Back to Journals » Cancer Management and Research » Volume 13
Interpectoral Lymph Node Dissection Can Be Spared in pN0/N1 Invasive Breast Cancer Undergoing Modified Radical Mastectomy: Single-Institution Experience from Mainland China
Authors Yan Y, Jiang L, Fang J, Dai Y ![]() , Chenyu X, Ding J
, Chenyu X, Ding J ![]()
Received 7 April 2021
Accepted for publication 22 June 2021
Published 27 July 2021 Volume 2021:13 Pages 5855—5863
DOI https://doi.org/10.2147/CMAR.S313971
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sanjeev K. Srivastava
Yun Yan,1 Li Jiang,2 Jianjiang Fang,2 Yi Dai,3 Xingzi Chenyu,3 Jinhua Ding4
1Department of Ultrasound, Ningbo Medical Center Lihuili Hospital, Ningbo, Zhejiang, 315000, People’s Republic of China; 2Department of General Practice, Ningbo Medical Center Lihuili Hospital, Ningbo, Zhejiang, 315000, People’s Republic of China; 3Ningbo University School of Medicine, Ningbo, Zhejiang, 315000, People’s Republic of China; 4Department of Breast and Thyroid Surgery, Ningbo Medical Center Lihuili Hospital, Ningbo, Zhejiang, 315000, People’s Republic of China
Correspondence: Jinhua Ding
Department of Breast and Thyroid Surgery, Ningbo Medical Center Lihuili Hospital, No. 1111, Jiangnan Road, Ningbo, Zhejiang, 315000, People’s Republic of China
Tel +86 13957498690
Email [email protected]
Purpose: Interpectoral lymph nodes (IPNs) are one of the lymphatic drainage pathways in breast cancer. However, the clinical significance of IPN dissection is controversial, and there is no international consensus regarding the management of IPN for resectable breast cancer. Our study aims to identify the independent predictors of IPN metastasis in invasive breast cancer (IBC) and provide some evidence for rational decision-making.
Methods: Data from 214 IBC patients who were treated with modified radical mastectomy (MRM) plus IPN dissection or biopsy in Ningbo Medical Center Lihuili Hospital were retrospectively reviewed. Univariate analysis and multivariate logistic regression analysis were used to analyse the correlations between IPN occurrence or metastasis and clinicopathological characteristics.
Results: The occurrence rate of IPN in overall population was 75.2%. Univariate analysis showed that tumour size, involvement of axillary lymph nodes (ALNs), histological grading, Ki67 index and molecular subtype were associated with the occurrence of IPN. However, involvement of ALN was the only independent predictor by multivariate logistic regression analysis. In 161 patients whose IPNs were detected, 46 (28.6%) patients had one or more metastatic IPNs. Univariate analysis showed that tumour size, involvement of ALN, oestrogen receptor status and molecular subtype were associated with IPN metastasis. However, involvement of ALN was the only predictor by multivariate logistic regression analysis. In total, 0%, 5.0%, 26.1% and 84.2% of pN0, pN1, pN2, and pN3 patients had metastatic IPNs, respectively.
Conclusion: The relatively low rate of IPN metastasis in patients with pN0/N1 breast cancer suggests that IPN dissection can be safely spared in patients with low tumour burden in axillary lymph nodes (pN0/N1), when MRM even breast conservation surgery is performed.
Keywords: breast cancer, interpectoral lymph node, axillary lymph node, metastasis
Introduction
Interpectoral lymph nodes (IPNs) were first reported by Grossman in 1896.1 Three years later, Rotter described these nodes in half of 33 surgical specimens from patients with breast carcinoma.2 Anatomically, IPNs are located between the pectoralis major and minor muscles in the interpectoral fascia and do not belong to axillary lymph nodes (ALNs) and may further drain into the central or subclavicular node groups representing a possible “skip pathway” for tumour cells to metastasize from the breast to level III nodes while bypassing levels I or II.3,4 Numerous studies have showed that sentinel lymph node biopsy (SLNB), instead of axillary lymph node dissection (ALND), has better cosmetic results5 and is associated with less arm and shoulder complications.6–8 However, in mainland China, ALND is still an essential surgical procedure for certain patients in whom cancer cells have spread heavily to axillary lymph nodes (ALNs) or who are unwilling to undergo SLN due to excessive anxiety.
