Back to Journals » Clinical Ophthalmology » Volume 16
Interpersonal Communication in Eye Care: An Analysis of Potential Impacts on Cataract Surgery Candidates’ Expectations and Behaviors
Authors Hellem A ![]() , LaBelle S, Matossian C
, LaBelle S, Matossian C ![]() , Karpecki P
, Karpecki P ![]()
Received 22 January 2022
Accepted for publication 3 March 2022
Published 5 April 2022 Volume 2022:16 Pages 1003—1008
DOI https://doi.org/10.2147/OPTH.S356895
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Amy Hellem,1 Sara LaBelle,1 Cynthia Matossian,2 Paul Karpecki3
1School of Communication, Chapman University, Orange, CA, USA; 2Matossian Eye Associates, Pennington, NJ, USA; 3Kentucky Eye Institute, Lexington, KY, USA
Correspondence: Amy Hellem, School of Communication, Chapman University, Orange, CA, USA, Tel +1-610-304-6746, Email [email protected]
Purpose: To identify cataract surgery candidates’ knowledge, beliefs, desires and emotions as they relate to cataract surgery generally as well as to their behavioral intent to adhere to a doctor-recommended pre-surgical ocular surface prep routine designed to improve refractive outcomes and prevent surgical complications.
Methods: This national, noninterventional, cross-sectional, mixed methods survey included 278 US adults ages 65 and older with no history of cataract surgery in either eye.
Results: Only 20% of participants said they want to have cataract surgery, and even fewer (8%) said they wish they could have cataract surgery right away. Fear was the predominant emotion in one out of every three respondents and was correlated with intention to delay having cataract surgery for as long as possible (r = 0.44). Fewer than 2% of participants said their doctors recommended home-health strategies to combat the risks of ocular surface disease preoperatively. However, most say they would use a pre-surgical prep kit if their doctor gave them one (87%), asked them to buy one (83%), or directed them to obtain one online (71%).
Conclusion: These findings negate the popular assumption that patients are in a hurry to have their cataract surgery right away and, therefore, may resist physician recommendations to address ocular surface disease pre-operatively.
Keywords: cataract surgery, dry eye treatment, ocular surface disease, pre-operative prep, hygiene, compliance
Introduction
Cataract surgery is one of the most commonly performed procedures in the United States with more than 3.6 million surgeries performed each year.1 Post-operatively, patients report better mental and emotional well-being, improved social interactions, enhanced facial recognition, and an easier time reading and watching television.2,3 Correspondingly, the vast majority of patients (95%) enjoy best-corrected visual acuity of 20/40 after surgery.2,4 What’s more, a recent analysis of the American Academy of Ophthalmology Intelligent Research in Sight (IRIS) Registry5 data from 1,824,196 patients who underwent bilateral cataract surgery revealed that more than 20% of patients had 20/20 uncorrected visual acuity (UCVA) post-operatively in the first and/or second eye.6
With this in mind, it’s no surprise that today’s cataract surgery patient is thought to have high expectations, potentially anticipating post-operative spectacle-free vision.7 Such patient expectations are often attributed to the paradigm shift made possible by the very technological advances that have made the premium refractive outcomes described above so common. The assumption is that, as visual outcomes improve in more and more patients, expectations go up for the cataract community at large and all patients begin to demand more. The trouble with this hypothesis is that there is no evidence to support it. No investigation to date has linked cataract surgery outcome trends with specific patient behavior, such as demanding more of the surgeon or refusing to adhere to a prescribed treatment regimen, for example. In short, causal relationship claims of this nature are entirely anecdotal. To address this research gap, the following mixed methods investigation aims to identify cataract surgery candidates’ knowledge, beliefs, desires and emotions as they relate to cataract surgery generally as well as to their behavioral intent to adhere to a doctor-recommended pre-surgical ocular surface prep routine designed to improve refractive outcomes and prevent surgical complications.
