Back to Journals » Journal of Pain Research » Volume 19
Interpectoral and Pectoserratus Plane Blocks Compared with Serratus Anterior Plane Blocks for Postoperative Pain Management in Breast Surgery (Mastectomy, Lumpectomy, and Reconstruction): A Narrative Review
Authors Wolf MC ![]() , Thompson FC, Manthei M, Shetty V, Brandt W, Tirumala S, Shekoohi S
, Thompson FC, Manthei M, Shetty V, Brandt W, Tirumala S, Shekoohi S ![]() , Ahmadzadeh S
, Ahmadzadeh S
Received 31 January 2026
Accepted for publication 21 May 2026
Published 26 May 2026 Volume 2026:19 599379
DOI https://doi.org/10.2147/JPR.S599379
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jinlei Li
Madison C Wolf,1 Francis Clay Thompson,2 Mills Manthei,2 Viraj Shetty,3 William Brandt,3 Sridhar Tirumala,3 Sahar Shekoohi,3 Shahab Ahmadzadeh3
1School of Medicine, Louisiana State University Health Sciences Center New Orleans, New Orleans, LA, USA; 2School of Medicine, Louisiana State University Health Sciences Center at Shreveport, Shreveport, LA, 71103, USA; 3Department of Anesthesiology, Louisiana State University Health Sciences Center at Shreveport, Shreveport, LA, 71103, USA
Correspondence: Sahar Shekoohi, Email [email protected]
Abstract: Postoperative pain remains a major concern following breast surgery, with persistent pain rates varying by definition and duration of follow-up. Optimizing perioperative analgesia is essential to enhance recovery and reduce the risk of chronic postmastectomy pain syndrome (PMPS). Ultrasound-guided fascial plane blocks, including interpectoral plane (IPP), pectoserratus plane (PSP), and serratus anterior plane (SAP) blocks, have gained increasing use as regional analgesic techniques targeting chest wall innervation while avoiding the risks associated with more invasive regional approaches such as thoracic epidural or paravertebral blocks. A narrative review of the literature was conducted using PubMed, with studies selected based on relevance to postoperative pain outcomes in breast surgery. Evidence suggests that IPP, PSP, and SAP blocks are associated with reduced postoperative pain scores and opioid consumption compared with systemic analgesia alone. Comparative studies generally demonstrate similar overall analgesic efficacy between techniques, although differences in dermatomal coverage and onset characteristics have been reported. IPP primarily targets the pectoral nerves, whereas PSP provides broader coverage of the intercostal and intercostobrachial nerves, including the axillary region. In contrast, SAP blocks provide wider lateral thoracic wall coverage through blockade of the lateral cutaneous branches of the intercostal nerves. Evidence regarding effects on chronic pain outcomes remains limited and heterogeneous. These techniques demonstrate favorable safety profiles when performed under ultrasound guidance. Selection of block technique should be individualized based on surgical approach, anticipated pain distribution, and patient-specific factors.
Keywords: breast surgery analgesia, chronic postmastectomy pain, interpectoral plane block, pectoserratus plane block, postoperative pain management, regional anesthesia, serratus anterior plane block, ultrasound-guided nerve block
Introduction
Breast cancer surgery, a common oncological procedure, is frequently associated with significant postoperative pain. When inadequately managed, this pain can progress to chronic pain syndromes and adversely impact long-term quality of life. Reported rates of persistent pain vary depending on definition and duration of follow-up, with estimates ranging from approximately 20% to 50%.1,2 Optimizing perioperative pain control is essential for improving immediate postoperative comfort and may help reduce the risk of developing chronic postmastectomy pain syndrome (PMPS). PMPS is a neuropathic pain condition characterized by persistent pain in the chest wall, axilla, and/or upper arm following mastectomy or lumpectomy procedures.2 In this review, persistent postoperative pain is used broadly to describe pain extending beyond the expected period of surgical recovery, whereas PMPS refers more specifically to a neuropathic pain condition involving the chest wall, axilla, and/or upper arm after breast surgery; however, the primary focus of this review is on acute postoperative pain outcomes and opioid consumption.
Regional anesthesia techniques play a vital role within multimodal strategies for managing perioperative pain in breast surgeries. Although thoracic epidural and thoracic paravertebral (TPV) blocks have traditionally provided effective analgesia, they are associated with risks such as hypotension, pneumothorax, and urinary retention.3 Recently, ultrasound-guided fascial plane blocks have gained popularity as minimally invasive alternatives with improved safety profiles. These blocks include interpectoral plane (IPP), pectoserratus plane (PSP), serratus anterior plane (SAP), and erector spinae plane (ESP) blocks, which have all been investigated for perioperative analgesia in breast and thoracic procedures.4,5 To improve consistency in terminology, recent consensus guidelines from the American Society of Regional Anesthesia and Pain Medicine (ASRA) and the European Society of Regional Anesthesia (ESRA) recommend anatomically descriptive nomenclature for chest wall blocks.6 Accordingly, the IPP block (formerly PECS I) involves deposition of local anesthetic between the pectoralis major and minor muscles, while the PSP block (formerly PECS II) extends this approach with an additional injection between the pectoralis minor and serratus anterior muscles, providing broader coverage by targeting the pectoral nerves as well as the lateral cutaneous branches of the upper intercostal nerves (approximately T2-T6), including contributions to the intercostobrachial nerve.7 In contrast, the SAP block may be performed as either a superficial approach, with local anesthetic deposited superficial to the serratus anterior muscle, or a deep approach, with injection between the posterior surface of the serratus anterior muscle and the periosteum of the rib.6 These techniques are intended to anesthetize the lateral cutaneous branches of the thoracic intercostal nerves, commonly spanning T2 to T9 depending on local anesthetic spread.8
These blocks are indicated for postoperative analgesia in breast surgeries such as mastectomy (particularly modified radical mastectomy), lumpectomy, reconstruction, and axillary lymph node dissection.7,8 They are valued for their ease of use, efficacy, and favorable safety profiles compared with more invasive regional techniques such as thoracic epidural and thoracic paravertebral blocks.3 By targeting peripheral nerves involved in surgical pain transmission, IPP, PSP, and SAP blocks have been associated with opioid-sparing analgesia, decreased opioid-related side effects, and improved postoperative recovery.9,10
This narrative review aims to evaluate the anatomical targets, analgesic efficacy, clinical applications, and safety considerations of IPP, PSP, and SAP blocks for postoperative pain management in breast surgery, with a primary focus on acute postoperative pain outcomes and opioid consumption. Additional discussion will include their potential role in reducing the incidence of chronic postoperative pain and explore future directions for optimizing their use in perioperative care.2,11
Methods
A narrative review of the literature was conducted to evaluate the role of IPP, PSP, and SAP blocks in postoperative pain management following breast surgery. A structured search of the PubMed database was performed using combinations of the following keywords: “pectoral nerve block,” “PECS block,” “interpectoral plane block,” “pectoserratus plane block,” “serratus anterior plane block,” “SAP block,” “breast surgery analgesia,” and “regional anesthesia breast surgery.” Reference lists of selected articles were also reviewed to identify additional relevant studies. The final literature search was conducted in March 2026. Additional recent randomized trials, meta-analyses, and practice guidelines were incorporated during revision to ensure inclusion of contemporary evidence relevant to current clinical practice.