The management of IPN has historically been controversial. Some surgeons held the view that IPN should be routinely dissected for breast cancer patients regardless of ALN status because as high as 4% of patients had IPN metastasis even in patients who had no metastatic ALNs,9 and IPNs have also been identified as a site of recurrence.4 However, other surgeons had moderate views that IPN dissection was only necessary for patients with locally advanced disease (large tumour or positive ALNs).10 Limited to rare high-quality studies of evidence-based medicine, the authoritative guideline of the National Comprehensive Cancer Network (NCCN) had no definite recommendation on the management of IPN for breast cancer patients. Whether IPN dissection or biopsy was performed often depended on the experience of the surgeons.
Regarding IPNs, several questions have not been answered until now. First, previous studies did describe the lower rate of IPN metastasis in patients without positive ALNs, and the much higher rate in patients with positive ALNs; however, these studies did not specify the possibility of IPN metastasis based on the tumour burden in the ALNs, and they simply drew the conclusion that IPN dissection was necessary for all patients with positive ALNs. Second, surgeons were greatly interested in the IPNs from the 1960s to 1990s, after which less attention had been paid to this field; especially in the era of SLNB, the value of IPNs dissection for patients who had no positive SLNs or 1 to 3 positive SLNs was unknown, and more studies are needed. Third, as a developing country, China’s mainstream population has the greatest number of breast cancer patients, and even in some underdeveloped areas, MRM is still the mainstream surgery; however, the study of IPNs in Chinese patients is still relatively deficient. Therefore, our study aimed to investigate the specific metastasis rates of IPN in Chinese breast cancer patients with different tumour burden in the axillas, to determine the predictors for IPN metastasis and to further provide some evidence for rational decision-making.
Materials and Methods
Patient Selection
The study obtained approval from the Institutional Ethics Committee of Ningbo Medical Center Lihuili Hospital (approval number KY2020PJ026). Informed consent was waived, because on the informed consent for surgery, there was a statement that data of patients could be used for clinical research and non-commercial in the future, and patients agreed. Data of patients were confidential, and the study protocol was conducted in accordance with the recommendations outlined in the Helsinki Declaration. Then, we collected and analysed the data of patients with IBC in our hospital between November 2014 and August 2018. MRM was performed on every patient, and INPs were removed separately. Exclusion criteria included the following: (1) metastatic breast cancer; (2) locally advanced breast cancer treated with neoadjuvant therapy; (3) breast cancer with less than 15 ALNs removed; (4) incomplete clinicopathological information.
Data Collection
Clinical and pathological data were collected from medical records of the patients included in the study. The data included the following: patient age, laterality and location of the tumour, tumour size, histological grading, numbers of ALNs and IPNs removed, numbers of ALNs and IPNs involvement, oestrogen receptor (ER), progesterone Receptor (PR), human epidermal growth factor receptor-2 (HER2) and Ki-67 label index. ER and PR assays should be considered positive if immunostaining is seen in more than 1% tumour nuclei.11 HER2 positivity was defined as either immunohistochemistry (IHC) 3+ or gene amplification by fluorescence in situ hybridization (FISH).12 Adjuvant chemotherapy, radiotherapy, endocrine therapy and anti-HER2 therapy were administered in appropriate patients according to currently available clinical practice guideline.
Statistical Analysis
Chi-square or Fisher’s exact tests were performed to assess associations between the rate of IPN occurrence or metastasis and categorical variables. Multivariate logistic regression analysis, including all variables from the univariate analysis that were associated with IPN occurrence or metastasis rate, was performed to test for factor independence. P <0.05 was considered to indicate statistical significance, and statistical test was two-sided. Hazard ratios (HRs) and 95% confidence intervals (CIs) were also calculated. Analyses were performed using SPSS v. 20.0 Software (SPSS,Chicago, IL, http://www.spss.com).