Materials and Methods
This was a national, noninterventional, cross-sectional survey conducted in June 2021. Data were collected through a one-time, online, anonymous Qualtrics-based survey. Adults 65 years of age and older were recruited using purposeful sampling8 by Prime Panels.9 Exclusion criteria included a history of cataract surgery in either eye. Participants who qualified and provided informed consent completed the 15–20-minute questionnaire. The study protocol was approved by the Chapman University Institutional Review Board and all study methods and protocols comply with the Declaration of Helsinki.
The survey instrument was divided into two sections. Part 1, reported herein, was designed to quantitatively and qualitatively identify knowledge, beliefs and emotions as they relate to cataract surgery and to measure behavioral intent to adhere to a doctor-recommended pre-surgical ocular surface prep routine (see Table 1 for sample items). Part 2, to be reported elsewhere, was designed to conduct a full theoretical test of the Health Belief Model10 in the context of cataract surgery.
 |
Table 1 Sample Survey Items |
Desire to have cataract surgery, cataract surgery timing preferences, fear, visual expectations, awareness of risk, and intent to use a pre-surgical prep-kit if instructed to do so were measured on 5-point Likert scales. In addition, participants were asked to respond to an open-ended prompt: “In your own words, how would you describe cataract surgery?” Finally, demographic information was collected. Statistical analysis of quantitative items and scales was carried out using the Statistical Package of Social Science (SPSS) (version 27, IBM Corp). Thematic coding was performed for the qualitative item using NVivo (version 12, QSR International).
Results