Relevant studies were selected based on their focus on postoperative pain outcomes in adult patients undergoing breast surgery. Randomized controlled trials, systematic reviews, and observational studies were included to provide a comprehensive overview of current evidence. Studies were also included when they provided meaningful insight into anatomical considerations, clinical applications, or safety. The available evidence is primarily derived from studies involving modified radical mastectomy, with more limited data available for lumpectomy and reconstructive procedures.
Articles were screened for relevance based on topic and abstract, followed by full-text review. Data was synthesized qualitatively, with emphasis on analgesic efficacy, opioid consumption, dermatomal coverage, and safety profiles and organized into structured tables to allow comparison of study characteristics and outcomes across the included literature. Analgesic outcomes were summarized in a structured evidence table (Table 1), while safety considerations, including reported complications, proposed mechanisms, and risk mitigation strategies, were summarized separately in Table 2. Terminology was standardized according to the ASRA-ESRA consensus nomenclature for chest wall blocks.
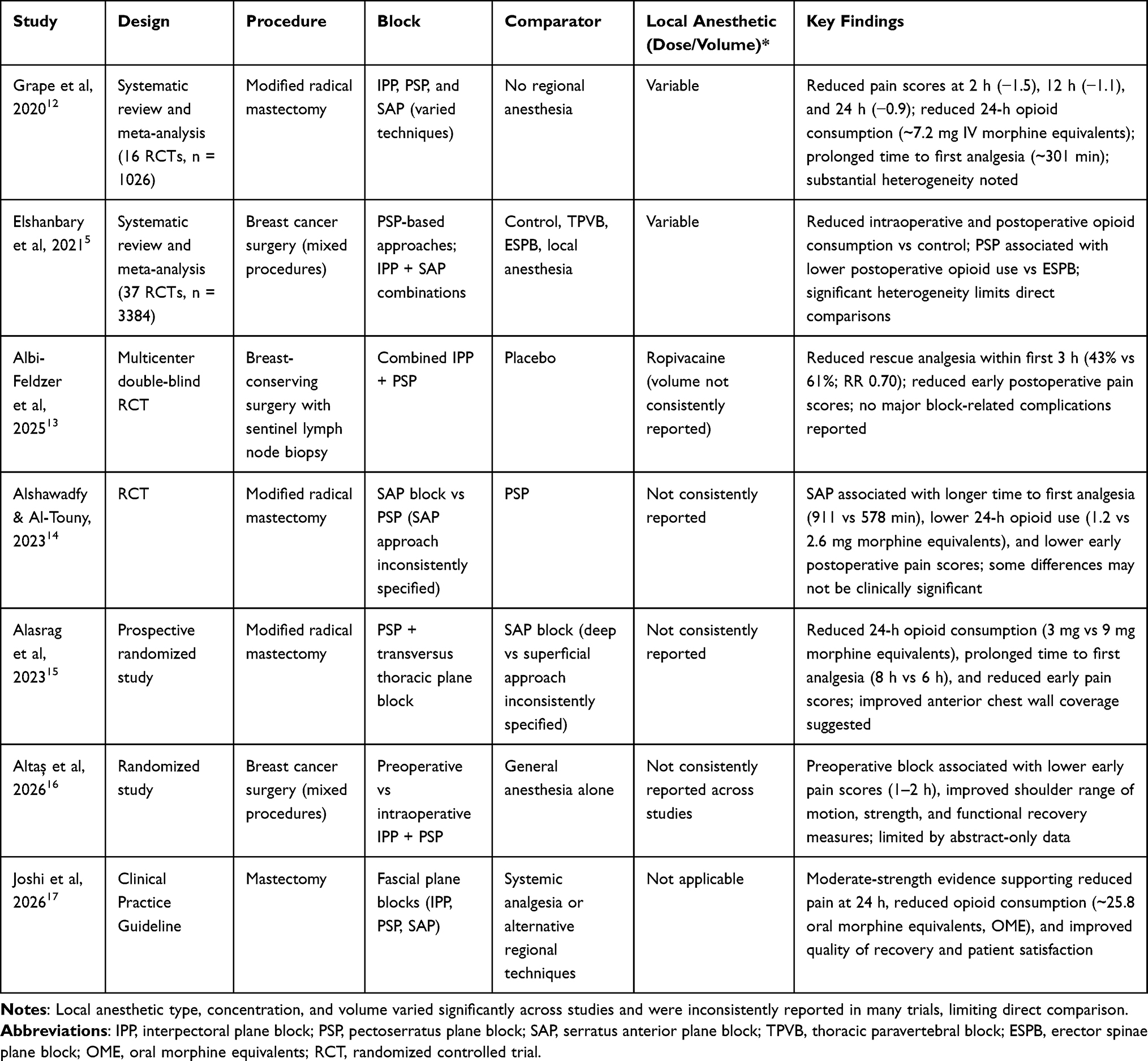 |
Table 1 Summary of Key Studies Evaluating IPP, PSP, and SAP Blocks for Postoperative Analgesia in Breast Surgery |
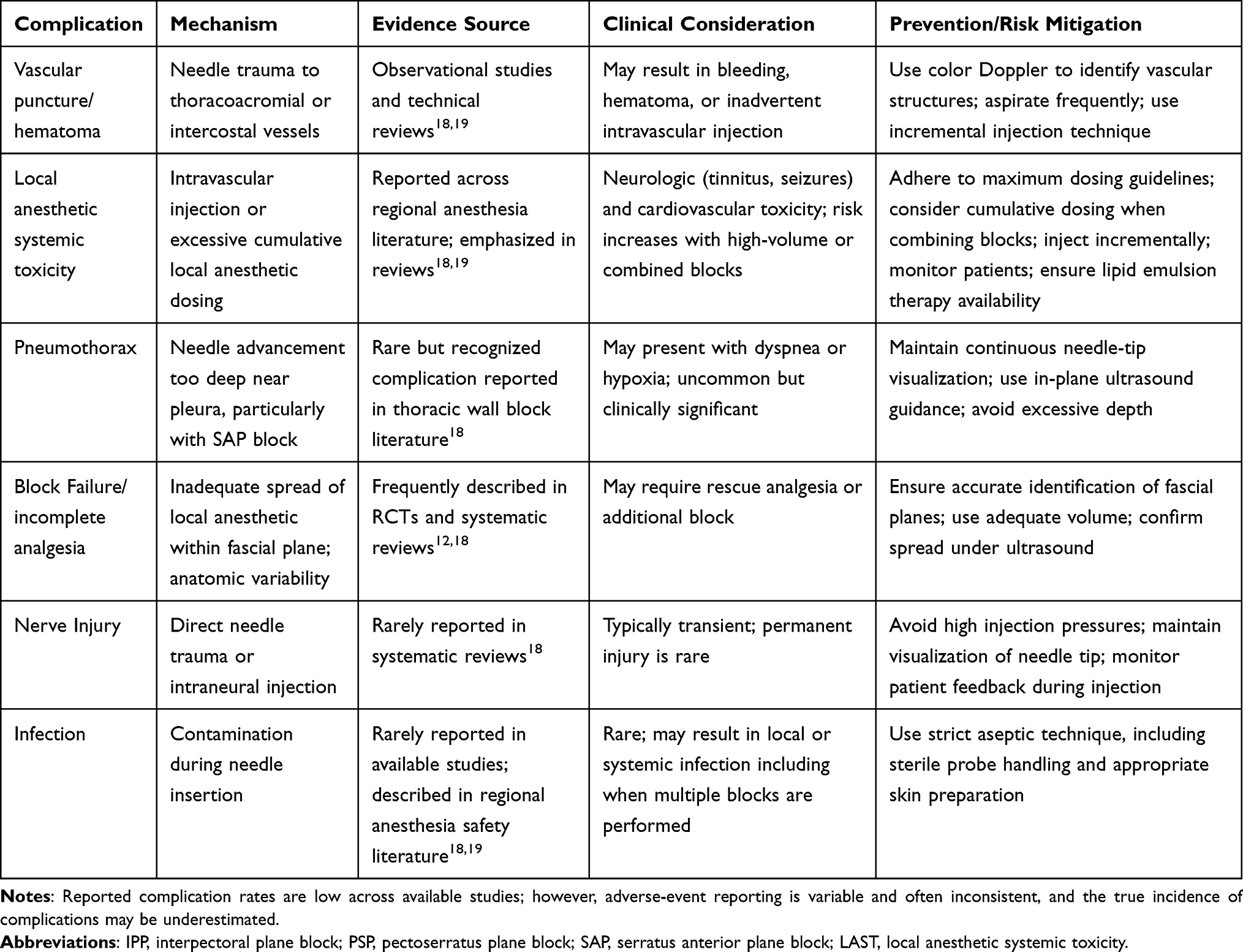 |
Table 2 Reported Complications and Safety Outcomes of IPP, PSP, and SAP Blocks |
Anatomical Considerations and Mechanism of Action of IPP, PSP, and SAP Blocks