Results
Patient Characteristics
Between November 2014 and August 2018, 1213 breast cancer patients received surgical treatment. According to the exclusion criteria, 214 eligible patients were included in our study. Figure 1 shows the flow chart of the study. All patients were female, and the median age was 51 years, ranging from 34 to 71. The percentages of pathological stage I/II/III were 19.6% (42/214), 33.6% (72/214), 46.7% (100/214), respectively. Details of clinicopathological characteristics and demographic features are shown in Table 1. IPN was detected in 161 patients, and the IPN occurrence rate was 75.2% (161/214). Among 161 patients, the average number of IPNs removed was 1.4, ranging from 1 to 6. Of them, 103 patients had one IPN, 45 patients had two IPNs, 13 patients had three or more IPNs. The clinicopathological characteristics of 161 patients in whom IPN was detected are shown in Table 2.
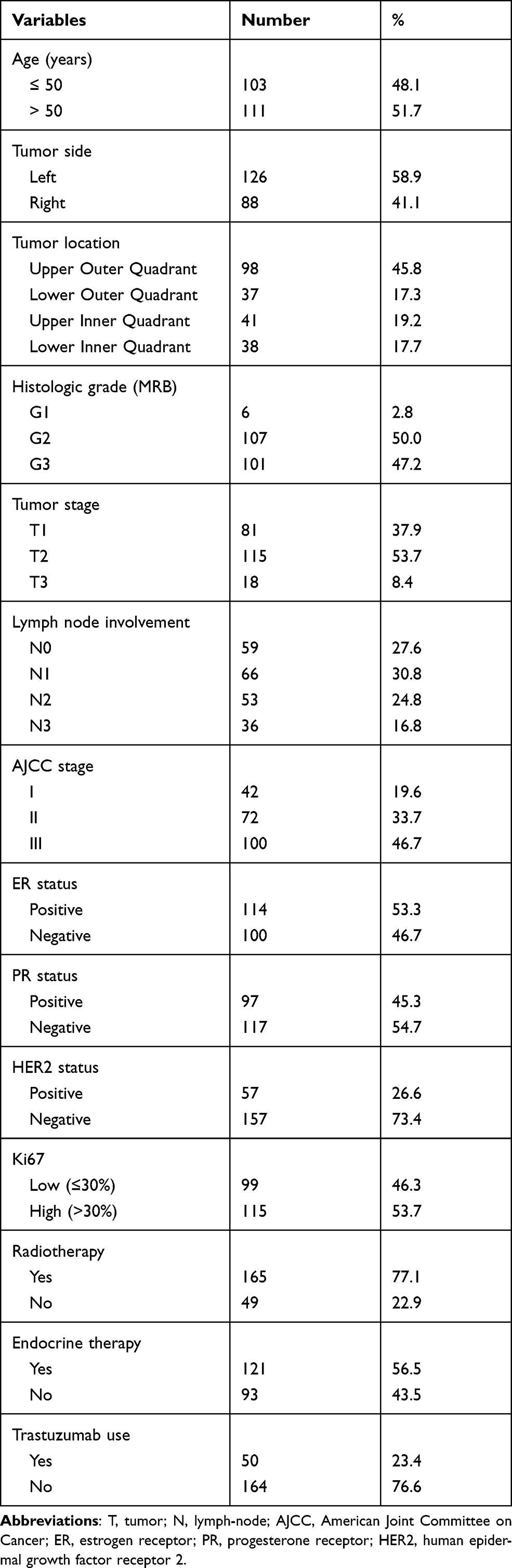 |
Table 1 Clinicopathologic Features of Patients Undergoing Modified Radical Mastectomy (N=214) |
 |
Table 2 Clinicopathologic Features of Patients with Interpectoral Lymph Node Occurrence (N=161) |
 |
Figure 1 Flow chart of the study. |
Predictors for IPN Occurrence
Univariate analysis found that tumour size, histological grading, ALN involvement, Ki67 label index and molecular typing were associated with IPN occurrence; however, multivariate logistic regression analysis found that only ALN involvement was an independent predictive factor for IPN occurrence (Table 3).