A total of 278 US adults met the inclusion criteria (age 65 and older with no history of cataract surgery in either eye) and were included in the final sample. Participants were predominantly female (n = 160, 57.8%), White (n = 249, 89.6%) and retired (n = 224, 81.2%). The vast majority (>98%) report having some form of medical insurance, with most participants (79.3%) indicating that they are covered by Medicare (see Table 2 for detailed demographic information).
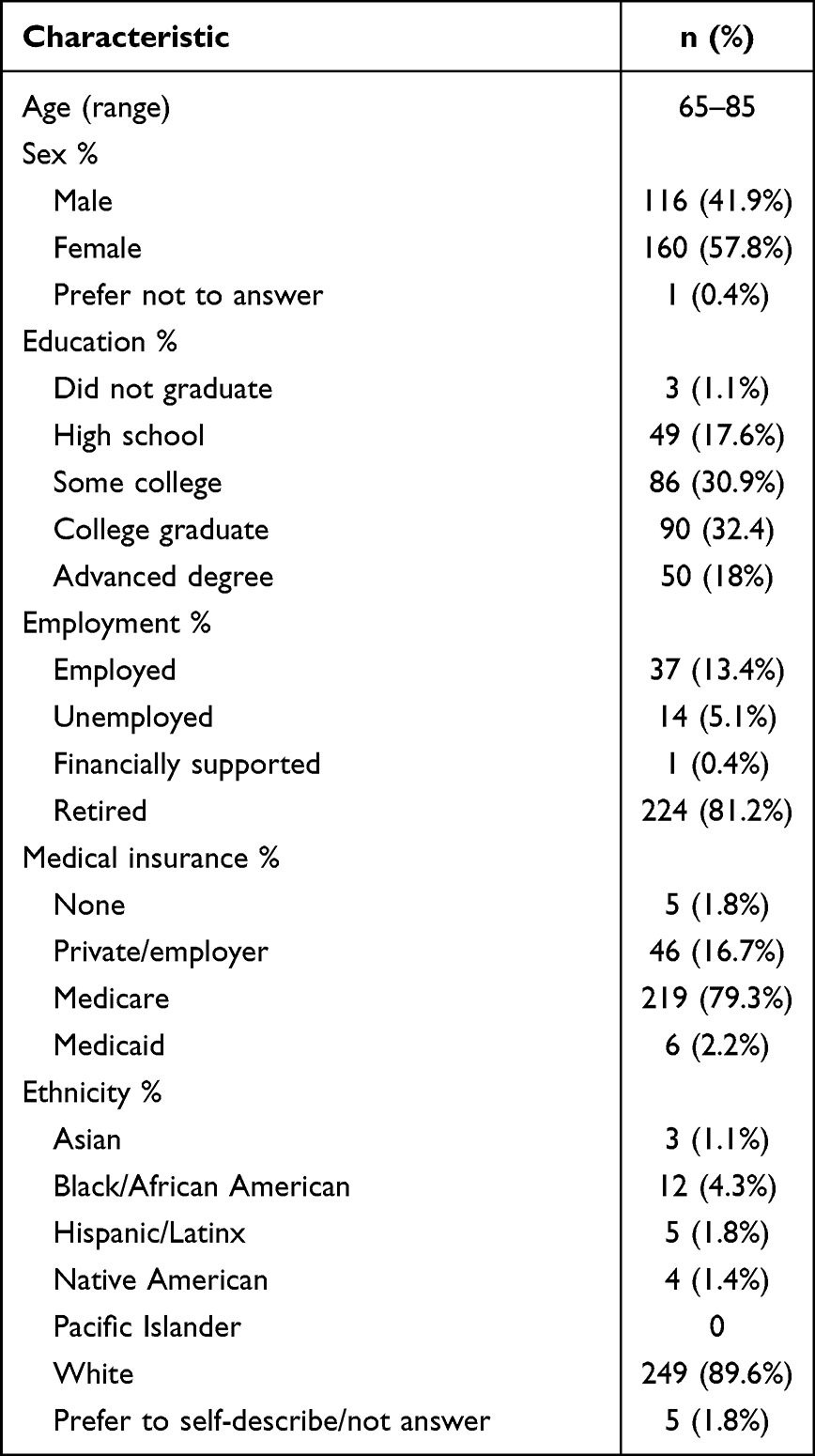 |
Table 2 Participant Demographics |
Descriptive statistics reveal mean desire to have cataract surgery was below the midline at 2.2 on a 5-point scale ranging from 1 = strongly disagree to 5 = strongly agree (n = 278, SD = 1.32). Similarly, mean urgency (ie, wish to have cataract surgery right away) was only 1.69 on the 5-point scale (n = 277, SD = 1.07). Conversely, fear of cataract surgery (n = 278, M = 2.72, SD = 1.36) and intention to delay having surgery (n = 278, M = 3.13, SD = 1.49) were notably higher. For complete item descriptions and frequencies, see Table 3.
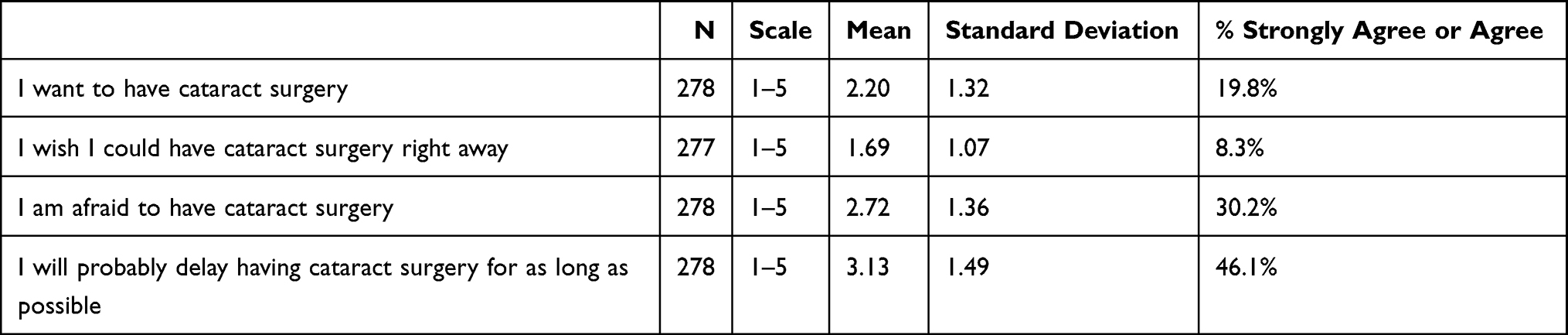 |
Table 3 Descriptive Statistics |
To measure post-operative visual expectations, participants were asked to describe how good they think their vision will be after they have cataract surgery. Most (32.7%) answered “I’m not sure” (n = 91). Other responses included “my vision will probably be similar to what it is now” (11.5%, n = 32), “my vision will be a little bit better than it is now” (18%, n = 50), “my vision will be a lot better than it is now” (21.9%, n = 61), “my vision will be so much better that I’ll only need glasses or contacts some of the time” (9.4%, n = 26), and “my vision will be so much better and I won’t need to wear my glasses or contacts anymore” (6.1%, n = 17).