IPP, PSP, and SAP blocks have gained popularity for postoperative pain control in breast surgery by targeting nerves that innervate the pectoralis major, pectoralis minor, and serratus anterior muscles.7,8 The IPP primarily targets the medial and lateral pectoral nerves that innervate the pectoral muscles. The PSP, which extends this approach, involves injection in the plane between the pectoralis minor and serratus anterior muscles and is intended to provide analgesia by targeting the intercostobrachial nerve (T2), intercostal nerves (T3–T6), and the long thoracic nerve.9,14,20
In contrast, the SAP block is administered into the fascial plane either superficial or deep to the serratus anterior muscle. This may result in blockade of the lateral cutaneous branches of the thoracic intercostal nerves (typically T2–T9), as well as potential spread to adjacent nerves such as the long thoracic and thoracodorsal nerves depending on the depth of injection and local anesthetic distribution.6,14 Compared to IPP and PSP, SAP blocks are performed in a more posterior and lateral plane, which may allow for broader lateral thoracic wall coverage.14
These techniques function by delivering local anesthetic into fascial planes under ultrasound guidance, where the agent inhibits voltage-gated sodium channels on neuronal membranes, preventing the initiation and propagation of action potentials and thereby reducing nociceptive transmission.21 For IPP and PSP blocks, the transducer is positioned in the infraclavicular region to visualize the pectoral muscles, with local anesthetic deposited between the pectoralis major and minor muscles (IPP) and between the pectoralis minor and serratus anterior muscles (PSP).14 The SAP block is typically performed at the midaxillary line near the level of the fifth rib, with local anesthetic injected either superficial or deep to the serratus anterior muscle.8 Accurate anatomical visualization via ultrasound is essential to ensure adequate spread of local anesthetic and minimize complications.