 |
Table 3 Univariate and Multivariate Analysis of Clinicopathological Factors Predicting IPN Occurrence (N=161) |
Predictors for IPN Metastasis
Among all 214 patients, 46 patients had one or more metastatic IPNs, and the IPN metastasis rate was 21.5% (46/214). In 161 patients in whom IPN had been detected, the IPN metastasis rate was 28.6% (46/161). In the 46 patients who had metastatic IPNs, 58 metastatic IPNs were detected, and the rates of one and two metastatic IPNs were 73.9% (34/46) and 26.1% (12/46), respectively.
Univariate analysis found that tumour size, ALN involvement, ER status and molecular typing were associated with IPN metastasis; however, multivariate logistic regression analysis found that only ALN involvement was an independent predictive factor for IPN metastasis (Table 4).
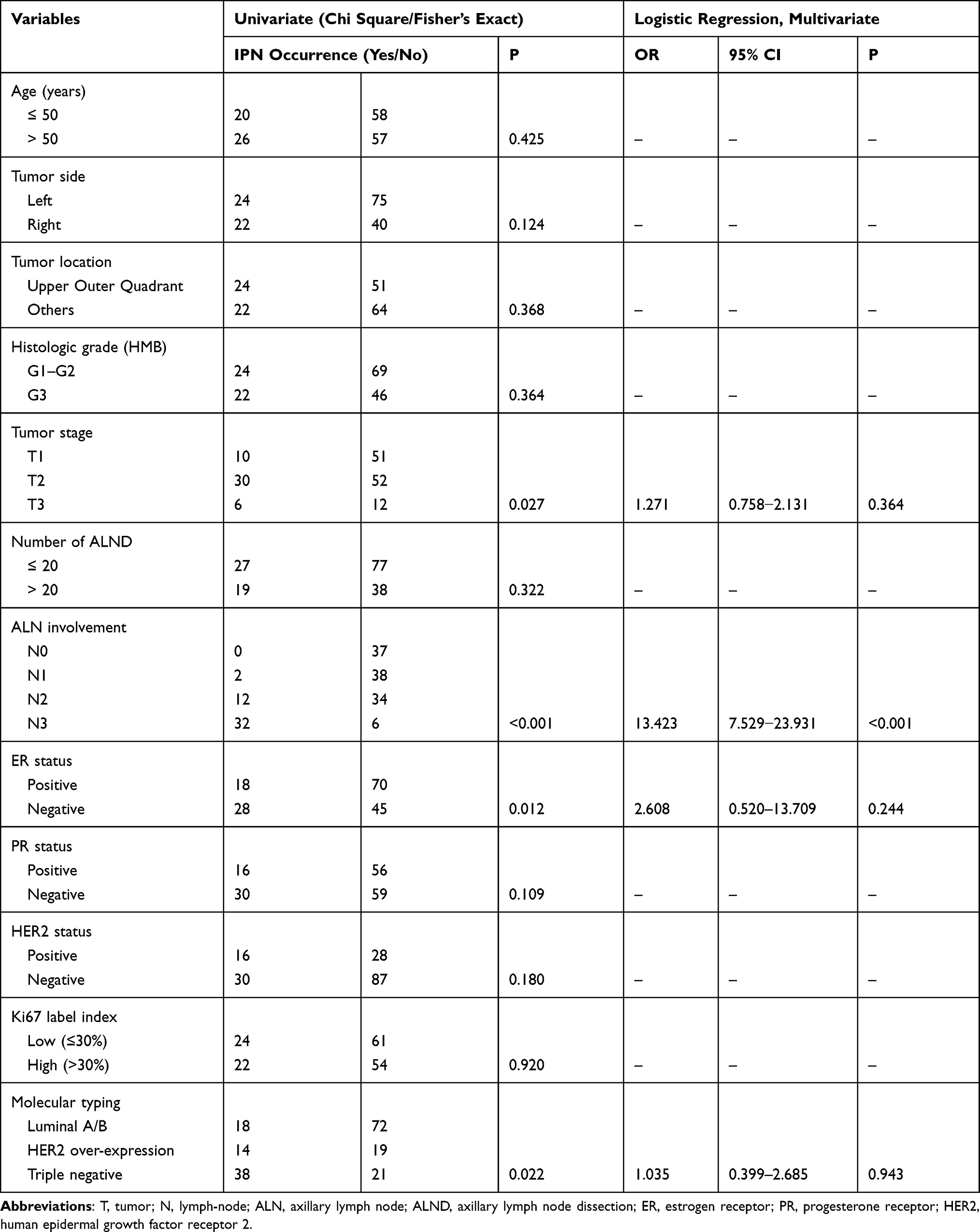 |
Table 4 Univariate and Multivariate Analysis of Clinicopathological Factors Predicting IPN Metastasis (N=161) |
IPN Metastasis in Different Subgroups
According to pathological nodal staging, the rates of IPN metastasis were 0% (0/37), 5.0% (2/40), 26.1% (12/46) and 84.2% (32/38) in patients with axillary pN0, pN1, pN2, pN3, respectively. In axillary pN1 patients, 2 patients with one involved ALN had one metastatic IPN, and the remaining 44 patients, 10 with axillary pN2 and 22 with axillary pN3 had one metastatic IPN, 2 with axillary pN2 and 10 with axillary pN3 had two metastatic IPNs. When metastatic IPNs were added up to the metastatic axillary lymph nodes, the pathological nodal staging never changed in any of the patients.
Discussion
Previous studies have often focused on the occurrence and metastasis of IPN in nonmetastatic breast cancer. Anatomically, the number of IPNs varies from 0 to 4, and relative lymphatic drainage accounts for 0.7% of the entire breast.13 An early retrospective study showed that the detection rate of IPNs was as high as 73%,14 while the detection rate in Chinese breast cancer patients ranged from 9% to 46%. In the present study, IPNs were