Two risk awareness items measured on a 5-point scale (1 = not at all, 5 = a great deal) assessed beliefs about the degree to which ocular surface disease can damage overall ocular health (n = 275, M = 3.13, SD = 1.19) and impact vision (n = 278, M = 3.30, SD = 1.16).
A 5-point scale (1 = strongly disagree to 5 = strongly agree) was used to measure intent to adhere to doctors’ directions, which was operationalized as intent to use a pre-surgical prep-kit prior to cataract surgery if the doctor recommended it. Participants were presented with four scenarios: “If the doctor’s office gave me a pre-surgical prep kit and instructions on how to use it, I would use it as directed before having cataract surgery” (n = 275, M = 4.48, SD = 0.84); “If the doctor’s office asked me to purchase a pre-surgical prep kit at the front desk and gave me instructions on how to use it, I would use it as directed before having cataract surgery (n = 273, M = 4.36, SD = 0.92); “If the doctor’s office told me to go to the pharmacy to buy a pre-surgical prep kit, I would obtain one and use it as directed before having cataract surgery” (n = 274, M = 4.24, SD = 0.96); If the doctor’s office gave me a brochure with directions about how to order a pre-surgical prep kit online at the manufacturer’s website, I would obtain the kit and use it as directed before having cataract surgery. (n = 276, M = 4.02, SD = 1.10).
Finally, two dichotomous items measure whether patients recall their doctors discussing negative consequences associated with ocular surface disease and cataract surgery (8.3% yes, 91.7% no, n = 278) and whether their doctors have asked them to use a commercial eye hygiene product, such as an eyelid wipe, spray or compress (1.8% yes, 98.2% no, n = 278).
Bivariate two-tailed Pearson’s correlations were conducted to assess the relationships between variables of interest and found two positive correlations. First, there was a strong and statistically significant relationship (r = 0.66, p < 0.001) between patient desire to have cataract surgery and urgency (ie, wishing to have cataract surgery right away). Second, fear of having cataract surgery was moderately correlated with cataract surgery candidates’ intention to delay having surgery for as long as possible (r = 0.44, p < 0.001).
Regarding the qualitative analysis, iterative coding revealed three predominant themes: vision, fear and uncertainty. When asked to describe cataract surgery, most participants connected the procedure to vision (36%), followed by uncertainty (14%) and fear (8.5%). In many cases, codes overlapped. For example, one participant expressed the following: “I have no idea what cataract surgery is. I’m so fearful. I need to get more informed about it.”
Discussion
In the United States, half of all visual impairment in adults over age 40 is caused by cataracts,11 yet the current analysis reveals that many of these patients plan to defer care for as long as possible, creating a considerable public health concern since, globally, cataracts remain a leading cause of blindness.11 Notably, these findings negate the popular assumption that patients are in a hurry to have their cataract surgery right away and, therefore, may resist physician recommendations to address ocular surface disease pre-operatively. In fact, in this investigation, only 20% of participants said they want to have cataract surgery, and even fewer (8%) say they wish they could have cataract surgery right away. Not surprisingly, these two variables were positively correlated, which further elucidates the characteristics of this vocal minority.
In contrast to describing cataract surgery candidates as demanding and impatient, this data show that fear is a predominate emotion in one out of every three respondents, a finding that was further strengthened by qualitative analysis. In addition, although thematic data demonstrate that older adults understand that cataract surgery is intended to have visual benefits, the quantitative measures reveal that only 6.1% expect that their vision will be so much better after surgery that they will not need glasses or contact lenses anymore.