Commonly used local anesthetics include bupivacaine, ropivacaine, and lidocaine. The typical volume injected ranges from 20 to 40 mL, administered incrementally to achieve adequate spread within the targeted fascial plane.22–24 In terms of anesthetic distribution, IPP and PSP blocks are intended to provide coverage primarily within the T2–T6 dermatomal distribution, whereas SAP blocks may provide broader lateral thoracic spread extending from approximately T2 to T9.9,14,20 However, the extent of dermatomal coverage is variable and depends on factors such as injection technique, local anesthetic volume, and individual patient anatomy.
Although these techniques are effective in reducing postoperative pain, their dermatomal spread and targeted nerve pathways differ, which may influence block selection based on the surgical field and expected pain distribution. A detailed understanding of these anatomical considerations is essential for selecting the appropriate regional technique and optimizing postoperative analgesia in breast surgery.
Clinical Significance and Applications of IPP, PSP, and SAP Blocks
The use of regional anesthesia techniques such as IPP, PSP, and SAP blocks has gained prominence in breast surgery for their role in reducing postoperative pain, minimizing opioid requirements, and enhancing recovery. These blocks are utilized across a variety of procedures, including simple and modified radical mastectomies, breast-conserving surgeries (eg, lumpectomy), sentinel lymph node biopsies, axillary lymph node dissections, and reconstructive interventions. Multiple studies have demonstrated that these techniques improve analgesia in operations involving the breast and axillary regions.7–9
Selection of regional technique should be individualized based on surgical approach, anatomical considerations, patient comorbidities, and specific analgesic goals. Patients at increased risk for opioid-related adverse effects may derive particular benefit, as these blocks have been shown to reduce intraoperative and postoperative opioid requirements.9 Regional anesthesia techniques may be associated with a reduced incidence of persistent postoperative pain; however, current evidence remains limited and heterogeneous, and a definitive causal relationship has not been established.2 Careful patient assessment is essential prior to performing these blocks. Contraindications include infection at the injection site, clinically significant coagulopathy or ongoing anticoagulation therapy, allergy to local anesthetics, and inability of the patient to cooperate with positioning or remain still during the procedure. Relative contraindications may include altered anatomy or prior surgical disruption of fascial planes that could affect local anesthetic spread or ultrasound visualization.
IPP and PSP blocks offer distinct advantages in various breast procedures. For mastectomies, PSP is intended to provide effective analgesia by targeting the pectoral nerves and upper intercostal nerves, thereby improving pain control and reducing opioid consumption. PSP may also be beneficial in reconstructive procedures involving subpectoral implants or tissue expanders, where anterior chest wall and axillary analgesia are required.7 Additionally, some studies suggest that PSP may provide improved analgesia for axillary dissection, although findings are variable and dependent on technique and study design.25
SAP blocks have demonstrated utility in procedures involving the lateral thoracic wall, including reconstructive breast surgery, chest drain placement, and cosmetic breast procedures.8 Due to its more lateral and posterior injection plane, a SAP block may provide broader dermatomal coverage, particularly for lateral chest wall pain. In more extensive procedures such as modified radical mastectomy with axillary clearance, the combined use of IPP, PSP, and SAP blocks may provide complementary analgesia by expanding dermatomal coverage and improving overall pain control, although this approach requires further study.9,15,24
The clinical significance of IPP, PSP, and SAP blocks lies in their ability to provide targeted, opioid-sparing analgesia within a multimodal pain management framework. When appropriately selected and performed under ultrasound guidance, these techniques can improve postoperative recovery, reduce opioid-related adverse effects, and support enhanced recovery after surgery protocols. Their integration into perioperative care pathways represents a meaningful advancement in regional anesthesia for breast surgery. However, variability in technique, patient anatomy, and surgical approach should be considered when interpreting outcomes and selecting the most appropriate block.
Efficacy and Pain Management Outcomes
Ultrasound-guided regional anesthesia techniques, including IPP, PSP, and SAP blocks, have been shown to provide clinically meaningful reductions in postoperative pain and opioid consumption following breast surgery. A systematic review and meta-analysis including 16 randomized controlled trials and 1026 patients demonstrated that fascial plane blocks significantly reduced postoperative pain scores at multiple time points compared with no regional anesthesia. Specifically, mean differences in pain scores were −1.5 at 2 hours, −1.1 at 12 hours, and −0.9 at 24 hours on a 0–10 scale. This was accompanied by a reduction in 24-hour opioid consumption of approximately 7.2 mg intravenous morphine equivalents and prolongation of time to first rescue analgesia by approximately 301 minutes, or about 5 hours.12 However, interpretation of these pooled findings is limited by heterogeneity across included studies, including variation in block techniques, multimodal analgesic regimens, and outcome definitions.12 A summary of the major findings reported by Grape et al is provided in Table 1.