detected in 75.2% breast cancer patients. On one hand, since IPN could be detected in approximately 75% patients and the dissection or biopsy of IPN was easily done and did not cause extra harm to patients, IPN dissection or biopsy could be performed to patients with potential benefits. On the other hand, when the estimated rate of IPN metastasis is high, IPN dissection or biopsy should be performed routinely to decrease the potential recurrence at this site.
For patients in whom IPN was detected, the rate of IPN metastasis was 28.6%, which was slightly higher than the 20.0% reported by Vrdoljak et al.9 The status of ALNs in the two study may explain the difference in IPN metastasis. In that study, nearly half of patients had negative ALNs, while in our study, only 23.0% (37/161) patients had negative ALNs. In our study, in the patients who had positive ALNs, the metastasis rate was 37.1% (46/124), which was consistent with 35 and 31.5% in previous studies.9,15 All these results indicate that a routine IPN dissection or biopsy needs to be performed because the surgical approach of this group is easy and the aesthetic result is not affected.
Our retrospective study showed that ALN involvement was not only an independent predictor for IPN occurrence, but also for IPN metastasis. In the study, the rates of IPN metastasis were 0 and 37.1% (46/161) in patients with or without positive ALNs, respectively. Although metastatic IPNs were also reported in patients who had negative ALNs,9 the proportion was small. Considering that the pedicle of the pectoral can produce damage at this level, which could also mean that the great pectoral muscle could develop partial atrophy, IPN dissection or biopsy is not recommended in patients with negative ALNs. Of course, SLNB is the preferred option for patients who are free from clinically ALN involvement. Since no metastasis is present in ALNs, including sentinel lymph nodes (SLNs), the rate of IPN metastasis is low enough that IPN dissection or biopsy can also be safely avoided.
