherpbier A. Understanding attitude of health care professional teachers toward interprofessional health care collaboration and education in a southeast Asian country. J Multidiscip Healthc. 2018;11:557–571. | ||
Geertz C. The Religion of Java. Chicago, IL: University of Chicago Press; 1976. | ||
Hofstede Hofstede G G, Minkov M. Cultures and organizations: software of the mind. Intercultural Cooperation and Its Importance for Survival. 3rd ed. New York: McGraw Hill; 2010. | ||
Claramita M, Nugraheni MDF, van Dalen J, van der Vleuten C. Doctor–patient communication in Southeast Asia: a different culture? Adv Health Sci Educ Theory Pract. 2013;18(1):15–31. | ||
Susilo AP, Van Dalen J, Scherpbier A, Tanto S, Yuhanti P, Ekawati N. Nurses’ roles in informed consent in a hierarchical and communal context. Nurs Ethics. 2013;20(4):413–425. | ||
Mckinn S, Duong TL, Foster K, Mccaffery K. ‘I do want to ask, but I can’t speak’: a qualitative study of ethnic minority women’s experiences of communicating with primary health care professionals in remote, rural Vietnam. Int Equity Health. 2017;16(1):190. | ||
Tong WT, Lee YK, Ng CJ, Lee PY, Jenn Ng C, Lee YP. Factors influencing implementation of a patient decision aid in a developing country: an exploratory study. Implement Sci. 2017;12(1):40. | ||
Rimondini M, Mazzi MA, Deveugele M, Bensing JM. How do national cultures influence lay people’s preferences toward doctors’ style of communication? A comparison of 35 focus groups from an European cross national research. BMC Public Health. 2015;14(15):1239. | ||
Alden DL, Friend J, Lee PY, et al. Who decides: me or we? family involvement in medical decision making in eastern and Western countries. Med Decis Making. 2018;38(1):14–25. | ||
Claramita M, Susilo AP, Kharismayekti M, van Dalen J, van der Vleuten C. Introducing a partnership doctor-patient communication guide for teachers in the culturally hierarchical context of Indonesia. Educ Health (Abingdon). 2013;26(3):147. | ||
Utami AF, Claramita M, Huriyati E. Validity of Communication Guideline Using ‘greet-invite-discuss’ for the Dietetics. Yogyakarta: Repository of Universitas Gadjah Mada, Faculty of Medicine, Undergraduate Dietetics Program; 2012. | ||
Mulyono I, Claramita M, Susilo AP & Irawati S. Clients Communication Analysis Using RIAS. Surabaya: Repository of Universitas Surabaya, Faculty of Pharmacy, Magister Program in Pharmacy, 2014. | ||
Claramita M, Tuah R, Riskione P, Prabandari YS, Effendy C. Comparison of communication skills between trained and untrained students using a culturally sensitive nurse-client communication guideline in Indonesia. Nurse Educ Today. 2016;36(1):236–241. | ||
Potter PA, Perry AG. Fundamentals of Nursing. St Louis: Mosby Elsevier; 2004. | ||
Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. | ||
Mcmillan SS, King M, Tully MP. How to use the nominal group and Delphi techniques. Intl J Clin Pharm. 2016;38(3):655–662. | ||
Kurtz S, Silverman J, Draper J. Teaching and Learning Communication Skills in Medicine. Boca Raton: CRC Press; 2016. | ||
Boet S, Bould MD, Layat Burn C, Reeves S. Twelve tips for a successful interprofessional team-based high-fidelity simulation education session. Med Teach. 2014;36(10):853–857. | ||
Sandars J, Murdoch-Eaton D. Appreciative inquiry in medical education. AMEE guide No. 113. Med Teach. 2016;39(2):123–127. | ||
van de Ridder JM, Stokking KM, McGaghie WC, ten Cate OT. What is feedback in clinical education? Med Educ. 2008;42(2):189–197. | ||
Gilligan C, Outram S, Levett-Jones T. Recommendations from recent graduates in medicine, nursing and pharmacy on improving interprofessional education in University programs: a qualitative study. BMC Med Educ. 2014;4(1):52. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.