Additional meta-analytic data further support the opioid-sparing benefit of these techniques. In a systematic review and meta-analysis including 37 randomized controlled trials, Elshanbary et al reported that PSP-based approaches significantly reduced intraoperative opioid consumption compared with controls and also reduced postoperative opioid consumption compared with controls. The same review found that IPP blocks combined with SAP blocks reduced intraoperative opioid requirements compared with controls, and that PSP blocks were associated with lower postoperative opioid consumption than ESP blocks. These findings support the analgesic benefit of IPP and PSP-based techniques, although the authors reported substantial heterogeneity across comparisons, limiting definitive conclusions regarding superiority between block types.5
Recent randomized evidence also expands the applicability of these blocks beyond modified radical mastectomy. In a double-blinded, multicenter randomized controlled trial of patients undergoing oncologic breast-conserving surgery with sentinel lymph node biopsy, Albi-Feldzer et al found that combined IPP and PSP blocks with ropivacaine reduced the incidence of rescue analgesia during the first 3 postoperative hours compared with placebo, 43% versus 61%, corresponding to a relative risk of 0.70 and an approximately 30% reduction in rescue analgesic use. Pain scores at 30 minutes were also lower both at rest and during mobilization, and no block-related complications or serious adverse events were reported during 30-day follow-up.13 This study is particularly relevant because it provides procedure-specific evidence in breast-conserving surgery, an area less represented in earlier literature focused primarily on modified radical mastectomy.
Across direct comparative studies, findings remain variable, with differences in analgesic outcomes influenced by block technique, surgical approach, and outcome definitions. Some randomized controlled trials have reported longer time to first analgesic request and reduced opioid consumption with SAP blocks compared with PSP blocks. For example, in patients undergoing modified radical mastectomy, SAP blocks were associated with prolonged time to first analgesic request, 911 minutes versus 578 minutes, and lower 24-hour morphine consumption, 1.2 mg versus 2.6 mg, with lower pain scores observed in the post-anesthesia care unit and at 2, 8, and 24 hours.14 Additionally, fewer patients required rescue analgesia in the SAP block group, 52% versus 92%, although the authors noted that some statistically significant findings may not represent clinically meaningful differences.14
In contrast, other randomized prospective data suggest that PSP-based approaches may provide improved analgesic outcomes in certain settings, particularly when combined with adjunctive anterior plane blocks. In one study, patients receiving PSP blocks combined with superficial parasternal intercostal plane (PIP) blocks (formerly transversus thoracic plane) had lower 24-hour morphine consumption, 3 mg versus 9 mg, prolonged time to first rescue analgesia, 8 hours versus 6 hours, and lower early postoperative pain scores compared with SAP blocks alone.15 The improved analgesia observed with this combined approach may be related to enhanced anterior chest wall coverage, as the PIP block anesthetizes the anterior cutaneous branches of the intercostal nerves supplying the parasternal region, which is not consistently covered by SAP block alone.15
Emerging evidence also suggests that timing of block placement may influence both pain control and early functional recovery. In a 2026 study comparing preoperative IPP and PSP blocks, intraoperative IPP and PSP blocks, and general anesthesia alone, Altaş et al reported that preoperative block placement produced significantly lower VAS scores at 1 and 2 hours after surgery compared with the other groups. At 6, 12, and 24 hours, both block groups had lower pain scores than controls. Importantly, the preoperative block group also demonstrated better shoulder abduction and flexion range of motion on postoperative day 1, greater extension strength, sustained muscle strength improvements at day 10, and improved QuickDASH and Beck Depression Inventory scores.16 Although currently available to us in abstract form, these findings are useful because they highlight patient-centered recovery outcomes beyond pain scores and opioid use.
Recent clinical practice guideline data further support the role of fascial plane blocks in mastectomy. The 2026 American Society of Anesthesiologists practice guideline recommends fascial plane or paravertebral blocks for adults undergoing mastectomy to reduce pain and/or opioid requirements in the first 24 postoperative hours, with moderate-strength evidence. In pooled mastectomy data, single-injection fascial plane blocks, including IPP, PSP, and SAP blocks, reduced pain at rest at 24 hours, reduced dynamic pain at 24 hours, decreased opioid consumption by approximately 25.8 oral morphine equivalents, and improved quality of recovery and patient satisfaction.17 These guideline findings support the clinical relevance of fascial plane blocks while also reinforcing the need to interpret individual block comparisons cautiously.
When considered collectively, these findings highlight the heterogeneity of comparative outcomes between techniques. SAP blocks may provide more sustained early postoperative analgesia and reduced opioid consumption in some studies, whereas PSP-based approaches may offer improved anterior and axillary coverage, particularly when combined with additional anterior chest wall techniques. Importantly, pooled evidence does not demonstrate consistent superiority of one fascial plane block technique across all breast procedures, and differences in clinical performance are likely driven by anatomical distribution, timing of administration, surgical approach, and multimodal analgesic regimens rather than intrinsic superiority of one block over another.5,12,17
IPP, PSP, and SAP blocks are effective components of multimodal analgesia for breast surgery. SAP blocks may provide broader lateral thoracic coverage, whereas PSP blocks are intended to target the pectoral nerves, intercostobrachial nerve, and upper intercostal nerves, making it particularly useful for anterior chest wall and axillary procedures.14,15 Accordingly, optimal block selection should be individualized based on surgical approach, anticipated pain distribution, timing of block placement, and the need for medial versus lateral chest wall coverage.13,16,17
Safety and Complications of IPP, PSP, and SAP Blocks
Reported complications, proposed mechanisms, and safety considerations, including strategies for risk mitigation, are summarized in Table 2. IPP, PSP, and SAP blocks are generally considered safe and minimally invasive regional anesthesia techniques when performed under ultrasound guidance.18 However, as with all regional anesthesia procedures, potential complications may occur. Reported risks include vascular puncture, local anesthetic systemic toxicity (LAST), pneumothorax, infection, and block failure.19 The use of real-time ultrasound guidance has significantly reduced these risks by enabling accurate identification of anatomical structures and continuous visualization of needle advancement and local anesthetic spread.19
Vascular puncture may occur during needle advancement, particularly in regions containing the thoracoacromial or intercostal vessels, potentially resulting in hematoma formation or inadvertent intravascular injection.19 The use of color Doppler imaging and frequent aspiration during injection are recommended strategies to mitigate this risk.19 Pneumothorax, although uncommon, remains a potential complication, particularly with deeper injections in proximity to the pleura during SAP blocks.18 Maintaining visualization of the needle tip at all times and advancing the needle in-plane with the ultrasound transducer are critical to minimizing this risk.19 As summarized in Table 2, serious complications are infrequently reported; however, inconsistent adverse-event reporting across studies limits accurate estimation of incidence.