Previous studies always considered patients with positive ALN as a whole, and then concluded that a routine IPN dissection or biopsy should be performed on breast cancer patients with positive ALNs. Different tumor burdens in ALN have different nodal stages and may have different probability of IPN metastasis. Our study is the first to specify the rate of IPN metastasis based on different tumour burdens in the ALNs. Indeed, in our study, we observed different rates of IPN metastasis in different nodal stages, with 0%, 5.0%, 26.1% and 84.2% in patients with axillary pN0, pN1, pN2, pN3, respectively.
In pN1 patients, the 5% IPN metastasis rate in our study was low enough that IPN dissection or biopsy should also be spared, which can be deduced from the American College of Surgeons Oncology Group (ACOSOG) Z0011 trial. In ALND group, 86.3% patients had one to three involved ALNs (pN1 patient), and the remaining 13.7% patients had four or more positive ALNs; after a median follow-up of 6.3 years, no recurrence was found at IPN site.16,17 In our study, as low as 5% metastatic IPNs were found, and metastatic IPN occurred in patients with a low tumour burden (one positive ALN), which seems to indicate that IPN dissection or biopsy could also be safely spared. Of course, the sample number of patients with pN1 disease in our study was small, and a large-scale study is needed to further test our result.
Our findings have important clinical significance for patients who undergo MRM. In the current study, there was no IPN metastasis when ALN was negative, and only 5% of patients had IPN metastasis when one to three ALNs were involved, which indicated that IPN dissection could be safely spared. Even for patients who undergo breast conserving surgery (BCS) and SLNB, our study also has potential significance. In the Z0011 trial, only 1.0% of patients had four or more involved ALNs in the SLNB group, and after a median follow-up of 6.5 years, there was no recurrence at the site of IPNs.16,17 Of course, if the IPNs were the SLN in certain patients, and these IPNs were not removed during the procedure of SLNB, we could not accurately assess the status of SLNs. Fortunately, there is little possibility for SLNs to serve as INPs. Estourgie et al3 found that only 2.2% cN0 patients with invasive breast cancer exhibited drainage toward INPs as SLNs, and the rates of INPs as SLNs were 2.6%, 2.1%, 1.1%, 2.7% and 2.3% in patients when the tumour was located in the upper outer, upper inner, lower outer, lower inner quadrants and the center, respectively. Therefore, we can conclude that IPN dissection can also be spared when the patients meet the inclusion criteria of the Z0011 trial: tumor ≤ 5 cm, no palpable or swollen lymph node, no more than three involved SLNs and receiving whole-breast irradiation. Of course, large-scale prospective studies are necessary for patients who meet the inclusion criteria and undergo BCS and SLNB to further verify our findings.
The limitations of this study should also be acknowledged. First, retrospective nature and small sample size may lead to bias in data selection and analysis. Second, in the study, the analysis of the predictors for IPN metastasis was based on the patients in whom IPN was successfully detected. However, IPNs were not detected in as many as 24.8% of patients, which may have influence on final analysis. If the IPNs were actually present but were ignored by either surgeons or pathologists, the rate of IPN metastasis in our study would not be accurate. Third, our analysis was based on the final pathology, and the status of ALN and the number of metastatic ALNs were not known intraoperatively. Thus, it seems to be somewhat difficult to make decisions whether to perform IPN dissection or biopsy. However, SLNB and intraoperative pathology can provide relatively accurate information on the status of SLNs.
Acknowledgment
We would like to thank all the subjects included in this study. This study was funded by Ningbo Science and Technology Foundation (2018A610325).
Disclosure
The authors declare no competing financial and non-financial interests in this work.