Another important takeaway from the qualitative investigation is that older adults experience significant uncertainty about cataract surgery. This contrasts with their accurate assumptions that ocular surface disease is damaging (as reported by 37% of participants) and can impact vision (as reported by 44% of participants). We use the term “assumptions” here because only 8% of participants report that their doctors have discussed these risks with them and even fewer (<2%) have recommended home-health strategies to combat it, despite a preponderance of evidence demonstrating that visual outcomes largely depend on the accuracy of pre-operative measurements, which may be off target in patients who have ocular surface disease.12,13 Furthermore, compromised ocular surface health can jeopardize astigmatism measurement accuracy14 and have negative impacts on post-operative comfort and susceptibility to infection.13 To that end, the imperative to proactively address ocular surface disease has been the focus of several recent reports that call attention to the fact that the incidence of ocular surface disease in patients presenting for cataract surgery is between 60% and 80%.12–16
With this in mind, in the current study, intention to adhere to doctor recommendations was operationalized as agreement to use a pre-surgical prep kit as directed. This measure was chosen since home lid hygiene, unlike prescription treatments and in-office therapies, can benefit most patients regardless of the severity of their disease. For example, use of a moist heat eye compress, lid wipes, and hypochlorous acid solution have been shown to improve ocular surface health and limit bacteria and can be performed in the weeks leading up to surgery.13
Since, as this study shows, patients who are afraid of cataract surgery are also more likely to delay having surgery for as long as possible, the authors question the extent to which a daily hygiene routine may empower patients, giving frightened patients greater agency and autonomy, in effect preparing them both emotionally and physically at a time when they might otherwise avoid proper care and delay surgery. Such analysis would prove exceedingly valuable and is strongly recommend as an area for future research, particularly in light of the fact that 87% of participants in the current study say they would use a presurgical prep kit if their doctor gave them one. In fact, even when obtaining a kit is more challenging or costly to the patient, most (73%) still say they would use it. Future directions might also investigate the role of personal autonomy and perceived efficacy when engaging in self-care in combination with in-office methods such as thermal pulsation or intense pulse light therapy.
This study has several limitations, beginning with the cross-sectional design, which restricts the authors’ ability to make causal claims. The use of behavioral intention as a surrogate for actual behavior is also a concern, since intentions translate into action only about half the time.17 A more robust experimental design is needed to untangle these two endpoints.
Finally, generalizability is compromised in this investigation by the fact that participants were mostly White and insured. Notably, IRIS data show that both race and insurance type are associated with worse outcomes,6 which likewise raises concerns about patients’ feelings and beliefs about surgery and the risks involved.
Conclusion
As trends in cataract surgery became increasingly refractive, there may be a tendency to heed the demands of the vocal minority, rather than consider the journey of the larger population. To that end, this investigation aimed to broadly identify patients’ beliefs and emotions as they relate to cataract surgery and measured willingness to adhere to a doctor-recommended pre-operative prep routine. Results provide a glimpse into the psyche of cataract candidates and offer insights that reveal patients’ dangerous tendency to avoid cataract care due to fear. However, evidence also reveals that most patients are compelled to do their part to improve outcomes. Due to participants’ expression of acceptance of at-home hygiene, combined with support in the medical literature for the use of eyelid wipes, hypochlorous acid spray and a moist heat eye compress in the days and weeks preceding surgery,12–14,18–21 the authors strongly recommend future study on the use of a pre-surgical prep-kit as a mechanism to reduce fear and delays in necessary eye care services.
Disclosure
Professor Amy Hellem reports grants from Bruder Healthcare, during the conduct of the study; personal fees from Bruder Healthcare, Johnson & Johnson, Allergan, and Zeiss, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Grzybowski A. Recent developments in cataract surgery. Ann Transl Med. 2020;8(22):1540. doi:10.21037/atm-2020-rcs-16
2. Moshirfar M, Milner D, Patel BC. Cataract surgery. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2021.
3. Lamoureux EL, Fenwick E, Pesudovs K, Tan D. The impact of cataract surgery on quality of life. Curr Opin Ophthalmol. 2011;22(1):19–27. doi:10.1097/ICU.0b013e3283414284