Neurological complications are rare and are typically related to direct needle trauma or unintended intraneural injection rather than the specific anatomical target itself.18 Accordingly, emphasis should be placed on precise ultrasound-guided needle-tip control, avoidance of high injection pressures, and careful monitoring of patient feedback during block placement to reduce the risk of nerve injury.19
Block failure may occur due to anatomic variability, suboptimal needle positioning, or inadequate spread of local anesthetic within the intended fascial plane. While SAP blocks may allow for broader and more superficial spread in some cases, successful analgesia with all techniques depends on accurate identification of fascial planes and appropriate injectate distribution.19
Systematic reviews evaluating the safety of chest wall blocks have reported a low incidence of serious complications, with no major adverse events such as permanent nerve injury or clinically significant local anesthetic systemic toxicity described in the included studies.18 However, adverse-event reporting across studies is variable and often inconsistent, and the true incidence of complications may be underestimated.
IPP, PSP, and SAP blocks demonstrate favorable safety profiles when performed using appropriate ultrasound-guided techniques. Careful attention to needle-tip visualization, injection technique, and patient-specific risk factors is essential to minimizing complications and ensuring safe and effective analgesia.18
Safe administration of local anesthetics requires adherence to established maximum dosing guidelines, with consideration of cumulative dosing when combining regional techniques. Clinicians should remain vigilant for signs of LAST, including neurologic and cardiovascular symptoms, and ensure that appropriate monitoring and resuscitation protocols, including lipid emulsion therapy, are readily available.19
Discussion
IPP, PSP, and SAP blocks have emerged as important ultrasound-guided fascial plane techniques for postoperative analgesia following breast surgery. Current evidence suggests that these blocks reduce acute postoperative pain scores and perioperative opioid requirements, supporting their role within multimodal analgesia pathways.9,12 Although comparative studies generally demonstrate similar overall analgesic efficacy, differences in anatomical coverage may guide block selection based on surgical approach and anticipated pain distribution. SAP blocks may provide broader lateral thoracic wall coverage, commonly involving T2 to T9 dermatomes, whereas PSP blocks are intended to provide more focused anterior chest wall and axillary coverage through its effect on the pectoral nerves, intercostobrachial nerve, and upper intercostal nerves.7,14
The use of ultrasound guidance has been central to the safe and effective application of these techniques. Real-time imaging allows visualization of fascial planes, needle trajectory, vascular structures, and local anesthetic spread, thereby improving technical accuracy and reducing procedural risk.4,24 Compared with thoracic epidural and TPV techniques, IPP, PSP, and SAP blocks are more superficial and may be associated with less hemodynamic instability, making them attractive options for patients in whom deeper regional techniques may be less desirable.4,18
In clinical practice, incorporation of IPP, PSP, and SAP blocks into perioperative analgesic protocols aligns with ERAS principles by reducing opioid exposure, limiting opioid-related adverse effects, and supporting earlier postoperative recovery.2,9,12 However, block selection should remain individualized. PSP blocks may be particularly useful for procedures involving the anterior chest wall, axilla, or subpectoral manipulation, whereas SAP blocks may be advantageous when broader lateral thoracic wall analgesia is needed. For more extensive procedures, including modified radical mastectomy with axillary dissection, combined or complementary block strategies may provide more complete dermatomal coverage. However, evidence supporting combined approaches remains limited and heterogeneous.9,15,24
Recent evidence also broadens the discussion from analgesic efficacy alone to recovery quality and functional outcomes. Albi-Feldzer et al provide contemporary multicenter randomized evidence supporting combined IPP and PSP blocks for breast-conserving surgery and sentinel lymph node biopsy, a population less represented in earlier mastectomy-heavy studies.13 Altaş et al further suggest that preoperative block placement may improve early shoulder range of motion, muscle strength, disability scores, and psychological recovery measures compared with intraoperative block placement or general anesthesia alone.16 These findings support the need for future studies to evaluate patient-centered outcomes beyond pain scores and opioid consumption.
The 2026 ASA practice guideline also supports the clinical relevance of fascial plane blocks for mastectomy, recommending fascial plane or paravertebral blocks to reduce pain and/or opioid requirements in the first 24 postoperative hours, while noting that fascial plane blocks may improve quality of recovery and patient satisfaction.17 This guideline-level evidence strengthens the rationale for incorporating IPP, PSP, and SAP blocks into multimodal analgesia pathways, while also emphasizing that technique selection should remain procedure-specific and individualized. As highlighted in Table 2, safe implementation of these techniques depends on adherence to ultrasound-guided principles and appropriate dosing strategies.
Limitations of Current Evidence
The current body of literature is subject to several important limitations. First, there is substantial heterogeneity across studies in terms of block technique, including single versus multi-injection PSP approaches and superficial versus deep SAP approaches, as well as local anesthetic volume, concentration, timing of block placement, and use of multimodal analgesic regimens. Second, many studies focus on patients undergoing modified radical mastectomy, limiting generalizability to less invasive procedures such as lumpectomy, breast-conserving surgery, and reconstructive procedures. Recent evidence from Albi-Feldzer et al helps address this gap by evaluating IPP and PSP blocks in breast-conserving surgery with sentinel lymph node biopsy, but additional procedure-specific trials remain needed.13 Third, outcome measures vary considerably between studies, including differences in pain score timing, opioid reporting metrics, rescue analgesia definitions, and thresholds for clinically meaningful benefit. Finally, long-term outcomes, particularly persistent postoperative pain, remain inconsistently evaluated, limiting conclusions regarding the impact of these techniques on chronic pain development. These limitations should be considered when interpreting the findings summarized in Table 1.5,12,17 Safety data summarized in Table 2 are similarly limited by inconsistent reporting of adverse events, precluding precise estimates of complication rates.