References
1. Grossman F. Ueber die Axillaren Lymphdrusen: Inaugural Dissertation. [About the Axillary Lymph Glands: Inaugural Dissertation]. Berlin, Germany; 1896. German.
2. Rotter J. Zur topagraphie des mamma-carcinoma. Arch Klinische Chirurgie. 1899;58:346–356.
3. Estourgie SH, Nieweg OE, Olmos RA, et al. Lymphatic drainage patterns from the breast. Ann Surg. 2004;239(2):232–237. doi:10.1097/01.sla.0000109156.26378.90
4. Komenaka IK, Bauer VP, Schnabel FR. Interpectoral nodes as the initial site of recurrence in breast cancer. Arch Surg. 2004;139(2):175–178. doi:10.1001/archsurg.139.2.175
5. Isik A, Karavas E, Peker K, et al. Male Mondors disease is a rare entity. Breast J. 2016;22(6):700–701. doi:10.1111/tbj.12657
6. Krag D, Weaver D, Ashikaga T, et al. The sentinel node in breast cancer- a multicenter validation study. N Engl J Med. 1998;339(14):941–946. doi:10.1056/NEJM199810013391401
7. Kuwajerwala NK, Feczko C, Dekhne N, et al. Comparison of lymphedema in patients with axillary lymph node dissections to those with sentinel lymphnode biopsy followed by immediate and delayed ALND. Am J Clin Oncol. 2013;36(1):20–23. doi:10.1097/COC.0b013e31823a4956
8. Isik A, Peker K, Firat D, et al. Importance of metastatic lymph node ratio in non-metastatic, lymph node-invaded colon cancer: a clinical trial. Med Sci Monit. 2014;20:1369–1375. doi:10.12659/MSM.890804
9. Vrdoljak DV, Ramljak V, Muzina D, et al. Analysis of metastatic involvement of interpectoral (Rotter’s) lymph nodes related to tumor location, size, grade and hormone receptor status in breast cancer. Tumori J. 2005;91(2):177–181. doi:10.1177/030089160509100214
10. Joshi S, Noronha J, Hawaldar R, et al. Merits of level III axillary dissection in node-positive breast cancer: a prospective, single-institution study from India. J Glob Oncol. 2019;5:1–8. doi:10.1200/JGO.18.00165
11. Hammond ME, Hayes DF, Wolff AC, et al. American society of clinical oncology/college of American pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer. J Oncol Pract. 2010;6:195–197. doi:10.1200/JOP.777003
12. Yaziji H, Goldstein LC, Barry TS, et al. HER-2 testing in breast cancer using parallel tissue-based methods. JAMA. 2004;291:1972–1977. doi:10.1001/jama.291.16.1972
13. Blumgart EI, Uren RF, Nielsen PM, et al. Predicting lymphatic drainage patterns and primary tumour location in patients with breast cancer. Breast Cancer Res Treat. 2011;130(2):699–705. doi:10.1007/s10549-011-1737-2
14. Cody HS, Egeli RA, Urban JA. Rotter’s node metastases. Therapeutic and prognostic considerations in early breast carcinoma. Ann Surg. 1984;199(3):266–270. doi:10.1097/00000658-198403000-00003
15. Senofsky GM, Moffat FL, Davis K, et al. Total axillary lymphadenectomy in the management of breast cancer. Arch Surg. 1991;126(11):1336–1342. doi:10.1001/archsurg.1991.01410350026004
16. Giuliano AE, Ballman KV, McCall L, et al. Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: long-term follow-up from the American college of surgeons oncology group (alliance) ACOSOG Z0011 randomized trial. Ann Surg. 2016;264(3):413–420. doi:10.1097/SLA.0000000000001863
17. Giuliano AE, Ballman KV, McCall L, et al. Effect of axillary dissection vs no axillary dissection on 10-year overall survival among women with invasive breast cancer and sentinel node metastasis: the ACOSOG Z0011 (alliance) randomized clinical trial. JAMA. 2017;318(10):918–926. doi:10.1001/jama.2017.11470
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.