4. Nizami AA, Gulani AC. Cataract StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021.
5. American Academy of Ophthalmology. IRIS registry. Available from: https://www.aao.org/iris-registry.
6. Owen JP, Blazes M, Lacy M, et al. Refractive outcomes after immediate sequential vs delayed sequential bilateral cataract surgery. JAMA Ophthalmol. 2021;139(8):876–885. doi:10.1001/jamaophthalmol.2021.2032
7. Haldipurkar SS, Shetty V, Shah D, et al. Comparison of post-cataract surgery visual outcomes and quality of life in patients bilaterally implanted with multifocal intraocular lenses. Ophthalmol Ther. 2021;10(1):101–113. doi:10.1007/s40123-020-00321-2
8. Tracy SJ. Qualitative Research Methods. Wiley-Blackwell; 2019.
9. Chandler J, Rosenzweig C, Moss AJ, Robinson J, Litman L. Online panels in social science research: expanding sampling methods beyond Mechanical Turk. Behav Res Methods. 2019;51(5):2022–2038. doi:10.3758/s13428-019-01273-7
10. Rosenstock IM, Strecher VJ, Becker MH. Social learning theory and the health belief model. Health Educ Q. 1988;15(2):175–183. doi:10.1177/109019818801500203
11. Olson RJ, Braga-Mele R, Chen SH, et al. Cataract in the adult eye preferred practice pattern®. Ophthalmology. 2017;124(2):P1–p119. doi:10.1016/j.ophtha.2016.09.027
12. Epitropoulos AT, Matossian C, Berdy GJ, Malhotra RP, Potvin R. Effect of tear osmolarity on repeatability of keratometry for cataract surgery planning. J Cataract Refract Surg. 2015;41(8):1672–1677. doi:10.1016/j.jcrs.2015.01.016
13. Starr CE, Gupta PK, Farid M, et al. An algorithm for the preoperative diagnosis and treatment of ocular surface disorders. J Cataract Refract Surg. 2019;45(5):669–684. doi:10.1016/j.jcrs.2019.03.023
14. Matossian C. Impact of thermal pulsation treatment on astigmatism management and outcomes in meibomian gland dysfunction patients undergoing cataract surgery. Clin Ophthalmol. 2020;14:2283–2289. doi:10.2147/OPTH.S263046
15. Gupta PK, Drinkwater OJ, VanDusen KW, Brissette AR, Starr CE. Prevalence of ocular surface dysfunction in patients presenting for cataract surgery evaluation. J Cataract Refract Surg. 2018;44(9):1090–1096. doi:10.1016/j.jcrs.2018.06.026
16. Trattler WB, Majmudar PA, Donnenfeld ED, McDonald MB, Stonecipher KG, Goldberg DF. The prospective health assessment of cataract patients’ ocular surface (PHACO) study: the effect of dry eye. Clin Ophthalmol. 2017;11:1423–1430. doi:10.2147/OPTH.S120159
17. Sheeran P, Webb TL. The intention-behavior gap. Soc Personal Psychol Compass. 2016;10(9):503–518. doi:10.1111/spc3.12265
18. Stroman DW, Mintun K, Epstein AB, et al. Reduction in bacterial load using hypochlorous acid hygiene solution on ocular skin. Clin Ophthalmol. 2017;11:707–714. doi:10.2147/OPTH.S132851
19. Song P, Sun Z, Ren S, et al. Preoperative management of MGD alleviates the aggravation of MGD and dry eye induced by cataract surgery: a prospective, randomized clinical trial. Biomed Res Int. 2019;2019:2737968. doi:10.1155/2019/2737968
20. Eom Y, Na KS, Hwang HS, et al. Clinical efficacy of eyelid hygiene in blepharitis and meibomian gland dysfunction after cataract surgery: a randomized controlled pilot trial. Sci Rep. 2020;10(1):11796. doi:10.1038/s41598-020-67888-5
21. Peral A, Alonso J, García-García C, Niño-Rueda C, Calvo Del Bosque P. Importance of lid hygiene before ocular surgery: qualitative and quantitative analysis of eyelid and conjunctiva microbiota. Eye Contact Lens. 2016;42(6):366–370. doi:10.1097/ICL.0000000000000221
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.