Future Directions
Future research should focus on well-designed comparative trials that evaluate acute pain scores and opioid consumption in addition to patient-centered outcomes such as quality of recovery, satisfaction, shoulder range of motion, functional recovery, disability scores, psychological recovery, and persistent postoperative pain. An ideal head-to-head trial would include procedure-specific stratification, such as mastectomy versus lumpectomy versus reconstruction, standardized multimodal analgesia protocols, consistent opioid reporting using morphine milligram equivalents or oral morphine equivalents, clearly defined rescue analgesia criteria, and extended follow-up to assess long-term outcomes such as chronic pain. Other fascial plane techniques, such as ESP blocks, have also been explored for breast surgery analgesia; however, direct comparisons remain limited, and these approaches were not the primary focus of this review.4
Additional studies are needed to clarify optimal local anesthetic volume, concentration, and timing of block placement. The potential role of combined approaches, such as PSP blocks with SAP blocks or PSP blocks with anterior chest wall blocks, warrants further investigation, particularly for surgeries involving both medial and lateral breast tissue.15,24 Given recent evidence suggesting improved early functional outcomes with preoperative block placement, future studies should also evaluate whether timing of administration affects rehabilitation, shoulder mobility, and return to baseline function.16
IPP, PSP, and SAP blocks represent safe, effective, and adaptable components of multimodal analgesia for breast surgery. Their clinical utility lies in their ability to provide targeted analgesia tailored to surgical anatomy and expected pain distribution. However, variability in technique, patient factors, and study design should be considered when interpreting current evidence. Continued research and refinement of these techniques will help define their optimal role within perioperative pain management strategies.
Conclusion
Effective postoperative pain management in breast surgery is essential for optimizing recovery, minimizing opioid exposure, and addressing the risk of persistent postoperative pain. IPP, PSP, and SAP blocks have emerged as valuable regional anesthesia techniques that provide targeted analgesia while avoiding many of the risks associated with deeper regional approaches.
This topic remains highly relevant, as breast cancer continues to be one of the most commonly treated malignancies worldwide, and persistent postoperative pain can significantly impact long-term quality of life. Integration of regional anesthesia techniques such as IPP, PSP, and SAP blocks into perioperative care pathways may enhance recovery and may be associated with a reduction in persistent postoperative pain, although current evidence remains limited and heterogeneous.
Available evidence suggests that IPP, PSP, and SAP blocks are associated with reductions in acute postoperative pain and opioid requirements compared with systemic analgesia alone. Differences between techniques appear to be related primarily to anatomical distribution, surgical approach, and timing of administration rather than consistent differences in overall analgesic efficacy. SAP blocks may provide broader lateral thoracic coverage in some cases, whereas PSP is intended to provide more targeted anterior chest wall and axillary analgesia. All techniques demonstrate favorable safety profiles when performed under ultrasound guidance, although reported complication rates may be influenced by variability in study design and adverse-event reporting.
The clinical value of these techniques lies in their ability to provide opioid-sparing analgesia within a minimally invasive framework while supporting postoperative recovery. However, variability in technique, patient factors, and study methodology should be considered when interpreting current findings. Further high-quality, procedure-specific studies are needed to better define optimal block selection and their impact on long-term outcomes, including persistent pain and functional recovery.
Compliance with Ethical Guidelines
This article is based on previous studies and contains no new studies with human participants or animals performed by any authors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding or sponsorship was received for this study or publication of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gärtner R, Jensen MB, Nielsen J, Ewertz M, Kroman N, Kehlet H. Prevalence of and factors associated with persistent pain following breast cancer surgery. JAMA. 2009;302(18):1985–11. doi:10.1001/jama.2009.1568
2. Andersen KG, Kehlet H. Persistent pain after breast cancer treatment: a critical review of risk factors and strategies for prevention. J Pain. 2011;12(7):725–746. doi:10.1016/j.jpain.2010.12.005
3. Kairaluoma PM, Bachmann MS, Rosenberg PH, Pere PJ. Preincisional paravertebral block reduces the prevalence of chronic pain after breast surgery. Anesth Analg. 2006;103(3):703–708. doi:10.1213/01.ane.0000230603.92574.4e
4. Helander EM, Webb MP, Kendrick J, et al. PECS, serratus plane, erector spinae, and paravertebral blocks: a comprehensive review. Best Pract Res Clin Anaesthesiol. 2019;33(4):4. doi:10.1016/j.bpa.2019.07.003
5. Elshanbary AA, Zaazouee MS, Darwish YB, et al. Efficacy and safety of pectoral nerve block (Pecs) compared with control, paravertebral block, erector spinae plane block, and local anesthesia in patients undergoing breast cancer surgeries: a systematic review and meta-analysis. Clin J Pain. 2021;37(12):925. doi:10.1097/AJP.0000000000000985
6. El-Boghdadly K, Wolmarans M, Stengel AD, et al. Standardizing nomenclature in regional anesthesia: an ASRA-ESRA Delphi consensus study of abdominal wall, paraspinal, and chest wall blocks. Reg Anesth Pain Med. 2021;46(7):571–580. doi:10.1136/rapm-2020-102451
7. Blanco R. The “pecs block”: a novel technique for providing analgesia after breast surgery. Anaesthesia. 2011;66(9):847–848. doi:10.1111/j.1365-2044.2011.06838.x
8. Blanco R, Parras T, McDonnell JG, Prats-Galino A. Serratus plane block: a novel ultrasound-guided thoracic wall nerve block. Anaesthesia. 2013;68(11):1107–1113. doi:10.1111/anae.12344
9. Bakeer AH, Kamel KM, Abdelgalil AS, Ghoneim AA, Abouel Soud AH, Hassan ME. Modified pectoral nerve block versus serratus block for analgesia following modified radical mastectomy: a randomized controlled trial. J Pain Res. 2020;13:1769–1775. doi:10.2147/JPR.S252539
10. Wang W, Song W, Yang C, et al. Ultrasound-guided pectoral nerve block i and serratus-intercostal plane block alleviate postoperative pain in patients undergoing modified radical mastectomy. Pain Physician. 2019;22(4):E315–E323. doi:10.36076/ppj/2019.22.E315
11. Chapman CR, Donaldson GW, Davis JJ, Bradshaw DH. Improving individual measurement of postoperative pain: the pain trajectory. J Pain. 2011;12(2):257–262. doi:10.1016/j.jpain.2010.08.005
12. Grape S, Jaunin E, El-Boghdadly K, Chan V, Albrecht E. Analgesic efficacy of PECS and serratus plane blocks after breast surgery: a systematic review, meta-analysis and trial sequential analysis. J Clin Anesth. 2020;63:109744. doi:10.1016/j.jclinane.2020.109744
13. Albi-Feldzer A, Gayraud G, Dureau S, Augé M, Lemoine A, Raft J. Efficiency of interpectoral and pectoserratus plane blocks for breast surgery: a randomized controlled trial. J Clin Anesth. 2025;103:111805. doi:10.1016/j.jclinane.2025.111805
14. Alshawadfy A, Al-Touny SA. Comparing the quality of analgesia with ultrasound-guided pectoral nerve block and serratus anterior plane block II in patients undergoing modified radical mastectomy: a randomised clinical trial. Anaesthesiol Intensive Ther. 2023;55(1):52–59. doi:10.5114/ait.2023.126218
15. Alasrag AS, Elkeblawy AM, Abo Elyazid MME, Ezz HAA. Analgesic efficacy of ultrasound-guided PECS II and transversus thoracic plane blocks compared to serratus anterior plane block for modified radical mastectomy: a randomized prospective study. Egypt J Anaesth. 2023;39(1):1. doi:10.1080/11101849.2023.2182991
16. Altaş ÖF, Altaş EU, Kebabci E. Effect of intraoperative vs. preoperative interpectoral-pectoserratus plane block on postoperative pain, analgesic use, shoulder range of motion, and muscle strength in breast cancer surgery. Minerva Anestesiol. 2026. doi:10.23736/S0375-9393.26.19518-2
17. Joshi GP, Mariano E, Elkassabany N, et al. 2026 American Society of Anesthesiologists Practice Guideline on perioperative pain management using local and regional analgesia for cardiothoracic surgeries, mastectomy, and abdominal surgeries. Anesthesiology. 2026;144(1). doi:10.1097/ALN.0000000000005790
18. Jack JM, McLellan E, Versyck B, Englesakis MF, Chin KJ. The role of serratus anterior plane and pectoral nerves blocks in cardiac surgery, thoracic surgery and trauma: a qualitative systematic review. Anaesthesia. 2020;75(10):10. doi:10.1111/anae.15000
19. Nair AS, Sahoo RK, Ganapathy M, Mudunuri R. Ultrasound guided blocks for surgeries/ procedures involving chest wall (Pecs 1, 2 and serratus plane block). Anaesth Pain Intensive Care. 2019;23(4):348–351.
20. Kubodera K, Fujii T, Akane A, et al. Efficacy of pectoral nerve block type-2 (Pecs II block) versus serratus plane block for postoperative analgesia in breast cancer surgery: a retrospective study. Nagoya J Med Sci. 2020;82(1):93–99. doi:10.18999/nagjms.82.1.93
21. Strichartz G. Molecular mechanisms of nerve block by local anesthetics. Anesthesiology. 1976;45(4):4. doi:10.1097/00000542-197610000-00012
22. Ben Aziz M, Hendrix JM, Mukhdomi T. Regional anesthesia for breast reconstruction. In: StatPearls. StatPearls Publishing; 2025. Available from: http://www.ncbi.nlm.nih.gov/books/NBK567732/.
23. Battista C, Krishnan S. Pectoralis nerve block. In: StatPearls. StatPearls Publishing; 2025. Available from: http://www.ncbi.nlm.nih.gov/books/NBK547691/.
24. Yesiltas S, Türköz A, Çalım M, et al. Comparison of serratus plane block alone and in combination with pectoral type 1 block for breast cancer surgery: a randomized controlled study. Hippokratia. 2021;25(1):1.
25. Robinson H, Mishra S, Davies L, et al. Anatomical evaluation of a conventional pectoralis II versus a subserratus plane block for breast surgery. Anesth Analg. 2020;131(3):3. doi:10.1213/ANE.0000000000005039
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy of Ultrasound-Guided Thoracic Paravertebral Block on Postoperative Quality of Recovery in Patients Undergoing Percutaneous Nephrolithotomy: A Randomized Double-Blind Placebo-Controlled Trial
Yan Z, Lin H, Yang Y, Yang J, Li X, Yao Y
Journal of Pain Research 2023, 16:1301-1310
Published Date: 19 April 2023
Postoperative Pain Management Strategies Following Peroral Endoscopic Myotomy (POEM): A Review
Lu J, Ji W, Sang C, Wang Z, Bo L
Journal of Pain Research 2025, 18:2761-2773
Published Date: 31 May 2025
Serratus Posterior Superior Intercostal Plane Block and Serratus Anterior Plane Block Compared with Conventional Analgesia for Postoperative Analgesia in Breast Cancer Surgery: A Randomized Controlled Trial

Baytar MS, Baytar Ç, Kuyumcu BS, Köksal İncegül BG, Karadeniz Cakmak G
Journal of Pain Research 2026, 19:604864
Published Date: 13 May 2026